icd 10 documentation preparation leveraging … · physician query questions could be addressed in...
TRANSCRIPT

1
Shatondra Surulere, MBA, RHIA, CCS, CCS‐P, CHTS‐PW, AHIMA Approved Trainer and AmbassadorSenior Consultant, Revenue Cycle Consulting
ICD‐10 Documentation Preparation and Leveraging Documentation Templates and Coding Queries
2
Presentation Objectives
Identify ICD-10 documentation requirements for hospitals and physician practices
Gain an understanding of today’s documentation challenges
Review key ICD-10 documentation requirements
Review ICD-10 documentation improvement strategies
3
IF IT ISN’T DOCUMENTED, IT CANNOT BE CODED
4
In a Perfect World…
All clinical documentation would be:
Legible
Complete
Clear
Consistent
Precise

5
The Real World…
Clinical Documentation Practices
VS.
Coding Documentation Needs
6
The Role of Clinical Documentation
Clinical information for patient care
Quality/core measures Hospital profiling Physician profiling Disease reporting Compliance
Government and payor reviews
Others

7
The Connection to Coding
Clinical documentation paints a picture
Patient’s acute condition
Complicating condition(s)
Clinical, therapeutic and/or diagnostic treatment and patient responses to treatment
Translates to codes
o Billing
o Incentive payments
8
1. Billing and AR
2. Quality incentives
3. Discharged Not Final Billed (DNFB)
4. Patient status (inpatient, outpatient, observation)
5. APDRG/APRDRG/MS-DRG reimbursement
6. Compliance
The Relationship to Reimbursement

9
The Reality – For Many Health Information Management Departments
Accountability
Tools Documentation
Coding Benchmarks
Responsibility
Tools Documentation
Coding Benchmarks
10
Polling Question
In your opinion, does your facility do a good job holding physicians accountable for the quality of their documentation?
A. Yes
B. No
C. Not sure

11
From the Provider’s Point of View
12
Basic Clinical Documentation
+
Quality Requirements
+
Meaningful Use
+
Regulatory and Compliance Initiatives
+
Operational Challenges
+
EHR Template Requirements
+
ICD-10 Initiatives
Overwhelming Documentation Requirements

13
Inconsistent Tools and Requirements
Incomplete and inconsistent documentation tools Physician query questions could be addressed in
current tools Inconsistent physician query questions between
clinical documentation improvement and/or coding staff
Quality, Joint Commission, infection control, and other requirements are often not incorporated in documentation tools
14
ICD-10 Documentation Requirements

15
The Importance of Specificity
Specificity in documentation is key, because, in ICD-10, fewer “unspecified” codes exist
Specific documentation benefits
Reduces physician queries and AR delays
Reduces denials/request for medical records
More accurate quality and infection control reporting
Your documentation is, the less queries you will receive from the CDI specialist and the coders
16
ICD‐10 … A Refresher in Documentation Requirements
Below are some general documentation tips
that you can begin using now to create a
seamless transition to the new system:
Specific diagnosis
o Document the diagnosis to the
greatest level of specificity
Specific anatomy
o Document the exact body location
Document ALL conditions identified and treated during the encounter
o Secondary diagnosis ARE IMPORTANT

17
ICD‐10 … A Refresher in Documentation Requirements
Laterality
Document which side of the body- right or left
o Note: approximately 5,000+ codes have a right and left distinction
Dominant verses non-dominant side
Document dominant verses non-dominant side for all paralytic syndrome conditions
Initial verses recurrent
Document whether the condition is initial or recurrent
Combination codes for conditions and common symptoms or manifestations
o Secondary diagnosis ARE IMPORTANT
18
Cardiovascular Example
CAD (coronary arteriosclerosis) is specified as of native vessel, bypass graft, or transplanted heart.
Combination codes to include CAD with angina (unstable, with spasm, other) as well as CAD with ischemic chest pain.
Document exact date of MI New/initial MI: Occurred or diagnosed within the past four
weeks but not previously treated Old MI: Report a "healed or old MI" whether the patient is
currently experiencing problems or not Subsequent MI: subsequent, new MI occurring within the
four-week timeframe of the initial MI Document type of MI
STEMI vs. NSTEMI

19
Cardiovascular Documentation Examples
Physician office documentation: “reports history of CAD, HTN, MI, and angioplasty”
o Need additional documentation CAD is present after angioplasty of a native artery (I25.10) or of the bypass (I25.810)
o Documentation regarding the date and specifies of the MI will be required
Inpatient physician documentation: “patient has history of ESRD, CHF, and high blood pressure and
past MI”o There is conflicting documentation on this chart from another
physician, stating that the patient has HTN. HBP and HTN are coded differently, and, if the patient truly has HTN (I10), it should be documented as such, not as HBP (R03.0).
o Documentation regarding the date and specifies of the MI will be required
20
Laterality Documentation Examples
For all body parts that can be defined as left, right, or bilateral side(s), the specific “side” must be documented
Physician office documentation “patient complains of hearing
loss (right); large right cerumen impaction” – good example of laterality documentation (H61.21 –impacted cerumen, right ear)
Physician office documentation “patient presents with glaucoma
and senile cataract” – This would need specification for the glaucoma and cataract(s), are they right, left, or bilateral?
21
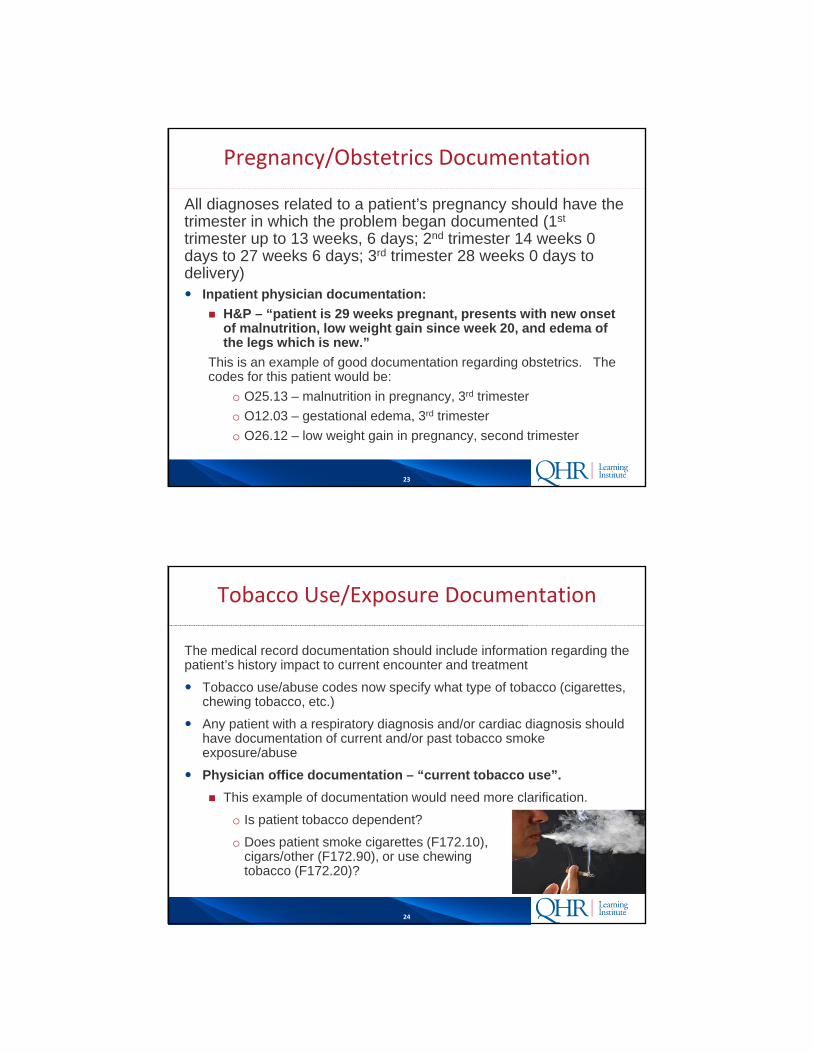
Fracture Documentation Requirements
More information will be required to accurately code fractures in ICD-10 type of fracture specific anatomical site whether the fracture is
displaced or not laterality routine versus delayed healing nonunion and malunions
22
Injury Documentation Requirements
Documentation for injuries should include the “encounter type”
Initial encounter
Subsequent encounter for fracture with routine healing
Subsequent encounter for fracture with delayed healing
Sequela of fracture
23
Pregnancy/Obstetrics Documentation
All diagnoses related to a patient’s pregnancy should have the trimester in which the problem began documented (1st
trimester up to 13 weeks, 6 days; 2nd trimester 14 weeks 0 days to 27 weeks 6 days; 3rd trimester 28 weeks 0 days to delivery) Inpatient physician documentation:
H&P – “patient is 29 weeks pregnant, presents with new onset of malnutrition, low weight gain since week 20, and edema of the legs which is new.”
This is an example of good documentation regarding obstetrics. The codes for this patient would be:
o O25.13 – malnutrition in pregnancy, 3rd trimester
o O12.03 – gestational edema, 3rd trimester
o O26.12 – low weight gain in pregnancy, second trimester
24
Tobacco Use/Exposure Documentation
The medical record documentation should include information regarding the patient’s history impact to current encounter and treatment
Tobacco use/abuse codes now specify what type of tobacco (cigarettes, chewing tobacco, etc.)
Any patient with a respiratory diagnosis and/or cardiac diagnosis should have documentation of current and/or past tobacco smoke exposure/abuse
Physician office documentation – “current tobacco use”.
This example of documentation would need more clarification.
o Is patient tobacco dependent?
o Does patient smoke cigarettes (F172.10), cigars/other (F172.90), or use chewing tobacco (F172.20)?

25
Procedure Documentation
Standard terminology Example, in ICD-9, “excision” can mean different things,
depending on the body site/procedure being done. In ICD-10, excision means “cutting out or off, without replacement, a portion of a body part”
Expandability – to accommodate new procedures and technologies
Specificity – specify approach, body part and devises Example, in ICD-9, 39.31 means suture of an artery. In
ICD-10, specific codes exist for each artery.
26
27
Step 1: Develop The Plan
Identify the team
Develop a detailed plan
Specific steps and timelines
Milestones
Testing
Monitoring
Accountability
28
Collaboration is Required!

29
Build a Collaborative Team
ICD-10 governance structure Clinical documentation work
group
Physician champions
Coding specialists (hospital and physician practice)
Administration
Information technology
Physician practice management
30
Step 2: Understand Current State
Communication is Key!

31
Understand the Physician Environment
Evaluate physician perception of documentation work flow, requirements, and concerns
Identify opportunities to develop and/or expand physician champion strategyDevelop physician champion strategy
Physician champion roles and responsibilities
Engage physician leadersBy specialty
Consider physician feedback strategies
Engage physician practice managers
32
Identify your most common diagnoses and procedures and pull a sample of medical records by physician.
Conduct an ICD-10 documentation gap analysis. Identify gaps and trends
By disease
Specialty
Physician
Start with the Documentation

33
Step 3: Work Flow Optimization
Consider work flow re-design sessions
Evaluate dashboards Documentation issues by disease
Physician query trends
A/R delays due to non-specific and/or missing documentation
Identify opportunities to utilize technology Enhance tracking, trending and reporting to capture
trends and delays
34
Step 4: Develop Future State Tools
A successful conversion to ICD-10 will require a review of current tools to identify enhancements to facilitate capture documentation required for code assignment CPOE Templates EHR Templates Physician Query Forms
Identify ICD-10 specific documentation requirements Engage Physicians to identify opportunities to enhance
compliance and acceptance A few things to consider
Work flow re-design sessions Utilizing an ICD-10 Approved Trainer
Start NOW!

35
ICD‐10 Mitral Valve Disorder Code Revisions
ICD-9 Code
ICD-9 Descriptions ICD-10 Code ICD-10 Description
424.0Mitral Valve Disorders
I34.0Nonrheumatic mitral (valve) insufficiency
I34.8Other nonrheumatic mitral valve disorders
Mitral Valve DisordersDocumentation Specificity Required for Code Assignment
36
Problem List/CPOE Templates
Problem Non-Specific Documentation Specific Documentation
Hypertension, heart disease, kidney disease
1) HTN; 2) CAD; 3) CKD
Hypertensive heart and CKD, stage 4, w/out heart failure
Hypertension, heart disease, kidney disease, CHF
1) CHF; 2) CAD; 3) CKD; 4) HTN
Hypertensive heart disease; Stage 3 CKD; Primary essential hypertension; Acute/Chronic systolic heart failure
MI or Not? ACS Atherosclerotic heart disease of native coronary artery with unstable angina pectoris
MI NQWMI NSTEMI
MI STEMI STEMI involving left circumflex coronary artery
Sample Problem List and Physician Order Specificity for Reporting Cardiac Ischemia
37
EHR Documentation Templates
Review documentation templates by disease
Identify ICD-10 documentation needs
Develop future state tables and prompts to support ICD-10 documentation requirements
Coordinate physician practice and hospital templates for like diseases
Engage vendors to identify timelines and upgrade requirements
38
EHR Documentation Templates‐Obstetrics
Obstetrics Specify trimester for which condition occurs
o 1st trimester less – than 14 weeks, 0 days
o 2nd trimester – 14 weeks, 0 days to less than 28 weeks, 0 days
o 3rd trimester- 28 weeks, 0 days until delivery
Specify # weeks of pregnancy Specify pre-existing or pregnancy
induced Complications affecting pregnancy

39
Acute Myocardial Infarction (MI) MI episode of care
o Initial refers to initial episode of care for an acute MI
o Subsequent refers to care for a subsequent, new Acute MI occurring within the 4 week time frame
Type of MI
o STEMI
o NSTEMI
Site and artery (if known)
Complications of the MI
CABG Aorta to coronary artery
(aortocoronary)
Coronary artery to coronary artery
Coronary vein to coronary artery (percutaneous only)
Left internal mammary (LIMA) to coronary artery
Right internal mammary (RIMA) to coronary artery
Abdominal to coronary artery (gastroepiploic anastomosis)
Thoracic to coronary artery
EHR Documentation Templates‐MI/CABG
40
Body Part
Coronary Artery, One Site
Coronary Artery, Two Site
Coronary Artery, Three Site
Coronary Artery, Four or More Sites
Device
No Device (direct anastomosis)
Autologous Arterial Tissue
Autologous Venous Tissue
Nonautologous Tissue Substitute
EHR Documentation Templates‐MI/CABG (Continued)
41
Type
Diabetes mellitus due to underlying condition
Drug or chemical induced diabetes mellitus
Type 1 diabetes mellitus
Type 2 diabetes mellitus
Other specified diabetes mellitus
Control
ICD-10 no longer recognizes “uncontrolled”
Poorly controlled, out of control, or inadequately controlled are coded to diabetes by type with hyperglycemia
Complications of Diabetes
EHR Documentation Templates‐Diabetes
42
EHR Documentation Templates‐Acute Respiratory Failure/Asthma/Bronchitis/COPD
Respiratory Failure
Acuity
Hypercapnic/Hypoxic
Tobacco usage/exposure/history

43
EHR Documentation Templates‐Acute Respiratory Failure/Asthma/Bronchitis/COPD (Continued)
Asthma/Bronchitis/ COPD Identify the type of asthma
o Allergic extrinsic, childhood, chronic obstructive, exercise-induced, hay fever, persistent, due to other agents
Identify the type of bronchitiso Allergic, asthmatic, chemical, chronic obstructive,
smoker’s, viral, due to other agents
Identify the type of COPDo Chronic bronchitis with tracheobronchitis, emphysema,
decompensated, due to other agents
Acuity Tobacco usage/exposure/history
44
EHR Documentation Templates – Traumatic Fracture
Site Laterality Open
Gustilo classification for long bone fractures
Closed Episode of care
Initial (active phase of treatment) Subsequent (after active phase)
o With delayed healing o With malunion o With nonunion o With routine healing or aftercare
Sequela/late effect

45
Document if sepsis was present on admission
Document underlying local infection Pneumonia, UTI, and post operative infections are examples
Urosepsis-MUST specify sepsis with UTI, versus UTI only
o Urosepsis is not recognized in ICD-10
Specify causal relationship to local infection and/or procedure
Identify causative organism
Severity With septic shock
Without septic shock
Associated organ dysfunction when documenting severe sepsis
EHR Documentation Templates‐Sepsis
46
Location of insertion Atrium, right
Inferior vena cava (IVC)
Innominate vein
Subclavian vein (e.g., midline cath)
Superior vena cava (SVC)
Approach Open
Percutaneous
Percutaneous endoscopic
Radiological guidance *No guidance performed
ECG (electrocardiography)
Fluoroscopic
Ultrasonic
Contrast Used None
High osmolar
Low osmolar
Other contrast
EHR Documentation Templates PICC/CVC Placement

47
EHR Templates‐Obstetrics
48
EHR Templates‐Obstetrics

49
EHR Templates‐PICC Line
50
EHR Templates‐Orthopedics
51
Template Case Study
52
Polling Question
Do you have a clinical documentation improvement program?
A. Yes
B. No
C. Not sure

53
Physician Query Redesign
Review Trends Physician response rate
Most common queries by disease
Evaluate process and identify opportunities for improvement
Re-design physician query forms (standard vs. free text) Be clearly and concisely written
Contain precise language
Present the facts but not lead the clinician
54
Physician Query Redesign
Include
ICD-10 specific documentation needed for diagnoses
o Sepsis, urosepsis
o Obstetrics
ICD-10 specific documentation needed for procedures
o PICC/CVC insertion
o Transfusions

55
Physician Education Recommendations
ICD-10 documentation changes
Emphasis on physician specialty
Specificity in documentation of diagnoses
Specificity in documentation of procedures
Importance of coding secondary diagnoses
More than four diagnoses (physician office)
56
Coder Education Recommendations
ICD-10 Official Coding Guidelines for Coding and Reporting
Chapters specific changes
Specificity in the coding of diagnoses
Specificity in the coding of procedures
Emphasis on secondary diagnosis coding
ICD-10 Coding Clinics
ICD-10 documentation and physician query guidelines

57
Step 5: Implement the Plan
Develop a “Roll Out Schedule” Physician queries
o By disease
o In conjunction with physician, coding, and/or CDI education
Floor coaching Hospital
Physician practice
Hotline and ongoing assistance
Monitoring and reporting
58
Step 6: Hardwiring Solution
New physician and/or staff orientation
Documentation tools maintenance
Control
Re-design
Testing

59
60
Intended for internal guidance only, and not as recommendations for specific situations. Readers should
consult a qualified attorney for specific legal guidance.
Thanks for Attending!