iabp troubleshooting
TRANSCRIPT

IABP troubleshooting Dr Siva Subramaniyan
PGIMER &Dr.RML Hospital
New Delhi

IABP
• The intra-aortic balloon pump (IABP) is a mechanical device that is temporarily used to improve cardiac function.
• In many situations, the IABP is life-saving in its ability to stabilize patients as they await procedures such as heart transplant, coronary artery bypass grafting (CABG), or percutaneous coronary interventions (PCI) such as PTCA.
• An IABP may be further indicated in the management of cardiogenic shock

Basic principles of counterpulsation
• Counterpulsation (augmentation) is a term that describes balloon inflation in diastole and deflation in early systole.
• Balloon inflation causes ‘volume displacement’ of blood within the aorta, both proximally and distally. This leads to a potential increase in coronary blood flow and potential improvements in systemic perfusion by augmentation of the intrinsic ‘Windkessel effect’, whereby potential energy stored in the aortic root during systole is converted to kinetic energy with the elastic recoil of the aortic root.



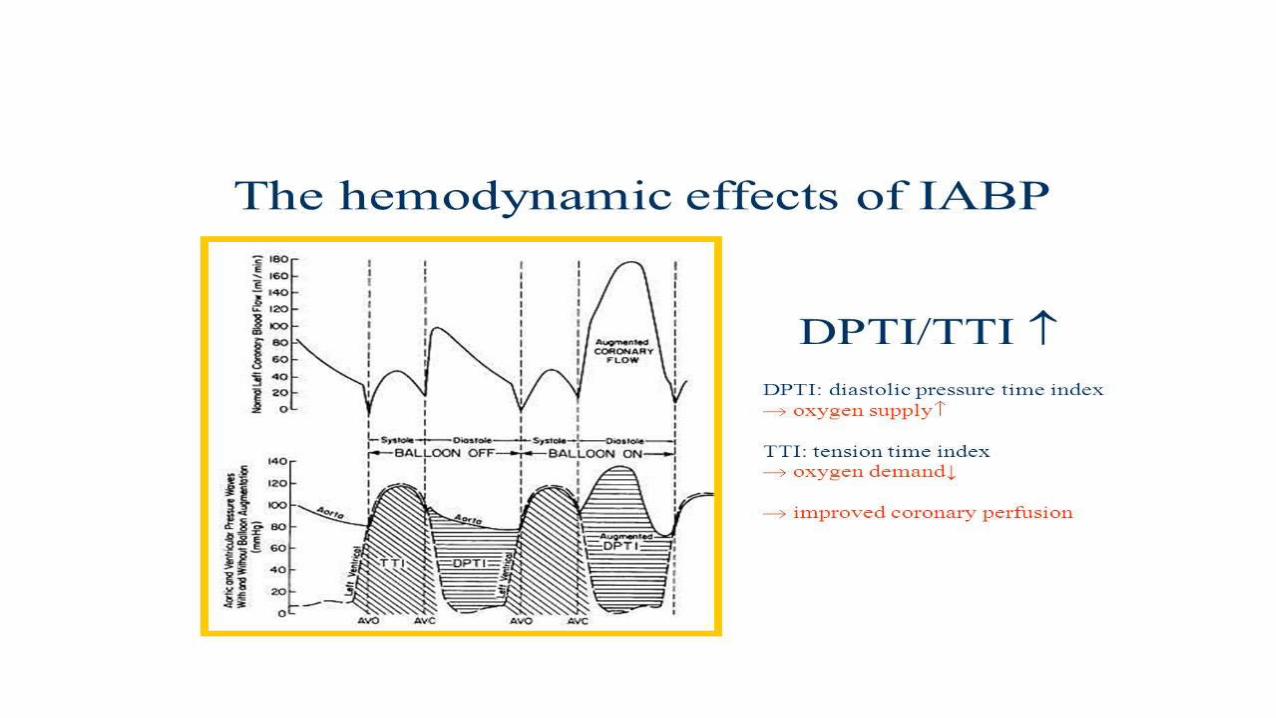
Physiological effects of IABP therapy
• The primary goal of IABP treatment is to improve the ventricular performance of the failing heart by facilitating an increase in myocardial oxygen supply and a decrease in myocardial oxygen demand.



Expected changes with IABP support in hemodynamic profile in patients with Cardiogenic shock
- Decrease in SBP by 20 %
- Increase in aortic Diastolic Press. by 30 % ( raise coronary blood flow)
- Increase in MAP
- Reduction of the HR by 20%
-Decrease in the mean PCWP by 20 %
- Elevation in the COP by 20%

• Although these effects are predominately associated with enhancement of LVperformance, IABP may also have favourable effects on right ventricular (RV)function by complex mechanisms including accentuation of RV myocardial bloodflow, unloading the left ventricle causing reduction in left atrial and pulmonaryvascular pressures and RV afterload.
• IABP inflates at the onset of diastole, thereby increasing diastolic pressure anddeflates just before systole, thus reducing LV afterload

The magnitude of these effects depends upon:
(i) Balloon volume: the amount of blood displaced is proportional to the volume of the balloon.
(ii) Heart rate: LV and aortic diastolic filling times are inversely proportional to heart rate; shorter diastolic time produces lesser balloon augmentation per unit time.
(iii) Aortic compliance: as aortic compliance increases (or SVR decreases), the magnitude of diastolic augmentation decreases.


14
IABP –instrumentation and techniques

15
The IAB Counter pulsation system
two principal partsA flexible catheter -2 lumen
• first - for distal aspiration/flushing or pressure monitoring • second - for the periodic delivery and removal of helium gas to a closed balloon.
A mobile console • system for helium transfer • computer for control of the inflation and deflation cycle

BALLOON
IABP catheter:
• 10-20 cm long polyurethane bladder
• 25cc to 50cc capacity
• Optimal 85% of aorta occluded (not 100%)
• The shaft of the balloon catheter contains 2 lumens:
- one allows for gas exchange from console to balloon
- second lumen for catheter delivery over a guide wire formonitoring of central aortic pressure after installation.

17
BALLOON SIZING
Sizing based on patients height
Four common balloon sizes
Balloon length and diameter increases with each larger size
40 cm³ balloon is most commonly used
Paediatric balloons also available : sizes 2.5, 5.0, 12.0 and 20 cm³
Balloon size Height
50 cm³ > 6 feet
40 cm³ 5 feet 4 inch
to 6 feet
34 cm³ 5 feet to 5
feet 4 inch
25 cm³ < 5 feet

18
INTRA AORTIC BALLOON

TIP





24
- The end of the balloon should be just distal (1-2 cm) to the takeoff of the left subclavian artery
- Position should be confirmed by fluoroscopy or chest x-ray
POSITIONING

25
Connecting to console: - Connect helium gas tube to the console via a long extender - Open helium tank.
- The central lumen of the catheter is flushed and connected to pressure tubing with 3 way and then to a pressure transducer to allow for monitoring of central aortic pressure.
- Zero the transducer
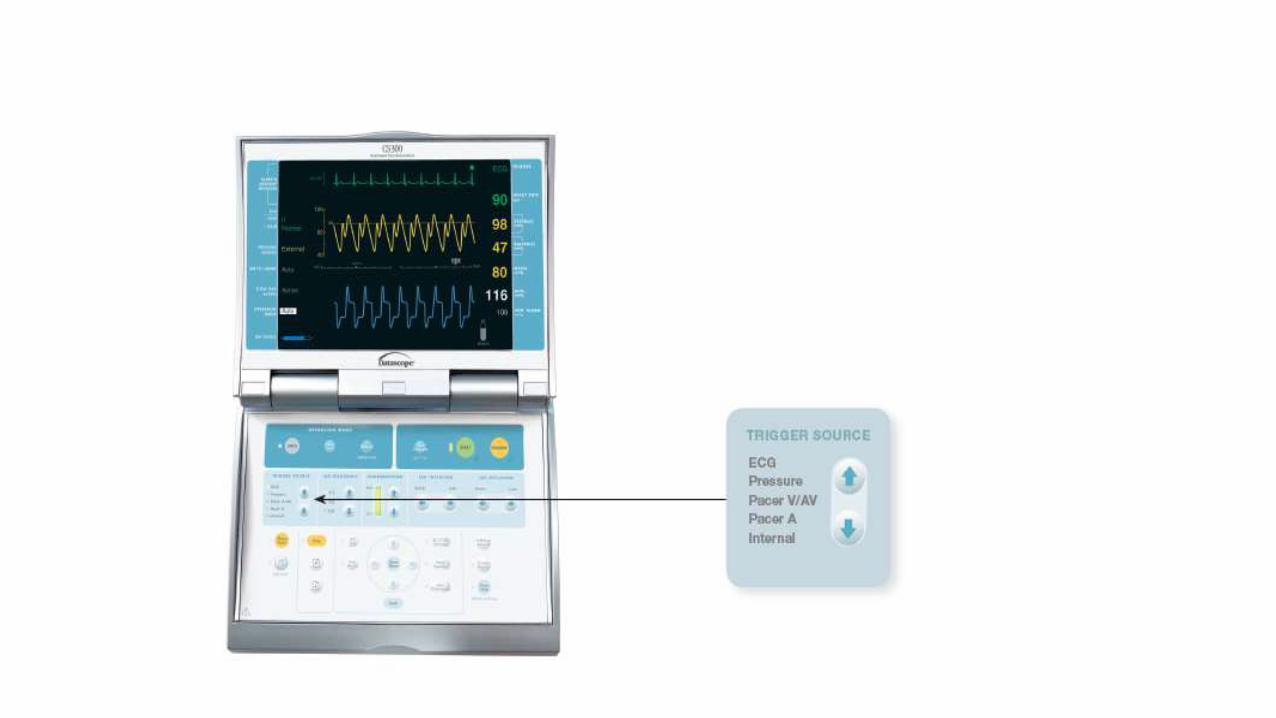
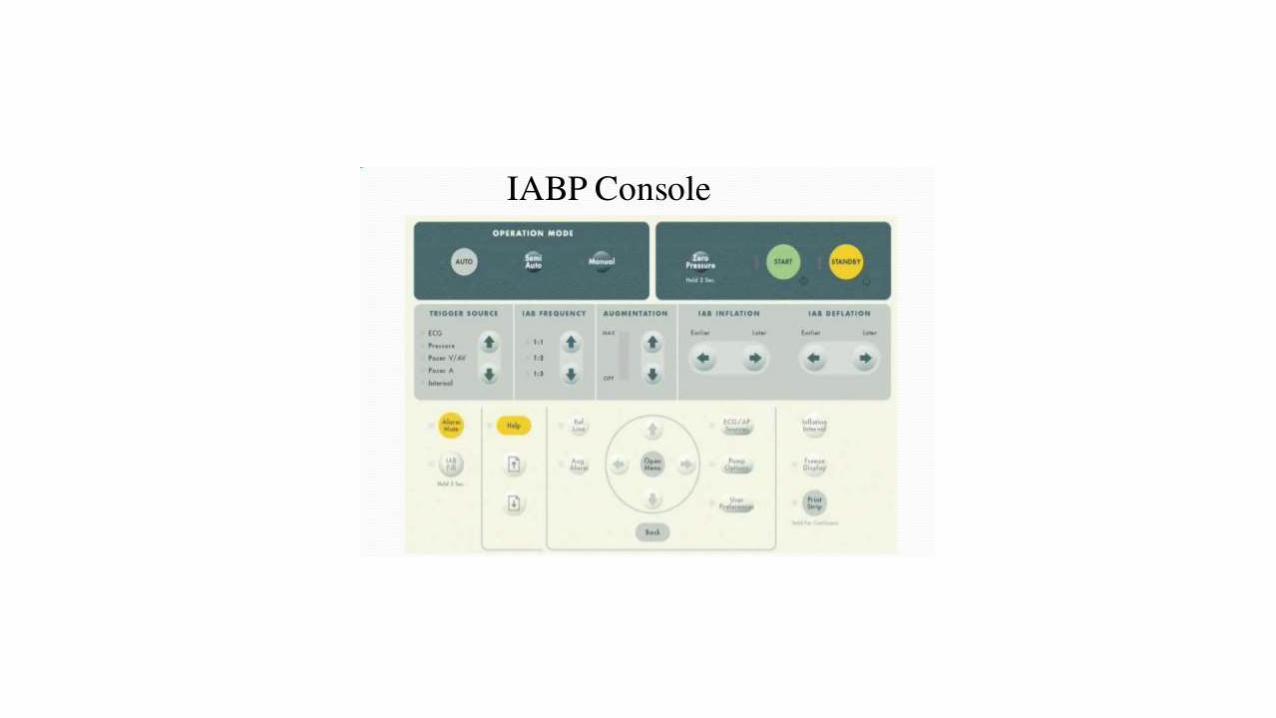
Initial set-up:- Once connected properly the console would show ECG and pressure
waveforms.- Check Basal mean pressure- Make sure the setting is at “auto”- Usually IABP started at 1:1 or 1:2 augmentation- Usually Augmentation is kept at maxim

Modes of operation:
• The trigger can be “automatic”, the computer sets trigger source, computer sets inflation and deflation times. Trigger automatically searches for most optimal source if initial trigger is not detected.
• The Trigger can also be “semi automatic” the operator sets the source, operator sets initial inflation and deflation times. Computer will determine subsequent timing intervals.

30

31
32




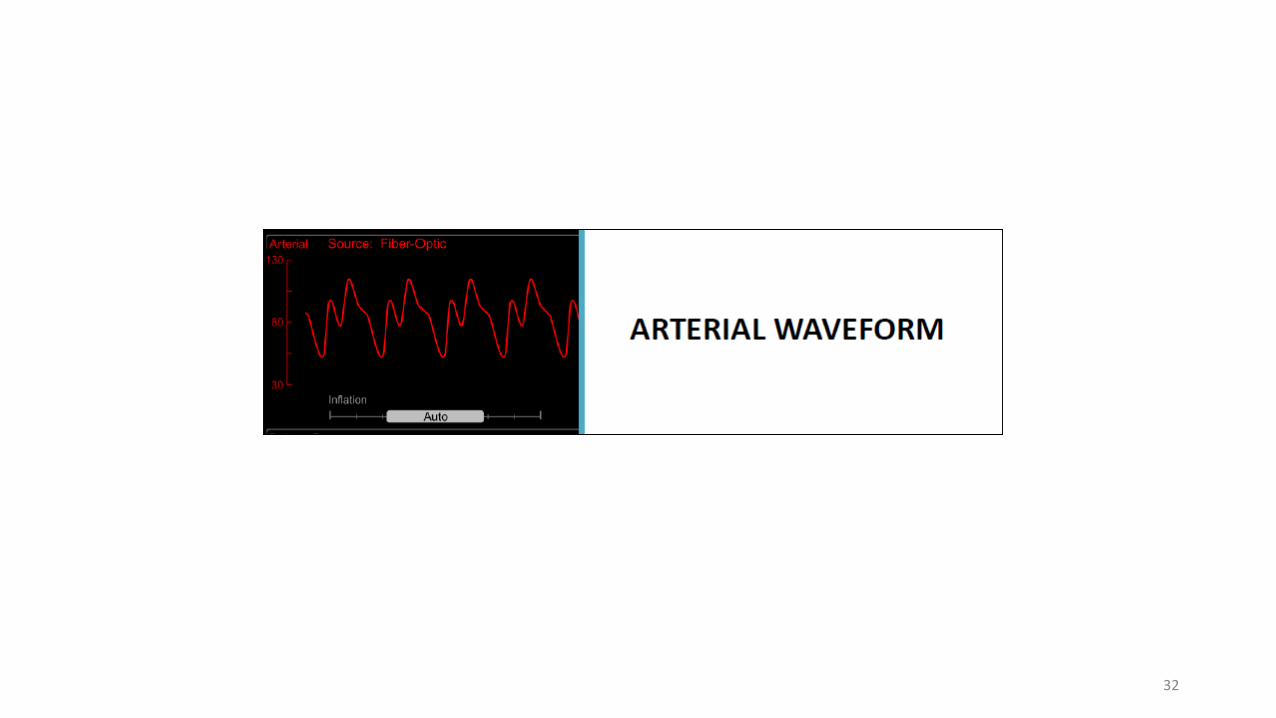
waveform is acceptable ?
• First change from 1:1 to 1:2 augmentation
• Check the dicrotic notch
• As the balloon inflates at the onset of diastole, a sharp and deep ‘V’ is observed at the dicrotic notch. Balloon inflation causes augmentation of diastolic pressure and a second peak is observed. This peak is referred to as diastolic augmentation. Diastolic augmentation is ideally higher than the patient’s systolic pressure except when reduced stroke volume causes a relative decrease in augmentation


2) Confirm if end diastolic wave following the augmented wave is less than an non augmented wave.

• The balloon aortic end-diastolic pressure is 5 mmhg to 10 mmhg less than the patient’s aortic end-diastolic pressure and
• The assisted systolic pressure is 5 mmhg to 10 mmhg less than the patient’s previous systolic pressure


41
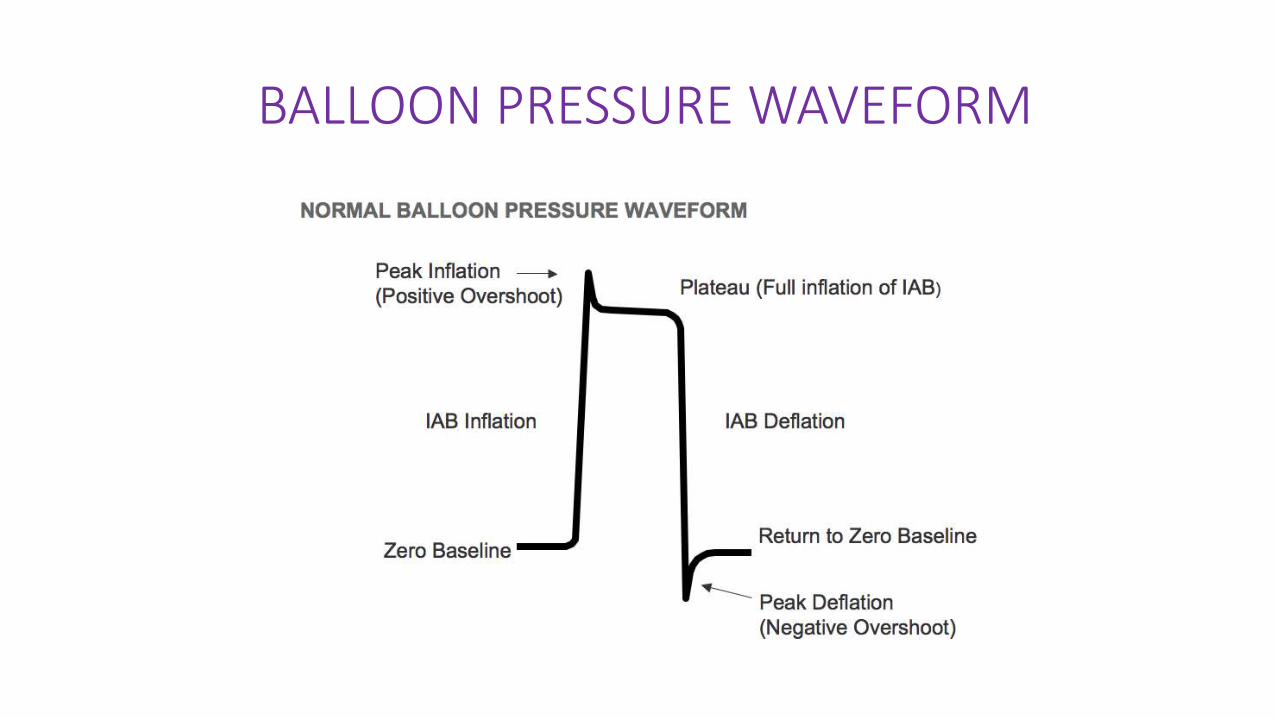
BALLOON PRESSURE WAVEFORM

TROUBLESHOOTING OF IABP
TROUBLESHOOTING
• Challenges can occur when IABP therapy is used in the CCU. The most frequent causes for IABP malfunction include the possibility that the
- balloon may not adequately augment CO,
- ECG trigger may not be functioning properly, or
- autofill function may fail

1) Augmentation below the set limit
Reasons for low diastolic augmentation include the following issues:
● Incorrect timing of balloon inflation and deflation. This problem can be corrected by adjusting inflation and deflation on console.
● Leak in the balloon catheter. Occasionally balloons can rupture or tear. This problem warrants prompt changing of the balloon catheter.
● Leak in the gas circuit resulting in poor inflation. Check all connections from the catheter to the gas cylinder and tighten them as necessary.
●Balloon not unwrapped completely. This issue results in poor or incomplete opening of the balloon. Check the position of the catheter with an x-ray. Attempt to inflate the balloon with an appropriate-sized syringe. If this measure is unsuccessful, the catheter will need to be replaced.
● Poor cardiac function or low vascular resistance. If appropriate, add positive inotropic agents and vasoactive agents.
● Dysrhythmias such as atrial fibrillation or ventricular tachycardia that result in low stroke volume. To correct these conditions, administer antiarrhythmics as ordered, and improve oxygen and electrolyte imbalances.


EARLY INFLATION

DELAYED INFLATION

EARLY DEFLATION

LATE DEFLATION

2) NO TRIGGER
• On occasion, the ECG trigger may not function properly.
• Common causes of a faulty trigger include poor electrode placement, low ECG voltage, faulty electrode pads or cables, dysrhythmias, and other equipment’s interference with the ECG signal.
• If the problem cannot be easily rectified, switching to the arterial pressure trigger will be necessary until the problem can be solved.
3) Autofill Failure
• The autofill feature on the IABP maintains the volume of gas within the balloon. if this feature is not functioning properly, an autofill alarm will sound. The cause of this problem could be an insufficient amount of gas in the tank or occlusion of the gas outlet. The amount of gas in the tank should be checked and the tank replaced as needed.


4) Check IAB Catheter

5) IAB Disconnected

6) Prolonged Time in Standby

3) Rapid Gas Loss or Leak in IAB Circuit
59
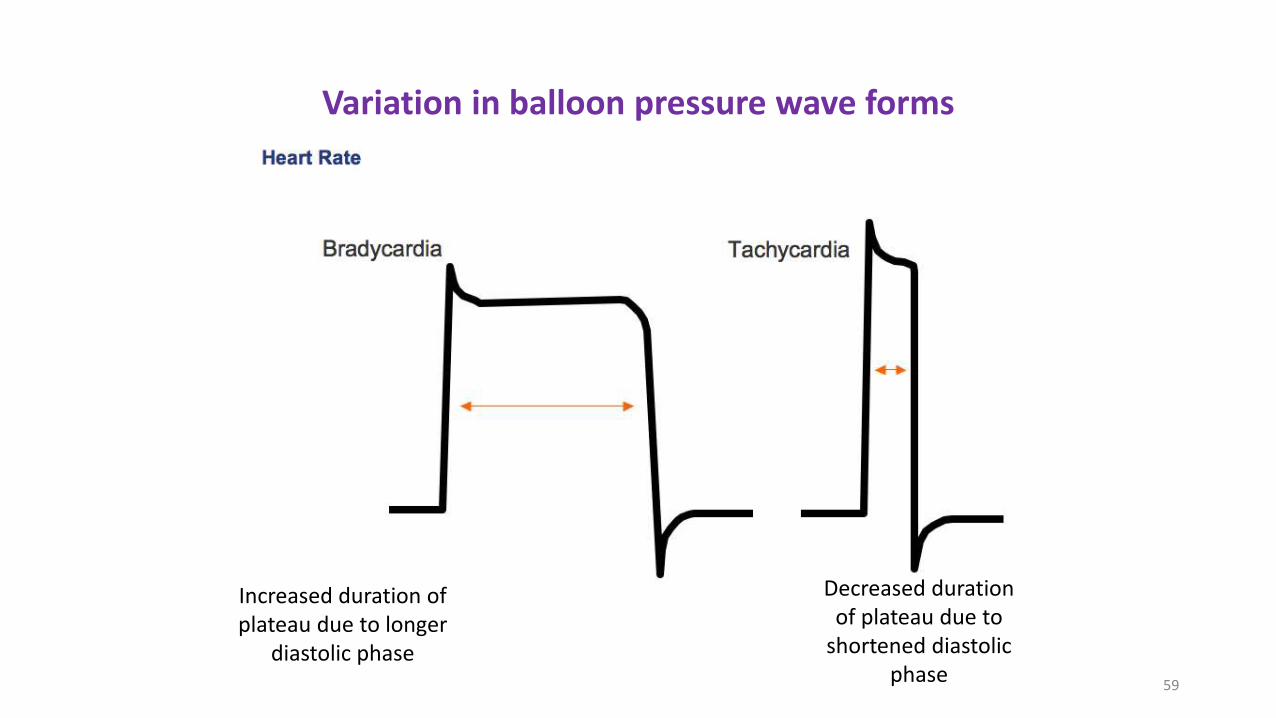
Variation in balloon pressure wave forms
Increased duration ofplateau due to longer
diastolic phase
Decreased durationof plateau due to
shortened diastolicphase

60
Variation in balloon pressure wave forms
Varying R-R intervalsresult in irregularplateau durations

61
Variation in balloon pressure wave forms
Increased heightor amplitude ofthe waveform
Decreased heightor amplitude of thewaveform

62
Variation in balloon pressure wave forms
Gas leak
Leak in the closed system causing theballoon pressure waveform to fall belowzero baseline..
- due to a loose connection- a leak in the IAB catheter- H2O condensation in the external tubing- a patient who is tachycardiac and febrile which causes increased gasdiffusion through the IAB membrane

63
CATHETER KINK
Rounded balloon pressure waveform- Loss of plateau resulting from a kink or
obstruction of shuttle gas
- Kink in the catheter tubing- Improper IAB catheter position- Sheath not being pulled back to allow
inflation of the IAB- IAB is too large for the aorta- IAB is not fully unwrapped

64
“Balloon too large” syndrome



ACC/AHA 2013Practice Guidelines (ESC 2012- IIb)
67

ESC 2014 GUIDELINES
68





THANK YOU