ic06-l: why hand surgeons should care about osteoporosis
TRANSCRIPT

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH.
No statement or presentation made is to be regarded as dedicated to the public domain.
IC06-L: Why Hand Surgeons Should Care about
Osteoporosis
Moderator(s): Jennifer Moriatis Wolf, MD, PhD
Faculty: Carolyn Crandall, MD, Scott M. Tintle, MD and Tamara D. Rozental, MD
Session Handouts
76th Annual Meeting of the ASSH
September 30 – October 2, 2021
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: [email protected]

Strategies for Improving Bone Health in Your Practice
Jennifer Moriatis Wolf, MD PhDThe University of Chicago

Why?

Practical Implementation
• Electronic Medical Record (EMR)• Patient-facing information• Flags for tests• Follow-up – who and how?
• Bone Health Programs

Using EMR to Improve Bone Health
• Use of automated reminders and flags has been shown to improve • Patient outcomes Garg et al, JAMA, 2005
• Provider adherence to standard screening
• Can also provide patient information
Patient-Facing Information
• EMR instructions or education sections• Vitamin C/D recommended dosing• Diet recommendations• Future fracture risk from current fracture
• Can use custom smartphrases, patient information

From bones.nih.govWhy Does Bone Health Matter?• Our bones support us and allow us to move. They protect our brain, heart, and other organs from injury. Our bones also store minerals such as calcium and phosphorous, which help keep our bones strong, and release them into the body when we need them for other uses.
• There are many things we can do to keep our bones healthy and strong. Eating foods rich in calcium and vitamin D, getting plenty of exercise, and having good health habits help keep our bones healthy.
• But if we don’t eat right and don’t get enough of the right kinds of exercise, our bones can become weak and even break. Broken bones (called fractures) can be painful and sometimes need surgery to heal. They can also cause long-lasting health problems.
• But the good news is that it is never too late to take care of your bones.

From the International Osteoporosis Foundation (www.osteoporosis.foundation)
You can help prevent osteoporosis by leading a bone healthy lifestyle at all stages of life.In fact, osteoporosis prevention begins in childhood, when a bone-healthy diet and plenty of exercise helps children achieve their highest possible ‘peak bone mass’. This is important because the more bone mass you have when you reach adulthood, the less likely you are to have weak and breakable bones at older age. Read ‘Building strong bones in children and adolescents’.For women early prevention is especially important. The diagram below shows how bone loss occurs rapidly after menopause, at around the age of 50, when the protective effect of estrogen is lost.

My EMR smartphrase (customized) – button on patient instructions in Epic
• Vitamin D and Calcium Dosing
• I would recommend that you take Vitamin D and calcium for optimal bone health - to improve your bone's strength, ability to heal fractures, and protect you in the long term. Both of these medicines can be bought at the drugstore without a prescription.
• The recommended dosing of Vitamin D is 2000 IU/day. If recovering from fracture, we may recommend up to 5000 IU/day for a limited period.
• For calcium, it is recommended that you get calcium partially from dietary sources and from supplements. Good food sources of calcium are:• milk, cheese and other dairy foods.• green leafy vegetables – such as broccoli, cabbage and okra, but not spinach.• soybeans• tofu.• soy drinks with added calcium.• nuts.• bread and anything made with fortified flour.• fish where you eat the bones – such as sardines and pilchards
• Depending on how much calcium you get from the food you eat, I would recommend taking 500mg a day of calcium. The total recommended doses of calcium are:
• 1000 mg/day for men as well as women prior to menopause.
• 1200-1500 mg/day for women after menopause. In early recovery from fracture, we would recommend these doses as well.

Does EMR-Delivered Patient Information Make a Difference?
• Alerts and reminders – yes• Perri-Moore et al reviewed 50 publications regarding the use of patient
alerts and reminders – showed improved satisfaction, mixed outcomes for adherence Patient Educ Couns, 2017
DiabetesDermatologyOncology
• No data on patient education/information - ?• Noted that the ability to personalize this information may be one of the most powerful uses of EMR

Alerts/Flags for the Provider• EMR can be customized to flag
• Every fracture patients• Every distal radius fracture patient• Every woman >50 years of age
• BUT• Have to be judicious in choosing what to flag• ‘Alert fatigue’ is real in EMRs
• One of the features of most EMR systems is pop-up alerts that trigger for any number of reasons and interrupt the flow of charting to inform you of some problem or demand some action. Some of these are useful, such as a pop-up warning that the patient is allergic to the antibiotic that you just tried to order. Others are merely annoying, such as the Medicare two midnight certification you have to attest to before you can make your over-65 patient an inpatient admission. But the net effect of all of these pop-ups is alert fatigue. They happen so often, and are so often for trivial reasons, that you tend to ignore them and click the boxes until the alert goes away and you can get on with your work.
Physician’s Weekly, 2015
Studies of Inaction Despite Flags
• Chart review of abnormal glucose values in 130 patients showed that only 36% of abnormal values were followed up
Bowen et al, Health Serv Res Mgmt, 2017
• Studies of alert overrides show highest amount in age-related reminders (79%), renal recommendations (78%), and patient allergies (77%)Nanji et al, J Am Med Inform Assoc, 2014
So how can we use EMR to help?• Patient information
• Button: You have sustained a fracture and are a woman >50 years of age. We would recommend bone density testing.
• Button: Here are my Vitamin D/Calcium recommendations• Flags
• 1-2 max• Fracture in persons >50y – bone health referral vs order DEXA
vs other

Setting Up Fracture Liaison Service (Bone Health Clinic)
• Options• Integrated inpatient with outpatient followup• Free-standing outpatient clinic staffed by advanced-practice
provider• Automate your bone health ‘order set’
LabsDXAEndocrinology referral

Integrated Flow between Fracture Admissions and Bone Health Evaluation
• Several studies have shown higher rates of bone density testing and medication initiation in patients identified and evaluated as inpatients
• Spechbach et al, Osteoporosis Intl, 2019• Naranjas et al, Arch Osteopor, 2017
• Canadian coordinator-based service identified patients in both environments and arranged physician followup, testing, and personally contacted patients after treatment Bogoch et al, J Bone Joint Surg Am, 2017
Bone Health Clinic
• Separately staffed clinic run by APPs• Evaluate, order labs/tests, and start medications
• Followup done by PCP
• (Uchicago model)

EMR Order Set to get patient started
• Bone density (DXA) order• Labs
• Markers of bone formation: P1NP, P1CP, bone alkaline phosphatase, osteocalcin
• Markers of bone resorption: CTX-1, tartrate-resistant acid phosphatase, osteoprogeterin, cathepsin K
• Consult endocrinology pr PCP for followup on testing

Bottom Line: Needs to be EASY and Seamless to Work• First, need to commit to supporting bone health – we as hand surgeons see many patients with a ‘sentinel fracture’ of the distal radius
• Set up EMR or some flow to target further workup Ward et al, Osteopor Int, 2007
• Coordinator or bone health support staff will improve this process
• Most importantly: talk to the patient about this topic• Literature has shown that surgeon addressing this with patient most
closely correlates with patient adherence and followupBogoch et al, J Bone Joint Surg Am, 2006; Tosi et al, J Bone Joint Surg Am, 2008; Akesson et al, Osteopor Int, 2013
7/14/21
1
WHAT’S NEW IN OSTEOPOROSIS:DRUGS, MARKERS AND SCREENING
Tamara D. Rozental, MDProfessor of Orthopaedic SurgeryHarvard Medical SchoolBeth Israel Deaconess Medical Center
1
Osteoporosis and Fragility FracturesNumbers
• 44 million people with osteoporosis in US
• 71 million by 2030
• 2 million fractures per year in US
• 1/3 of women over 50
• 1/5 men over 50
• 2025 predictions in US
• 3 million fractures per year
• $253 billion per year
2
Osteoporosis and Fragility FracturesWhy hand surgeons care
3
Osteoporosis and Fragility FracturesDefinitions
4
• Reduced mass and altered bone microarchitecture• Primary cause of fragility fractures• Fracture that occurs from low energy trauma
• Fall from standing height
• Fragility fractures place individuals at risk for second fracture• 62% femoral neck and 75% intertrochanteric fractures occurred after contralateral hip
fracture • Schroder et al, CORR, 1993
• Low-energy distal radius fracture confers a 2-4 fold higher risk of a second fragility fracture• Mallmin et al. Calcif Tiss Int 1993 • Crandal CJ et al. J Bone Miner Res. 2015
4
5
• Primary Imaging: BMD by DXA• Measures bone density and provides a T score • Reference to same gender young healthy population bone density
• T -1 to -2.5 – osteopenia• T> -2.5 – osteoporosis
• Subset of patients with fragility fractures have normal or osteopenic T-scores
Diagnosis
5
FRAX
6
• Created by the World Health Organization in 2008
• More comprehensive assessment which includes DXA
• Provides a 10 year prediction of fracture risk• Specific hip fracture risk (3% treatment)
• Major osteoporotic fractures (20% treatment)
• Can be used in decision-making for starting pharmacologic treatment
• Threshold for intervention is not well defined
6

7/14/21
2
7
7
Fracture Risk Stratification
8
• Very High RiskRecent fracture Very low t score
High fall risk Fracture while on therapy
• High RiskDx of osteoporosis Prior fracture
• Moderate RiskNo prior fracture FRAX <3% and/or <10% risk
t score >-2.5
• Low RiskNo prior fracture FRAX >3% and/or >10% risk
t score >-1
8
• Micro MRI provides high resolution images of cortical and trabecular bone
• No radiation
• Gradient echo sequences
• Trabecular analysis
• Scale: bone volume
• Topology: network structure
• Orientation: degree of anisotropy
DiagnosisMRI
9
• Micro MRI bone paramteres discriminate vertebral fx better than BMD
• Wehrli et al. J Bone Mine.r Res. 2001
• Promise as a tool to monitor treatment
• Chestnut et al. J Bone Mine.r Res. 2005
• Wehrli et al. J Bone Mine.r Res. 2008
• No current studies looking at patients with DRF
DiagnosisMRI
10
• Ultrasound allows scanning of central axis sites• Lumbar• Proximal femur
• No ionizing radiation• Conversano et al. Ultrasound Med Biol. 2015• Pisano et al. New Frontiers 2014.
• No data looking at patients with DRF
DiagnosisUltrasound
11
DiagnosisMicro CT
• High resolution peripheral quantitative CT
• Allows assessment of cortical and cancellous bone
• Evaluation of microarchitecture
• HR-pQCT parameters:
• Trabecular density (Dtrab) and thickness (Tb.Th)
• Cortical density (Dcort) and thickness (Ct.Th)
• Trabecular number (Tb.N) and separation (Tb.Sp)
• Trabecular bone volume fraction (BV/TV)
12

7/14/21
3
•Demographics• 40 fracture (FX) patients and 80 controls (CONT).
• No differences in age, race, BMI or other characteristics•BMD by DXA.
• Total density similar at hip, spine and forearm.• Trend towards lower BMD in FX group
•HR-pQCT.• FX had lower total density, trabecular density, trabecular number and thickness (6 to 14%)• Differences remained after adjusting for age and BMD by DXA
DiagnosisMicro CT
13
• Differences in architecture by HR-pQCT are associated with fragility fractures independently of BMD• Boutroy et al. J Clin Endocrin Metab 2005• Boutroy et al. J Bone Miner Res 2008
•HR-pQCT detects differences not measured by DXA• Current use is limited.
• Potential to identify early stages of skeletal fragility
•Cross sectional study doesn’t allow future fracture prediction• Fractures at young age may be risk factors for later fracture.
DiagnosisMicro-CT
14
Reference point indentation: measures distance a probe indents the bone
DiagnosisMicroindentation
15
• Patient population• 57 DRF, 41 Hip Fractures (HF), 93 Controls (CONT)
• BMD lower in DRF and HF vs. controls
• BMSi measured by microindentation• Lower DRF vs. CONT p<0.003• Differences remain after controlling for age, BMI and BMD• No association between BMSi and HF
• BMSi measures different element of skeletal fragility than BMD.
• BMSi may be useful in predicting fracture risk in DRF patients independent of BMD
DiagnosisMicroindentation
16
•High turnover associated with bone loss and increased fracture risk• Sornay-Rendu et al. J Bone Min Res 2005
• Szulc et al. Bone 2005
•Markers of bone formation
• N-terminal extension propeptide I collagen (P1NP)
• Bone specific alkaline phosphatase (BSAP)
• Osteocalcin (OC)
•Markers of bone resorption
• C-terminal telopeptide of type I collagen (CTX)
DiagnosisMarkers of Bone Metabolism
17
Independent Multivariable Risk Factors Associated with Distal Radius Fracture in Females 50 Years and Older
PredictorAdjusted
Odds Ratio95%
Confidence Interval P Value†
Age (yr) 1.05 1.02 – 1.08 0.03*
BMI (kg/m2) 1.00 0.94 – 1.05 0.97
History of fracture 3.00 1.51 – 5.78 <0.001*
Calcium supplements 0.40 0.23 – 0.85 0.014*
25-hydroxyvitamin D (per decrease 1 SD) 0.88 0.65 – 1.25 0.48
CTX (per increase 1 SD) 0.80 0.47 – 1.24 0.39
P1NP (per increase 1 SD) 2.17 1.52 – 3.06 <0.001*
Osteocalcin (per increase 1 SD) 1.14 0.78 – 1.77 0.50
Total hip BMD (per decrease 1 SD) 2.02 1.38 – 3.01 <0.001*
DiagnosisMarkers of Bone Metabolism
18
7/14/21
4
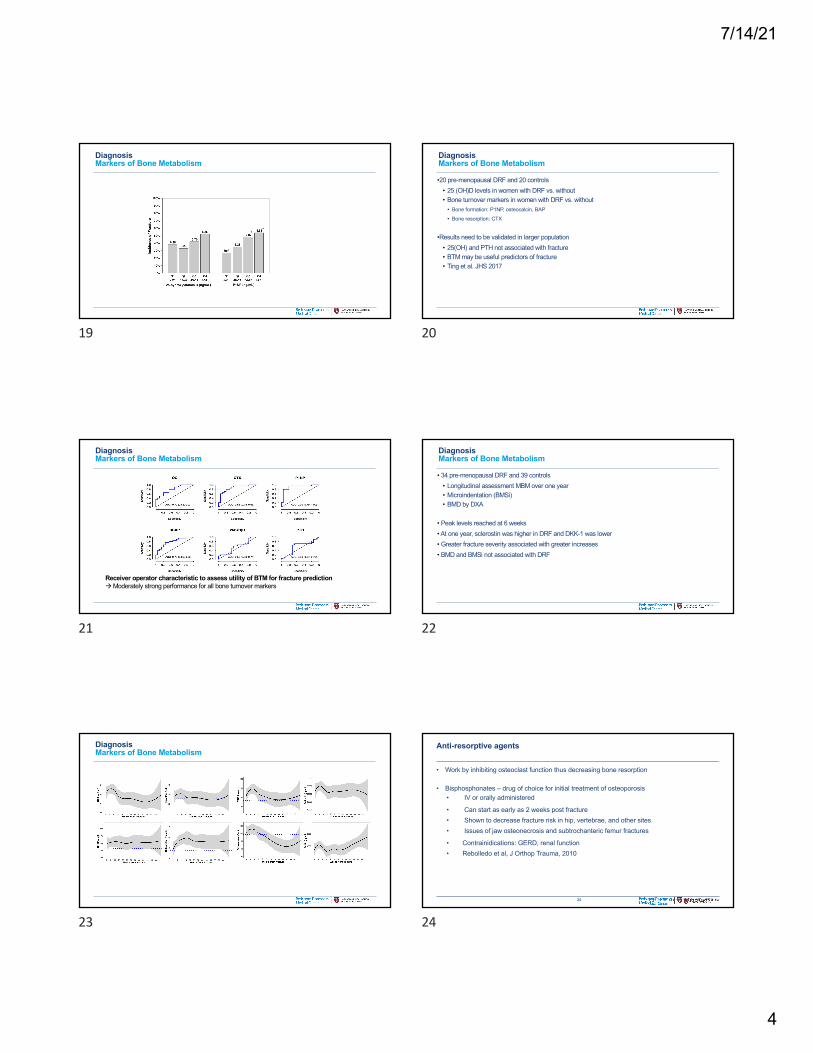
DiagnosisMarkers of Bone Metabolism
19
•20 pre-menopausal DRF and 20 controls• 25 (OH)D levels in women with DRF vs. without • Bone turnover markers in women with DRF vs. without
• Bone formation: P1NP, osteocalcin, BAP
• Bone resorption: CTX
•Results need to be validated in larger population• 25(OH) and PTH not associated with fracture• BTM may be useful predictors of fracture• Ting et al. JHS 2017
DiagnosisMarkers of Bone Metabolism
20
Receiver operator characteristic to assess utility of BTM for fracture prediction !Moderately strong performance for all bone turnover markers
DiagnosisMarkers of Bone Metabolism
21
• 34 pre-menopausal DRF and 39 controls• Longitudinal assessment MBM over one year• Microindentation (BMSi)• BMD by DXA
• Peak levels reached at 6 weeks• At one year, sclerostin was higher in DRF and DKK-1 was lower• Greater fracture severity associated with greater increases• BMD and BMSi not associated with DRF
DiagnosisMarkers of Bone Metabolism
22
DiagnosisMarkers of Bone Metabolism
23
24
• Work by inhibiting osteoclast function thus decreasing bone resorption
• Bisphosphonates – drug of choice for initial treatment of osteoporosis• IV or orally administered
• Can start as early as 2 weeks post fracture• Shown to decrease fracture risk in hip, vertebrae, and other sites• Issues of jaw osteonecrosis and subtrochanteric femur fractures
• Contrainidications: GERD, renal function• Rebolledo et al, J Orthop Trauma, 2010
Anti-resorptive agents
24

7/14/21
5
25
• Selective estrogen receptor modulators (SERMs)• Work by binding to estrogen receptors in bone and decreasing bone resorption
• Raloxifene and others have been shown to decrease vertebral fractures & increase BMD • DVT –adverse event – relative risk of 3.1• Clemett et al, Drug Eval, 2000
• Estrogen/progesterone hormone replacement• Recommendations limited to 5 years of use• Increased risks of breast cancer and cardiac disease
• Eriksen et al, Minerv Gynecol, 2012
Anti-resorptive agents
25
26
• Calcitonin • Decreases calcium mobilization from bone
• Acts to impede osteoclast activity
• Denosumab• Antibody to RANK ligand, key osteoclast activator
• Comparative studies have shown improved bone density and fracture reduction compared to alendronate
• Kendler et al, J Bone Miner Res, 2010
Anti-resorptive agents
26
• Parathyroid hormone (PTH) – teriparatide• Stimulates bone formation• Increases bone density, decreases fracture risk up to 80%• Suggested to enhance fracture healing• Cannot use in patients at high risk for developing osteosarcoma• Current recommendations for treatment up to two years• Walsh et al. Calcif Tissue Int, 2012
• Abaloparatide• Recently approved• Sustained improvement in BMD• Reduction in vertebral fractures• Leder BZ. Et al. J Clin Endocrinol Metab, 2019 – Watts NB et al. Osteop Int, 2020
27
Anabolic agents
27
Thank [email protected]
28

9/24/2021
1
A Bone to Pick: Whom to Screen for Osteoporosis
Carolyn J. Crandall, MD, MS, FACP, CCD, fellow of ASBMR
Professor of Medicine
David Geffen School of Medicine at University of California, Los Angeles
Board member, North American Menopause Society
Conflicts of Interest
None
Objectives
• To learn:• Current osteoporosis screening guidelines
• Including role of formal risk prediction tools in screening
1
2
3

9/24/2021
2
United States Preventive Services Task Force (USPSTF) 2018 screening recommendations
• Men:
• current evidence is insufficient to assess the balance of benefits and harms of screening for osteoporosis to prevent osteoporotic fractures in men. (I statement)
(JAMA. 2018;319(24):2521‐2531
United States Preventive Services Task Force (USPSTF) 2018 screening recommendations
• Women 65 years and older:
• screen with bone mineral density (BMD) test (B recommendation)
• Postmenopausal women younger than 65 years:
• screen with BMD test if they are at increased risk of osteoporosis (smoking, parental hip fracture, excess alcohol, low body wt), using a formal clinical risk assessment tool. (B recommendation)
(JAMA. 2018;319(24):2521‐2531
Screening postmenopausal women ≤ 65 y/o: USPSTF 2018
Risk assessment tool Threshold scorefor screening BMD
Fracture Risk Assessment Tool (FRAX) ≥ 8.4% 10‐yr risk of MOF
The Simple Calculated Osteoporosis Risk Estimation (SCORE)
≥6
Osteoporosis Risk Assessment Instrument (ORAI) ≥9
Osteoporosis Index of Risk (OSIRIS) <1
Osteoporosis Self‐Assessment Tool (OST) <2
(Table I created from information in JAMA. 2018;319(24):2521‐2531)
4
5
6

9/24/2021
3
OST = (wt kg – age years)/5
Truncate to integer
BMD test: score < 2
(Cadarette et al 2004, Geusens et al 2002, Gourlay et al 2005)
Fracture Risk Assessment Tool
AgeSexWeightAlcohol consumption ≥ 3 units/dRheumatoid arthritisParental hip fractureCorticosteroid useSecondary osteoporosisHeightCurrent smokingPrior fractureScreen if predicted risk of MOF ≥ 8.4%
Identifying women aged 50-64 years with Femoral Neck T-score ≤ -2.5?
Sensitivity
FRAX ≥ 9.3% SCORE (score >7) OST (score <2)
Sensitivity 88 / 258 = 34.1% 191 / 258 = 74.0%
206 / 258 = 79.8%
Area under receiver operating characteristic curve (AUC)
0.60 (poor) 0.75 0.72 (acceptable, not excellent)
(Crandall et al 2014, JBMR, 29(7): 1661‐1666)
7
8
9

9/24/2021
4
How well do tools identify major osteoporotic fracture (MOF) 10 years of follow-up?
(Crandall et al, J Clin Endocrinol Metab. 2014 99(12):4514‐22)
Remember….
• Goal of osteoporosis screening: identify postmenopausal women with BMD T‐score ≤ ‐2.5 for pharmacologic therapy. In this age group:• OST and SCORE work better than FRAX for that.
• OST sensitivity 80% vs. FRAX sensitivity 34%• OST is simplest.
• Similar findings in Canada (Leslie JCD 2013)
Upshot among women aged 50‐64 years• Screening strategies for younger postmenopausal women need reevaluation.
• Tools with more risk factors do not have better discrimination (AUC) to identify T‐score ≤ ‐2.5 than tools with fewer risk factors. (Viswanathan JAMA 2018 systematic review)
10
11
12

9/24/2021
5
Formal risk assessment tool:• OST‐simplest “WAGE” mnemonic• SCORE• FRAX• ORAI• OSIRIS
USPSTF approachDoes she have any risk factors:
• Excessive alcohol consumption• Low body weight• Parental history hip fracture• Smoking
Encourage:• Weight‐bearing and
resistance exercise• Sufficient calcium and
vitamin D intake• Avoid excessive
alcohol, smoking
No Yes
Order dual‐energy x‐ray absorptiometry test
Meets threshold for screening
Does not meet threshold
Frequency of screening DXA?
The randomized clinical trial!
The gold standard:
DXA DXA
DXA DXA
↓Fracture
DXA
Compare
Time
DXA
13
14
15

9/24/2021
6
(intentionally blank)
We don’t have that RCT in this age group…. • Or in any age group!
(Viswanathan et al JAMA 2018)
• I’ll show you best evidence to date, absent an RCT. • The only national U.S. sample focused on this age group‐the Women’s Health Initiative.
Bone density change assessment
Incident fracture assessment
Baseline BMD
Year 3 BMD
16 years max.
(Crandall et al, JAMA Intern Med. 2020 Sep 1;180(9):1232‐1240)
Mean follow‐up duration 12 years from baseline.(139 women (1.9%) experienced ≥1 hip fractures, 732 women (9.9%) experienced ≥ 1 MOF.)
16
17
18

9/24/2021
7
Change in total hip BMD between bland year 3 and incident fracture risk
Hip Fracture Major Osteoporotic FractureHR (95% CI) per 1SD lower
p-value HR (95% CI) p-value
Baseline BMD 1.80 (1.45, 2.24) <0.001 1.50 (1.37, 1.64) <0.001HR (95% CI) per 1SD decrease
p-value HR (95% CI) p-value
BMD change, adj. baseline
BMD
1.29 (1.08, 1.54) 0.004 1.11 (1.03, 1.20) 0.005
(1 SD decrease in absolute BMD corresponded to: 0.011372 g/cm2 at total hip, 0.011696 g/cm2 at femoral neck, 0.016676 g/cm2 at lumbar spine. Crandall et al, JAMA Intern Med. 2020 Sep 1;180(9):1232‐1240) Similar findings for femoral neck, lower for LS
Total hip BMD for discriminating hip and major osteoporotic fracture in postmenopausal women
(Crandall et al, JAMA Intern Med. 2020 Sep 1;180(9):1232‐1240)Similar results at femoral neck, lower at LS
Hip fracture MOF
Monitoring: Untreated younger postmenopausal women in WHI Study
If no osteoporosis at baseline (all T-scores >-2.5)*
the time required for 1% of women to experience hip or clinical vertebral fracture:
50-54 years-old 12 years 55-59 years-old 11 years60-64 years-old 7 years
Women 50-64 y/o without osteoporosis on 1st BMD test are unlikely to benefit from frequent rescreening before age 65. (based on information in Gourlay, Overman, Fine, Ensrud, Crandall, et al Meno. 2015)
(*At femoral neck, total hip, or lumbar spine)
19
20
21
9/24/2021
8
Summary serial DXA
• Change in BMD (baseline to 3 yrs) in young postmenopausal women does not add meaningfully to distinguish between women who do, and women who do not, experience subsequent fracture.
?????????
Benefits Risks
Before ordering a screening BMD test:Counsel about the relative lack of information regarding the balance of risks and benefits of osteoporosis drug treatment at this stage of life.
Conclusion about screening
• Do not routinely screen men (but do case‐finding, i.e. if secondary osteoporosis suspected)
• Selectively screen young postmenopausal women
• Routinely screen women aged ≥ 65 y/o.
22
23
24

9/24/2021
9
AcknowledgementsChristopher A. AndrewsLaura D. CarboneJane A. CauleyZhao ChenJeffrey R. CurtisMridul DattaMeghan G. DonaldsonBeatrice J. EdwardsKristine E. EnsrudMargery L. GassScott B. GoingMargaret L. GourlayKathleen M. HoveyRebecca JacksonKaren C. JohnsonAndrew M. KaunitzAndrea Z. LaCroixDeepika LadduJoseph C. Larson
Erin LeBlancWilliam D. LeslieMeryl S. LeBoffWenjun LiLisa M. LixJoAnn E. MansonSuzanne N. MorinMary Jo O’SullivanJohn A. RobbinsMaryam SattariJohn T. SchousboeMarcia L. StefanickMara VitolinsRobert WallaceNelson B. WattsJean Wactawski‐WendeCatherine R. WomackNicole C. WrightVedat Yildiz
The WHI program is funded by the National Heart, Lung, and BloodInstitute, National Institutes of Health, U.S. Department of Health and Human Services through contracts HHSN268201600018C, HHSN268201600001C, HHSN268201600002C, HHSN268201600003C, and HHSN268201600004C
References
• Screening for Osteoporosis to Prevent Fractures: US Preventive Services Task Force Recommendation Statement. JAMA. 2018 Jun 26;319(24):2521‐2531. PMID: 29946735.
• Crandall CJ, et al. Osteoporosis screening in postmenopausal women 50 to 64 years old: comparison of US Preventive Services Task Force strategy and two traditional strategies in the Women's Health Initiative. J Bone Miner Res. 2014 Jul;29(7):1661‐6. PMID: 24431262
• Crandall CJ, et al. Comparison of fracture risk prediction by the US Preventive Services Task Force strategy and two alternative strategies in women 50‐64 years old in the Women's Health Initiative. J Clin Endocrinol Metab. 2014 Dec;99(12):4514‐22. PMID: 25322268.
References
• Crandall CJ, Hovey KM, Cauley JA, et al. Wrist Fracture and Risk of Subsequent Fracture: Findings from the Women's Health Initiative Study. J Bone Miner Res. 2015 Nov;30(11):2086‐95. PMID: 25990562.
• Crandall CJ, Larson J, Manson JE, et al. A Comparison of US and Canadian Osteoporosis Screening and Treatment Strategies in Postmenopausal Women. J Bone Miner Res. 2019 Apr;34(4):607‐615. PMID: 30536628.
• Crandall CJ, Larson J, LaCroix A, et al. Predicting Fracture Risk in Younger Postmenopausal Women: Comparison of the Garvan and FRAX Risk Calculators in the Women's Health Initiative Study. J Gen Intern Med. 2019 Feb;34(2):235‐242. PMID: 30334182.
25
26
27

9/24/2021
10
References
• Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA; Manitoba Bone Density Program. Selection of women aged 50‐64 yr for bone density measurement. J Clin Densitom. 2013 Oct‐Dec;16(4):570‐8. PMID: 23452870.
• Leslie WD, Lix LM, Binkley N. Comparison of screening tools for optimizing fracture prevention in Canada. Arch Osteoporos. 2020 Oct 27;15(1):170. PMID: 33111193.
• Leslie WD, Morin SN, Lix LM; Manitoba Bone Density Program. Rate of bone density change does not enhance fracture prediction in routine clinical practice. J Clin Endocrinol Metab. 2012 Apr;97(4):1211‐8. PMID: 22278427.
• Berry SD, Samelson EJ, Pencina MJ, McLean RR, Cupples LA, BroeKE, Kiel DP. Repeat bone mineral density screening and prediction of hip and major osteoporotic fracture. JAMA. 2013 Sep 25;310(12):1256‐62. PMID: 24065012; PMCID: PMC3903386.
References
• Crandall CJ, et al. Postmenopausal weight change and incidence of fracture: post hoc findings from Women's Health Initiative Observational Study and Clinical Trials. BMJ. 2015 Jan 27;350:h25. PMID: 25627698.
• Crandall CJ, Larson J, Wright NC, et al. Serial Bone Density Measurement and Incident Fracture Risk Discrimination in Postmenopausal Women. JAMA Intern Med. 2020 Sep 1;180(9):1232‐1240. PMID: 32730575
• Gourlay ML, Overman RA, Fine JP, Ensrud KE, Crandall CJ, Gass ML, Robbins J, Johnson KC, LeBlanc ES, Womack CR, Schousboe JT, LaCroix AZ; Women’s Health Initiative Investigators. Baseline age and time to major fracture in younger postmenopausal women. Menopause. 2015 Jun;22(6):589‐97. PMID: 25349960.
References
• Hillier TA, Stone KL, Bauer DC, Rizzo JH, Pedula KL, Cauley JA, Ensrud KE, Hochberg MC, Cummings SR. Evaluating the value of repeat bone mineral density measurement and prediction of fractures in older women: the study of osteoporotic fractures. Arch Intern Med. 2007 Jan 22;167(2):155‐60. PMID: 17242316.
28
29
30

9/24/2021
11
OST(Weight in kg ‐ age in years) ÷ 2Truncate to integerScreen if score < 2ORAIAge 55‐64 yrs 5 pointsAge 45‐54 yrs 0 pointsWeight <60 kg 0 pointsWeight 60‐69 kg 9 pointsWeight ≥ 60 kg 3 pointsNo current estrogen use 0 pointsScreen if score ≥ 9
OSIRISAge: years X ‐0.2 pointsWeight kg X 0.2 pointsCurrent estrogen use 2 pointsPrior low‐impact fracture ‐2 pointsScreen if score <1
SCOREAge: 3 X 1st digit of ageWeight ‐1 X (lb 10) X 0.2 pointsNo estrogen use 1 pointNonblack race 5 pointsRheumatoid arthritis 4 pointsPrior fracture after age 45 (nontraumatic rib, wrist, hip) 4 points for each fracture type (maximum of 12)Truncate to integerScreen if score ≥ 6
The formal risk tool formulas
FRAX proprietary formulaAgeSexWeightAlcohol consumption ≥ 3 units/dRheumatoid arthritisParental hip fractureCorticosteroid useSecondary osteoporosisHeightCurrent smokingPrior fractureScreen if predicted risk of MOF ≥ 8.4%
31

All property rights in the material presented, including common-law copyright, are expressly reserved to the speaker or the ASSH. No statement or presentation made is to be regarded as dedicated to the public domain.
Speaker has not
provided a handout for
this presentation.
Session Handouts
OnDemand
76TH ANNUAL MEETING OF THE ASSH
SEPTEMBER 30 – OCTOBER 2, 2021
SAN FRANCISCO, CA
822 West Washington Blvd
Chicago, IL 60607
Phone: (312) 880-1900
Web: www.assh.org
Email: [email protected]