impact of cancer, type, site, stage and treatment on the nutritional
TRANSCRIPT

Impact of Cancer, Type, Site, Stage and Treatment on theNutritional Status of Patients
F. BOZZETTI, M.D., S. MIGLIAVACCA, M.D., A. SCOTTI, M.D., M. G. BONALUMI, M.D., D. SCARPA, M.D.,F. BATICCI, M.D., M. AMMATUNA, M.D., A. PUPA, M.D., G. TERNO, M.D., C. SEQUEIRA, M.D.,C. MASSERINI, M.D., H. EMANUELLI, M.D.
This study analyzed the nutritional status of cancer patientsin relation to type and site of origin of the tumor, stage ofdisease, and previous chemical or radiation therapy. The anal-ysis was performed on 321 patients (280 with cancer and 41controls). The nutritional parameters included per cent ofweight loss, anthropometric indices (arm circumference, tricepsskinfold, arm muscle circumference), creatinine-height index,serum protein, albumin, total iron binding capacity and cho-linesterase, C3 and C4 components of complement, total pe-ripheral lymphocytes, and skin tests. The statistical comparisonbetween patients with different tumors and controls, betweenpatients with different stages of the same tumor, and betweenpatients treated with or without previous chemical or radiationtherapy led to the following conclusions: 1) malnutrition ismainly related to the type and site of origin of the tumor and,in the early stages of disease, is more pronounced in patientswith cancer of the esophagus and stomach; 2) except in patientswith breast and cervix cancer, malnutrition gets more severeas the disease becomes advanced; 3) chemical or radiation ther-apy has a variable impact on the nutritional status, but in se-lected patients it causes a drop in body weight, arm circum-ference, arm muscle circumference, and peripheral lymphocytes;4) body weight, cutaneous delayed hypersensitivity and serumalbumin are the most commonly altered parameters.
A LTHOUGH RECENT SURVEYSN1T on the nutritionalA status of hospitalized patients have shown that a
significant protein-calorie malnutrition commonly oc-curs both in general medical and surgical services, onlya few reports12-"7 have focused their attention on thenutritional state of cancer patients. Moreover, the pri-mary goal of some of these studies was just to analyzethe correlation of some nutritional indices with post-operative infections or with response to treatment andfinal outcome and not to evaluate the influence of thetumor on the nutritional state of patients.To analyze the impact of cancer (type, site of origin,
stage, and treatment by chemotherapy or radiation) onthe nutritional status of patients, a prospective studywas undertaken from January 1979 to May 1980 at theIstituto Nazionale Tumori of Milan.
Submitted for publication October 22, 1981.
From the Istituto Nazionale per lo Studio e la Cura deiTumori, Milano, Italy
Plan of the Study
The main purposes of this study were to 1) determinethe nutritional status of patients with cancer of varioustypes and site of origin in comparison with a controlgroup (patients without cancer); 2) evaluate the influ-ence of the stage comparing the nutritional status ofpatients with radically resectable solid tumors versusa nonresectable previously untreated group; 3) analyzethe impact of radiotherapy or chemotherapy in patientsboth with limited or advanced disease. The general planof the study is outlined in Figure 1.The control group included 34 surgical patients (13
males and 21 females), mean age 49 years (±13.5),affected by minor benign, inflammatory, or dysplasticdiseases not involving the digestive tract. Patients whowere compared with this group had either a probablesystemic disease (16 lymphomas staged as follows: 10Stage I-IIA and 6 Stage IIB, III-IV; 6 microcytomas,8 disseminated cancers from a primary unknown) ora limited local or regional disease that was staged patho-logically at surgery. These patients with limited solidneoplasia were divided into three groups: GE (cancerof the esophagus, 6 patients; cancer of the stomach, 17patients), non-GE (cancer of the colon-rectum, 10 pa-tients; head-neck, 15 patients; testis, 11 patients; lung,1 1 patients), and patients with breast (15, T1-T2-T3ANI-2 MO) or cervix (16, Stage I-IIA) carcinoma.These patients were subsequently compared with agroup of patients with the same types of tumors (GE-12 esophagus, 14 stomach; non-GE-7 colon-rectum,2 head-neck, 3 testis, 26 lung; and 8 breast and 3cervix), that proved to be unresectable clinically or atsurgery or that showed distant metastases at clinicalpresentation. In this regard it should be pointed out thata patient was considered unresectable also when after
0003-4932/82/0800/0170 $01.30 C J. B. Lippincott Company
170

CANCER AND NUTRITIONAL STATUS
MISCELLANEOUS GROUP (MICROCYTOMA, LYMPHOMA,
t PRIMARY UNKNOWN)
, |IMPACT OF TYPE-SITE
UNRESECTABLE (GE, NON-GE
ADVANCED TREATED (GE, NC
, BREAST-CERVIX)(preop. therapy)
I-NECK TREATEDA
TESTIS(adjuvant therapy) I
IMPACT OF RT OR CT| --TEI S| ' ~~~~~~~~TESTISTREATED
)N-GE, BREAST-CERVIX)
LYMPHOMA UNTREATED-4-o-uLYMPHOMA TREATED
FIG. 1. Plan of the study.
a surgical excision there was microscopic confirmationof residual tumor in the body.
Finally, the impact of chemotherapy or radiotherapywas analyzed in the group of patients with advanceddisease (GE-2 esophagus, 3 stomach; non-GE 10colon-rectum, 7 head-neck, 8 testis, 3 lung; and 14breast, 3 cervix), the group with nonsolid tumors (lym-phomas staged as Stage I-II, 3 cases, and Stage IIB-IV, 11 cases), and the group with limited disease sub-mitted to adjuvant or preoperative treatment. Since theevaluation was generally performed after more than 1month after the patients terminated their course of ther-apy, it does not analyze the acute toxicity of chemicalor radiation therapy but the chronic long-standing nu-tritional effects of these treatments. None of the pa-tients analyzed was on enteral or parenteral nutritionalsupport when the nutritional status was assessed.
Radiotherapy or chemotherapy were performed ac-cording to the conventional schedules or study protocols.Usually, dose-limiting factors included only bone mar-row toxicity or presence of severe sepsis independentlyof the nutritional status. The clinical characteristics anddistribution of the population of the patients enteredin the study is shown in Table 1.
In an attempt to better characterize the malnutritionof GE resectable patients, a comparison was also madewith a group of seven patients with a non-neoplasticdisease of the digestive tract (GE control). The overallanalysis was therefore performed on 321 patients (280with cancer and 41 controls).
Methods
The following measurements and laboratory exami-nations were performed on each patient: body height
ControlGE controlMicrocytomaLymphomaPrimary unknown
Group GE (stomach,esophagus)
ResectableUnresectableAdvanced treated*
Group non-GE (colon-rectum, head-neck, testis, lung)
Resel&ableUnresectableAdvanced treatedt
Group breast-cervixResectableUnresectableAdvanced treatedt
Lymphoma(chemotherapy-radiotherapy)§
Head-neck(preoperativetreatment)"
Testis (adjuvanttreatment)¶
No. ofPatients
3476168
5423265
113473828
5729i117
Mean age ± SD(years)
49.30 ± 13.5742.33 ± 13.4449.00 ± 9.6943.60 ± 13.3057.87 ± 14.08
61.09 ± 10.8657.31 ± 8.2465.40 ± 7.50
51.55 ± 13.2857.39 ± 11.9647.71 ± 14.67
Sex
13 M5 M5 M
12 M5 M
21 F2 FI F4 Fi F
14 M 9 F17 M 9 F4M I F
37M lOF35 M 3 F21 M 7F
49.32 ± 12.2053.64 ± 9.8345.93 ± 9.84
29 F11 F17 F
14 42.46 ± 17.78 8 M 6 F
6 54.17 ± 7.76
6 24.17 ± 3.87
S M
6 M
I F
* Three patients received chemotherapy and two radiotherapy.t Sixteen patients received chemotherapy, seven radiotherapy, and five both.
t Six patients received chemotherapy, four radiotherapy and seven both.
§ Five patients received chemotherapy, six radiotherapy and three both.
Ii Two patients received chemotherapy, three radiotherapy and one both.
1T Six patients received chemotherapy.
Vol. 196 * No. 2
C O N T R O L
171
RESECTABLE (GE, NON-GE, BREAST-CERVIX)
TABLE 1. Clinical Characteristics of Patients EnteredInto the Study
IMPACT OF ST _1

Ann. Surg. * August 1982BOZZETTI AND OTHERS
and weight, triceps skinfold, mid-upper arm circumfer-ence, 3-day urinary creatinine, serum protein, serumalbumin and serum cholinesterase, total iron bindingcapacity, peripheral lymphocyte count, skin test profileconsisting of purified protein derivative (PPD), strep-tokinase-streptodornase, and Candida albicans, serumC3 and C4 component of complement (C3C, C40). Bodyheight was measured against a vertical measuring rodwith a headpiece. Body weight was determined on alever balance scale and the percentage of weight lossfrom the usual weight was evaluated. Skinfold mea-surements were obtained with a Lange caliper. Tricepsskinfolds were measured by identifying the midpointbetween the olecranon and the acromion processes onthe nondominant arm and measuring the skin that waspulled gently away from the underlying triceps muscle.The average of three readings was recorded. To deter-mine the mid-upper arm circumference, the circumfer-ence of the arm was taken at the previously determinedmidpoint using a nonstretchable soft cloth tape. Themid-upper arm muscle circumference was obtainedfrom the mid-upper arm circumference as follows: arm-muscle circumference = arm circumference - 3.14X triceps skinfold. No attempt was made to comparethe anthropometric parameters with the standard de-veloped by Jelliffe'8 and based on international mea-surements. In fact, recent studies'9'20 have shown thatJelliffe's standards are intended for use in nonindus-trialized societies; the reported values would be high formen's triceps skinfold thickness, women's arm circum-ference and women's arm muscle circumference, andsignificantly low for women's triceps skinfold thickness,men's arm circumference and men's arm muscle cir-cumference. However, to present more completely theauthors' population patients, Table 2 reports height/weight index, weights and anthropometric parametersexpressed as percentile of United States data collectedduring the Health and Nutrition survey of 1971-19421,221974.2l2Serum total protein, albumin, total iron binding ca-
pacity and cholinesterase were determined by standardcolorimetric and electrophoretic methods. Urinary cre-atinine was determined by the picric acid technique.The C3-C4 components of complement were analyzedby the single radial immune diffusion in agar method(H-Partigen, Beheringwerke). The absolute lymphocytecounts were obtained from total white blood cell countsand the percentage of lymphocytes in the differentialcounts. All patients were skin tested for delayed hy-persensitivity response by intradermal injection of thefollowing recall antigens: one-tenth ml each of strep-tokinase-streptodornase (4U-1U) (Varidase), purifiedprotein derivative (10 U) (PPD), and C. albicans in a1:10,000 solution. The antigens were injected intrader-mally on the volar surface of the forearm, and the re-
sponse was recorded after 24 and 48 hours. Readingswere recorded by the same observer in millimeters oferythema and induration. The response was graded aspositive if at least erythema or induration > 5 mm forat least one of the three recall antigens was recorded.
Patients were considered not eligible for the study ifone nutritional parameter was omitted or proved to beunreliable. There was no apparent difference betweenpatients selected or rejected because of incomplete pa-rameters of evaluation. Patients with edema, malignanteffusion, severe dehydration, renal or hepatic failure,or evident endocrine disorders were not included in theprotocol to avoid bias in the evaluation of the anthro-pometric parameters and the weight, and of those bio-chemical indices that are expressed in term of concen-tration. No other exclusion criterion was adopted.The statistical evaluation of the difference in the al-
terations of the nutritional indices was performed byStudent's t-test, except for skin tests, which were an-alyzed by the chi square method. When the analysiswas performed with the aim of detecting a differencein the frequency of some parameters, Fisher's exact testor the chi square test with Yates' correction dependingon total sample and the smallest expected numbers wasadopted. Differences were accepted as significant whenthe p value was less than 0.05. However, when multiplegroups of patients were compared, to guard against therisk of multiple inference, each test was performed atmore stringent level, a* = a/n, a being the overall levelof significance considered and n the number of per-formed tests.
Results
Mean values of the nutritional parameters are re-ported in Tables 3 to 8. Table 3 shows that patientswith radically resectable cancer of the colon-rectum,head-neck, oat cell carcinoma, lymphoma, and un-known primary had no significant alteration of the nu-tritional status. In contrast, patients with GE cancerhad a significant depletion of five parameters: bodyweight, triceps skinfold, total protein, serum albumin,cholinesterase.
Table 4 shows the impact of stage of disease. Thestage did not influence the general state of patients withbreast or cervical carcinoma, slightly influenced that ofpatients with GE cancer (who are already severelymalnourished) and also showed a decrease in the cre-atinine-height index, and mainly affected patients withnon-GE cancer. These exhibited a consistent drop inthe creatinine-height index, serum albumin, total ironbinding capacity, and cholinesterase, but they had anincrease in C4C. However, if the unresectable patientsare compared with the controls, a significant malnutri-tion is apparent in GE and non-GE groups. In fact,
172
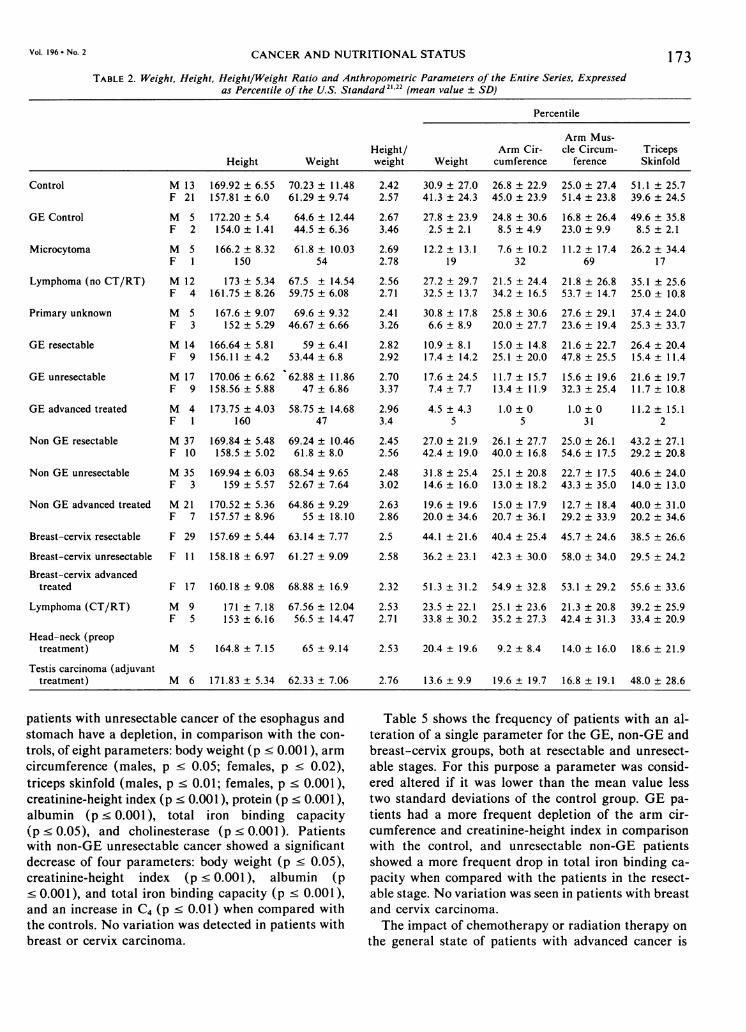
CANCER AND NUTRITIONAL STATUS 173TABLE 2. Weight, Height, Height/Weight Ratio and Anthropometric Parameters of the Entire Series, Expressed
as Percentile of the U.S. Standard 21'22 (mean value ± SD)
Percentile
Arm Mus-Height/ Arm Cir- cle Circum- Triceps
Height Weight weight Weight cumference ference Skinfold
M 13 169.92 ± 6.55 70.23 ± 11.48F 21 157.81 ± 6.0 61.29 ± 9.74
2.42 30.9 ± 27.0 26.8 ± 22.9 25.0 ± 27.4 51.1 ± 25.72.57 41.3 ± 24.3 45.0 ± 23.9 51.4 ± 23.8 39.6 ± 24.5
GE Control
Microcytoma
Lymphoma (no CT/RT)
Primary unknown
M 5F 2
M 5F 1
172.20 ± 5.4 64.6 ± 12.44154.0 ± 1.41 44.5 ± 6.36
166.2 ± 8.32150
61.8 ± 10.0354
M 12 173 ± 5.34 67.5 ± 14.54F 4 161.75 ± 8.26 59.75 ± 6.08
M 5 167.6 ± 9.07 69.6 ± 9.32F 3 152 ± 5.29 46.67 ± 6.66
2.673.46
2.692.78
27.8 ± 23.92.5 ± 2.1
12.2 ± 13.119
24.8 ± 30.68.5 ± 4.9
7.6 ± 10.232
16.8 ± 26.423.0 ± 9.9
11.2 ± 17.469
49.6 ± 35.88.5 ± 2.1
26.2 ± 34.417
2.56 27.2 ± 29.7 21.5 ± 24.4 21.8 ± 26.8 35.1 ± 25.62.71 32.5 ± 13.7 34.2 ± 16.5 53.7 ± 14.7 25.0 ± 10.8
2.41 30.8 ± 17.8 25.8 ± 30.6 27.6 ± 29.1 37.4 ± 24.03.26 6.6 ± 8.9 20.0 ± 27.7 23.6 ± 19.4 25.3 ± 33.7
GE resectable
GE unresectable
166.64 ± 5.81156.11 ± 4.2
170.06 ± 6.62158.56 ± 5.88
59 ± 6.4153.44 ± 6.8
62.88 ± 11.8647 ± 6.86
GE advanced treated M 4 173.75 ± 4.03 58.75 ± 14.68 2.96 4.5 ± 4.3 1.0 ± 0 1.0 ± 0 11.2 ± 15.1F 1 160 47 3.4 5 5 31 2
Non GE resectable M 37 169.84 ± 5.48 69.24 ± 10.46F 10 158.5 ± 5.02 61.8 ± 8.0
2.45 27.0 ± 21.9 26.1 ± 27.7 25.0 ± 26.1 43.2 ± 27.12.56 42.4 ± 19.0 40.0 ± 16.8 54.6 ± 17.5 29.2 ± 20.8
Non GE unresectable M 35 169.94 ± 6.03 68.54 ± 9.65 2.48 31.8 ± 25.4 25.1 ± 20.8 22.7 ± 17.5 40.6 ± 24.0F 3 159 ± 5.57 52.67 ± 7.64 3.02 14.6 ± 16.0 13.0 ± 18.2 43.3 ± 35.0 14.0 ± 13.0
Non GE advanced treated M 21 170.52 ± 5.36 64.86 ± 9.29F 7 157.57 ± 8.96 55 ± 18.10
2.63 19.6 ± 19.6 15.0 ± 17.9 12.7 ± 18.4 40.0 ± 31.02.86 20.0 ± 34.6 20.7 ± 36.1 29.2 ± 33.9 20.2 ± 34.6
Breast-cervix resectable
Breast-cervix unresectable
Breast-cervix advancedtreated
Lymphoma (CT/RT)
Head-neck (preoptreatment)
Testis carcinoma (adjuvanttreatment)
F 29 157.69 ± 5.44 63.14 ± 7.77 2.5 44.1 ± 21.6 40.4 ± 25.4 45.7 ± 24.6 38.5 ± 26.6
F 11 158.18 ± 6.97 61.27 ± 9.09 2.58 36.2 ± 23.1 42.3 ± 30.0 58.0 ± 34.0 29.5 ± 24.2
F 17 160.18 ± 9.08 68.88 ± 16.9 2.32 51.3 ± 31.2 54.9 ± 32.8 53.1 ± 29.2 55.6 ± 33.6
M 9 171 ± 7.18 67.56 ± 12.04 2.53 23.5 ± 22.1 25.1 ± 23.6 21.3 ± 20.8 39.2 ± 25.9F 5 153
±6.16 56.5
±14.47 2.71 33.8
±30.2 35.2
±27.3 42.4
±31.3 33.4
±20.9
M 5 164.8 ± 7.15 65 ± 9.14 2.53 20.4 ± 19.6 9.2 ± 8.4 14.0 ± 16.0 18.6 ± 21.9
M 6 171.83 ± 5.34 62.33 ± 7.06 2.76 13.6 ± 9.9 19.6 ± 19.7 16.8 ± 19.1 48.0 ± 28.6
patients with unresectable cancer of the esophagus andstomach have a depletion, in comparison with the con-
trols, of eight parameters: body weight (p < 0.001), armcircumference (males, p < 0.05; females, p c 0.02),triceps skinfold (males, p < 0.01; females, p < 0.001),creatinine-height index (p < 0.001), protein (p < 0.001),albumin (p < 0.001), total iron binding capacity(p < 0.05), and cholinesterase (p < 0.001). Patientswith non-GE unresectable cancer showed a significantdecrease of four parameters: body weight (p < 0.05),creatinine-height index (p < 0.001), albumin (p< 0.001), and total iron binding capacity (p < 0.001),and an increase in C4 (p < 0.01) when compared withthe controls. No variation was detected in patients withbreast or cervix carcinoma.
Table 5 shows the frequency of patients with an al-teration of a single parameter for the GE, non-GE andbreast-cervix groups, both at resectable and unresect-able stages. For this purpose a parameter was consid-ered altered if it was lower than the mean value lesstwo standard deviations of the control group. GE pa-
tients had a more frequent depletion of the arm cir-cumference and creatinine-height index in comparisonwith the control, and unresectable non-GE patientsshowed a more frequent drop in total iron binding ca-
pacity when compared with the patients in the resect-able stage. No variation was seen in patients with breastand cervix carcinoma.
The impact of chemotherapy or radiation therapy on
the general state of patients with advanced cancer is
Vol. 196 * No. 2
Control
M 14F 9
M 17F 9
2.822.92
2.703.37
10.9 ± 8.117.4 ± 14.2
17.6 ± 24.57.4 ± 7.7
15.0 ± 14.825.1 ± 20.0
11.7 ± 15.713.4 ± 11.9
21.6 ± 22.747.8 ± 25.5
15.6 ± 19.632.3 ± 25.4
26.4 ± 20.415.4 ± 11.4
21.6 ± 19.711.7 ± 10.8

BOZZETTI AND OTHERS00
-4r .
oen-.-e.s00ooo o C_4_
+l +1 +1 +1 +1 +1 +1 +I +I +I +I +I +I +I +I%T 0Orrt0en - U 0oO r- 00 0 r
. 00 .0% I oo Cric 4O , or
t-O V- e.0
0n en oo t~- et ON )N O
"_t- - - (:w^_t
0
+l +l +l +l +l +l +l +l +l +l +l +l +l +l +l--
0otn C 00 00 14 00
- IC 4 tnoo
e
cl od 06Wo_
el 06_ t_
'D
oo
"ol-nWI Cl tnc _ _t-: v- r_ 6c t-
N
a%N0 N ooN) o~ t- C1 No I'*l * -
.0% 00
f6 Ni c ooC)N -+1 +1 +1 +1 + ++l +l +l +l o +l +loo t 4 N 00 Cq si D en a en rN
"t.) 0 6I t o0- 00
e'j 0%i 0 en )e oI *a t. oafat.) _ o. 0%*oat.)o r̂l
4ltCN OO 6/.)%Oa. Os
C- C (6XIn _ o6o en 4omN-
+1 +1 +1 +l +l +l +l +I +I +I +I +Iat en - 00d cn -<o M r- t
_ 00 -e; 0rv 09
t 00 o10
C C C-_ enr. OatoC-
'I oll- fn.Cl400 0%%oat.)~C_ .-O -o
WI W) <4 £- - ON en en ofi Z* 4£ £i 4 C4 vi vi eC-;n O O " -
+l +1 +1 +1 +1 +1 +1 +I +I +I +1 +I +1+1 +I +Ie It 0000 - a)oNr- a- 00 as0t
C 0 00 0-elNf car)0 %OtoCI 4 Cl- __ t _.-
C-
.4-* * * a l00 N-o too
N 1N 1t m cq C; O~ O,* .-ooo t} t-_00 ri Ci Ci c-Cl i en 00000 at.) " i Cl4
+l +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 a; +1 +1a. 00 It ICCo -tI' t 1C4 m en £ No b1- 0a 00 CN - at.)0C_ WI.CO .-C Cl4 -\0 0 --I_NN -NN- Cl%O -
C4 -
ena.0
cl0%N -Cl Cl NCleq 0%N
+ +l +l +l +l +l +l +I+lI+I+I++I ' +I +I00 r
)00l-%O N N CF0% N 00 N-00%coola.)0N 00~00v%oOOeo*.o )..6 .
4" .o-. -: ;. ~ 6-0%00-0rlCl4Cl%O WI-N- 0%0I
ClCl-Cl Cl- OenN -C*
f< F < WF<FU)HcoU)X)
C) C
EE~~--. -' E
mu4).
~~~ .~ ~~wUg.U -U"
4)
1e
C OC04CO6_ 0.
00'0 o8 1w0-_
0 a-O,D0.0
* 4)
COC4)
000
---
Cq
+1
.K
.2
a.-
3c
k.
-
Cq
m)6,
;>%c)0.
c)00
C.0
0
..DV
P-
DQ >
z -Co
a. CO-0
C (O
0o
CZLCIL
aD 0.
r
.0
IL) 'A
CO
CJ eq
C) Clq
4)_4)v
4)4)
SCO
0.0
._
z
Ann. Surg. * August 1982
00 enN N cr C - oo
F F Nee00 o%o
* *
I-F~~~~~~~~t W) W
O.oo 1%tF
wi 4 r- i en o o o "t xo CA _
+1 +1 +1 +1+1+1+1+1+1+18 +1+100 1^ tt)2 --- at m)%O 0. N 01 as as WI tCI 0% 00 C".)CI%0_0%N Nt
N-
0~
I- C.)4I.)~~~~mtn00 -C --
O ooo00 en 00Cl 0% ON en t as * as-. - 0_ _% C In 0 maqt n r _;c.0.00-c'WI 'CC-
+1 +1 +1 +1 +1 +1 +1 +1 +1 +1 8+ +Ia'. en Cl - 00 qt en- 0en r-Nt.)mN _ o o -s }_* (}_I t
- 6 .-m _ ,omat no6o0
oo o
C_CoC_ -en
f. t- 01oooo _Cl4 -
** att.)0 -- £o %n "Ct oO£0vt _ a,o en r- r- W) r- *, * kn oo"t oO00 17 Oll ID 0 o5 n " o en WI WI °°
+l +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 sD +1 +1r- Cl e n - N o 0% 00 00 i _
0-0%%0e'.)r'.)%00 Oe^I -- _o0000 O ClN%
Cl4
'I N
%0 0%-
0 06 0%%0at. N_ 49F ** -
+l +1 +1 +1 +1 +1 +1 + +I +I +I +I +lI +I +II", e % 00 l-- t. I'l N en) 00 0% I'l
ri 000- c cl- en!tu)0o o I
N--ooCl-Cl- 0%00 -
Cl4 -
00 N-000 0%1-0N%C _0 N enIt t 00,
COO-%S>^00-% _e W
+l +l +l +l +l +l +l +l +l +l +l +l +l +l +len O ON - 00°-00 d
%
- -00 R eVIl)r- C l 00 * tCl0%(I OI£CC -ClCl 00 .0 Oat.) oC'4 C14 C,4
0W)
Cl-
lt.C000 C0 oo rCC NT"o cr u£oyoo a- 00 n p t- ON _; r. uoo t -o£o en rq "irE1-t *; mn oo t06 N C4 N qi CN C en o 0 oo in "t C _
+l +1 +1 +1 +1 +1 +1 +I +I +I +I +I +I +I +ION 00 'T % Cl - "F.t Cl"(n Cl %o0 %0 ClNe - C% 00 " lN- *a'.)**a'.)Q% CS!InsC6 _- oNi toO wi 4 C' -
e <en o
N
CA elN -- ^ O -
C-
C)~~~~~
C)v S C)*v
00
*° ~ ~ *5 C
<F- < QF<F-QFcrUQ
174
+1
.:
PI.
0
.k
F-
X:
C3
eV
JK
c
COr0.~. 0w -00
.Y 0.
co
.CO0
o -~
~0.
C)--,
* C
.0
c)
_)
0O12
OCOCO\
0._
zd
0
'A0.4-
'A0.
*4)VI. ..
cicCOC)
c
Oa
CO.
0.
CO
0
'0
-
*co
0
0
&oC
.0
C0
4-
c-4
i-

CANCER AND NUTRITIONAL STATUS
analyzed in Table 6. latrogenic alteration of some pa-rameters could be detected in GE patients (arm cir-cumference, arm muscle circumference). A drop in pe-ripheral lymphocytes was observed in non-GE andbreast-cervix patients. If these patients are comparedwith the control group, the rate of malnutrition is muchmore evident and accounts for the eventual cachexiapresent in the late stages of disease. In fact, GE patientshad a significant decrease in nine parameters: bodyweight (p < 0.001), arm circumference (males, p< 0.001), triceps skinfold (males, p < 0.02), arm musclecircumference (males, p c 0.01), creatinine-height in-dex (p < 0.01), albumin (p < 0.05), cholinesterase (p< 0.001), total iron binding capacity (p < 0.02), andskin test reactivity (p < 0.01). Non-GE patients hada decrease in four parameters: body weight (p < 0.001),total iron binding capacity (p < 0.05), cholinesterase(p < 0.01) and total lymphocytes (p < 0.001), and asignificant increase in C4C (p< 0.001). Patients withbreast or cervix carcinoma had a drop only in peripherallymphocytes (p < 0.001). Some nutritional parameterswere also more frequently altered in patients treatedfor advanced cancer in comparison with the unresect-able previously untreated patients, i.e., the skin testreactivity in the GE group and triceps skinfold in thenon-GE group (Table 5).The effects of radiotherapy and chemotherapy were
also investigated in patients with lymphoma and in pa-tients receiving preoperative or postoperative adjuvanttherapy (Table 7). Only patients with testis carcinomashowed some depletion of body weight and the creati-nine-height index after adjuvant treatment. However,if these patients are compared with the controls, a nu-tritional depletion is evident in all groups: patients withlymphoma exhibited a drop in the creatinine-height in-dex (p < 0.05), albumin (p < 0.05) and skin tests (p< 0.01). Male patients treated for head-neck cancerhad a decrease in triceps skinfold (p < 0.01), and pa-tients with testis carcinoma had a lower body weight(p < 0.01) and a lower creatinine-height index (p< 0.05).
Finally, Table 8 shows the nutritional parameters ofseven patients with nonneoplastic disease involving thedigestive tract. When the resectable GE group was com-pared with these patients, no difference was detectedexcept for a significant hypoalbuminemia in cancer pa-tients.
Discussion
The aim of this study was to investigate the nutri-tional state of patients with cancer. The parameters thatwere adopted are commonly accepted as valid measuresof the nutritional status for clinical epidemiologic sur-veys also by the authors23 who deny their value in in-
+lC)
0
0C)
C'
C)
S:
:0
C)
C)C)
0
*_0-0
2C:0
I._
0
C)
C)
C)
Co
CZ) C
0
C 0.
>
C)Dr
Co 0Q
C) CXCQ 0.t
-
H
D0.
C)_ 0o
CoCo
0.
Co
z
0000 0oooo x oo or-
4+4+4) -++ 4+
4
40) c= cc
i~
Cor_ .0=_ . ._
4+4+ 4+4-+4+ 44+4+4+0 000 1PI 0.-0 0 R\04+
rO rO O ,H,H,HO) .E,- t q f
Lo -a o o o oo O 0 0
t ttIDITc'I ttIt I
. . . . -.
0000000000000
4+* 4+4+* 4+4+4+4+ 4+4+
r- (Z alralONm r- aN C) db ff
- o O r -O 0 °
C E
_ _,
C) C), CA. < U U
,£ CCtN _
0 0 C) _0£NO£N ^0
Vol. 196 * No. 2 175
o_ _
c 00
04 00 ._
6 -0. _
O 0.
6 00Vl0 Co
* C)
C)_ Co
0 Co
Co;
0.CoQ
_CoE- C)
~C) CL
OC)
._ 0

BOZZETTI AND OTHERS
00 %O %0
+1 +1 +100 0a _a- -
.4 .1Un cn C
+1 +1 +100 st en%0 0 a-es 0% 00
es -
4+e4 0%4 00 If ON
000C- e~: CON.0000N *' en -
+l +1 +1 +1 +1 +1 +1 +l +1
(Di Oq q 0m 0N-
00 asNN ^ ^ 00 t 00
- 006 eaai00
00 en)es4 tr-e -..00
e0 OOF N _o-llN I", ONin _- * W_
CI- 'fo - o
0
en i000CA-
* ^cf} N t--NN 00 ONv el
t0N 0%- 0- en aJC 0tnt ntne
+l +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 0o +1 +1w r-
mo It o1otn 1. M %
o". .
soM WI r- 'I 2 6C ~C! 14 l~C
N-
r-:te;6 4 4 6oo somm oo so
- - - - - - f f*)o
00 I'--000ooo
£NN̂t NN O F es-s
00(0 %0'f 00%
+ +1 +1 +1 +1 +1 +1 +I+lI+I +I+I0 +I +I-e_ M e - N %0 0C% 00 - _00 in a,
00 e o en en _o 0o--e4 -5 00 000ON 5%
I I_ ~ C_CooiC ICC-4
4- e N-e^, _
e%0 N__ el - r^-0e5%0 ''N
+1 +1 +1 +1 +1 +1 +1 +1 +1 +1 0 + +l' l
en a-, r-s 00
C-4en6 0~ C 0% es es"' C
C- Zo~6eic n
00 N 00%0 0%_00N 'oor S fen* t%wi R00") 'I£ £ ") c- 'f C4 enOoWI^+l +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1en asa0% 0 - d 00 -00 t %0 ,0 - 00 Rt c
. . .O . . . .O 00N0e" - 00 "0% C
_NN000%0r ~_ Oo 0
-e5e5 (Nel 0-O 0"
' E-
f~~~0 E . '0 i
I. ). 0 00 '
H<F < QH<HUHc/2QQ
0 +1
0. +
VI :
o. a)
0.e
c)
C) C
c0 _
U) 0
..
-Ua)
a)
0
0sS.a)
-)
*0
. 0
E.C)
00
00
c)
.00
0
0-
E00.E
0.
.0H
0.0
a.)
H.40.
0...4z
I..
a.)
c
cx
u).)
c
a
0
C.)
H-'-,-- 0.
U -.
H
H0.
O _~
z
H0.
z
U-0.~
CO0.
E
co0
:-.z
Ann. Surg. * August 1982
+l +l1+l +l +1+l +1+l +l +l +1+l +l r-2 +l +lq O- so en 4n - WI uotz-so}<t 4
.1 O1 1 +1r- r-
_ON,
enI'l
en r-_ N_D _6 io ci -6 C
%0e4~C'en
at %o 0%0_̂ ei oo
0% £J- ~ N t 2O Io O °
+l +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +1 +l +1- _0n0 00oot O -000C0Oe r ea-Ci 06 06 In 0Oo 4N0o %O r)o F o*t rN _o _coW NNoo
eI C - -o t- - t('-
ene
N Os en U 00 £.00- e*n*N WI o6 "P 'OO oo U) _
en
+1"
+1 +1 +1 +1 +1 +1 +l++ ,, +l +l+1 f00 r x -C4 N--t 01- 1r- 00C- cn Ci IR0 0 - 1-
> o
eaN eN 0 -sr_'6'0 e-0
o t as t N o * * tt
F
_o 08 - _ 00'4 %
+1 +1 +1 +1 ++l +l +l+1 l ++ei +l0 00 O0 0o0- % 0°%)1-£ O
*-le ( o-N!t elNen -Weq _ N _ t-tI _
C-r
+1 +1 +1 +1
+1 +1 +1 +1
r- es
~ 11
C)1 -
E
02 .- .
a
*
o00000 000%2C.,m_; lt0
oo : tn-e CboC;0%s-+1 +1 +1 +1 +1+1 8 +1 +1oo es 0oen rs en 'o
r1i 09 a, 0
-
_ t_- r- o0o No r oo _
00 1-, ci 0_ r-
on-;';-2 .-4 -Ne 0
en es4
176
+1a)
0
0a)
a)S.)0a)
'0a)C)
0.0
a)
0
I-a)C)
0r--)
0S.)
0
0
0
L.
a)
0
0S..a)
0
a)
*0
0
0,0S..a)
0*00
0
C)00.
-6w'-5CO
H
_>e
z^-
CL
'> 0
- _
0
8zC.)
'0
CC
I CO-
'0 _o
C)0CZ
CO
'0 ) C£
C) U
-o
<-
._C0._C.
a)e'
O.0
Vi0.*
co:CO
csC.
00
0'U
1._
I)
co0.co
00c._
0.0c0
4-
1-

Vol. 196 - No. 2 CANCER AND NUTRITIONAL STATUS
dividual patients and in dynamic conditions and arecurrently used in clinical practice. The criteria the au-thors used to collect patients with different cancers inthis group (i.e., stomach and esophagus cancer in theGE group, colon-rectum, head-neck, lung, testis car-cinoma in the non-GE group, and breast and cervixcarcinoma in one group) and to distinguish three dif-ferent stages (resectable, unresectable and advancedtreated) deserve some consideration. Patients with dif-ferent cancers were collected in one group only aftera statistical analysis was done within the single groupsand failed to demonstrate any marked difference amongthem. The distinction into stages is largely conventionaland criticizable, because it would have been more cor-rect to avoid some overlapping between resectable andunresectable patients and to include in the radicallyresectable group only those patients with limited cancermanageable with surgery and actually cured from theirdisease. This would have required a long-term follow-up and proved to be impractical for this study.
Finally, the population of advanced cancer patients,with or without previous treatment, is favorably se-lected. In fact, the majority of these patients proved tobe unresectable during surgical exploration or had dis-tant metastases discovered during hospitalization andgenerally were not in terminal condition. Indeed, it isthe policy of this Institute to admit advanced cancerpatients only when some palliation can be obtained bya surgical, radiological or pharmacologic approach. Asa consequence of this unavoidable selection, these re-sults probably slightly underestimate the rate of mal-nutrition in advanced patients, with or without previoustreatment. As far as the statistical evaluation is con-cerned, it must be noted that the extensive use of thet-test for multiple parameters can diminish its power.Therefore, the credibility of a significant result is notabsolute but rather must be considered as a trend thatwarrants further confirmation. Despite all these limi-tations this study clearly shows that malnutrition canaffect patients with cancer, even if its rate and fre-quency range considerably depending substantially onthe type and site of the tumor, stage of disease, and,to a lesser extent, on the treatment performed.
If solid tumors are considered in an initial stage whenthe disease is radically manageable with surgery, it isobserved that malnutrition is present only in GE pa-tients. In these patients, inadequate intake of nutrientscaused by the mechanical impairment of digestion, cou-pled with an inappropriately high energy expenditure,24despite starvation and weight loss, are the prime de-terminants of malnutrition. The type of malnutritionis peculiar, since fat stores and visceral protein com-partment are mainly depleted. The fat loss that wasobserved is in keeping with data from other authors who
177TABLE 8. Nutritional Status of Patients with Gastrointestinal
Benign Disease (Seven Patients)
Nutritional Parameter mean value ± SD
Weight loss (%) -6.18 ± 4.96Arm circumference (cm) { M 28.60 ± 4.20
F 25.00 ± 1.40Triceps skinfold (mm) M 11.60 ± 8.60
F 13.50 ± 2.10Arm muscle circumference (cm) M 24.50 ± 3.00
F 20.50 ± 0.70Creatinine/height index 116.14 ± 34.94Total protein (g/dl) 6.94 ± 0.48Albumin (g/dl) 3.74 ± 0.19Total iron binding capacity (Ag/dl) 333.85 ± 40.38Cholinesterase (mU/ml) 2589.42 ± 370.05Total lymphocytes (/mm3) 1990.14 ± 549.06Skin test (% of positive) 100C3C (mg/dl) 99.42 ± 17.06C4C (mg/dl) 45.42 ± 10.32
have shown that the fat content of muscles of cancerpatients is significantly lower than that of the controls,25and the oxidation of free fatty acids is less suppressedand with higher blood glucose concentration in patientswith advanced cancer than in normal volunteers.26'27 Asthe disease progresses, further progress of malnutritioncan be observed in GE patients who also present a sig-nificant depletion of muscle proteins, a finding con-firmed by recent quantitative measurements of bodycomposition.28 Characteristically, in the unresectablenon-GE patients, malnutrition first appears as a deple-tion of proteins in both visceral and somatic compart-ments. The extent of malnutrition is much more evidentwhen the unresectable patients are compared with con-trols. In this way the authors can observe a depletionof body weight, lean body mass, fat mass, muscle andvisceral protein in GE patients and body weight andmuscular and visceral protein in the non-GE group.Chemical or radiation therapy did cause a drop in
arm circumference and arm muscle circumference inGE advanced patients and a significant lymphopeniaboth in non-GE and breast-cervix patients. With theexception of the increase in the creatinine-height indexin non-GE patients after chemotherapy or radiotherapy,there was no evidence that these treatments improvedthe nutritional state. Again, these differences are mag-nified if the advanced patients are compared with thecontrol group.When chemical or radiation therapy was adminis-
tered as adjuvant postoperative (testis carcinoma) orpreoperative (head-neck- carcinoma) treatment or inlymphoma, different patterns were observed. No effectwas detected in head-neck cancer patients treated bypreoperative radiotherapy and chemotherapy or in pa-tients with lymphoma, but adjuvant therapy for testiscarcinoma consisting of adriamycin (40 mg/M2 day 1 )

Ann. Surg. * August 1982
plus Endoxan (200 mg/M2 days 1, 2, 3, and 4 every 4weeks) or vinblastine (6 mg/M2 days 1 and 2) plusbleomycin (15 mg/M2 days 2, 3, 4, 5 and 6 every 35days) was able to cause some decrease in body weightand the creatinine-height index. The interpretation ofthese conflicting results is not easy. A probable expla-nation is that the nutritional effects of radiotherapy andchemotherapy range considerably depending on thedose and fractions, the field of irradiation or the toxicityof the single chemotherapeutic agents. It is also possiblethat in responsive and advanced tumors the negativeeffects of the therapy on the nutritional state are fa-vorably outweighed by the decrease in the tumor bur-den, while in patients probably free of disease the un-balanced effects of precautional chemotherapy can onlyadversely affect the nutritional status. The patients withbreast-cervix cancer never showed malnutrition exceptfor lymphopenia in the treated group. An increased fre-quency of obesity29 probably related to an imbalanceof adrenal estrogens could explain the good mainte-nance of some anthropometric parameters in operablebreast cancer patients, while hormonal manipulation orradio-induced castration could account for the sameeffects in subjects with advanced disease.As far as the frequency of altered parameters is con-
cerned, we can see that in resectable patients there wasin descending order a depletion of body weight (15.3%),cutaneous delayed hypersensitivity (11.2%), and serumalbumin (6.1%). In unresectable patients there wasweight loss (in 25.3%), skin test anergy (in 17.3%), andhypoalbuminemia (in 12.1%), and in advanced treatedpatients there was skin test anergy (24%) and a decreasein arm muscle circumference (18%) and body weight( 16%). The more frequently involved indices were there-fore weight loss, skin test reactivity, and serum albumin.
Characteristically, skin test anergy was maximal inthe GE resectable group (30.5%), in GE advancedtreated (60%), and in patients treated for lymphoma(42.9%). Moreover, it is the leading parameter thatproved to be altered in the advanced treated group (in24% of the patients). Although this study provides somedata on the rate and distribution of malnutrition withinsome groups of patients with cancer, it fails to indicatethe pathogenesis of this malnutrition: that is, how muchit depends on limited supply of protein-calorie sub-strates or on altered host metabolism. In this regard thecomparison between resectable GE cancer patients andGE controls deserves further discussion. Since the nu-tritional parameters of these two groups were fullyequivalent, one could conclude that skin test reactivityis related more to the nutritional status than to thetumor per se, while hypoalbuminemia would representa characteristic feature of neoplastic dysmetabolism.The first statement is in keeping with the results ob-tained by Daly et al. 30 and Bozzetti et al.,3' who were
negative skin tests to positive during 2 to 4 weeks ofintravenous hyperalimentation.Hypoalbuminemia is probably caused by a decrease
in serum albumin synthesis, while its rate of degrada-tion, the transcapillary escape rate, and the extravas-cular/intravascular ratio are increased.32'33 In fact,should the cause of hypoalbuminemia depend on limiteduptake of substrates, one would expect a more relevantalteration of proteins with a shorter half-life, i.e., totaliron binding capacity (8 days) and cholinesterase (1day). Furthermore, there is some evidence of a factorin serum of cancer patients that can cause a decreasein the rate of synthesis of serum albumin,34 a findingthat might explain reports of failure to restore to normalserum albumin in cancer patients treated by forced en-
teral feeding.35'36The value of serum complement as a marker of mal-
nutrition is quite limited. Although low levels of C3Chave been reported in undernourished patients37'38 andthe synthesis rate is relatively rapid (on the order of 1-2% per hour), its turnover depends on the activity ofthe complement system as well as hepatic synthesis. Incancer patients there are two opposite trends on com-
plement alteration: one induced by malnutrition and theother by the presence of the tumor mass, which wouldserve as an antigenic stimulus for continued antibodyproduction. As a consequence of this, elevated levels ofC4, which is synthesized mainly by macrophages, were
found in patients with unresectable non-GE cancer (incomparison with resectable patients and to controls)and in advanced treated non-GE patients (in compar-
ison with the controls), similarly to the data publishedby other authors.'3'39-41 On the contrary, the authorsfound C3 levels were always normal also in seriouslyundernourished cancer patients.
Since this investigation has indicated that malnutri-tion frequently affects the patients with cancer, it shouldbe asked which are the practical implications of thisdemonstration. There is increasing evidence that mal-nutrition has an adverse impact on morbidity and mor-
tality: nutritional depletion may determine a higher sus-
ceptibility to infections in surgical cancer patients,'3'39depletion of muscular and visceral protein stores andcutaneous anergy are related to a higher mortality, bothin medical and surgical patients,'4 and anergic patientsare less responsive to chemotherapy.30 Recently DeWyset al.42 using data from 3047 patients enrolled in 12chemotherapy protocols of the Eastern CooperativeOncology Group, definitely showed that median survivalwas significantly shorter in nine protocols for the pa-
tients with weight loss compared with the patients withno weight loss, and chemotherapy response rates were
lower in patients with weight loss. Decreasing weightand frequency of weight loss were generally correlatedwith decreasing performance status and with increasing
able to convert a variable percentage of patients with
178 BOZZETTI AND OTHERS
number of anatomic sites involved with metastases, but

Vol. 196 * No. 2 CANCER AND NUTRITIONAL STATUS 179
within pertormance status categories and categories ofanatomic involvement, weight loss was associated withdecreased median survival. Finally, 10 to 23% of ter-minal cancer patients ultimately die exclusively becauseof cachexia.44'45 Although intravenous hyperalimenta-tion has proved efficient in restoring to normal severalnutritional parameters previously depleted,3' the dem-onstration of the clinical benefit on the final outcomeof patients receiving nutritional support is still lackingand is currently being investigated in clinical trials.46
AcknowledgmentThe authors thank Ms. B. Johnston for editing and preparing the
manuscript.
References1. Bistrian BR, Blackburn GL, Hallowell E, et al. Protein status of
general surgical patients. JAMA 1974; 230:858-868.2. Bistrian BR, Blackburn GL, Vitale J, et al. Prevalence of mal-
nutrition in general medical patients. JAMA 1976; 235:1567-1570.
3. Butterworth CE, Blackburn GL. Hospital malnutrition. NutrToday 1975; 10:8-18.
4. Hill GL, Blackett RL, Pickford I, et al. Malnutrition in surgicalpatients. An unrecognised problem. Lancet 1977; 1:689-692.
5. Kassiadou A, Domingos JG, Vianna R, et al. Malnutrition ingeneral medical and surgical patients: an anthropometric sur-vey in Niteroi, Brazil, JPEN 1979; 3:470.
6. Letsou AP, Connaughton MC, O'Donnell TP. Nutrition surveyof a university hospital population. JPEN 1977; 1:40.
7. Mullen JL, Gertner MH, Buzby GP, et al. Implications of mal-nutrition in the surgical patient. Arch Surg 1979; 114:121-125.
8. Seltzer MH, Bastidas JA, Cooper DM, et al. Instant nutritionalassessment. JPEN 1979; 3:157-159.
9. Thomas L, Malquarti V, Kirkorian G, et al. Etat nutritional desmalades admis en r6animation. Relation avec la mortalit6.Nouv Press MMd 1979; 8:409-414.
10. Willcutts HD. Nutritional assessment of 1000 surgical patientsin an affluent suburban community hospital. JPEN 1977;1:25B.
11. Young GA, Hill GL. Assessment of protein-caloric malnutritionin surgical patients from plasma proteins and anthropometricmeasurements. Am J Clin Nutr 1978; 31:429-435.
12. Daly JM, Dudrick SJ, Copeland EM. Evaluation of nutritionalindices as prognostic indicators in the cancer patient. Cancer1979; 43:925-931.
13. Dionigi P, Dionigi R, Nazari S, et al. Nutritional and immuno-logical evaluation in cancer patients. Relationship to surgicalinfections. JPEN 1980; 4:351-356.
14. Harvey KB, Bothe A, Blackburn GL. Nutritional assessment andpatient outcome during oncological therapy. Cancer 1979;43:2065-2069.
15. Hickman DM, Miller RA, Rombeau JL, et al. Serum albuminand body weight as predictors of postoperative course in co-lorectal cancer. JPEN 1980; 4:314-316.
16. Nixon DW, Heymsfield SB, Cohen AE, et al. Protein-calorieundernutrition in hospitalized cancer patients. Am J Med 1980;68:683-690.
17. Rombeau JL, Goldman SL, Apelgren KN, et al. Protein-caloriemalnutrition in patients with colorectal cancer. Dis Colon Rec-tum 1978; 21:587-589.
18. Jelliffe DB. The assessment of nutritional status of the commun-ity; with special reference to field surveys in developing regionsof the world. World Health Organization Monogr 53, 1966.
19. Burgert SL, Anderson CF. An evaluation of upper arm mea-surements used in nutritional assessment. Am J Clin Nutr1979; 32:2136-2142.
20. Gray GE, Kulhanek-Gray L. Validity of anthropometric norms
used in the assessment of hospitalized patients. JPEN 1979;3:366-371.
21. Bishop BW, Bowen PE, Ritchey FJ. Norms for nutritional as-sessment of american adults by upper arm anthropometry. AmJ Clin Nutr 1981; 34:2530-2539.
22. Vital and Health Statistics. Weight and height of adults 18-74years of age, U.S., 1971-1974, DHEW Publication No (PHS)79-1656, Series 11, No 212, Public Health Service. Washing-ton D.C.: Government Printing Office, 1979.
23. Forse RA, Shizgal HM. The assessment of malnutrition. Surgery1980; 88:17-24.
24. Bozzetti F, Pagnoni AM, Del Vecchio M. Excessive caloric ex-penditure as a cause of malnutrition in patients with cancer.Surg Gynecol Obstet 1980; 150:229-234.
25. Costa G. Cachexia, the metabolic component of neoplastic dis-eases. Cancer Res 1977; 37:2327-2335.
26. Edmonson JH. Fatty acid mobilization and glucose metabolismin patients with cancer. Cancer 1966; 19:277-280.
27. Waterhouse C, Kempermann JH. Carbohydrate metabolism insubjects with cancer. Cancer Res 1971; 31:1273-1278.
28. Cohn SH, Gartenhaus W, Sawitsky A, et al. Compartmental bodycomposition of cancer patients by measurement of total bodynitrogen. potassium, and water. Metabolism 1981; 30:222-229.
29. DeWaard F, Baandens-Van Halewijin EA, Huizinga J. The bi-modal age distribution of patients with mammary carcinoma.Evidence for existence of 2 types of human breast cancer. Can-cer 1964; 17:141-151.
30. Daly JM, Dudrick SJ, Copeland EM. Intravenous hyperalimen-tation. Effect on delayed cutaneous hypersensitivity in cancerpatients. Ann Surg 1980; 192:587-592.
31. Bozzetti F, Terno G, Baticci F, et al. Effect of supportive intra-venous hyperalimentation on the nutritional status of cancerpatients. Tumori 1980; 66:241-254.
32. Trotter JM, Caine S, Raines G, et al. Albumin metabolism incancer patients with weight loss. EORTC Symposium on Nu-trition of the Cancer Patient. Brussels, January 8-9, 1981.
33. Wannemacher RW, Yatvin MB. Protein reserves and growth ofthe Walker carcinosarcoma in rats. J. Nutr 1965; 85:393-399.
34. Toporek M. Effects of whole blood or albumin fraction from tu-mor-bearing rats on liver protein synthesis. Cancer Res. 1973;33:2579-2583.
35. Pareira MD, Conrad EJ, Hick W, et al. Clinical response andchanges in nitrogen balance, body weight, plasma proteins andhemoglobin following tube feeding in cancer cachexia. Cancer1955; 8:803-808.
36. Trotter JM, McAllister EJ, Boyle P, et al. Enteral hyperalimen-tation in cancer patients with weight loss. EORTC Symposiumon Nutrition of the Cancer Patient. Brussels, January 8-9,1981.
37. Kielmann AA, Curcio LM. Complement (C3), nutrition, and in-fection. Bull WHO 1979; 57:113-121.
38. Sirisnha RS, Suskind R, Edelman R, et al. Complement and C3proactivation levels in children with protein-calorie malnutri-tion and effect of dietary treatment. Lancet 1973; 2:1016- 1020.
39. McKenzie D, Colsky J, Hetrick L. Complement reactivity of can-cer patients. Measurements by immunohemolysis and immu-noadherence. Cancer Res 1967; 27:2386-2394.
40. Verhaegen H, DeCock W, DeCree J, et al. Increase of serumcomplement levels in cancer patients with progressing tumors.Cancer 1976; 38:1608-1613.
41. Zarco RM, Flores E, Rodriguez F. Serum complement levels inhuman cancer. J Philippine Med Assoc 1964; 40:839-846.
42. DeWys WD, Begg C, Lavin PT, et al. Prognostic effect of weightloss prior to chemotherapy in cancer patients. Am J Med 1980;69:491-497.
43. Bozzetti F, Baticci F, Terno G, et al. Impact of cancer site, stageand treatment on the nutritional status of the patients. JPEN1980; 4:430.
44. Inagaki J, Rodriguez V, Bodey GB. Causes of death in cancerpatients. Cancer 1974; 53:568-573.
45. Warren S. The immediate causes of death in cancer. Am J MedSci 1932; 184:610-615.
46. Brennan MF. Total parenteral nutrition in the cancer patients.N Engl. J Med 1981; 305:375-382.