implications for senior adults with prostate cancer in ... · 19.11.2015 1 saeu.cab.15.11.0097 (nov...
TRANSCRIPT

19.11.2015
1
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Implications for Senior Adults
with Prostate Cancer in Daily
Practice
Arti Hurria
Duarte, CA, USA
Material for Healthcare Professionals only
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)SA
EU
.CA
B.1
5.1
1.0
09
7 (N
ov 2
01
5)
Implications of
CHAARTED, STAMPEDE and RTOG-0521 trials
in daily practice
Droz JP et al. Lancet Oncol 2014;15:e404-14

19.11.2015
2
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
SIOG recommendations for
older adults with PCa
• Treatment recommendations for older men with PCa
should be based on:
Droz JP et al. Crit Rev Oncol Hematol 2010;73:68-91; Droz JP et al. BJU Int 2010;106:462-9;
Droz JP et al. Lancet Oncol 2014;15:e404-14
Health status (mainly driven by comorbidities)
Patient preferences
NOT chronological age
AND
“These care decisions should be made while taking into
account patient preference”
PCa: prostate cancer
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)SA
EU
.CA
B.1
5.1
1.0
09
7 (N
ov 2
01
5)
Key components for decision making
1. Capacity for decision making
2. Understand the treatment benefits
3. Understand the treatment risks
Making cancer treatment decisions in the context of the
patient’s goals, values, and preferences
Involvement of the multidisciplinary team
19.11.2015
3
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
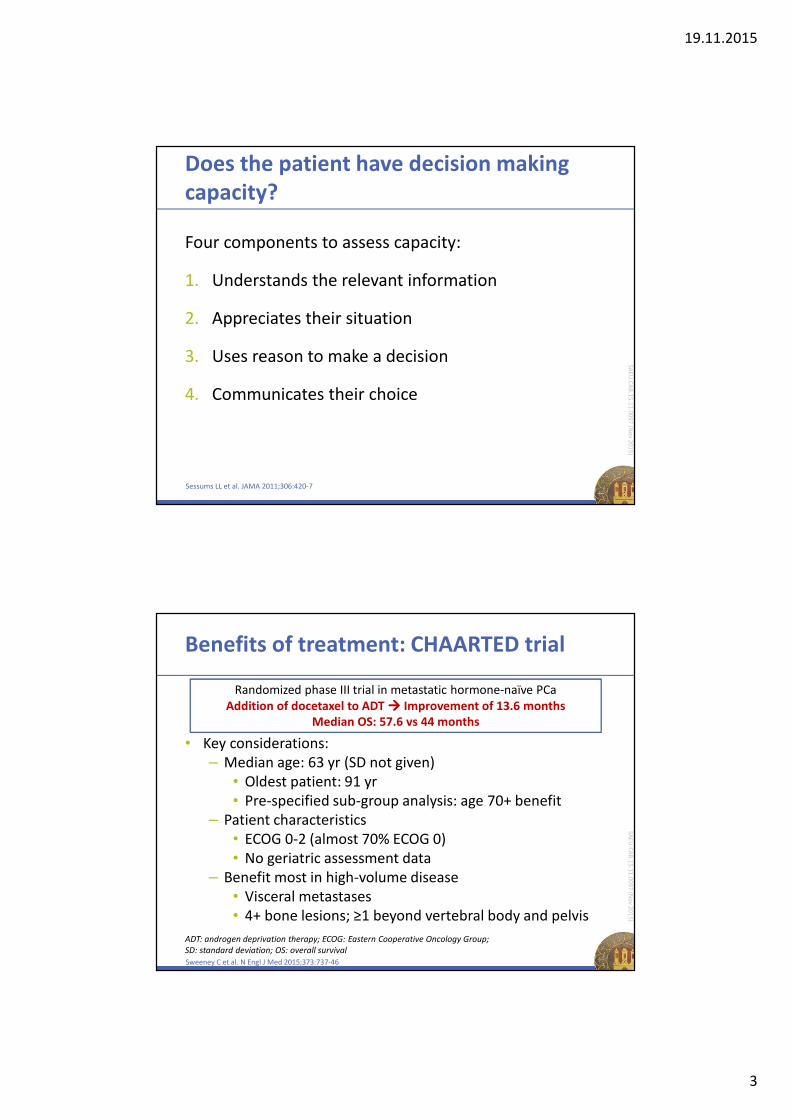
Four components to assess capacity:
1. Understands the relevant information
2. Appreciates their situation
3. Uses reason to make a decision
4. Communicates their choice
Does the patient have decision making
capacity?
Sessums LL et al. JAMA 2011;306:420-7
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Benefits of treatment: CHAARTED trial
• Key considerations:
– Median age: 63 yr (SD not given)
• Oldest patient: 91 yr
• Pre-specified sub-group analysis: age 70+ benefit
– Patient characteristics
• ECOG 0-2 (almost 70% ECOG 0)
• No geriatric assessment data
– Benefit most in high-volume disease
• Visceral metastases
• 4+ bone lesions; ≥1 beyond vertebral body and pelvis
Sweeney C et al. N Engl J Med 2015;373:737-46
Randomized phase III trial in metastatic hormone-naïve PCa
Addition of docetaxel to ADT ���� Improvement of 13.6 months
Median OS: 57.6 vs 44 months
ADT: androgen deprivation therapy; ECOG: Eastern Cooperative Oncology Group;
SD: standard deviation; OS: overall survival

19.11.2015
4
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Benefits of treatment: STAMPEDE trial
• Key considerations:
– Median age: 65 yr (SD not given)
• Oldest patient: 84 yr
– Patient characteristics
• “Fit for therapy:” WHO 0-2– 78% WHO 0
– Only 1% WHO 2
• No geriatric assessment data
James ND et al. J Clin Oncol 2015;33(15S): abstract 5001 (podium presentation ASCO 2015)
Randomized phase III trial in hormone-naïve PCa (M0/M1)
Addition of docetaxel to ADT ���� Improvement of 10 months
Median OS (M0/M1): 77 vs 67 months
Median OS (M1): 65 vs 43 months
WHO: World Health Organization
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Benefits of treatment: RTOG-0521 trial
• Key considerations:
– Median age: 66 yr
• SD and range not given
– High-risk disease:
• 53% Gleason 9-10
• 27% cT3-4
Sandler H et al. J Clin Oncol 2015;33(15S): abstract LBA5002
Randomized phase III trial in high-risk localized PCa
Addition of docetaxel to RT and ADT
4 year OS: 93% vs 89% (favoring chemotherapy arm)
RT: radiation therapy

19.11.2015
5
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Risks of treatment
CHAARTED1: 29.6% ≥ grade 3 toxicity
– 1% grade 3 motor/sensory neuropathy
– 4% grade 3 fatigue
– 6% grade 3-4 febrile neutropenia
– 2.3% grade 3-4 infection with neutropenia
STAMPEDE²: 51% ≥ grade 3 toxicity
– 12% grade 3 febrile neutropenia
– No data on fatigue and neuropathy
RTOG-0521³: 65% ≥ grade 3 toxicity
1. Sweeney C et al. N Engl J Med 2015;373:737-46; 2. James ND et al. J Clin Oncol 2015;33(15S): abstract 5001 (podium
presentation ASCO 2015); 3. Sandler H et al. J Clin Oncol 2015;33(15S): abstract LBA5002
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Who will benefit?
Estimating life expectancy
Walter LC. JAMA 2014;311:1336-47 (eAppendix 3) - Calculation from US 2010 Life Tables 10
20
16
12
9
64
15
11
8
54
3
9
64
32
1
0
5
10
15
20
25
70 year 75 year 80 year 85 year 90 year 95 year
Life
ex
pe
cta
ncy
(y
ea
rs)
Top 25th percentile (FIT seniors)
50th percentile (MEDIAN life expectancy)
Lowest 25th percentile (FRAIL seniors)
Age

19.11.2015
6
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
www.eprognosis.org
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
ONCODAGE – G8
• Cut-off: abnormal if ≤14
• Sensitivity: 76.6%
• Specificity: 64.4%
• Reproducibility: kappa:
0.65
• Duration of the test:
4.4 minutes
Bellera CA et al. Ann Oncol 2012;23:2166-72; Kenis C et al. J Clin Oncol 2014;32:19-26
http://espacecancer.sante-ra.fr/oncogeriatrie/default.aspx (access Nov 4 2015)

19.11.2015
7
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
ONCODAGE – G8 impact on OS
Kenis C et al. J Clin Oncol 2014;32:19-26
Ove
rall
surv
iva
l (p
rob
ab
ility
)
Time (months)
No. at risk
Normal 240 219 202 177 126 67 22
Abnormal 697 517 420 324 208 104 23
1.0
0.8
0.6
0.4
0.2
0 10 20 30 40
Normal
Abnormal
Log-rank P < .001
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Droz JP et al. Lancet Oncol 2014;15:e404-1414
>14
No geriatric
assessment
requested
≤14
Geriatric
assessment
requested
G8 Screening
VULNERABLE FRAILFIT
GERIATRIC INTERVENTIONS
Not reversibleReversible
19.11.2015
8
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
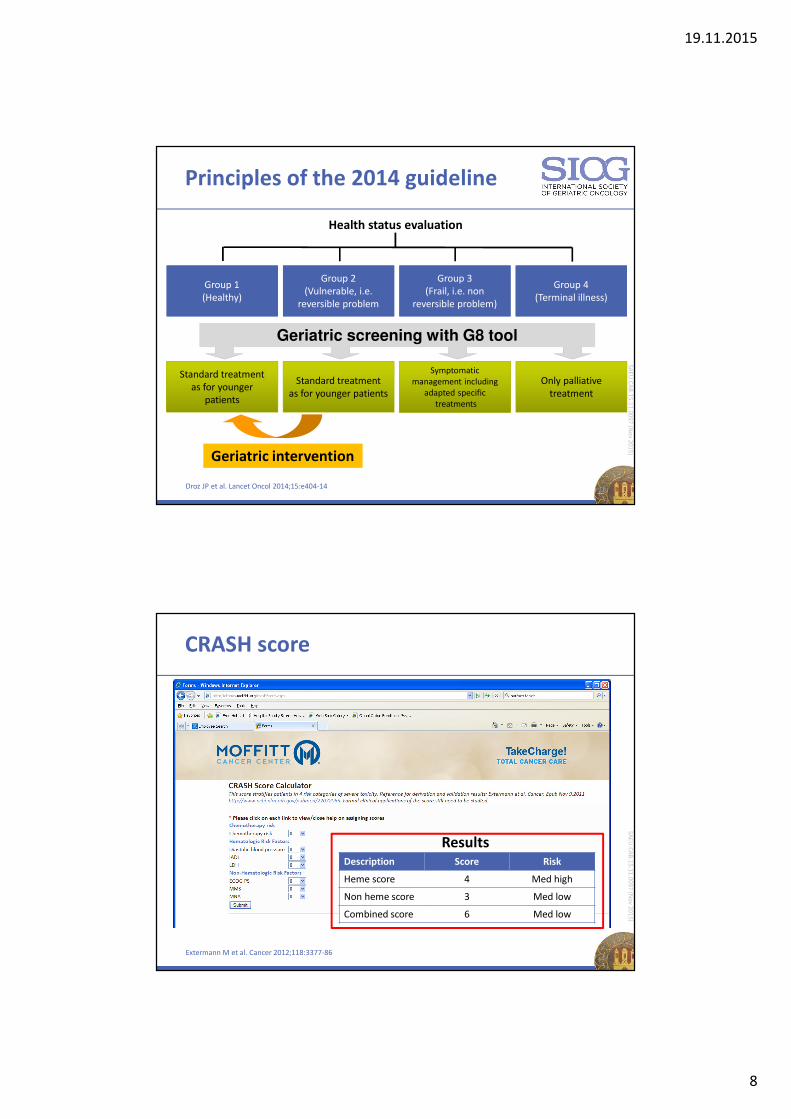
Principles of the 2014 guideline
Droz JP et al. Lancet Oncol 2014;15:e404-14 15
Health status evaluation
Geriatric intervention
Standard treatment
as for younger
patients
Standard treatment
as for younger patients
Symptomatic
management including
adapted specific
treatments
Only palliative
treatment
Group 1
(Healthy)
Group 2
(Vulnerable, i.e.
reversible problem
Group 3
(Frail, i.e. non
reversible problem)
Group 4
(Terminal illness)
Geriatric screening with G8 tool
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
CRASH score
Extermann M et al. Cancer 2012;118:3377-86
ResultsDescription Score Risk
Heme score 4 Med high
Non heme score 3 Med low
Combined score 6 Med low

19.11.2015
9
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
CARG toxicity calculator
Hurria A et al. J Clin Oncol 2011;29:4217-8
http://www.mycarg.org/Chemo_Toxicity_Calculator (access Nov 4 2015)
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Placing decision in the context of
the patient’s goals, values, and preferences

19.11.2015
10
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Functional status
Comorbidities
Finances
Age
Individual’s
treatment decision
Cancer stage
Psychological status
Cancer therapeutics
Organ function
Cognition
Spirituality
Polypharmacy
Social support
Culture Literacy
Key factors contributing to decision
making
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Knowledge gaps:
Opportunities for geriatric oncology
1. Geriatric assessment data needed to weigh the risk and
benefits
• Functional vs chronological age
2. Additional outcomes of relevance:
• Impact of therapy on function
3. Additional data regarding toxicities (including grade 2)
• Neuropathy, fatigue
4. Tolerance of therapy in age 75+
5. Treatment of individuals who did not meet eligibility for
these studies (i.e. vast majority had PS 0)
6. Geriatric assessment guided interventions to improve
treatment tolerancePS: Performance status

19.11.2015
11
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Geriatrics OncologyGeriatric oncology
Thank you!SA
EU
.CA
B.1
5.1
1.0
09
7 (N
ov 2
01
5)
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)
Evaluation form
• Please fill in the evaluation form and hand it over to
the staff as you leave the room

19.11.2015
12
SAE
U.C
AB
.15
.11
.00
97
(No
v 20
15
)SA
EU
.CA
B.1
5.1
1.0
09
7 (N
ov 2
01
5)
?
?
?
QuestionsSA
EU
.CA
B.1
5.1
1.0
09
7 (N
ov 2
01
5)