impact of cross-sectoral approach to addressing konzo · pdf fileimpact of cross-sectoral...
TRANSCRIPT
DEMOCRATIC REPUBLIC OF CONGO
IMPACT OF CROSS-SECTORAL APPROACH TO ADDRESSING KONZO IN DRC
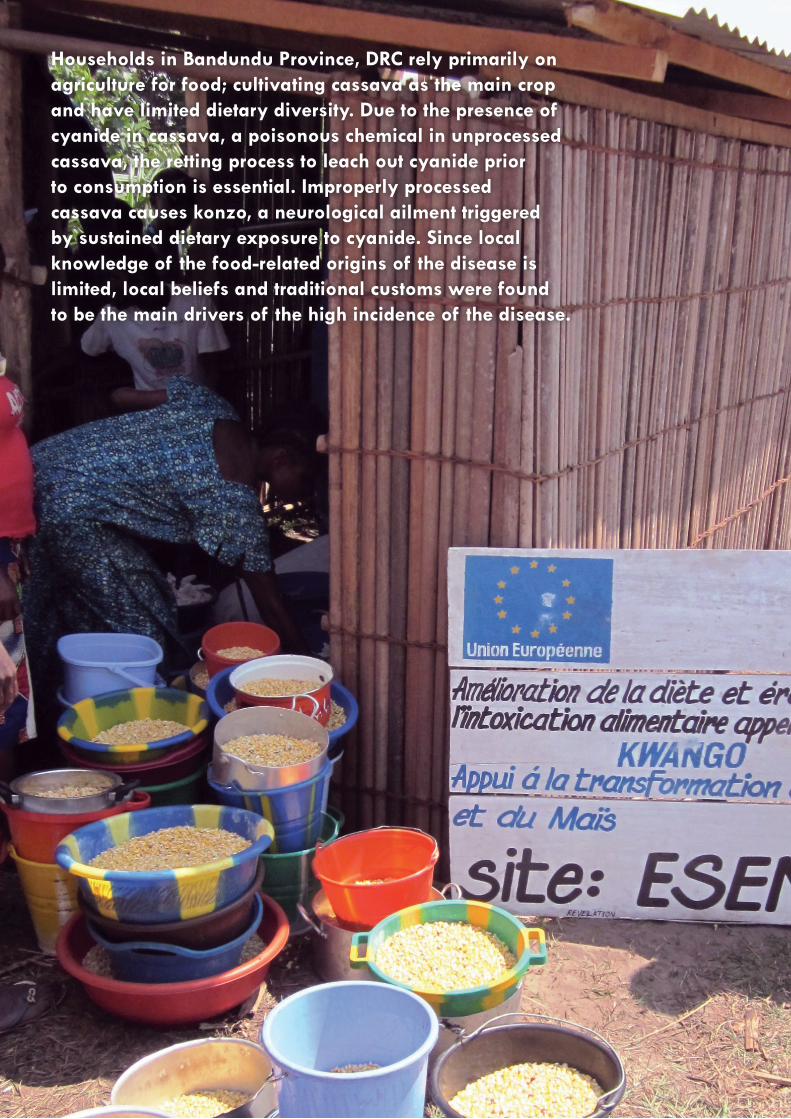
Households in Bandundu Province, DRC rely primarily on agriculture for food; cultivating cassava as the main crop and have limited dietary diversity. Due to the presence of cyanide in cassava, a poisonous chemical in unprocessed cassava, the retting process to leach out cyanide prior to consumption is essential. Improperly processed cassava causes konzo, a neurological ailment triggered by sustained dietary exposure to cyanide. Since local knowledge of the food-related origins of the disease is limited, local beliefs and traditional customs were found to be the main drivers of the high incidence of the disease.

3
From December 2009 to October 2011, Action Against Hunger (ACF-USA) implemented an intervention in the Bandundu province of the Democratic Republic of Congo (DRC), addressing factors underlying the konzo epidemic affecting the population of Kwango district.
The “Integrated Programme for the Eradication of Konzo in the Territory of Kwango in DRC” project was financed by the European Union (EU) Food Facility and aimed to eradicate the disease through a cross-sectoral approach focused on nutrition education and training, dietary diversification, improved water access and agricultural processing.
The strategy also aimed to address the high rates of malnutrition seen in konzo cases [25.8% global acute malnutrition (GAM) prevalence in konzo affected children less than 18 years old, 69.3% of GAM in konzo affected adults]. A total of 22,000 households benefited from these activities. Due to limited resources, project activities were not carried out in all konzo locations, but rather in the most affected villages.
Vulnerability Context
Background
Konzo is a sudden epidemic spastic paraparesis (paralytic) disease which leads to a permanent paralysis of the affected person’s lower limbs. It is a neurological ailment triggered by sustained dietary exposure to cyanide present in improperly processed cassava. Overall, vulnerability to konzo is heightened by the combination of low protein intake (associated with low dietary diversity), poor soil conditions (which favor the cultivation and consumption of bitter cassava varieties high in cyanide), and lack of sufficient water resources for thorough processing.
DRC
Kinshasa
Bandundu
Figure 1: ACF program area in Kwango district, Bandundu province, DRC
What is Konzo?
4 © ACF - Haïti
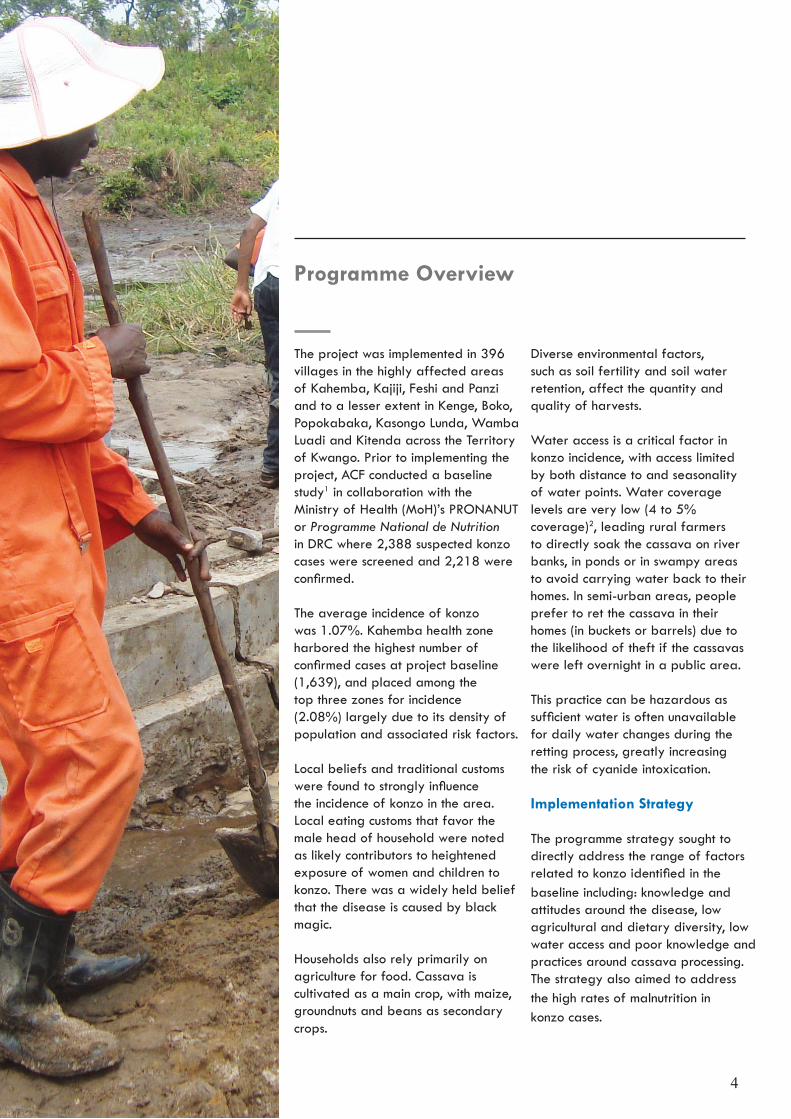
Diverse environmental factors, such as soil fertility and soil water retention, affect the quantity and quality of harvests.
Water access is a critical factor in konzo incidence, with access limited by both distance to and seasonality of water points. Water coverage levels are very low (4 to 5% coverage)2, leading rural farmers to directly soak the cassava on river banks, in ponds or in swampy areas to avoid carrying water back to their homes. In semi-urban areas, people prefer to ret the cassava in their homes (in buckets or barrels) due to the likelihood of theft if the cassavas were left overnight in a public area.
This practice can be hazardous as sufficient water is often unavailable for daily water changes during the retting process, greatly increasing the risk of cyanide intoxication.
Implementation Strategy
The programme strategy sought to directly address the range of factors related to konzo identified in the baseline including: knowledge andattitudes around the disease, low agricultural and dietary diversity, low water access and poor knowledge and practices around cassava processing. The strategy also aimed to address the high rates of malnutrition inkonzo cases.
Programme Overview
The project was implemented in 396 villages in the highly affected areas of Kahemba, Kajiji, Feshi and Panzi and to a lesser extent in Kenge, Boko, Popokabaka, Kasongo Lunda, Wamba Luadi and Kitenda across the Territory of Kwango. Prior to implementing the project, ACF conducted a baseline study1 in collaboration with the Ministry of Health (MoH)’s PRONANUT or Programme National de Nutrition in DRC where 2,388 suspected konzo cases were screened and 2,218 were confirmed.
The average incidence of konzo was 1.07%. Kahemba health zone harbored the highest number of confirmed cases at project baseline (1,639), and placed among the top three zones for incidence (2.08%) largely due to its density of population and associated risk factors.
Local beliefs and traditional customs were found to strongly influence the incidence of konzo in the area. Local eating customs that favor the male head of household were noted as likely contributors to heightened exposure of women and children to konzo. There was a widely held belief that the disease is caused by black magic.
Households also rely primarily on agriculture for food. Cassava is cultivated as a main crop, with maize, groundnuts and beans as secondary crops.

5
Knowledge and Attitudes on Konzo and Nutrition
Project design used a cross-sectoral approach to address underlying factors in a holistic manner.
Community Outreach, Mobilization and Education
ACF employed a community outreach and mobilization approach with the creation of 647 community nutrition forums across 395 villages for discussion on konzo and nutrition. These served as launch pads for a broadly based educational campaign extending to churches, schools, local health professionals, community volunteers and leaders, traditional authorities, etc.
Information, Education & Communication (IEC) materials and messages on food processing and preparation, nutrition and konzo were developed in collaboration with PRONANUT, displayed in a variety of public areas and broadcast on local radio.
Mass sensitization sessions were organized in churches, mosques and schools. Senior MoH staff, community leaders and authorities, and local volunteers were trained to pass the message broadly. Volunteers supported community nutrition forums and facilitated weekly dialogues. Cooking demonstrations were organized in each forum around improved fufu recipes based on mixed cassava and maize flour.
Agricultural and Hydraulic Infrastructure Support
ACF introduced two improved food crop varieties, niébé (cowpea) Vita 7 and Muyaya, and sweet cassava TME119, Mwuazi, Nsasi, Disanka and Butamu for increased consumption of sulphur amino acids contained in cereal and leguminous foods and complement consumption of traditional cyanide-heavy bitter cassava varieties.
ACF delivered agricultural trainings to 12,500 households and supported installation of 13 village based mills to increase access to milling services and improve flour quality. In order to increase water access, ACF implemented a variety of hydraulic constructions: public retting tanks to process cassava, boreholes, springs, rainwater harvesting systems and piped distribution networks.
MethodsThe impact study was conducted across the project area. A stratified sampling approach was used, with six of eleven intervention health zones selected purposively, and 40 of 395 intervention villages selected randomly. In each selected village, six beneficiary households were randomly selected to participate in household surveys (234 in total). Household surveys were supplemented with information from key informants and focus groups.
Changes in knowledge at endline compared to baseline suggest that community outreach and education activities were effective in challenging long held local beliefs on konzo and nutrition. At project baseline, 74% of sampled population attributed the disease to a metaphysical origin, while 88% correctly noted the food-related causes of konzo at endline.
Participation in a community nutrition forum was found to be correlated with knowledge of the food-related cause of konzo. In addition, there were strong inverse correlations between both ‘participation’ and ‘lack of knowledge’, and ‘participation’ and ‘belief in a metaphysical origin’.
These findings reveal the importance of outreach and education activities delivered both within the community forums and directly by ACF. Similar results were found regarding knowledge, attitudes and practice on prevention strategies based on effective messaging that encouraged appropriate processing of cassava and inclusion of protein in diets through incorporation of maize flour into fufu preparation and legumes (pulses) in the diet.
Findings

6
New varieties of niébé were largely accepted across the intervention zone and integrated into the diet, notably on the eastern axis (Kahemba, Kajiji) where populations were unfamiliar with niébé. Sweet cassava was readily integrated into both east and west Kwango, with results showing a general increase in the intercropping of both bitter and sweet varieties, as well as increased cultivation of sweet varieties on their own.
In Kahemba, the bitter cassava variety, Mwambo, is widely cultivated and consumed to the exclusion of other varieties, whereas both bitter and sweet varieties are cultivated and consumed along the western axis.
However, sweet varieties were well accepted in Kahemba as they offer shorter processing times and are immediately consumable. Notable improvement was seen in overall food stocks and diversity of food items held by households over the life of the project.
The positive trend in diversity and volume of household food stocks may be attributed to project impact, in particular Information, Education and Communication (IEC) activities around balanced diets, food processing and preparation, as well as external factors such as climate, crop disease and seasonal fluctuations.
ACF supported the installation of village based mills to increase access to maize and cassava milling services and improve the quality of the flour. ACF also implemented a variety of hydraulic construction: public retting tanks to process cassava, boreholes, springs, rainwater harvesting systems and piped distribution networks.
Knowledge of community leaders and member households of community nutrition forums regarding cassava retting and drying techniques similarly improved. Community leaders correctly reporting optimal processing time increased from 60% to 99%. Constraints around access to processing sites and water quality limited optimal practice.
At endline, a majority of households indicated they were processing cassava in rivers or ponds, and had largely abandoned utilization of home retting techniques that rely on prolonged use of the same water, saturated in acid and less effective in cyanide detoxification. Constraints to optimal practice include the risk of theft of tubers at open river and pond sites, as well as dietary and income pressures.
Impacts on cassava retting practice from ACF’s establishment of communal retting tanks were not known as the infrastructures were in process of installation at the time of survey.
A surveillance system for screeningand identification of konzo cases in Kahemba health zone was established by the local health structure in 2009, with annual caseload an estimated 1,300 individuals in 2009.
MoH educational activities and ACF integrated activities on konzo were launched in early to mid-2010, with a marked decrease in cases recorded that year. A further reduction in caseload between 2010 and 2011was noted during the critical months of June, July and August with 47 new cases recorded in 2011, an 84% reduction in annual incidence.
The greatest reduction in new cases was observed among the under 5 years of age group. The results on reduced incidence are confirmed by ACF analytical findings of urine and cassava flour sample cyanide content, taken from 100 randomly selected beneficiary households at project endline.
A 50% reduction in flour samples presenting medium to high cyanide levels (20 to 40 ppm) was observed compared with baseline, as well as a 16% reduction in thiocyanate levels in urine samples (>300µmol). These reductions translate into a slightly lower risk of developing konzo.
Konzo Incidence Cassava Retting Techniques and Water Access
Food Stocks and Dietary Diversification
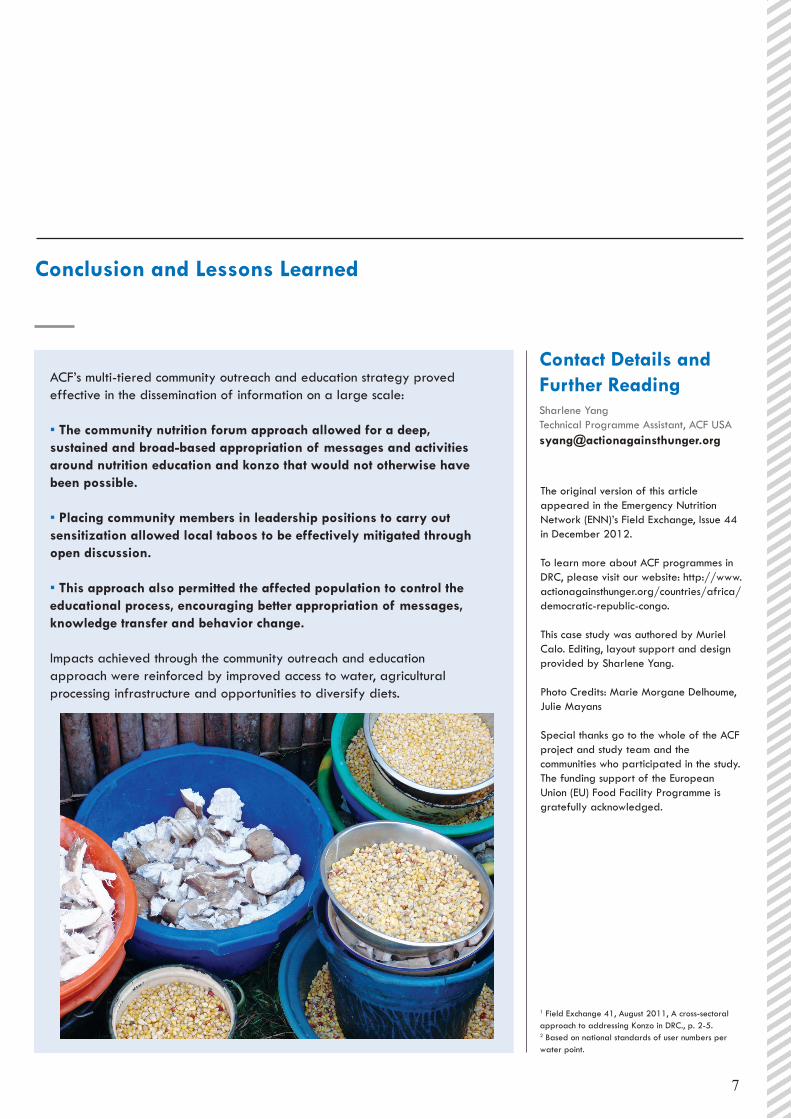
Contact Details andFurther Reading ACF’s multi-tiered community outreach and education strategy proved
effective in the dissemination of information on a large scale:
▪ The community nutrition forum approach allowed for a deep, sustained and broad-based appropriation of messages and activities around nutrition education and konzo that would not otherwise have been possible.
▪ Placing community members in leadership positions to carry out sensitization allowed local taboos to be effectively mitigated through open discussion.
▪ This approach also permitted the affected population to control the educational process, encouraging better appropriation of messages, knowledge transfer and behavior change.
Impacts achieved through the community outreach and education approach were reinforced by improved access to water, agricultural processing infrastructure and opportunities to diversify diets.
Conclusion and Lessons Learned
7
Sharlene YangTechnical Programme Assistant, ACF [email protected]
The original version of this article appeared in the Emergency Nutrition Network (ENN)’s Field Exchange, Issue 44 in December 2012.
To learn more about ACF programmes in DRC, please visit our website: http://www.actionagainsthunger.org/countries/africa/democratic-republic-congo.
This case study was authored by Muriel Calo. Editing, layout support and design provided by Sharlene Yang.
Photo Credits: Marie Morgane Delhoume, Julie Mayans
Special thanks go to the whole of the ACF project and study team and the communities who participated in the study. The funding support of the European Union (EU) Food Facility Programme is gratefully acknowledged.
1 Field Exchange 41, August 2011, A cross-sectoral approach to addressing Konzo in DRC., p. 2-5.2 Based on national standards of user numbers per water point.
This document is part of a set of case studies on ACF Food Security and Livelihoods interventions which aim to reduce and/or prevent undernutrition. It has been developed by the ACF “Aligning Food Security and Livelihoods with Nutrition” Working Group. The aim of the “Aligning Food Security and Livelihoods with Nutrition” Working Group is to promote and scale up nutrition-sensitive Food Security and Livelihoods interventions, within ACF as well as partner organizations. The Working Group promotes these interventions by gathering lessons, building evidence, developing tools and guidance and building capacity.
For more information on the “Aligning” approach, please refer to the ACF manual: Maximising the nutritional impact of Food Security and Livelihoods interventions. A manual for field workers. http://www.actionagainsthunger.org/publication/2011/07/maximising-nutritional-impact-food-security-and-livelihoods-interventions-manual