impact of genomics and exposures on disparities in …feistweiller.org/clientuploads/clinical...
TRANSCRIPT

Amendment 2: 11/23/2011 1 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
NCI Protocol #: 97609 WF Protocol #: CCCWF 97609 IND # (If applicable): NA
Impact of Genomics and Exposures on Disparities in Breast Cancer Radiosensitivity
Research Base Name: Comprehensive Cancer Center of Wake Forest CCOP Research
Base (CCCWF CCOP RB) Name of RB Principal Edward G. Shaw, MD, MA Investigator: Wake Forest School of Medicine Dept. of Radiation Oncology
2000 West First Street, Suite 401 Winston-Salem, NC 27104 Telephone (336) 716-0891 Fax (336) 716-6275 E-mail address:
Organization Name: CCCWF CCOP RB Protocol Principal Investigator: James J. Urbanic, MD Dept. of Radiation Oncology Wake Forest School of Medicine
Medical Center Boulevard Winston-Salem, NC 27157 Telephone (336) 713-6542 Fax (336) 713-6565 E-mail address:
Organization: University of Miami School of Medicine Co-Principal Investigator: Jennifer Hu, PhD Department of Epidemiology and Public Health 1511 Clinical Research Bldg
1120 NW 14th Street Miami, FL 33136
Phone (305) 243-7796 Fax (305) 243-2997 Email: [email protected] Organization: Wake Forest School of Medicine Co-Investigator: Zheng Cui, PhD Department of Pathology, Section on Tumor Biology Medical Center Boulevard
Winston-Salem, NC 27157-1092 Phone (336) 716-6185 Fax (336) 716-6757 Email: [email protected]

Amendment 2: 11/23/2011 2 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Organization: University of Miami School of Medicine Co-Investigator: Jean L. Wright, M.D.
Department of Radiation Oncology 1475 N.W. 12th Avenue Miami, FL 33136 Phone (305) 243-4916 Fax (305) 243-4363 Email:
Organization: CCCWF CCOP RB Statistician: Doug Case, Ph.D. Department of Biostatistical Sciences
Division of Public Health Sciences Wake Forest School of Medicine
Medical Center Boulevard Winston-Salem, NC 27157 Telephone (336) 716-1048 Fax (336) 716-5425 E-mail address: [email protected]
Organization: University of Miami School of Medicine Co-Statisticians: Isildinha M. Reis, PhD and Hosanna Soler-Vila, PhD Department of Epidemiology and Public Health Clinical Research Bldg - 1063
1120 NW 14th Street Miami, FL 33136
Phone (305) 243-8208 Fax (305) 243-2997 Email: [email protected] RB Administrator: Gina Enevold, MSN, GNP Wake Forest School of Medicine Department of Radiation Oncology 2000 West First Street, Suite 401 Winston-Salem, NC 27104 Telephone: (336) 716-4035 Fax: (336) 716-6275 Email:
Site Coordinator: June Fletcher-Steede, BS, RT(R)(T), CCRP Wake Forest School of Medicine Department of Radiation Oncology 2000 West First Street, Suite 401 Winston-Salem, NC 27104 Telephone: (336) 716-6733 Fax: (336) 716-6275 Email: [email protected]
RB Clinic Nurse: Robin Rosdhal, RN, OCN Wake Forest School of Medicine Department of Radiation Oncology Outpatient Comprehensive Cancer Center Medical Center Boulevard Winston-Salem, NC 27157 Telephone: (336) 713-6519 Fax: (336) 713-6476 Email: [email protected]

Amendment 2: 11/23/2011 3 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Grant: NCI/Division of Cancer Prevention 6130 Executive Blvd., Room 2117
Bethesda, MD 20892 (For FedEx, use Rockville, MD 20852) (301) 496-8563 Agent(s)/Supplier: Protocol Version Date: 11/09/11
N/A
Approval Dates: PRC: 08/25/09 NCI: 07/22/11 FDA: NA IRB: 09/20/10 Activation Date: WF: 09/20/11 Sites: 09/20/11 NCI Version Date: 06/09/11 Renewal Dates: 1: 08/10/11 Amendment/Update # & Date: 1: 09/16/11 2: 11/23/11

Amendment 2: 11/23/2011 4 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
This study is supported by the NCI Cancer Trials Support Unit (CTSU). Institutions not aligned with WF CCOP Research Base will participate through the CTSU mechanism
as outlined below and detailed in the CTSU logistical appendix (Appendix 17). • The study protocol and all related forms and documents must be downloaded from the
protocol-specific Web page of the members’ section of the CTSU Web site located at www.ctsu.org.
• Send completed site registration documents to the CTSU Regulatory Office. Refer to the CTSU
logistical appendix for specific instructions and documents to be submitted. • Patient enrollments will be conducted by the CTSU. Refer to the CTSU logistical appendix for
specific instructions and forms to be submitted. • Data management will be performed by the CCCWF CCOP Research Base Data Management
Center (DMC). Case report forms (with the exception of patient enrollment forms), signed consents, clinical reports, and transmittals must be sent via mail or fax to the CCCWFCCOP Research Base DMC unless otherwise directed by the protocol. Your institutions standard fax transmittal cover sheet should accompany all data submissions. Do not
send study data or case report forms to CTSU Data Operations.
• Data query and delinquency reports will be sent directly to the enrolling site by CCCWF CCOP Research Base DMC. Please send query responses and delinquent data to CCCWF CCOP Research Base DMC and do not copy the CTSU Data Operations. Each site should have a designated CTSU Administrator and Data Administrator and must keep their CTEP IAM account contact information current. This will ensure timely communication between the clinical site and the CCCWF CCOP Research Base DMC.

Amendment 2: 11/23/2011 5 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
CTSU CONTACTS TABLE To submit site registration documents:
For patient enrollments: Submit study data directly to the Lead Cooperative Group unless otherwise specified in the protocol:
CTSU Regulatory Office 1818 Market Street, Suite 1100 Philadelphia, PA 19103 Phone – 1-866-651-CTSU Fax – 215-569-0206
CTSU Patient Registration Voice Mail – 1-888-462-3009 Fax – 1-888-691-8039 Hours: 9:00 AM – 5:30 PM Eastern Time, Monday – Friday (excluding holidays) [Registrations received after 5:00 PM ET will be handled the next business day. For CTSU patient enrollments that must be completed within approximately one hour, or other extenuating circumstances, call 301-704-2376 between 9:00 am and 5:30 pm.]
CCCWF CCOP Research Base Attn: Data Management Center Outpatient Comprehensive Cancer Center Medical Center Boulevard Winston Salem, NC 27157-1030 FAX: 336-713-6476 Do not submit study data or forms to CTSU Data Operations. Do not copy the CTSU on data submissions.
For patient eligibility or treatment-related questions contact the Research Nurse listed on the protocol cover page. For questions unrelated to patient eligibility, treatment, or data submission
CTSU General Information Line – 1-888-823-5923, or
contact the CTSU Help Desk by phone or e-mail:
[email protected]. All calls and correspondence will be triaged to the appropriate CTSU representative.
The CTSU Web site is located at: www.ctsu.org.
CTSU logistical information is located in Appendix 17.

Amendment 2: 11/23/2011 6 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
SCHEMA
candidate identified for post-lumpectomy, - quadrantectomy, or –mastectomy RT
consent and registration
Baseline labs, questionnaires, photographs
Week 3 Photographs for patients receiving standard fractionation only
Last Day RT; 1 month post RT; 2 months post RT; 6 months post RT; 12 months post RT – complete labs, Questionnaires and photographs as indicated in Section 7.9 Study Parameters Table
Study Sample: 1000 (400 White, 200 African American, 200 Hispanic/Latino, 100 Asian/Native Hawaiian or Pacific Islander, 100 American Indian/Alaskan Native) Study Duration: 52 weeks Brief Inclusion Criteria: • Female subjects newly diagnosed with breast carcinoma, stage 0–IIIA, post-lumpectomy,
quadrantectomy, or mastectomy • Plan to receive adjuvant radiation to the breast or chest wall +/- regional lymph nodes. The following
parameters must be met: total dose >40Gy, dose per fraction >1.8 including hypofractionated regimens, use of 2D, 3D conformal, or IMRT treatment techniques (skin sparing IMRT patients excluded ).
• Adjuvant hormonal therapy will be allowed prior to, during and/or after RT at the discretion of a medical oncologist.
• Targeted therapies such as Herceptin will be allowed prior to, during, and/or after RT at the discretion of the medical oncologist.
Amendment 2: 11/23/2011 7 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
INDEX
COVER PAGE SCHEMA 1. OBJECTIVES ........................................................................................................................................ 8 2. BACKGROUND AND RATIONALE. .................................................................................................. ..8 3. SUMMARY OF STUDY PLAN……………………………………………………………………………….18 4. PARTICIPANT SELECTION ............................................................................................................... 20 5. AGENT ADMINISTRATION ............................................................................................................... n/a 6. REGISTRATION/RANDOMIZATION.................................................................................................. 22 7. CLINICAL EVALUATIONS AND PROCEDURES ............................................................................. 23
8. PROTOCOL SPECIFIC TRAINING REQUIREMENTS ..................................................................... n/a
9. SPECIMEN MANAGEMENT .............................................................................................................. 29 10. REPORTING ADVERSE EVENTS ..................................................................................................... 32 11. STUDY MONITORING ........................................................................................................................ 34 12. STATISTICAL CONSIDERATIONS ................................................................................................... 36
REFERENCES INFORMED CONSENT APPENDICES
1. Data Submission Checklist 2. Eligibility Checklist/Registration Form 3. Performance Status Criteria 4. MedWatch 5. Study Parameters Table 6. TNM Nomenclature and Staging for Breast Cancer 7. Baseline Breast Cancer Study Risk Questionnaire 8. Follow-up Breast Cancer Study Risk Questionnaire 9. Modified Skindex-16 Questionnaire 10. B39 Quality of Life Questionnaire (10A Intact Breast) (10B Chest Wall) 11. RTOG SOMA Criteria for RT-Induced Breast/Chest Wall Late Skin Toxicity 12. Instructions for Photographs 13. Breast/Chest Wall RT Completion Form 14. ONS Criteria for Radiation Induced Acute Skin Reaction 15. FACT-B QOL Questionnaire 16. Specimen Kit Shipping Form 17. CTSU Logistics 18. Flow Sheet/Addenda 19. Flyer

Amendment 2: 11/23/2011 8 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
1.0 OBJECTIVES 1.1 Primary Objective
The primary objective of the proposed research is to develop and validate prediction biomarkers for RT-induced acute and chronic skin reactions and quality of life in five racial/ethnic groups of breast cancer patients, Whites, Black/African Americans (AA), Hispanic/Latinos, Asians/Native Hawaiians/Pacific Islanders, and American Indians/Alaskan Natives. Specific Aim 1: To develop polygenic models of RT-induced skin reactions with a comprehensive evaluation of genome-wide nonsynonymous single nucleotide polymorphisms (nsSNPs; n=21,877). This approach will identify new genomic markers and test 9 major cancer-related candidate pathways, angiogenesis, apoptosis, proliferation, cell-cycle control, developmental processes, DNA repair, cell signaling, cell migration and immunology/inflammation. We hypothesize that amino-acid-altering nsSNPs lead to protein sequence and functional changes relevant to IR response. We will also assess the additive and/or multiplicative effects of multiple specific genes on RT-induced skin reactions using a newly developed data mining tool, Multivariate Adaptive Regression Splines logit models. Specific Aim 2: To evaluate the levels of DNA damage (Comet assay) and radio sensitivity (Cell Cycle G2 Delay assay) in lymphocytes before and after RT and test the hypothesis that individuals with more severe acute and chronic RT-induced skin reactions will have higher IR-induced DNA damage and radio sensitivity. Specific Aim 3: To test the effect of gene-gene and gene-smoking interactions on RT-induced skin reactions. Candidate nsNSPs-genotypes will be those identified as potential risk factors, that is, those that best discriminate between cases and controls as resulting from analyses under Specific Aim1. Specific Aim 4:
The outcome from this research will provide insight into the roles of genetic susceptibility in acute and chronic RT-induced skin reactions at the individual level. As we learn more about the contributions of and interactions among genetic susceptibility to more severe skin reactions, we can develop targeted preventive strategies for those predicted to be at higher risk.
To assess race-ethnic differences in RT-induced skin reactions, DNA damage, and radio sensitivity and to determine if the gene effects are consistent across race-ethnicities (gene-race/ethnic interactions).
2.0 BACKGROUND AND RATIONALE
2.1 Background
Breast Cancer Statistics Breast cancer is the most frequently diagnosed cancer in women. In 2010, approximately 209,060 US women would be diagnosed with invasive breast cancer (26% cancer cases among women), and 40,230 would die of this malignancy (Jemal et al., 2010). In addition to invasive breast cancer, 54,010 new cases of in situ breast cancer were expected to occur among American women in 2010. Considering tumor size, stage, and other characteristics, as well as patient preference, treatment may involve lumpectomy or mastectomy, radiotherapy (RT), chemotherapy, hormone therapy, or targeted biologic therapy. As early-detection methods and treatments for breast cancer have improved over the past decades, there are more than two million US breast cancer survivors. Therefore, it is important to address survivorship issues, including treatment adverse response, physical, and psychosocial issues at diagnosis, during treatment, and for the

Amendment 2: 11/23/2011 9 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
remaining years of their lives. Clinical guidelines recommend that when breast-conserving surgery is provided as primary therapy for early-stage breast cancer, radiation therapy should follow.
Benefit and Quality of Life Issues Related to Breast Conservation Adjuvant RT Two recent meta-analyses of randomized clinical trials showed that compared with surgery alone, the addition of RT to breast cancer therapy reduced the rate of local cancer recurrence (Clarke et al., 2005; Viani et al., 2007). The conclusion from one meta-analysis is that the addition of radiation therapy to lumpectomy results in an approximate 60% reduction in breast cancer recurrence, with no benefit for survival or distant metastases as compared to excision alone. Patients with high-grade DCIS lesions and positive margins benefited most from the addition of radiation therapy. It is not clear yet which patients can be successfully treated with lumpectomy alone; until further prospective studies answer this question, radiation to the entire breast was recommended after lumpectomy for all patients without contraindications. Although well tolerated by most patients, both acute and chronic skin toxicities are potential side effects after RT completion (Lilla et al., 2007). The development of these normal tissue reactions in breast cancer patients receiving adjuvant external beam RT demonstrates significant heterogeneity among individuals (Twardella et al., 2003), which can be attributed to a variety of individual, tumor stage, cellular, and molecular factors. During the past several years, an increasing amount of evidence has suggested that individual genetic variations may also play a significant role in the development of adverse radiation responses (Alsbeih et al., 2007a; Andreassen et al., 2006; De Ruyck et al., 2005). The impact of radio sensitivity candidate genes and variants in the development of adverse radiation responses becomes an active area of investigation. Some of the genetic variations on these genes are also associated with elevated breast cancer risk and/or local recurrence (Broeks et al., 2006; Edvardsen et al., 2007; Walsh et al., 2006) or survival (Einarsdottir et al., 2006). Several studies, including our work, also suggest that cellular radio sensitivity is associated with amino acid substitution variants in susceptible genes and correlates with the number of risk alleles (Hu et al., 2001; 2002; Alsbeih et al., 2007; Jones et al., 2007; Wilding et al., 2007).
Survival Benefit of PMRT in Node-Positive Breast Cancer Patients
Treatment for breast cancer may involve surgery consisting of lumpectomy, quadrantectomy, or mastectomy, RT, cytotoxic chemotherapy, hormone therapy, and/or targeted biologic therapy. Studies show that the choice of mastectomy over breast-conserving surgery is becoming more common, especially in patients with early-stage breast cancer (McGuire et al., 2009). At the same time, increasing data demonstrates a local control and overall survival advantage with the use of PMRT in all node-positive patients. Randomized studies from British Columbia and Denmark originally published in the 1990’s demonstrated a survival advantage to post mastectomy radiation therapy (PMRT) in node-positive patients (Overgaard et al., 1997; Ragaz et al., 2005; Overgaard et al., 1999). However it was not until the publication of the “Oxford Overview” meta-analyses of randomized clinical trials in 2005, which showed that compared with surgery alone, the addition of PMRT reduced both the rate of local cancer recurrence and improved 15-year breast cancer mortality by 5% (Clarke et al., 2005), that the survival benefit of PMRT became more widely accepted. Thus the number of patients with an indication for PMRT is increasing, and investigating quality of life and clinical outcomes in this subset of patients becomes increasingly important. The majority of studies examining quality of life after mastectomy focus on cosmetic and psychosocial issues, and there is little data available on acute toxicity of PMRT, and specifically how this toxicity impacts quality of life.
Amendment 2: 11/23/2011 10 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
RT-Related Adverse Reactions Radiation side effects associated with radiation to the breast or chest wall are variable and depend on many factors. The majority of data available regarding side effects is generated from patients receiving radiation to the intact breast. In general, side effects are grouped as acute, occurring < 12 weeks following radiation treatment, and late, occurring more than 12+ weeks after completion of treatment. During RT, most patients have some degree of treatment-related fatigue. The other common acute toxicity is related to the skin within the irradiated volume; the skin typically becomes erythematous and/or hyperpigmented, and may desquamate, in particular in the area of skin folds, such as the inframammary fold, axilla, and/or supraclavicular fossa. Desquamation may be dry or moist. At its extreme, ulceration, hemorrhage, or even necrosis can occur. There is a great deal of variation in the severity of acute skin reactions. A randomized trial investigating the use of intensity-modulated RT (IMRT) in the setting of breast conservation therapy (BCT) demonstrated moist desquamation in 31% receiving IMRT and 48% with standard 2D or 3D conformal radiation treatment, respectively (Pignol et al., 2008). The primary factor that predisposed to moist desquamation was large breast size; race-ethnicity and genetic factors were not assessed in this Canadian study. Factors contributing to variation in EASRs in patients receiving PMRT have not been well studied.
Acute skin toxicities are generally more severe in the setting of PMRT than breast conserving therapy, as the skin itself is considered part of the radiation target with PMRT. Despite this, there is remarkably little data available on adverse skin reactions in PMRT patients. The three large randomized trials investigating the use of PMRT either do not report toxicity (Overgaard et al., 1997; Overgaard et al., 1999), or report only late toxicity (changes in pigmentation, pain, edema, fibrosis, telangiectias, ulceration) but not acute toxicities (Ragaz et al., 2005). One small retrospective series of 89 patients receiving PMRT using electrons reports that 19 patients developed dry desquamation, and 5 moist desquamation (Hehr et al., 1999). In contrast, a series of 118 patients treated with a similar technique reports that 52% of patients developed acute grade 3-4 skin toxicity (moist desquamation, hemorrhage, and/or necrosis) by RTOG criteria, and 31% of patients required an unplanned treatment break to recover from these acute effects (Spierer et al., 2004). This is significant in that it has been shown that prolonged radiation treatment time due to unplanned breaks negatively impacts clinical outcomes in breast cancer patients (Bese et al., 2007), and this has also been found to be true in other disease sites including head and neck cancers and gynecologic malignancies (Delaloye et al., 1997; McCloskey et al., 2009; Suwinski et al., 2003; Yamazaki et al., 2006). In the group of patients receiving PMRT, the majority of whom are node-positive and who thus have a poorer prognosis than many patients undergoing BCT, the ability to complete the prescribed treatment is critical. If acute radiation-induced skin toxicities result in treatment breaks or early termination of treatment, this could have a detrimental impact on clinical outcomes including local recurrence and survival. Thus, assessing risk factors for acute radiation reactions in the PMRT population may ultimately have prognostic significance as well.
In addition to local control, several recent studies suggest that RT also has unique biological effects and that, in addition to killing tumor cells, it might favorably alter the microenvironment at the primary tumor site during wound healing and trigger antitumor immune responses (Formenti and Demaria, 2008; Lugade et al., 2008; Matsumura et al., 2008). To pilot test this hypothesis, we will evaluate immune/inflammatory genotyping data and keep 50% of the cryopreserved lymphocytes for performing future immune functional assays. The proposed research will develop new prediction models for breast cancer clinical outcome combining genetic susceptibility risk models.

Amendment 2: 11/23/2011 11 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Table 1. RT-Related Adverse Reactions in PMRT patients
In terms of late toxicity of PMRT, the breast or chest wall may remain tender to palpation and the skin remains hyperpigmented for 6 to 9 months after treatment. Fibrosis may develop (Lilla et al., 2007), affecting the texture and contour of the breast or chest wall, and in the most severe cases interfering with shoulder mobility and thus ability to complete activities of daily living. The most common permanent effects on normal tissue are minor changes in the aesthetic appearance of the breast resulting from volume loss, fibrosis, or retraction at the tumor-bed site (Collette et al., 2008; Poortmans et al., 2009). Telangiectasias may also develop over time (Lilla et al., 2007). Breast or chest wall pain, increased risk of rib fracture, increased risk of cardiac morbidity, and lymphedema are also known late side effects of radiation (Buchholz et al., 2009). The most serious potential late complications of RT are injury to the lungs and heart and the risk of inducing secondary cancers. Improvements in radiation equipment and technique have helped reduce these risks (Giordano et al., 2005). Current techniques also minimize the small carcinogenic risks associated with radiation therapy by reducing the volume of normal tissue within the treatment fields and reducing the dose from scatter radiation to the contralateral breast (Borghero et al., 2007).
The development of normal tissue toxicities in breast cancer patients receiving adjuvant external beam RT demonstrates significant heterogeneity among individuals (Twardella et al., 2003) which can be attributed to a variety of individual, tumor, cellular, and molecular factors. During the past several years, increasing evidence has suggested that individual genetic variations may also play a significant role in the development of adverse radiation responses (Alsbeih et al., 2007; Andreassen et al., 2006; De Ruyck et al., 2005), but these remain poorly understood. In Table 1, we summarize the results from studies evaluating PMRT-related side effects in breast cancer patients. It is notable that the majority of
Sample Size Clinical Outcome Study Variables References 41 Late tissue fibrosis and
telangiectasias XRCC1&3, TGFB1, SOD2, APEX SNPs
Andreassen et al., 2003
118 52% grade 3-4 acute skin toxicity; 31% unplanned RT break
- Spierer et al., 2004
89 19 dry desquamation; 5 moist desquamation
- Hehr et al., 1999
358 Notably moist desquamation as early reaction
31.2% in IMRT patients 47.8% in standard RT
Pignol et al., 2008
390 Late fibrosis (>4 yrs; 7%) GSTA1; CAT SNPs Kuptsova et al., 2008
5178 Late fibrosis (10 years) 28% in 1797( with boost) 13% in 1827 (without boost)
Collette et al., 2008
251 Local relapse in cases with microscopically incomplete lumpectomy
10 Gy boost: 44% local relapse and 20% fibrosis 26 Gy boost: 31% local relapse and 50% fibrosis
Poortmans et al., 2009

Amendment 2: 11/23/2011 12 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
studies focus on patients undergoing breast conserving therapy and few studies focus on patients undergoing PMRT.
Genetic Susceptibility to Radiation-Induced Adverse Response In response to RT, some breast cancer patients may experience potential early adverse skin reactions, such as bright erythema, breast/chest wall tenderness, dry and moist desquamation, and even ulceration, hemorrhage, and/or necrosis. Patients with severe acute skin reactions may miss one or more radiotherapy days and thus creating an unplanned “treatment break” which usually results in incomplete tumor cell killing which may lead to a higher risk of local recurrence and worse disease-free and potentially overall survival (Bese et al., 2005; 2007). Previous studies provide evidence to suggest that minority women are less likely than white women to receive the recommended adjuvant RT and have higher risk for developing acute radiation-related skin reactions.
Genetic variants in several genes, including ATM, APE1, TGFB1, XRCC1, XPD, XRCC3, p21 and TP53, have been recognized as potential predictors of RT-induced adverse responses. To guide our genetic variation selection, we have conducted a systematic evaluation of published literature and summarized the study results in Table 2. With limited sample size, small numbers of genes and SNPs studied, and lack of replication, the results from these studies suggest an association between ATM 1853 Asn allele and late adverse response of RT (Andreassen et al., 2006; Ho et al., 2007).
Table 2. Genetic Predictors for RT-Induced Adverse Response in Normal Tissue
* Same study population There are racial/ethnic differences in the distribution of ATM missense mutations/polymorphisms as reported in the Multiethnic Cohort Study with 428 breast cancer cases: 117 African-Americans (higher frequency for D126E, L546V, P872S, and M1040V), 101 Hispanics, 100 Japanese, and 110 Caucasians (higher frequency for D1853N) (Bretsky et al., 2003). In addition, there are racial/ethnic differences in adverse responses in ATM sequence variant carriers: 17% Hispanics, 23% African Americans, and 8% whites, respectively (Ho et al., 2007). Comparable data for other minority populations, such as Hawaiian natives, pacific islanders, American Indians, and Alaskan natives, will also be collected.
Sample Size(# Adverse
Response)
Genes Or SNPs
Outcome (% Adverse
Effects) Results References
254 (70) 3 XRCC1 SNPS
Acute Effects (28%)
Risk: XRCC1 194 TRP Allele
Moullan et al., 2003
446 (77)* XRCC1; APE1; XPD
Acute Effects (17%)
Protective: XRCC1 399 GLN and APE1 148
GLU Alleles
Chang-claude et al., 2005
446 (77)* TP53; P21 Acute Effects (17%)
Protective: TP53 72 PRO Allele and P21 SER/SER Genotype
Tan et al., 2006
41 (22) 26 ATM SNPS
Late Effects (54%)
Risk: ATM 1853 ASN/ASP and
ASN/ASN
Andreassen et al., 2006
131 (69) ATM SNPS Late Effects (53%)
Risk: ATM 1853 ASN Allele
Ho et al., 2007

Amendment 2: 11/23/2011 13 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Ionizing Radiation (IR)-Induced Cell Cycle Control, Apoptosis, and DNA Repair Recognition and signaling of IR-induced DNA damage is a prerequisite for the induction of subsequent cellular responses such as increased repair, cell cycle arrest and apoptosis. Recognition of DNA breaks is accomplished by a group of phosphatidylinositol-3-kinases. These kinases are ATM (Savitsky et al., 1995; Smith et al., 1999), ATR (ataxia telangiectasia related) and the catalytic subunit of DNA–PK (Hartley et al., 1995). Their targets share the consensus sequence Ser–Thr–Gln–Glu (Kim et al., 1999). ATR and ATM can bind to DNA ends of damaged DNA, which results in activation of the kinase activity. ATM/ATR in DNA repair, cell cycle control and apoptosis. Recognition and signaling of DNA damage is mediated by ATM and ATR, which bind to broken DNA ends and possibly some DNA adducts. Upon activation of their intrinsic kinase activity, ATM/ATR phosphorylate Chk1/Chk2, which in turn phosphorylate p53 and CDc25, thus provoking cell cycle arrest. In addition, ATM/ATR phosphorylate several other proteins (NBS1, Brca1) in DNA repair or, at high damage level, the induction of apoptosis. Several DNA-repair proteins such as BRCA1, MSH2, MSH6, MLH1, ATM, BLM, and the RAD50–MRE11–NBS1 complex, can be co-immunoprecipitated in the BRCA1-associated surveillance complex (Christmann et al., 2003).
IR-Induced DNA Damage and Repair IR induces many types of damage to DNA, requiring multiple repair pathways to restore genomic integrity, including Base-Excision Repair (BER) and two Double-Strand Break Repair (DSBR) pathways, homologous recombination (HR) and non-homologous end-joining (NHEJ). Most of the repair pathways are extremely complex, and many genes are involved in different repair pathways (Spry et al., 2007). BER is responsible for removing DNA-damaged bases, which can be recognised by specific enzymes, the DNA glycosylases. The main lesions subjected to BER are oxidised DNA bases, arising spontaneously within the cell, during inflammatory responses, or from exposure to exogenous agents, including ionizing radiation and long-wave UV light. Another main source of lesion repaired by BER is DNA alkylation induced by endogenous alkylating species and exogenous carcinogens such as nitrosamines. Also, various anticancer drugs such as DTIC and temozolomide induce alkylation lesions repaired by BER. Mechanism of base excision repair (BER). Recognition of the DNA lesion occurs by a specific DNA glycosylase which removes the damaged base by hydrolyzing the N-glycosidic bond. The remaining AP site is processed by APE. Depending on the cleavability of the resulting 5′dRP by Polβ, repair is performed via the short or long patch BER pathway. Lesions removed from DNA by BER include incorporated uracil, fragmented pyrimidines, N-alkylated purines, 8-oxo-7,8-dihydroguanine (8-OxoG), thymine glycol and many others. The major oxidised purine, 8-OxoG, is highly mutagenic because of mispairing with adenine. In general, there are five BER steps: (1) recognition, base removal and incision, (2) nucleotide insertion; (3) decision between short- and long-patch repair; (4) strand displacement and DNA-repair synthesis by long-patch BER; and (5) ligation by DNA ligases I and III (Christmann et al., 2003). DNA double-strand breaks (DSBs) are highly potent inducers of genotoxic effects (chromosomal breaks and exchanges) and cell death. In higher eukaryotes a single non-repaired DSB inactivating an essential gene can be sufficient for inducing cell death via apoptosis. There are two main pathways for DSB repair, homologous recombination (HR) and non-homologous end-joining (NHEJ), which are error-free and error-prone, respectively (see Fig. 3 and Fig. 4). In simple eukaryotes like yeast, HR is the main pathway, whereas in mammals the NHEJ pathway predominates (Cromie et al., 2001; Haber, 2000). The usage of NHEJ and HR also depends on the phase of the cell cycle. NHEJ occurs mainly in G0/G1, whereas HR occurs during the late S and G2 phases (Johnson and Jasin, 2000; Takata et al., 1998).

Amendment 2: 11/23/2011 14 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Mechanism of homologous recombination (HR). During HR, the damaged chromosome enters into physical contact with an undamaged DNA molecule with which it shares sequence homology and which is used as a template for repair Homologous recombination which starts with nucleolytic resection of the DSB in the 5′→3′ direction by the MRE11–Rad50–NBS1 complex, forming a 3′ single-stranded DNA fragment to which Rad52 binds. Rad52 interacts with Rad51, provoking a DNA strand exchange with the undamaged, homologous DNA molecule. Assembly of the Rad51 nucleoprotein filament is facilitated by different Rad51 paralogues (such as Rad51B, Rad51C and Rad51D, XRCC2 and XRCC3). After DNA synthesis, ligation and branch migration, the resulting structure is resolved (Christmann et al., 2003). Mechanism of non-homologous end joining (NHEJ). The NHEJ system ligates the two ends of a DSB without the requirement of sequence homology between the DNA ends. Recognition of and binding to damaged DNA occurs by the Ku70–Ku80 complex. Thereafter, the Ku heterodimer binds to DNA–PKcs, forming the DNA–PK holoenzyme. DNA–PK activates XRCC4–ligase IV, which links the broken DNA ends together. Before re-ligation by XRCC4–ligase IV, the DNA ends are processed by the MRE11–Rad50–NBS1 complex, presumably involving FEN1 and Artemis. Deficiency for FEN1 leads to a strong reduction in the usage of the NHEJ pathway. Another protein involved in processing overhangs during NHEJ is the protein Artemis, which acts in a complex with DNA–PK. Artemis displays single-strand-specific exonuclease activity. Upon forming a complex with and being phosphorylated by DNA–PKcs, Artemis acquires endonuclease activity, degrading single-strand overhangs and hairpins, which seems to be necessary for processing 5′ and 3′ overhangs during NHEJ (Christmann et al., 2003).
Biomarkers for Predicting Radiation-Induced Acute and Chronic Skin Toxicities IR is widely and successfully applied in breast cancer treatment. However, because of dose restrictions, a definitive cure cannot be achieved. Despite the advanced radiotherapy facilities available, high doses of radiation still induce early and late skin effects. Unacceptable normal tissue reactions remain the limiting factor for delivering high doses in radiotherapy. Changes in radiotherapy practice over the years include recognition of the importance of fraction size, fraction number, total dose, overall time for both tumor and normal tissue reactions, and the introduction of conservative therapy. Radiotherapy outcomes might be further improved by a greater understanding of the individual variations in normal tissue reactions that determine tolerance. When accurate genetic-based or cell-survival-based predictive assays are available to study tumor and normal tissue radiosensitivity, RT will become an exact science, allowing truly individual optimization and the prediction of adverse reactions. It is of great importance to identify the variations in intrinsic (cellular) radiosensitivity and extrinsic factors that are associated with a change in the risk of morbidity. It has yet to be determined whether intrinsic cell radiosensitivity or extrinsic factors have a greater influence on individual differences in damage expression. Several previous studies evaluated whether intrinsic molecular radiosensitivity can predict skin reactions to RT (Lopez et al., 2005; Pinar et al., 2007). The results were inconsistent. DNA damage levels in lymphocytes obtained from breast cancer patients before radiotherapy did not correlate with acute and late skin reactions to RT (Lopez et al., 2005). However, a more recent study showed a relationship between the sensitivity of in vitro-irradiated peripheral blood lymphocytes and the risk of developing late toxic effects (Pinar et al., 2007). This study opens up the possibility of predicting normal tissue response to RT in individual patients.
Racial/Ethnic Differences in RT-Induced Radiation-Induced Skin Reactions In a study of prognostic significance of race in breast cancer patients treated with lumpectomy and RT, African-American patients fared more poorly than white patients with respect to overall cosmetic outcome and all specific EASRs, such as edema, fibrosis, and

Amendment 2: 11/23/2011 15 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
pigmentation (Ryan et al., 2007). There are racial/ethnic differences in the distribution of cell cycle and DNA repair mutations and polymorphisms, which may contribute to higher risk for EASRs in African Americans and underserved minority populations. For example, there were racial/ethnic differences in RT-induced EASRs in ataxia-telangiectasia (ATM) sequence variant carriers: 17% Hispanics, 23% African Americans, and 8% Whites, respectively (Ho et al., 2007). However, their sample size was quite small (n=131). Physical Activity Physical activity has been associated with increased general quality of life, physical functioning, and lower fatigue levels among breast cancer patients receiving RT and/or other treatments. This is clinically significant as fatigue and low general quality of life increase distress, disrupt daily activities, and affect treatment outcomes. More importantly, physical activity, through its effect on adiposity, bioavailability of estrogens, and insulin sensitivity, has been associated with disease progression. Therefore, there is a critical need to evaluate rates of physical activity during cancer treatment as well as effects of physical activity on clinical outcomes, treatment completion rates, and response to treatment, disease biomarkers, and quality of life. This is particularly critical for breast cancer patients receiving RT, an understudied population.
Tobacco Smoking Exposure Assessment Exposure to tobacco smoke, particularly secondhand smoke (SHS), is not easily quantified. Questionnaires that assess exposure have been the primary tool used in epidemiologic studies of SHS and disease (Cummings et al., 1989; 1990). The recent data from the 1999-2002 National Health and Nutrition Examination Survey showed that among non-smoking adults living in counties with extensive smoke-free law coverage, 12.5% were exposed to SHS, compared with 35% with limited coverage, and 46% with no law (Pickett et al., 2006). Biomarkers also are used for assessing SHS exposure, these include cotinine and tobacco-specific nitrosamines, and polycyclic aromatic hydrocarbon (PAH)-DNA adducts (Hecht, 2004). Cotinine, the primary proximate metabolite of nicotine, has been used as a preferred marker for tobacco smoke over nicotine partly because it has longer half-life than that of nicotine (Jarvis et al. 1988; Benowitz, 1996). Each of these approaches has strengths and limitations, and preference will depend on the research questions. While it is very likely that cotinine measurements may provide a valid and quantitative measure of average human SHS exposure over time, we will assess recent and current SHS exposures using urine to measure cotinine level. In urine, cotinine values between 11 ng/mL and 30 ng/mL may be associated with light smoking or secondhand smoking exposure, and levels in active smokers typically reach 500 ng/mL or more. We will use urine cotinine level >10 ng/mL in non-smoker as an indicator of secondhand smoking exposure.
Active Smoking and/or SHS Exposures in RT-Adverse Response and Survival Active, passive, or environmental tobacco smoke contains numerous human carcinogens for which the 2006 US Surgeon General's report concluded there is no safe level of exposure. Some of the mammary carcinogens in tobacco smoke include: (1) aromatic hydrocarbons; (2) nitrosamines; (3) aliphatic compounds; (4) arylamines and nitrarenes (International Agency for Research on Cancer). These carcinogens can be activated into electrophilic intermediates by drug metabolism enzymes in the human breast epithelial cells. In breast cancer patients, it is not clear whether smoking history or status impacts survival. For example, in one study, smokers are not only more likely to die of other diseases, but also have a higher mortality from breast cancer. The best prognosis, however, was found in those who had given up smoking (Fentiman et al., 2005). In a second study, a history of smoking increased mortality following diagnosis with breast cancer, but did not increase mortality from breast cancer (Holmes et al., 2007). However,

Amendment 2: 11/23/2011 16 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
another study suggested that smokers who are postmenopausal or obese at diagnosis may have higher mortality (Sagiv et al., 2007). In the cell culture system, cigarette smoke condensate (CSC) induced transformation of normal human breast epithelial cells (Narayan et al., 2004) and inhibits long-patch BER (Kundu et al., 2006). Many carcinogenic compounds are present in side-stream smoke that are 2-6 times more toxic than mainstream smoke (Schick and Glantz, 2005a; 2005b). Furthermore, cigarette smoke also impacts structure and function of fibroblasts that are critical for tissue repair and remodeling (Wong et al., 2004). Therefore, we hypothesize that cigarette smoke exposure lowers plasma total antioxidants, increases oxidative DNA damage, and lowers DNA repair which contributes to higher risk for RT adverse response in normal tissue.
Active and/or Secondhand Smoking (SHS) Exposures and Antioxidant/Oxidant Balance
For current smoking exposures, cotinine and tobacco-specific nitrosamines, and polycyclic aromatic hydrocarbon (PAH)-DNA adducts have been studied (Hecht, 2004). Cotinine, the primary proximate metabolite of nicotine, has been used as a preferred marker for tobacco smoke over nicotine partly because it has longer half-life than that of nicotine (Benowitz, 1996; Jarvis et al. 1988). In general, smokers had lower intakes of vitamins, fruits and vegetables, higher consumption of alcohol, lower physical activity and lower total serum antioxidant, measured by the oxygen radical absorbance capacity (ORAC) assay, than non-smokers (Kanaya et al., 2004; Ueda et al., 2004). In addition, nearly half of nonsmoking Americans are still regularly exposed to cigarette smoke. The question of how to protect subjects with smoking exposure from developing adverse responses to breast cancer RT has not been addressed. Based on the observations that tobacco smoking exposure contributes to higher oxidative DNA damage (Lodovici et al., 2005), we will test the hypothesis that higher current smoking exposure may lead to decreased total antioxidants, oxidative stress, and increased adverse response in breast cancer patients treated with RT.
Clinical Outcome Measures Women undergoing breast conserving surgery followed by whole breast radiotherapy have generally reported adequate quality of life. We plan to focus much of our efforts of this clinical study on broadly assessing the impact of radiotherapy on the lives of breast cancer survivors. We plan to use several metrics to make an assessment across a variety of domains. The Breast Cancer Treatment Outcomes Scale (BCTOS) is a validated instrument which has been used to assess three subscales including cosmetic status, functional status, and breast specific pain.(Stanton el al; Krishnan et al.) This validated scale was assessed in 185 women who underwent BCT and radiotherapy for Stage 0-II disease with 3 months to 18 years of follow-up. The BCTOS produced a factor structure with three internally consistent subscales (i.e., cosmetic status, functional status, and breast specific pain) that demonstrated predictive validity. With patient age, diagnosis duration, and other BCTOS subscales controlled, greater breast specific pain predicted greater depressive symptoms (P < 0.01) and lower QOL related to mental health (P < 0.05) and physical health (P < 0.05). Cosmetic status predicted QOL related to physical health (P < 0.05). The relations of breast specific pain with QOL indicators varied somewhat as a function of diagnosis duration. The BCTOS has been embedded into the currently ongoing NSABP B39 / RTOG 0413 trial as a portion of the larger quality of life metric used on that trial. In addition, it is the metric currently being used on the RTOG 1005 clinical trial which is assessing two different whole breast radiotherapy fractionation techniques. We plan to use the BCTOS/B39 metric and correlate the outcomes measured with more general

Amendment 2: 11/23/2011 17 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
physical functioning as assessed by the Functional Asssessment of Cancer Therapy – Breast (FACT-B) scale which has been selected to provide additional information regarding social, emotional and general functional endpoints. With the planned accrual goals across different racial/ethinc groups we hope to have enough data to look at differences in these patient reported outcomes across various populations. The FACT-B is a 44 item instrument which is comprised of nine items specific to quality of life in breast cancer patients that has been coupled to the more general FACT-G scale. The scale has been validated across a number of languages, is written at a sixth grade reading level, and takes approximately 10 minutes to complete. (Brady et al) We plan to compare outcomes reported in this metric with the more detailed breast cancer specific metrics in the BCTOS/B39 scale, across racial and ethnic groups as separated in this study, and with the acute measures of skin toxity measured per the Skindex 16 and the Acute Radiation Induced Skin Reaction Score. The Acute Radiation Induced Skin Reaction score is a metric we have shortened from the metric used on the RTOG 9713 trial to focus on the most likely range of skin reactions that patients will experience during radiotherapy. It is a six point metric to allow for a greater discrimination of skin reactions than would be otherwise obtained with the NCI CTCAE criteria. The Skindex 16 is a single page instrument which has been validated to accurately and sensitively measure how much patients are bothered by their skin conditions.(Chren MM et al.) This is a metric that has been validated in dermatologic practice and dovetails nicely with our study which is attempting to measure the impact of radiation induced skin reactions on patients. The Skindex-16 in particular was designed to assess the degree of bother a patient is experiencing rather than frequency.
2.2 Rationale
2.2.1 Introduction Breast cancer is the most frequently diagnosed cancer and the second leading cause of cancer death in American women. Breast conserving surgery and postoperative adjuvant radiotherapy becomes a common option in the management of early-stage breast cancer. Although well tolerated by most patients, about 30% of RT patients develop a Grade 2 or worse early adverse skin reactions (EASRs) as a result of RT. This is substantiated by the Canadian randomized trial comparing breast IMRT to standard field design in which 31 versus 48% of patient experienced moist desquamation as defined by the NCI CTC version 2. (Pignol et al 2008). Other studies have shown similar findings. For example, Chen et al in a Taiwanese population using what they describe as the “RTOG scale” found 23% of the sudy population having moist desquamation, 26% for patients who underwent chest wall irradiation and 19% for those that received whole breast irradiation. (Chen et al 2010) They described grade 2 skin toxicity as tender or bright erythema, patchy moist desquamation / moderate erythema, and Grade 3 skin toxicity as confluent moist desquamation other than skin fold, pitting edema. Both were included in their assessment of those who experienced toxicity. This description of skin toxicity (grade 2 or 3) is an apt summary of what we will classify in general as an “Early Adverse Skin Reaction” (EASR). Patients with severe EASRs may miss one or more radiotherapy days and thus create a "treatment break” which usually results in incomplete tumor cell killing and may lead to a greater chance of local recurrence and worse survival. The results from previous studies suggest that African-American women and underserved populations are less likely than Whites to receive the recommended adjuvant RT and have higher risk for developing radiation-induced skin toxicities. Therefore, the primary objective of the proposed research is to develop and validate prediction biomarkers for RT-induced acute and chronic skin reactions and quality of life in five racial/ethnic groups of breast cancer patients, Whites, Black/African

Amendment 2: 11/23/2011 18 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Americans (AA), Hispanic/Latinos, Asians/Native Hawaiians/Pacific Islanders, and American Indians/Alaskan Natives. We will test the working hypothesis that RT-induced skin reactions occur more frequently in individuals with: (1) elevated DNA damage and radio sensitivity, (2) mutations and genetic polymorphisms in cell cycle checkpoints and DNA repair genes, and (3) environmental factors, such as active and secondhand smoking exposure. As we learn more about the contributions of, and interactions among genetic susceptibility and environmental risk factors to adverse response, we can develop targeted preventive strategies for those recognized to be at higher risk. The outcome from this research will provide insight into the roles of genetic susceptibility in acute and chronic RT-induced skin reactions at the individual level. As we learn more about the contributions of and interactions among genetic susceptibility to more severe skin reactions, we can develop targeted preventive strategies for those predicted to be at higher risk.
Gender and Ethnicity In 2007, about 19,010 new breast cancer cases are expected to be diagnosed among African-American (AA) women (27% cancer cases among women), and 5,830 (19%) will die of this malignancy (Jemal et al., 2007). The five-year relative survival rates are 90% and 77% for non-Hispanic White (NHW) and AA women, respectively (Jemal et al., 2007). This difference can be attributed to both later stage at detection and poorer stage-specific survival. The reasons for this survival differential have been studied extensively. Poorer outcomes among AA women persist even after accounting for socioeconomic status. Unequal receipt of prompt, high-quality treatment persisted for AA women compared to NHW. For example, using the data from 1992 through 2002 in 12 geographic areas of the National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) tumor registries, African-American women were 24% less likely than Caucasians to receive the recommended adjuvant RT (95% confidence interval: 1.18-1.32). Breast cancer is the most commonly diagnosed cancer among Hispanic/Latino women; an estimated 14,300 (34%) of these women are expected to be diagnosed and an estimated 1,740 (16%) deaths will occur from breast cancer in 2006 (Cancer Facts and Figures for Hispanics, American Cancer Society, 2006). Breast cancer is less likely to be diagnosed at the earliest stage in Hispanic/Lation women. There is also evidence that aggressive tumor characteristics, such as triple-negative tumors, are more common in AA women than non-Hispanic white women (21% vs 10%) (Morris et al., 2007). Furthermore, triple-negative breast cancers affect younger, Hispanic/Latino and non-Hispanic/Latino white women in areas of low socioeconomic status. The tumors diagnosed at later stage were more aggressive; these women had poorer survival regardless of stage. Additionally, AA women with late-stage triple-negative breast cancer had the poorest survival of any comparable group (Bauer et al., 2007).
3.0 SUMMARY OF STUDY PLAN
Laboratory Study Plan A total of 1000 breast cancer patients prior to RT will be recruited and consented. For genetic risk factors, we will target 21,877 nsSNP in 48 genes of four pathways with established functions in IR-damage signaling and repair. For radiosensitive phenotypes, we will test two functional assays for DNA damage and radio sensitivity in lymphocytes before and after RT. Importantly, we will also test whether cigarette smoke exposures influences total plasma antioxidants, increases basal DNA damage and radio sensitivity, and contributes to RT-induced adverse response, particularly in genetic susceptible subpopulations. From each patient, we will collect questionnaires, blood and urine samples before and after RT for
Amendment 2: 11/23/2011 19 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
genotyping, DNA damage and cell cycle assays, total antioxidant levels, urine cotinine to estimate cigarette smoke exposure, and quality of life. Whole blood (≈25 -30 ml) will be collected at baseline and end of RT). The tubes containing the whole blood will be sent at room temperature along with the urine sample, which will be sent frozen using a custom designed insulated shipper to the Research Base specimen core for further processing and storage. Some assays will be performed at the University of Miami (specimens will be batch shipped from Wake Forest in liquid nitrogen containers); other will be done at Wake Forest. Section 9 provides details of specimen handling, shipping, and processing.
Clinical Study Plan Once the radiation oncologist has determined the patient is a candidate for post-lumpectomy, - quadrantectomy, or –mastectomy RT, and the patient has given consent to proceed with the recommended RT, they will be approached for this study. RT typically begins 4 to 8 weeks after surgery or completion of chemotherapy. The most common targeted volume is the ipsilateral breast or chest wall, with or without the supraclavicular lymph nodes. Once the patient has consented to participate in the study, their baseline pre-RT assessments can be completed during the radiation treatment-planning process. RT to the post-lumpectomy or – quadrantectomy intact breast or chest wall, +/- regional nodes, will be given using standard opposed tangential fields alone or three-field technique using 2D, 3D conformal, or IMRT treatment planning approaches. Supine or prone positioning will be allowed. Patients treated with MammoSite® or any other form of brachytherapy will not be eligible. The total radiation dose must be at > 40Gy. Dose per fraction must be >1.8 Gy. Hypofractionated treatment regimens will be allowed as they are equivalent to standard fractionation regimens with regard to both efficacy and toxicity. Six, 10, or 18 MV photons will be allowed. Bolus will be allowed for post mastectomy patients if needed to increase the superficial dose. Boost treatments to the lumpectomy cavity or mastectomy scar will be allowed per the treating radiation oncologists discretion. Adjuvant hormonal therapy will be allowed prior to, during or after RT at the discretion of a medical oncologist (name/dose of agent to be recorded). However, no chemotherapy will be allowed concurrent with radiation, though it is permitted prior to or after radiotherapy. Patients are generally treated Monday through Friday, with weekends and holidays off, for approximately 3 - 6 weeks.
During the course of treatment, the patient sees the radiation oncologist in clinic every week to review the patient’s treatment chart, monitor treatment efficacy/ skin toxicity, and answer questions. Breaks in the treatment schedule should be avoided whenever possible, because delays can adversely affect efficacy, but breaks necessitated by RT skin toxicity or for other reasons will be recorded. Radiation oncologists typically see patients in follow-up on a periodic basis for up to one year to assess the patient for RT-induced skin and other toxicities that may have occurred. These assessments will also occur for study patients. Long-term follow-up care of these patients is provided by the radiation, medical, and/or surgical oncologist to monitor the patient for local and/or systemic recurrence as well as treatment toxicity.

Amendment 2: 11/23/2011 20 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
4.0 PARTICIPANT SELECTION
4.1 Inclusion Criteria
4.1.1 Female subjects newly diagnosed with breast carcinoma, stage 0–IIIA 4.1.2 Status post-lumpectomy, -quadrantectomy, or -mastectomy 4.1.3 Plan to receive adjuvant radiation to the whole breast or chest wall +/- regional
lymph nodes. 4.1.4 Total dose >40Gy 4.1.5 Dose per fraction >
4.1.6 Concurrent and sequential boost techniques are allowed for both standard and hypofractionated regimens.
1.8 use of 2D, 3D conformal, or IMRT treatment techniques allowed. Skin sparing IMRT patients excluded. A daily fraction of 2.7 Gy to the whole breast is suggested for hypofractionated regimens.
4.1.7 Adjuvant hormonal therapy will be allowed prior to, during and/or after RT at the discretion of a medical oncologist.
4.1.8 Targeted therapies such as Herceptin will be allowed prior to, during, and/or after RT at the discretion of the medical oncologist.
4.1.9 Patients who are willing to sign protocol consent form. 4.1.10 Patients who are > 18 years old. 4.1.11 Race/Ethnicity to include Whites, Black/African Americans (AA), Hispanic/Latinos,
Asians/Native Hawaiians/Pacific Islanders, and Native American or Alaskan.
4.2 Exclusion Criteria
4.2.1 No prior radiation to the involved breast or chest wall. 4.2.2 No concurrent chemotherapy.(Patients may receive chemotherapy prior to
radiation or following radiation at the treating physician’s discretion.) 4.2.3 Patients who underwent immediate breast reconstruction following mastectomy 4.2.4 Patients undergoing partial breast irradiation. 4.2.5 Patients who have undergone MammoSite® or any other form of brachytherapy 4.2.6 Sites that cannot send blood/urine specimens to Wake Forest by overnight (next day) express shipping. 4.2.7 Does not speak or read English.
4.3 Inclusion of Women and Minorities The study is only for females with breast cancer. Women who are Caucasian, African-American, Hispanic/Latino, Asian, Hawaiian Native or Pacific Islander, American Indian or Alaskan Native are eligible for this trial. Based on the different populations of patients accrued in the Research Base vs. University of Miami, project accrual by race/ethnicity is shown below for Research Base patients (first table), U Miami patients (second table). In total, 1000 patients, 400 White, 200 Black, 200 Hispanic/Latino, 100 Asian/Hawaiian Native/Pacific Islander, and 100 American Indian/Alaskan Native (third table). With the combined resources of the Research Base, including recruitment of additional CCOPs and MB CCOPs as well as opening the study to the CTSU, accrual goals should be met in a timely fashion.

Amendment 2: 11/23/2011 21 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
CCCWF CCOP Research Base Accrual
Race/Ethnicity
Gender White,
not of Hispanic
Origin
Black, not of
Hispanic Origin
Hispanic/
Latino
Asian, Hawaiian
Native or Pacific Islander
American Indian or Alaskan Native
Total
Male 0 0 0 0 0 0
Female 380 177 143 100 100 900 Total 380 177 143 100 100 900
University of Miami Accrual
Race/Ethnicity
Gender White, not of
Hispanic Origin
Black, not of
Hispanic Origin
Hispanic/
Latino
Asian, Hawaiian
Native or Pacific Islander
American Indian or Alaskan Native
Total
Male 0 0 0 0 0 0
Female 20 23 57 0 0 100
Total 20 23 57 0 0 100 Total Accrual
Race/Ethnicity
Gender White, not
of Hispanic
Origin
Black, not of
Hispanic Origin
Hispanic/
Latino
Asian, Hawaiian
Native or Pacific Islander
American Indian or Alaskan Native
Total
Male 0 0 0 0 0 0 Female 400 200 200 100 100 1000
Total 400 200 200 100 100 1000

Amendment 2: 11/23/2011 22 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
4.4 Recruitment and Retention Plan
Feasibility At the present time, the Comprehensive Cancer Center of Wake Forest CCOP Research Base is comprised 27 CCOPs, 2 non-CCOP Prevention members, and Wake Forest, for a total of 169 individual sites located in 25 states in the Midwest, Northeast, and Southeast United States. In the fall of 2010 we surveyed our participating sites to assess their interest in participating in the study. Interest was high among sites, with an estimated accrual of 90-130 patients per month. The Wake Forest Research Base has 5 Minority-Based CCOPs including Brooklyn MBCCOP (African American and Hispanic/Latino patients), LSU New Orleans and LSU Shreveport MBCCOP (African American patients), Georgia Health Sciences (African American patients), and Stroger Memorial MBCCOP (African American and Hispanic/Latino patients). In addition, our non-CCOP Prevention Member in Wilmington, NC has a large African American population. To enhance the likelihood of recruiting the minority populations required for the study, we plan to recruit several other CCOPs and MB CCOPs, including the Bay Area Tumor Institute (Asian and Pacific Islander, and Hispanic/Latino patients), Colorado Cancer Research Program CCOP (Hispanic/Latino patients), Mt. Sinai CCOP (African American and Hispanic/Latino patients),Cancer Research Center of Hawaii MB-CCOP, (Asian, Hawaiian Native, and Pacific Islander patients), University of New Mexico Cancer Center (a MB-CCOP), (Hispanic/Latino and American Indian patients), Queens Cancer Center MBCCOP (African American, Asian, and Hispanic/Latino patients), MeritCare Hospital North Dakota (American Indian patients), San Juan MB-CCOP (Hispanic/Latino patients), Sioux Community Cancer Consortium CCOP (American Indian patients), and Virginia Mason Research Center CCOP, and Northwest CCOP (Asian patients). Opening the study to the CTSU will help overall accrual as well as accrual of the four minority patient groups. If necessary, the study can be closed to certain racial/ethnic patient groups if accrual for that subpopulation is complete. We will concentrate our efforts to recruit minority patients, and recruitment will be discussed at each ESC meeting. After (no later than) one year, we will decide if recruitment is feasible separately for each minority group. If it is not feasible for a specific race-ethnicity (e.g., we have accrued less than half the anticipated number), we will stop accrual to that minority group and spread the extra accruals over the remaining groups. This will not be done lightly, and it is our intention to complete accrual for all race-ethnicities.
Recruitment:
At each site, specific recruitment plans may include the following according to the site’s institutional policy: screening clinic charts, tumor registry data, identify referral sources such as patient advocate groups, retirement communities, churches, support organizations, community organizations, newspapers, radio, patient recruitment posters and recruitment letters.
5. AGENT ADMINISTRATION – N/A 6. Registration/Randomization (CTSU participants refer to Appendix 17)
IRB letter of approval and an IRB approved consent form must be received by the Research Base Protocol Information Office – Attn: Site Coordinator prior to patient registration. Fax: (336) 716-6275 or email: [email protected].
Fill out, “Eligibility Checklist / Registration Form’. Use this to
complete the on-line registration.

Amendment 2: 11/23/2011 23 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Online Registration Log on to the CCCWF Research Base registration web site at https://ccrbis.phs.wfubmc.edu. Enter your user name and password (which may be obtained by contacting June Fletcher-Steede at [email protected]) In the ‘Patient Registration and Protocol Information’ table, click the ‘Register Patient/Patient Info’, with the corresponding protocol number found in the drop down box to the right. Fill in the eligibility criteria forms using the drop down boxes. Once the patient information has been entered online print a copy of the eligibility checklist/registration form for your records. Press the submit button, a confirmation page will appear. Print this confirmation sheet for your records.
The CCCWF On-line Protocol Registration/Eligibility form, initial flow sheet, signed consent, histology reports, scan reports and lab reports (as required in protocol) should be faxed to (336) 713-6476 or mailed to the Research Base Data Management Center:
Research Base Data Management Center
Department of Radiation Oncology 1st Floor Outpatient Comprehensive Cancer Center
Wake Forest Baptist Medical Center 1 Medical Center Boulevard Winston-Salem, NC 27157
These forms should be retained in the patient’s study file. These forms will be evaluated during an institutional NCI/CCCWF CCOP Research Base site member audit.
If you have questions related to the registration process or require assistance with registration, please contact the CCCWF CCOP Research Base DMC between 8:30am and 4:00pm EST, Monday through Friday at (336) 713-3172 or 713-6507.
7. CLINICAL EVALUATIONS AND PROCEDURES
7.1 Schedule of Events
Patients will complete the Baseline Breast Cancer Study Risk Questionnaire with the assistance of a research nurse or other clinical research professional. For breast cancer and skin-specific quality of life, the FACT-B, the B39 QOL Questionnaire, as well as a modification of the Skindex-16, a validated multi-domain instrument used in the dermatopathology literature (Chren et al, 2001), will also be required at baseline. Baseline blood and urine samples will be obtained and shipped to the Wake Forest Specimen Handling Core as outlined in Section 9 and Appendix16 . A baseline assessment for acute toxicity will be completed by research staff using the ONS Criteria for Radiation-Induced Acute Skin Toxicity as some patients may have some baseline erythema (grade 1 or 2 acute skin toxicity) as a residual effect from surgery. Baseline photographs of the breast or chest wall that will undergo RT (ipsilateral breast or chest wall) and the contralateral normal breast must be obtained as specified in the Instructions for Photographs (See Section 7.8 and Appendix 12). We suggest that the aforementioned baseline activities be conducted while the patient is undergoing RT treatment planning, which normally takes one to two weeks.

Amendment 2: 11/23/2011 24 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
General Overview– Once the patient has begun radiation therapy, patients receiving the standard 6 week fractionation regimen
will need an assessment for acute skin toxicity and photographs obtained by the research staff during week 3. This should be obtained as close to the midway point of treatment to the whole breast/chest wall (usually the 13th to 14th treatment) as possible.
As close to the last day of radiotherapy as possible including the boost treatments, the patient is to complete the FACT-B, Skindex-16, the B39 QOL Questionnaire, and the first page of the Follow-up Breast Cancer Study Risk Questionnaire. Blood/urine samples, acute skin toxicity assessment, photographs and the second page of the Follow-up Breast Cancer Study Risk Questionnaire and the ONS Criteria for Radiation-Induced Breast Cancer Acute Skin Toxicity will be obtained by the research staff. Research staff should submit the Breast/Chest Wall RT Completion Form. All patients will then be assessed at 1 month after completion of radiotherapy. The patient is to complete the FACT-B, Modified Skindex-16, the B39 QOL Questionnaire, and the first page of the Follow-up Breast Cancer Study Risk Questionnaire. Acute skin toxicity assessment, photographs and the second page of the Follow-up Breast Cancer Study Risk Questionnaire will be obtained by the research staff. All patients will be assessed at 2 months after completion of radiotherapy. An acute skin toxicity assessment and photographs will be repeated by the research staff.
The final assessments will be done at 6 months and 1 year with all patients, completing FACT-B, B39 QOL Questionnaire, Skindex-16, and the first page of the Follow-up Breast Cancer Study Risk Questionnaire. Chronic skin toxicity (RTOG SOMA Criteria for RT- Induced Breast/Chest Wall Late Skin Toxicity) and photographs will be obtained by the research staff. The radiation treatment approach to the intact whole breast following lumpectomy or quadrantectomy, or chest wall following mastectomy, with or without treatment to the regional nodes, will be at the discretion of the radiation oncologist and will not be specified by the protocol other than the total radiation dose must be at > 40Gy, and dose per fraction must be at > 1.8 Gy.
7.2 Baseline Testing (All patients)
• Baseline Breast Cancer Risk Study Questionnaire (Appendix 7) • FACT-B (Appendix 15) • Modified Skindex-16 (Appendix 9) • B39 QOL Questionnaire (Appendix 10A Intact Breast) OR • Blood and urine samples (see Section 9.0 and Appendix 16)
(Appendix 10B Chest Wall)
• ONS Criteria for Acute Radiation-Induced Skin Reaction (Appendix 14) • Photographs (prior to start of RT) (Appendix 12) • Data Submission Checklist (Appendix 1) • Flow Sheet/ Addenda (Appendix 18)
Amendment 2: 11/23/2011 25 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
7.3 Week 3 Evaluation (
6 week fractionated regimen only)
• ONS Criteria for Acute Radiation-Induced Skin Toxicity (Appendix 14) • Photographs (Appendix 12) This should be obtained as close to the midway point of
treatment to the whole breast/chest wall (usually the 13th to 14th treatment) as possible. • Data Submission Checklist (Appendix 1) • Flow Sheet/ Addenda (Appendix 18)
7.4 Last day of radiotherapy evaluation (All patients)
• Follow-Up Breast Cancer Study Risk Questionnaire (Appendix 8) • FACT-B (Appendix 15) • Modified Skindex-16 (Appendix 9) • B39 QOL Questionnaire (Appendix 10A Intact Breast) OR • Blood and urine samples (see Section 9.0 and Appendix 16)
(Appendix 10B Chest Wall)
• ONS Criteria for Acute Radiation-Induced Skin Reaction (Appendix 14) • Photographs (+/- 2 days) (Appendix 12) • Breast/Chest Wall RT Completion Form (Appendix 13) • Data Submission Checklist (Appendix 1) • Flow Sheet/ Addenda (Appendix 18)
7.5 Month 1 post radiotherapy evaluation (+/- 7 days)
• FACT-B (Appendix 15) • Modified Skindex-16 (Appendix 9) • B39 QOL Questionnaire (Appendix 10A Intact Breast) (Appendix 10B Chest Wall) • Follow-Up Breast Cancer Study Risk Questionnaire (Appendix 8) • ONS Criteria for Acute Radiation-Induced Skin Reaction (Appendix 14) • Photographs (+/- 7 days) (Appendix 12) • Data Submission Checklist (Appendix 1) • Flow Sheet/ Addenda (Appendix 18)
7.6 Month 2 post radiotherapy evaluation (+/- 7 days)
• ONS Criteria for Acute Radiation-Induced Skin Reaction (Appendix 14) • Photographs (+/- 7 days) (Appendix 12) • Data Submission Checklist (Appendix 1) • Flow Sheet/ Addenda (Appendix 18)
7.7 6 month and 1 year evaluation (+/- 4 weeks)
• FACT-B (Appendix 15) • Skindex-16 (Appendix 9)

Amendment 2: 11/23/2011 26 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
• B39 QOL and functioning metric (Appendix 10A Intact Breast) (Appendix 10B Chest Wall)
• Follow-Up Breast Cancer Study Risk Questionnaire (Appendix 8) • RTOG SOMA Criteria for RT-Induced Breast/Chest Wall Late Skin Toxicity (Appendix
11) • Photographs (Appendix 12) • Data Submission Checklist (Appendix 1) • Flow Sheet/ Addenda (Appendix 18)
7.8 Instructions for Photographs: (CTSU Sites Exempt)
Sites should test their cameras and downloading capabilities prior to enrolling their first patient. Only jpeg images taken with a digital camera will be accepted. Pictures taken with cameras on phones are not allowed. Photographs are optional for sites without digital cameras or downloading capabilities, which should be documented on the Flow Sheet/Addenda page (Appendix 18). Photographs should only be taken as agreed upon by the patient in the informed consent.
Photographs will be taken at: • Baseline (May be taken after consent, but prior to the start of radiation therapy.) • Week 3 (standard fractionated regimen only) photographs
• Last day of radiotherapy (+/- 2 days)
should be obtained as close to the midway point of treatment to the whole breast/chest wall (usually the 13th to 14th treatment) as possible.
• 1 month post radiotherapy (+/- 7 days) • 2 months post radiotherapy (+/- 7 days) • 6 months post radiotherapy (+/- 1 month) • 12 months post radiotherapy (+/- 1 month)
o Photographs must be taken within the time period listed above (including
weekends and holidays) to be valid. Photographs should not be taken if outside the specified window of time.
o Patients should be labeled in each image by the identifier explained in number 3 below. (Ie. 97609001BC) Patient initials are also acceptable if PID is not yet available.
o Images should be uploaded after each visit in a timely manner. o If images are lost, inadvertently deleted, missing, etc, please make a note on the
addendum sheet (Appendix 18) documenting the reason.
To upload images:
1. Visit the CCCWF CCOP Research Base website (www.wakehealth.edu/cancer/researchbase) and click on “Member Area” and select “Patient Registration” to enter CCRBIS.
2. In CCRBIS, click on ‘Information’ and find “Upload Image.” Those registered patients who belong to site’s MD group and gave consent to take their photos will be listed on the dropdown list. Select the PID, which will bring up another page.

Amendment 2: 11/23/2011 27 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
3. Select from the drop down menu for the appropriate PID, visit number and view. For example, patient 97609001 at her Baseline visit with the ‘C’ view would be labeled 97609001BC. Subsequent items will be labeled: Week 3 (W3), Last Day (LD), Month 1 (M1), Month 2 (M2), Month 6 (M6), Month 12 (M12)
4. Click “Browse” to select the JPG image from your image pool. After clicking “Open,” the selected picture address will be inserted in the “Source” field. If you made a wrong choice, just use “Browse” again to select the correct one.
5. Upload only one image per menu selection. Once an image is uploaded, that dropdown menu item will no longer appear. Some menu items will not be used depending on if the patient has intact breasts or is post mastectomy. Images will be transferred to a secure server at WF once the upload is complete.
6. Images should be deleted from sites’ servers once files have been uploaded in CCRBIS. 7. If you made any mistake please call our data management personnel ASAP. Please do
not try to correct it or re-upload it by yourself. 8. If images are lost, inadvertently deleted, missing, etc, please make a note on the
addendum sheet (Appendix 18) documenting the reason. Examples of images and further instructions are located on Appendix 12, Instructions for Photographs.

Amendment 2: 11/23/2011 28 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
7.9 Study Parameters Table
Baseline evaluations are to be conducted within 4 weeks prior to registration. Protocol therapy must begin within 4 weeks of registration.
Evaluation/Procedure Baseline Week 3E Last Day RT
1 months post RT
2 months post RT
6 months post RT
12 months post RT
Informed Consent x
Height and Weight x
Baseline Breast Cancer Study Risk Questionnaire (C)(D) x
F/U Breast Cancer Study Risk Questionnaire (C)(D) x x x x
Skindex-16 (D) x x x x x
B39 QOL (D) Two forms, use applicable one (F) Post Lumpectomy Intact Breast
Post- Mastectomy Chest Wall or
x x x x x
Urine samples (B) x x
Blood samples (B) x x
ONS Acute Skin Reaction (C) x x x x x
Photographs (Appendix 12) (A) (C) x x x x x x x
FACT-B (D) x x x x x
RTOG SOMA Criteria for RT-Induced Breast/Chest Wall Late Skin Toxicity (C) x x
Breast/Chest Wall RT Completion Form (C) x
Data Submission Checklist/ Flow Sheet/ Addenda (C) x x x x x x x
A) Patient may choose to not have photographs taken. Patients must sign permission for acceptance or refusal for photographs to be taken on consent form. CTSU sites are exempt from taking photographs.
B) Baseline Blood/Urine Biomarkers must be obtained prior to start of RT. Specimens must be collected Mondays, Tuesdays, Wednesdays or Thursdays and shipped to Wake Forest the same day collected. Pre-printed label identification (Spl # = RT __) must be entered on Specimen Shipping Form and entered into CCRBIS
C) The following forms are to be completed by research staff: ONS Acute Radiation-Induced Skin Toxicity, Photographs, RTOG SOMA Criteria for RT-Induced Breast/Chest Wall Late Skin Toxicity, the second page of the Follow-up Breast Cancer Study Risk Questionnaire, Breast/Chest Wall RT Completion Form, Data Submission Checklist, and Flow Sheet/Addenda
D) The following forms will be completed by the patient: FACT-B, B39 QOL Questionnaire, Baseline Breast Cancer Study Risk Questionnaire, Skindex 16, and the first page of the Follow-up Breast Cancer Study Risk Questionnaire.
E) Week 3 evaluation (standard fractionated regimen only) should be obtained as close to the midway point of treatment to the whole breast/chest wall (usually the 13th to 14th treatment) as possible.
F) B39 QOL Questionnaire is comprised of two forms. One form is Post Lumpectomy Intact Breast, the other Post Mastectomy Chest Wall. Patient is to complete only the form that is applicable.

Amendment 2: 11/23/2011 29 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
7.10 Off Study Criteria
Participants may go ‘off-study’ for the following reasons: the protocol has been completed, adverse event, serious adverse event, lost to follow-up, non-compliance, concurrent chemotherapy use, medical contraindication, withdraw consent, or death. The reason(s) the patient goes ‘off-study’ should be recorded.
8.0 Protocol Specific Training Requirements – N/A 9.0 Specimen Management
9.1 Collection and Handling Procedures – CCOP Research Base Participants (non-Wake
Forest) IMPORTANT NOTE: Specimens must be collected only on Mondays, Tuesdays,
Wednesdays or Thursdays and shipped to Wake Forest on the same day collected. Do not centrifuge samples.
See Appendix 16
for detailed instructions for Specimen Collection and Shipping
9.2 Shipping Instructions
Initial Shipping Kits: Sites should request shipping kits at the time of study approval in advance of putting patients on study and should use the Specimen Kit Request Form found on page 1 of Appendix 16. This form should be faxed to the Protocol Information Office at (336) 716-6275, attn: Gina Enevold along with the site IRB study approval letter. Additional Shipping Kits: If additional kits are needed, sites should contact Ms. Gulya Kourman, the technician responsible for specimen shipping and handling, at the email address below or fax additional Specimen Kit Request Forms. The contact information for the Dr. Lively’s laboratory is:
Breast Cancer Biomarker Study c/o Ms. Gulya Kourman/Lively Lab Structural Biology Center, BGTC Wake Forest School of Medicine
Medical Center Blvd. Winston-Salem, NC 27157
Phone: (336) 716-2581 Fax: (336) 777-3242
Email: [email protected]
9.3 Overview of Assays
Blood and urine specimens received by Dr. Mark Lively’s laboratory will be cataloged, processed, duplicated, and stored, eventually being sent to the laboratories of Drs. Jennifer Hu (U Miami) and Zheng Cui (Wake Forest) for testing. The various assays are described
Amendment 2: 11/23/2011 30 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
below. The laboratory assay data files from U Miami and WF will be merged into the main Research Base database using patients’ Research Base study identification number. A specific quality-control program for molecular epidemiological studies has been developed in Dr. Hu’s laboratory and will be used at both the U Miami and WF laboratories. Several approaches will be applied to ensure quality of the data output: (1) two external controls will be included for each batch of samples (for assessing reproducibility or batch-to-batch variability); (2) laboratory assays will always be performed with coded samples; (3) samples from pre- and post-RT will be collected and processed concurrently; (4) each genotype assay will be repeated at least twice; and (5) the functional repair assay will be conducted in triplicates following Good Laboratory Practice (GLP) guidelines. Triplicate samples with greater than a 30% intra-sample coefficient of variation (CV) will be reanalyzed or excluded from the final data analysis. Data sharing between the U of Miami and Wake Forest will occur per the signed Data Use Agreement between the two institutions. Data shared between institutions will be done through secure electronic means and de-identified as it relates to patient identification such as name, address, contact information, and medical record numbers.
9.3.1 SNPs Genotyping
The BeadArray System (Illumina Inc., San Diego, CA) will be used for high-throughput genotyping of the final custom panel. Quality control/assurance will include (1) 4 internal controls in each plate, and (2) the Hardy-Weinberg Equilibrium (HWE) test will be used to identify potentially problematic SNPs.
9.3.2 DNA Damage – Comet Assay
Dr. Jennifer Hu’s lab has used the alkaline comet assay routinely for molecular epidemiology studies (Smith et al., 2003a; Lockett et al., 2006). In brief, the quick-thawed lymphocytes with greater than 95% viability will be suspended in low-melting-point agarose gel, layered onto the comet slide, and treated with 3 Gy γ-ray using a 137Cs Gammacell 40 irradiator (Nordion, Ottawa, ON, Canada) to generate single-strand breaks. Cells will be lysed with a high-salt and detergent solution at pH 10 for alkaline lysis and followed by DNA unwinding and electrophoresis. Following electrophoresis, the slides will be removed, fixed in ethanol, dried, and stained with SYBR Green. For each study subject, we will collect data on basal and IR-induced DNA damage. For quantitation, the comet tail moment of 100 cells will be analyzed using the LAI Automated Comet Assay Analysis System (Loats Associates, Inc., Westminster, MD). The results will be presented as the average tail moment, defined as the product of the percentage of DNA in the comet tail and the distance between the means of the head and tail distributions.
9.3.3 H2AX Phosphorylation Assay
Cryopreserved lymphocytes with >90% viability will be used for the flow-cytometry-based assay of basal and IR-induced γ-H2AX (9 Gy) as described previously (Muslimovic et al., 2008). In brief, 30 minutes after irradiation, cells will be treated with 0.2% IGEPAL 630 (NP-40) on ice in the dark for one hour to block non-specific binding sites, then incubated with fluorescein isothiocyanate (FITC)-labeled anti-γ-H2AX antibody (#16-202A; www.millipore.com), to stain for gamma-H2AX and propidium iodide to stain DNA content. After one-hour incubation in the dark, which is done on ice to prevent phosphatase action, the nuclei will be analyzed directly in a flow cytometer using FITC channel to detect γ-H2AX and the violet channel for DNA content. Dual staining for γ-H2AX and DNA content allows measurement of γ-H2AX signal in different cell cycle stages and allows gating so that signal from degraded nuclei and debris can be omitted. The method specifically measures γ-H2AX, as lower signal was obtained in irradiated lmphoblastoid cells from patients with ataxia

Amendment 2: 11/23/2011 31 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
telangiectasia (AT). The γ-H2AX signal increases linearly in the dose range from 1 to 20 Gy of irradiation. As most radiotherapy regimens use 2–5 Gy radiation doses, the method will also have application as a measure of DSB induction in patients undergoing radiotherapy. Data will be exported to SAS software packages for further statistical analysis.
9.3.4 Cell-Cycle G2 Delay Assay
The PI’s lab has developed and validated the cell-cycle G2 delay assay for molecular epidemiology studies (Hu et al., 2001; 2002). In brief, the quick-thawed lymphocytes with greater than 95% viability will be incubated in RPMI medium with 20 μg/ml phytohemagglutinin for 72 hours. Using a 137Cs Gammacell 40 irradiator (Nordion, Ottawa, ON, Canada), the cells will be exposed to 3 Gy γ-irradiation. Cells with or without (as control) irradiation will be harvested 24 hours later, and the percentages of cells in the G0/G1, G2/M, and S phase of the cell cycle will be determined by using a Becton Dickinson dual laser fluorescence activated cell sorter (FACS) as described previously (Hu et al., 2001; 2002). The mitotic delay index will be calculated as (% of cells in G2/M with IR exposure - % of control cells in G2/M) / (% of control cells in S phase) x 100%.
9.3.5 Urine Cotinine Measurement The urine cotinine level will be measured by the Brunswick Laboratories using the method as described previously (Bernert et al. 1997, 2000). Briefly, duplicate plasma samples will be equilibrated with a trideuterated cotinine internal standard and then extracted using ChemElute columns, concentrated, and analyzed by LC/MS/MS. The assay will be performed under Good Laboratory Practices (GLP, 21 CFR Part 58) guidelines.
9.3.6 Oxygen Radical Absorbance Capacity (ORAC) Assay
The ORAC method is the only method that takes total antioxidants into a single quantity. The high-throughput ORAC assay, developed in our consultant’s, Dr. Ou’s lab, will be used to estimate total plasma antioxidant level (Huang et al., 2002). First, 2,2'-azobis(2-amidinopropane) dihydrochloride will be mixed with fluorescein and standards (Trolox for peroxyl radicals and gallic acid for hydroxyl radicals) or plasma and incubated in a dual-scanning spectrofluorometer (GEMINI SpectraMAX; Molecular Devices). The fluorescence decay will be monitored for 70 min (excitation, 546 nm; emission, 565 nm). The ORAC values will be calculated using the areas under the curves with the SOFTmax PRO (Molecular Devices) and expressed as micromole standard per liter. The assay will be performed under Good Laboratory Practices (GLP, 21 CFR Part 58) guidelines.
9.3.7 Urine 8-hydroxy-2'-deoxyguanosine (8-OHdG) Assay Urinary 8-OHdG is considered to be a biomarker of cellular oxidative stress and to be associated with exposures to carcinogens (Yamazaki et al., 2005). To estimate the oxidative stress caused by radiotherapy, we will monitor urinary 8-OHdG levels in patients before and after RT using the OxiSelect™ Oxidative DNA Damage ELISA Kit (Cell Biolabs, Inc.).
9.3.8 Inflammatory Immune Response Biomarkers The results from a recent study suggest that inflammatory processes may be associated with fatigue symptoms during RT for breast cancer (Bower et al., 2009). We also hypothesize that lower levels of adiponectin, among obese patients will have higher risk of EASRs and worse quality of life, particularly in underserved minority

Amendment 2: 11/23/2011 32 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
patients. Irradiation may modulate the levels of C-reactive protein and adiponectin related to inflammation as suggested by a previous study (Bower et al., 2009; Blakely et al., 2010; Chow et al., 2010). Therefore, we will also measure plasma levels of C-reactive protein and adiponectin in patients before and after RT. Plasma C-reactive protein will be measured by using an ELISA kit (GenWay Biotech, Inc., San Diego, CA). Plasma adiponectin will be measured using the ELISA kit (B-Bridge International, Inc. Mountain View, CA).
9.3.9 Tumor Killing Activity
When the anti-tumor response was examined, leukocytes of the innate immune system, including neutrophils, macrophages and NK cells, infiltrated the tumor site for a multipronged killing response. Each cell type had independent killing activity against the cancer cells. A second aspect of this multipronged response was that cancer cells could be killed either via necrosis in vivo or via apoptosis by purified macrophages. We hypothesize that higher tumor killing activity is associated with better immune response and clinical outcome. The cytolytic destruction of cancer cells by innate leukocytes will be measured by Dr. Zheng Cui’s laboratory at Wake Forest (Cui et al., 2003; Hicks et al, 2006).
9.3.10 Laboratory Assay Quality Assurance/Control
Several approaches will be applied to ensure assay quality: (1) two external controls will be included for each batch of samples (for assessing reproducibility or batch-to-batch variability); (2) laboratory assays will always be performed with coded samples; (3) samples from pre- and post-RT will be collected and processed concurrently; and (4) the functional repair assay will be conducted in triplicates following Good Laboratory Practice (GLP) guidelines.
10. REPORTING SERIOUS ADVERSE EVENTS
DEFINITION: ICH Guideline E2A and Fed. Reg. 62, Oct. 7, 1997 define serious adverse events as those events, occurring at any dose, which meet any of the following criteria: Results in death; is life threatening (Note: the term life-threatening refers to an event in which the patient was at risk of death at the time of the event; it does not refer to an event which hypothetically might have caused death if it were more severe).
• Requires inpatient hospitalization or prolongation of existing hospitalization • Results in persistent or significant disability/incapacity • Is a congenital abnormality/birth defect • Events that may not meet these criteria, but which the investigator finds very unusual
and/or potentially serious, will also be reported in the same manner.
10.1 Adverse Events 10.1.1 Reportable Adverse Events
Since this study is not a treatment study but is a study that includes longitudinal follow-up of study participants for acute and chronic skin toxicity, adverse events will not be reported. Only serious adverse events Grade 4 and Grade 5 will be reported using the MedWatch form as instructed in section 10.2.
10.2 Reporting Serious Adverse Events
In order to assure complete and timely reporting of adverse events and toxicity, the following general guidelines are to be observed. When protocol-specific guidelines

Amendment 2: 11/23/2011 33 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
indicate more intense monitoring than the standard guidelines, the study-specific reporting procedures supersede the General Guidelines. Serious Adverse Event reporting begins after the patient is registered to the study (or begins the run-in period of the study or begins the wash out period of the study). Serious Adverse Events occurring within 30 days of study completion must be reported via FDA Form 3500 (MedWatch).
1. The protocol Principal Investigator will report to the RB Data Management Staff
within 24 hours of discovering the details of all unexpected severe, life-threatening (grade 4) and fatal adverse events (grade 5) regardless of attribution.
2. All deaths during protocol treatment or within 30 days of completion or termination
of protocol treatment regardless of attribution require notification within 24 hours of discovery.
3. Any expected or unexpected Grade 4 or Grade 5 medical event which precipitates
hospitalization or prolongation of existing hospitalization must be reported regardless of attribution.
4. A written report, including all relevant clinical information and all data collection
forms due up to and including the date of the event will be sent by mail or FAX to the RB DMC within 10 calendar days unless specified otherwise within the protocol. The material must be labeled:
Attention: Adverse Event Reporting
Research Base Data Management Center Department of Radiation Oncology
1st Floor Cancer Center WFBH
Medical Center Boulevard Winston-Salem, NC 27157
5. The Research Base Grant PI, Safety and Toxicity Review Committee and/or Study
Chair will take appropriate action to inform the membership and statistical personnel of any protocol modifications and/or precautionary measures, if this is warranted.
6. Serious adverse events will be communicated by phone and MedWatch as soon as
identified to the CCCWF Research Base Data Management Center (DMC) at (336) 713-3172. The DMC is responsible for communicating with the FDA, the drug sponsor, WF IRB, and other regulatory agencies, as well as reporting all SAE’s grade 4 or 5 to the Safety and Toxicity Review Committee (STRC).
7. Institutions must comply with their individual Institutional Review Board (IRB) policy
regarding submission of documentation of adverse events. All MedWatch reports should be sent to the local IRB in accordance with the local IRB policies.
8. When submitting SAE reports and supporting documentation, the study number and
the case number (PID #) must be recorded on the FDA Form 3500 (Mandatory MedWatch) so that the case may be associated with the appropriate study file.
10.2.1 Follow-up of SAE

Amendment 2: 11/23/2011 34 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Site staff should send follow-up reports as requested when additional information is available. Additional information should be entered on the MedWatch form in the appropriate format. Follow-up information should be sent to the RB Data Management Center as soon as available. SAEs for this protocol should be followed until resolved.
11. STUDY MONITORING 11.1 Data Management Schedule
The Eligibility checklist/Registration Form should be completed on-line. Data forms will be submitted to the CCCWF CCOP Research Base. See Section 6.0 for mailing address, or fax to (336) 713-6476 according to the timetable below:
Form Submission Schedule Eligibility Checklist, Informed Consent Baseline Baseline Breast Cancer Study Risk Questionnaire Baseline F/U Breast Cancer Study Risk Questionnaire Last day RT, Month 1, 6 and 12 post RT Skindex-16 QOL Questionnaire Baseline, Last day RT, Month 1, 6,and 12 post RT B39 QOL Questionnaire Baseline, Last day RT, Month 1, 6 and 12 post RT Urine samples Baseline, Last Day RT Blood samples Baseline, Last Day RT
ONS Acute Skin Reaction Baseline, Week 3, Last day RT, Month 1 and 2 post RT,
Photographs Baseline, Week 3 (standard fractionated regimen only), Last day RT, Month 1, 2, 6 and 12 post RT
FACT-B Baseline, Last day RT, Month 1, 6 and 12 post RT RTOG SOMA Criteria for RT-Induced Breast/Chest Wall Late Skin Toxicity Month 6 and 12 post RT
Breast/Chest Wall RT Completion Form Last day RT
Data Submission Checklist Baseline, Week 3, Last day RT, Month 1, 2, 6 and 12 post RT
Flow Sheet/Addenda Baseline, Week 3, Last day RT, Month 1, 2, 6 and 12 post RT
11.2 Case Report Forms
Participant data will be collected using protocol-specific case report forms (CRF). 11.3 Source Documents
Source documents are the original signed and dated records of participant information (e.g., the medical record, shadow chart) which may include electronic documents containing all the information related to a participant’s protocol participation. Source documents are used to verify the integrity of the study data, to verify participant eligibility, and to verify that mandatory protocol procedures were followed. An investigator and other designated staff are required to prepare and maintain adequate and accurate documentation that records all observations and other data pertinent to the investigation for each individual participating in the study. All data recorded in the research record (including data recorded on CRFs) must originate in the participant’s medical record, study record, or other official document sources.
Source documents substantiate CRF information. All participant case records (e.g., flow sheets, clinical records, physician’s notes, correspondence) must adhere to the following standards:

Amendment 2: 11/23/2011 35 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
• Clearly labeled in accordance with HIPAA practices so that they can be
associated with a particular participant or PID; • Legibly written in ink; • Signed and dated in a real time basis by health care practitioner evaluating or
treating the participant; • Correction liquid or tape must not be used in source documents or on CRFs. • Corrections are made by drawing a single line through the error. Do not obliterate
the original entry. Insert the correct information, initial, and date the entry.
All laboratory reports, pathology reports, x-rays, imaging study and scans must have:
• Complete identifying information (name and address of the organization performing, analyzing, and/or reporting the results of the test); and
• Range of normal values for each result listed.
11.4 Data and Safety Monitoring Board
The Data Safety Monitoring Board meets every six months to review all phase II and phase III protocols. The Board includes members demonstrating experience and expertise in oncology, biological sciences and ethics. The DSMB report is generated by the statistician. Areas of review may include the following: Study Duration; Study Objectives; Patient Accrual; Patient Status and Retention; Study Status; Last Contact Status; Patient Compliance; Number of Biopsies/Labs as needed; Patient Characteristics; Summary of Observed Toxicities; Adverse Events; Date, Event briefly described, Relationship to Drug, Arm assigned; Summary of Secondary Measures.
11.5 Record retention
Clinical records for all participants, including CRFs, all source documentation (containing evidence to study eligibility, history and physical findings, laboratory data, results of consultations, etc.), as well as IRB records and other regulatory documentation will be retained by the Investigator in a secure storage facility in compliance with HIPAA, OHRP, FDA regulations and guidance, and NCI/DCP requirements unless the standard at the site is more stringent.
Record retention should be 2 years after the study is discontinued (i.e. publications) for studies without an IND (21 CFR 312.62).
11.6 CDUS Reporting
The CCCWF CCOP Research Base Data Management Center will submit quarterly reports to DCP/CTEP by electronic means using the Clinical Data Update System (CDUS)
Amendment 2: 11/23/2011 36 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
12. STATISTICAL CONSIDERATIONS 12.1 Study Design/Endpoints
An observational design will be used to evaluate RT-induced EASRs in 1000 newly recruited multi-racial/ethnic breast cancer cases receiving RT to the breast or chest-wall. For this study, no interventions will be given; rather, we will follow patients and obtain blood samples and questionnaires at specified intervals over time. The blood samples will be used to obtain genotype data on 21,877 nsSNPs and several biomarkers of interest, allowing us to assess our primary specific aims.
Specific Aim 1 will test the working hypothesis that nsSNPs from multiple candidate pathways have dominant, recessive, additive, and/or multiplicative effects on RT-induced EASRs. Specific Aim 2 will evaluate the levels of DNA damage (Comet assay), signal transduction (γ-H2AX) and cell cycle G2 delay in lymphocytes pre-RT (exposed to IR in vitro) and test the hypothesis that individual’s cellular responses to IR contribute to RT-induced EASRs in normal tissue.
Specific Aim 3 will test the effect of gene-gene and gene-smoking interactions on RT-induced adverse event.
Specific Aim 4 will assess race-ethnic differences in RT-induced skin reactions, DNA damage, and radio sensitivity and to determine if the gene effects are consistent across race-ethnicities (gene-race/ethnic interactions).
12.2 Sample Size/Accrual Rate
We will accrue a total of 1000 participants to this study, 100 of whom will be recruited from the University of Miami (UM) and 900 from the CCCWF CCOP Research Base and CTSU- affiliated cooperative groups.. For all participants combined, we expect to have 1000 accruals (400 White, 200 African American, 200 Hispanic/Latino, 100 Asian/Native Hawaiian or Pacific Islander, 100 American Indian/Alaskan Native). Accrual as a function of race/ethnicity by institution (RB and UM) is shown in Section 4.3. Our sample size was chosen so we could detect reasonable SNP/EASR associations, even within race/ethnic subgroups, as shown below.
Specific Aim 1: Considering each genotype may have different distributions, we calculate the minimal detectable OR with 80% power assuming the proportion of controls with high-risk genotype (P0) ranges from 5% to 50% (nQuery Advisor). With an estimate that 50% or 30% of the participants may develop RT-induced EASRs, we determined the minimal detectable (MD) odds ratios in total and each racial/ethnic group (1000 total, 400 NHW, 200 AA and HW, and 100 ASPI and AIAN) (Table 12.1). Using a 2-sided Fisher’s exact test at the 5% significance level, we can detect moderate association between genotype and EASRs. Obviously, we can only reasonably detect larger associations for the minority populations, although fairly large associations have already been reported in previous genetic studies with relatively small sample sizes (Ho et al., 2007; Kuptosova et al., 2008). However, any positive study results derived from small sample size will need to be validated in future larger studies.

Amendment 2: 11/23/2011 37 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Table 12.1. Minimal Detectable (MD) Odds Ratios Associating Genotypes with RT-induced EASRs
% Risk Genotype
in Controls
50% Developed EASRs 30% Developed EASRs 500/500 (Total)
200/200 (NHW)
100/100 (AA/HW)
50/50 (ASPI/AIAN)
700/300 (Total)
280/120 (NHW)
140/60 (AA/HW)
70/30 (ASPI/AIAN)
5% 2.07 3.00 4.22 7.15 2.23 3.36 5.08 8.62 10% 1.74 2.33 3.13 4.87 1.83 2.54 3.58 5.69 20% 1.54 1.96 2.54 3.73 1.60 2.10 2.80 4.24 30% 1.47 1.84 2.35 3.43 1.52 1.95 2.57 3.86 40% 1.44 1.80 2.28 3.42 1.49 1.90 2.51 3.84 50% 1.44 1.81 2.35 3.65 1.49 1.91 2.56 4.10
Specific Aim 2: The three functional assays, DNA damage, γ-H2AX, and cell cycle G2 delay, will generate quantitative measurements in 1000 patients (400 NHW, 200 AA and HW, and 100 ASPI and AIAN). We estimate the minimal detectable differences (MDD) based on the estimated EASR rate at 50% or 30% with the corresponding sample size. Table 12.2 presents MDD between the two groups of patients (with or without EASRs) at 80% power with a significance level (alpha) of 0.05 using a two-sided two-sample Student’s t-test. Even in the smallest minority populations (ASPI and AIAN), we will have 80% power to detect relative MDDs of ≤ 22% for all assays.
Table 12.2. Minimal Detectable Differences (MDD) of Functional Phenotypes
Assay % EASR Rate 50% 30%
Control/Case 500/500 (Total)
200/200 (NHW)
100/100 (AA/HW)
50/50 (ASPI/AIAN)
700/300 (Total)
280/120 (NHW)
140/60 (AA/HW)
70/30 (ASPI/AIAN)
Basal Comet Mean 11.42 11.80 12.23 12.83 11.48 11.89 12.36 13.02 (10.78+3.63)1 Difference 0.64 1.02 1.45 2.05 0.70 1.11 1.58 2.24
% Difference 6% 9% 12% 19% 6% 10% 13% 21% IR-Comet Mean 22.10 22.62 23.18 24.00 22.19 22.73 23.37 24.25
(21.24+4.88)1 Difference 0.86 1.38 1.94 2.76 0.95 1.49 2.13 3.01 % Difference 4% 6% 8% 13% 4% 7% 9% 14%
Basal H2AX Mean 6.86 6.98 7.12 7.32 6.88 7.01 7.16 7.38 (6.65+1.18)2 Difference 0.21 0.33 0.47 0.67 0.23 0.36 0.51 0.73
% Difference 3% 5% 7% 10% 3% 5% 7% 11% IR-H2AX Mean 30.45 31.17 31.97 33.12 30.56 31.34 32.23 33.47
(29.23+6.88)2 Difference 1.22 1.94 2.74 3.89 1.33 2.11 3.00 4.24 % Difference 4% 7% 9% 13% 4% 7% 9% 15%
G2 Delay Mean 38.32 39.69 41.22 43.41 38.54 40.01 41.71 44.08 (36.0+13.1)3 Difference 2.32 3.69 5.22 7.41 2.54 4.01 5.71 8.08
% Difference 6% 10% 13% 21% 7% 11% 14% 22% 1 Data derived from 118 breast cancer cases (Hu et al., 2002). 2 Data derived from 70 breast cancer cases (Smith et al., 2003). 3 Data derived from 64 breast cancer cases (Table 6; pilot data).
Specific Aim 3 will test the effect of gene-gene and gene-smoking interactions on RT-induced adverse events. Candidate nsNSPs-genotypes will be those identified as potential risk factors, that is, those that best discriminate between cases and controls as resulting from analyses under Specific Aim1. In Table 12.3, we present power to detect gene-gene or gene-smoking interactions, assuming K=2 levels of genotype for each nsSNPs (high and low) and for cigarette smoke exposure (smoker v. non-smoker). Specifically, we assume OR =1.5 and 3.0 (odds ratio of the cigarette smoke exposure among the non-carrier of the
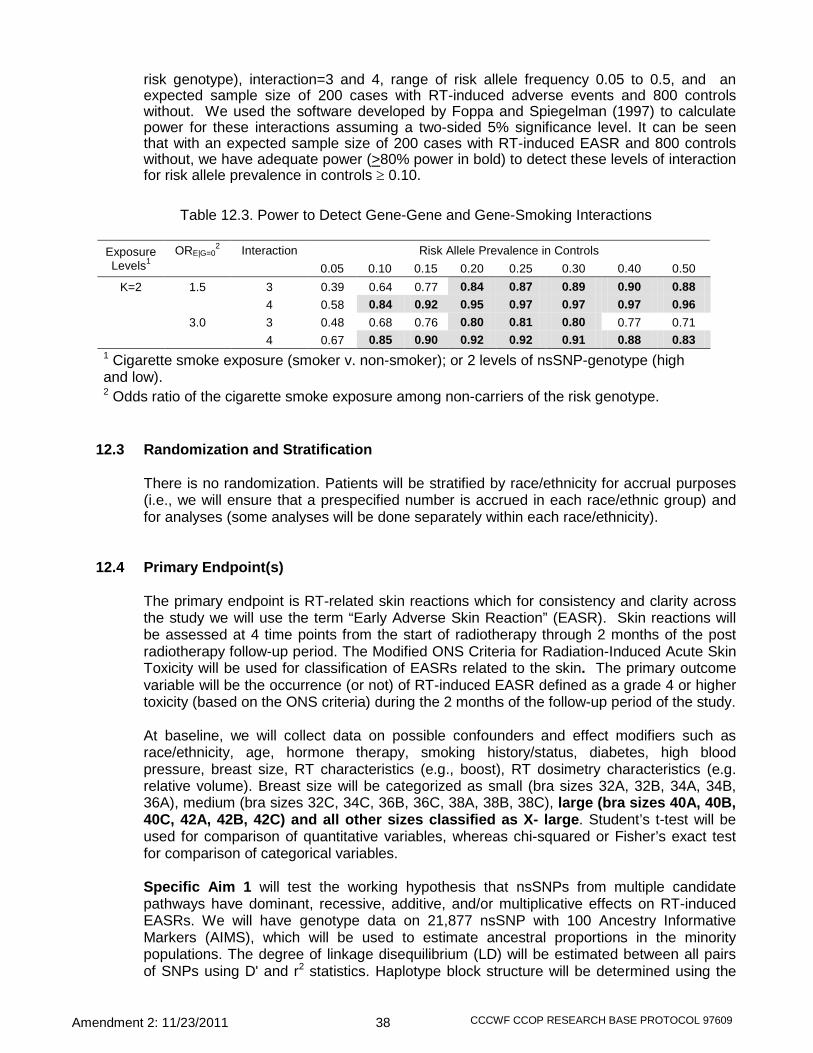
Amendment 2: 11/23/2011 38 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
risk genotype), interaction=3 and 4, range of risk allele frequency 0.05 to 0.5, and an expected sample size of 200 cases with RT-induced adverse events and 800 controls without. We used the software developed by Foppa and Spiegelman (1997) to calculate power for these interactions assuming a two-sided 5% significance level. It can be seen that with an expected sample size of 200 cases with RT-induced EASR and 800 controls without, we have adequate power (>80% power in bold) to detect these levels of interaction for risk allele prevalence in controls ≥ 0.10.
Table 12.3. Power to Detect Gene-Gene and Gene-Smoking Interactions
Exposure Levels1
ORE|G=02 Interaction Risk Allele Prevalence in Controls
0.05 0.10 0.15 0.20 0.25 0.30 0.40 0.50 K=2 1.5 3 0.39 0.64 0.77 0.84 0.87 0.89 0.90 0.88
4 0.58 0.84 0.92 0.95 0.97 0.97 0.97 0.96 3.0 3 0.48 0.68 0.76 0.80 0.81 0.80 0.77 0.71
4 0.67 0.85 0.90 0.92 0.92 0.91 0.88 0.83 1 Cigarette smoke exposure (smoker v. non-smoker); or 2 levels of nsSNP-genotype (high and low). 2 Odds ratio of the cigarette smoke exposure among non-carriers of the risk genotype.
12.3 Randomization and Stratification
There is no randomization. Patients will be stratified by race/ethnicity for accrual purposes (i.e., we will ensure that a prespecified number is accrued in each race/ethnic group) and for analyses (some analyses will be done separately within each race/ethnicity).
12.4 Primary Endpoint(s)
The primary endpoint is RT-related skin reactions which for consistency and clarity across the study we will use the term “Early Adverse Skin Reaction” (EASR). Skin reactions will be assessed at 4 time points from the start of radiotherapy through 2 months of the post radiotherapy follow-up period. The Modified ONS Criteria for Radiation-Induced Acute Skin Toxicity will be used for classification of EASRs related to the skin. The primary outcome variable will be the occurrence (or not) of RT-induced EASR defined as a grade 4 or higher toxicity (based on the ONS criteria) during the 2 months of the follow-up period of the study.
At baseline, we will collect data on possible confounders and effect modifiers such as race/ethnicity, age, hormone therapy, smoking history/status, diabetes, high blood pressure, breast size, RT characteristics (e.g., boost), RT dosimetry characteristics (e.g. relative volume). Breast size will be categorized as small (bra sizes 32A, 32B, 34A, 34B, 36A), medium (bra sizes 32C, 34C, 36B, 36C, 38A, 38B, 38C), large (bra sizes 40A, 40B, 40C, 42A, 42B, 42C) and all other sizes classified as X- large. Student’s t-test will be used for comparison of quantitative variables, whereas chi-squared or Fisher’s exact test for comparison of categorical variables.
Specific Aim 1 will test the working hypothesis that nsSNPs from multiple candidate pathways have dominant, recessive, additive, and/or multiplicative effects on RT-induced EASRs. We will have genotype data on 21,877 nsSNP with 100 Ancestry Informative Markers (AIMS), which will be used to estimate ancestral proportions in the minority populations. The degree of linkage disequilibrium (LD) will be estimated between all pairs of SNPs using D' and r2 statistics. Haplotype block structure will be determined using the

Amendment 2: 11/23/2011 39 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Solid Spine of LD option of Haploview (Barrett et al., 2005) with the block extended if pairwise D' between SNPs is >0.80.
Each SNP will be tested for allelic association with RT-induced EASRs using chi-square or Fisher’s exact tests. Association between modes of inheritance (dominant, additive, and recessive) and RT-induced skin reactions will be tested using logistic regression adjusting for individual estimates of admixture. We will use the program Admixmap (McKeigue et al., 2000) to model the distributions of admixture and to generate score tests of allelic association, adjusted for individual estimates of admixture. Ancestral allele frequencies will be estimated from the genotyped control populations (Gallagher et al., 2007). We will use multiple logistic regression models to test whether a specific nsSNP-genotype is an independent risk factor for RT-induced EASRs. These analyses will be adjusted for potential confounders, such as age, race, body mass index, treatment characteristics, smoking history, and specifically individual estimates of admixture for African Americans and/or American Indians. In these logistic regression models, the outcome variable will be an indicator of RT-induced EASR event (1=with grade 4 or higher toxicity based on the ONS criteria as cases, 0=no, control), and the potential risk factor will be a specific nsSNP-genotype included as a dichotomous variable (0=low risk and 1=high risk).
We will test the goodness-of-fit of different models using the likelihood ratio test and other chi-square tests implemented in the SAS Proc Logistic (SAS Institute, Cary NC). Relative risk of RT-induced EASRs associated with individual genotypes or combined variants will be estimated by odds ratios (OR) comparing exposure frequencies among cases and controls with and without EASRs [71]. We will also evaluate the application of genotype profiles in building predictive models of RT-induced EASRs. We will first use an ad hoc approach based on univariate logistic regression analyses. The SNPs with the twenty smallest p-values will be considered in the polygenic model. Then a multivariate logistic regression model will be fitted with all features in the gene profile; this leads to individual prognoses. We will evaluate individual genes as well as gene clusters in 9 major cancer-related pathways, angiogenesis, apoptosis, proliferation, cell-cycle control, developmental processes, DNA repair, cell signaling, cell migration and immunology/inflammation. In exploratory analyese, we will also assess the additive and/or multiplicative effects of multiple specific genes on RT-induced skin reactions using a newly developed data mining tool, Multivariate Adaptive Regression Splines (MARS) logit models.
Specific Aim 2 will evaluate the levels of DNA damage (Comet assay), signal transduction (γ-H2AX) and cell cycle G2 delay in lymphocytes pre-RT (exposed to IR in vitro) and test the hypothesis that individual’s cellular responses to IR contribute to RT-induced EASRs in normal tissue. First, we will use Student’s t-test to compare mean DNA damage, γ-H2AX, and G2 delay levels in patients with and without EASRs. A more sophisticated analysis will apply analysis of variance (ANOVA) after adjustment for other effect modifiers, such as age, race, breast size, treatment characteristics, and smoking history. The variables will be transformed, if necessary, to achieve an approximate normal distribution and to stabilize the variance. The rationale for us to select these three functional assays to access overall IR sensitivity are: (1) the Comet DNA damage assay measures single strand breaks either as basal or IR-induced level, (2) γ-H2AX reflects basal and IR-induced double-strand-break load as a signal for DNA repair, and (3) cell cycle G2 delay assay can measure the combined defects in damage signaling and/or DNA repair. We hypothesize that subjects with higher Comet DNA damage, γ-H2AX, and/or cell cycle G2 delay may have elevated risk of normal tissue toxicity.

Amendment 2: 11/23/2011 40 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Specific Aim 3 will test the effect of gene-gene and gene-smoking interactions on RT-induced adverse events. Candidate nsNSPs-genotypes will be those identified as potential risk factors, that is, those that best discriminate between cases and controls as resulting from analyses under Specific Aim1. We will use multiple logistic regression analysis with RT-induced adverse event status as the dependent variable, and measurements of nsSNPs-genotype and cigarette smoke exposure (smokers, secondhand smoker, non-smoker) as potential risk factors. These models will be adjusted for potential confounders, such as race/ethnicity, age, family history, and disease stage. To assess departures from interaction on a multiplicative scale, the likelihood ratio test will compare models with interaction terms for gene (nsSNPs-genotype) and smoke to models with main effects for gene and smoke exposure only. Furthermore, exploratory analysis using MARS-logit hybrid model will be carried out on the subset of nsNSPs-genotypes that were identified as potential risk factors in the previous analyses, to evaluate gene-gene and gene-smoking interactions. (Cook et al., 2004; Hu et al., 2005; Lin et al,. 2006a, 2006b; Van Emburgh et al., 2007). We will use the MARS software (Salford Systems, San Diego, CA) for this analysis. The final analysis will entail the fit of a multiple logistic regression model including the individual nsNSPs-genotypes, interactions identified by MARS and potential confounders, carried out using Proc Logistic in SAS software (SAS Institute, Cary NC). Relative risk of RT-induced EASR associated to individual genotypes or combined variants will be estimated by odds ratios (OR) comparing exposure frequencies among cases and controls (Khoury and Beaty, 1994).
Multiple Testing
: It is well recognized that when one tests multiple hypotheses, the individual P values of the tests may not be an appropriate guide to actual statistical significance. Failure to adjust for multiple testing adequately may produce excessive false positives or overlook true positive associations. Although the Bonferroni method of adjusting for multiple comparisons is easy to compute, but is well known to be too conservative in the presence of LD. Therefore, we will use two methods to control type I error. First, we will use a newly-developed universal False Discovery Rate (FDR) methodology to assign a single global probability value per SNP to maximize power (Forner et al., 2008). Second, we will explore the use of a new multiple testing correction method developed at the UM Miami Institute of Human Genomics (MIHG), which is a simple, fast and more accurate method for genome-wide association studies to control type I error (Gao et al., 2008).
Specific Aim 4 will assess race-ethnic differences in RT-induced skin reactions, DNA damage, and radio sensitivity and to determine if the gene effects are consistent across race-ethnicities (gene-race/ethnic interactions). Linear models (ANOVA) will be used to determine if DNA damage and radio sensitivity differ between race-ethnicities. Transformations will be sought to ensure model assumptions are met (normality, constant variances). Separate models will be run which include additional patient covariates to see if any of the race-ethnic differences can be described by differences in patient characteristics such as age. The gene-race/ethnic interactions will be assessed as described in the analyses for Aim 3.
12.5 Secondary Endpoint(s)
Quality of life will be assessed using the FACT-B, a modification of the Skindex-16, and a modified version of the NSABP B39 Quality of Life metric. Descriptive statistics (means, standard deviations, frequencies, etc.) will be presented for quality of life at baseline and at each follow-up point stratified by race/ethnicity. A repeated measures model for longitudinal data will be used to obtain estimates of QOL across time and to test for race/ethnicity differences in the changes over time. Several covariance structures will be used to model the within patient correlation, and the final choice will be the one that minimizes the BIC statistic. In additional analyses, EASR, DNA damage, and radio

Amendment 2: 11/23/2011 41 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
sensitivity will be included as (possibly) time varying covariates to assess race/ethnic differences after adjustment for skin toxicity. Pearson and Spearman correlation coefficients will be calculated to quantitate the strength of the linear and monotonic correlations in these QOL measures at each time. Linear regression models will be used to assess the effect of early skin reactions on FACT-B, Skindex-16, and the NSABP B39 measure. Additional simple linear models will be used to assess race/ethnic differences in the change in QOL over time adjusting for other demographic characteristics and the maximum degree of skin toxicity.
12.6 Reporting and Exclusions All patients who meet the eligibility criteria will be included in the analyses and included in all reports which summarize the results. If secondary analyses are done which exclude some participants (e.g., those who get a limited radiation dose), these exclusions will be described in detail in the study reports.
12.7 Evaluation of Toxicity
Participants will be followed for radiation induced skin toxicity – the primary endpoint of this study. Only (Grades 4 and 5) SAE’s will be reported (see Section 10). Other toxicities will not be recorded as this is an observational study, not a treatment study.
12.8 Data Analysis We will generate reports describing accrual, retention, data completeness, acute and
chronic skin toxicities, and SAEs for the DSMB which meets every six months. Accrual is monitored monthly during the RB executive committee meetings

Amendment 2: 11/23/2011 42 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
REFERENCES Alsbeih G, Al-Harbi N, Al-Buhairi M, Al-Hadyan K, Al-Hamed M. Association between TP53 codon 72
single-nucleotide polymorphism and radiation sensitivity of human fibroblasts. Radiat Res. 2007a;167:535-40.
Alsbeih, G., et al., Radiosensitivity of human fibroblasts is associated with amino acid substitution variants in susceptible genes and correlates with the number of risk alleles. Int J Radiat Oncol Biol Phys, 2007. 68(1): p. 229-35.
Altman DG. Statistics in medical journals: some recent trends. Statist Med 2000;19:3275-89. Alsbeih G, El-Sebaie M, Al-Harbi N, Al-Buhairi M, Al-Hadyan K, Al-Rajhi N. Radiosensitivity of human
fibroblasts is associated with amino acid substitution variants in susceptible genes and correlates with the number of risk alleles. Int J Radiat Oncol Biol Phys. 2007;68:229-35.
Andreassen, C.N., et al., Prediction of normal tissue radiosensitivity from polymorphisms in candidate genes. Radiother Oncol, 2003. 69(2): p. 127-35.
Andreassen CN, Alsner J, Overgaard M, Sorensen FB, Overgaard J. Risk of radiation-induced subcutaneous fibrosis in relation to single nucleotide polymorphisms in TGFB1, SOD2, XRCC1, XRCC3, APEX and ATM--a study based on DNA from formalin fixed paraffin embedded tissue samples. Int J Radiat Biol. 2006;82:577-86.
Barcellos-Hoff MH. How tissues respond to damage at the cellular level: orchestration by transforming growth factor-ß (TGF-ß). BJR Suppl 2005;27:123-7.
Barrett JC, Fry B, Maller J, Daly MJ: Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 2005;21:263-265.
Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer. 2007;109:1721-8.
Benowitz NL. Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol Rev. 1996;18:188-204.
Bernert JT Jr, Turner WE, Pirkle JL, Sosnoff CS, Akins JR, Waldrep MK, Ann Q, Covey TR, Whitfield WE, Gunter EW, Miller BB, Patterson DG Jr, Needham LL, Hannon WH, Sampson EJ. Development and validation of sensitive method for determination of serum cotinine in smokers and nonsmokers by liquid chromatography/atmospheric pressure ionization tandem mass spectrometry. Clin Chem. 1997;43:2281-91.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995;57:289-300.
Bernert JT Jr, McGuffey JE, Morrison MA, Pirkle JL. Comparison of serum and salivary cotinine measurements by a sensitive high-performance liquid chromatography-tandem mass spectrometry method as an indicator of exposure to tobacco smoke among smokers and nonsmokers. J Anal Toxicol. 2000;24:333-9.
Bese NS, Sut PA, Ober A. The effect of treatment interruptions in the postoperative irradiation of breast cancer. Oncology. 2005;69:214-23.
Bese NS, Sut PA, Sut N, Ober A. The impact of treatment interruptions on locoregional control during postoperative breast irradiation. J BUON. 2007;12:353-9.
Blakely WF, Ossetrova NI, Whitnall MH, Sandgren DJ, Krivokrysenko VI, Shakhov A, Feinstein E. Multiple parameter radiation injury assessment using a nonhuman primate radiation model-biodosimetry applications. Health Phys. 2010;98:153-9.
Borghero, Y.O., et al., Multileaf field-in-field forward-planned intensity-modulated dose compensation for whole-breast irradiation is associated with reduced contralateral breast dose: a phantom model comparison. Radiother Oncol, 2007. 82(3): p. 324-8.
Bower JE, Ganz PA, Tao ML, Hu W, Belin TR, Sepah S, Cole S, Aziz N. Inflammatory biomarkers and fatigue during radiation therapy for breast and prostate cancer. Clin Cancer Res. 2009;15:5534-40.
Brady MJ, Cella DF, Mo F, Bonomi AE, Tulsky DA, Lloyd SR, Deasy S, Cobleigh M, Shiomoto G. Reliability and Validity of the Functional Assessment of Cancer Therapy – Breast quality of life instrument. J Clin Oncol 1997; 15:974-986.

Amendment 2: 11/23/2011 43 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Bretsky P, Haiman CA, Gilad S, Yahalom J, Grossman A, Paglin S, Van Den Berg D, Kolonel LN, Skaliter R, Henderson BE. The relationship between twenty missense ATM variants and breast cancer risk: the Multiethnic Cohort. Cancer Epidemiol Biomarkers Prev. 2003;12:733-8.
Broeks A, Braaf LM, Huseinovic A, Nooijen A, Urbanus J, Hogervorst FB, Schmidt MK, Klijn JG, Russell NS, Van Leeuwen FE, Van 't Veer LJ. Identification of women with an increased risk of developing radiation-induced breast cancer: a case only study. Breast Cancer Res. 2007;9:R26.
Buchholz, T.A., Radiation therapy for early-stage breast cancer after breast-conserving surgery. N Engl J Med, 2009. 360(1): p. 63-70.
Chang-Claude J, Popanda O, Tan XL, Kropp S, Helmbold I, von Fournier D, Haase W, Sautter-Bihl ML, Wenz F, Schmezer P, Ambrosone CB. Association between polymorphisms in the DNA repair genes, XRCC1, APE1, and XPD and acute side effects of radiotherapy in breast cancer patients. Clin Cancer Res. 2005;11:4802-9.
Chen MF, Chen WC, Lai CH, Hung CH, Liu KC, Cheng YH. Predictive factors of radiation induced skin toxicity in breast cancer patients. BMC Cancer 2010; 10: 508.
Chow EJ, Simmons JH, Roth CL, Baker KS, Hoffmeister PA, Sanders JE, Friedman DL. Increased cardiometabolic traits in pediatric survivors of acute lymphoblastic leukemia treated with total body irradiation. Biol Blood Marrow Transplant. 2010 May 31. [Epub ahead of print]
Chren MM, Lasek RJ, Sahay AP, Sands LP. Measurement properties of Skindex 16: a brief quality of life measure for patients with skin diseases. J Cutan Med Surg 2001; 5: 105-110.
Christmann M, Tomicic MT, Roos WP, Kaina B. Mechanisms of human DNA repair: an update. Toxicology. 2003;193:3-34.
Cromie GA, Connelly JC, Leach DR. Recombination at double-strand breaks and DNA ends: conserved mechanisms from phage to humans. Mol Cell. 2001;8:1163-74.
Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans E, Godwin J, Gray R, Hicks C, James S, MacKinnon E, McGale P, McHugh T, Peto R, Taylor C, Wang Y; Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005 366:2087-106.
Collette, S., et al., Predictors of the risk of fibrosis at 10 years after breast conserving therapy for early breast cancer: a study based on the EORTC Trial 22881-10882 'boost versus no boost'. Eur J Cancer, 2008. 44(17): p. 2587-99.
Collins-Schramm HE, Chima B, Morii T, Wah K, Figueroa Y, Criswell LA, Hanson RL, Knowler WC, Silva G, Belmont JW, Seldin MF. Mexican American ancestry-informative markers: examination of population structure and marker characteristics in European Americans, Mexican Americans, Amerindians and Asians. Hum Genet. 2004;114:263-71.
Cook NR, Zee RY, Ridker PM. Tree and spline based association analysis of gene-gene interaction models for ischemic stroke. Stat Med 2004;23:1439-53.
Craven P, Wahba G. Smoothing noisy data with spline functions. Estimating the correct degree of smoothing by the method of generalized cross-validation. Numerical Mathematics 1979; 31:317-403.
Cui Z, Willingham MC, Hicks AM, Alexander-Miller MA, Howard TD, Hawkins GA, Miller MS, Weir HM, Du W, DeLong CJ. Spontaneous regression of advanced cancer: identification of a unique genetically determined, age-dependent trait in mice. Proc Natl Acad Sci U S A. 2003;100:6682-7.
Cummings KM, Markello SJ, Mahoney MC, Marshall JR. Measurement of lifetime exposure to passive smoke. Am J Epidemiol. 1989;130:122-32.
Cummings KM, Markello SJ, Mahoney M, Bhargava AK, McElroy PD, Marshall JR. Measurement of current exposure to environmental tobacco smoke. Arch Environ Health. 1990;45:74-9.
Delaloye, J.F., et al., Radiation therapy duration influences overall survival in patients with cervical carcinoma. Int J Gynaecol Obstet, 1997. 57(3): p. 295-303.
De Ruyck K, Van Eijkeren M, Claes K, Morthier R, De Paepe A, Vral A, De Ridder L, Thierens H. Radiation-induced damage to normal tissues after radiotherapy in patients treated for gynecologic tumors: association with single nucleotide polymorphisms in XRCC1, XRCC3, and OGG1 genes and in vitro chromosomal radiosensitivity in lymphocytes. Int J Radiat Oncol Biol Phys. 2005;62:1140-9.
Edvardsen H, Tefre T, Jansen L, Vu P, Haffty BG, Fossaa SD, Kristensen VN, Borresen-Dale AL. Linkage disequilibrium pattern of the ATM gene in breast cancer patients and controls; association

Amendment 2: 11/23/2011 44 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
of SNPs and haplotypes to radio sensitivity and post-lumpectomy local recurrence. Radiat Oncol. 2007;2:25 [Epub ahead of print]
Einarsdottir K, Rosenberg LU, Humphreys K, Bonnard C, Palmgren J, Li Y, Li Y, Chia KS, Liu ET, Hall P, Liu J, Wedren S. Comprehensive analysis of the ATM, CHEK2 and ERBB2 genes in relation to breast tumour characteristics and survival: a population-based case-control and follow-up study. Breast Cancer Res. 2006;8:R67.
Fentiman IS, Allen DS, Hamed H. Smoking and prognosis in women with breast cancer. Int J Clin Pract. 2005;59:1051-4.
Foppa I, Spiegelman D. Power and sample size calculations for case-control studies of gene-environment interactions with a polytomous exposure variable. Am J Epidemiol. 1997;146:596-604.
Gallagher CJ, Keene KL, Mychaleckyj JC, Langefeld CD, Hirschhorn JN, Henderson BE, Gordon CJ, Freedman BI, Rich SS, Bowden DW, Sale MM. Investigation of the estrogen receptor-alpha gene with type 2 diabetes and/or nephropathy in African-American and European-American populations. Diabetes. 2007;56:675-84.
Giordano, S.H., et al., Risk of cardiac death after adjuvant radiotherapy for breast cancer. J Natl Cancer Inst, 2005. 97(6): p. 419-24.
Goodman SN. Multiple comparisons, explained. Amer J Epidemiol 1998;147:807-12. Haber JE. Partners and pathwaysrepairing a double-strand break. Trends Genet. 2000;16:259-64. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic
(ROC) curve. Radiology 1982; 143:29-36. Harrell Jr FE. Regression Modeling Strategies. Springer: New York, 2001. Hecht SS. Carcinogen derived biomarkers: applications in studies of human exposure to secondhand
tobacco smoke. Tob Control. 2004;13 Suppl 1:i48-56. Hehr, T., et al., Evaluation of predictive factors for local tumour control after electron-beam-rotation
irradiation of the chest wall in locally advanced breast cancer. Radiother Oncol, 1999. 50(3): p. 283-9.
Hicks AM, Willingham MC, Du W, Pang CS, Old LJ, Cui Z. Effector mechanisms of the anti-cancer immune responses of macrophages in SR/CR mice. Cancer Immun. 2006;6:11.
Ho AY, Fan G, Atencio DP, Green S, Formenti SC, Haffty BG, Iyengar P, Bernstein JL, Stock RG, Cesaretti JA, Rosenstein BS. Possession of ATM Sequence Variants as Predictor for Late Normal Tissue Responses in Breast Cancer Patients Treated with Radiotherapy. Int J Radiat Oncol Biol Phys. 2007;69:677-84
Holm S. A simple sequentially rejective multiple test procedure. Scand J Statistics 1979;6:65-70. Holmes MD, Murin S, Chen WY, Kroenke CH, Spiegelman D, Colditz GA. Smoking and survival after
breast cancer diagnosis. Int J Cancer. 2007;120:2672-7. Hosmer DW, Lemeshow S. Applied Logistic Regression (2nd Ed.). NY: John Wiley & Sons, Inc. 2000. Hu JJ, Smith TR, Miller MS, Mohrenweiser HW, Golden A, Case LD. Amino acid substitution variants
of APE1 and XRCC1 genes associated with ionizing radiation sensitivity. Carcinogenesis. 2001;22:917-22.
Hu JJ, Smith TR, Miller MS, Lohman K, Case LD. Genetic regulation of ionizing radiation sensitivity and breast cancer risk. Environ Mol Mutagen. 2002;39:208-15.
Hu JJ, Hall MC, Clark PE, Phillips JJ, Lockett KL, Xu J, Zhengg SL, and Chuang SC. DNA-repair nsSNPs in prostate cancer risk and tumor aggressiveness. Proc. AACR 2005;46:9371.
Huang D, Ou B, Hampsch-Woodill M, Flanagan JA, Prior RL. High-throughput assay of oxygen radical absorbance capacity (ORAC) using a multichannel liquid handling system coupled with a microplate fluorescence reader in 96-well format. J Agric Food Chem. 2002;50:4437-44.
Hwang SJ, Beaty TH, Liang KY, Coresh J, Khoury MJ. Minimum sample size estimation to detect gene-environment interaction in case-control designs. Amer J Epidemiol 1994;140:1029-37.
Jarvis MJ, Russell MA, Benowitz NL, Feyerabend C. Elimination of cotinine from body fluids: implications for noninvasive measurement of tobacco smoke exposure. Am J Public Health. 1988;78:696-8.
Jemal A, Siegel R, Xu J, Ward E. Cancer Statistics, 2010. CA Cancer J Clin 2010;60;277-300. PubMed PMID: 20610543.
Johnson RD, Jasin M. Sister chromatid gene conversion is a prominent double-strand break repair pathway in mammalian cells. EMBO J. 2000;19:3398-407.

Amendment 2: 11/23/2011 45 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Jones IM, Thomas CB, Xi T, Mohrenweiser HW, Nelson DO. Exploration of methods to identify polymorphisms associated with variation in DNA repair capacity phenotypes. Mutat Res. 2007;616:213-20.
Kanaya S, Ikeya M, Yamamoto K, Moriya T, Furuhashi K, Sonoda M, Goto K, Ochi H. Comparison of an oxidative stress biomarker "urinary8-hydroxy-2'-deoxyguanosine," between smokers and non-smokers. Biofactors. 2004;22:255-8.
Kastan MB, Bartek J. Cell-cycle checkpoints and cancer. Nature 2004;432:316-23. Khoury MJ, Beaty TH. Applications of the case-control method in genetic epidemiology. Epidem Rev
1994;16:134-50. Kim GD, Choi YH, Dimtchev A, Jeong SJ, Dritschilo A, Jung M. Sensing of ionizing radiation-induced
DNA damage by ATM through interaction with histone deacetylase. J Biol Chem. 1999;274:31127-30.
Kirshner J, Jobling MF, Pajares MJ, Ravani SA, Glick AB, Lavin MJ, Koslov S, Shiloh Y, Barcellos-Hoff MH. Inhibition of transforming growth factor-beta1 signaling attenuates ataxia telangiectasia mutated activity in response to genotoxic stress. Cancer Res. 2006;66:10861-9.
Krishnan L, Stanton AL, Collins CA, Liston VE, Jewell WR. Form or Function? Part 2. Objective cosmetic and functional correlates of quality of life in women treated with breast conserving surgical procedures and radiotherapy. Cancer 2001; 91:2282-2287.
Kundu CN, Balusu R, Jaiswal AS, Gairola CG, Narayan S. Cigarette smoke condensate-induced level of adenomatous polyposis coli blocks long-patch base excision repair in breast epithelial cells. Oncogene. 2006; [Epub ahead of print].
Kurz EU, Lees-Miller SP. DNA damage-induced activation of ATM and ATM-dependent signaling pathways. DNA Repair (Amst) 2004;3:889-900.
Lilla C, Ambrosone CB, Kropp S, Helmbold I, Schmezer P, von Fournier D, Haase W, Sautter-Bihl ML, Wenz F, Chang-Claude J. Predictive factors for late normal tissue complications following radiotherapy for breast cancer. Breast Cancer Res Treat. 2007 Jan 13; [Epub ahead of print]
Lilla, C., et al., Predictive factors for late normal tissue complications following radiotherapy for breast cancer. Breast Cancer Res Treat, 2007. 106(1): p. 143-50.
Lin H-Y, Hall MC, Clark PE, Phillips JJ, Hu JJ. Gene-gene interactions of DNA-repair nsSNPs in prostate cancer recurrence Proc Amer Assoc Cancer Res 2006a;47:1205.
Lin H-Y, Velasco C, Myers L, Hu JJ. Variable selection in the Multivariate Adaptive Regression Splines (MARS)-logit models for detecting gene-gene interactions. Proc JSM 2006b:368.
Lockett KL, Hall MC, Clark PE, Chuang SC, Robinson B, Lin HY, Su LJ, Hu JJ. DNA damage levels in prostate cancer cases and controls. Carcinogenesis. 2006;27:1187-93.
Lodovici M, Caldini S, Luceri C, Bambi F, Boddi V, Dolara P. Active and passive smoking and lifestyle determinants of 8-oxo-7,8-dihydro-2'-deoxyguanosine levels in human leukocyte DNA. Cancer Epidemiol Biomarkers Prev. 2005;14:2975-7.
Lopez E, Guerrero R, Nunez MI, del Moral R, Villalobos M, Martinez-Galan J, Valenzuela MT, Munoz-Gamez JA, Oliver FJ, Martin-Oliva D, Ruiz de Almodovar JM. Early and late skin reactions to radiotherapy for breast cancer and their correlation with radiation-induced DNA damage in lymphocytes. Breast Cancer Res. 2005;7:R690-8.
Marchetti F, Coleman MA, Jones IM, Wyrobek AJ. Candidate protein biodosimeters of human exposure to ionizing radiation. Int J Radiat Biol. 2006;82:605-39.
McCloskey, S.A., et al., Radiation Treatment Interruptions Greater Than One Week and Low Hemoglobin Levels (12 g/dL) are Predictors of Local Regional Failure After Definitive Concurrent Chemotherapy and Intensity-Modulated Radiation Therapy for Squamous Cell Carcinoma of the Head and Neck. Am J Clin Oncol, 2009.
McGuire, K.P., et al., Are mastectomies on the rise? A 13-year trend analysis of the selection of mastectomy versus breast conservation therapy in 5865 patients. Ann Surg Oncol, 2009. 16(10): p. 2682-90.
McKeigue PM, Carpenter JR, Parra EJ, Shriver MD: Estimation of admixture and detection of linkage in admixed populations by a Bayesian approach: application to African-American populations. Ann Intern Med 2000;64:171-186.
Amendment 2: 11/23/2011 46 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Morris GJ, Naidu S, Topham AK, Guiles F, Xu Y, McCue P, Schwartz GF, Park PK, Rosenberg AL, Brill K, Mitchell EP. Differences in breast carcinoma characteristics in newly diagnosed African-American and Caucasian patients: a single-institution compilation compared with the National Cancer Institute's Surveillance, Epidemiology, and End Results database. Cancer. 2007;110:876-84.
Moullan N, Cox DG, Angele S, Romestaing P, Gerard JP, Hall J. Polymorphisms in the DNA repair gene XRCC1, breast cancer risk, and response to radiotherapy. Cancer Epidemiol Biomarkers Prev. 2003;12:1168-74.
Moye LA. P-value interpretation and alpha allocation in clinical trials. Ann Epidemiol 1998;8:351-7. Narayan S, Jaiswal AS, Kang D, Srivastava P, Das GM, Gairola CG. Cigarette smoke condensate-
induced transformation of normal human breast epithelial cells in vitro. Oncogene 2004;23:5880-9. Ottenbacher KJ. Quantitative evaluation of multiplicity in epidemiology and public health research.
Amer J Epidemiol 11998;47:615-9. Ou B, Huang D. Fluorescent approach to quantitation of reactive oxygen species in mainstream
cigarette smoke. Anal Chem. 2006;78:3097-103. Overgaard, M., et al., Postoperative radiotherapy in high-risk premenopausal women with breast
cancer who receive adjuvant chemotherapy. Danish Breast Cancer Cooperative Group 82b Trial. N Engl J Med, 1997. 337(14): p. 949-55.
Overgaard, M., et al., Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen: Danish Breast Cancer Cooperative Group DBCG 82c randomised trial. Lancet, 1999. 353(9165): p. 1641-8.
Pignol, J.P., et al., A multicenter randomized trial of breast intensity-modulated radiation therapy to reduce acute radiation dermatitis. J Clin Oncol, 2008. 26(13): p. 2085-92.
Pinar B, Lara PC, Lloret M, Bordon E, Nunez MI, Villalobos M, Guerrero R, Luna JD, Ruiz de Almodovar JM. Radiation-induced DNA damage as a predictor of long-term toxicity in locally advanced breast cancer patients treated with high-dose hyperfractionated radical radiotherapy. Radiat Res. 2007;168:415-22.
Poortmans, P.M., et al., Impact of the boost dose of 10 Gy versus 26 Gy in patients with early stage breast cancer after a microscopically incomplete lumpectomy: 10-year results of the randomised EORTC boost trial. Radiother Oncol, 2009. 90(1): p. 80-5.
Ragaz, J., et al., Locoregional radiation therapy in patients with high-risk breast cancer receiving adjuvant chemotherapy: 20-year results of the British Columbia randomized trial. J Natl Cancer Inst, 2005. 97(2): p. 116-26.
Reiner A, Yekutieli D, Benjamini Y. Identifying differentially expressed genes using false discovery rate controlling procedures. Bioinformatics 2003;19: 368-375.
Ryan JL, Bole C, Hickok JT, Figueroa-Moseley C, Colman L, Khanna RC, Pentland AP, Morrow GR. Post-treatment skin reactions reported by cancer patients differ by race, not by treatment or expectations. Br J Cancer. 2007;97:14-21.
Sagiv SK, Gaudet MM, Eng SM, Abrahamson PE, Shantakumar S, Teitelbaum SL, Britton JA, Bell P, Thomas JA, Neugut AI, Santella RM, Gammon MD. Active and passive cigarette smoke and breast cancer survival. Ann Epidemiol. 2007;17:385-93.
Savitsky K, Bar-Shira A, Gilad S, Rotman G, Ziv Y, Vanagaite L, Tagle DA, Smith S, Uziel T, Sfez S, Ashkenazi M, Pecker I, Frydman M, Harnik R, Patanjali SR, Simmons A, Clines GA, Sartiel A, Gatti RA, Chessa L, Sanal O, Lavin MF, Jaspers NG, Taylor AM, Arlett CF, Miki T, Weissman SM, Lovett M, Collins FS, Shiloh Y. A single ataxia telangiectasia gene with a product similar to PI-3 kinase. Science. 1995;268:1749-53.
Schick S, Glantz S. Philip Morris toxicological experiments with fresh sidestream smoke: more toxic than mainstream smoke. Tob Control. 2005a;14:396-404.
Schick S, Glantz S. Scientific analysis of second-hand smoke by the tobacco industry, 1929-1972. Nicotine Tob Res. 2005b;7:591-612.
Schwartz G. Estimating the dimension of a model. Ann Stat 1979;6:461-4. Seldin MF, Morii T, Collins-Schramm HE, Chima B, Kittles R, Criswell LA, Li H. Putative ancestral
origins of chromosomal segments in individual African Americans: implications for admixture mapping. Genome Res. 2004;14:1076-84.
Shiloh Y. ATM and ATR: networking cellular responses to DNA damage. Curr Opin Genet Dev 2001;11:71-7.

Amendment 2: 11/23/2011 47 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Shiloh Y. ATM and related protein kinases: safeguarding genome integrity. Nat Rev Cancer 2003;3:155–68.
Smith GC, d'Adda di Fagagna F, Lakin ND, Jackson SP. Cleavage and inactivation of ATM during apoptosis. Mol Cell Biol. 1999;19:6076-84.
Smith TR, Miller MS, Lohman KK, Case LD, Hu JJ. DNA damage and breast cancer risk. Carcinogenesis. 2003;24:883-9.
Speed T (ed.) Statistical analysis of gene expression microarray data. Chapman & Hall/CRC, 2003. Spierer, M.M., et al., Postmastectomy CT-based electron beam radiotherapy: dosimetry, efficacy, and
toxicity in 118 patients. Int J Radiat Oncol Biol Phys, 2004. 60(4): p. 1182-9. Spry M, Scott T, Pierce H, D'Orazio JA. DNA repair pathways and hereditary cancer susceptibility
syndromes. Front Biosci. 2007;12:4191-207. Stanton Al, Krishnan L, Collins CA. Form or Function? Part 1. Subjective cosmetic and functional
correlates of quality of life in women treated with breast conserving surgical procedures and radiotherapy. Cancer 2001; 91:2273-2281.
Steyerberg EW, Harrell Jr FE, Borsboom GJ, Eijkemans MJ, Vergouwe Y, Habbema JD. Internal validation of predictive models: efficiency of some procedures for logistic regression analysis. J Clini Epi 2001; 54:774-781.
Suga T, Ishikawa A, Kohda M, Otsuka Y, Yamada S, Yamamoto N, Shibamoto Y, Ogawa Y, Nomura K, Sho K, Omura M, Sekiguchi K, Kikuchi Y, Michikawa Y, Noda S, Sagara M, Ohashi J, Yoshinaga S, Mizoe J, Tsujii H, Iwakawa M, Imai T. Haplotype-based analysis of genes associated with risk of adverse skin reactions after radiotherapy in breast cancer patients. Int J Radiat Oncol Biol Phys. 2007;69:685-93.
Suwinski, R., et al., Time factor in postoperative radiotherapy: a multivariate locoregional control analysis in 868 patients. Int J Radiat Oncol Biol Phys, 2003. 56(2): p. 399-412.
Takata M, Sasaki MS, Sonoda E, Morrison C, Hashimoto M, Utsumi H, Yamaguchi-Iwai Y, Shinohara A, Takeda S. Homologous recombination and non-homologous end-joining pathways of DNA double-strand break repair have overlapping roles in the maintenance of chromosomal integrity in vertebrate cells. EMBO J. 1998;17:5497-508.
Tan XL, Popanda O, Ambrosone CB, Kropp S, Helmbold I, von Fournier D, Haase W, Sautter-Bihl ML, Wenz F, Schmezer P, Chang-Claude J. Association between TP53 and p21 genetic polymorphisms and acute side effects of radiotherapy in breast cancer patients. Breast Cancer Res Treat. 2006;97:255-62.
Twardella D, Popanda O, Helmbold I, Ebbeler R, Benner A, von Fournier D, Haase W, Sautter-Bihl ML, Wenz F, Schmezer P, Chang-Claude J. Personal characteristics, therapy modalities and individual DNA repair capacity as predictive factors of acute skin toxicity in an unselected cohort of breast cancer patients receiving radiotherapy. Radiother Oncol. 2003;69:145-53.
Ueda Y, Trung Duc Son le N, Inoue H, Kunii D, Yamamoto S, Azuma M. Relationship between smoking habits and serum oxygen radical absorbance capacity and dietary intake in Japanese adults. Clin Exp Pharmacol Physiol. 2004;31:S35-6.
Van Emburgh BO, Hu JJ, Levine EA, Mosley LJ, Case LD, Lin HY, Knight SN, Perrier ND, Rubin P, Sherrill GB, Shaw CS, Carey LA, Sawyer LR, Allen GO, Milikowski C, Willingham MC, Miller MS. Polymorphisms in drug metabolism genes, smoking, and p53 mutations in breast cancer. Mol Carcinog. 2007 Aug 7; [Epub ahead of print].
Viani GA, Stefano EJ, Afonso SL, De Fendi LI, Soares FV, Leon PG, Guimaraes FS. Breast-conserving surgery with or without radiotherapy in women with ductal carcinoma in situ: a meta-analysis of randomized trials. Radiat Oncol. 2007;2:28.
Walsh T, Casadei S, Coats KH, Swisher E, Stray SM, Higgins J, Roach KC, Mandell J, Lee MK, Ciernikova S, Foretova L, Soucek P, King MC. Spectrum of mutations in BRCA1, BRCA2, CHEK2, and TP53 in families at high risk of breast cancer. JAMA. 2006;295:1379-88.
Wheeler DL, Barrett T, Benson DA, Bryant SH, Canese K, Chetvernin V, Church DM, DiCuccio M, Edgar R, Federhen S, Geer LY, Kapustin Y, Khovayko O, Landsman D, Lipman DJ, Madden TL, Maglott DR, Ostell J, Miller V, Pruitt KD, Schuler GD, Sequeira E, Sherry ST, Sirotkin K, Souvorov A, Starchenko G, Tatusov RL, Tatusova TA, Wagner L, Yaschenko E. Database resources of the National Center for Biotechnology Information. Nucleic Acids Res. 2007;35:D5-12.

Amendment 2: 11/23/2011 48 CCCWF CCOP RESEARCH BASE PROTOCOL 97609
Wilding CS, Curwen GB, Tawn EJ, Sheng X, Winther JF, Chakraborty R, Boice JD Jr. Influence of polymorphisms at loci encoding DNA repair proteins on cancer susceptibility and G2 chromosomal radiosensitivity. Environ Mol Mutagen. 2007; Winer BJ, Brown DR, Michels KM. Statistical principles in experimental design. New York: McGraw-Hill, Inc, 1991;48:48-57.
Winer BJ, Brown DR, Michels KM. Statistical principles in experimental design. New York: McGraw-Hill, Inc, 1991.
Wong LS, Green HM, Feugate JE, Yadav M, Nothnagel EA, Martins-Green M. Effects of "second-hand" smoke on structure and function of fibroblasts, cells that are critical for tissue repair and remodeling. BMC Cell Biol. 2004;5:13.
Wood RD, Mitchell M, Lindahl T. Human DNA repair genes. Mutat Res. 2005;577:275-83. Yamazaki H, Inoue T, Koizumi M, Tanaka E, Yoshioka Y, Nakamura H, Shuo X, Inoue T. Urinary 8-
hydroxy-2'-deoxyguanosine excretion as a biomarker for estimating DNA oxidation in patients undergoing external radiotherapy and/or brachytherapy. Oncol Rep. 2005;13:847-51.
Yamazaki, H., et al., Radiotherapy for early glottic carcinoma (T1N0M0): results of prospective randomized study of radiation fraction size and overall treatment time. Int J Radiat Oncol Biol Phys, 2006. 64(1): p. 77-82.