in the know: her2+ - lbbc.org slides_06.25.18.pdf · 100 92.6 80 60 40 20 2 years 0 0 1 2 3 4 5 6 7...
TRANSCRIPT

In the know: HER2+
Sara M. Tolaney, MD, MPH
Dana-Farber Cancer Institute

All Breast Cancers
Triple negative
15%
ER+ 65%-75%
HER2+ 15%-20%
2
Clinical Breast Cancer Subtypes

Milestones in HER2+ Breast Cancer
Trastuzumab for ABC
Trastuzumab for EBC
Lapatinib for ABC
Pertuzumab for ABC
T-DM1 for ABC
Pertuzumab for preop therapy
Pertuzumab for EBC
Neratinib for EBC
1998 2005 2007 2012 2013 2017

First-Generation Adjuvant Trastuzumab Trials
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute

What standard therapy?
• Both ACTH and TCH are effective, and TCH
should be considered in patients with risk
factors for cardiac toxicity

OBSERVATION n=1698
Women with locally determined HER2-positive invasive early breast cancer
Surgery + (neo)adjuvant CT ± RT
Centrally confirmed IHC 3+ or FISH+ and LVEF ≥ 55%
Randomization
1 year Trastuzumab 8 mg/kg – 6 mg/kg 3 weekly schedule
n=1703
2 years Trastuzumab 8 mg/kg – 6 mg/kg 3 weekly schedule
n=1701
After ASCO 2005, option of switch to Trastuzumab
HERA TRIAL DESIGN Accrual 2001 – 2005 (n=5102)
CT, chemotherapy; RT, radiotherapy
M Piccart SABCS 2012

Overa
ll S
urv
ival
(%)
Years from randomization No. at risk
Trastuzumab 2 years 1553 1553 1525 1485 1438 1382 1317 1193 708 208
Trastuzumab 1 year 1552 1552 1513 1461 1413 1364 1329 1218 732 225
100
80
60
40
20
0
0 1 2 3 4 5 6 7 8 9
OS FOR 2 YEARS VS. 1 YEAR TRASTUZUMAB AT 8 YRS MFU
97.4%
96.5% 91.4%
92.6% 86.4%
87.6%
Trastuzumab 1 year
Trastuzumab 2 years
Pts Events HR (2 vs 1) 95% CI p-value
2 years 1553 196 1.05 (0.86-1.28) 0.63
1 year 1552 186

Optimal Duration of Trastuzumab
PHARE Study Non-inferiority study; pre-specified HR 1.15
HR = 1.28 (p = 0.29) 2 yr DFS: Tras 12 mos = 93.8% Tras 6 mos = 91.1%
6 months inferior to 12 months of trastuzumab
n = 3,380
FINHER study Subset with HER2+ disease
HR = 0.42 (p = 0.01) 3 yr RFS: Tras 9 weeks = 89% No Tras = 78%
Benefit for only 9 weeks of trastuzumab

Persephone Study Design
Presented By Helena Earl at 2018 ASCO Annual Meeting

Disease-free survival
Presented By Helena Earl at 2018 ASCO Annual Meeting

Duration of anti-HER2 therapy?
• 12 months of trastuzumab remains the
standard, though consideration of
shorter duration in patients who
experience toxicity on therapy is
reasonable

Can we do better?
• Adding targeted agents
– Pertuzumab
– Neratinib

HER2 receptor
Trastuzumab
Pertuzumab
Dimerisation domain of HER2
• Inhibitor of HER dimerization: binds HER2 and prevents formation of homo- or heterodimers
• Suppresses activation of several intracellular signaling cascades driving cancer cell growth
Another “add on” strategy: pertuzumab?

NEOSPHERE1 TRYPHAENA2 TRYPHAENA2
Treatment
Pertuzumab,
Trastuzumab,
Docetaxel
THP x 4
FEC x 3 post-op)
Docetaxel/Carbo/Trast
uzumab/Pertuzumab
TCHP x 6
FEC x 3 THP x 3
N 107 77 75
ypT0/is ypN0 (%) 39.3 63.6 54.6
Neoadjuvant Pertuzumab/Trastuzumab (3 regimens FDA approved 9/2013)
1. Gianni L, et al. Lancet Oncol. 2012;13:25-32. 2. Schneeweiss A, et al. Ann Oncol. 2013;24:2278-2284.

APHINITY: Randomized Adjuvant Phase 3 Trial
A=doxorubicin, E=epirubicin, C=cyclophosphamide, T=taxane (paclitaxel or docetaxel), F=5-fluorouracil, H=trastuzumab, P=pertuzumab
N=3800 planned (4800 enrolled)
trastuzumab + pertuzumab* x 1 year
S
U
R
G
E
R
Y
Central confirmation
of HER2 status
ACT or TCH
trastuzumab + placebo* x 1 year
ACT or TCH
*antibody therapy starts with taxane
Population: Node + or high risk node negative
Von Minckwitz et al. ASCO 2017 Abs LBA500

APHINITY: Disease-Free Survival
4yr iDFS: HR = 0.81 (p = 0.045)
Absolute benefit = 1.7%
Δ % (H/P vs. H)
Absolute Δ
N0 96.7 v 96.2% 0.5%
N1 89.9 v 86.7% 3.2%
ER/PR+ 93 v 91.6% 1.4%
ER/PR- 91 v 88.7% 2.3%
iDFS subset analysis
*No difference in iDFS by type of chemotherapy
von Mickwitz G et al, ASCO 2017

Who should get adjuvant pertuzumab?
• Should be reserved for high-risk patients:
– Node-positive
– Hormone-receptor negative

Can we do better?
• Adding targeted agents
– Pertuzumab
– Neratinib

Neratinib
• Low-molecular-weight, irreversible, pan-HER inhibitor (ErbB1,2,4)
Neratinib
Burstein et al JCO. 2010. 28:1301

ExteNET Study Design
• Primary endpoint: invasive disease-free survival (iDFS)a
• Secondary endpoints: overall survival, DFS-DCIS, distant DFS, time to distant recurrence, CNS metastases, safety,
• Stratification: nodes 0, 1-3 vs 4+, ER/PR status, concurrent vs sequential trastuzumab
• Study blinded: Until primary analysis; OS remains blinded
Neratinib × 1 yr 240 mg/day
n=1420
Placebo × 1 yr n=1420
Randomize 1:1
N=2840 Primary analysis
iDFSa
Extended follow-up:
5-yr for iDFS &
overall survival
Prior adjuvant trastuzumab
2 years
a All iDFS events up to the cutoff date of 2 years + 28 days for each patient were included in the primary analysis.

0 12 24 36 48 60
Months after randomization
Neratinib
Placebo
HR (95% CI): 0.95 (0.66-1.35) Two-sided P=0.762
604 559 541 520 464 407 400 391 384 376 362
605 575 548 529 495 448 444 435 427 416 402
97.5%
94.7% 92.8%
91.8% 90.8%
90.4% 89.9%
89.3% 88.8%
88.9%
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 12 24 36 48 60
Dis
ea
se
-fre
e s
urv
iva
l
Months after randomization
Neratinib
Placebo
HR (95% CI): 0.60 (0.43-0.83) Two-sided P=0.002
At risk
Neratinib 816 757 731 705 642 571 565 558 554 544 523
Placebo 815 779 750 719 647 581 567 556 551 542 525
iDFS by Hormone Receptor Status 5-Year Analysis
98.1%
96.1% 95.4%
91.7% 4.4% Δ
93.6%
89.8%
92.6%
88.5%
91.2%
86.8%
Hormone receptor positive Hormone receptor negative
(Descriptive P value)

Antidiarrheal Prophylaxis Reduces the Incidence and Severity of Diarrhea
ExteNET and Study 6201 (CONTROL)
22%
24% 23%
31%
5%
23%
32%
40%
None
Grade 1
Grade 2
Grade 3
25%
28% 27%
20%
ExteNET n=1408
Loperamide n=137
Loperamide + budesonide n=64
46%
26%
20%
8%
Colestipol + loperamide n=39

Can we do better?
• Adding targeted agents
– Pertuzumab
– Neratinib
• Improvement in DFS within hormone-
receptor positive patients, but associated
with increased toxicity
• Unclear if benefit would persist after
pertuzumab

Can we deescalate therapy?
• Small HER2+ tumors

APT Trial: Study Design
HER2+
ER+ or ER-
Node Negative
< 3 cm
Enroll
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
T
P
PACLITAXEL 80 mg/m2 + TRASTUZUMAB 2 mg/kg x 12
T T T T T T T T T T T T T
FOLLOWED BY 13 EVERY 3 WEEK DOSES
OF TRASTUZUMAB (6 mg/kg)*
Planned N=400
*Dosing could alternatively be 2 mg/kg IV weekly for 40 weeks
** Radiation and hormonal therapy was initiated after completion of paclitaxel
Tolaney SM et al, ASCO 2017

APT: Recurrence Free Interval
Time (Months)
Re
cu
rre
nce
-Fre
e In
terv
al
0 12 24 36 48 60 72 84 96
0.0
0.2
0.4
0.6
0.8
1.0
0 12 24 36 48 60 72 84 96
0.0
0.2
0.4
0.6
0.8
1.0
All patientsNumber at risk
406 388 385 378 362 347 247 120 34
RFI Events=
•Invasive Local/Regional Recurrence
•Distant Recurrence
•Death from Breast Cancer
Point Est. 95% Conf. Interval No. of
events
3-yr RFI 99.2% 98.4% to >99.9% 3
5-yr RFI 98.1% 96.8% to 99.5% 7
7-yr RFI 97.5% 95.9% to 99.1% 9
Tolaney SM et al, ASCO 2017

APT: Implications
• Paclitaxel and trastuzumab (TH) can be considered a
reasonable and appealing approach for the majority of
patients with stage I HER2+ breast cancer
– Not all patients require adjuvant trastuzumab-based
chemotherapy (particularly T1aN0)
– Standard regimens from the pivotal trials can be
considered for patients with particularly high risk
features
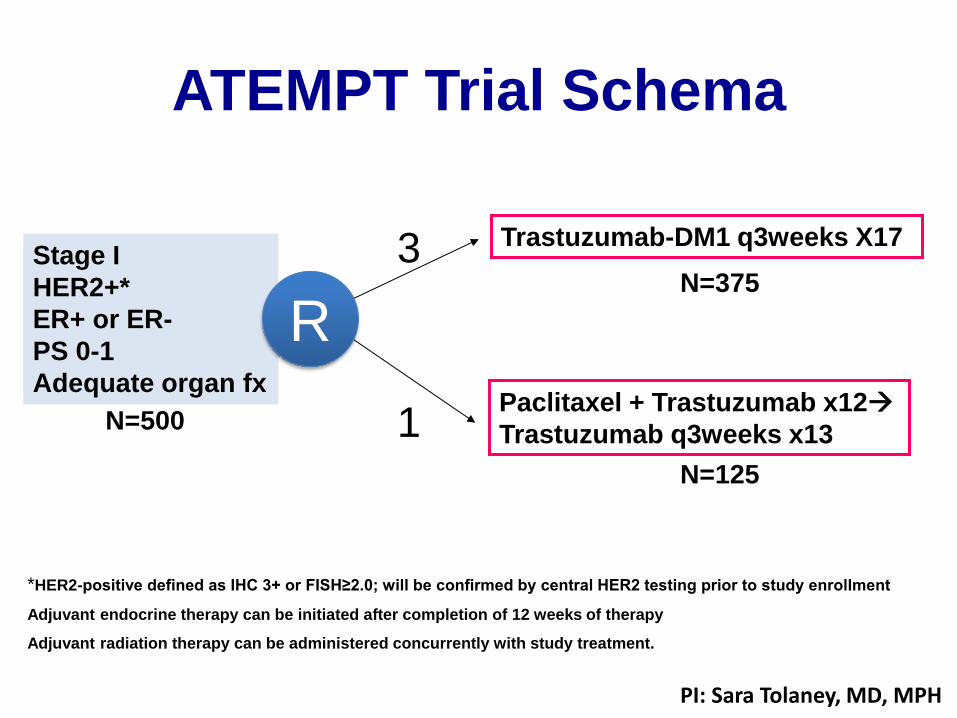
ATEMPT Trial Schema
Stage I
HER2+*
ER+ or ER-
PS 0-1
Adequate organ fx
N=500
Trastuzumab-DM1 q3weeks X17
*HER2-positive defined as IHC 3+ or FISH≥2.0; will be confirmed by central HER2 testing prior to study enrollment
Adjuvant endocrine therapy can be initiated after completion of 12 weeks of therapy
Adjuvant radiation therapy can be administered concurrently with study treatment.
Paclitaxel + Trastuzumab x12
Trastuzumab q3weeks x13
N=375
N=125
R
3
1
PI: Sara Tolaney, MD, MPH

Summary: Early Stage Disease
• Trastuzumab significantly improves survival in both adjuvant and neoadjuvant setting
• Pertuzumab can be considered in patients with node-positive and hormone-receptor negative disease
• Neratinib can be considered in high risk ER+ patients
• TH is a reasonable standard for stage I disease

Survival with HER2+ Metastatic Disease

CLEOPATRA Study Design
HER2-positive MBC centrally confirmed
(N = 808)
Placebo + trastuzumab
1:1
Docetaxel
≥ 6 cycles
n = 406
n = 402
Pertuzumab + trastuzumab
Docetaxel
≥ 6 cycles
PD
PD
Baselga J, et al. N Engl J Med 2012; 366:109–119.
• Randomization stratified by geographic region and
neo/adjuvant chemotherapy
• Study dosing q3w:
– Pertuzumab/placebo: 840 mg loading → 420 mg maintenance
– Trastuzumab: 8 mg/kg loading → 6 mg/kg maintenance
– Docetaxel: 75 mg/m2 → 100 mg/m2 escalation if tolerated

CLEOPATRA: Final OS Analysis Median follow-up 50 months (range 0–70 months)
ITT population. Stratified by geographic region and neo/adjuvant chemotherapy.
CI, confidence interval; Pla, placebo; Ptz, pertuzumab. 32
OS
(%)
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 70 60
Time (months)
HR 0.68 95% CI = 0.56, 0.84
p = 0.0002
Ptz + T + D
Pla + T + D
1 28 104 226 268 318 371
0 23 91 179 230 289 350
n at risk
Ptz + T + D
Pla + T + D
402
406
40.8 months 56.5
months Δ 15.7
months
Swain et al, ESMO 2014
ORR
80.2%
69.3%
p=0.001

Pertuzumab for Advanced HER2+ Disease
• Standard of care to give chemotherapy with HP for first line therapy
– Taxane (Docetaxel or paclitaxel) or Vinorelbine
• Use of pertuzumab in the 2nd line setting in a patient who never received pertuzumab is reasonable
• No data for use of pertuzumab beyond progression

Trastuzumab Emtansine (T-DM1)
• T-DM1 is a novel antibody drug-
conjugate.
• Trastuzumab linked to DM1, a
microtubule inhibitor
• T-DM1 binds to HER2 with affinity
similar to trastuzumab
LoRusso Pet al, Clinical Cancer Research 2011

T-DM1: Standard 2nd line therapy
1:1
HER2+ (central) LABC or MBC
(N=980)
• Prior taxane and trastuzumab
• Progression on metastatic tx or within 6 mos of adjuvant tx
T-DM1
Capecitabine + Lapatinib
Dieras V et al, Lancet Oncology 2017
EMILIA
Overall Survival

SYD985: [vic-]trastuzumab duocarmazine
• HER2-targeting antibody-drug conjugate (ADC) based on trastuzumab
• Protease cleavable linker with a DNA alkylating toxin duocarmycin
• Toxin incorporated into the linker-drug as an inactive prodrug
• Proteolytic cleavage results in release of the membrane permeable active toxin
http://clicktoeditURL.com

37
Trastuzumab Deruxtecan (DS-8201a)

Her2-Directed ADCs Agent Payload Drug to
Antibody Ratio
Phase of Development
ORR in HER2+
ORR in HER2 low
Trastuzumab-DM1 (T-DM1) 1
DM1 (antitubulin)
3.5 FDA Approved 43.6% ------
Trastuzumab Duruxtecan (DS-8201A)2
Exatecan derivative (topoisomerase I)
8 II/III (NCT03248492)
61.4% 31.6%
SYD9853 Duocarmacine derivative (alkylator)
2.8 III (NCT03262935) 33% 31%
XMT-15224 Monomethyl Auristatin F (antitubulin)
12 I (NCT02952729) unknown unknown
ARX788 Amberstatin 269 (AS269) (antitubulin)
1.9 I (NCT03255070) unknown unknown
DHES0815A Pyrrolo[2,1-c][1,4]benzodiazepine monoamide (PBD-MA) (alkylator)
2 I (NCT03451162) unknown unknown
MEDI-4276 Tubulysin (antitubulin)
3.6 I (NCT02576548) unknown unknown
1Verma S et al, NEJM 2012, 2Modi S et al, SABCS 2017 3Saura C et al, ASCO 2018,4Yurkovetskiy A et al, AACR 2017

Novel Approaches
• Cdk 4/6 Inhibitors
• HER2 TKIs
• Immunotherapy

• HR+/HER2+ MBC
• No prior treatment in the advanced setting beyond induction treatment
• No evidence of disease progression after induction treatment
Anti-HER2 Therapy + Endocrine Therapy
Palbociclib + Anti-HER2 Therapy +
Endocrine Therapy
N=496
Abemaciclib 150 mg
Q12hr PO +
fulvestrant +
trastuzumab
Trastuzumab +
physican’s choice
single agent
chemotherapy
N = 225
R
A
N
D
O
M
I
Z
E
1:1:1
Abemaciclib 150 mg
Q12hr PO +
trastuzumab
monarcHER
PI: Otto Metzger
Can the addition of cdk 4/6 inhibition to anti-HER2 therapy improve outcomes for ER+ HER2+
disease?

Tucatinib – Potent & Selective HER2
Inhibitor Additive with multiple SOC agents in preclinical models
Demonstrated clinical activity in HER2+ patients
Superior safety profile in patients
Improved convenience of an oral drug vs. IV mAbs
Compound
Cellular Selectivity Data
HER2
IC50 (nM)
EGFR
IC50 (nM)
p95 HER2
IC50 (nM)
HER2 IC50 (nM)
50% Human Serum
Tucatinib 8 4000 7 67
Neratinib 7 8 NT 39
Lapatinib 49 31 NT 810
HN
HN
O
N
N
N
NN
N
O
Tucatinib

HER2Climb: Does tucatinib add to trastuzumab/capecitabine?

Loi et al, SABCS 2017

Loi et al, SABCS 2017

Current Approach for Metastatic HER2+ Breast Cancer
1st Line 2nd Line 3rd Line -10th Line+
THP ( ET if ER+) T-DM1 Capecitabine + lapatinib
Chemotherapy + Trastuzumab
Endocrine therapy (ET) + HL or HP
THP + PD-L1
THP ET+ palbociclib
DS8201A Capecitabine + Trastuzumab + Tucatinib
DS8201A
SYD985
Capecitabine + Neratinib
Capecitabine + Pyrotininb
Abemaciclib + Trastuzumab (+Fulvestrant)
Margetuximab + Chemotherapy
Potential Future Therapy Options

Summary • The addition of pertuzumab to trastuzumab and capecitabine in the 2nd
line does not result in a statistically significant improvement in PFS or OS, but there is a trend to benefit in OS
– Consideration of addition of pertuzumab to chemotherapy and trastuzumab in a pertuzumab-naïve patient beyond the first line is reasonable
• T-DM1 remains a standard in the 2nd line setting, but several new ADCs are in development
– Phase 3 studies ongoing with SYD985 and DS8201a
• Several new tyrosine kinase inhibitors in development being explored with capecitabine, including tucatinib which is more specific for HER2
• Work ongoing exploring immunotherapy and cdk 4/6 inhibitors