increasing the use of midlines in place of central lines...
TRANSCRIPT
Increasing the Use of Midlines in Place of Central Lines: Pros and Cons
Ruth Carrico PhD APRN FNP-C CIC Associate Professor
University of Louisville School of Medicine

Objectives
• Review some of the basic points about bloodstream infection and intravascular devices
• Address the controversy surrounding Midline v. Central Venous Catheters as a CLABSI prevention strategy

Objectives • Review some of the basic points about
bloodstream infection and intravascular devices
• Address the controversy surrounding Midline v. Central Venous Catheters as a CLABSI prevention strategy

3
1 = 60%
2 = 12%
3 = <1%
Unk = 28%
Safdar N, Maki DG. The pathogenesis of catheter-related bloodstream infection with noncuffed short-term central venous catheters. Int Care Med. 2004;30:62-67.
Skin organisms Endogenous Skin flora Extrinsic HCW hands or Contaminated disinfectant
Contaminated catheter hub Endogenous Skin flora Extrinsic HCW hands
Contaminated Infusate Extrinsic Fluid or Medication Intrinsic Manufacturer
Hematogenous from distant infection
Skin Vein
Fibrin sheath, thrombus

Femoral Vein Last choice
Subclavian Vein First Choice
Internal Jugular Second choice
Traditional Sites for Central Venous Catheter

CVL Insertion Bundle Component: Maximum Sterile Barrier Precautions
Hat and mask
Persons within 6 feet also wear head cover and mask
Sterile gown
Sterile gloves

CVL Insertion Bundle Component: Skin Preparation
• Gross debris or dirt should be removed
– with an alcohol pad, prior to using the skin preparation
– by washing with soap and water, prior to using the skin preparation
• Clean with friction for minimum of 30 seconds
• Allow preparation to completely dry, before procedure for best results.
• DO NOT REMOVE skin preparation after the procedure is completed.

Central Line- Associated
Bloodstream Infection
Poor/ImproperTechnique
Line Colonization/Contamination
Number ofCatheters and/or
Lumens
AntibioticUsage
ContaminatedSupplies
EducationStaffing
Acuity/TimeSite Selection
Lack of hand hygiene
Line inserted without
using sterile technique
Dressing not changed on time
Dressing not occlusive or lacking correct use
of chlorhexidine sponge
Line accessed withoutclean technique including adequate
disinfection of access site
Poor technique when obtaining blood cultures
More lumens on line than needed
Line not needed but not removed
More than one
central venous catheter
Inadequate gown, mask, gloves or hair
covering during insertion
Appropriate skin disinfectant not
used or not allowed to dry prior to
line insertion
Line manipulation or adjustment
Multiple attempts
Breaks in sterile technique
Inadequateuse of maximum draping prior
to insertion
Treatment basedon false positive/contaminatedblood cultures
Blood cultures drawn through
line and results
questionable
Antibiotic use outside hospital
guidelines
Blood leftIn line/end cap
Line from ED/field not changed
Blood at insertion site not
removed
Vascular end caps not
changed or changed too frequently
Blood left in end caps
IV tubing hanging without covered end
IVF and components not changed
according to policy
Dressing changes done without appropriate
supplies
Improper technique when using ultrasound devices
during line insertion
Reuse of single-use items
Inexperienced clinicians
Resident unfamiliar with policy
Nurses do not know dressing change
due; no dates on dressing
Policies not written or not current
Supplemental staff unaware of
policy/lack training
Policy unavailable to medical staff
Medical staff not supportive of policies
Internaljugular or femoral site used
Insertion site near
tracheostomy
Nurses too busy to change
dressingMD inserts
line alone-too busy to get
nurse assistance
Supplemental nursing staff
Inexperienced nursing staff
Other opportunity for dressing
Contamination
Midline v. PICC
Line inserted via undesirable
site (i.e., femoral) not changed
Lack of data to demonstrate outcomes/adherence
High patient volume/acuity
Poor environmental conditions
Use of multi-dose vials without attention to
safe injection practices
Use of contaminated supplies(e.g., dropped or used multiple
times during procedure
Kits do not contain all needed items
Line remains inbut no longer
needed
Investigating Practices to Prevent CLABSI (Do we have problems with….)
Ruth Carrico PhD APRN FNP-C CIC University of Louisville School of Medicine, Division of Infectious Diseases [email protected] Rev 08/16
5 Rights of Intravascular Devices
Every patient has the RIGHT to best practice care 1. Right device for that individual patient 2. Right route of the device based on the intended
use of the device 3. Right device for the medication to be
administered 4. Right device for the dose of medication to be
given 5. Right timing for the device
1. Right Device for That Individual Patient
• Early assessment – Before central access device is placed – Vessel health – Anticipatory care – Short term versus long term use – Risks associated with the device(s)

2. Right Route of the Device Based Upon the Intended Use of the Device
• What is the intended use of the device – Short term versus long term – Anticipated difficulty with device insertion – Risk for adverse events associated with a long
term v. short term device – Existing skill of those caring for the device – Existing skill of those choosing the type of device – Existing skill of those inserting the device

Why Do These Patient Develop BSI?
• Site care • Access technique • Care of junction sites and access ports • Hand hygiene of personnel • Medication administration • Intrinsic patient factors

Some Prefilled Saline Syringes Are for Flushing ONLY • The saline flush syringes in the clear cellophane package is
ONLY for flushing – According to the manufacturer, DO NOT use for
medication dilution. • The inside of the barrel & the fluid pathway is all that is sterile on
these syringes. • When you push out saline, the outer side of the plunger
contaminates the inside of the barrel. • Then, when you draw back into the syringe, you are pulling the
plunger over areas that were just contaminated. • If you do this, you could be pushing pathogens into the patients’
bloodstreams.
• The saline flush syringes in the sterile peel pack may be used for medication dilution.

Disconnecting tubing Sterile end cap in place
Not recommended by manufacturer. Off-label use.
How do you know if the tubing tip is still sterile?
Indicates tip sterility maintained
B
C A
D
Traditional Central Venous Catheter Placement

Peripherally Inserted Central Catheter

Midline Catheter

Diameter of vessel for Midline
Diameter of vessel for PICC
3. Right Device for the Medication
• What medication are anticipated to be administered – Hydration using non-irritating fluids – Irritants or vesicants – Nutrition (10% dextrose or greater) – Length of time medication anticipated to be
needed – What if therapy fails and next line drugs needed – Lab draws?

4. Right Device for the Dose
• What are anticipated doses – Escalating therapy – Increased nutrition (10% dextrose or greater) – Increasing time intervals or continuous therapy – What if therapy fails and next line drugs needed – Lab draws?
5. Right Timing for the Device
• Changes in patient condition – Anticipated course of illness – Ability to identify alternatives for infusion therapy – Comorbidities – Other medications or combinations

Midlines v. Central Catheters
• Challenges – Prevent CLABSI (reporting) – Prevent adverse events (no reporting required)
• What is the real question?
– What drives decision regarding line selection – Will attention to care of the device and reduced
rates of complication/infection change the approach

How to Make a Patient-Centered Decision
• Existing data (not perception) – Outcome data – Process data
• Performance Improvement • Implementation Sciences

A Problem WHAT
How
Where
Who
When
Why

Plan-Do-Study-Act Enables Testing of Change in a Real World Setting
• Plan: – Identify existing processes that have
resulted in the current results – Design/redesign workflow to incorporate
desired changes; – Determine metrics to demonstrate
results – Identify tools to support the new design;
• Do: Implement the plan • Study: Look at the metrics; determine
results
• Act: Fix any “misses” in the process and repeat the process
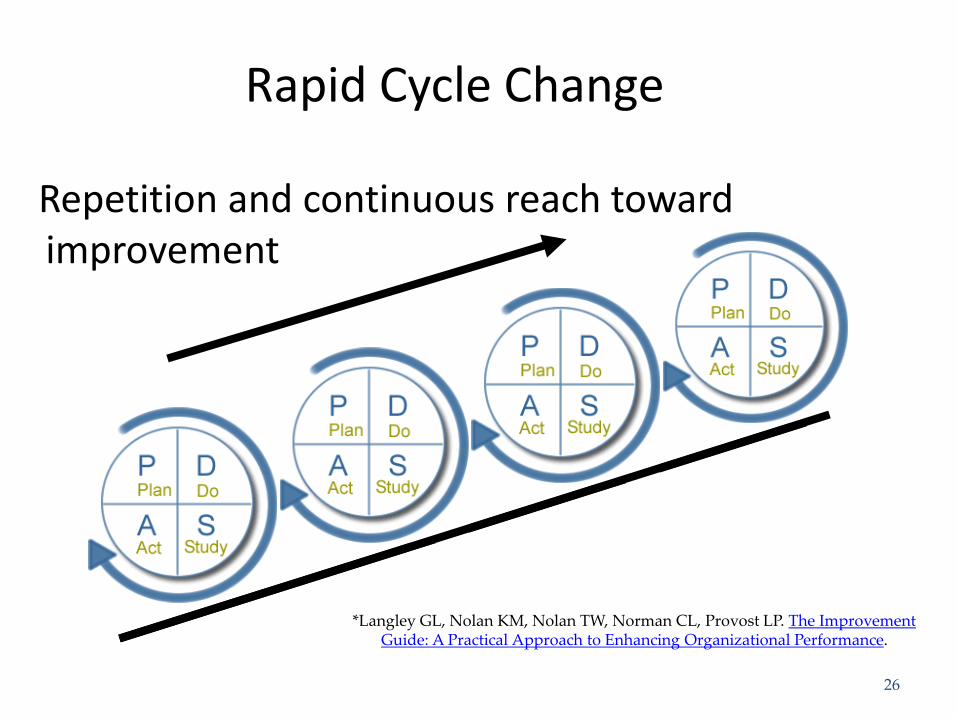
Rapid Cycle Change
Repetition and continuous reach toward improvement
*Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance.
26
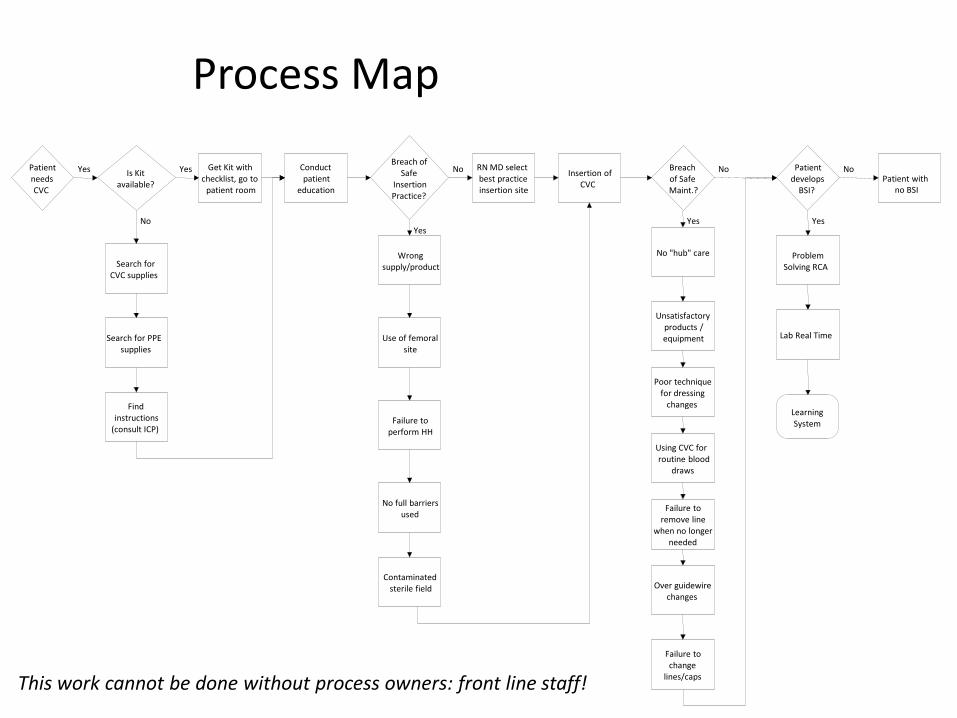
Process Map
Patient needs CVC
Is Kit available?
Yes Get Kit with checklist, go to
patient room
Yes Conduct patient
education
Breach of Safe
Insertion Practice?
RN MD select best practice insertion site
No Insertion of CVC
Breach of Safe Maint.?
Search for CVC supplies
No
Search for PPE supplies
Find instructions
(consult ICP)
Wrong supply/product
Yes
Use of femoral site
Failure to perform HH
No full barriers used
Contaminated sterile field
No "hub" care
Yes
Unsatisfactory products / equipment
Poor technique for dressing
changes
Using CVC for routine blood
draws
Failure to remove line
when no longer needed
Over guidewire changes
Failure to change
lines/caps
Patient develops
BSI?
No Patient with
no BSI
No
Problem Solving RCA
Yes
Lab Real Time
Learning System
This work cannot be done without process owners: front line staff!
Implementation of Improvements
• Applying quality improvement strategies • Measure results before and after • Use many of the same designs to study ability
to apply and sustain change • Evaluation of interventions is the most
important step • Do not substitute a care process that may be
less than ideal simply to prevent reporting of results associated with an ideal process

Resources • Masters, B., Hickish, T., & Uña Cidon, E. (2014). A midline
for oxaliplatin infusion: the myth of safety devices. BMJ Case Reports, 2014.
• Deutsch, G.G., Sathyanarayan, S.A., Singh, N. et al (2014). Ultrasound-guided placement of midline catheters in surgical intensive care unit: a cost-effective proposal for timely central line removal. J Surg Res. Sep;191(1):1-5.
• Nolan, M.E., Yadav, H., Cawcutt, K.A., et al (2016). Complication rates among peripherally inserted central venous catheters and centrally inserted central catheters in the medical intensive care unit. J Crit Care. Feb;31(1):238-42.