infection control unit faculty of dentistry the british
TRANSCRIPT

Infection Control Unit
Faculty of Dentistry
The British University in Egypt
2020

2

3
BUE Organization of Infection Control Unit in Faculty of Dentistry
Professor Tarek Abbas Faculty Dean
Prof. Reham Magdy Faculty vice Dean for community service & Head of Infection Control Unit
Prof. Ibrahim Yehia Director of infection control unit
Dr Engy Farag Hospital infection control coordinator for personal infection protection means
Dr Shereen Nader Awareness coordinator for infection prevention & protection
Departments Coordinatorsʼ :
Dr. Dina Mostafa Teaching assistant in Medical Science ( Microbiology )
Dr. Farah Mohey Demonstrator in Medical Science (Microbiology)
Dr. Cindrella Mamdooh Assistant Lecturer in Crown and Bridge Dep.
Dr. Raneem Mustafa Clinician in Crown and Bridge Dep.
Dr. Sara Tarek Demonstrator in Endodontics Dep.
Dr. Heba Metwally Assistant Lecturer in Endodontics Dep
Dr. Norhan Youssef Demonstrator in Pediatric dentistry Dep.
Dr. Yasmine Mohamed Demonstrator in Pediatric dentistry Dep.
Dr. Ahmed Hesham Assistant Lecturer in Surgery Dep.
Dr. Basma Abalkader Assistant Lecturer in Surgey Dep.
Dr. Ahmed Abd El Hady Assistant Lecturer in Orthodontics Dep.
Dr. Abd El Rahman Alaa Demonstrator in Prosthesis Dep.
Dr.Adham Youssef Demonstrator in Prosthesis Dep
Dr. Nada Ashraf Demonstrator in Medicine, Perio and Diagnosis , X Ray Dep.
Dr. Rana Tantawy Demonstrator in Medicine, Perio and Diagnosis , X Ray Dep.
Dr. Amr Shalby Demonstrator in Operative Dep
Dr. Nermeen Hamada Demonstrator in Operative Dep .
Administration support:
Ms Elhaam Abd El Hameed Head of Nurses
Mr. Maher Mansoor Hospital building manger
Ahmed Abd El Latif Administration support
Shaimaa Hamed

4
*Background…………………………………………………………….P.5
*I-Strategies to prevent transmission by patient evaluation
and assessment ……………………………………………………….P.6
A-Patient selection……………………………………………………..P.7
B-Patient evaluation…………………………………………………...P.9
*II-Strategies to prevent transmission in waiting area & upon
arrival to dental clinic………………………………………………….P.10
*III- Strategies to prevent transmission by preparing dental room
& clinic settings……………………………………………………....P.15
*IV-Strategies to prevent transmission by personal protective
equipment (PPE)………………………………………………….….P.20
*V-Strategies to prevent transmission during dental
treatment……………………………………………………………...P.26
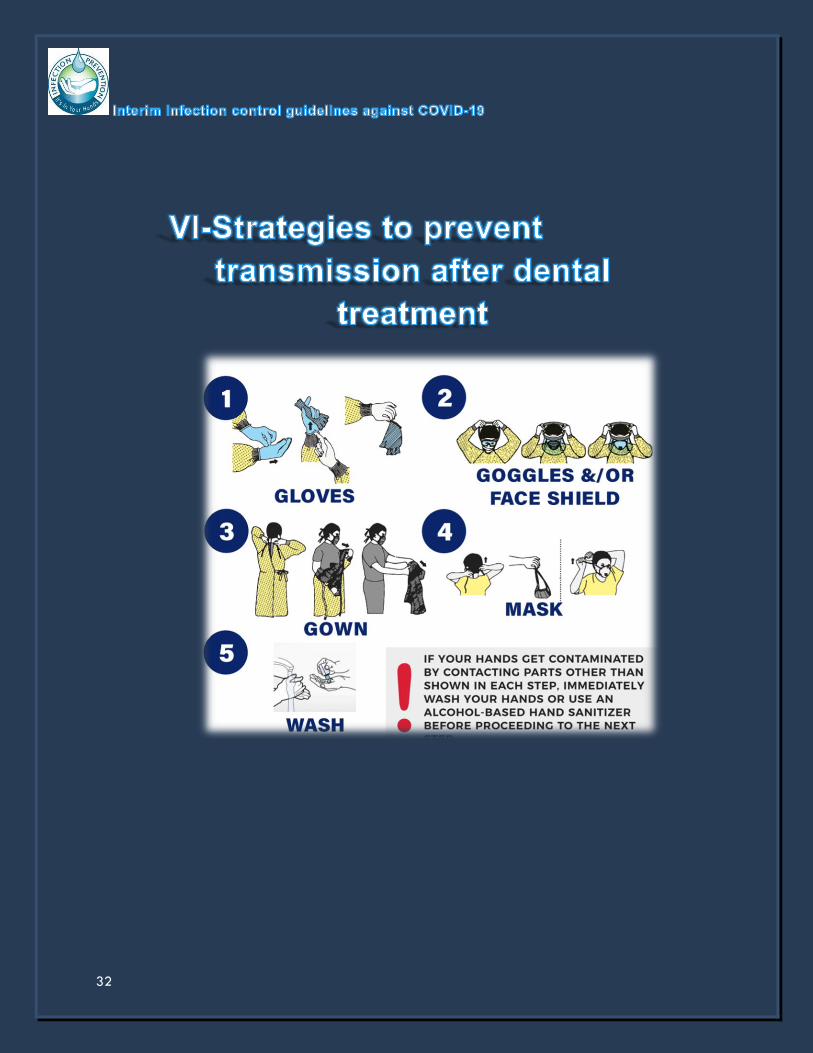
* VI-Strategies to prevent transmission after dental
treatment……………………………………………………………...P.32
*References…………………………………………………………...P.37

5
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2). Common symptoms include fever, cough,
and shortness of breath . As of 19 April 2020, more than 2.34 million cases have been reported
across 185 countries and territories, resulting in more than 161,000 deaths. The current
tendency of COVID-19 epidemic is increasing and spreading in the world.
The virus is primarily spread between people during close contact, often via small droplets
produced by coughing, sneezing, or talking. While these droplets are produced when breathing
out, they usually fall to the ground or onto surfaces rather than being infectious over long
distances. People may also become infected by touching a contaminated surface and then
touching their eyes, nose or mouth.
In most instances, coronaviruses, including SARS-CoV-2, are transmitted from person to person
through large respiratory droplets produced during normal conversation or when coughing and
sneezing, either by inhalation or deposition on mucosal surfaces. Other routes implicated in
transmission of coronaviruses include contact with contaminated fomites (e.g. frequently
touched surfaces) and inhalation of aerosols produced during aerosol generating procedures
(AGPs). Viral RNA has also been detected in blood specimens, albeit rarely, but there is no
evidence of transmission through contact with blood.
Recent evidence suggests that even someone who is not symptomatic can spread COVID-19
with high efficiency, and conventional protective measures, such as face masks, provide
insufficient protection; suggesting that people can be infected by patients with subclinical
infection, either by droplets or by direct contact with secretions from infected cases, followed
by subsequent inoculation into the mucous membranes .
Dental professionals are at high risk for nosocomial infection and can become potential carriers
of the disease. These risks can be attributed to the unique nature of dental interventions, which
include aerosol generation, handling of sharps, and proximity of the provider to the patient’s
oropharyngeal region. In addition, if adequate precautions are not taken, the dental office can
potentially expose patients to cross contamination.

6

7
1-Tele screening via telephone
- any exposure to a person with
known or suspected COVID-
19
- any recent travel history to an
area with high incidence of
COVID-19
- presence of any symptoms of
febrile respiratory illness such
as fever or cough
* A positive response: dental care
should be deferred for at least
2 weeks or more & patients
should be encouraged to
engage in self-quarantine
2- Upon arrival, screening
questionnaire
- In the past 14 days, have you
had a fever (> 37.5°C), cough,
sore throat, or breathing
problems ?
- Any loss of taste or smell?
- Have you had close or family
contact with a suspected or
confirmed case of COVID-19 ?
- Does it come from areas with a
higher risk of COVID-19 in the
last 14 days?
(Figure 1)

8

9
. COVID screening & Chest CT
. Contact &airborne precaution
. Report to local health care agency
Signs/Symptoms of
COVID-19
Travel
history/Epidemiological
link
Suspected COVID-19
patient Perform dental
treatment
Elective Care Urgent Care (Acute pain) Emergency Care
- Defer treatment for 2 weeks
& more
- Follow up using telephone
- Pharmacologic Management
Antibiotics
Analgesics
- Follow using telephone
Recommendation
- Perform dental
treatment in negative
pressure room/Air
borne infection
isolation rooms

10

11
-Dental professionals should measure the patient’s body
temperature using a noncontact forehead thermometer or with
cameras having infrared thermal sensors.
- Patients should be seated in a separate, well-ventilated waiting
area at least 6 ft apart.
-Removing Carpets for easier floor cleaning and magazines,
Antiques, curtains, or anything that may be touched by others and
which are not easily disinfected.

12
-Arranging chairs in the waiting area with social distancing 2
meters apart.
- Avoid crowding by proper patient scheduling and contact patient
by mobile phone when it’s their turn.
-Visual signs as posters for hygiene instructions and standard
recommendations should be hanged.

13
-The patient should put disposable shoes cover or disinfect the
shoes at the clinic door.
-Patients are to sanitize their hands immediately after they arrive.
-Patients should wear a surgical mask and follow proper
respiratory hygiene, such as covering the mouth and nose with a
tissue before coughing and sneezing and then discarding the
tissue.

14
-Disinfection of elevator, handles, doorbell switches, doorknobs,
leather chairs, tables, pens, computer mouse and keyboard and
other frequently touched objects with surface disinfectant e.g 70%
alcohol.
-Provide alcohol hand rub tissues 70-95% and automatic hand
sanitizer dispenser.

15

16
-Use of disposable (single-
use) devices such as mouth
mirror, syringes, and blood
pressure cuff to prevent
cross contamination is
encouraged.
-Clinical contact surfaces are
surfaces that can be touched
frequently with gloved hands
during treatment or that can
become contaminated with blood.
Protective barrier covers (eg, clear
plastic wrap) can be used for these
surfaces, particularly those that are
difficult to clean.
-Only essential items and instruments
available on dental cabinets

17
-Protected surfaces should be
disinfected at the end of each day
and between patients. Most clean
surfaces should be cleaned only
with water and detergent. While,
for superficial and non-critical
disinfection of patient care
equipment, 0.05 % chlorine solution
( 1: 100 ) dilution is currently being
used. All surfaces and objects in a
distance 2 meter from the patient
head or touched by the patient
should be disinfected with 0.1 %
chlorine solution (1: 50 dilution) or
75% ethanol.
-Make sure to flush
waterlines at beginning of
workday and between
each patient.

18
-The floor of the clinical
area must be cleaned at
least 3 times/ day with
0.5% sodium hypochlorite
(1:10 dilution) and avoid
vacuum cleaners.
-Sterilization methods that can
be used for critical or semi-
critical dental instruments and
materials can be sterilized
with high pressure steam
(autoclave) & chemical steam
(formaldehyde).
-Ventilation systems that
provide air movement from a
clean to contaminated flow
direction should be installed.
Relying on natural air
ventilation through open
windows and natural air flow
is preferred. Air conditioning
filter and air water pipes
should be cleaned by
peracetic acid 0.2%
(recommended every 12 Hrs)

19
-Bio-decontamination unit
high output, short cycle
time, and ease of
operation with high
capacity hydrogen
peroxide vapor
catalyzation unit shortens
decontamination cycles in
rooms
-Untouchable waste bins
must be available.

20

21
1-GOWN
-FULLY COVER FROM NECK TO
KNEES
,ARMS TO END OF WRISTS &WRAP
AROUND THE BACK &FASTEN IN
BACK OF NECK &WAIST
2-MASK OR RESPIRATOR
-SECURE TIES OR ELASTIC BANDS AT
MIDDLE OF HEAD &NECK
-FIT FLEXIBLE BAND TO NOSE
BRIDGE
-FIT SNUG TO FACE & BELOW CHIN
-FIT-CHECK RESPIRATOR

22
SURGICAL MASK
*Protects from splashes &large particles
*Not properly sealed & may leak up to
80% in aerosolized areas
*Can be worn for 6-8 hours a day
*Preferred to be used on top of respirator
to minimize its contamination
N95 MASK OR EQUIVALENT
*PROPER FIT ON THE FACE
*PROVIDES 95% PROTECTION TO
SMALL PARTICLES
*Can be worn for the whole working
day (except for aerosol producing
procedures must be changed after
each patient)
N95 MASK WITH VALVE
*Prevent inhalation of small particles but will
not prevent particles from spread to
surrounding environment thus not
recommended to be used in dental settings
by medical staff . Valved respirators make it
easier to exhale air and do not filter the
wearer’s exhalation. This one-way protection
puts others around the wearer at risk.
Elastomeric Half Facepiece Respirator
*Reusable device made of synthetic or rubber. *May be equipped with filters that block 95%, 99%, or 100% of very small particulates. Also may be equipped to protect against vapors/gases. *When properly fitted, minimal leakage occurs
around edges of the respirator when user inhales.*Reusable and must be cleaned/
disinfected and stored between each patient interaction

23
3-GOOGLES & FACE SHEILD
-PLACE OVER FACE AND EYES AND
ADJUST TO IT
4-GLOVES
- EXTEND TO COVER WRIST OF
ISOLATION GOWN

24
GOOGLES
*Tight fit over &around eyes (or
glasses)
*Have anti-fog coating
*Have adjustable elastic strap
FACE SHEILD
*Protection to eyes ,nose ,lips
*Cover forehead, extend below
chin & wrap around sides of the
face

25
NEEDS
Waiting
area
Patient
Diagnosis
Non-
AGPs
AGPS
Gloves * * * Non-Water resistant
gowns * *
Water resistant gowns
*
Surgical Mask * * *
N 95 * Face shield /Goggles * *
Sealed Googles * Hand Hygiene * * * *

26

27
1-Doors of dental room clinics should be kept closed all the time
to confine the aerosol generated during dental procedures within
limited area.
2-Supply the patient with a head cap and disposable apron
before entering the examination room to avoid getting his clothes
and hair contaminated.
3-Preprocedural mouth rinse with 0.2% povidone-iodine might
reduce the load of corona viruses in saliva for 30 seconds. Another
alternative would be to use 0.5-1% hydrogen peroxide mouth
rinse, as it has non specific virucidal activity against corona viruses.

28
4-Based on the assessment of emergency questionnaire, clinicians
can gauge the severity of the dental condition and make an
informed decision to either provide or defer dental care.
4-Radiographs: extraoral imaging such as panoramic
radiography or cone-beam computed tomographic imaging
should be used to avoid gag or cough reflex that may occur with
intraoral imaging.
5-When intraoral imaging is mandated, sensors should be double
barriered to prevent perforation and cross contamination.

29
6-Dentists should use a rubber dam to minimize splatter
generation. It may be advantageous to place the rubber dam so
that it covers the nose.
7-Dentists should minimize the use of ultrasonic instruments, high-
speed handpieces, and 3-way syringes to reduce the risk of
generating contaminated aerosols
8-Recommended: Negative-pressure treatment rooms/ airborne
infection isolation rooms (AIIRs): it is worth noting that patients with
suspected or confirmed COVID-19 infection should not be treated
in a routine dental practice setting. Instead, this subset of patients
should only be treated in negative-pressure rooms or AIIRs.

30
9-Avoid aerosol-generating procedures (AGP) whenever possible
and if mandatory let the appointment be the last in the day. It is
recommended to avoid entering to the clinic from 15-30 minutes
after finishing aerosol generating procedures so that to settle
down before disinfecting the clinic.
10-High volume suction and four-handed dentistry are
recommended.
11- Use patients shields with Dental aerosol production if possible.

31
12-All dental work (impressions, …….) after receiving or before
sending to dental lab should be cleaned with soap and water, and
sterilized or disinfected in impression disinfectant solution then
wrap it.
• Metal ceramic restorations can be safely sterilized in the
autoclave in separate sterilization pouches.
All items must be thoroughly rinsed under running tap water
following disinfection
*Ethyl alcohol 70% :-Spraying Some rubbers may harden.
-Items should be spraying till saturation then covered to reach total
contact time of 10 minutes.
*Chlorine solution 0.5% (1:10 dilution):-Immersion Zinc oxide eugenol impression.
-Preferably prepared daily
and kept in covered dark
containers.
*All chlorine dilution solutions that are used ,are prepared from 5% sodium hypochlorite.
*Glutaraldehyde 2% : Dental alginate & polyether impressions may distort after 10 minutes.
- Extremely irritating.
*70% alcohol (Ethanol): highly effective against most common viruses
*peracetic acid 0.2%: to sterilize medical, surgical, and dental instruments chemically, function
as oxidizing agents ,recommended by CDC
*0.5% sodium hypochlorite: used for disinfecting areas contaminated with body fluids,
including large blood spills (the area is first cleaned with detergent before being disinfected
32

33

34

35

36
“Management of ... medical waste must also be done according
to routine procedures”
(a) The use of a single leak-resistant bag is usually adequate for
the containment of medical waste, provided the bag is resistant
and the waste does not contaminate the outside of the bag.
(b) Contamination or perforation of the bag requires its placement
in a second biohazard bag.
(c) All bags must be tightly closed for disposal.
(d) A rigid container must be used for sharps.
(e) For waste transportation, plastic bags are required to be
contained in a rigid container
(f) Regulated medical waste is decontaminated to reduce
microbial load and to make by-products safe for further handling
and elimination.
(g) The treatment need not render the waste “sterile”.
(h) Treatment processes may include autoclaving, incineration,
chemical disinfection, grinding/crushing/ disinfection methods,
energy-based technologies (eg, microwave or radio wave
treatments) and disinfection/encapsulation methods
(i) The bags containing waste can be disinfected with a solution
containing chlorine at 1000 mg/L, before transport.
(j)For household waste generated by the treatment of patients,
double-layer yellow bags with “gooseneck” ligation should be
used.

37
-Centers for Disease Control and Prevention. Transmission of
coronavirus disease 2019 (COVID19). Available at:
https://www.cdc.gov/coronavirus/2019-
ncov/about/transmission.html.
-Symptoms of Coronavirus (2020) U.S. Centers for Disease Control
and Prevention (CDC). Link: https://bit.ly/3bC6bnx
-Coronavirus Update (live) (2020): 1,001,069 Cases and 51,378
Deaths from COVID-19 Virus Outbreak-Worldometer. Link:
http://www.worldometers.info.
-Q&A on Coronaviruses (2020) World Health Organization.
-Chang D, Xu H, Rebaza A, Sharma L, Dela Cruz CS. Protecting
health-care workers from subclinical coronavirus infection. Lancet
Respir Med. 2020; 8: e13
-Ather A, Patel B, Ruparel,Diogenes A,Hargreaves K. Coronavirus
Disease 19 (COVID-19): Implications for Clinical Dental Care. JOE
2020;46
-WHO director-general’s opening remarks at the media briefing
on COVID-19. https://www.who.int/dg/speeches/detail/who-
director-general-s-opening-remarks-at-the-media-briefing-on-
covid-19—3-march-2020.
- Peng X, Xu X, Li Y, et al. Transmission routes of 2019-nCoV and
controls in dental practice. Int J Oral Sci 2020;12:9.
- Wang Y, Wang Y, Chen Y, Qin Q. Unique epidemiological and
clinical features of the emerging 2019 novel coronavirus

38
pneumonia (COVID-19) implicate special control measures. J Med
Virol 2020. https://doi.org/10.1002/jmv.25748.
- Centers for Disease Control and Prevention. Infection control:
severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
https://www.cdc.gov/coronavirus/2019-ncov/infection-
control/control-recommendations.html.
-Eggers M, Koburger-Janssen T, Eickmann M, Zorn J. In vitro
bactericidal and virucidal efficacy of povidone-iodine
gargle/mouthwash against respiratory and oral tract pathogens.
Infect Dis Ther 2018;7:249–59.
-Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of
coronaviruses on inanimate surfaces and its inactivation with
biocidal agents. J Hosp Infect 2020;104:246–51.
- Hokett SD, Honey JR, Ruiz F, et al. Assessing the effectiveness of
direct digital radiography barrier sheaths and finger cots. J Am
Dent Assoc 2000;131:463–7.
-Van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and
surface stability of HCoV-19 (SARS-CoV-2) compared to SARS-
CoV-1. N Engl J Med 2020 March 17. https://doi.org/
10.1056/NEJMc2004973.
-ADA recommending dentists postpone elective procedures.
Available at: https://www.ada.org/ en/publications/ada-
news/2020-archive/march/ada-recommending-dentists-
postponeelective-procedures. Accessed March 18, 2020.

39
-ELEVATORS SANITIZATION CHECKLIST – ELEVATORS GERMS PROTECTION
https://blog.droom.in/elevators-sanitization-checklist
-Peng, X., Xu, X., Li, Y. et al. Transmission routes of 2019-nCoV
and controls in dental practice. Int J Oral Sci 12, 9 (2020).
https://doi.org/10.1038/s41368-020-0075-9