human intestinal microbiota - isim · • catheter-associated sepsis in icu patientsassociated...
TRANSCRIPT

Human Intestinal Microbiota&&
Clostridium difficile Infection
J. Bishara, M.D.Infectious Diseases UnitInfectious Diseases Unit
Rabin Medical Center; Beilinson Hospital

Microbes vs HumansMicrobes vs Humans
From the microbial perspective:“H b i thi th“Human beings are nothing more than
walking microbial planets”
Spellberg B et al. CID, Jan 15, 2008

Human MicrobiotaHuman MicrobiotaIt is difficult to say where the body ends and the microbes begin
• 100 trillions prokaryotes• 100 trillions prokaryotes
• 100 times > human cells
• Microbiome : – 150 time > human genes150 time > human genes

why do we carry billions of microbial species in our intestines?our intestines?

These inhabitants are crucial for ourThese inhabitants are crucial for our…
• Evolution
• Development
M t b li• Metabolism
• Immune defense
• Susceptibility to infections
• Susceptibility to noncommunicable diseases

The Multiple Immunomodulatory Activities of the Bacteroides fragilis Polysaccharide Molecule (PSac)
• Germ-free animals have defects in CD4 T-cell development
• Bacteroides fragilis corrects these• Bacteroides fragilis corrects these deficiencies through the expression of PSA
Mazmanian SK, et al. Cell 2005;122

Nature, Vol. 453, May 2008, , y


Purified PSA Protects against Experimental ColitisPurified PSA Protects against Experimental Colitis
Mazmannian et al, Nature, Vol. 453, May 2008

Nature 444, 1027-131 (21 December 2006)

An obesity-associated gut microbiome
Peter J. Turnbaugh et al. Nature 444, 1027-131 (21 December 2006)

Colonization Resistance”"Colonization Resistance


The role of human intestinal microbiota in the development of Clostridium-difficile associated disease
7
Goldberg E, Gofna U, Zafran M, Amir I, Bishara J
5
6
4
5
of c
opie
s)
Cdiff
2
3
Log
(no.
o
Clostridium sp.
Bacteroides sp.
1
2
0CD(-) D)-(CD(-) D(+)CD(+) D)-(CD(+) D(+)
Group
In press

Microbes R Us!!
AB as growth promoters in adults?!




Sub therapeutic antibiotics for 7 weeksFig 1
Sub-therapeutic antibiotics for 7 weeks
Fig 1

Fig 1

Fig 3

Proposed model for establishment of C. difficile-mediated dybiosis and successful bacteriotherapy
Lawley TD et al. PloS Pathogens, 25 October, 2012

• Obesity & CDI - both related to an increased Firmicutes/Bacteroidetes ratio in the intestinal microbiota.
• An association between obesity and CDI is unknown

Hypothesis & ObjectivesHypothesis & Objectives
• Hypothesis: obese patients might be more ibl Csusceptible to CDI
• Objective: to assess the association between b it d CDIobesity and CDI

MethodsMethods
• Retrospective case-control study• From January to December 2011y• All consecutive hospitalized patients with CDI• 2 IMDs / 2 hospitals• 2 IMDs / 2-hospitals• Controls:
di h h i li d d i h i d d i h– No diarrhea, hospitalized during the same period and in the same department
t h d (1 1) f (±5 ) d bidit– matched (1:1) for age (±5 years), gender, comorbidity, length of stay (LOS) ± 2 days, and antibiotic use during the last three months.last three months.

ExclusionsExclusions
• Aged ≤18 yrsP t• Pregnant
• Asymptomatic carriers of C. difficiley p ff• Lacked data for calculating the BMI &
Charlson scoreCharlson score
DefinitionsDefinitions
• Diarrhea: passage of 3 or > unformed stools for at least 2 consecutive days. y
• CDI -diarrhea not attributed to any other cause and associated with a positive stool test for Cand associated with a positive stool test for C. difficile toxin A/B
• EIA for C. difficile toxin A/B (TechLab, Inc., Blacksburg, VA, USA)Blacksburg, VA, USA)
• BMI (weight [Kg]/height2 [m2])

Statistical Analysis & EthicsStatistical Analysis & Ethics
• Mean values (±SD) • 2 for the categorical variables
S d ’ f i i bl• Student’s t - tests for continuous variables • Univariate analysis.• Multivariate model of Conditional Logistic Regression for matchedMultivariate model of Conditional Logistic Regression for matched
pairs– Stata12 Statistical Software (StataCorp LP® (College Station, TX, USA) was utilized
• Approved by the IRB of the Holy Family Hospital, Nazareth, and the ZivMedical Center, Safed.
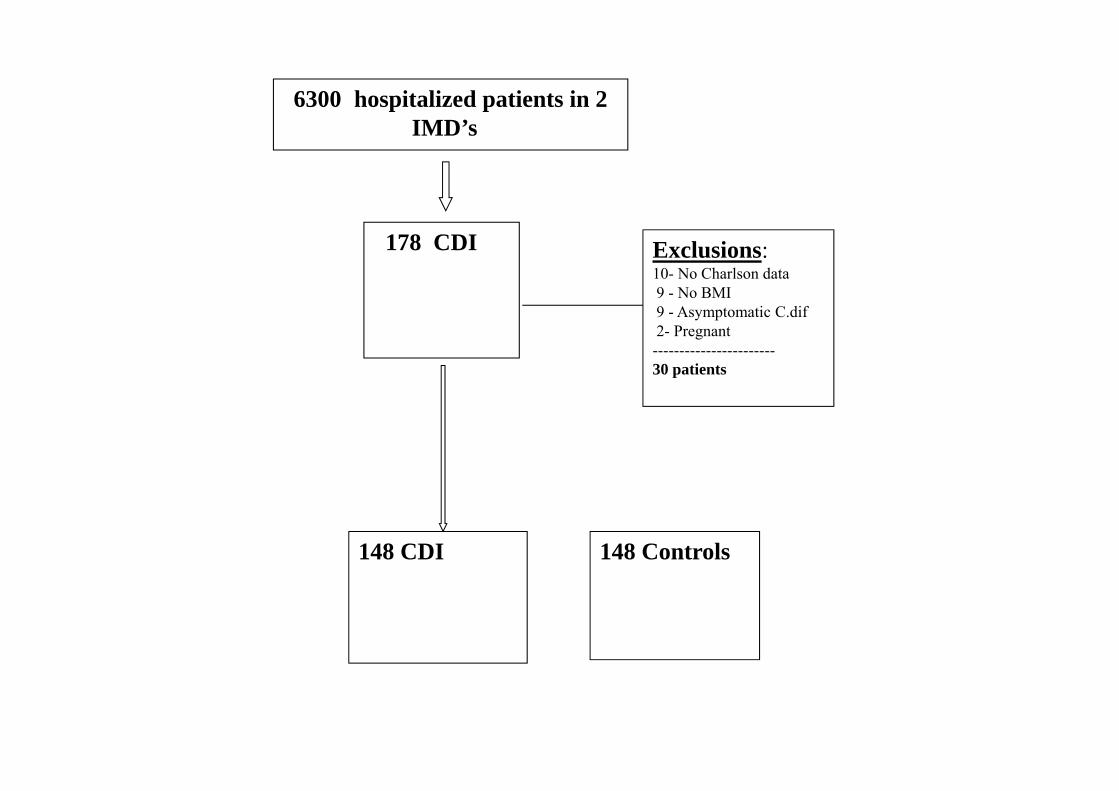
6300 hospitalized patients in 2IMD’sIMD’s
178 CDI Exclusions:10- No Charlson data9 - No BMI9 - Asymptomatic C.dif2- Pregnant-----------------------30 patients
148 Controls148 CDI



ResultsResults
• A difference of five points on the BMI scale l i il h i lamong people similar to those in our sample
(i.e., with higher-than-average BMI values) doubles the chance for having a CDI condition.
DiscussionDiscussion
• First study on association between CDI & obesityy
• Obesity is a significant and independent risk factor for CDIfactor for CDI
• BMI's "restriction-of-range" in our sample– Low BMI values were underrepresented

Obesity as a risk of several infectionsObesity as a risk of several infections
• Nosocomial bacteremia in elderly patients • Septic shockp• VAP• Catheter associated sepsis in ICU patients• Catheter-associated sepsis in ICU patients• Higher risk of ICU admission or death in patients
ith th 2009 i fl A (H1N1)with the 2009 influenza A (H1N1)
• Kaye KS, et al. J Am Geriatr Soc, 2011; Bercault N, et al. Crit Care Med, 2004; • Dossett LA, et al, 2009; Fezeu L et al. Obes Rev 2011.

Obesity associated comorbiditiesObesity associated comorbidities
• Type 2 DM• HypertensionHypertension• Atherosclerosis• Immune system dysregulation
– decreased cell-mediated immune responses– decreased cell-mediated immune responses• Respiratory dysfunction

Study LimitationsStudy Limitations
• Retrospective study, some CDI patients missed ??• Low sensitivity of the EIA Tox A/B, underestimated y
prevalence !• Cohort from a single countryCohort from a single country• CDI risk due to obesity per se or due to comorbidities
induced by obesity ?? significant on multivariateinduced by obesity ??, significant on multivariate analysis

ConclusionsConclusions
• Obesity should be considered as a risk factor for CDI • Further restriction and prudent use of antibiotics in p
obese patients is recommended• Future studies should focus on the relationshipFuture studies should focus on the relationship
between the increasing incidence of CDI and obesity in the USA and many western countriesin the USA and many western countries
• The exact mechanisms underlying the association between obesity and CDI remain to be fullybetween obesity and CDI remain to be fully understood and further studies are warranted

ThanksThanks