ibsc: question 1 by alan mcleod. getting the best marks read the whole question – a latter section...
TRANSCRIPT

iBSc: Question 1
By Alan McLeod

Getting the best marks
Read the whole question – a latter section may give you a
clue about an earlier one.
To see how many points you need look at the marks
allocated – for example a 3 point question is generally looking for 3 salient points
If giving a list answer put the best answers first – examiners will not usually mark answers too
far down a list
Always write something – it may get you part of a mark and is anonymised so
no one will think you are stupid!
If you genuinely have no clue then re-write the question to see if this sparks
some ideas.
If not then move on and come back at the end. And remember – always
write something.
Good luck!

Question 1
Mr Smith, a 68 year old smoker,
presents to A+E with a 2 hour
history of severe crushing chest
pain.
• Q1.1• List 5 differentials for
chest pain (5)

Question 1
Your SHO asks you to do an ECG and
cardiac specific bloods
Q1.2• What ECG changes might
you expect if the cause is STEMI or NSTEMI? (3)
Q1.3• What cardiac specific
blood tests would you request? (2)

Question 1
After ECG and blood tests, Mr Smith is diagnosed with
STEMI caused by occlusion of one of
his coronary vessels
Q1.4
Label these vessels (4)

Question 1
The loss of blood supply can
damage cardiac muscle
Q1.5• List differences
between cardiac and skeletal muscle (3)

Question 1
In this case, atherosclerotic disease is to
blame.
Q1.5• Describe a model for the formation
of atherosclerotic plaques (5)
Q1.6• List 2 modifiable and 2 non-
modifiable risk factors for atherosclerotic disease (2+2 = 4 pts)

AA
DD
BB
CC
EndocardiumEndocardium
FoldFold
EE
Question 1.7Lable these layers of cardiac muscle and other tissues

Question 1
In this patient’s notes is a letter from his GP stating that Mr
Smith is ‘non-compliant with
smoking cessation measures’.
Q1.8
• Describe compliance and concordance (2)
• 33 marks total for question 1

The Answers
View these on ‘note view’ rather than on full screen – additional
notes are provided for some slides

Generating Differentials:I’D GET VINO…
I Infectious / inflammatory
D Degenerative
G Genetic / Idiopathic
E Endocrine
T Trauma
V Vascular
I Iatrogenic / ingested
N Neoplastic
O Organs

Causes of Chest Pain I Infectious / inflammatory Pneumonia, pleurisy, Costochondritis
D Degenerative
G Genetic / ideopathic
E Endocrine
T Trauma Fractured rib, pulled muscle, pneumothorax
V VascularMyocardial infarction, angina, aortic dissection, PE
I Iatrogenic / ingested Surgical scar
N Neoplastic Bony mets
O Organs / other
Oesophagus (spasm, reflux), heart (pericarditis)Lung, Aorta, bones, muscle, cartilage, anxiety

STEMI and NSTEMIA: Normal ECG
B: ST Elevation
C: ST Depression
ST elevation in response to Isoelectric line (I)
I
B
C
A
P TQRS
ST Segment

Evolution of ECG Changes in STEMI
• Minutes to hours– Peaked T waves
• Hours– ST elevation
• Hours to days– T wave inversion– Loss of R wave
• Days– Pathological Q wave

Cardiac Enzymes

Right: Right Ventricle, most of Right Atrium, Part of Left Atrium
Left: Left Ventricle, part of Right atrium, most of Left atrium
Left circumflex: Left margin of heart and its entire posterior wall, Left atrium, posterior IV septum
LAD: Anterior 2/3 of IV septum, anterior portion of LV, whole apex

SA Node: Right 51-65%, Left 35-45%, Bilateral <10%
AV Node: Right 80-90%, Left 10-20%
ALL HIGHLY VARIABLE!!!

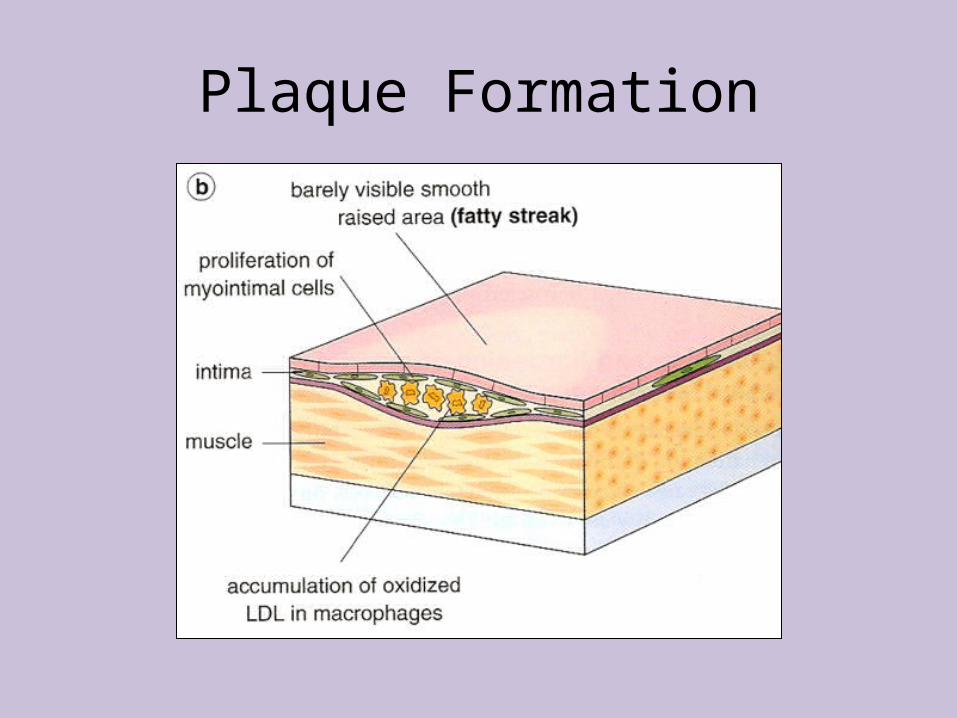
Plaque Formation
Plaque Formation

Plaque Formation

Plaque Formation

Plaque Anatomy
Plaque Anatomy (early)• Free Lipid• Foam cells• Increased myointimal
cells• Collagen• Disruption of internal
elastic lamina
Plaque Anatomy (later)• Collagen cap• Extracellular lipid mass• Foam cells• Myointimal cells• Disrupted internal elastic
lamina• Pressure atrophy of
muscle collagenous replacement

Atheroma – Risk factors
Non-preventable• Increasing age• Male sex• Family history
Preventable• Hyperlipidaemia
– LDL and Cholesterol
• Hypertension– Diastolic most
important
• Diabetes• Smoking

Muscle Comparison
Skeletal Cardiac Smooth
Voluntary Involuntary Involuntary
Striated Striated Non-striated
Multinucleated Mononucleated Mononucleated
Unbranched Branched Unbranched
No gap junctions Gap junctions No gap junctions

Fibrous Pericardium
Fibrous Pericardium
Parietal Layer of Serous PericardiumParietal Layer of
Serous Pericardium
MyocardiumMyocardium
Pericardial Space
Pericardial Space
EndocardiumEndocardium
FoldFold
Visceral Layer of Serous PericardiumVisceral Layer of
Serous Pericardium
Layers of the Heart

Health Behaviour
• Compliance– Extent to which
patient’s behaviour matches recommendations from the prescriber
• Adherence– Extent to which the
patient’s behaviour matches agreed recommendations from the prescriber.
• Concordance– Extent to which the
patient’s behaviour matches agreed recommendations from the prescriber after exploring and discussing the patients beliefs, views and opinions.

The End
The slides here should allow you to mark your own work – remember 1 mark per
answer up to the maximum for the question. Multiply by 3 to get percentage points. I assume a 60% pass mark. Sorry but I am unable to give further advice on
answers due to time constraints.