liverpool sdl iabp
TRANSCRIPT
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 1/26
Liverpool Health ServiceIntensive Care Unit
Self Directed Learning Package:
Intra-Aortic Balloon Pumping
Written by: Linda Williams
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 2/26
How to use this package
This package is designed to be used in the clinical area as a self directed learning tool.
At the start of the package is a pre test which covers the information contained inside.
You should read through the pretest and answer the questions. If you have any
problems with any of the questions, this will provide you with some guidance as to
the areas that you should focus on in the package.
The package is divided into sections. At the end of each section is a self test to
determine how well you have understood the information contained in that section.
You will need to complete the self tests at the end of each section and ensure that you
have mastered the content before moving on to the next section.
If you have any trouble with the self test, go back over the section and revise the
content. If you are still unsure then you will need to speak with one of the educators in
your area.
Once you have worked through the entire package, you should complete the post test.
The answers to the post test are contained at the end of the package. If you have any
trouble with the post test, go back to the section in the package and revise it. If you
are still unsure, contact the educator in your area.
GOOD LUCK!!!
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 3/26
Learning package objectives
By the completion of this package, the registered nurse will be able to:
1. Discuss the indications for intra-aortic balloon pumping in the Intensive Care
Unit.
2. Discuss the insertion procedure and catheter position
3. Identify correct timing of balloon inflation and deflation
4. Describe the physiological effects of IABP
5. Discuss trouble shooting timing errors in balloon inflation and deflation
6. Discuss nursing management of IABP
• Weaning
• Complications
• Troubleshooting machine problems
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 4/26
Pretest
1. Why is an IABP used?
2.
What are the effects that are achieved when using IABP therapy?
3. Describe the mechanism of counterpulsation?
4. Why is helium used to inflate the balloon?
5. Describe the correct positioning of the IAB Catheter. Why is it important?
6. Why is the size of the IABP important?
7.
What are the two ways that ECG and pressure can be monitored to use the IABP?
8. Why is correct timing important for the patient?
9. When should the IAB be inflated, and what is the effect of inflation?
10. When should the IAB be deflated, and what is the effect of deflation?
11.
Discuss the complications associated with the use of the IABP?
12. How is weaning achieved at Liverpool Hospital? What other ways can weaning
be achieved?
13. What are the signs of failure to wean an IABP?
14. What does augmentation mean on the IABP? What is the most common problem
if augmentation is not full?
15. How long should an IABP Catheter remain insitu and not operating, and why not
any longer?
16. During a cardiac arrest, what mode should be used for the IABP?
17. What actions should be taken if a patient requires defibrillation while requiring
IABP therapy?
18. What effect do pacemakers have on the timing of the IABP?
19. Describe the nursing care required for a patient on the IABP?
20. What is the correct procedure if the IABP fails?
21.
What would you do if you lose your trigger for the IABP?
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 5/26
22. How would you tell if your IAB catheter had ruptured? What procedure would
you use if this occurred?
23. In AF what is the best way to maximise therapy?
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 6/26
Introduction
The Intra-Aortic Balloon Pump (IABP) is a circulatory assist device that is used to
support the left ventricle. The IABP uses counterpulsation where aortic blood is
displaced with the inflation and deflation of the balloon catheter, which is timed to the
cardiac cycle. Couterpulsation provides both an augmented diastolic arterial pressureand an decreased end-diastolic pressure. The balloon is connected to a console that
regulates the inflation or deflation of the balloon with the passage of helium. Helium
is used as it is easily dissolved in blood and prevents the risk of air emboli if the
catheter ruptures.
The IABP has the following effects:
• Increases coronary artery perfusion
•
Increases myocardial oxygen supply
• Decreases myocardial oxygen demand
• Decreases myocardial work by reducing afterload
• Increases blood pressure
• Decreases Pulmonary artery pressure
Indications
The IABP is used in:-
• Acute left ventricular failure post cardiac surgery
• Severe unstable angina
• Cardiogenic shock post myocardial infarction
• Bridge to cardiac transplantation
• Stunned myocardium after myocardial infarction
Contraindications
• Severe aortic insufficiency
• Aortic or abdominal aneurism
• Severe peripheral vascular disease
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 7/26
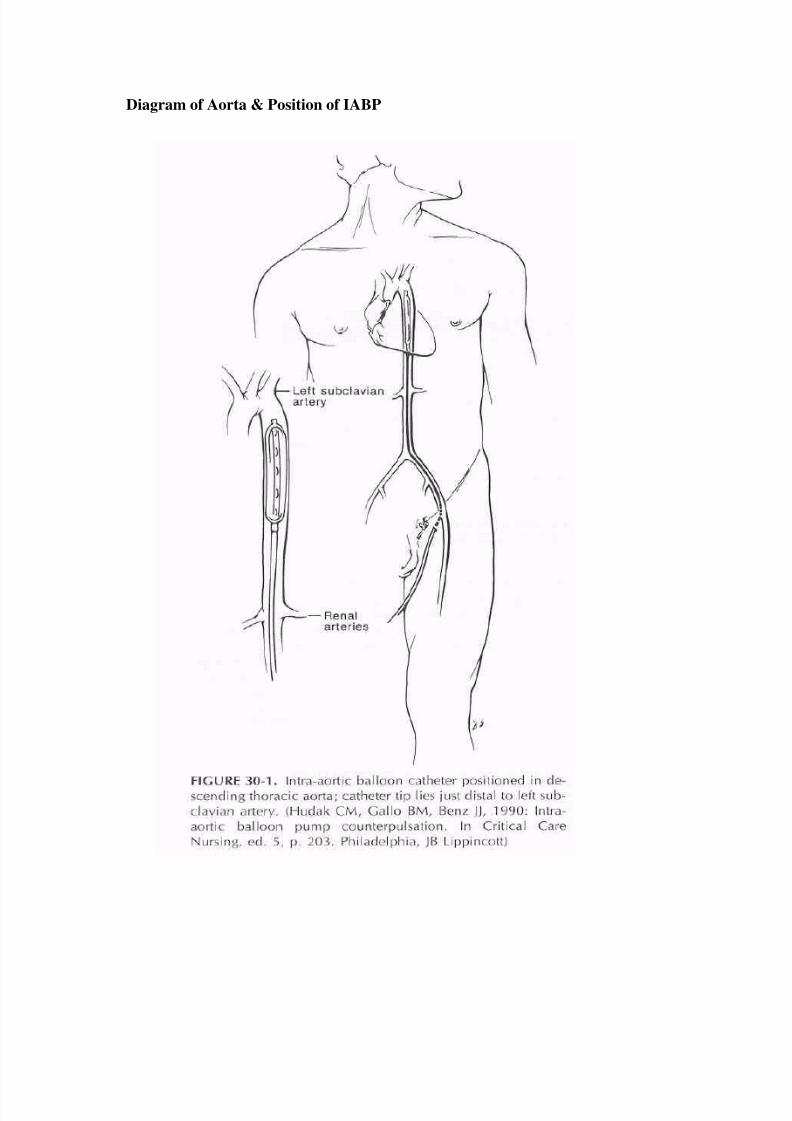
Diagram of Aorta & Position of IABP
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 8/26
Insertion
The balloon catheter is inserted either percutaneously or surgically by cutdown into
the patients’ femoral artery. The catheter can be inserted at the bedside, in a cathlab
or operating room theatre. The catheter is threaded up through the femoral artery and
located in the descending thoracic aorta, distal to the subclavian artery and proximalto renal arteries.
IABP Size
The size of the balloon is dependent on the patients height to prevent occlusion of
sub-clavian or renal arteries.
<160 cm use 34 cc
160 – 182cm use 40 cc
>182cm use 50cc
For process of insertion and nursing care required, please refer to the Clinical
Resource manual for the protocol on IABP.
Note: Need to check that the guide wire has been removed post insertion as it will
make the balloon less pliable and may not unwrap completely.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 9/26
Before you go any further, try the following self test.
Self test 1.
1. Why is an IABP used?
2. What are the effects that are achieved when using IABP therapy?
3. Describe the mechanism of counterpulsation?
4. Why is helium used to inflate the balloon?
5. Describe the correct positioning of the IAB Catheter. Why is it important?
6. Why is the size of the IABP important?
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 10/26
Trigger:
The trigger is the way the IABP identifies the beginning of the cardiac cycle. There
are 5 ways triggering may be achieved.
1. ECG Uses R wave on the ECG to initiate the pumping.
2. Pressure the arterial pressure waveform is used to trigger.
3. Internal this allows a synchronous trigger set at 80 beats/min. Internal
mode should never be used if a patient is generating a cardiac
output.
4. Pacer V/AV uses ventricular spike to trigger an event, is not an appropriate
trigger for demand pacing.
5. Pacer A the R wave on the ECG is the trigger, the atrial pacer spikes are
enhanced and rejected. This mode is only used if ECG trigger is
not able to interpret R wave with A pacing. Never use if
patient is ventricularly paced.
Augmentation
This is the ability of the balloon to be fully expanded and contain the full amount of
helium for the catheter. During normal pumping it should be maintained on full
(meaning all lights on) to prevent blood clots forming by the sides of the pump and
preventing thrombosis formation. The ability of the balloon to forward flow blood
when inflated may be affected if blood is allowed to flow down the sides of catheter.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 11/26
Setting Up the Machine to Commence Pumping.
1. Connect to mains power to ensure the battery is preserved. The battery can
withstand pumping for approximately 24 hours (depending on the battery charge).
2. Check the helium tank is open at the back of the pump.
3. Ensure both an ECG and pressure trace can be obtained from the patient on the
screen of the IABP. This can be obtained from either direct monitoring or the use
of the slave cables taking the signal from the monitor.
4.
The IABP can obtain a trigger, which stimulates the pumping of the balloon.
5.
Frequency when first commencing pumping is on 1:1, which means that for each
heart beat the balloon, will be inflated. When proceeding to weaning or timing the
frequency is changed.
6. To commence balloon pumping, inflation and deflation points should be set at the
midline and then once pumping is established, timing should be reassessed.
7.
Connect the extension tubing to the balloon catheter and on the balloon console at
the back.
Note: The tubing is made to be easily pulled apart if the patient moves their leg, this
avoids the balloon catheter being dislodged. So the tubing is not to have any tape
applied to the connections at any time.
Once connected, press the IAB fill button, holding it down for a second. A prompt on
the screen will come up so you know it is filling.
8. Once filled, commence pumping by pressing the assist/standby button. Then
increase slowly the augmentation to maximum. This will unwrap the balloon; if
done too fast, the balloon may unwrap incompletely. Maximum augmentation is
maintained at all times to ensure that the balloon is fully inflated and blood clots
are not able to form beside the balloon or in wrapping.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 12/26
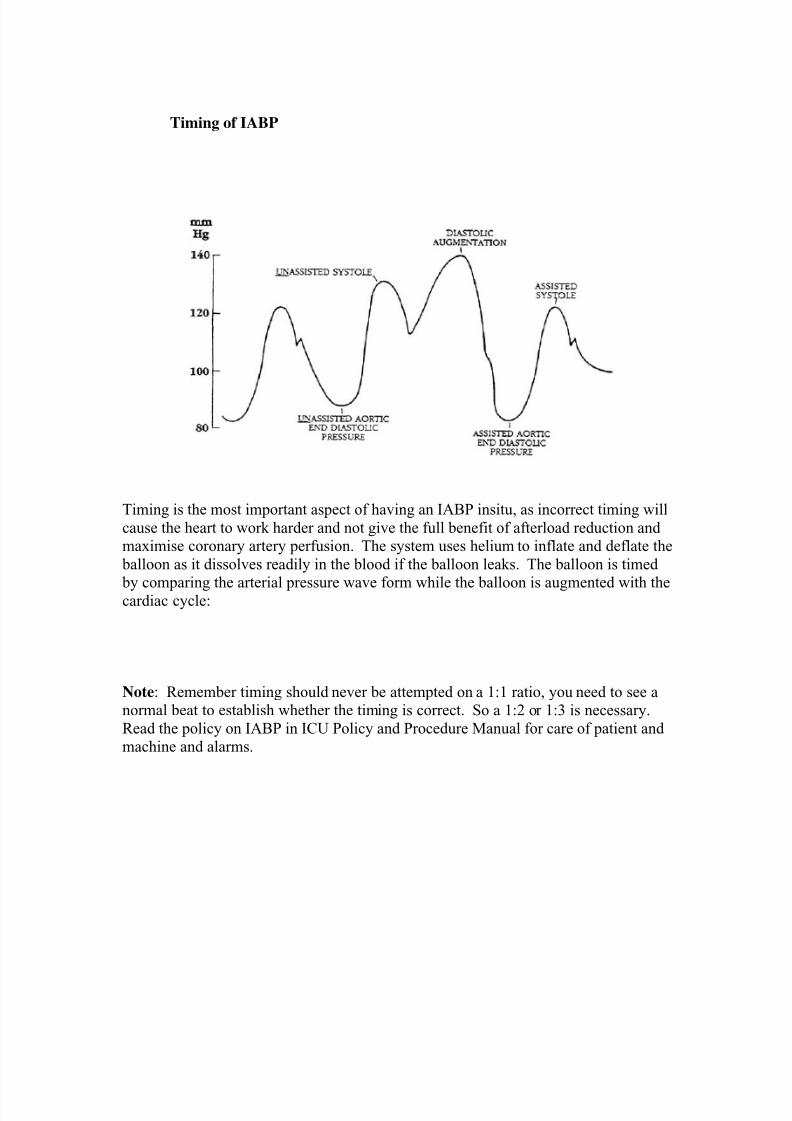
Timing of IABP
Timing is the most important aspect of having an IABP insitu, as incorrect timing will
cause the heart to work harder and not give the full benefit of afterload reduction and
maximise coronary artery perfusion. The system uses helium to inflate and deflate the
balloon as it dissolves readily in the blood if the balloon leaks. The balloon is timed
by comparing the arterial pressure wave form while the balloon is augmented with thecardiac cycle:
Note: Remember timing should never be attempted on a 1:1 ratio, you need to see a
normal beat to establish whether the timing is correct. So a 1:2 or 1:3 is necessary.
Read the policy on IABP in ICU Policy and Procedure Manual for care of patient and
machine and alarms.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 13/26
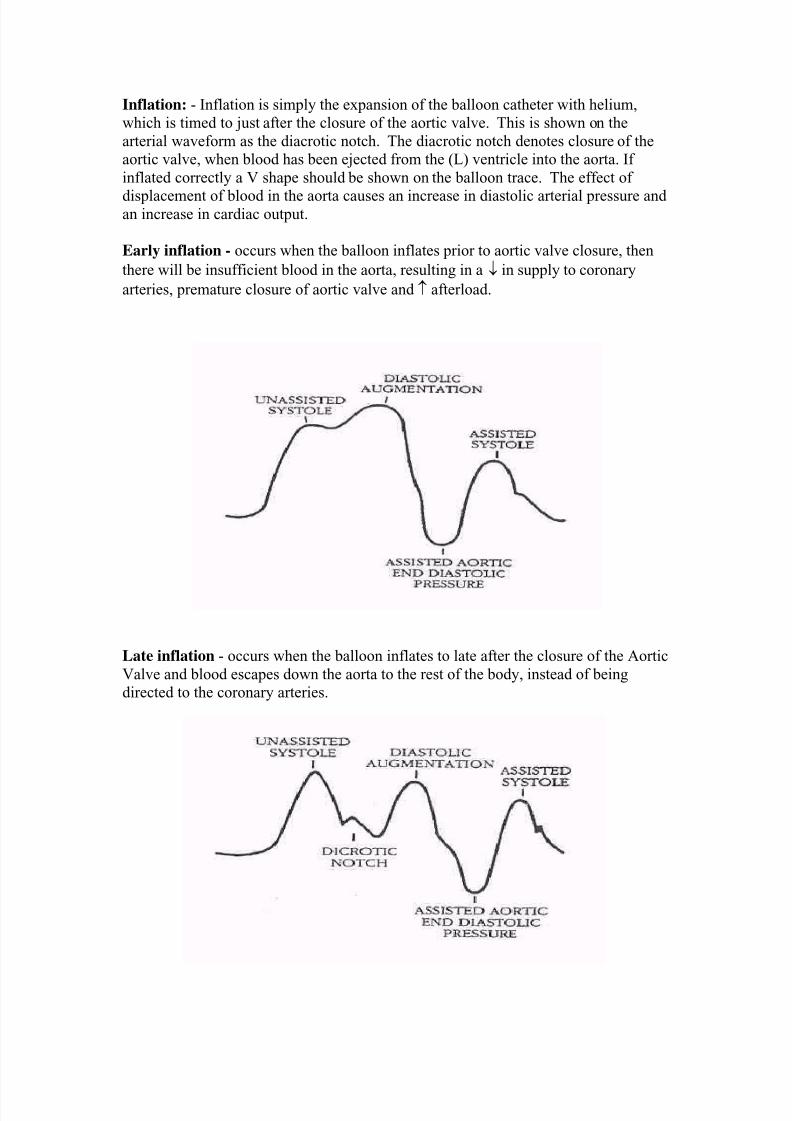
Inflation: - Inflation is simply the expansion of the balloon catheter with helium,
which is timed to just after the closure of the aortic valve. This is shown on the
arterial waveform as the diacrotic notch. The diacrotic notch denotes closure of the
aortic valve, when blood has been ejected from the (L) ventricle into the aorta. If
inflated correctly a V shape should be shown on the balloon trace. The effect of
displacement of blood in the aorta causes an increase in diastolic arterial pressure andan increase in cardiac output.
Early inflation - occurs when the balloon inflates prior to aortic valve closure, then
there will be insufficient blood in the aorta, resulting in a ↓ in supply to coronary
arteries, premature closure of aortic valve and ↑ afterload.
Late inflation - occurs when the balloon inflates to late after the closure of the Aortic
Valve and blood escapes down the aorta to the rest of the body, instead of being
directed to the coronary arteries.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 14/26
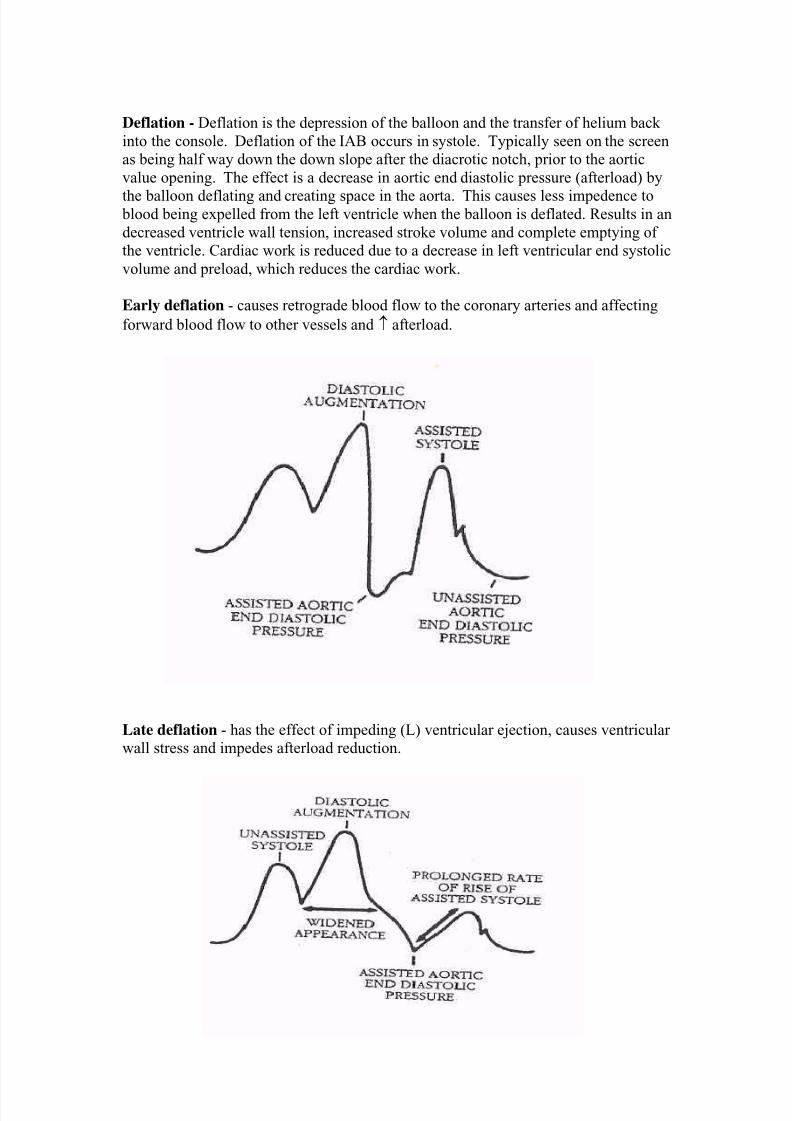
Deflation - Deflation is the depression of the balloon and the transfer of helium back
into the console. Deflation of the IAB occurs in systole. Typically seen on the screen
as being half way down the down slope after the diacrotic notch, prior to the aortic
value opening. The effect is a decrease in aortic end diastolic pressure (afterload) by
the balloon deflating and creating space in the aorta. This causes less impedence to blood being expelled from the left ventricle when the balloon is deflated. Results in an
decreased ventricle wall tension, increased stroke volume and complete emptying of
the ventricle. Cardiac work is reduced due to a decrease in left ventricular end systolic
volume and preload, which reduces the cardiac work.
Early deflation - causes retrograde blood flow to the coronary arteries and affecting
forward blood flow to other vessels and ↑ afterload.
Late deflation - has the effect of impeding (L) ventricular ejection, causes ventricular
wall stress and impedes afterload reduction.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 15/26
Weaning
Weaning of the IABP is commenced when the patient is haemodynamically stable and
it is evident that it is no longer required.
Weaning can be achieved by decreasing the frequency of assistance, meaningdecreasing to 1:2, then to 1:3 and observing the patients haemodynamics. The
balloon is to be removed by a medical officer. It is important when removing the
balloon to allow the site to bleed; this allows clots to be removed, thus decreasing the
risk of emoboli.
During the weaning process the patient may show signs of increases in PAP, decrease
in BP, CO and CI. This may show that the heart is not coping with the withdrawal
process, and should not continue, therapy should be continued.
Complications of IABP
- Limb Ischaemia
-
Bleeding from site and internal
- Infection/Sepsis
- Aortic dissection
- Embolism
- Thrombosis
- False aneurism
-
Aortic Valve Rupture
- Catheter obstruction due to improper positioning with renal arteries or subclavian
- Inappropriate timing causing ↑ afterload and stress of left ventricle.
- Pump failure
-
Balloon Catheter rupture and gas loss
- Haemolysis
- Inability to wean
- Incorrect timing
- Compartment syndrome
- Acute renal failure
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 16/26
Before you go any further, try the following self test.
Self test 2.
1. What are the two ways that ECG and pressure can be monitored to use the
IABP?
2. Why is correct timing important for the patient?
3. When should the IAB be inflated, and what is the effect of inflation?
4. When should the IAB be deflated, and what is the effect of deflation?
5. Discuss the complications associated with the use of the IABP?
6. How is weaning achieved at Liverpool Hospital? What other ways can
weaning be achieved?
7. What are the signs of failure to wean an IABP?
8. What does augmentation mean on the IABP? What is the most common
problem if augmentation is not full?
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 17/26
Nursing Care
- Hourly haemodynamics recorded
- Hourly circulation observations
- Hourly IABP ratio and level of augmentation
-
Nursed supine, 30o
elevated or on side (ensuring that the leg which has the ballooninserted through the groin is straight at all times, avoid bending it.
- Hourly urine output to indicate an early sign of IAB catheter migration.
- Daily CXR to monitor position of IAB catheter
- Observe insertion site for infection and bleeding.
- Observe and maintain normal coagulation and electrolyte balance
- Monitor and observe the external tubing from the catheter to pump for any
condensation or bloodstains.
- Ensure patient is quiet and relaxed with minimal movement around the bed.
Sedation may be required.
- Maintain a patient airway. The patient may be extubated if awake and orientated
and satisfies extubation protocol.
Cardiac Arrest
In the event of a cardiac arrest, the IABP can be used in normal mode of either ECG
or pressure trigger, as the system will synchronise to the rate and rhythm of chest
compressions. Internal trigger in some institutions are used, this provides a fixed rate
of 80 beats per minute. The IABP in the unit in the event of a cardiac arrest is either
left on ECG trigger or placed on standby. An IABP can remain on standby insitu for
no more than 30 minutes. Any longer may cause clots forming on catheter, resulting
in thrombosis being pushed through the system.
Defibrillation
The current IABP is completely isolated from the patient and safe to have the patient
defibrillated, ensuring staff remains clear from the IABP when shock is delivered.
Arrhythmias
In the event of AF the IABP should be triggered from ECG and deflation point should be moved to the extreme right. This will cause an automatic deflation on the R wave,
maximising the time the IAB catheter is inflated with an irregular HR and arterial
pressure.
Pacemaker
If the ECG trigger is unable to determine an R wave with the pacing spike, then Pacer
V/AV or Pacer A may be used.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 18/26
Troubleshooting:
The following are common problems that may occur when using an IABP.
a) No trigger – This means that the IABP has lost its tracing of ECG or Pressure and
is unable to time the inflation and deflation:
Action: To reconnect the ECG leads or pressure cable, or change the ECG leads
or tracing lead to obtain a better trace.
b) IAB Disconnected – this means the IAB catheter extension tubing has been
disconnected and the pump will stop working.
Action: Reconnect the extension tubing, PRESS IAB Fill for 3 seconds till
prompt is on the screen and the PRESS Assist/Standby to start pumping.
c) Rapid Gas Loss - This will appear if there is a leak or hole in the balloon or
extension tubing. This means the balloon may be ruptured, you will see flecks of
blood in the tubing ( no gushing blood, as blood is under pressure).
Action: If the balloon is losing its gas and filling is frequently necessary, or blood
flecks have been identified in the tubing, then stop pumping and call the RMO. It
will mean that the catheter will need to removed and replaced. Check all
connections for any leaks or disconnections.
d) Check IAB Catheter – this means that the IAB Catheter is either kinked insitu or
at the insertion site or it has not unwrapped fully insitu.
Action: Examine the catheter and extension tubing for any signs of kinking.
Ensure that full augmentation is on, making sure the balloon has the ability toexpand. Examine the skin insertion, as this is a common place for kinking. If
problem continues, contact RMO.
e)
Low Helium – this means that the supply of helium is less than 24 fills.
Action: The helium cylinder needs replacing. Please ensure that the O ring is not
dislodged while changing the cylinder as this ensures the seal.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 19/26
f) Low Battery – This means the battery has less than 30 minutes of operating time.
Action: Ensure that the balloon pump is connected to the mains power at all
times, to recharge the battery.
g) IAB Failure – This means that the IABP console fails to pump, usually as a result
of electrical malfunction or the presence of blood in the condensers.
Action: Contact RMO. Disconnect patient from the IAB console and obtain
another IAB console (this should only to be attempted if the balloon is not
ruptured, as the same problem will occur). Ensure that the machine is not labelled
faulty. Depending on the patients haemodynamic status, the IAB catheter maybe
removed.
h) Augmentation Below Limit Set - This means that the augmented diastolic has
fallen below the alarm set.
Action: Review the alarm set and consider lowering it in line with the patients
progress or if concerned with the drop, then contact RMO.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 20/26
Before you go any further, try the following self test.
Self test 3.
1. How long should an IABP Catheter remain insitu and not operating, and why not
any longer?
2. During a cardiac arrest, what mode should be used for the IABP?
3. What actions should be taken if a patient requires defibrillation while requiring
IABP therapy?
4. What effect do pacemakers have on the timing of the IABP?
5. Describe the nursing care required for a patient on the IABP?
6.
What is the correct procedure if the IABP fails?
7. What would you do if you lose your trigger for the IABP?
8.
How would you tell if your IAB catheter had ruptured? What procedure would
you use if this occurred?
9. In AF what is the best way to maximise therapy?
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 21/26
Post test
1. Why is an IABP used?
2.
What are the effects that are achieved when using IABP therapy?
3. Describe the mechanism of counterpulsation?
4. Why is helium used to inflate the balloon?
5. Describe the correct positioning of the IAB Catheter. Why is it important?
6. Why is the size of the IABP important?
7. What are the two ways that ECG and pressure can be monitored to use the IABP?
8. Why is correct timing important for the patient?
9. When should the IAB be inflated, and what is the effect of inflation?
10. When should the IAB be deflated, and what is the effect of deflation?
11. Discuss the complications associated with the use of the IABP?
12. How is weaning achieved at Liverpool Hospital? What other ways can weaning
be achieved?
13. What are the signs of failure to wean an IABP?
14. What does augmentation mean on the IABP? What is the most common problem
if augmentation is not full?
15. How long should an IABP Catheter remain insitu and not operating, and why not
any longer?
16.
During a cardiac arrest, what mode should be used for the IABP?
17. What actions should be taken if a patient requires defibrillation while requiring
IABP therapy?
18. What effect do pacemakers have on the timing of the IABP?
19.
Describe the nursing care required for a patient on the IABP?
20.
What is the correct procedure if the IABP fails?
21. What would you do if you lose your trigger for the IABP?
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 22/26
22. How would you tell if your IAB catheter had ruptured? What procedure would
you use if this occurred?
23. In AF what is the best way to maximise therapy?
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 23/26
Post test - answers
1. Why is an IABP used?
The Intra-Aortic Balloon Pump (IABP) is used to provide circulatory assist to support
a failing left ventricle. It is used for the following conditions:
• Acute left ventricular failure post cardiac surgery
• Severe unstable angina
• Cardiogenic shock post myocardial infarction
• Bridge to cardiac transplantation
• Stunned myocardium after myocardial infarction
2. What are the effects that are achieved when using IABP therapy?
The IABP has the following effects:
•
Increases coronary artery perfusion• Increases myocardial oxygen supply
• Decreases myocardial oxygen demand
• Decreases myocardial work by reducing afterload
• Increases blood pressure
• Decreases Pulmonary artery pressure
3. Describe the mechanism of counterpulsation?
Counterpulsation is the process where blood is displaced with the inflation and
deflation of the balloon catheter, this is timed to the cardiac cycle. Meaning that blood
is expelled against a force, being the balloon in an opposite direction.
4. Why is helium used to inflate the balloon?
Helium is used as it is easily dissolves in blood than air and prevents the risk of air
emboli if the catheter ruptures.
5. Describe the correct positioning of the IAB Catheter. Why is it important?
The IAB catheter is threaded up through the femoral artery and is positioned in the
descending thoracic aorta, distal to the subclavian artery and proximal to renal
arteries. It is important to avoid obstruction of these arteries as CVA and/or renal
failure may be caused.
6. Why is the size of the IABP important?
The size of the balloon is important, as it’s based on the height of the patient.
Incorrect sizing will cause occlusion of sub-clavian or renal arteries as the balloon
will be too long. If the balloon is too short then sub-optimal therapy will be provided
and the Left Ventricle will not have and assistance.
7. What are the two ways that ECG and pressure can be monitored to use the
IABP?
ECG and pressure monitoring can be achieved by directly from the patient, meaning
another set of ECG dotes and pressure measurement from the balloon. These are
usually called direct monitoring. The other way is indirect or slaving from the
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 24/26
monitor for both ECG and pressure traces. The pressure is arterial blood pressure,
aortic which is measured in the direct method.
8. Why is correct timing important for the patient?
Timing is the most important aspect of having an IABP insitu, as incorrect timing will
cause the heart to work harder and not give the full benefit of afterload reduction andmaximise coronary artery perfusion. Incorrect timing may cause further damage to an
already failing heart if it has to work harder to achieve demand.
9. When should the IAB be inflated, and what is the effect of inflation?
Inflation of IAB should occur just after the closure of the aortic valve in diastole.
This is shown on the arterial waveform as the diacrotic notch. The diacrotic notch
denotes closure of the aortic valve, when blood has been ejected from the (L)
ventricle into the aorta. The effect is a displacement of blood in the aorta which
causes an increase in diastolic arterial pressure and an increase in cardiac output.
10. When should the IAB be deflated, and what is the effect of deflation?Deflation of the IAB occurs in systole. Typically seen on the screen as being half
way down the down slope after the diacrotic notch, prior to the aortic value opening.
The effect is a decrease in aortic end diastolic pressure (afterload) by the balloon
deflating and creating space in the aorta. This causes less impedence to blood being
expelled from the left ventricle. Resulting in an decreased ventricle wall tension,
increased stroke volume and complete emptying of the ventricle. Cardiac work is
reduced due to a decrease in left ventricular end systolic volume and preload, which
reduces the cardiac work.
11. Discuss the complications associated with the use of the IABP?
Complications of the IABP are the following:
-
Limb Ischaemia
- Bleeding from site and internal
- Infection/Sepsis
- Aortic dissection
- Embolism
- Thrombosis
- False aneurysm
-
Aortic Valve Rupture
-
Catheter obstruction due to improper positioning with renal arteries or subclavian -
Inappropriate timing causing ↑ afterload and stress of left ventricle.
- Pump failure
-
Balloon Catheter rupture and gas loss
- Haemolysis
- Inability to wean
- Incorrect timing
- Compartment syndrome
- Acute renal failure
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 25/26
12. How is weaning achieved at Liverpool Hospital? What other ways can
weaning be achieved?
Weaning of the IABP is commenced when the patient is haemodynamically stable and
it is evident that it is no longer required. It is achieved by decreasing the frequency of
assistance, meaning decreasing to 1:2, then to 1:3 and observing the patients
haemodynamics. Weaning can also be achieved by decreasing the augmentation ofthe balloon, however there are dangers with the potential for thrombosis being formed
if this method is used.
13. What are the signs of failure to wean an IABP?
Signs of failure in the weaning process are increases in PAP, decrease in BP, CO and
CI. This may show that the heart is not coping with the withdrawal process, and
should not continue, therapy should be continued.
14. What does augmentation mean on the IABP? What is the most common
problem if augmentation is not full?
This is the ability of the balloon to be fully expanded and contain the full amount ofhelium for the catheter. During normal pumping it should be maintained on full
(meaning all lights on) to prevent blood clots forming by the sides of the pump and
preventing thrombosis formation. The ability of the balloon to forward flow blood
when inflated may be affected if blood is allowed to flow down the sides of catheter.
15. How long should an IABP Catheter remain insitu and not operating, and why
not any longer?
The IABP catheter should remain insitu not inflating and deflating for no longer than
30 minutes. If the balloon is not being operated then blood will clot due to stasis. If
then pumping is commenced clots will be propelled through the body and thrombosis
or an anuerysm may form the aorta.
16. During a cardiac arrest, what mode should be used for the IABP?
In the event of a cardiac arrest, the IABP can be used in normal mode of either ECG
or pressure trigger, as the system will synchronise to the rate and rhythm of chest
compressions. The internal trigger may be used, this provides a fixed rate of 80 beats
per minute. The IABP in the unit in the event of a cardiac arrest is either left on ECG
trigger or placed on standby.
17. What actions should be taken if a patient requires defibrillation while
requiring IABP therapy?The current IABP is completely isolated from the patient and safe to have the patient
defibrillated, ensuring staff remains clear from the IABP when shock is delivered.
18. What effect do pacemakers have on the timing of the IABP?
The pacemaker or pacing spike may not be able to be determined by ECG triggering,
as it relies on R wave to pump. Changing the trigger to Pacer V/AV or Pacer A may
be used.
8/17/2019 Liverpool SDL IABP
http://slidepdf.com/reader/full/liverpool-sdl-iabp 26/26
19. Describe the nursing care required for a patient on the IABP?
- Hourly haemodynamics recorded
- Hourly circulation observations
- Hourly IABP ratio and level of augmentation
-
Nursed supine, 30o
elevated or on side (ensuring that the leg which has the ballooninserted through the groin is straight at all times, avoid bending it.
- Hourly urine output to indicate an early sign of IAB catheter migration.
- Daily CXR to monitor position of IAB catheter
- Observe insertion site for infection and bleeding.
- Observe and maintain normal coagulation and electrolyte balance
- Monitor and observe the external tubing from the catheter to pump for any
condensation or bloodstains.
- Ensure patient is quiet and relaxed with minimal movement around the bed.
Sedation may be required.
- Maintain a patient airway. The patient may be extubated if awake and orientated
and satisfies extubation protocol.
20. What is the correct procedure if the IABP fails? The IABP console failure is usually as a result of electrical malfunction or the
presence of blood in the condensers. Action is to contact RMO. Disconnect the
patient from the IAB console and obtain another IAB console (this should only be
attempted if the balloon is not ruptured, as the same problem will occur). Ensure that
the machine is not labeled faulty. Depending on the patients haemodynamic status,
IABP therapy may be ceased and IAB catheter removed.
21. What would you do if you lose your trigger for the IABP?
If the IABP tracing of ECG or Pressure is lost the IABP can not function. Action is to
reconnect the ECG leads or pressure cable, or change the ECG leads or tracing lead to
obtain a better trace. Then commence pumping.
22. How would you tell if your IAB catheter had ruptured? What procedure
would you use if this occurred?
A ruptured IAB catheter will not show the classic blood gushing out as it is under a
pressure. Blood flecks will be seen in the tubing and the IABP will have gas loss and
check catheter alarms. These after a few silences will no longer be able to be rectified
this way and the pump will stop working to prevent blood contamination of the
condensers. Then stop pumping and call the RMO. It will mean that the catheter willneed to removed and replaced. Check all connections for any leaks or disconnections.
23. In AF what is the best way to maximise therapy?
In the event of AF the IABP should be triggered from ECG and deflation point should
be moved to the extreme right. This will cause an automatic deflation on the R wave,
maximising the time the IAB catheter is inflated with an irregular HR and arterial
pressure.