immunology for surgeons: the basics 101 principles of surgery jeff warren, md, frcsc october 19,...
TRANSCRIPT
Immunology for Surgeons:The Basics 101
Principles of SurgeryJeff Warren, MD, FRCSC
October 19, 2010
Objectives The Players -- T-cells and B-cells Immunoglobulins Antigen Recognition Phagocytosis Mediators and Complement Immunization Hypersensitivity Reactions Transplant Immunology Basics

Immunology Conceptually challenging Complex series of reactions triggered by
immunogens Compartmentalize to simplify, but actual
events at molecular and cellular level are “boundary-less” and only partially understood
More we learn the less we know

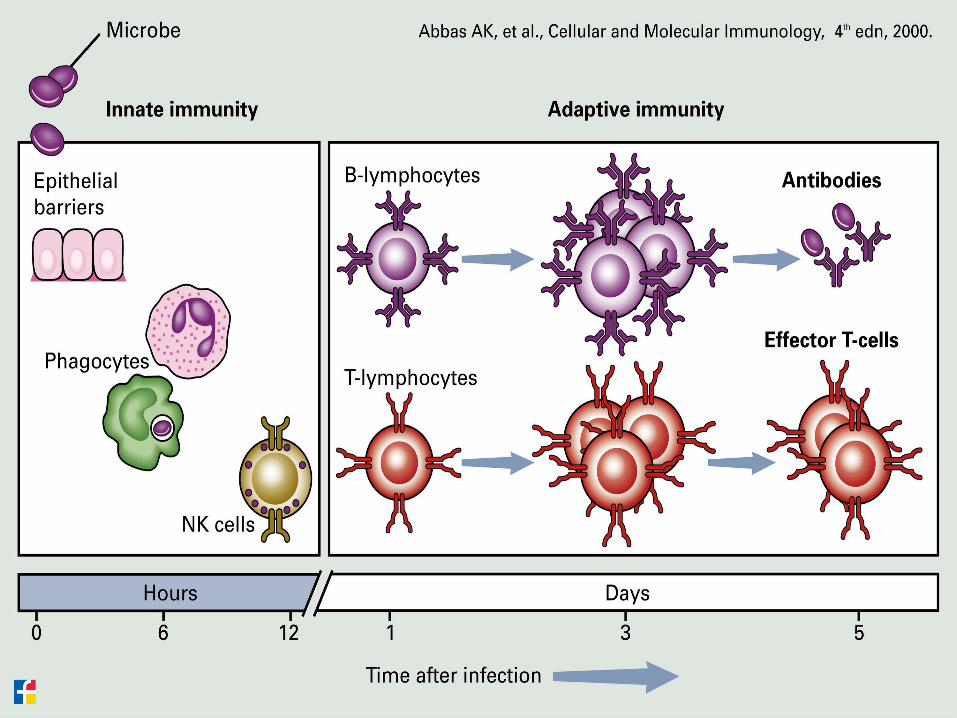
Introduction Innate vs Adaptive immunity Self vs non-self vs altered self Three phases of immune response:
Cognitive phase Activation phase Effector phase
Primary and Secondary responses Lymphoid organs: primary/secondary Humoral and Cell-mediated responses

Lymphocytes
T-cells Thymus CD3+ CD4+ -- Helper and DTH CD8+ -- cytotoxic and
suppressor
NK Cells Non B-cell, non T-cell
lymphocytes +IL-2 --> LAK cells
B-cells Bursa fasicularis (birds) Fetal liver and bone
marrow CD19+/CD20+ --> plasma cells --> Ab
production APCs

B-cell-->Plasma cell--> Ig production
IgA: secretory, dimer
IgG: most abundant, 2o response, opsonin, C’ binding
IgM: 1o repsonse, C’binding, pentamer IgE: mast cells and basophils, Type I hypersensitivity
IgD: small quantities, ??

Immunoglobulin
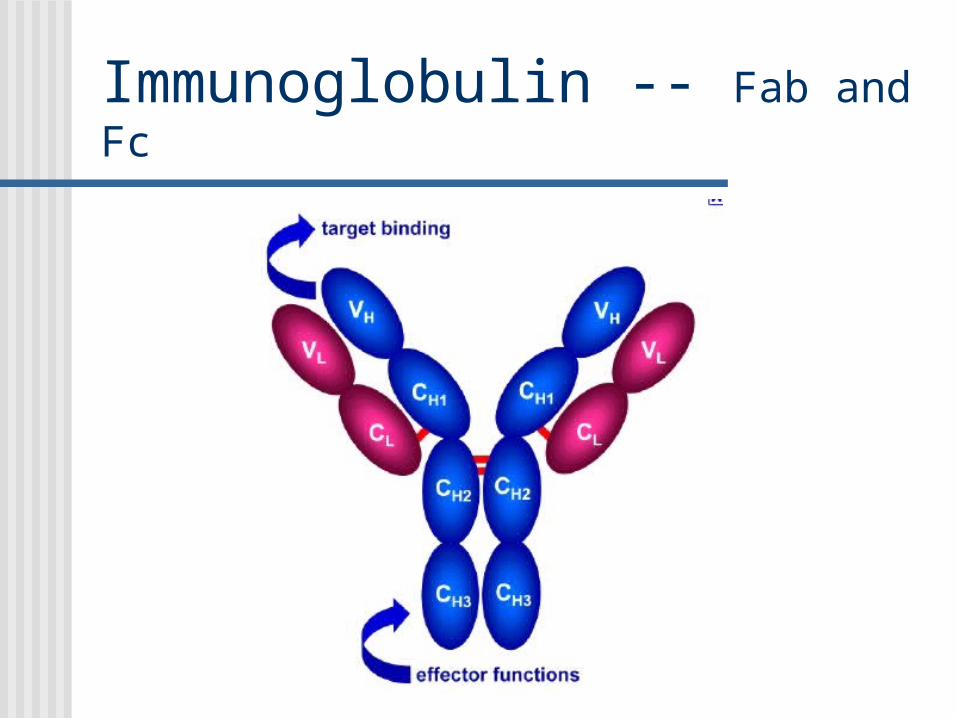
Immunoglobulin -- Fab and Fc

Antigen Recognition Immunogen: can stimulate immune response Antigen: recognized by immune system
Immunogenicity: Complexity: proteins > CHO > nucleic acids > lipids Size: usually > 5000 Da Foreigness: xenogeneic > allogeneic > syngeneic >
autologous

MHC HLA in humans on chromosome 6 With Ag --> Self vs non-self vs altered self Class I: A and B regions, on all nucleated cells and
platelets, recognized CD8+ T-cells --> lysis Class II: D region, on APCs, recognized CD4+ helper
T-cells --> activation and proliferation of helper T-cells (--> cytokines), cytotoxic T-cells (--> lysis), and B-cells (--> plasma cells --> Ab)
Class III: Complement
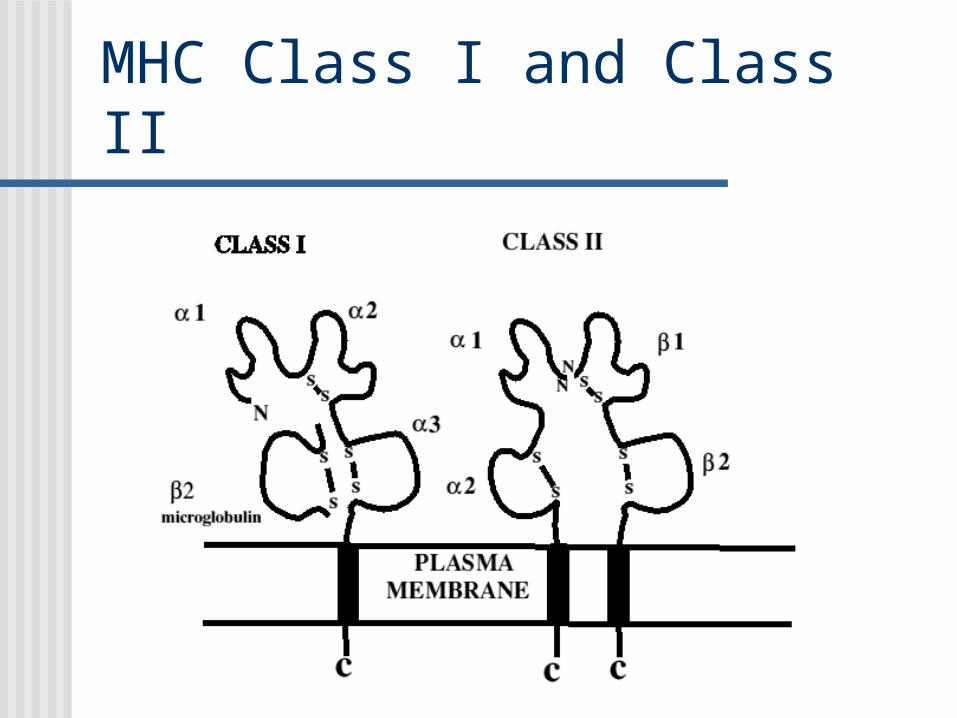
MHC Class I and Class II

Antigen Presenting Cells (APC) Capable of activating CD4+ T-cells Recognition usually occurs in 2o lymphoid
organs: spleen, lymph nodes, GALT, Peyer’s patches…
Monocyte and macrophage lineage: Dendritic cells (skin) Kupfer cells (liver) Glial cells (CNS)
B-cell subset

Anynucleatedcell
APC
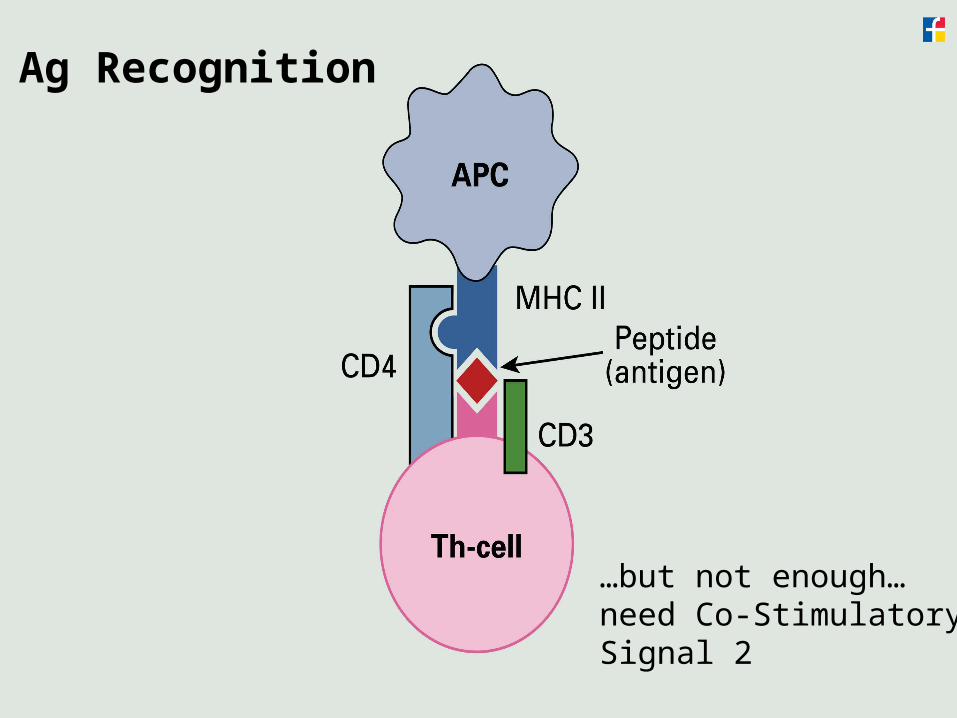
Ag Recognition
…but not enough…need Co-StimulatorySignal 2


T-cell receptor

Phagocytosis Mononuclear (monocytes) vs
polymorphonuclear (neutrophils) Engulfed foreign particle --> phagosome +
lysosome --> phagolysosome Oxygen-dependent mechanisms:
Myeloperoxidase, superoxide anion, H2O2, singlet O2, OH- radicals
Oxygen-independent mechanisms: Cationic proteins, lysozymes, proteinases
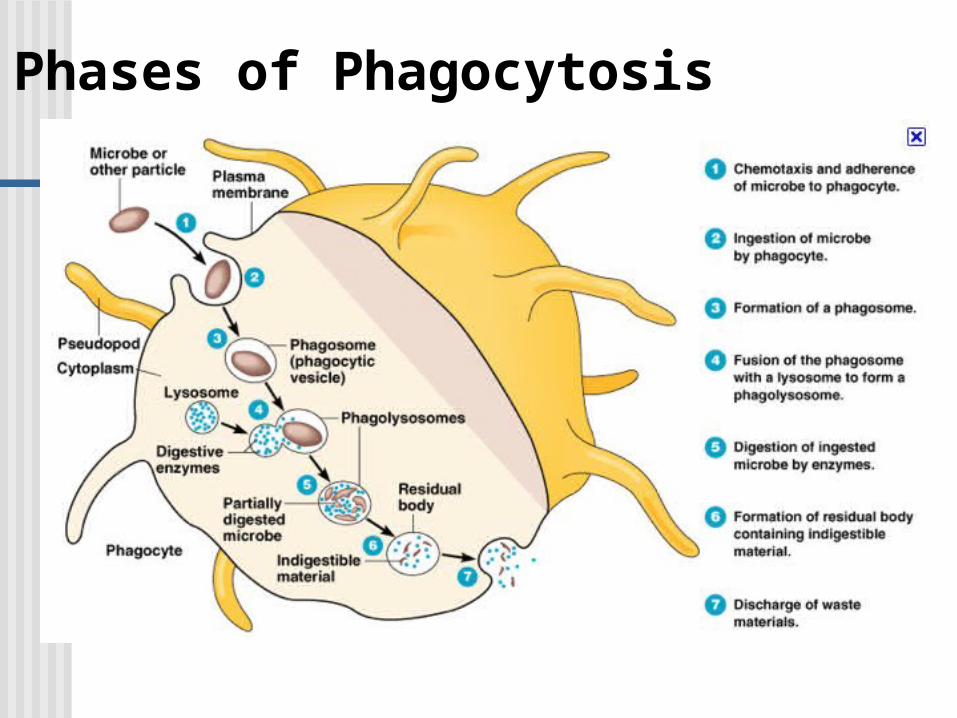
Phases of Phagocytosis

Complement Component proteins mediators of inflammation and cell lysis Numbered according to chronological discovery, not
necessarily order of activity in cascade reactions Traditionally divided into Classic, Alternative, and Lectin
pathways Small stimulus --> amplified effect Initiated by Ag-Ab immune complexes and microbial products C3a and C5a are chemotactic Some components are anaphylatoxins --> mast cell
degranulation, smooth muscle contraction, increased vascular permeability
End-product is C5b-8 MAC
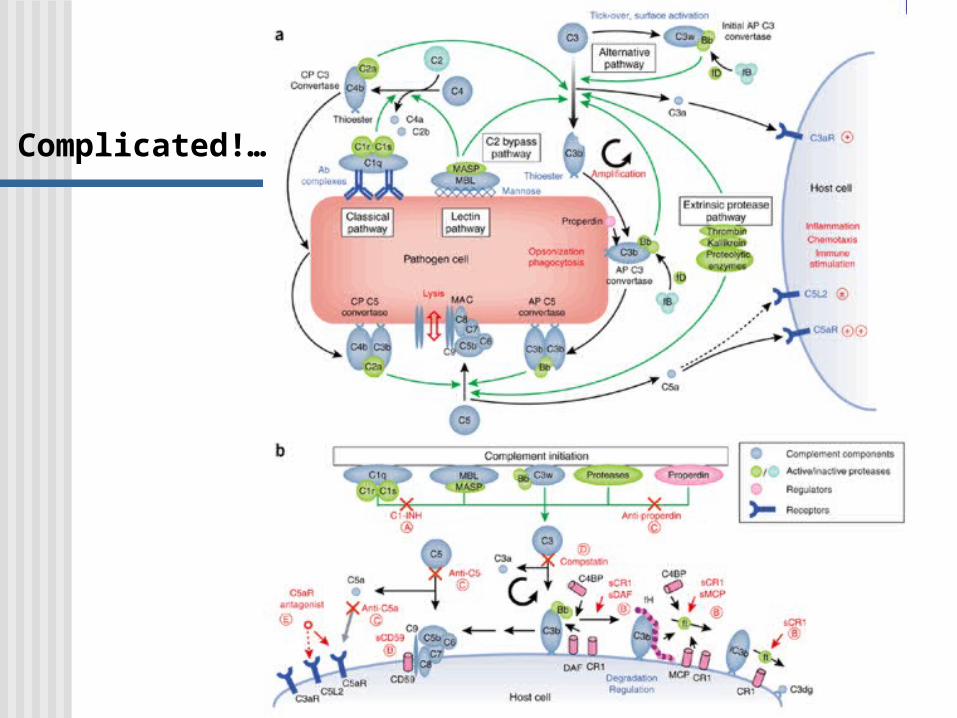
Complicated!…
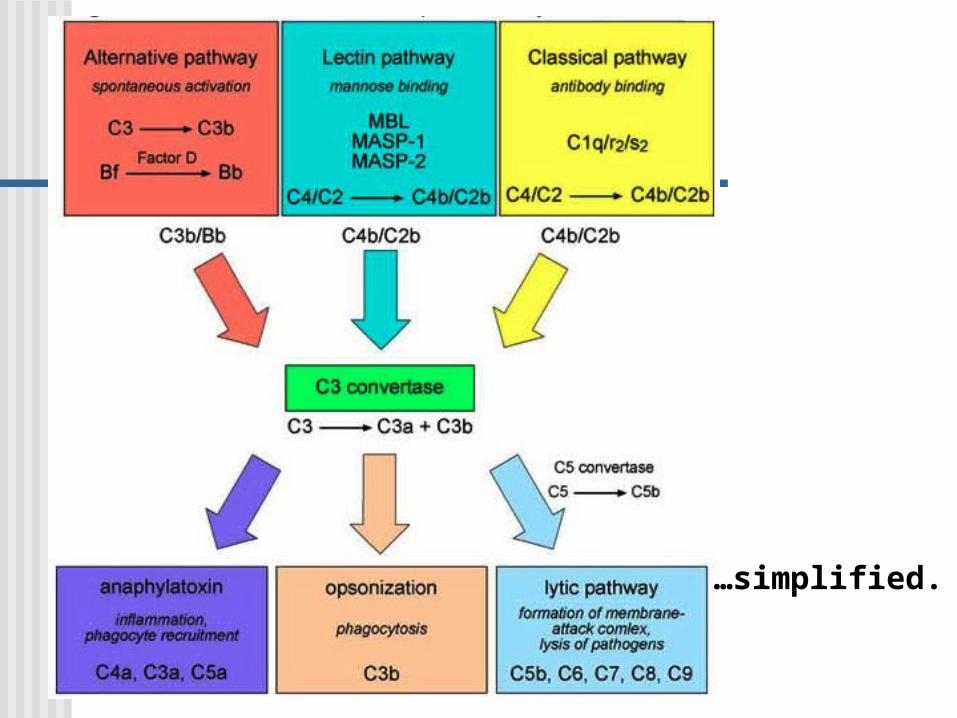
…simplified.

Cytokines
Greek -cyto, cell; and -kinos, movement Large group of cell-signaling molecules:
proteins, glycoproteins, peptides Grossly include interleukins, lymphokines,
and chemokines; redundancy and pleitropism make this classification obsolete today.

Interleukins IL-1: pro-inflammatory and wound healing; macrophages,
neutrophils, fibroblasts, NK cells, endothelial cells, vascular smooth muscle; fever, vasodilation, hypotension, collagen deposition, T-and B-cell proliferation, IL-2 and IL-2R up-regulation
IL-2: “T-cell growth factor” in response to IL-1; NK cells and activated T-cells (auto- and para-crine); up regulates many other cytokines, namely TNF and CSF; deficiency --> SCID
IL-3: hematopoetic growth factor IL-4: inhibits macrophages IL-6: inhibits TNF IL-8: neutrophil chemokine IL-10: inhibits monocytes/macrophages and anti-inflammatory
IL-4, 6, and 10 are “inhibitory” cytokines

IL-2

Tumor necrosis factor (TNF) Hemmorhagic necrosis in methycholanthrine -induced
sarcomas in mice
TNF-alpha: 1o monocytes/macrophages, but NK cells and neutrophils also Stimulates neutrophils Endothelial cells --> IL-1 Procoagulant, increased vascular permeability Catabolism and cachexia in malignant disease Apoptotic mediator Gram negative shock --> endotoxin --> TNF-alpha -->
hypotension + DIC TNF-ß: T- and B-cells
Wound healing, PG and collagen deposition Cytolytic and cytostatic for many tumor cell lines


Interferons Glycoproteins Inhibit viral proliferation via signaling pathways and
translation machinery inhibition INF-alpha -- macrophages INF-beta -- epithelial cells, fibroblasts, macrophages INF-gamma -- T-cells and NK cells Antiproliferative Can induce differentiation Stimulate or inhibit a variety of cells to release other
cytokines
Chemokines Low molecular weight cytokines that serve as
chemoattractants 4 cysteine molecules linke by disulfide bonds C-C or C-X-C and their receptors IL-8 is actually a chemokine that binds CXCR1
or CXCR2 on neutrophils 100s of chemokines identified and the
catalogue continues to grow!


Immunization Active: injection of intact attenuated organism or
component. Recipient mounts an immune response with the goal being memory DPT, MMR, pneumovax, HepB, vaccine, polio vaccines
Passive: exogenous active component is given to recipient; immediate but temporary immunity Antitoxins: C.tetani antitoxin Immunoglobulin: IgG to immundeficient recipient Specific immune globulin: RhoGAM (prevent sensitization to Rh
Abs crossing placenta from Rh+ infant at delivery)

Who were these guys?…
Dr. Albert Sabin Dr. Jonas Salk

Hypersensitivity Reactions Type I: immediate hypersensitivity
IgE mediated --> mast cells and basophils Anaphylaxis, hay fever, food allergy
Type II: cytotoxic reactions IgG and/or IgM mediated; preformed Abs ABO and Rh incompatibility, myasthenia gravis, Graves disease, ITP
Type III: immune complex mediated Deposition of Ab-Ag complexes PSGN, serum sickness, SLE, rheumatoid arthritis
Type IV: DTH Previously sensitized CD4+ T-helper cells Tuberculin skin test, contact dermatitis

Transplant Rejection Hyperacute
Preformed Ab; immediate: “in the OR” ABO incompatible or high titre donor specific HLA Class I
Ab Acute
T-cell mediated; days to weeks Treatment and prevention via T-cell depletion: ATG or IL-
2R blocker Chronic (CAN)
Kidneys IF/TA Immune and non-immune mechanisms Difficult to predict, prevent, or belay

Alternative: ANTIBODY vs CELLULAR rejection

THE END
Thank you and Good Luck!