hyponatremia -my prensentation
TRANSCRIPT

HYPONATREMIA Guide: prof.(Dr.) P.S. Singh
HOD (Medicine)
Dr. Sudhir K. Yadav
Introduction
Hyponatremia is commonly defined as a serum sodium concentration below 135meq/L but can vary to a small degree in different clinical laboratories.

DETERMINANTS OF THE SERUM SODIUM CONCENTRATION "tonicity" (effective plasma osmolality) refers to the osmotic activity
of solutes that do not easily cross cell membranes and therefore determine the transcellular distribution of water
The extracellular and intracellular fluids are in osmotic equilibrium, so plasma tonicity is equal to the effective intracellular osmolality and to the effective osmolality of the total body water (TBW)
Plasma tonicity = (Extracellular solute + Intracellular solute) —————————————————————— TBW

Exchangeable sodium salts (Nae) are the primary effective extracellular solute and exchangeable potassium (Ke) and its associated intracellular anions are the primary intracellular solutes; these solutes are the major determinants of the effective plasma osmolality
Approximately 30 percent of total body sodium and a smaller fraction of total body potassium are nonexchangable and therefore not osmotically active
Thus, plasma tonicity (effective plasma osmolality) can be expressed as:
Plasma tonicity ≈ (2 x Nae + 2 x Ke) ——————————— TBW
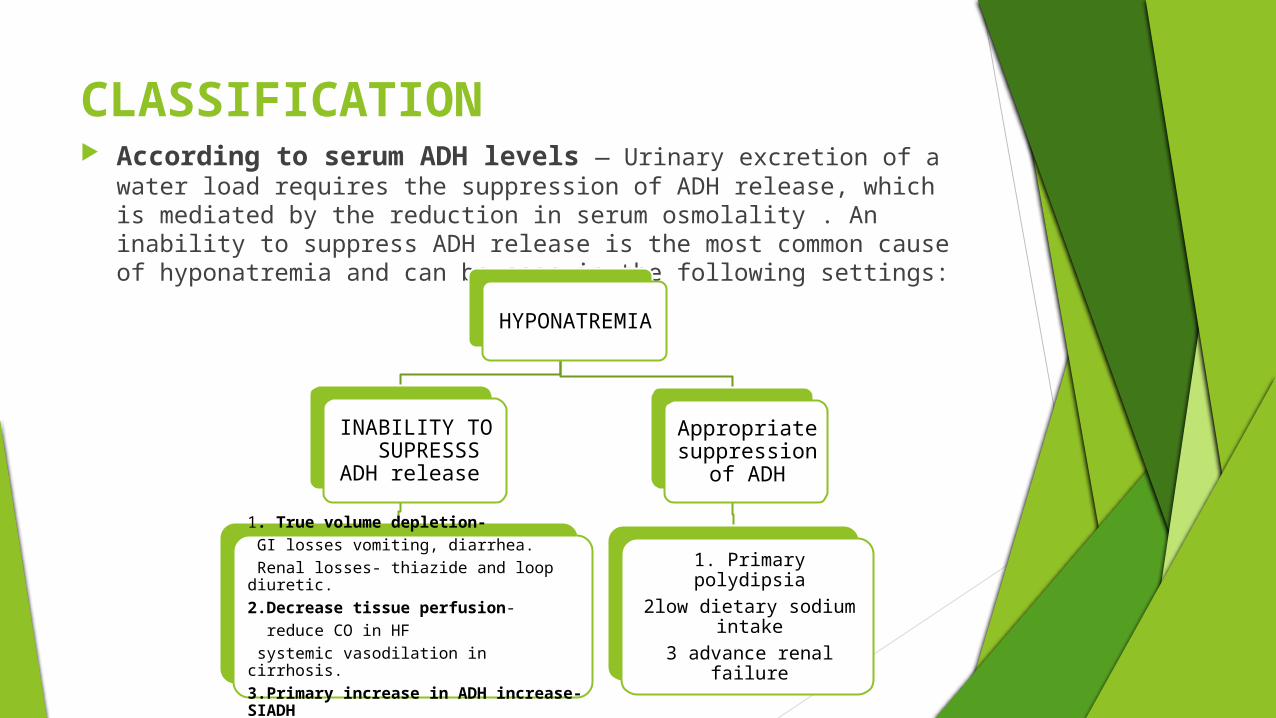
CLASSIFICATION According to serum ADH levels — Urinary excretion of a water
load requires the suppression of ADH release, which is mediated by the reduction in serum osmolality . An inability to suppress ADH release is the most common cause of hyponatremia and can be seen in the following settings:
HYPONATREMIA
INABILITY TO SUPRESSS
ADH release
1. True volume depletion- GI losses vomiting, diarrhea. Renal losses- thiazide and loop diuretic.2.Decrease tissue perfusion- reduce CO in HF systemic vasodilation in cirrhosis.3.Primary increase in ADH increase- SIADH
Appropriate suppression
of ADH
1. Primary polydipsia2low dietary sodium
intake3 advance renal failure

According to volume status
According to volume status
Hypovolumia1. GI losses2. Renal losses
Normovolumia1.SIADH2.Primary polydipsia3.Low dietary solute
Hypervolumia1.Heart failure 2.cirrhosis
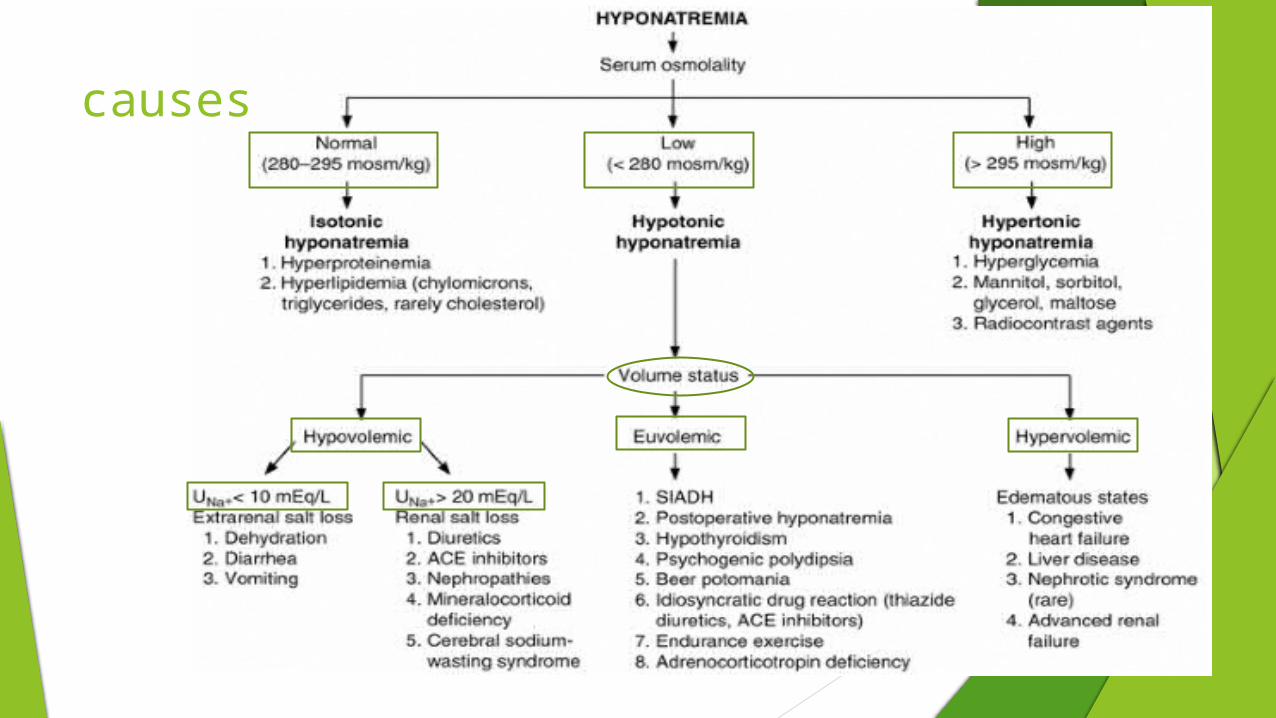
causes
Signs and symptom
Primarily neurological. Related to severity and particularly rapidity of
changes in the serum sodium concentration.
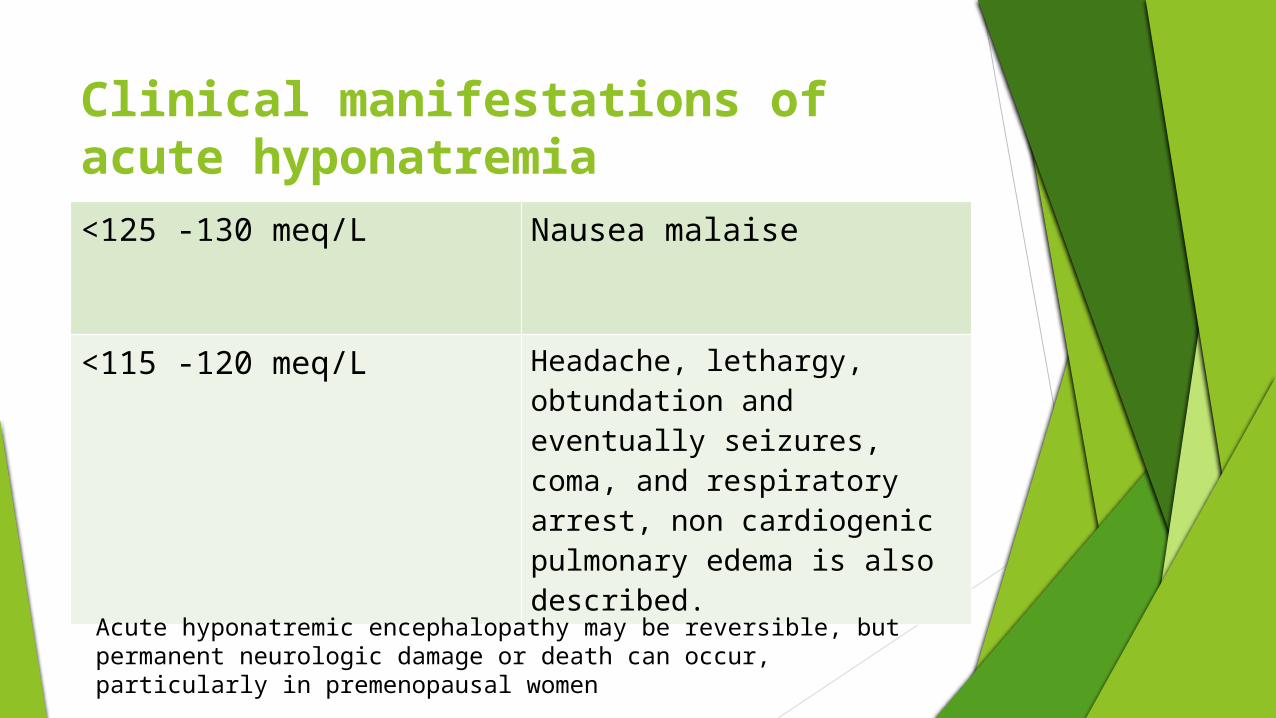
Clinical manifestations of acute hyponatremia<125 -130 meq/L Nausea malaise
<115 -120 meq/L Headache, lethargy, obtundation and eventually seizures, coma, and respiratory arrest, non cardiogenic pulmonary edema is also described.
Acute hyponatremic encephalopathy may be reversible, but permanent neurologic damage or death can occur, particularly in premenopausal women

ADAPTATION TO HYPONATREMIA
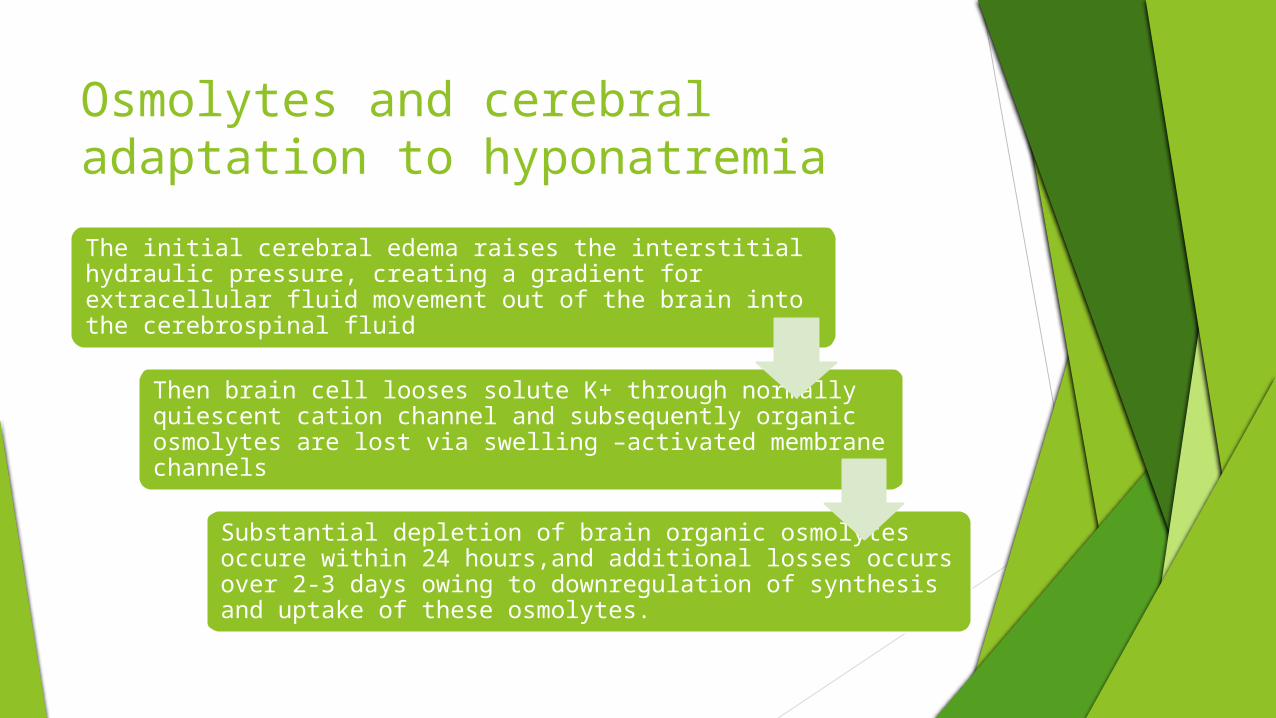
Osmolytes and cerebral adaptation to hyponatremiaThe initial cerebral edema raises the interstitial hydraulic pressure, creating a gradient for extracellular fluid movement out of the brain into the cerebrospinal fluid
Then brain cell looses solute K+ through normally quiescent cation channel and subsequently organic osmolytes are lost via swelling –activated membrane channels
Substantial depletion of brain organic osmolytes occure within 24 hours,and additional losses occurs over 2-3 days owing to downregulation of synthesis and uptake of these osmolytes.

Clinical manifestations of chronic hyponatremia The cerebral adaptation permits patients with chronic hyponatremia to
appear to be asymptomatic despite a serum sodium concentration below 120mmol/L. When symptoms occurs they are relatively nonspecific.
Fatigue Nausea Dizziness Gait disturbances Forgetfulness Confusion Lethargy Muscle cramps

Evaluation of patient with hyponatremia• A history of fluid loss (eg, vomiting, diarrhea, diuretic therapy)
and, on examination, signs of extracellular volume depletion, such as decreased skin turgor, a low jugular venous pressure (which is not diagnostic), or orthostatic or persistent hypotension.
● A history of low protein intake and/or high fluid intake.● A history consistent with one of the causes of SIADH, such as small cell carcinoma or central nervous system disease● Use of medications associated with hyponatremia.● Signs of peripheral edema and/or ascites, which can be due to heart failure, cirrhosis, or renal failure● Symptoms and signs suggestive of adrenal insufficiency or hypothyroidism.
HISTORY AND EXAMINATION

Laboratory tests
1. serum osmolarity 2. urine osmolarity 3. urine sodium potassium and chloride
concentration.

Finding in SIADH A low serum osmolality An inappropriately elevated urine osmolality (above
100 mosmol/kg and usually above 300mosmol/kg) A urine sodium concentration usually above 40 meq/L Low blood urea nitrogen and serum uric acid concentration A relatively normal serum creatinine concentration Normal acid-base and potassium balance Normal adrenal and thyroid function

MANAGEMENT
SODIUM DEFICIT FORMULA
Although sodium itself is restricted to the extracellular fluid, changes in the serum sodium concentration reflect changes in osmolality and are distributed through the total body water. TBW is estimated as lean body weight times 0.5 for women and 0.6 for men
Sodium deficit = TBW x (desired serum Na - actual serum Na)

Approach therapy of Hyponatremia
Patient risk stratification:
1. duration of hyponatremia 2. severety of hyponatremia 3. symptom of patient

Duration of hyponatremia
Hyperacute Within previous few hours
Acute Within previous 24 hr
Subacute Within 24- 48 hours
Chronic Within >48 hours

2. Severity of hyponatremia
Mild hyponatremia Serum sodium between 130-135 meq/L
Moderate hyponatremia Serum sodium between 121-129 meq/L
Severe hyponatremia Serum sodium between <120meq/L

3. Presence of symptoms
Absent symptoms Frequently
Mild to moderate symptoms Non specific nausea vomiting fatigue gait disturbance and confusion
Severe symptoms Seizure , obtundation, coma , respiratory arrest.
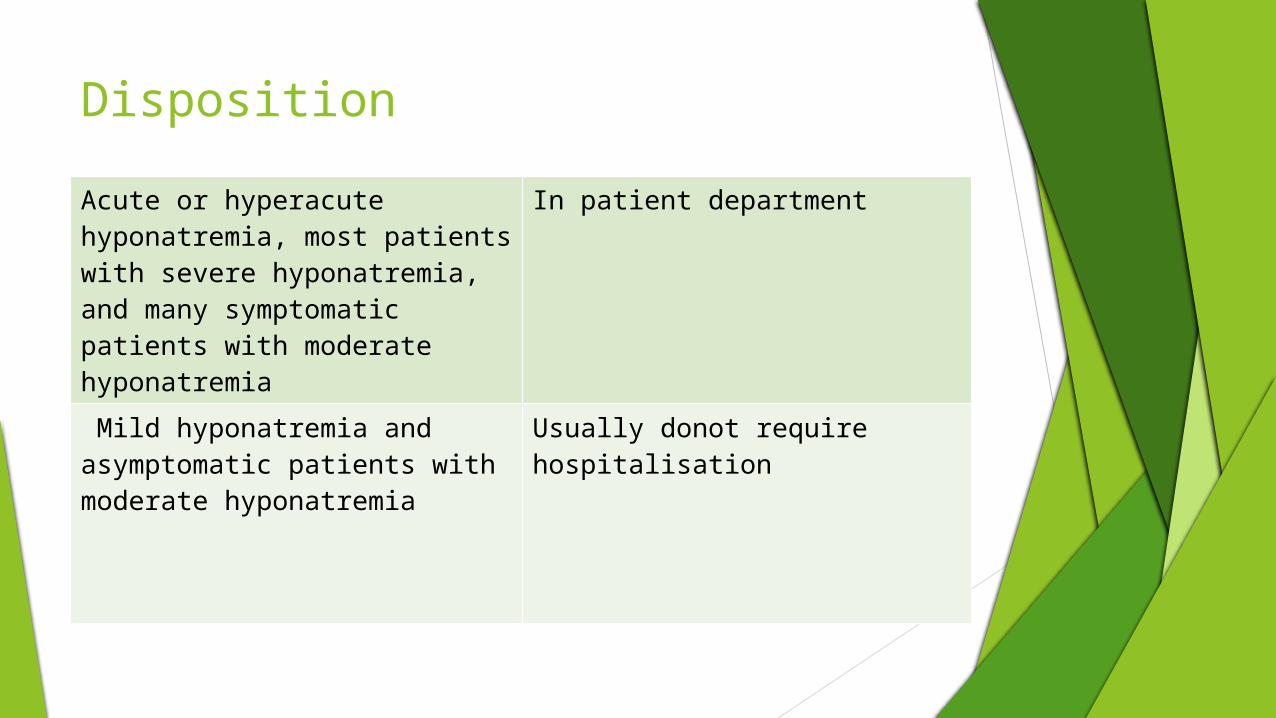
DispositionAcute or hyperacute hyponatremia, most patients with severe hyponatremia, and many symptomatic patients with moderate hyponatremia
In patient department
Mild hyponatremia and asymptomatic patients with moderate hyponatremia
Usually donot require hospitalisation
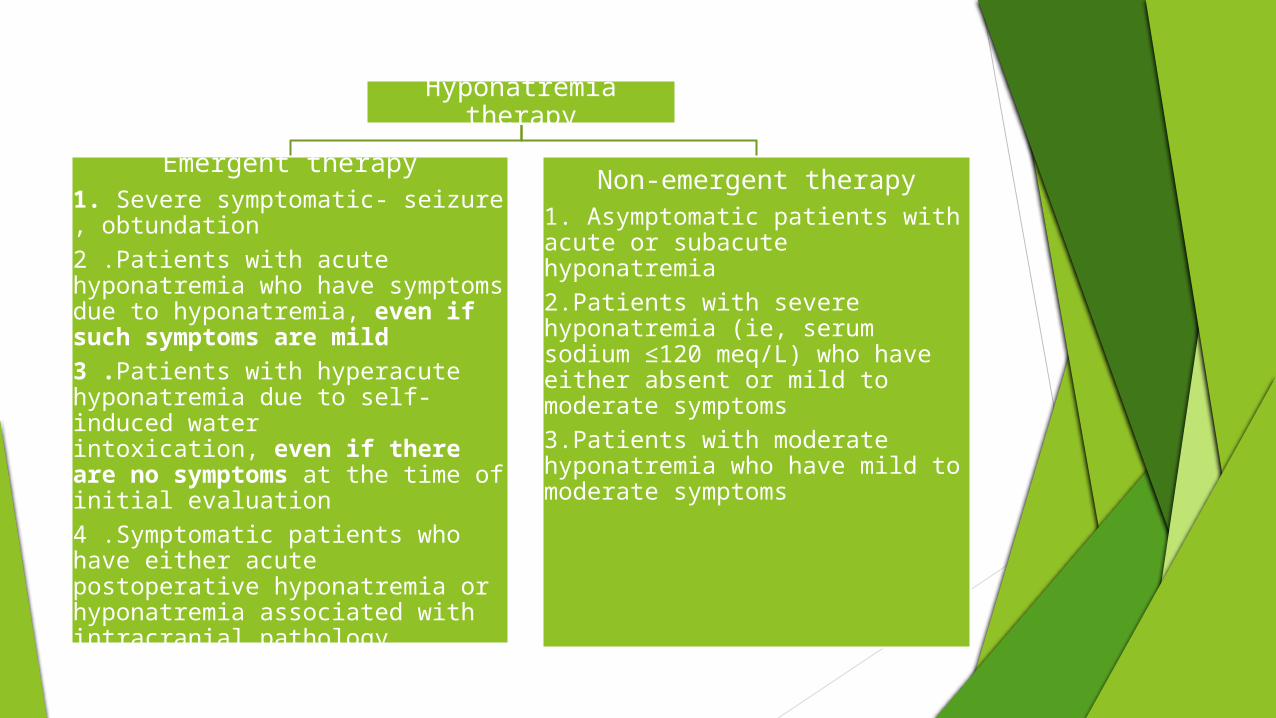
Hyponatremia therapy
Emergent therapy1. Severe symptomatic- seizure , obtundation2 .Patients with acute hyponatremia who have symptoms due to hyponatremia, even if such symptoms are mild3 .Patients with hyperacute hyponatremia due to self-induced water intoxication, even if there are no symptoms at the time of initial evaluation4 .Symptomatic patients who have either acute postoperative hyponatremia or hyponatremia associated with intracranial pathology
Non-emergent therapy1. Asymptomatic patients with acute or subacute hyponatremia2.Patients with severe hyponatremia (ie, serum sodium ≤120 meq/L) who have either absent or mild to moderate symptoms3.Patients with moderate hyponatremia who have mild to moderate symptoms

Goals of therapy
Emergent therapyrapidly increase the serum sodium by 4 to 6 meq/L over
a period of several hours. However, the increase in serum sodium should not
exceed 8 meq/L in any given 24-hour period.
Non-emergent therapyslowly raise the serum
sodium and alleviate symptoms. In general, raising
the serum sodium by 4 to 6 meq/L should improve a patient's symptoms. The increase in serum sodium
should not exceed 8 meq/L in any given 24-hour period
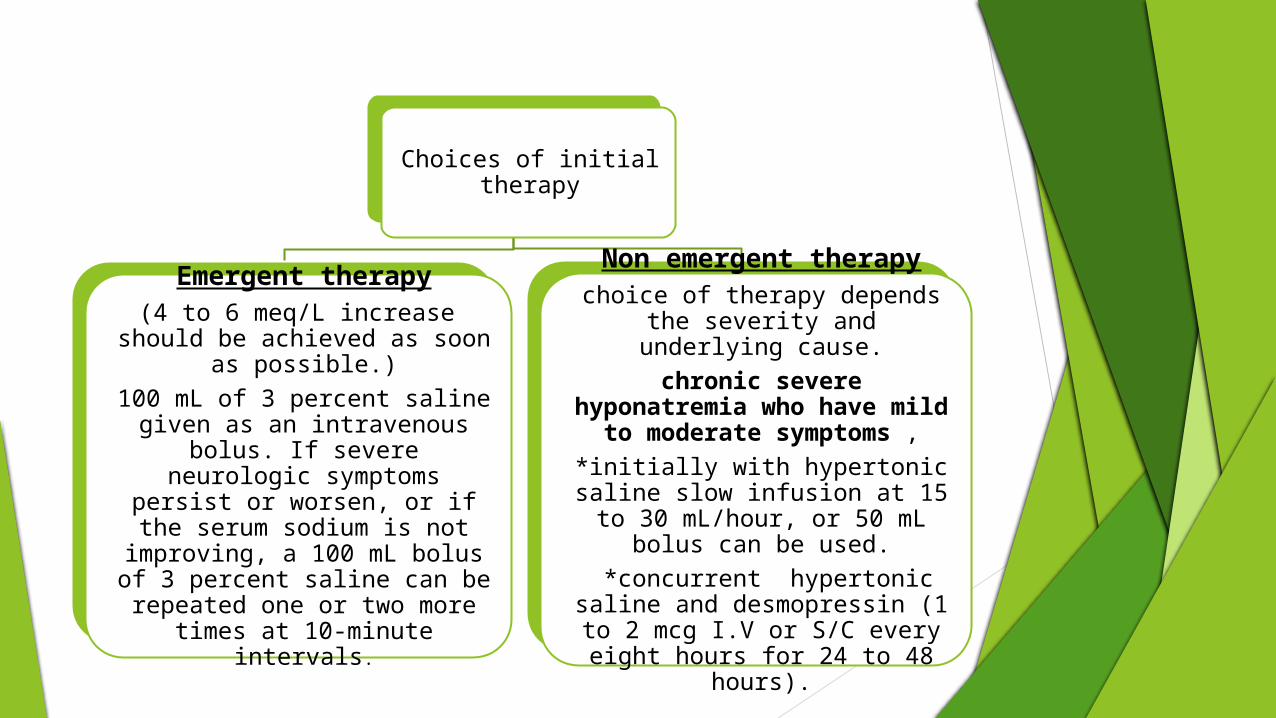
Choices of initial therapy
Emergent therapy(4 to 6 meq/L increase should
be achieved as soon as possible.)
100 mL of 3 percent saline given as an intravenous bolus. If severe neurologic symptoms
persist or worsen, or if the serum sodium is not
improving, a 100 mL bolus of 3 percent saline can be repeated one or two more times at 10-
minute intervals.
Non emergent therapychoice of therapy depends the severity and underlying cause.
chronic severe hyponatremia who have
mild to moderate symptoms ,
*initially with hypertonic saline slow infusion at 15 to
30 mL/hour, or 50 mL bolus can be used.
*concurrent hypertonic saline and desmopressin (1 to 2 mcg I.V or S/C every eight hours for
24 to 48 hours).
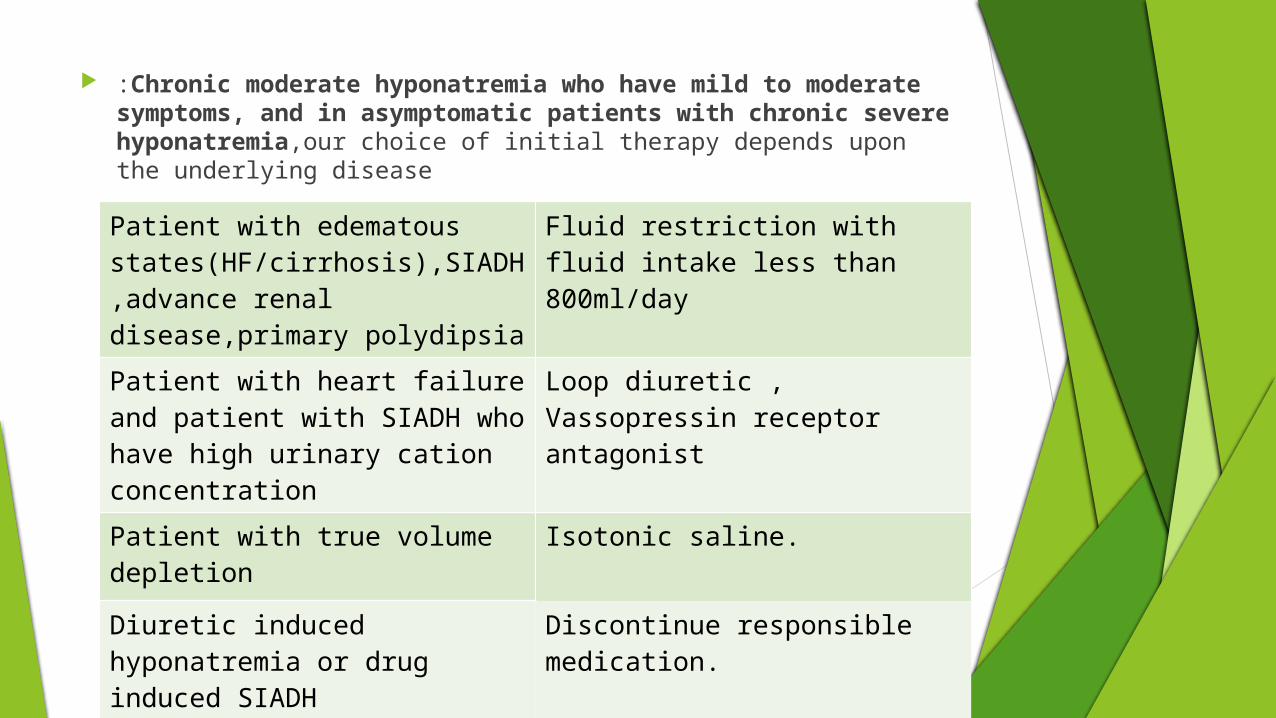
:Chronic moderate hyponatremia who have mild to moderate symptoms, and in asymptomatic patients with chronic severe hyponatremia,our choice of initial therapy depends upon the underlying disease
Patient with edematous states(HF/cirrhosis),SIADH,advance renal disease,primary polydipsia
Fluid restriction with fluid intake less than 800ml/day
Patient with heart failure and patient with SIADH who have high urinary cation concentration
Loop diuretic ,Vassopressin receptor antagonist
Patient with true volume depletion
Isotonic saline.
Diuretic induced hyponatremia or drug induced SIADH
Discontinue responsible medication.

Regimen of hypertonic saline with or without desmopressin in the nonemergent setting Asymptomatic patients with acute hyponatremia and mildly or
moderately symptomatic patients with chronic severe hyponatremia should generally receive hypertonic saline. the total elevation in serum sodium should be 4 to 6 meq/L and no more than 8 meq/L in any given 24-hour period
Acute asymptomatic hyponatremia
50 mL hypertonic saline over 10 minutes. Two or three additional boluses of 50 to 100 mL can be given if symptoms develop and/or the serum sodium does not improve.
Severe chronic hyponatremia with mild or moderate symptoms
I.V. inf. hypertonic saline at 15 to 30 mL/hour, usually in combination with desmopressin at 1 to 2 mcg IV or SC q8h for 24 to 48 hours. The infusion rate should be titrated, aiming for a correction rate of 6 meq/L per day.**Frusemide can be given with hypertonic saline in edematous patient
*Desmopressin should not be used in self induced water intoxication edematous pt and pt with known chronic SIADH.

CONDITION IN WHICH HYPERTONIC SALINE IS NOT REQUIRED chronic moderate hyponatremia who have mild to
moderate symptoms, asymptomatic patients with severe hyponatremia.
*Fluid restriction,±loop diuretic,vasopressin receptor antagonist occasionally
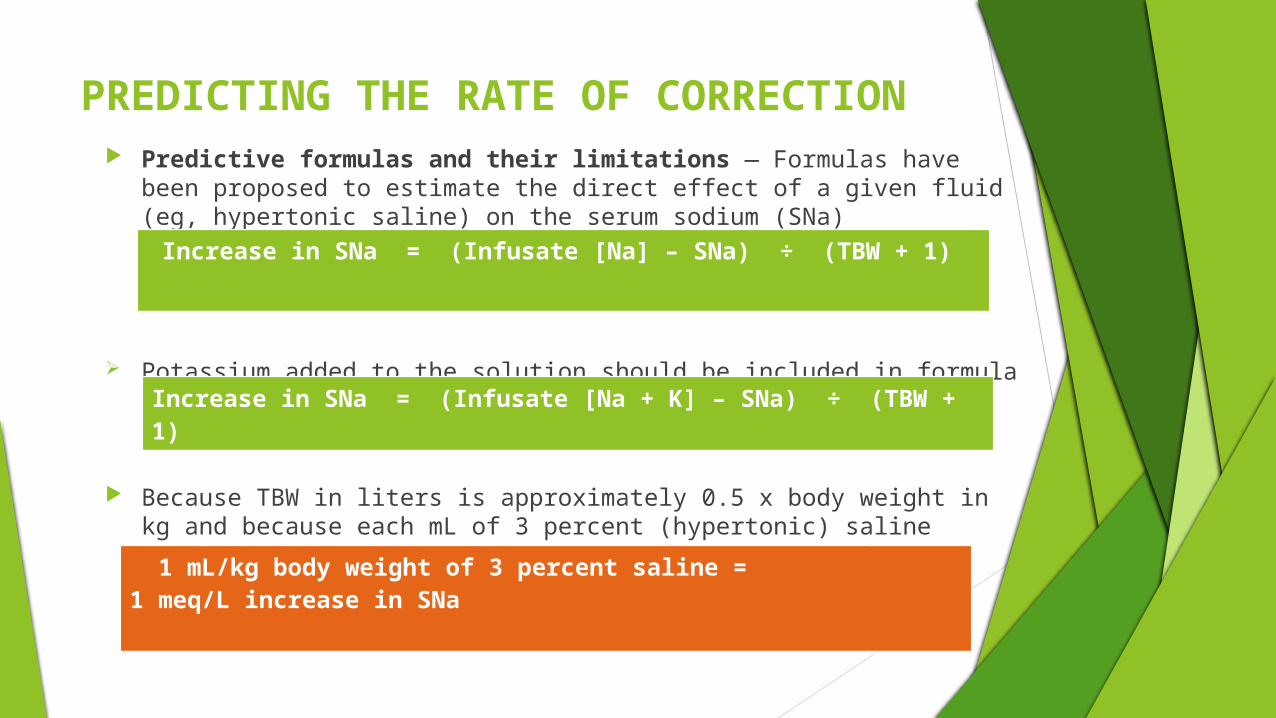
PREDICTING THE RATE OF CORRECTION Predictive formulas and their limitations — Formulas have been
proposed to estimate the direct effect of a given fluid (eg, hypertonic saline) on the serum sodium (SNa) concentration, for example
Potassium added to the solution should be included in formula
Because TBW in liters is approximately 0.5 x body weight in kg and because each mL of 3 percent (hypertonic) saline contains 0.5 meq of sodium, a simplified version of the formula predicts:
Increase in SNa = (Infusate [Na] – SNa) ÷ (TBW + 1)
Increase in SNa = (Infusate [Na + K] – SNa) ÷ (TBW + 1)
1 mL/kg body weight of 3 percent saline = 1 meq/L increase in SNa

Osmotic demyelination syndrome Overly rapid correction of
hyponatremia(almost always 120 meq/L or less and 115 meq/L
Demyelination is more diffuse and does not neccesorly involve pons.
manifestations of ODS are typically delayed for two to six days after overly rapid elevation of the serum sodium concentration
dysarthria, dysphagia, paraparesis or quadriparesis, behavioral disturbances, lethargy, confusion, disorientation, obtundation, and coma; seizures may also be seen but are less common. Severely affected patients may become "locked in"; they are awake, but are unable to move or communicate

Monitoring of therapy Patients receiving emergent therapy should have their serum sodium
measured every two hours. patients who are treated for chronic hyponatremia in the hospital
should have their serum sodium measured every four hours. the urine output should be monitored, and, if increasing, the urine
osmolality, urine sodium, and urine potassium should be measured. An increase in urine output and a decrease in the urine cation concentration can signify that the rate of correction is accelerating.
If the risk of overly rapid correction is low, the frequency of measurements can be reduced, but measurements should still be taken at least every 12 hours until the serum sodium is 130 meq/L or higher.
If desmopressin is given concurrently with hypertonic saline, the frequency of monitoring can be reduced to every six hours once the desired rate of correction has been achieved because, with this regimen, there is a lower likelihood of inadvertent overly rapid correction.

Choice of therapy in case of SIADHSEVERE SYMPTOMS Hypertonic saline (100 ml I.V. 3% NaCl
given as bolus increases S. Na approximately 1.5 meq/L in men and 2 meq/L in women.)
MILD TO MODERATE SYMPTOMS
Initially hypertonic saline to raise the S. sodium @ 1meq/L/hr may be justified in first 3-4 hours then maintainance therapy
MAINTAINANCE THERAPY
Fluid restriction 800 ml/dayOral salt 3 grams or one and half tsf TDS, total dose of 9 gms/day

THANK YOU

PSEUDOHYPONATREMIA
Pseudohyponatremia, which is associated with a normal serum osmolality, refers to those disorders in which marked elevations in serum lipids or proteins result in a reduction in the fraction of serum that is water and an artificially low serum sodium concentration