identifying respiratory viral pathogens
TRANSCRIPT

Identifying Respiratory Viral Pathogens
Theo Sloots Unit Director
Queensland Paediatric Infectious Diseases Laboratory
Children’s Health Service, Brisbane
Queensland Children’s Medical Research Institute
Sakzewski Virus Research Centre
Pathology Queensland Central
The University of Queensland
“Helping Kids Get Better Sooner”

Viruses in May, 2011
Activities are focussed on 3 areas:
• Clinical investigations and clinical trials
• Development of diagnostic assays
• Research in paediatric infectious disease.
QPID laboratory core business
• Together with the Director of Infectious Diseases, the QPID laboratory performes clinical investigations to diagnose unresolved infectious disease in children.
• Quantitative PCR for BKV and CMV in immunosuppressed kids. • Fungal infections in BMT
• The QPID laboratory also includes a Clinical Trial Unit
• Over the last 5 years the CTU has completed approximately 42 clinical trials, sponsored by industry.

Viruses in May, 2011
Develop and validate new (molecular) diagnostic procedures for infectious diseases.
• Diagnostic PCR assays • Quantitative real-time PCR • Typing assays (rep PCR, MLST, SNP, Sequenom technologies) • Drug resistance detection and characterisation
• Validate and transfer assays for routine use at Pathology Queensland
• More than 70 assays developed so far
• Most notable; • meningococcus, • gonococcus • enteric viruses • respiratory viruses, including “swine flu”
• Funded by Qld Health, PQ, RCH Foundation
QPID laboratory core business

Viruses in May, 2011
QPID laboratory core business
Conduct research in (paediatric) infectious diseases
• Pseudomonas aeruginosa in Cystic Fibrosis • Typing using rep-PCR, MLST, Sequenom • Antibiotic resistance markers and mechanisms • Virulence factors
• Characterisation of viral enteric disease • Epidemiology of known and new enteric viruses
• Characterisation of paediatric respiratory disease • Epidemiology of known and new respiratory viruses • Birth Cohort - acquisition of respiratory viruses during the first 2 years of life • New virus discovery
• Funded by RCH Foundation, NHMRC, ARC, NIH.
Until 1999 the Pathology Queensland Diagnostic Virology laboratory
employed traditional methods for the detection of respiratory viruses
• Virus isolation in cell culture using roller tubes
• Direct Fluorescent staining (DFA)
The algorithm was modified to a more rapid protocol.
• Direct Fluorescent staining (DFA)
• Culture amplified DFA (48 hr culture followed by DFA
staining)
This method showed 99.7% sensitivity and 99.3% specificity
compared to the traditional method.
It reduced the turn around time for 85% of the results from 7 days to
3 days
Detection of Respiratory Viruses

Then in 2003 we developed the first molecular test for
respiratory viruses and applied it to routine diagnostic use.
• This method employed conventional multiplex PCR for
7 respiratory viruses.
• Amplification products were detected by individual
virus-specific biotinylated probes in a 96-well
microtitration plate using digoxigenin (Roche) and
colour detection (ELAHA).
This assay was validated by
analysing 1500 respiratory
samples (at least 20 positives)
and comparing the results against
DFA /CA-DFA
Diagnosis of Respiratory Viruses
Syrmis et al. Journal of Molecular Diagnostics (2004), 6: 125-131

Viruses in May, 2011
Diagnosis of Respiratory Viruses
During 2003 approximately 3000 respiratory samples were tested
using the PCR assay.
DFA/CA-DFA (+) PCR (+) % Increase
RSV 56 68 21
PIV 1 20 23 15
PIV 2 20 24 20
PIV 3 25 33 32
INF A 40 48 20
INF B 20 22 10
ADV 40 48 20
Positive 261 322 23
Negative 1239 1178 -5
The PCR assay showed a significant increase in sensitivity (approximately 23%
overall) with 99.8% specificity compared to the DFA/CA-DFA algorithm
Viruses in May, 2011
Tests were performed on a LightCycler I as monoplex assays.
RSV and ADV PIV 1,2,3 INF A and B HMPV and EHV (internal control)
Applied Biosystems 7500 QIAGEN RotorGene LightCycler 480
Real-time PCR Assays

Viruses in May, 2011
Real-time PCR Assays – Impact on the Laboratory
The introduction of real-time PCR for respiratory viruses has vastly increased demand but has provided significant additional benefits to our organisation
• Greater sensitivity & specificity of diagnostic tests • Improved turn around times (3 – 24 hours) • Reduced costs; particularly labour component • Better patient care (positive diagnosis limits use of antibiotics/Changed barrier nursing)
0
5000
10000
15000
20000
25000
30000
35000
40000
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
20
11
“swine flu” N
um
ber
of S
am
ple
s
Increase ranges from 12 – 43% per year

RSV
PIV
FLU
ADV
43%
23%
16%
18%
RSV
PIV
FLU
ADV
NEG
11%
5.5%
4%
4.5%
75%
Using these assays, the majority
of virus detections have typically
been attributed to RSV
However, these viruses account only
for approximately 25% of diagnoses
leaving ~70% of cases undiagnosed.
69% Bacteria (6%)
Common Viral Causes of Acute Respiratory Tract Infections
Proportion of Viruses in Positive Specimens
% Positive in All Samples Tested
We examined 8200 NPAs collected between 2003-2006 from children with acute respiratory symptoms for common respiratory viruses

Other Viral Causes of Acute Respiratory Tract Infections
Other known viruses have been implicated in ARTI, but clinically have been considered to be of limited significance. As a result they are often not tested for routinely.
Some of these are: o rhinoviruses o coronaviruses OC43 and 229E o enteroviruses (parechovirus) o other adenoviruses o influenza C o parainfluenza 4
We sought to establish the epidemiology and clinical impact of these viruses as agents of ARTI
Viruses in May, 2011

RSV
PIV
FLU A & B
ADV
HRV
HEV
HCoV
FLU C
PIV 4
Neg
11.2
3.5
4.1
6.0
32.8
2.5
1.8
1.1
0.6
36.4
%
32.8
36.4
11.2
We examined 8200 NPAs collected between 2003-2006 from children with acute respiratory symptoms for the other known viruses
Viruses in May, 2011

o 36% of patients with clinical symptoms of acute respiratory infection still remained undiagnosed.
o This suggests that other as yet unknown respiratory viruses may be circulating in the community.
o This notion was supported by the discovery of human metapneumovirus by the Osterhaus group in the Netherlands in 2001.

* van den Hoogen, B. G., et al. 2001. Nat. Med. 7:719–724.
In 2001 van den Hoogen et al *, reported the existence of a new virus isolated from 28 children with respiratory tract disease (bronchiolitis)
Symptoms attributed ranged from mild upper respiratory infection, severe cough to severe bronchiolitis (requiring mechanical ventilation)
Clinical symptoms were indistinguishable from ARTI caused by RSV
500 nasopharyngeal swabs taken from well children were negative for the virus by culture and PCR
Discovery of Human Metapneumovirus
Ab Osterhaus
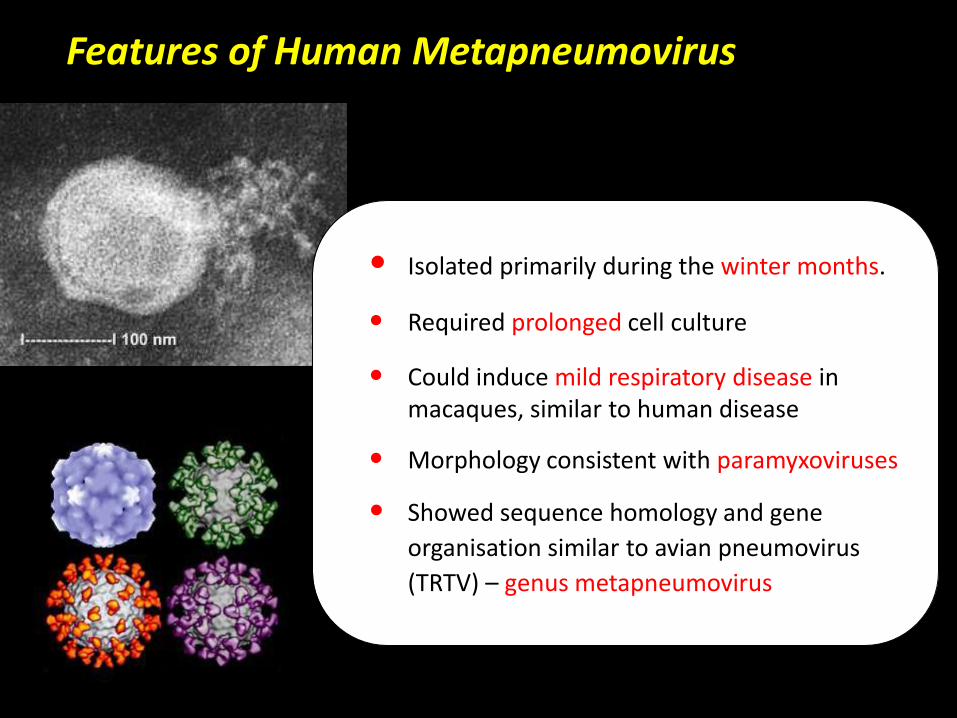
Features of Human Metapneumovirus
• Isolated primarily during the winter months.
• Required prolonged cell culture
• Could induce mild respiratory disease in macaques, similar to human disease
• Morphology consistent with paramyxoviruses
• Showed sequence homology and gene
organisation similar to avian pneumovirus
(TRTV) – genus metapneumovirus

In 2003 the QPID laboratory commenced an NHMRC Project to investigate the epidemiology and clinical characteristics of hMPV in Queensland children. Tested 10,329 respiratory samples collected over 2001 to 2004 Specifically, we examined:
the incidence of hMPV infection
the seasonality of hMPV
the molecular epidemiology of hMPV strains
clinical impact of hMPV infection
Human Metapneumovirus in Queensland

723 hMPV-positive specimens were detected
giving an average incidence in our population of
7.0%. (Range 6.4% – 7.6%)
2001 7.1%
2002 7.0%
2003 6.4%
2004 7.6%
INCIDENCE OF hMPV
• 82.8% of all positives were
from children younger than
10 years of age.
• Subjects older than 40
years appear to be at
greater risk
Human Metapneumovirus in Queensland

TEMPORAL DISTRIBUTION OF hMPV INFECTION
• Infection with hMPV
occurred primarily
during late winter and
spring.
• However there was
considerable variation
between years
Human Metapneumovirus in Queensland

0.0
5.0
10.0
15.0
20.0
25.0
30.0
Percen
tag
e p
osit
ive
Month
Month
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
Percen
tag
e p
osit
ive
Month
Month
summer autumn winter spring summer autumn winter spring
2005 2006
2007 2008
IA
IB
PIV1
PIV 2
PIV 3
ADV
RSV
HMPV

Amplification and sequencing of
the HMPV P-gene was
performed on 322 positive
samples followed by
phylogenetic analysis.
HMPV showed the presence in
our population of two genotypes
A & B, each with two subtypes,
A1,A2 & B1,B2
A1
A2
B1
B2
A
B
MOLECULAR EPIDEMIOLOGY OF hMPV

0
10
20
30
40
50
60
1 2 3 4
A1
A2
B1
B2
2001 2002 2003 2004
% o
f To
tal P
osit
ive
s
hMPV Subtypes Detected
All four subtypes were detected in each of the years studied.
Each year showed a
predominant virus subtype
present in the population
A different subtype was
dominant in successive
years. (influenced by pre-
existing immunity?)
In total, subtype B1 was
most frequently detected
over the 4 years
Human Metapneumovirus in Queensland

We found a significant correlation between disease severity and genotype A1
Approximately 28% of cases were scored as “severe” – ie. requiring ventilation, IV fluids and hospitalization for > 5 days.
Have observed 13 proven cases of nosocomial infection at the RCH. (This has also been reported by others)
Two deaths in immunocompromised adults following lung transplant and BM Tx. (Confirmed by Immuno-histochemical staining of hMPV in lung tissue).
Clinical Impact of Human Metapneumovirus
Sloots et al. Emerg Infect Dis. 2006. 12(8):1263-6.

Viruses in May, 2011
Lia van der Hoek, The Netherlands
2004 – Described the presence of a new human coronavirus - NL63 in a 7-month-old child with bronchiolitis.
Nat Med. 2004 Apr;10(4):368-73
Patrick Woo, Hong Kong
2005 – Discovered a novel coronavirus, HKU1, from a patient with pneumonia. J Virol. 2005 Jan;79(2):884-95
Tobias Allander, Sweden
2005 – Reported the presence of human bocavirus in respiratory tract samples.
Proc Natl Acad Sci U S A. 2005 Sep 6;102(36):12891-6
Discovery of New Respiratory Viruses

Viruses in May, 2011
NL63 has been found in respiratory samples from children with URTI & LRTI. (1.7%-9.3%)
Studies in German, Canada and South Korea showed that NL63 infection alone was the cause of croup and bronchiolitis in children.
Seasonal peaks have been described from January to March in temperate climates.
QPID was the first to show that HKU1 was more widespread than originally described. Samples from 2004 showed that 3.1% were positive for HKU1; most were children younger than 2 years of age.
A study in USA (n = 1048) showed 1% of respiratory samples (negative for other viruses) were positive for HKU1 and that clinical manifestations included URT & LRT disease.
The New Human Coronaviruses
Coronavirus NL63
Coronavirus HKU1
Viruses in May, 2011
The initial Swedish study showed that 3.1% of NPAs from children hospitalized with respiratory symptoms were positive for human bocavirus.
Additional evidence for infection early in life comes from a Swedish prospective study of a birth cohort, in which 4.5% of the first acute respiratory tract infection was attributed to human bocavirus.
The virus has now been identified on several continents with incident rates ranging from 1.5 to 20%.
Rates of co-infection have found to be very high (14-72%).
Evidence has shown that bocavirus causes both upper and lower respiratory disease.
Human Bocavirus – Respiratory Disease
Viruses in May, 2011
Role in acute gastrointestinal disease Early studies at QPID showed that HBoV was present in 4.8% of
stool samples collected from children with gastroentiritis.
Other studies showed HBoV in stools (0.8% - 9.1%) of patients with GE.
Recent discovery of new human bocaviruses causing GE in Pakistani & Scottish children
Possible role in the development of Kawasaki disease. Study in France, samples from children with Kawasaki disease
showed 31.2% of the samples positive for HBoV compared to 1.2% of controls.
High viral loads present in adenoidal and tonsillar tissue
Human Bocavirus – Other Disease

RSVPIVFLU A & BADVHRVHEVHCoVFLU CPIV 4HMPVHBoVNeg
11.2 3.5 4.1 6.0
32.8 2.5 2.3 1.1 0.6 7.0 5.2
23.7
%
32.8
23.7
11.2
Average Annual Incidence over 4 years
Study Samples Tested (N= 8200) - 2003 – 2006
Viruses in May, 2011
7.0
5.2
%
~24% of cases still
remained undiagnosed

To answer this question we used a dual approach: • Sought to identify new variants of known viruses • Initiated a virus discovery program

QPID had an interest in typing
rhinoviruses
Used high throughput sequencing
We noted an association of some HRV
strains with LRTI
Typing these, we identified a novel
HRV variant
These were mainly associated with asthma,
bronchiolitis or pneumonia
In the QPID laboratory
Ian Mackay Peter McErlean
(Post-doc) (PhD scholar)
36 additional novel HRV strains were
detected in 2500 specimens (1.4%)
collected during 2005-2006
These are now recognised as a new
rhinovirus subtype HRV type C
McErlean et al, JCV, March 2007 5’ UTR
Mc Erlean et al. PLoS ONE, 3(4): e1847.

PLoS ONE | April 2008 | Volume 3 | Issue 4 | e1847
JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2007, p. 3655–3664
Emerging Infectious Diseases • Vol. 14, No. 6, June 2008
J Clin Virol. 2009 Sep;46(1):85-9. Epub 2009 Jul 5.
Human Rhinovirus C
This study was a prospective population-based surveillance in 2 US counties among children <5 years of age hospitalized with acute RTI or fever from October 2001 to September 2003.
1052 children enrolled and tested for rhinoviruses by RT-PCR
167 (16%) had HRVs detected. o 147 samples successfully sequenced,
o 77 HRV-Cs, 64 HRV-As, 6 HRV-Bs.
Children with HRV-Cs significantly more likely than HRV-A to have underlying high-risk conditions, such as asthma (42% vs 23%, P=0.023) and to have had a discharge diagnosis of asthma (55% vs 36%, P=0.022).
Suggests this novel group causes a substantial burden of paediatric disease.
Human Rhinovirus C and Asthma

New Virus Discovery
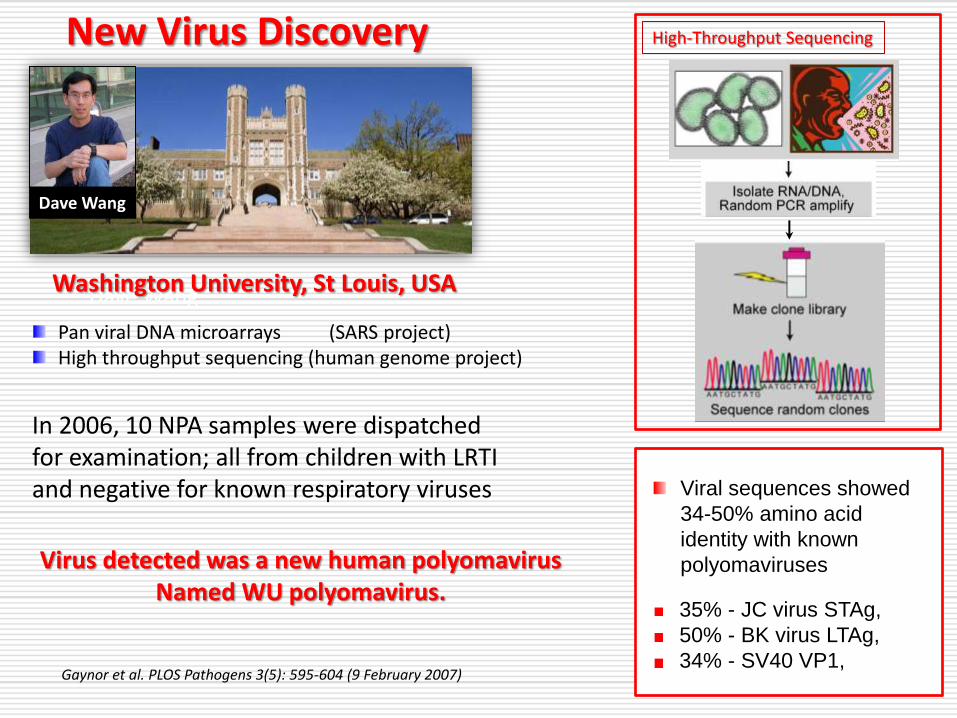
Dave Wang
Pan viral DNA microarrays (SARS project) High throughput sequencing (human genome project)
High-Throughput Sequencing
Viral sequences showed 34-50% amino acid identity with known polyomaviruses
35% - JC virus STAg, 50% - BK virus LTAg, 34% - SV40 VP1,
In 2006, 10 NPA samples were dispatched for examination; all from children with LRTI and negative for known respiratory viruses
Washington University, St Louis, USA
Dave Wang
New Virus Discovery
Dave Wang
Pan viral DNA microarrays (SARS project) High throughput sequencing (human genome project)
High-Throughput Sequencing
Viral sequences showed 34-50% amino acid identity with known polyomaviruses
35% - JC virus STAg, 50% - BK virus LTAg, 34% - SV40 VP1,
Virus detected was a new human polyomavirus Named WU polyomavirus.
Gaynor et al. PLOS Pathogens 3(5): 595-604 (9 February 2007)
In 2006, 10 NPA samples were dispatched for examination; all from children with LRTI and negative for known respiratory viruses
Washington University, St Louis, USA
Dave Wang
Viral sequences showed
34-50% amino acid
identity with known
polyomaviruses
35% - JC virus STAg,
50% - BK virus LTAg,
34% - SV40 VP1,
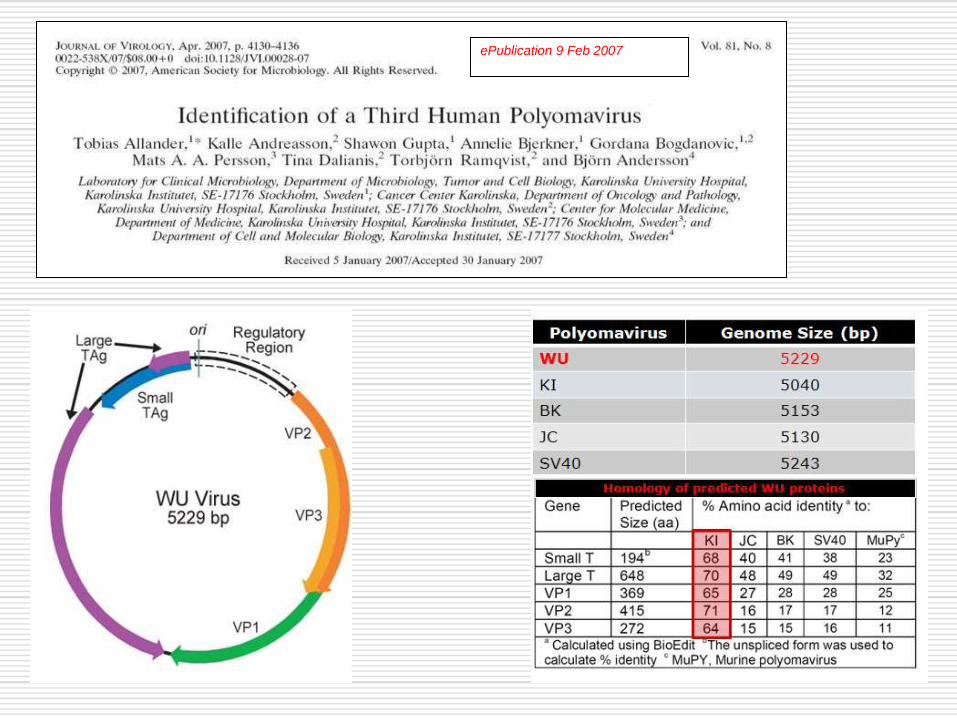
ePublication 9 Feb 2007
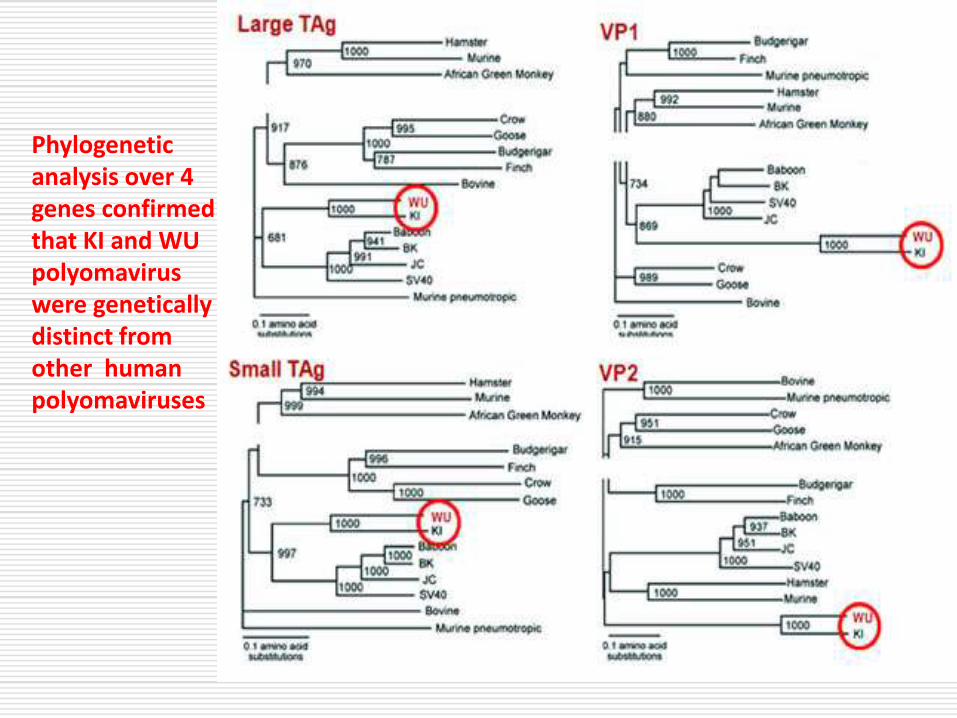
Phylogenetic analysis over 4 genes confirmed that KI and WU polyomavirus were genetically distinct from other human polyomaviruses

Little seasonal variation
was observed for KI
infection
Both KI and WU
polyomaviruses are
more prevalent in
children under 10 years
of age 0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
J F M A M J J A S O N D
KIV
WUV
Month
Perc
enta
ge P
ositiv
e
Bialasiewicz et al, J Clin Virol. 2007 Sep;40(1):15-8.
Bialasiewicz et al, J Clin Virol. 2008 Feb;41(2):63-8.
2866 respiratory samples collected from patients with acute respiratory tract infection (Jan—Dec 2003) were examined.
2.6% average annual prevalence of KI. (2009 = 3.8%) 4.5% average annual prevalence of WU (2009 = 5.8%)

N=1247 RSV IFAV PIV ADV HMPV HRV HCoV HBoV KIV WUV
Total detections
71 34 36 31 67 331 54 101 30 34
Single detections (% of total)
72% 74% 89% 52% 76% 75% 73% 39% 40% 27%
Co-detections) (% of total)
28% 26% 11% 48% 24% 25% 27% 61% 60% 73%
WU and KI polyomaviruses were frequently co-detected with
another respiratory virus.
6 [1]
(53%) (80%)
(17%)
(2%)
Out of 1247 samples tested, 53% had 1 or more viruses detected.
• 80% had 1 virus • 20% had more than 1
PIV was least frequently co-detected

Viruses in May, 2011
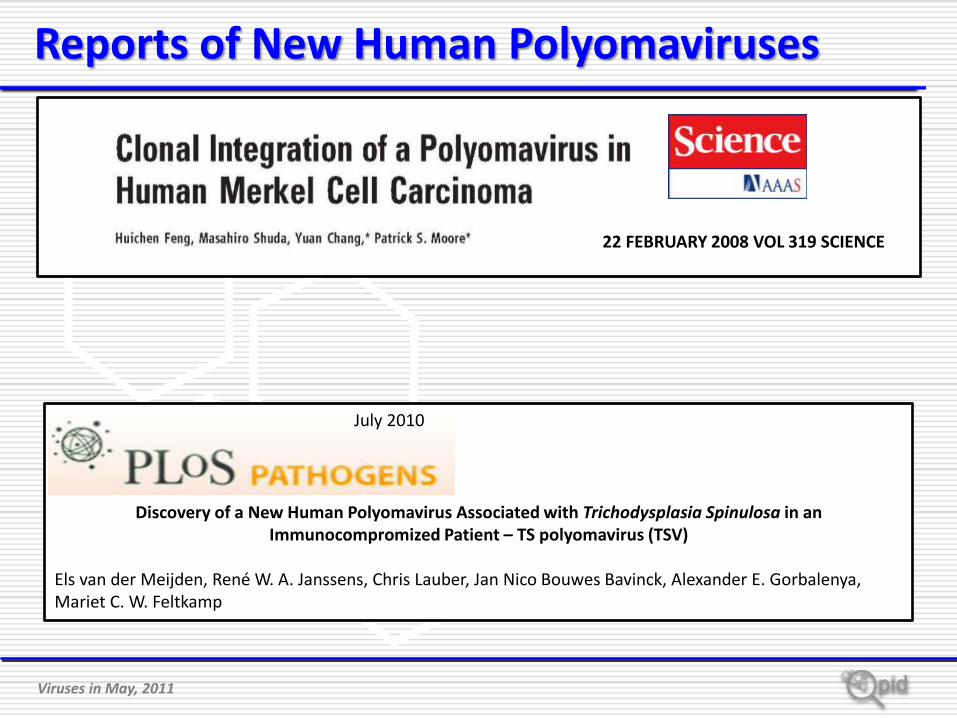
22 FEBRUARY 2008 VOL 319 SCIENCE
Reports of New Human Polyomaviruses
Emerging Infectious Diseases (2009), 15(3): 492-494
Viruses in May, 2011
22 FEBRUARY 2008 VOL 319 SCIENCE
Discovery of a New Human Polyomavirus Associated with Trichodysplasia Spinulosa in an Immunocompromized Patient – TS polyomavirus (TSV)
Els van der Meijden, René W. A. Janssens, Chris Lauber, Jan Nico Bouwes Bavinck, Alexander E. Gorbalenya, Mariet C. W. Feltkamp
July 2010
Reports of New Human Polyomaviruses
What is the Clinical Importance of These New Polyomaviruses ?
Are they new agents of respiratory disease?

Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 15, No. 8,
August 2009
By age 5 years ~90% of the population is
infected with WU and/or KI polyomavirus
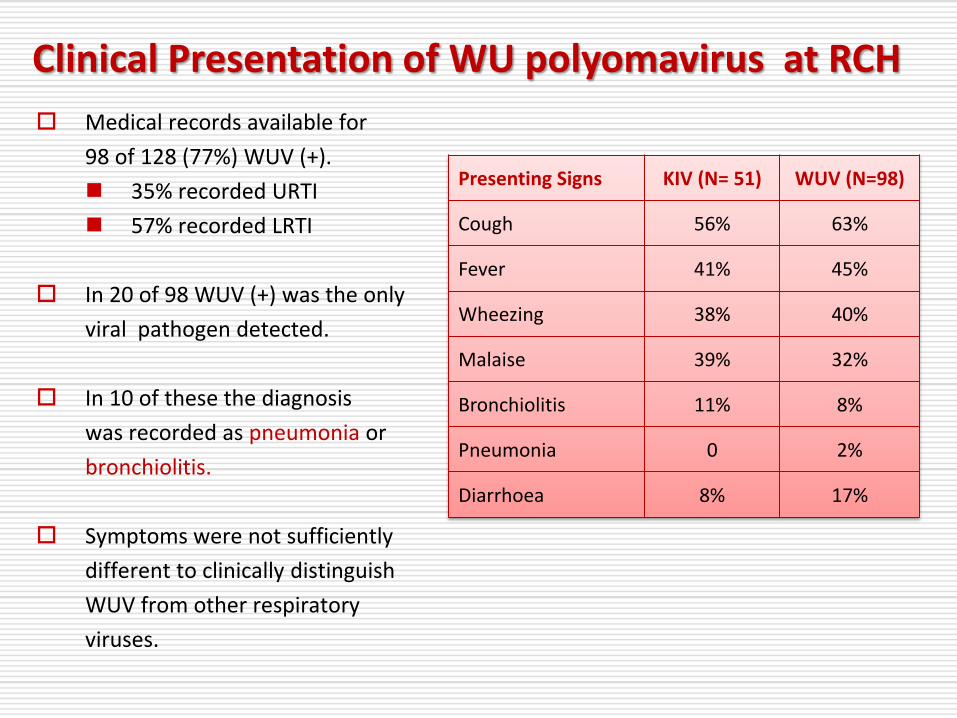
Medical records available for
98 of 128 (77%) WUV (+).
35% recorded URTI
57% recorded LRTI
In 20 of 98 WUV (+) was the only
viral pathogen detected.
In 10 of these the diagnosis
was recorded as pneumonia or
bronchiolitis.
Symptoms were not sufficiently
different to clinically distinguish
WUV from other respiratory
viruses.
Presenting Signs KIV (N= 51) WUV (N=98)
Cough 56% 63%
Fever 41% 45%
Wheezing 38% 40%
Malaise 39% 32%
Bronchiolitis 11% 8%
Pneumonia 0 2%
Diarrhoea 8% 17%
Clinical Presentation of WU polyomavirus at RCH


Sero-prevalence studies show first infection occurs in
children younger than 5 years of age.
WU and KI polyomaviruses are found in (6.8%) respiratory
secretions of patients with ARTI and not in controls
Prevalence of WUV is 6x greater in immunocompromised
children with ARTI compared with immunocompetent
children with ARTI.
WUV found in patients with progressive multifocal
encephalopathy (PML) in absence of other polyomaviruses.
MCV found in 24% of Merkel cell carcinoma biopsies
(integrated genome)
MCV also found in respiratory secretions (6%)

0.0
5.0
10.0
15.0
20.0
30.0
25.0
0.0
2.0
4.0
6.0
8.0
10.0
Jan-0
5
Feb-0
5
Mar-
05
Apr-
05
May-0
5
Jun-0
5
Jul-
05
Aug-0
5
Sep-0
5
Oct-
05
Nov-0
5
Dec-0
5
Jan-0
6
Feb-0
6
Mar-
06
Apr-
06
May-0
6
Jun-0
6
Jul-
06
Aug-0
6
Sep-0
6
Oct-
06
Nov-0
6
Dec-0
6
Jan…
Mar…
May…
Jul-…
Sep…
Nov…
Jan
-08
Fe
b-0
8
Ma
r-08
Ap
r-08
Ma
y-0
8
Jun
-08
Jul-0
8
Au
g-0
8
Se
p-0
8
Oct-
08
Nov-0
8
Dec-0
8
12.0
Su Au Wi Sp Su Au Wi Sp Su Au Wi Sp Su Au Wi Sp S
2005 2006 2007 2008
% P
ositiv
e o
f Tota
l Teste
d Influenza A
Influenza B
Until April 2009, specimens for clinical diagnosis of Influenza were tested using a consensus duplex real-time PCR assay for INF A & INF B targeting the gene coding for the matrix protein. *
This assay was previously validated against a large number of influenza A strains (human, avian) including H5N1**.
** Vietnamese; Indonesian strains
*Whiley et al. Diagnostic Microbiology and Infectious Disease 53 (2005) 335–337
Any Influenza A-positive samples are then screened further with a
H5N1-specific assay targeting the haemagglutinin gene. All positive specimens are forwarded to the QH Public Health Virology laboratory for Influenza typing and confirmation of any H5N1 result

The Australian National Incident Room (NIR) was notified by WHO on 24 April 2009 of outbreaks in Mexico & USA of a novel strain of A/H1N1 influenza (Swine flu).
H1N1 influenza 09 was a novel influenza A virus infecting humans.
H1N1 influenza 09 emerged after reassortment of human and swine-origin influenza strains, creating a virus against which humans had little or no immunity.
Positive control: Auckland influenza H1N1 2009 strain. (kindly provided by WHO-Melbourne, FSS-Brisbane)
Range of Flu Isolates: H3N2 (n=18) H1N1 (n=14) years 2000-2002 (kindly provided by FSS-Brisbane)
Wild-type porcine H1N1 (kindly provided by AAHL,Geelong )
Clinical samples: n = 152, from years 2008-2009 Influenza A - not detected n = 91
Influenza A - DETECTED n = 61 (H1N1 = 6; H3N2 = 23; Not typed = 32) (kindly provided by Pathology Queensland, Brisbane)
1. Can the Matrix consensus screening assay detect swine flu?
2. Need to develop a new real-time PCR assay for “swine flu” • H1 TaqMan (2009 A/H1N1 specific) • N1 TaqMan (2009 A/H1N1 specific)

1. Can the Matrix consensus screening assay detect swine flu?
2. Need to develop a new real-time PCR assay for “swine flu” • H1 TaqMan (2009 A/H1N1 specific) • N1 TaqMan (2009 A/H1N1 specific)
Assay protocol was transferred to Pathology Qld and introduced as a routine diagnostic procedure on 6 May 2009
RESULTS:
Matrix screening assay detected ALL subtypes including
human “swine flu”
Specific human swine flu assays ONLY detected pandemic
influenza H1N1 (2009)
The H1 assay was slightly more sensitive than the N1
assay (3 copies vs 8 copies/reaction)

First Australian case was detected by the Pathology Queensland laboratory on
the 7 May,
This result was confirmed by the WHO Reference
Laboratory on the 9 May,

First Australian case was detected by the Pathology Queensland laboratory on
the 7 May,
This result was confirmed by the WHO Reference
Laboratory on the 9 May, (June 6)

The integrated strategy for the detection of respiratory viruses in Queensland, delivers rapid, sensitive and specific results to the clinicians in Queensland Health
The extended screening of respiratory viruses provides comprehensive up to date epidemiological data about respiratory viruses circulating in our population.
Sophisticated molecular characterisation has resulted in the detection of new viruses, and previously unknown strains of known virus families.
Our current strategy allows a rapid response to new significant viral respiratory pathogens such as swine flu.
