immunoprint pattern in patients with allergic bronchopulmonary aspergillosis in different stages
TRANSCRIPT

noprint pattern in patient with aller onchopulmonary aspergillosis in
nt stages
Baur,* W. Weiss,* B. Jarosch,* G. Menz,** Chr. Schoch,** s Schmitz-Schumann,** and Chr. Virchow** Munich, West Germany, and
Davos-Wolfgang, Switzerland
lndividual immunoprint patterns of sodium dodecylsulfate-polyactylamide gel electrophoresis-separated Aspergillus fumigatus (Af) allergenslantigens were evaluated in 28 patients with allergic bronchopulmonary aspergillosis in stages II to V. It could be demonstrated that active disease (stage III) is characterized by a very strong IgE response against a variety of Af components, whereas the IgE antibody pattern in corticosteroid-treated patients who have demonstrated improvement is much weaker. In patients in remission (stage III, it is minimal. In contrast, many patients in stage V without corticosteroid treatment demonstrated a strong reactivity of IgE antibodies, indicating persisting active disease. The pattern of IgG antibodies with individual Af components resembles, in general, that of IgE antibodies; however, discrimination between different stages and between treated patients is much weaker. Our results indicate that a certain relationship between the different stages of allergic bronchopulmonary aspergillosis and Af immunoprint patterns exists. (J ALLERGY CLIN IMWNOL 1989;83:839-44.)
Because of unknown factors, the course of ABPA may be quite diverse. After several exacerbations, some patients demonstrate permanent remission, whereas other patients develop severe relapses during many years, which may eventually result in progres- sive lung fibrosis. The aim of our investigations was to examine whether the different stages of the disease correlate with variations in immunologic activity and, especially, whether they differ in their distinct anti- body patterns to individual electrophoretically sepa- rated Af allergens / antigens.
ATERIAL AND METHODS Patients
All patients had asthma and fulfilled at lesat six of the following seven criteria, as proposed by Rosenberg et al.’ and Patterson et al.? (1) blood eosinophilia >lOOO/mm’, (2) immediate cutaneous reactivity to Af antigens, (3) pre- cipitating antibodies against Af antigens, (4) elevated serum
From the *Pneumoiogische Abteilung, Medizinische Klinik I, Uni- versitlt, Miinchen, and **Hochgebirksglinik Davos-Wolfgang, Asthma- und Ailergieklinik, Davos-Wolfgang, Switzerland.
Received for publication June 21, 1988. Accepted for publication Oct. 24, 1988. Reprint requests: Xaver Baur, MD, Klinikum Grosshadem, PF 701
260, D-8000 Munich 70, West Germany.
Abbreviations used Af: Aspergillus fumigatus
ABPA: Allergic bronchopulmonary aspergillosis
SDS-PAGE: Sodium dodecylsulfate- polyacrylamide gel electrophoresis
PA: Protein A NC: Nitrocellulose
BSA: Bovine serum albumin MW: Molecular weight
q.o.d.: Every other day
IgE concentration, (5) history of roentgenographically il- lustrated infiltrates, (6) central bronchiectasis; and (7) ele- vated serum IgE and IgG antibodies to Af. Finally, the 28 patients with ABPA were subdivided into stages I to V, according to Patterson et al.*: acute stage, I; remission, II; recurrent exacerbation, III; co~icosteroid-dcpeodent asthma, IV; and fibrotic lung disease, V.
None of the patients were in stage I (acute stage). Du- ration of remission of patients 2.1 t3 2.5 (stage II, see Fig. 2, A) was at least 6 months. Recurrent exacerbations had occurred for at least 2 years in patients 3. I to 3.8 (stage III, see Fig. 2, B); all patients had exacerbation at the time of this study, although patients 3.1 and 3.4. only to a minor degree.
Corticosteroid treatment of patients 4.1 to 4.7 (stage IV,

3Q-
Af
FIG. 1. SDS-PAGE of Af proteins; A4, MW markers (protein stain); Ai” AF protein stain.
see Fig. 2, C) ranged from 1 to 5 years (mean 2.5 years), prednisone dose from 5 to 50 mg per q.o.d.
reparation of Af extract
Af antigens (Precipithal) were purchased from HAL (Haarlem, The Netherlands). Three batches were mixed, dissolved in water, dialyzed against 0.1% SDS, and stored at - 20” C until required.
Protein content of the extract was determined by the method of Lowry with the protocol described by Peterson3 BSA was used as standard.
Measurement of IgE antibodies to Af proteins
Specific IgE antibodies to Af proteins were estimated by the IgE RAST method (Pharmacia, Uppsala, Sweden), ac- cording to the manufacturer’s instructions.
Measurement of IgE antibodies to Af roteins (PA RAW)
PA RAST was performed as previously described.4 Briefly, A&coated paper disks were incubated in 100 p,l of human sera (diluted 1: 1600) for 18 hours. After disks were washed, they were then incubated for 2 hours in 100 pl of ‘Z51-labeled PA solution (approximately 80,000 cpm). Fi-
nally, after a further wash, the bound radioactivity was counted. Results are expressed in arbitrary units, as pub- lished previously.4 Values >2 U (co~espo~ding to values greater than the mean values + 2 SD of the healthy control subjects) were interpreted as positive.
Paper disks coated with Af proteins used for IgE RAST and PA RAST were purchased from Pharmacia.
lmmunoblotting method
SDS-PAGE. The Af extract was boiled for 3 minutes in 50 mmol/L of Tris HCL (pH 6.8) containing 2% SDS, 5% 2-mercaptoethanol, 10% sucrose, and 0.05% bromophenol blue; 1.5 ml of this solution (2 mg of protein per milliliter) was applied to a 12.5% polyacrylamide slab gel with a one- well comb. SDS-PAGE was carried out with the discontin- uous buffer system, described by Laemmhs
Blotting (electrophoretic transfer). On completion of SDS-PAGE, the separated polypeptides were electroblotted onto NC membranes (pore size 0.45 pm) (Schleicher & Schuell, Kassel, West Germany), according to the method of Towbin et al.6 Transfer was performed at 25 V overnight; transfer buffer was 25 mmol/L Tris, 192 mmollL glycin, 0.1% SDS, and 20% methanol, pH 8.5.
Detection of Af antigens/allergens. After the transfer of proteins to NC sheets, the matrix was either directly stained with the protein dye amido black (unspecific protein stain- ing) or allergens/antigens were specifically detected with an immunologic reaction. In the latter case, the NC membrane was first incubated with a blocking solution (Tris-saline, pH 7.5, 2.5% BSA, and 0.5% Tween 20) for 1 hour at 37” C to saturate the unspecific binding sites of the NC membrane. For immunodetection, the NC membrane was then cut into 5 mm wide longitudinal strips, which were incubated with patients’ sera overnight, as follows: For de- tection of IgG antibodies, 50 pl of serum (diluted 1: 50 in 0.9% saline and 3% BSA) was applied to each NC strip, and for detection of IgE antibodies, 200 ~1 of serum (diluted 1: 10) was applied to each NC strip.
After NC strips were washed with buffer (0.9% saline and 0.2% Tween 20), specifically bound human anti.bodies were detected with ‘251-labeled PA or ‘251-labeled anti-&E as second antibodies.
The isotope activity was I.5 X lo5 (PA) and ‘7 X lo4 cpm (anti-IgE), respectively (incubation time, 4 to 6 hours). After final washes, the NC strips were air-dried, and au- toradiographs were produced by exposing Kodak X-GMAT AR films (Eastman Kodak, Co., Rochester, N.U.) at - 70” C for 2 to 7 days. Single tests were performed, since preliminary studies had demonstrated highly ~eprodncible results. With this method we previously had de~~ons~ated that sera of healthy control subjects exhibited some weak IgG bands but no reactivity of IgE antibodies.4
RESULTS IgE RAST and PA RAST
With respect to IgE RAST and RAST results alone, there appeared to be no ~ig~i~c~t variation
VOLUME 83 NUMBER 4
lmmunoprint pattern in patients with ASP
ABPA-Patients in stage It ABPA-Patients in Stage 111
MW WI 94 - 67-
45-
30 -
a-
lb-
c
3.1 3.2 3.3 3.4 3.5 3.6 --..-_ ._. -.“-__. --^__ _ 3.7 3,s ABPA-Patimts Pn stage V .
4.1 42 4.3 44 4.5 4.6 4.7 5.1 5.2 5.3 5.4 5.5 5.6 5. 5.6
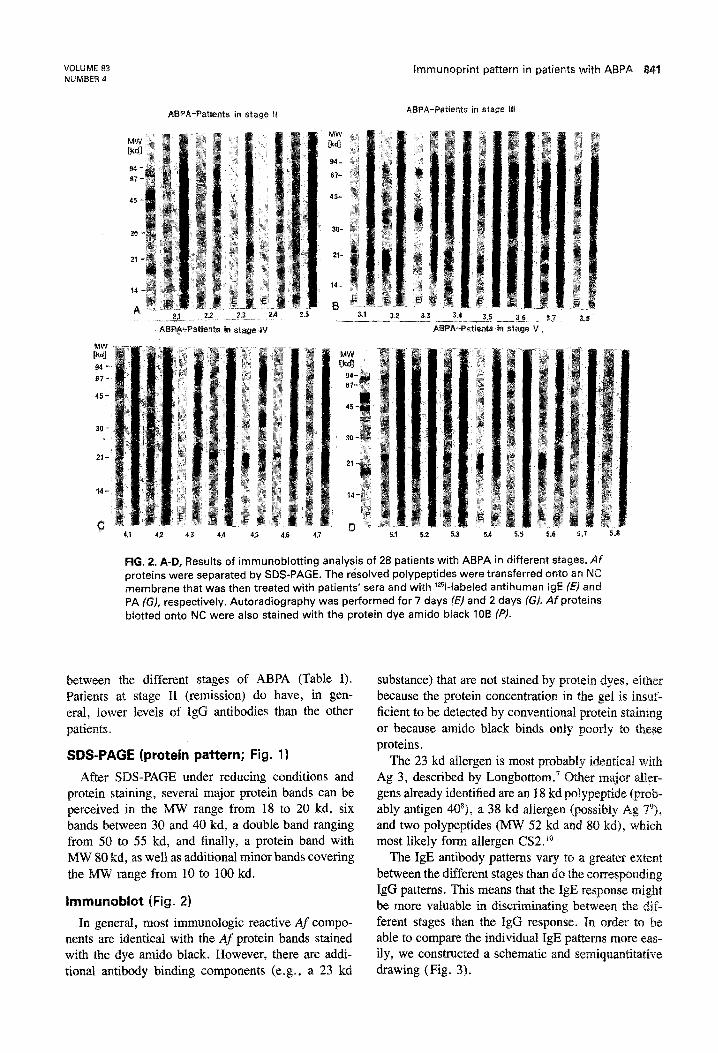
FIG. 2. A-D, Results of immunoblotting analysis of 28 patients with ABPA in different stages. Af proteins were separated by SDS-PAGE. The resolved polypeptides were transferred onto en NC membrane that was then treated with patients’ sera and with ‘Z51-labeled antihuman IgE (E) and
PA (G), respectively. Autoradiography was performed for 7 days IL?) and 2 days (G). Afproteins blotted onto NC were also stained with the protein dye amido black IOB (P).
between the different stages of ABPA (Table I). Patients at stage II (remission) do have, in gen- eral, lower levels of IgG antibodies than the other patients.
SDS-PAGE (protein pattern; Fig. 1)
After SDS-PAGE under reducing conditions and protein staining, several major protein bands can be perceived in the MW range from 18 to 20 kd, six bands between 30 and 40 kd, a double band ranging from 50 to 5S kd, and finally, a protein band with MW 80 kd, as well as additional minor bands covering the MW range from 10 to 100 kd.
Irnmunoblot (Fig. 2)
In general, most immunologic reactive Af compo- nents are identical with the Af protein bands stained with the dye amido black. However, there are addi- tional antibody binding components (e.g., a 23 kd
substance) that are not stained by protein dyes, either because the protein concentration in the gel is insuf- ficient to be detected by conventional protein staining
or because amido black binds only poorly to these proteins.
The 23 kd allergen is most probably identical with Ag 3, described by Longbottom. Other major alEer- gens already identified are an I8 kd polypeptide (prob- ably antigen 408), a 38 kd allergen (possibly Ag Tp), and two polypeptides (MW 52 kd and 80 kd), which most likely form allergen CS2.”
The IgE antibody patterns vary to a greater extent between the different stages than do the ~~~esp~~d~~g IgG patterns. This means that the IgE response might be more valuable in discriminating between the dif- ferent stages than the IgG response. In order to be able to compare the individual IgE patterns more eas- ily, we constructed a schematic and s~mi~~~~ti~tive drawing (Fig. 3).

aur et al. J. ALLERGY CLIN. IiMMLiNOL. APiU. 1989
. . .0.llQ
. . q m.m . .m..n
QO q .n QnmQn
q 0..0
3.1 32 33 3.4 35 3.6 3.7 3.8 III
FIG. 3. immunoblotting of Af allergens. Schematic pattern of Af allergens recognized by IgE antibodies of 28 patients with ABPA in different stages. Bands that were visible on X-ray film after 2 days of autoradiography (ml; bands appearing after 4 days (BI); bands that could only be observed after 1 week’s autoradiography (El).
limmunoblot pattern of patients in stage IA (remission)
Most striking, and very typical for these patients, is the poor IgE reaction, which demonstrated ony a few and very weak binding bands (Fig. 2, A). The TgG reaction is weaker than that observed with patients in the other stages, but in spite of low antibody levels to At, as measured by PA RAST, there is no great difference in the IgG band distribution throughout the various stages.
~mmu~oblo~ pattern of patients in stage Ill [recurrent exacerbation)
The numerous, very distinct IgE binding bands are distributed over the entire MW range from 12 to 90 kd. The IgG pattern is very similar to the IgE pattern (Fig. 2, B).
~mrnu~oblo~ pattern of patients in stage IV (corticosteroid-dependent asthma)
In most cases, strong IgE binding to Af allergens is observed only in the range from 18 to 23 kd, and weaker binding can be observed from 30 to 80 kd (Fig. 2, C). The IgG pattern is very distinctive with clear bands observed in the range of 18 to 80 kd.
ithin this patient group results do not appear to vary greatly in relation to corticosteroid dosage, since pa- tients with >16 mg of prednisone, q.o.d., demon- strated no significant differences from patients with <16 mg of prednisone, q.o.d.
lmmunoblot pattern of patients i (fibrotic lung disease)
These patients appeared to be composed of two subgroups, one demonstrating strong and another subgroup demonstrating weak antibody reactivity. The different reactivity did not correlate with corticoste- roid treatment carried out in a clinical setting. In gen-
eral, the IgE pattern in the MW region of 18 kd is similar to that of patients in stage III. However, < 18 kd, no, or only poor, antibody binding is observed (Fig. 2, D). The IgG pattern does not differ greatly from that of patients in stages III and IV.
DISCUSS10
In our experiments, some differences were dem- onstrated to exist between the intensity of the im- munoblot pattern and the concentrations of IgE and IgG antibodies (as evaluated by IgE RAST and PA RAST). One reason may be that different extracts were used in these methods; another reason may be that individual antigens/allergens may not be present in comparable amounts in the two techniques. In ad- dition, it should be mentioned that PA RAST values <2 U do not indicate absence of A&specific IgG an- tibodies, since this value represents that which ferentiates best between healthy persons and patients with ABPA.4 It is well-known that even healthy ger- sons have specific IgG antibodies against common allergens, including Af, this was also demonstrated with the immunoblot method in our previous study.”
VOLUME. 83
MUMSER 4 lmmunoprint pattern in patients with A
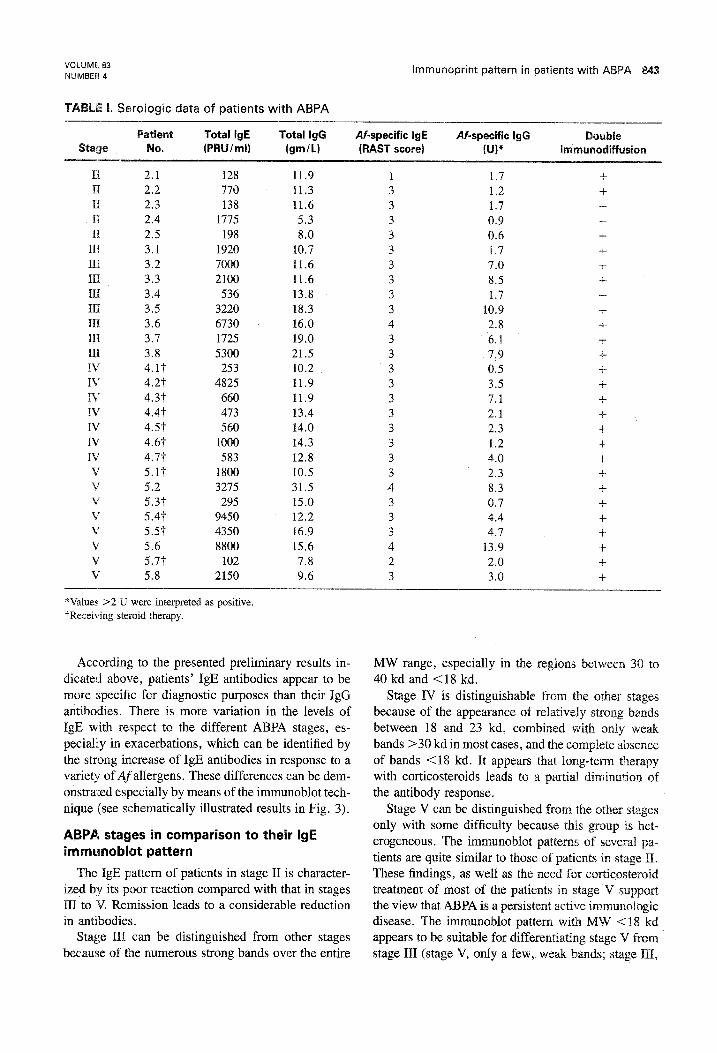
1. Serologic data of patients with ABPA
II 2.1 128 11.9 1 1.7 f 11 2.2 770 11.3 3 1.2 + II 2.3 138 11.6 3 1.7 4 II 2.4 1775 5.3 3 0.9 -
II 2.5 198 8.0 3 0.6 + III 3.1 1920 10.7 3 1.7 -t III 3.2 7000 11.6 3 7.0 + III 3.3 2100 11.6 3 8.5 + III 3.4 536 13.8 3 1.7 III 3.5 3220 18.3 3 10.9 -I- III 3.6 6730 16.0 4 2.8 -I- III 3.7 1725 19.0 3 6.1 + III 3.8 5300 21.5 3 7.9 + IV 4.1’F 253 10.2 3 0.5 + IV 4.2t 4825 11.9 3 3.5 + Iv 4.3t 660 11.9 3 7.1 + IV 4.4t 473 13.4 3 2.1 + IV 4.5t 560 14.0 3 2.3 l- IV 4.67 1000 14.3 3 1.2 -k IV 4.7t 583 12.8 3 4.0 + V 5.1t 1800 10.5 3 2.3 + V 5.2 3275 31.5 4 8.3 i- v 5.31‘ 295 15.0 3 0.7 + V 5.4t 9450 12.2 3 4.4 + v 5.51‘ 4350 16.9 3 4.7 + V 5.6 8800 15.6 4 13.9 + V 5.77 102 7.8 2 2.0 -I- V 5.8 2150 9.6 3 3.0 +
*Values >2 U were interpreted as positive, $Receiving steroid therapy.
According to the presented preliminary results in- dicated above, patients’ IgE antibodies appear to be more specific for diagnostic purposes than their IgG antibodies. There is more variation in the levels of IgE with respect to the different ABPA stages, es- pecially in exacerbations, which can be identified by the strong increase of IgE antibodies in response to a variety of Af allergens. These differences can be dem- onstrated especially by means of the immunoblot tech- nique (see schematically illustrated results in Fig. 3).
ABPA stages in comparison to their IgE Emmunoblot pattern
The IgE pattern of patients in stage II is character- ized by its poor reaction compared with that in stages III to V. Remission leads to a considerable reduction in antibodies.
Stage III can be distinguished from other stages because of the numerous strong bands over the entire
MW range, especially in the regions between 30 to 40 kd and ~18 kd.
Stage IV is distinguishable from the other stages because of the appearance of relatively strong bands between 18 and 23 kd, combined with only weak bands >30 kd in most cases, and the complete absence of bands Cl8 kd. It appears that long-term therapy with corticosteroids leads to a partial diminution of the antibody response.
Stage V can be distinguished from the other stages only with some difficulty because this group is het-
erogeneous. The immunoblot patterns of several pa- tients are quite similar to those of patients in stage II. These findings, as well as the need for co~ic5steroid treatment of most of the patients in stage V support the view that ABPA is a persistent active immunologic disease. The immunoblot pattern with MW Cl8 kd appears to be suitable for differentiating stage V from stage III (stage V, only a few, weak bands; stage III,

Baur et ai.
strong bands). To differentiate stage V from stage IV, the pattern in the region of 30 to 80 kd is best (stage V, strong bands; stage IV, weaker bands in most cases).
In short, there are recognizable differences between the various stages of ABPA. In current research, these findings could be substantiated by sequential patterns of three patients, two of whom progressed from stage II to stage III, and the third patient,” went into re- mission out of stage III. However, within the different stages, we observed no correlation between the im- munologic data on the one hand and the severity of clinical manifestations on the other hand. For differ- ential diagnoses it is noteworthy that subjects with asthma, but not ABPA, sensitized to Af exhibit only a few IgE bands comparable to stage II and that the IgG antibody reactivity of these patients is much weaker. I2
EFERENGES
Rosenberg M, Patterson R, Mintzer R, Cooper J, Roberts M, Harris KE. Clinical and immunological criteria for the diag- nosis of allergic bronchopulmonary aspergillosis. Ann Intern Med 197786:405’-14. Patterson R, Greenberger PA, Radin RC, Roberts M. Allergic bronchopuimonary aspergillosis: staging as an aid to manage- ment. Ann Intern Med 1982;96:286-91. Peterson GL. A simplification of the protein assay method of
4.
5.
6.
7.
8.
9.
10.
11.
12.
Lowry et al. which is more generally applicable. Anai Rio&em 1977;83:346-56. Dewair M, Baur X. Radioallergosorbent test (RAST) for ;he measurement of IgG antibodies to Aspergillusfumigatus in sera of patients with different lung disease. J Immunol Meth 1984;75:117-28. Laemmli UK. Cleavage of structural proteins during the as- sembly of the head of bacteriophage T4. Nature 1970;227:680- 85. Towbin H, Staehelin T, Gordon J. Electrophoretic transfer of proteins from polyacrylamide gels to nitrocellulose sheets: pro- cedure and some applications. Proc Nat1 Acad Sci USA 1979;74:4350-4. Longbottom JL. Antigens and allergens of Aspergillus f~mi- gatus. II. Their further identification and partial cbaracteriza- tion of a major allergen (Ag 3). J ALLERGY CLIN IMMUNOL 1986;78:18-24. Wallenbeck I, Aukrust L, Einarsson R. Antigenic variability of different strains of Aspergillus fumigatus. Int Archs Allergy Appl Immunol 1984;73:166-72. Harvey E, Longbottom JL. Characterization of a major anti- genie component of Aspergillus fumigatus. Clin Exp Immunol 1986;65:206-14. Piechura JE, Huang CJ, Cohen SH, Kidd JM, Kurup VJ, Calvanico NJ. Antigens of Aspergillus fumigates. II. Elec~o- phoretic and clinical studies. Immunology 1983;49:657-65. Baur X, Hahn D, Weiss W. Allergic bronchopulmonaq as- pergillosis with alveolitis and bronchial asthma induced by bay dust [in press]. International synopses. Baur X, Dewair M. Immunodiagnostik Aspergillus-bedingter bronchopulmonaler Erkrankungen. Schweiz Med Wochenscbr 1985;115:757-63.