initiation of coverage note
TRANSCRIPT

OSE IMMUNO Biotechnology
Wednesday, July 6th 2016
Ricky Bhajun, PhD, Financial Analyst Arnaud Guérin
[email protected] +(33) 2 40 44 94 10
at 5 July 2016
At the forefront of immunotherapy
OSE Immunotherapeutics is a company that develops a portfolio of immunotherapy
products. Immunotherapy seeks to stimulate the body's defences to fight against
certain diseases. Today, it is a real hot spot for clinical research. The two main
candidates developed by the company are Tedopi®, a combination of antigens tested
in non-small cell lung cancer (NSCLC), and FR104, a monoclonal antibody for
autoimmune diseases or graft-versus-host disease (GvHD).
NSCLC is the second most common cancer in the world, but also the most deadly with
1.6 million deaths per year (source: Globocan 2012). The main factor influencing the
development of this cancer is active smoking. With the rise of the latter in developing
countries, these figures are likely to increase in the coming years. NSCLC is now
considered cancer with strong therapeutic needs. By using Tedopi®, OSE
Immunotherapeutics provides, like a vaccine, the immune system with the keys
(antigens) to defend against cancer. Clinical results demonstrate that Tedopi®
triggers the immune defence against NSCLC, but especially that the product
substantially increases the lifespan of patients (i.e. HLA-A2+ patients, 45% of the
population). The product is currently in Phase III and the results are expected in
2018.
GvHD, occurring after transplantation and occurring in 35-50% of cases, represents a
global market of $ 4.3 billion (source: OSE Immunotherapeutics) with a blatant lack of
effective treatment in the long term. This is also the case of autoimmune diseases
where the immune system attacks its own constituents. Such diseases (e.g.
rheumatoid arthritis) are present in 8-10% of the population. The high incidence and
the lack of therapies also place these diseases in the category of strong therapeutic
needs. FR104 will address these needs by stimulating the immune system negatively
in patients, which will reduce inflammatory responses and therefore the intensity of
these pathologies. It is currently in Phase I and was the subject of a license option
exercised by Janssen Biotech in July 2016.
Finally, with Effi-7, the company is also interested in ICI (Immune Checkpoint
Inhibitors), which now represent a global market of € 1.3 billion and could reach € 30
billion by 2020 (source: Citigroup).
Our valuation is based on licensing models with milestone payments and royalties
although such agreement has not yet been signed for Tedopi®. We value OSE
Immunotherapeutics up to € 9.4 per share including the two products in clinical
development. Tedopi® is valued at € 6.4 / share and FR104 at € 3 / share by the NPV
method.
5
6
7
8
9
10
11
12
juil.-15 oct.-15 janv.-16 avr.-16 juil.-16
Price €6,69
Market Euronext - Comp. C ISIN / Mnemonic FR0012127173 / OSE Reuters / Bloomberg OSE.PA / OSE:F Index CAC Allshares PEA - PME Yes
Capitalisation ( €m ) 99,1 Float (%) 45,9% Nb of shares (m) 14,156 Closing date 31 - Déc
Shareholding Concert 45,8% Aperana Consulting 1,5% Debiopharm Diagnostics 2,7% Other 4,1%
15 16E 17E
Free Cash Flow -10,8 5,3 4,7 Financial INV 0,0 0,0 0,0 Capital increase 20,2 0,0 0,0 Changes in Cash 8,2 5,3 4,7 Net Cash position 9,3 14,7 19,4 Net Cash / share 0,93 1,04 1,37
Operating income 0,0 10,0 10,0 EBIT -5,4 5,5 4,9 % Operating income ns 55,0% 49,1% Declared Group Net inc. -5,6 5,3 4,7 % Operating income ns 53,3% 47,5%
Target €9,4
STRONG BUY (1)
Initiating coverage

OSE Immuno, 6 July 2016 2/66 Portzamparc
Swot matrix ....................................................................................................................................... 3
Investment thesis ............................................................................................................................ 4
Management team........................................................................................................................... 5
Company background .................................................................................................................... 8
Lexicon ............................................................................................................................................... 9
I – Valuation: Buy, target € 9.4, upside +25.46%................................................................ 12
I – 1 Tedopi® ......................................................................................................................................... 12
I – 2 FR104 .............................................................................................................................................. 13
I – 3 Sensitivity study ......................................................................................................................... 15
I – 4 Strong news flow ........................................................................................................................ 16
II – Neo-epitopes to revive the immune system .................................................................. 17
II – 1 Memopi® technology and NSCLC ..................................................................................... 17
II – 2 Tedopi® and therapeutic effects ...................................................................................... 31
II – 3 Other opportunities for Tedopi® ..................................................................................... 34
III – OSE Immunotherapeutics: synergy in immunotherapy ........................................... 36
III – 1 Effimune: brief history and merger ................................................................................ 36
III – 2 Restoration of the immune balance................................................................................ 37
III – 3 FR104: donation change for transplantation and autoimmune diseases ...... 42
III – 4 Effi 7: autoimmune diseases and transplantation via a different mechanism ...................................................................................................................................................................... 50
III – 5 Effi-DEM: a second-generation immune checkpoint inhibitor ........................... 52
IV – Repositioning in cystic fibrosis......................................................................................... 54
IV – 1 Cystic fibrosis ............................................................................................................................ 54
IV – 2 OSE-1101 and competition ................................................................................................. 54
V – Patents ....................................................................................................................................... 56
VI – Capital valuation methodology ......................................................................................... 57

OSE Immuno, 6 July 2016 3/66 Portzamparc
Swot matrix
Strengths Weaknesses Merger providing synergy in immunotherapy Substantial portfolio products A clinically advanced product (Phase III) and statistically significant correlation between immune response and survival Mastered mechanisms of action Strong intellectual property based on worldwide patents Orphan designations subject to rapid approvals Many publications denoting the beneficial effects of the products Good safety profiles of the products License option on FR104 exercised by J&J
Results statistically insignificant for Tedopi® in Phase II trials with regards to the median survival time and survival rate at one year Absence of partner (s) for the distribution of Tedopi® in Europe and North America
Opportunities Risks Several therapeutic indications (cancers, autoimmune diseases, transplantation, etc.) Accession to markets with strong potential, growing for some and with strong therapeutic needs Combination with other therapies related to immunity Academic partnerships with leading research centres in immunotherapy
Significant competition in the monoclonal antibodies sector and immune checkpoint inhibitors Hypothesis can vary greatly the development and access to markets (product prices, market shares, reimbursement problems, dates of clinical phases, etc.) Possibility of the existence of a depressed immune status of NSCLC patients in advanced stages leading to a statistically lower-than-expected therapeutic effect on the target populations

OSE Immuno, 6 July 2016 4/66 Portzamparc
Investment thesis
OSE Immunotherapeutics targets many markets and pathologies. The first target
market for the company is oncology including non-small cell lung cancer (NSCLC).
NSCLC represented a market of €4.9 billion in 2014 (source: Transparency
Market Research). Today, it is the second most common cancer in the world and
especially the most deadly with 1.59 million reported deaths in 2012 and a
median lifespan at five years of 22.6% (source: Globocan, OSE
Immunotherapeutics). There is still no truly effective treatment for the advanced
stages of the disease. The company also targets autoimmune disease in which the
body, through the immune system, attacks its own constituents. Approximately
7% of the population is affected by these diseases, more or less incapacitating.
The market is estimated at $50 billion (source: OSE Immunotherapeutics). No
very long-term solution exists yet to treat these diseases.
The OSE Immunotherapeutics solutions are immunotherapy products. The goal of
these technologies is to modulate the immune system of patients at different
levels so that they are agents of their own recovery. Most of the technologies of
the company are based on the modulation of T cells, cells associated with
adaptive immunity that identify pathogens and allow adaptation of the system to
these agents in order to destroy them.
The most advanced product of the company is Tedopi®. Currently being tested in
Phase III in NSCLC, it helps revive the immune system and direct it against some
cancers specifically to destroy them. The company’s product has shown very
positive results in the medium and long-term survival rates of patients with
statistically significant differences in the immune response and patient survival.
The company is seeking partnerships for the distribution of this product.
The second flagship product of the company is FR104, an antibody fragment that
binds to a key protein in the immune response, which was also the subject of a
license option exercised by Janssen Biotech (Group J&J) in July 2016. By binding
to this protein, FR104 significantly slows unwanted immune responses and
thereby alleviates autoimmune diseases, but also potentially prevents organ
transplant rejection, a market estimated at €4.3 billion. The product is currently
in Phase I in healthy subjects. The results of this phase are expected shortly.
Following the merger of the companies OSE Pharma and Effimune, the company
showed retroactively cash of €20 million at the end of 2015, which should enable
it to carry out all its projects for the next two years.
Our valuation of the company stands at €133 million, that is to say €9.4 per share.
This represents an upside of 25.5% from the last price. The valuation is based on
both the Tedopi® and FR104 products. Most of the valuation is based on
Tedopi® (68%), directly related to its strong clinical progress.

OSE Immuno, 6 July 2016 5/66 Portzamparc
Management team
Emile Loria: Chairman of the Board of Directors, non-executive
Doctor in oncology and former Chairman and CEO of Epimmune (2001-2006, San
Diego - company listed on Nasdaq), he developed the product OSE-2101
(formerly EP-2101) until Phase II. He later acquired OSE-2101 and all assets
related to the epitopes with the company Takeda in 2011-2012 via a Swiss
company OPI S (Geneva) against payment at the signing of delayed milestone
payments and limited royalties. Emile previously headed biotechnology and
consulting companies and has completed numerous industrial agreements with
international expertise in the implementation of agreements for the companies
BioAlliance, Epimmune, Biovector, Cygnus, Sanofi and Ciba-Geigy.
Maryvonne Hiance: Vice-Chairwoman of the Board, Director
Previously Chairwoman and co-founder of Effimune, and Nuclear Engineering
specialist, she managed for 14 years a nuclear programme on neutrons within
Framatome (Areva). She previously directed for more than 20 years various
innovative biotechnology companies: SangStat Atlantic (the parent company
Sangstat medical corporation was acquired by Genzyme in 2003 for its industrial
product portfolio in immunosuppression and transplantation). She also led the
innovation of the companies DrugAbuse Sciences and TcLand. Maryvonne
founded and directed Strategic Ventures, a consulting company supporting
technology companies. She was a member of the strategic advisory board and
Innovation Minister for SMEs and industry.
Dominique Costantini, CEO, Director
Founder and former CEO of BioAlliance Pharma (1997-2011, Paris, listed on
EuroNext, became Onxeo), she designed, developed and received approval for
therapeutic innovations in the field of oncology. She raised funds from 1999 to
2005 and introduced BioAlliance on EuroNext in late 2005, then raised funds in
2007 and 2011. This successful fundraising was based on milestones in product
development: three innovative products have been approved in Europe. She
concluded international industrial partnerships with more than € 130 million
signed contracts. BioAlliance Pharma is the only French Biotech to have
registered two products with the FDA. Dominique has over 15 years of
operational management in the pharmaceutical industry in HMR (now Sanofi).
She conducted R&D and marketing of the drug from research to market
(Immunology, Endocrinology, Inflammation, Infectious Diseases and Oncology).
Doctor, immunology, University of René Descartes Paris V.
Sophie Brouard, Director
Immunologist, veterinary, transplant specialist, she continued her post-doctorate
training at Harvard Medical School in Boston. Director of Research at CNRS,
Sophie heads an Inserm research group located in Nantes dedicated to
transplantation and its mechanisms. Her current research aims to understand the
mechanism of transplant rejection to find biomarkers of graft survival. In parallel,
she directs the Executive Committee of the Centaur foundation. Centaur is a
foundation with a worldwide reputation, a pioneer in pancreas transplantation
performing about 2/3 of simultaneous renal and pancreatic transplants in France.
This activity is linked to the strong commitment of both surgical and research
teams. Centaur also has worldwide recognition for its work on the immunological
mechanisms of diabetes in experimental models and in conducting clinical trials
in diabetic patients. Centaur brings together three pivotal centres of excellence in

OSE Immuno, 6 July 2016 6/66 Portzamparc
Nantes, Lyon and Paris, enabling them to work together on transplant research
projects with a European and American international committee.
Didier Hoch, Director
Doctor, he is Chairman of the Forum BioVision and of the start-up accelerator "Big
Booster". He is also a director of listed companies including Genticel and formerly
of DBV Technologies. From 2000 to 2010, he was Chairman of Sanofi Pasteur
MSD, a joint-venture company dedicated to vaccines, between Sanofi & Merck. He
has also held various management positions at Rhône Poulenc Rorer and Aventis
(“Vice Chairman Middle East-Africa”, Vice Chairman Middle East & Africa).
Former Chairman of the association of vaccine manufacturers' “Vaccine Europe”
and Chairman of the LEEM Biotechnology Committee.
Gérard Tobelem – Director
Gérard Tobelem won the Diderot Innovation award in 2006. He has held in
industrial, medical and scientific positions, including Executive Chairman of the
Etablissement Français du Sang, which he directed. Gérard Tobelem previously
exercised strategic functions within the Ministry of Higher Education and
Research. He advised various international pharmaceutical companies in their R
& D strategy. He is non-executive Chairman of the Board of Theradiag. He was
previously Professor of Haematology at the University of Paris 7 and Head of the
Blood Diseases department at the Lariboisière Hospital in Paris.
Guy Chatelain – Director
Lawyer, partner of Mentha & Associés, Guy is the representative of the company
OPI SA and MS Medical Synergy in Geneva.
He belongs to the association of lawyers of Geneva: Swiss Bar Association, Geneva
Association of Business Law.
Jean Théron – Director
Consultant for the pharmaceutical and biotechnology industry JT Conseils, John
assures structural audits, implementation of launch strategies, management
activities and training of marketing and sales operational managers. He created
the training programme for regional directors - ESSEC and a pharmaceutical
marketing and sales programme at ESCP Paris. He is co-founder of the companies
Imedial (pharmaceutical operations in North Africa and the Middle East),
BioAlliance Pharma and Vectans. Previously, he was Chairman of HMR France,
CEO of Hoechst, Behring, Roussel, Diamond, and Lutsia. He has acquired broad
international management experience in the world of pharmaceuticals and
biotechnology markets.
Jean-Patrick Demonsang – Director
He joined the OSE Pharma Board of Directors in 2014. Chairman and Managing
Director of Seventure Partners until 2013, he has supported remarkably the
activity of over 150 companies. Seventure is now one of the leaders of Venture
Capital in France with over € 500 million under management and a team of 12
professionals with two investment areas, Information Technology and Life
Sciences, in France and Europe.
Jean-Patrick Demonsang is also an entrepreneur with, to its credit, the creation
and management of a number of SMEs. He now leads an entrepreneurial project
for a theme park in the South of France. Jean-Patrick Demonsang holds an MBA
from HEC and is a physics graduate.

OSE Immuno, 6 July 2016 7/66 Portzamparc
David de Weese – Director
David joined Paul Capital Partners in 1995 and heads the firm. He is a pioneer in
the secondary markets for private securities markets ($ 6 billion under
management). David has 14 years of operational management experience in
Europe and the USA. David de Weese was founder, Chairman and CEO of two
biotechnology companies based in New York for SigA Pharmaceuticals and in
California, Cygnus Therapeutic Systems. Before Cygnus, he managed a software
company in Silicon Valley, Machine Intelligence. He also founded a medical
equipment company: Medical Innovations, until its acquisition.
David de Weese holds a degree from Stanford University and an MBA from
Harvard Business School. He trained at the Law Faculty of the University of
Stanford.
Walter Flamenbaum - Director
Founder of Paul Capital Partners, Walter is currently Emeritus partner of this
company. He has broad medical knowledge and extensive experience in health
investments. He has 30 years of medical experience in the development and
evaluation of pharmaceutical or biotechnology companies. He was involved in
drug development, medical device and diagnostic companies. He also has direct
experience as founder, Director and Strategic Advisor in several service and
health companies. Internist, nephrologist and pharmacologist, he was formerly
Professor of Medicine at the Faculty of Medicine of Mount Sinai in New York and
Tufts Medical School in Boston.
Doctor, graduated from Columbia University, he holds a degree from the
University of Washington.
Alexis Peyroles – Director representing employees, COO
EDHEC and "Executive MBA" of "Imperial College" in London; Alexis joined OSE
Pharma as Chief Financial Officer in September 2013. Alexis has over 15 years of
management experience abroad, mainly in the world of health for Sanofi in Japan
and in Eastern countries where he headed the Baltic countries management
control and the group's licensing activities (Business Development) in the Eastern
Europe area. Within Guerbet, he held the position of Director of Management
Control and then General Manager South America from its subsidiary in Brazil
where he managed all commercial and industrial operations. He has been the
Director OF Operations of OSE Pharma since 2014.
Source: OSE Pharma

OSE Immuno, 6 July 2016 8/66 Portzamparc
Company background
2004 Constitution of JT Pharma led by Jean Theron
2011 Takeover by Emile Loria of the optimised epitope technology for T-specific immunotherapy of cancer from Takeda through the company Biotech Synergy (USA)
2012 Transfer of assets to OSE Pharma International SA in Geneva (OPI)
Entry of Emile Lora and Dominique Costantini as shareholders of the company, transformation of company JT Pharma to a limited company and capital increase
Change of name of JT Pharma to Orphan Synergy Europe - Pharma. The company purpose is modified to ensure research and development for innovative medicines and to give priority to T-specific immunotherapy of cancer
Signing of a license for the European territory with the company OPI SA in Geneva to develop the OSE-2101 immunotherapy international programme in lung cancer
2013 Obtained orphan status in the US for OSE-2101 in non-small cell lung cancer in HLA-A2 positive patients
2014 Acquisition of all shares in the law company (active global patents and clinical applications for OSE-2101) Swiss OSE Pharma International SA, holder of the worldwide rights to patents for its medication and paid for by issuing OSE Pharma shares as part of a capital increase reserved for OPI associates and underwritten by offsetting their debt corresponding to the sale price
Phase III pivotal trial protocol in lung cancer submitted and accepted by both regulatory agencies: FDA in US and EMA in Europe
Capital increase of the company in the amount of nearly € 3.2 million with European "family offices", experts of the pharmaceutical world and specialised funds
2015 IPO of the company and capital increase in the amount of nearly € 21.1 million
First licensing agreement concluded and distribution for the Israeli territory concluded with Rafa Laboratories, a pharmaceutical company specialising in oncology and rare lung diseases
2016 Merger with Effimune, Nantes biotechnology company developing innovative products in immunotherapy Change of name to OSE Immunotherapeutics and relocation of the headquarters to Nantes

OSE Immuno, 6 July 2016 9/66 Portzamparc
Stock market movements and some key dates

OSE Immuno, 6 July 2016 10/66 Portzamparc
Lexicon
Adenocarcinoma The most common lung cancer starting in the glandular epithelium
DNA Deoxyribonucleic acid
Ag Antigen
NSAID Nonsteroidal anti-inflammatory drugs
AIRE Autoimmune regulator
ALK Anaplastic lymphoma receptor tyrosine kinase
ANCA Anti-neutrophil cytoplasmic antibody
Angiogenesis Production of blood vessels
APC Antigen presenting cells
RNA Ribonucleic acid
CD Cluster of differentiation (generic term for immunity molecules)
CFTR Cystic fibrosis transmembrane conductance regulator
MHC Major histocompatibility complex
CTLA-4 Cytotoxic T-lymphocyte-associated protein 4
Cytokines Molecules allowing cell signalling synthesised by different cells including immunity cells
EGFR Epidermal Growth Factor Receptor, often associated with cancers when mutated
Glandular epithelium Cell tissues capable of secreting a substance
Fab Sub part of an antibody (light chain + part of the heavy chain)
GvHD Graft-versus-host disease
HLA Human leukocyte antigen
HPV Human papillomavirus, DNA virus
ICI Immune checkpoint inhibitor, a class of drugs related to immunology
ICOSL Inducible T-cell co-stimulator ligand
IFN Interferon, proteins produced by the immune system cells
IL Interleukin, a type of cytokine
Kinase Protein whose function is to phosphorylate other proteins
MDSC Myeloid-derived suppressor cells
CIBD Chronic inflammatory bowel diseases
Neutropenia Lack of granulocyte cells (white blood cells or leukocytes)
NSCLC Non-small cell lung cancer
PD-1 Programmed cell death protein 1
PD-L1 Programmed death-ligand 1
PEG Polyethylene glycol
Self-recognition Immune system self-recognition of the host
Allogenic restriction Dual phenomenon of recognition for the proper functioning of immunity mediated by T cells

OSE Immuno, 6 July 2016 11/66 Portzamparc
SCLC Small cell lung cancer
SIRP Signal regulatory protein
TAM Tumour associated cells (macropgages)
TCR T cell receptor, receptor protein on the surface of T cells
Teff Effector T lymphocyte or CTL (cytotoxic T lymphocyte)
TNF Tumour necrosis factor
TNM Cancer classification method (tumour, node, metastasis)
Treg Regulatory T lymphocyte
VEGF Vascular endothelial growth factor, a protein with a role in angiogenesis
OSE Immuno, 6 July 2016 12/66 Portzamparc
T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4 T1 T2 T3 T4
Phase III
AMM (estimé)
Commercialisation
Phase II (estimé)
Phase III (estimé)
AMM (estimé)
2022 2023
TEDOPI
FR104
2016 2017 2018 2019 2020 2021
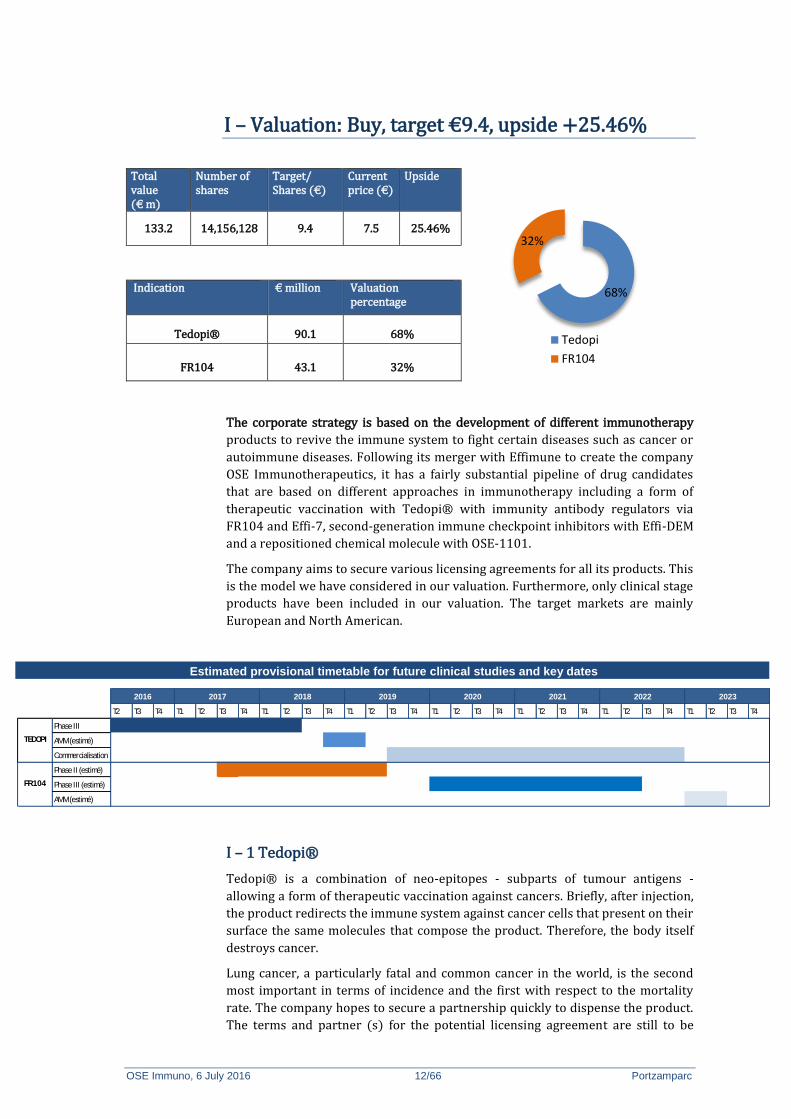
I – Valuation: Buy, target €9.4, upside +25.46%
Total value (€ m)
Number of shares
Target/ Shares (€)
Current price (€)
Upside
133.2 14,156,128 9.4 7.5 25.46%
Indication € million Valuation percentage
Tedopi® 90.1 68%
FR104 43.1 32%
The corporate strategy is based on the development of different immunotherapy
products to revive the immune system to fight certain diseases such as cancer or
autoimmune diseases. Following its merger with Effimune to create the company
OSE Immunotherapeutics, it has a fairly substantial pipeline of drug candidates
that are based on different approaches in immunotherapy including a form of
therapeutic vaccination with Tedopi® with immunity antibody regulators via
FR104 and Effi-7, second-generation immune checkpoint inhibitors with Effi-DEM
and a repositioned chemical molecule with OSE-1101.
The company aims to secure various licensing agreements for all its products. This
is the model we have considered in our valuation. Furthermore, only clinical stage
products have been included in our valuation. The target markets are mainly
European and North American.
Estimated provisional timetable for future clinical studies and key dates
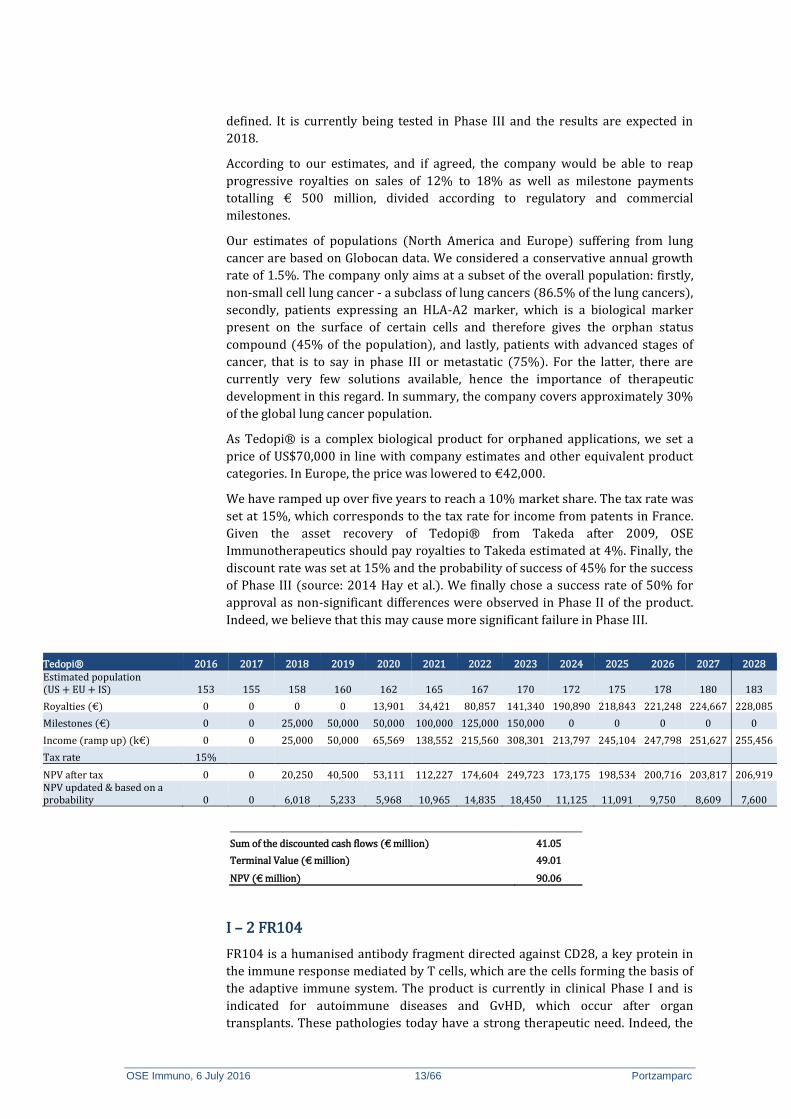
I – 1 Tedopi®
Tedopi® is a combination of neo-epitopes - subparts of tumour antigens -
allowing a form of therapeutic vaccination against cancers. Briefly, after injection,
the product redirects the immune system against cancer cells that present on their
surface the same molecules that compose the product. Therefore, the body itself
destroys cancer.
Lung cancer, a particularly fatal and common cancer in the world, is the second
most important in terms of incidence and the first with respect to the mortality
rate. The company hopes to secure a partnership quickly to dispense the product.
The terms and partner (s) for the potential licensing agreement are still to be
68%
32%
Tedopi
FR104
OSE Immuno, 6 July 2016 13/66 Portzamparc
defined. It is currently being tested in Phase III and the results are expected in
2018.
According to our estimates, and if agreed, the company would be able to reap
progressive royalties on sales of 12% to 18% as well as milestone payments
totalling € 500 million, divided according to regulatory and commercial
milestones.
Our estimates of populations (North America and Europe) suffering from lung
cancer are based on Globocan data. We considered a conservative annual growth
rate of 1.5%. The company only aims at a subset of the overall population: firstly,
non-small cell lung cancer - a subclass of lung cancers (86.5% of the lung cancers),
secondly, patients expressing an HLA-A2 marker, which is a biological marker
present on the surface of certain cells and therefore gives the orphan status
compound (45% of the population), and lastly, patients with advanced stages of
cancer, that is to say in phase III or metastatic (75%). For the latter, there are
currently very few solutions available, hence the importance of therapeutic
development in this regard. In summary, the company covers approximately 30%
of the global lung cancer population.
As Tedopi® is a complex biological product for orphaned applications, we set a
price of US$70,000 in line with company estimates and other equivalent product
categories. In Europe, the price was lowered to €42,000.
We have ramped up over five years to reach a 10% market share. The tax rate was
set at 15%, which corresponds to the tax rate for income from patents in France.
Given the asset recovery of Tedopi® from Takeda after 2009, OSE
Immunotherapeutics should pay royalties to Takeda estimated at 4%. Finally, the
discount rate was set at 15% and the probability of success of 45% for the success
of Phase III (source: 2014 Hay et al.). We finally chose a success rate of 50% for
approval as non-significant differences were observed in Phase II of the product.
Indeed, we believe that this may cause more significant failure in Phase III.
Tedopi® 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 Estimated population (US + EU + IS) 153 155 158 160 162 165 167 170 172 175 178 180 183
Royalties (€) 0 0 0 0 13,901 34,421 80,857 141,340 190,890 218,843 221,248 224,667 228,085
Milestones (€) 0 0 25,000 50,000 50,000 100,000 125,000 150,000 0 0 0 0 0
Income (ramp up) (k€) 0 0 25,000 50,000 65,569 138,552 215,560 308,301 213,797 245,104 247,798 251,627 255,456
Tax rate 15%
NPV after tax 0 0 20,250 40,500 53,111 112,227 174,604 249,723 173,175 198,534 200,716 203,817 206,919 NPV updated & based on a probability 0 0 6,018 5,233 5,968 10,965 14,835 18,450 11,125 11,091 9,750 8,609 7,600
Sum of the discounted cash flows (€ million) 41.05
Terminal Value (€ million) 49.01
NPV (€ million) 90.06
I – 2 FR104
FR104 is a humanised antibody fragment directed against CD28, a key protein in
the immune response mediated by T cells, which are the cells forming the basis of
the adaptive immune system. The product is currently in clinical Phase I and is
indicated for autoimmune diseases and GvHD, which occur after organ
transplants. These pathologies today have a strong therapeutic need. Indeed, the

OSE Immuno, 6 July 2016 14/66 Portzamparc
prevalence of autoimmune disorders is established between 3% and 10% of the
population; i.e. 7 out of 100 on average are affected by an autoimmune disease.
Depending on conditions, they are obviously incapacitating, e.g. rheumatoid
arthritis can be extremely debilitating as it can cause the patient to give up work
completely. In the case of GvHD, it manifests in 35-50% of cases depending on the
types of transplant with no really effective treatment in the long term.
Briefly, FR104 binds to the CD28 protein on the surface of T lymphocytes and thus
limits the immune response of the body by decreasing the response of cytotoxic T
lymphocytes (lifting the accelerator) and increasing that of regulatory T cells
(pressing a brake). Via this double effect, the immune system is slowed and
adverse events such as certain inflammatory processes or emissions are reduced.
In this way, autoimmune pathologies and GvHD are circumvented.
The product was subject to a license option exercised by Janssen Biotech (J&J
Group) in July 2016 following the publication of positive results of Phase I. Tests
will be conducted in the context of rheumatoid arthritis initially. Our sales
estimates are based on this last indication.
To estimate the addressable population for therapy, we first recovered an
incidence rate of the disease of 0.041% according to data from the Centers for
Disease Control and Prevention based on the study of Myasoedova al. published in
2010. Comparison with data from the World Population Prospect then provides
our average populations in Europe and North America. To determine the price of
the molecule, we relied on products of similar categories, including various
antibodies such as Rituximab, Etanercept or Abatacept. The price of the molecule
was set at $20,000 in North America and €12,000 in Europe.
We have ramped up over five years to reach a market share of 30% after the
marketing of the product that we estimated in 2023 in the light of initiation of
Phase II by Janssen. Similarly for Tedopi®, the tax rate was set at 15%.
Agreements with Janssen established milestones of € 155 million and royalties on
sales close to 10%. The discount rate was also set at 15% and the probability of
success was as follows: PII 30%; PIII 85% and 100% Acceptance (Hay et al. 2014).
FR104 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 Estimated population (US + EU + IS) 279 280 282 283 283 284 285 286 287 288 290
Royalties (€) 0 0 0 0 0 0 0 14,568 30,405 65,072 104,057
Milestones (€) 10,000 10,000 0 20,000 0 0 25,000 25,000 30,000 35,000 0
Income (ramp up) (k€) 10,000 10,000 0 20,000 0 0 25,000 39,568 60,405 100,072 104,057
Tax rate 15%
NPV after tax 8,500 8,500 0 17,000 0 0 21,250 33,633 51,344 85,061 88,448 NPV updated & based on a probability 7,391 1,928 0 2,916 0 0 2,037 2,804 3,722 5,362 4,848
Sum of the discounted cash flows (€ million) 10.08
Terminal Value (€ million) 33.06
NPV (€ million) 43.14

OSE Immuno, 6 July 2016 15/66 Portzamparc
I – 3 Sensitivity study
In summary, we have total valuation for OSE Immunotherapeutics (Tedopi® + FR104) of € 133 million.
Total
Sum of the discounted cash flows 51.3
Terminal value 82.1
Total 133
WACC discount rate
10-year OAT 0.19%
Market risk premium 5.78%
Beta 2.50
Specific risk premium 14.5%
WACC 15%
Growth rate to infinity 0.5%
Price drop 40%
The following tables show the effect of the discount rate, the market share, price of molecules and royalties on a consolidated basis:
WACC
10% 12% 14% 15% 16% 18% 20%
Market share
-5% 201,806 150,130 115,693 102,624 91,568 74,031 60,911
-3% 227,963 168,977 129,730 114,855 102,283 82,369 67,501
-1% 254,237 187,906 143,828 127,139 113,044 90,743 74,120
0% 267,201 197,247 150,784 133,200 118,355 94,875 77,386
1% 279,815 206,342 157,562 139,108 123,532 98,905 80,573
3% 305,606 224,935 171,417 151,183 134,113 107,142 87,086
5% 331,893 243,868 185,514 163,465 144,870 115,511 93,698
WACC
10% 12% 14% 15% 16% 18% 20%
Price of molecules
-25% 221,209 164,195 126,229 111,829 99,654 80,355 65,935
-15% 238,272 176,457 135,339 119,758 106,592 85,742 70,184
-5% 257,084 189,976 145,383 128,499 114,241 91,681 74,867
0% 267,201 197,247 150,784 133,200 118,355 94,875 77,386
5% 277,824 204,881 156,456 138,136 122,674 98,229 80,031
15% 300,690 221,313 168,664 148,762 131,972 105,448 85,725
25% 325,899 239,430 182,124 160,476 142,222 113,406 92,002

OSE Immuno, 6 July 2016 16/66 Portzamparc
WACC
10% 12% 14% 15% 16% 18% 20%
Royalties
-5% 185,714 140,328 109,678 97,928 87,924 71,907 59,779
-3% 218,309 163,096 126,121 112,037 100,096 81,094 66,822
-1% 250,903 185,863 142,563 126,146 112,269 90,282 73,865
0% 267,201 197,247 150,784 133,200 118,355 94,875 77,386
1% 283,498 208,630 159,005 140,255 124,441 99,469 80,908
3% 316,093 231,397 175,448 154,364 136,614 108,656 87,951
5% 348,688 254,165 191,890 168,473 148,786 117,843 94,994
In our low hypothesis, our valuations stand between €60 million and €100 million, while our high estimates show valuations exceeding €140 million and up to €350 million. These scenarios are those that have the lowest probability of occurrence.
I – 4 Strong news flow
With a consolidated portfolio of at least five products within which two in clinical phase, the short- and medium-term news flow is quite significant.
Firstly, the pivotal trial results of Phase III US-EU Tedopi® are expected in 2018. Meanwhile, the company hopes to have implemented various agreements, as much in developed countries as in BRIC and emerging countries by the end of 2016 and early 2017. A first test of Tedopi® in combination with an immune checkpoint inhibitor is planned for 2017.
For FR104, a license option was exercised by Janssen Biotech in July 2016 and Phase II will be considered. During 2017, the rest of the portfolio will make progress, especially Effi-7 and Effi-DEM, which could potentially enter the clinical phase.
With a consolidated cash position of approximately € 20 million, the company expects to complete its projects for the next two years. In addition, some of the projects are already partly funded, particularly for Effi-7, which explains the cash burn schedule evoked by the management.

OSE Immuno, 6 July 2016 17/66 Portzamparc
II – Neo-epitopes to revive the immune system
OSE Immunotherapeutics develops innovative immunotherapy products mainly for
lung disease including lung cancer via its flagship product Tedopi® (or OSE-2101)
and, to a lesser extent, via OSE-1101. There are various forms of lung cancer. OSE
Immunotherapeutics targets NSCLC, which represents approximately 86.5% of
lung cancers (Source: OSE Pharma). The NSCLC market represents $ 4.9 billion in
2014 (source: Transparency Market Research). The company also focuses on
other cancers for OSE-2101 including colon, ovarian and breast cancer. At the
same time and via the OSE Pharma/Effimune merger announced in February 2016,
the company approaches immunological diseases such as GvHD or certain
autoimmune inflammatory diseases (e.g. ulcerative colitis).
The objective of Tedopi® is to revive the immune system so that it is able to
recognise and destroy cancer cells via T-specific immunity. Based on Memopi®
technology comprising combinations of receptors present on the surface of cancer
cells called "epitopes", Tedopi® is a combination of modified neo-epitopes
generally present on the surface of lung cancer cells. Injection of the combination
allows the immune system to develop a defence against these epitopes and
ultimately against different types of cancer - not limited to the lung - expressing at
least one of these. Tedopi® is now considered a precision medicine since only
"positive HLA-A2" patients (45% of the population) are concerned by this
therapy.
The strategy of the company is to secure license agreements for all the products it
offers. Its revenues will therefore be based on milestone payments and royalties.
Tedopi® mechanism of action
Source: OSE Pharma / Portzamparc

OSE Immuno, 6 July 2016 18/66 Portzamparc
II – 1 Memopi® technology and NSCLC
The Memopi® technology developed by the company is based on tumour
antigens. These antigens are actually proteins expressed by certain cancers, but
the body is often unable to identify them since they are either part of the human
body (naturally expressed by the body, therefore not considered harmful) or are
undetectable due to other defence mechanisms developed by cancer.
Antigens highly expressed by cancers can be biomarkers, that is to say disease
prognosis or diagnosis factors. However, as they are innate elements, they are not
necessarily recognised as harmful and cancer is not spotted by the immune
system. Nearly 75 proteins have been identified as antigens associated with
cancers (source: Cheever et al., 2009).
The basic hypothesis of the technology developed by the company is that through
a modified injection of antigens to patients, the immune system will recognise
them and then be able to recognise and destroy tumour cells believed to express
the same antigens. Recognition in fact takes place at an area of the antigens called
"epitope" or "antigenic determinant". It is this area which will be recognised by
the patient’s immune system.
Recognition of pathogens by the immune system
Source: Yao Lian et al., 2014
Resulting from the Memopi® technology, Tedopi® is the main component of the company. It is a set of 10 epitopes (nine modified epitopes highly expressed in NSCLC and one helper T-cell epitope) carefully chosen for their affinity for the HLA-A2 receptor - often over-represented in patients with advanced cancer. It is currently indicated for NSCLC, but the company plans to expand its application to other cancers later.

OSE Immuno, 6 July 2016 19/66 Portzamparc
Global differences in the incidence and mortality of lung cancer
Source: GLOBOCAN
II – 1 – a) Lung cancer: a major challenge
Globally, lung cancer, also called bronchial or pulmonary cancer, is the second most
common cancer in the world. This cancer shows an extremely high mortality rate
rising to 87% in 2012 or 8.7 deaths per 10 detected cases (source: Globocan
2012). The average overall survival at five years is well established at 22.6%
according to the data from the SEER Cancer Statistics Review (CSR) and
considering all stages of cancer (Howlader et al. 2016). As a remainder, cancer can
be defined by a loss of cell control, that is to say totally uncontrolled cell
proliferation.
With 1.59 million deaths worldwide in 2012, the number of deaths from this cancer
is higher than the number of combined deaths from colon, breast and prostate
cancer. On the same scale, it is also the most common cancer in men with 1.2
million cases recorded in 2012. Women are, in turn, much less affected since
Globocan data showed only 583,000 cases in the world in 2012 - more than twice
less, but with equivalent survival statistics.

OSE Immuno, 6 July 2016 20/66 Portzamparc
cases in 100,000. According to some studies, the mortality rate of these cancers
increased in the United States until 1990 but has decreased since 2001 (source:
cancer.gov; 2014; Wingo et al. 1999). An upward trend is observed in the
incidence of lung cancer in some developing countries. This fact is highly
correlated with the progression of active smoking in these countries (source:
Youlden et al., 2008).
Demonstrated for over 200 years (Doll, 1998), it is accepted that the main factor
influencing the incidence of lung cancer is active smoking (Doll et al., 1951; Peto et
al., 2000; Cornfield et al., 2009). The trends mentioned above, particularly in
terms of origin and sex, are in fact highly correlated with the prevalence of
smoking since it has been shown that the risk of developing lung cancer decreases
when stopping cigarette smoking (Peto et al 2000; Parsons, 2010).
The incidence rate also increases by other factors, including exposure to passive
smoking (Hirayama 2000; Trichopoulos, 2006), some occupational exposures to
toxic substances such as radon (Darby et al., 2005) or arsenic (Hopenhayn-Rich et
al., 1997) and finally, air pollution (Arden Pope III et al., 2002). These factors,
however, have a lower impact on the incidence of lung cancer than active
smoking.
Probability of developing lung cancer when stopping cigarette smoking
Source: Peto et al.2000
Lung cancer can be classified mainly into two groups: small cell lung cancer (SCLC) and
non-small cell lung cancer (NSCLC).

OSE Immuno, 6 July 2016 21/66 Portzamparc
a) SCLC
This type of cancer represents on average 13.5% of cases of lung cancer. It is the
cancer showing the strongest positive correlation with active smoking. This type
of cancer usually develops in the central part of the lungs extremely quickly, but
initially shows few symptoms, so it is often too late to consider surgery at
diagnosis. Chemotherapy is usually recommended in these cases, particularly for
its positive role in the relief of symptoms and improvement of survival (Cook et al.
1993).
b) NSCLC
NSCLC, targeted by OSE Immunotherapeutics, represents 86.5% of remaining cases
of lung cancer. This type of cancer usually spreads more slowly than SCLC, but has
most of the same properties as them: its detection is often too late and at advanced
stages (Govindan et al., 2006), which prevents its surgical removal. In the same way
as SCLC, smoking is the leading cause of development of NSCLC, but the other
above mentioned factors also take a significant part in this development.
There are three main types of NSCLC: firstly, adenocarcinomas, which are the
most common type (40.8% of cases); secondly, squamous cell carcinomas, which
are the second most common form (21.4% of cases) and finally, lung carcinomas
in large cells, which represent about 3% of cases. The remaining 20% are actually
represented by different rare forms of NSCLC with pleomorphic tumours or
carcinoid tumours, for example. (Howlader N et al., 2013). These categories
represent in fact simply the cellular source from which emerges cancer.
Histology of small cells and non-small cells in the lung
Source: WebMD

OSE Immuno, 6 July 2016 22/66 Portzamparc
II – 1 – b) NSCLC: market and available treatments
Despite new treatments, NSCLC remains difficult to cure with survival rate at five
years at around 1% in case of metastasis (source: OSE Immunotherapeutics;
American Cancer Society - review 05/22/2013).
Approximately 84,000 patients in the United States and 134,000 patients in Europe
have NSCLC and are HLA-A2-positive according to the company. Moreover, the
presence of the HLA-A2 marker is considered an aggravating risk factor in
patients. Depending on the stage of cancer development and in case of failure to
stop cancer in too advanced stages, different treatments available to patients can
slow tumour progression. The type of treatment depends mainly on the stage of
cancer development.
a) Classification of NSCLC
The TNM (tumour, node, metastasis) is a system for classifying cancers according
to anatomical extension, that is to say spread around the cancer site (stage of
development). Developed between 1943 and 1952, the TNM system is based on
the spread of cancer in the tumour (T), the nodes (N) and finally in other areas of
possible metastases (M). Various revisions and formats are available, including
those specific for lung cancer (Rami-Porta et al., 2009).
According to this classification, NSCLC is called "evolutionary stage 0, Ia, Ib, IIa,
IIb, IIIa, IIIb or IV" based on the severity of the tumour. Until stage IIIa, NSCLC is
called "localised" and after, disseminated (IIIb) or metastatic (IV). As explained
above, NSCLC is usually diagnosed at stages already quite advanced, that is to say
stage IIIa to stage IV. Thus, two thirds of lung carcinoma NSCLC is diagnosed at
stage IV, which is the metastasis stage where it is currently complicated to treat.
TNM classification of lung cancer according to Rami-Porta et al..

OSE Immuno, 6 July 2016 23/66 Portzamparc
The major types of treatments available for these various stages are summarised
in the following table:
NSCLC treatment
a) C
h
i
m
i
o
t
h
b)
c)
d)
e) SSource: OSE Pharma
b) Antimitotic chemotherapy
Chemotherapy is thus the most widely used therapy in the context of NSCLC,
particularly with docetaxel, gemcitabine, paclitaxel, pemetrexed or vinorelbine,
either as first-line or last-line treatment. The choice of the molecule and the
duration of treatment vary according to the patient's age, general condition,
medical history and the type and stage of NSCLC. From the disseminated stage and
rarely at earlier but inoperable stages, platinum salts accompany chemotherapy.
In second-line treatment, docetaxel and pemetrexed allow survival from 5.5 to 8.3
months (source: OSE Immunotherapeutics; Ciuleanu T et al., 2012; Hanna N et al.,
2004.). Many of these molecules are blockbusters, that is to say molecules which
have reached sales of over one billion per year. This is typically the case of
docetaxel, which has grossed about $19 billion since 2001 (all cancers) or
pemetrexed, which has grossed $20 billion since 2004.
Most of these molecules act on cell division, but with unrestricted targets, either by
targeting microtubules, cell cytoskeletal components (e.g. pemetrexed), or folate,
an important source for the production of DNA (e.g. docetaxel). Although the main
targets of these molecules are cancer cells, they will interfere with some rapidly
multiplying healthy cells. The advantage of these products is their multiple use;
they are suitable for various cancers. However, they show multiple side effects on
capillary cells (hair), keratin (in particular nails), the gut wall causing vomiting,
nausea, stomatitis and diarrhoea and hematopoietic cells generating red and
white globules, and platelets causing neutropenia, thrombocytopenia and
anaemia.
Stage of
development
Treatment
Ia Ablation of a portion of the lung or the entire lung by
surgery
Radiation therapy if surgery is not possible
Ib Possible surgery followed by chemotherapy
Radiation therapy if surgery is not possible
IIa and IIb Surgery followed by chemotherapy
IIIa Chemotherapy, optionally in combination with surgery or
radiation therapy
IIIb Chemotherapy plus radiotherapy (exceptional surgery)
IV Chemotherapy and other treatment as targeted therapies

OSE Immuno, 6 July 2016 24/66 Portzamparc
c) Targeted therapies
Targeted therapies are references to specific products in a given biological target.
They are often accompanied by a diagnostic companion to test the expression of
the target and are, mostly, present only in a subset of the population.
Whatever the non-squamous lung cancer, that is to say adenocarcinoma and large-
cell carcinoma, a systematic search of the activating mutation of the EGFR gene
(Epidermal Growth Factor Receptor) is sought. It is estimated that this mutation is
present in 10-15% of the population (source: OSE Pharma). The EGFR gene
encodes a transmembrane protein of the protein kinase superfamily (protein
whose function is to add a phosphorus group to other macromolecules or
themselves). Activation of this protein via its autophosphorylation then leads to
cell proliferation, hence its importance in tumour development. In the presence of
mutations in the gene, blocking apoptosis (programmed cell death), increased
production of angiogenic factors and facilitation of the metastasis process are
observed. The goal is to block kinase in order to limit the tumour proliferation
process. Gefitinib and erlotinib are two tyrosine kinase inhibitors of EGFR that are
proposed, one or the other, in first-line EGFR+ mutation.
Similarly, crizotinib (Xalkori® of Pfizer) or ceritinib (Zykadia® of Novartis and
when crizotinib gives no result) is proposed in case of molecular rearrangement
at the ALK gene (Anaplastic Lymphoma Receptor Tyrosine Kinase),
rearrangement present in approximately 4% of the population). ALK gene
encodes a tyrosine kinase receptor, which belongs to the superfamily of insulin
receptors.
f) Antiangiogenic molecules
Angiogenesis is the phenomenon of the formation of new blood vessels from
existing vessels. Sometimes used in conjunction with chemotherapy in squamous
cell cancers, bevacizumab (Avastin® Roche) targets the VEGF (vascular
endothelial growth factor) receptor that plays a role in angiogenesis. Indeed, all
cancers have basic needs in nutritional intake and oxygen. By blocking the genesis
of blood vessels, the tumour is deprived of resources, limiting its development.
Generally more costly because of more complex creation processes, monoclonal
antibodies are molecules that generate significant income in the laboratories that
distribute them. Avastin® for example brought Roche over € 6 billion in 2013.
Oncology in 2013 represented 42% of indications of these biological molecules
and the rest was shared between inflammation (37%), immunology (16%) and
ophthalmology (5%) (source: Citigroup).
Vargatef® of Bohringer Ingelheim (small molecule) or Cyramza® of Eli Lilly
(monoclonal antibody) are also two anti-angiogenics that are combined with
chemotherapy and lead to better survival rates in patients able to withstand this
type of treatment.
All the methods mentioned above uses chemical or biological molecules. These
seek to block the activity of one or more biological processes but do not act on the
patients own defences: their immune system. Indeed, we can consider that each
individual develops "cancer" on a daily basis. In other words, every day, a cell
loses control over its divisions. However, the body is able to detect these cells and
trigger cell death (apoptosis) of these malignant cells. Escaping the self-protection
system is one of the first signs of cancer development per se.

OSE Immuno, 6 July 2016 25/66 Portzamparc
g) Immunotherapy
A growing number of studies are conducted on the ability of the immune system
to identify and destroy tumour cells. Immunotherapy is now considered a hot spot
in cancer treatment (Carvalho et al., 2016). In this case, the objective is not to
artificially block tumour proliferation, but to act on the patients’ immune system so
that they are able to fight against cancer themselves. The benefits are many:
supposedly shorter treatments, but above all, potentially providing long-term
effects as they will call on the patient’s immune system "memory" via adaptive
immunity.
Approaches based on immune checkpoint inhibitors (ICI; proteins that brake the
immune system’s response to cancer) have been launched or are being tested
since 2015. This is particularly the case of nivolumab (Opdivo® of Brystol Myers
Squibb) for squamous NSCLC and pembrolizumab (Keytruda® of Merck and Co)
in the case of patients showing elevated expression of PD-L1 protein. Lifting the
brake via immune checkpoints allows a higher production of non-specific
cytotoxic T lymphocytes, that is to say an improvement of the immune system as a
whole via the stronger production of lymphocytes without them being specifically
directed toward those cancers. The targets of these antibodies are currently CTLA-
4, PD-1 / PD-L1, LAG-3 and more recently, KIR or NKG2A. The ICI market is today
estimated at €1.3 billion, rising to €30 billion in 2020 (source: Citigroup).
Several authors have shown that this brake brings a clinical benefit in lung cancer
(Brahmer et al., 2013, Topalian et al., 2012). In Phase I/II in NSCLC, nivolumab, an
anti-PD-1 monoclonal antibody, showed a tumour regression response rate of
17%, a survival rate at one year and two years of 42% and 24% respectively, and
a median overall survival of 9.9 months (source: OSE Immunotherapeutics; World
conference on lung cancer, Sydney 2013). Since March 2015, the indications of
this product have also been extended to treat NSCLC in case of escaping first-line
chemotherapy treatment based on platinum salts and dependent on the pivotal
phase results, which have shown that nivolumab increased median survival to 9.2
months versus six months with chemotherapy.
Immune checkpoint inhibitors are obviously not limited to lung cancer. In fact,
they really stand out in liquid cancers. Nevertheless, these products have
relatively low response rates of between 10% and 30% (Brahmer and Pardoll,
2013; West, 2014). Biomarker research is therefore essential for efficient use of
these products.
However, a fear founded by different physicians is the potential runaway of the immune system when using ICI. Indeed, and as explained above, the responses obtained by ICI are not specific, which may induce unwanted systemic inflammatory responses due to potential loss of self-control of the immune system.

OSE Immuno, 6 July 2016 26/66 Portzamparc
Turnover of some anticancer drugs also indicated in NSCLC
Source: druganalyst, Portzamparc
Trials on other innovative products have also been launched. Belagenpumatucel-L
(Lucanix® of NovaRX) is a product derived from modified tumour cells seeking to
initiate a T-specific immune response (vaccination). If the primary endpoint was
not met in 532 NSCLC patients in stage III and IV, a subgroup of 305 patients for
whom survival of 20.7 months was observed (versus 13.4 months in the control
group) was identified. Although the P-value associated with this difference is
greater than the threshold commonly used of 5% (not significant), the difference
between the two groups is still quite significant leading to the initiation of Phase
III in this subpopulation. Finally, tecemotide (of Oncothyeron and Merck KGaA) is
a small peptide from tumour antigen MUC-1. Injection of this peptide in patients
allows a specific lymphocyte response against MUC.
A final strategy is the use of CAR-T (chimeric antigen receptor T cell) that
specifically targets certain tumour antigens. The objective of this strategy is to use
cytotoxic T lymphocytes of patients (autologous approach) or other patients
(allogeneic approach), change them and then reintroduce them to patients to
destroy cancer cells. The market for CAR-T across all approaches is estimated at $
30 billion for 2030 (source: Roots Analysis).
Whatever the approach, the pharmaceutical industry is now very interested in the
immunotherapy field: we can count more than 17 license agreements since 2013
(source: Medius Associates) with mean deals of $900 million and a mean upfront
of $112 million. We can assume that in case of agreement, this is about what might
await the company in terms of a deal.
h) Combination therapy
Given the strong success observed with immune checkpoint inhibitors, several
companies are seeking to develop combinations of solutions covering different
categories of products: two or more ICI in combination, ICI and chemotherapy, ICI
and immunotherapy, etc. (Brahmer and Pardoll, 2013; Ribas et al., 2013. Cooper et
al., 2014.). The goal is to significantly increase the number of responders to
different therapies by modifying the tumour microenvironment. This is done by
increasing the number of T lymphocytes, which will seek and destroy tumours,
and reducing regulatory T cells (Treg) immunosuppressors, which limit the action

OSE Immuno, 6 July 2016 27/66 Portzamparc
of T cells. Some examples of combinations are clinical trials between gp100 (an
anti-cancer peptide vaccine) and nivolumab, anti-HPV-16 combined with
nivolumab or Medi4736 (Astra Zeneca) or IDO inhibitors (decreasing Treg) with
pembrolizumab or Medi4736. These new combinations seek both to speed up the
immune system while lifting its brakes and are increasingly important in research
and development against cancers.
OSE Immunotherapeutics has its place typically in the context of the specific use of
the patient's immune system. By presenting not a single antigen, but a whole list of
antigens to the patient’s immune system, the company seeks to make the immune
system react while overcoming the problem of the heterogeneity of tumours and
potential losses of tumour antigen expression.
As shown in other studies, variability in the cell repertoire and in particular, the
immune status of patients has a major effect on the ability of the immune system to
defend against attacks, but also on patient survival. Thus, the more diverse the
status, the more patients' progression-free survival is high (Tada et al. 2016).
However, and as opposed to ICI, Tedopi® develops a specific form of immune
defence since the system is oriented towards only a few antigens. The technology
is thus less likely to trigger systemic inflammatory reactions.
Tedopi® is indicated after failure of first-line treatment in patients with stage IIIb
or IV inoperable metastasis representing 67% of the NSCLC population (source:
OSE Pharma). It is also important to note that these patients are usually patients
undergoing intensive treatments that have a significant impact on their immune
system. For example, chemotherapy also kills bone marrow cells, precursors of
immune cells. This non-specific destruction could ultimately make the immune
system less effective despite the use of products such as Tedopi®.
II – 1 – c) Memopi®: towards stimulation of cytotoxic T lymphocytes
Analysis of overall survival of cancer patients shows quite substantial disparities
in terms of the expression of certain proteins in these patients. Those showing a
high rate of protein CD8 or those with a high expression of HLA-A have a higher
survival probability than patients with lower levels of protein expression (Brown
et al. 2014).

OSE Immuno, 6 July 2016 28/66 Portzamparc
a) Adaptive immunity: Memopi® technology rational
Overall survival of patients based on the expression of CD8 and HLA-A
Source: Brown et al 2014
CD8 is a receptor expressed on the surface of cytotoxic T lymphocytes (also called
CD8 T lymphocytes). The role of these cells is to destroy foreign cells in the body
(e.g. cells infected by viruses or cancer cells). These cells originate from the bone
marrow and migrate to the thymus, hence the term "T cells". Following their
activation via antigen presentation by the major histocompatibility complex or
MHC (called "HLA" in humans), these cells are able to locate and destroy all cells
presenting this specific antigen.
Although this system is generally regarded as highly effective, tumours are still
able to get around it, especially during their escape phase when they develop
camouflage strategies by presenting antigens inefficiently. In this way, cancer
escapes the immune system and can grow more easily.
More specifically, the HLA system is a self-recognition system via the expression
of HLA molecules on the cell surface. This is actually an immune surveillance
system that identifies invasive cells to neutralize their action (s). There are two
kinds of HLA: HLA class I, whose molecules are present on all nucleated cells in
the body and are recognised by cytotoxic T lymphocytes, and HLA class II, where
molecules are expressed on only some cells such as dendritic cells or
macrophages and are recognised by CD4+ T lymphocytes (helper T lymphocytes).
During an infection, T helper (Th) cells initiate the recognition against foreign
agents by issuing cellular signals that attracts cytotoxic T lymphocytes (CTL) to
the infected cells. The meeting between T cells and infected cells allows the
activation of T cells. Activation is recognition of the antigen (Ag) presented by the
infected cells as a "key". Presented graphically, the cell therefore creates a "lock"
to identify these keys. Once activated, the cells seek and destroy all cells against
which they were pre-guided through activation, that is to say cells with the same
foreign antigen (the same key).

OSE Immuno, 6 July 2016 29/66 Portzamparc
HLA system and lymphocyte activation
Source: In Tech
This is typically what is called "adaptive immunity", which adapts progressively to
encounters with pathogens. This is firstly a specific immunity to certain antigens,
as we have seen, but also a immunity with a memory system upon re-exposure to
these antigens; even years later, the immune system is able to react more quickly
and effectively since it still "remembers" this foreign antigen.
T-specific immunity is actually based on two types of receptors and double
epitope recognition: initial recognition by HLA-A2 and a second recognition by the
TCR (T cell receptor) present on the surface of T lymphocytes. It is only in the
presence of antigenic protein derivatives modified and presented by the HLA
system that TCR receptors can recognise antigens. Without this double
simultaneous recognition, no response is possible. Lymphocytes must recognise
the derived peptide and the HLA molecule, a phenomenon called "allogeneic
restriction". This discovery brought a Nobel Prize, awarded in 1975 to its
discoverers R. Zinkernagel and P. Doherty.

OSE Immuno, 6 July 2016 30/66 Portzamparc
Allogenic restriction Optimisation
Source: OSE Pharma
Based on this allogenic restriction basis, the company sought to optimise its neo-
epitopes so that the cytotoxic T response is increased with the aim of presenting
cancer antigens to direct the immune system against these cancers.
b) Tedopi®
More than 70 proteins have been identified as antigens associated with the
presence of cancer (source: Cheever et al., 2009). Many of these antigens are also
associated with poor clinical prognosis. EGFR and MUC-1 are, for example, two
antigens that we have already encountered.
The epitope is a subset of antigens that allows recognition between the different
entities involved. Also called "antigenic determinants", epitopes are small
peptides of 10 amino acids that show an affinity for the HLA-A2 receptor resulting
in a cytotoxic T response as it is recognised by T cell receptors (TCR) specific to
them. Thus, only HLA-A2 positive patients are likely to have access to this therapy;
other patients are not eligible. The higher the affinity between the three molecules
(epitope, HLA-A2 and TCR), the stronger the immune response will be.
Therefore, OSE Immunotherapeutics chose a "multi-epitope" approach with a
combination of nine neo-epitopes directed against five tumour antigens chosen for
their poor clinical prognosis established in several cancers. The five antigens
retained by the company in their Tedopi® product are HER-2 / neu antigen, p53,
CEA (carcinoembryonic antigen), MAGE-2 (melanoma antigens) and MAGE-3
(Andre et al., 2004; Wang 2005; Matsuoka et al., 2007; Sienel et al., 2007; Calikusu
et al., 2009; Hanagiri et al., 2011;. Horinouchi et al., 2012). The exact composition
of Tedopi® is based on the epidemiological frequency of tumour antigens. The
company chose three epitopes against CEA (the most common antigen), two
epitopes against p53, two epitopes against HER2 / neu, one epitope against
MAGE- 2 and one epitope against MAGE-3. A last epitope stimulating the "helper"
T cell function was also added to the formulation. In summary, Tedopi® is the
combination of 10 synthetic peptides. The company estimates that 90% of
invasive tumours express at least one of the five tumour antigens.
To improve the immune response of their combined compound, the company also
sought to optimise different epitopes. These are chemically synthesized by the
company and are then modified (hence the term "neo-epitope") to improve
significantly the affinity of some epitopes for HLA-A2 receptors and other for TCR.
It is the combination of the two families of epitopes that induce the increased
cytotoxic T lymphocyte response. The addition of the T helper epitope also called

OSE Immuno, 6 July 2016 31/66 Portzamparc
"Pan DR epitope" (or PADRE) facilitates the immune response and sustainability
by co-stimulation.
R&D expenses of the selection work, modification, and optimisation and
combination amounts to €164 million, started more than a dozen years ago by the
team of Alex Sette and his company Epimmune.
Injection of the compound elicits a synergistic cytotoxic T lymphocyte immune
response by allogenic restriction without immuno-dominance. Indeed, despite the
allocation of nine neo-epitopes to the most frequently found antigens, there is no
preferential response for one or two epitopes. The result is then the tumour
destruction of cells expressing HLA-A2 and at least one of the five antigens via the
specific production of cytotoxic T lymphocytes. The main target tested for the use
of Tedopi® by the company is NSCLC; other tests will also be conducted for other
cancers. The company also plans trials in combination with other
immunotherapeutic products or targeted therapy.
II – 2 Tedopi® and therapeutic effects
The company has achieved three clinical trials in NSCLC: two Phase I / II trials to
determine the level of tolerance and pharmacological response to different doses
and administration rates, and one Phase II trial. In the first two cases, the tests
were conducted on positive HLA-A2 patients only.
II – 2 – a) Phase I/II (NSCLC)
During this study conducted in the US, 10 patients with early NSCLC (stage IIa and IIb) received six subcutaneous injections of 5 mg / epitope spaced three weeks apart with an efficacy endpoint on the quantification of the specific cytotoxic T response induced by neo-epitopes and natural epitopes. The T-cell response was measured by a test known as ELISPOT IFN-γ (enzyme-linked immunosorbent spot assay), which assesses the cytotoxic T lymphocyte response by measuring the levels of interferon gamma produced by cytotoxic T lymphocytes. Six patients completed treatment in its entirety.
II – 2 – b) Phase I/II (colon cancer)
This trial was also conducted in the US on 14 patients with stage III colon cancer
and 10 of them completed treatment in its entirety. They have also received six
doses spaced three weeks apart.
During these two Phases I/II, 15 of 16 patients (six NSCLC and 10 colon) receiving
six injections showed a positive immune response with regards to at least one
epitope. The non-responder patient actually showed an HLA A2 profile less
responding at least in terms of immunogenicity (a genetic sub-type called "HLA-
A*0207"). Eight patients of 15 responded to more than five epitopes with an
average induction of cytotoxic T4 response against four epitopes. These results
show the positive effect of the compound on the immune system in addition to good
tolerance of patients to the product.
In addition, blood sample studies of three patients (ex vivo study) showed effector
activity of T cells extracted from tumour cell samples (primary cells and cancer
cell lines) expressing the antigens targeted by the epitopes, indicating the
"memory" aspect of defence activated by Tedopi®.

OSE Immuno, 6 July 2016 32/66 Portzamparc
II – 2 – c) Phase II
The results of Phase II have generally shown positive results with beneficial
effects for patients including greater median survival in the medium and long
term, a higher survival rate at one year, stable disease for three months or more in
89% of cases, an improved survival effect in the case of response to multiple
epitopes and a good safety profile. However, the differences between the different
groups are not conclusive on the desired effect of the product regarding cancer
progression since the results did not show statistically significant differences
between groups. Note, however, that they were reviewed by a scientific committee,
which finally agreed to the launch Phase III, which confirms the therapeutic effect of
Tedopi®.
Survival curve
Source: OSE Pharma
In this multicentre trial conducted in the US, 135 patients (64 HLA-A2 positive
and 72 HLA-A2 negative) with advanced stages of NSCLC (IIIb and IV) were
selected, including 67% metastatic patients. The majority were Caucasian (83%),
the rest being composed of African Americans (9%) and Asians (8%) with a
median age of 64 years. Each member of HLA-A2 positive group received at least
one subcutaneous injection of 5 mg / peptide and the HLA-A2 negative group
received standard treatment determined by the doctor (reference group). Each
patient had experienced treatment failure of at least one first-line treatment.
The group treated with Tedopi® (HLA-A2+) showed higher median survival of
5.3 months and a higher survival rate by 10% compared to the reference group.
Despite higher survival rate in the Tedopi® treated group, differences were not
statistically significant (P-values of 0.063 and 0.086, respectively).
One patient of the 64 patients also showed a complete response and one patient, a
partial response. Considering the case of stabilisation of three months or more of
the patient, a benefit was observed in 89% of patients in the HLA-A2+ group. A
total of 17 patients were able to continue treatment for one year and showed no
evidence of disease progression. The same results were observed for the 14
patients who continued treatment up to two years.

OSE Immuno, 6 July 2016 33/66 Portzamparc
Long-term survival curve
Source: OSE Pharma
With Tedopi®, 25% of patients were still alive after four years. No head-on
comparison is available regarding this survival rate, but some publications show
that it was 1% after four years for metastatic NSCLC patients, which denotes the
very significant effect Tedopi® in this type of situation. The median time without
disease progression was estimated at 9.4 months with 47% of patients with no
progression of their cancer at one year.
Evaluation of the immune response showed that nine neo-epitopes were
immunogenic in at least one patient, 91% of patients responded to at least one
epitope, 85% to at least two epitopes, 64% to at least three epitopes, 39% to at
least four epitopes and finally 18% to five and more epitopes. Greater survival was
also observed for patients responding to a greater number of epitopes (P value
0.001) – a result that was determinant for passage in Phase III. Thus, patients
responding to four or five epitopes showed a median survival of 875 days against
406 days for patients responding to one epitope or less. In most cases, moreover,
the response of patients was significantly higher for neo-epitopes compared to
unmodified epitopes (wild type).
Percentage of patients responding to neo-epitopes
Source: OSE Pharma

OSE Immuno, 6 July 2016 34/66 Portzamparc
The cytotoxic T lymphocyte response is sustainable over time since it persists at
12 months. Finally, "helper" T cells directed against PADRE were detected in 18 of
33 patients tested.
In summary, despite no significant differences in survival at one year and median
survival, Tedopi® shows significant results since these two figures are
respectively increased in the group treated with the product. Given that median
survival is typically less than eight months in the context of conventional
chemotherapies such as pemetrexed and docetaxel presented in other studies, it
appears that the control group used for comparison of Phase II is biased heavily in
terms of overall survival (12 months). Thus, a more head-on comparison would in
theory show greater differences than those observed in this study. Tedopi®
causes a T-cell immune response directed against at least one of the epitopes of the
mixture.
The response to different epitopes and especially the number of epitopes is also
correlated to survival, which reinforces our use of the product in the context of
cancers presenting associated antigens. Finally, the safety profile was appropriate
with mostly local reactions or pain at the injection sites confirming the absence so
far of a systemic inflammatory response.
II – 2 – d) Phase III
Following these encouraging results, the company decided to continue product
development in NSCLC with Phase III (Atalanta 1) conducted under the leadership
of a steering committee co-chaired by two clinical expert specialists in lung
cancer: Dr Benjamin Bess and Professor Giuseppe Giaconne. The study - accepted
by the FDA (Food and Drug Administration) and the EMA (European Medicines
Agency) - started in January 2016 in Europe and the United States. This is a
multicentre, randomised study with a population of 500 HLA A2+ patients in
advanced stages of NSCLC (stage IIIb and IV). Tedopi® is tested against
chemotherapy (docetaxel / pemetrexed) after failure of first-line treatment
(50/50 ratio). The first patient was enrolled in February 2016. The primary
endpoint is overall survival and the secondary endpoints are progression-free
survival, quality of life, overall response rate and safety. The results of the study
are expected in 2018. Of the 500 patients, 80% were recruited in Europe.
II – 2 – e) First agreement for distribution in Israel
In May 11, 2015, the company signed an initial agreement for licensing and
distribution with the company Rafa Laboratories, a pharmaceutical company
specialised in oncology and rare lung diseases. The agreement allowed obtaining
an upfront payment of €100,000 and also planned milestone payments. If Phase
III is successful, OSE Immunotherapeutics will share equitably the profits from
sales of Tedopi®. Although Israel is a small market, this first agreement is
reassuring for the technology and its potential.
II – 3 Other opportunities for Tedopi®
Knowing that the antigens targeted by Tedopi® are not limited to lung cancer, but
are also found in other forms of cancer, the company also seeks to show efficacy in
these other cancers through the launch of various Phases II. The company is
currently planning a Phase II trial of which the choice has not been finalised,
except that the cancer must show a strong medical need, have some association

OSE Immuno, 6 July 2016 35/66 Portzamparc
with HLA A2 and where the five targeted tumour antigens are expressed at an
advanced stage of the chosen cancer. Without any restrictions, cancers considered
by the company are today ovarian, breast and colon cancer.
The management also plans combination trials for Tedopi®, especially with ICI
and other immunotherapy compounds to achieve synergistic effects on the
immune system (Pardoll, 2012).
II – 3 – a) Ovarian cancer
With about 240,000 diagnoses per year worldwide, ovarian cancer is the sixth
most frequently occurring cancer in women. The overall mortality rate is about
64%. The five-year survival rate in the context of metastatic cancer is 20%
(source: OSE Pharma). It is the leading cause of death in gynaecological cancers
and remains a major problem since this cancer is often resistant and recurrent
(Barnejee et al., 2013). In the same way as lung cancers, ovarian cancers are often
diagnosed at advanced stages.
II – 3 – b) Breast cancer
There are different genotypes of breast cancer; the company considers triple-
negative breast cancer that represents 15% to 25% of breast cancers. Triple-
negative breast cancers are cancers where neither the oestrogen or progesterone
hormone receptors, nor the HER2 protein are present in mammary cells. The
absence of these three receptors makes using the standard treatments (hormone
therapy and Herceptin®) obsolete.
The incidence of triple-negative breast cancers is 367,000 persons in Europe,
233,000 in the US and 183,000 in China. Diagnosis is usually made late so cancer
has usually already spread to other organs (source: OSE Pharma).
II – 3 – c) Colon cancer
Already tested on some patients with colon cancer in Phase I/II, the use of
Tedopi® for this type of cancer would be perfectly possible. Colon cancer is
ranked third in terms of frequency (13% of new cancer cases) and it significantly
affects the populations of industrialised countries. It is more or less equi-
distributed between men and women. In France, there are 40,000 new cases per
year and 17,500 deaths.
II – 3 – d) In combination
Finally, the company also plans to initiate a Phase II trial in 2017 with Tedopi® in
combination with an immune checkpoint inhibitor acting on PD-1 or PD-L1 in
priority in lung cancer. The choice has, again, not been decided. Nivolumab would
be an attractive target because of its approval in squamous NSCLC cancers.
In conclusion, these different indications are growth factors for the product that
show a significant number of patients and situations for which few options are
available, placing OSE Immunotherapeutics’ product in an excellent position to
provide benefit to patients.

OSE Immuno, 6 July 2016 36/66 Portzamparc
III – OSE Immunotherapeutics: synergy in immunotherapy
Announced in February 2016, the merger between OSE Pharma and Effimune to
create the company OSE Immunotherapeutics must bring significant synergy for
the different products that both companies offer. By pooling all of the drug
candidates of both companies, the new entity is left with a diversified portfolio of
five products in clinical and preclinical phases. These five products may also be
considered in combination to treat various diseases, including lung cancer.
Consolidated portfolio
Source: OSE Immunotherapeutics
III – 1 Effimune: brief history and merger
Effimune was registered in the Nantes R.C.S. in 2007 under the name of TCLand
Pharma, but in 2011 it was renamed "Effimune". The biotechnology company
specialises in immune regulation. It develops various clinical applications in
autoimmunity, transplantation and immunology-oncology.
The purpose of the merger between the two companies is to create an
international leading group dedicated to developing immunotherapy activation
and regulation. On 24 February 2016, the companies announced their merger,
which became effective on 31 May 2016.
After the merger, OSE Pharma shareholders own about 71% of OSE
Immunotherapeutics while Effimune shareholders own 29%. They received 1.93
new shares issued by OSE Pharma (about 4 million new shares) for each share
owned by Effimune. Given the strong academic relationships forged by Effimune
in the Nantes region, the headquarters of the new entity will be moved from Paris
to Nantes. The merger is slightly dilutive for OSE Pharma shareholders.

OSE Immuno, 6 July 2016 37/66 Portzamparc
III – 2 Restoration of the immune balance
Immune regulation requires a balance between self-recognition (self-tolerance)
and the destruction of any foreign element (e.g. cells infected with a virus) that can
be harmful to the body. Just as a scale, the regulation goes through a fine
expression of effectors on one side (e.g. cytotoxic T lymphocytes that will destroy
the infected cells, called T or Teff cells) and regulators on the other side (e.g.
regulatory T cells that will positively or negatively influence the effectors, called
Treg cells).
"Autoimmune" diseases are conditions where this self-recognition system is not
effective. The body begins to attack its own constituents and the patient’s immune
system acts as a pathogen system rather than a defence system.
Effimune is a company that develops optimised antibodies whose targets are key
receptors involved in immune regulation. Thus, the company seeks to regulate
immune balance (effector / regulators) to restore the immunological balance. One
of the differentiating advantages of the company is to act on the "brakes" of the
immune system rather than the "accelerators". Accordingly, Effimune’s products
will not balance the system by adding weights to one side or the other of the scale
as other competitors on the market - at the risk of disrupting other metabolic
pathways - but on the contrary, will reduce the weight on one side or the other in
order to achieve a more physiological balance.
Effimune: immune regulation
Source : OSE Immunotherapeutics
III – 2 – a) Markets addressed by Effimune
By developing monoclonal antibodies against various key players of immunology,
Effimune has diversified its addressable markets. The company addresses the
transplantation market and specifically graft rejection (GvHD), autoimmune
diseases including rheumatoid arthritis, multiple sclerosis, Crohn's disease or
ulcerative colitis and finally some liquid cancers, such as leukaemia, or solid
cancers, such as cancer of the kidney and liver.

OSE Immuno, 6 July 2016 38/66 Portzamparc
Biological product revenue by product type
Source: Ecker et al., 2015
In 2013, the global market for monoclonal antibodies totalled $75 billion, which
represented almost half of total revenues from the biopharmaceutical industry. In
2020, it is estimated that 70 antibodies (all types and all applications) will be on
the market and that sales of these antibodies will reach $125 billion (Ecker et al.,
2015). The annual growth rate of these molecules will fall between 8% and 10%
(Ecker et al., 2015. Effimune).
Effimune estimates show a transplantation market of $4.3 billion and $50 billion for
autoimmune diseases. These two indications are covered by FR104 currently in
clinical Phase I and Effi-7, currently in the preclinical phase. The company
estimates the market for liquid cancers, including acute lymphoblastic leukaemia, at
$2 billion. This contract is covered by Effi-DEM, a second-generation immune
checkpoint inhibitor antibody that is currently in preclinical development.
Vasculitis with ANCA (auto-antibodies against neutrophil components) and celiac
disease are two other autoimmune pathologies addressable by the company.
III – 2 – b) Autoimmune diseases: strong therapeutic need
There are more than 80 recorded autoimmune diseases (source: Effimune) with
some well-known diseases such as type 1 diabetes, multiple sclerosis, lupus
erythematosus or rheumatoid arthritis. There are actually two types of
autoimmune diseases: systemic diseases (e.g. systemic lupus erythematosus) and
the specific conditions of an organ (e.g. type 1 diabetes). The causes of these
diseases are multi-factorial: genetic origins, endocrine or environmental. Without
going into detail, some examples of chronic autoimmune diseases targeted by the
company are as follows.

OSE Immuno, 6 July 2016 39/66 Portzamparc
1. Some examples of autoimmune diseases
Rheumatoid arthritis
Rheumatoid arthritis is a chronic inflammatory disease that affects the joints.
With an incidence of 41 per 100,000 persons per year, this disease causes
swelling and pain in the hands, wrists and knees. In addition to night pain and
morning stiffness, inflammation leads in 20% to 30% of cases to degradation
of cartilage and bone, as well as their deformation. The disease can thus be
quite debilitating especially if untreated. In advance stages, the disease can
spread to other organs such as the eye, the heart, lungs, nerves or blood
vessels.
Inflammatory bowel disease (IBD)
The term IBD includes Crohn's disease and ulcerative colitis (incidence of 1.2 to
20 cases per year per 100,000 persons) characterised by chronic inflammation
of the gut wall. In Crohn's disease, the inflammation extends over the entire
gastrointestinal tract (from mouth to anus), whereas for ulcerative colitis is
found mostly in the rectum and colon. These are often diagnosed in young
subjects with 15% of cases in childhood. These diseases are characterised by
diarrhoea, sometimes bloody, abdominal pain, weight loss, anorexia or anal
injury (cracks and / or abscess). The evolution of the disease can also cause
narrowing or closure of the intestine, or the formation of fistula resulting in an
abnormal transit from the intestine to other organs, which require surgery.
Multiple sclerosis
Multiple sclerosis, affecting 2.5 million persons, is a nervous system disease
that affects the brain and spinal cord. The disease attacks the myelin sheath
around nerve cells, which blocks the passage of electrical signals between the
brain and body. The consequences of this blockage are multiple: visual
disturbances, muscle weakness, impaired coordination, numbness, and
impaired memory. Today, it is assumed that the destruction of the sheath is
partly due to the immune system.
The incidence varies greatly from one disease to another. Some are rare
diseases affecting less than one in 3,000 (e.g. systemic lupus, source: Orpha)
and others, more common, affecting up to 1% of the world population (e.g.
rheumatoid arthritis, source: Centers for Disease Control and Prevention). It is
estimated that 3% to 10% of the world population suffer from autoimmune
diseases (Dragin et al., 2016; Effimune). In this sub-population, 10% to 20%
could benefit from treatments based on stimulation of T cells (source:
Effimune).
Women are more affected by these diseases than men (up to 10 times). Indeed,
autoimmune diseases are pathologies involving sex hormones, especially
oestrogen causing this disparity: its expression in women causes a decrease in
the expression of the AIRE protein (autoimmune regulator), a central factor in
self-tolerance. This repression would increase the likelihood of developing an
autoimmune disease by playing, among others, on the population of
regulatory T cells (Dragin et al., 2016). Induced mutations in this gene can
also cause such phenomena, but autoimmune diseases are still polygenic
diseases, that is to say in which more than one gene is involved.

OSE Immuno, 6 July 2016 40/66 Portzamparc
2. Available treatments
Treatment of autoimmune diseases involves symptom relief, prevention of
disease outbreaks, opposition to the evolution to other organs and healing.
Today, there are different symptomatic or disease-modifying treatments to
alleviate autoimmune damage: nonsteroidal anti-inflammatory drugs
(NSAIDs), corticosteroids, immunosuppressors and immunomodulators.
NSAIDs are commonly used drugs for all inflammatory conditions. Their role is
essentially symptomatic. Two examples are ibuprofen and naproxen. NSAIDs
often lead to side effects such as gastrointestinal disorders, heartburn, ulcers
or gastrointestinal bleeding. They are therefore often combined with drugs
that will protect the stomach (e.g. omeprazole and misoprostol) in order to
overcome these various effects.
Corticosteroids, used since the 1950s, are steroid hormones that have anti-
inflammatory and immunosuppressive properties in high doses. The latter, in
particular cortisone, prednisone, prednisolone or methylprednisolone,
negatively affect T cells, antibodies and cytokine production. Used alone, they
are symptomatic treatments, but their side effects (weight gain, osteoporosis,
high blood pressure, infections, etc.) often prevent their very long-term use. In
case of severe crisis, intra-articular injections of corticosteroids may be
recommended one to four times per year.
Immunosuppressive drugs are aimed, as the name suggests, to eliminate or
reduce the immune system to prevent the progression of autoimmune diseases.
The mechanisms of action of these molecules are varied: reduction of the
activity of T cells and blocking transcription of interleukin-2 for cyclosporin A,
DNA synthesis and blocking of dividing cells (B and T lymphocytes) for
azathioprine, mycophenolate mofetil and methotrexate, or destruction and
reduction in the number of B lymphocytes and their immunoglobulin
production via inhibition of protein CD20 for rituximab.
Finally, immunomodulators target modulation of the immune system activity.
Unlike immunosuppressors, they are not limited to inhibition, but may also act
as activators. Anti-TNFα (like adalimumab (Humira), infliximab (Remicade)
and etanercept (Enbrel) are repressor immunomodulators. TNFα protein is a
protein that promotes inflammation in the fight against certain infections.
Most molecules targeting TNFα are monoclonal antibodies. By neutralizing the
TNFα protein (or preventing its binding to its receptor), these molecules
decrease the inflammation process and are therefore used to limit the disease.
Unfortunately, these antibodies end up being the target of the immune system
as the body puts up a defence against them and blocks their action. As such,
anti-TNFα is systematically combined with the introduction of
immunosuppressive treatment. Nevertheless, the patients do not respond to
this treatment in 20% of cases. In addition, in 50% of cases, they no longer
work in patients after one year of use.
Other biological targets of monoclonal antibodies in the context of
autoimmune diseases are CD40 (obinutuzumab of Roche), certain interleukins
such as IL-6R (tocilizumab of Roche), alpha-4 integrin (natalizumab of Biogen
Idec) or CD80 and CD86 (abatacept of BMS).
Intravenous immunoglobulins are also used in immunomodulatory
treatments, firstly for immunocompromised patients (e.g. primary immune
deficiency). These treatments are increasingly used in autoimmune diseases.

OSE Immuno, 6 July 2016 41/66 Portzamparc
To summarise, despite the technological advances of recent years, there is
currently no concrete and effective treatment in the long term against most
autoimmune diseases. Effimune thus appears as a prime competitor in this
market with its various innovative approaches.
III – 2 – c) Transplantation and bone marrow transplant
Transplantation of human organs has a history as old as the use of corticosteroids.
Indeed, the first successful in human kidney transplant was performed by Dr
Joseph Murray in 1954 between monozygotic twin brothers. Since then, many
major advances in surgery as in medicine, including the discovery of tissue groups
(major histocompatibility complex) and the use of suppressive drugs, has
improved the survival rates of transplant patients. Transplantation has become a
method of choice in cases of functional impairment to organs (kidney, liver, heart,
lungs and pancreas).
Today, there are over 3,000 kidney transplants each year in France (5,357
transplants in 2014, more than 60% of organ transplants), but rejection of these
grafts still remains a major problem. In fact, as these grafts being foreign elements,
the body attacks the graft to reject it - this is called alloreactivity, that is to say a
rejection of antigens of the same species, but with different genetics and tissue
structure. Use of immunosuppressors and more particularly the historical
combined use of cyclosporin A (a calcineurin inhibitor - a protein stimulating the
transcription of interleukin-2 and the growth and differentiation of T cells),
steroids and azathioprine (a compound acting against cell multiplication) helps to
slow the rejection. However, whether using this treatment or others, patients are
required to take these drugs daily and chronically to prevent rejection, which may
occur in months or years after transplantation.
In France, the second highest number of transplants after kidney transplants is
liver transplants (22%), followed by heart (8%), lung (6%) and pancreas (1.5%)
transplants. Moreover, it is estimated that over 500,000 persons worldwide are
living with a transplant.
Renal graft survival according to the transplantation period
Source: Effimune

OSE Immuno, 6 July 2016 42/66 Portzamparc
In a slightly different therapeutic universe, transplantation of haematopoietic
stem cells (cells differentiating into all lineages of blood cells, that is to say red
cells, white cells and platelets) is today used for patients with haematological
tumours (benign or malignant). In France in 2014, there were 1,943 bone marrow
transplants. Many complications are associated with this type of transplantation,
the most important being GvHD where the donor's T cells attack the cells of the
host. It is also a disease that appears after some blood transfusions. At a minimum,
the rate of GvHD after transplantation is around 35% (compatible patients),
which rises to 50% when the donor and recipient are not related.
In its acute form, GvHD starts within the first 100 days after transplantation and
causes damage to skin (burning sensation, rash, desquamation), digestive tract
(nausea and vomiting, diarrhoea, abdominal cramps) and liver (volume, jaundice,
liver failure). Depending on the level of damage mentioned above, the disease is
graded on four levels. Acute GvHD is also a major cause of morbidity and mortality
(MacMillan et al., 2002).
Acute GvHD grade
Grade Description
I (mild) Skin rash covering less than 25% of the body
II (moderate) Skin rash covering more than 25% of the body
Mild liver (bilirubin >3.1 mg / dl) and bowel disorders
III (severe) Generalised erythroderma
Moderate liver (bilirubin >6.1 mg / dl) and bowel disorders
IV (life-threatening) Generalised erythroderma with blisters and peeling
Severe liver (bilirubin >15 mg / dl) and bowel disorders
Source: Jacobsohn and Vogelsang, 2007 ; cancer.ca
Chronic GvHD, which usually occurs later after the transplantation, has a higher
probability of occurrence in patients with precedent acute GvHD. In addition to
the already mentioned effects, the chronic form affects more parts of the body
including the eyes (dryness) and mouth (tooth decay and gum disease, drought
and lesions).
Today, GvHD treatment is based on a combination of calcineurin inhibitors and
methotrexate - a duo that has not changed in over 30 years (source: Effimune).
With even higher rates of disease onset, it is particularly important to develop new
and more effective prevention strategies for the disease, but also to prevent graft
rejection.
III – 3 FR104: a change for transplantation and autoimmune diseases
As we have seen so far, T cells form the major components of the immune
response to self antigens or transplanted organs. In addition to the allogeneic
recognition system previously described (see page 28), the immune process
mediated by T cells is reinforced by costimulatory molecules called CD80 and
CD86 and presented by antigen-presenting cells (APC). To enhance the response,
these two molecules bind to a protein receptor on the surface of T cells: CD28.

OSE Immuno, 6 July 2016 43/66 Portzamparc
Recognition between T cells and other cells in the body
Source: Effimune
These costimulatory signals therefore regulate the lymphocyte response. More
generally, a body cell and a T cell seek to recognise each other via different
receptors on their respective surface. Following this recognition and function of
these couples, the immune response will be stronger or weaker.
III – 3 – a) Differentiation based on the mechanisms of action
In addition to CD28, CD80/86 molecules are also able to bind to other receptors,
including the checkpoint immune receptor CTLA 4 (cytotoxic T lymphocyte-
associated protein 4) present on the surface of these T cells. This receptor is today
widely known for its use in the treatment of liquid cancers particularly in
products like Yervoy®. Unlike the combination with CD28, when CD80/86
molecules bind to CTLA-4, they act as "off" switches of lymphocyte activity.
Mechanism of action of the CD28, CD80/86 and CTLA-4 trio
OSE Immuno, 6 July 2016 44/66 Portzamparc
In addition, CTLA-4 is also required for Treg cell function, which limits the
aberrant T-cell immune response and increases the tolerance of grafts (Poirier et
al., 2012). Thus, if the anti-CTLA-4 is an interesting strategy to revive T cells and
destroy cancer cells, their negative effect on Treg may be deleterious in the
context of transplantation (Kirk et al., 2001). In addition, several studies have
shown the theoretical superiority of CD28 targeting CTLA-4 in the context of T-
cell activation and in order to preserve the physiological biological processes of
the immune system and Treg cell function (Butte et al., 2007, 2008. Yao et al.,
2011; Poirier et al., 2011, 2012).
In summary, we have a three-component system: CD28 and CTLA-4 on the surface
of T cells and CD80/86 on the cells to recognise. On the one hand, recognition
between CD28 and CD80/86 promotes the activation, proliferation and survival of
T cells, but reduces Treg function. On the other hand, CTLA-4 and CD80/86 gives
an antiproliferative signal to T cells and is essential for the suppressive function of
Treg (Poirier et al., 2014).
The anti-CTLA-4 strategies such as that used by the ipilimumab is based on the
interaction of the CD80/86 and CTLA-4 combination and seek to prevent
recognition between molecules so that the T cell remains active and destroys the
cells (cancerous).
Contrarily, strategies used by Abatacept and Belatacept targeting the bond
between CD28 and CD80/86 by specifically inhibiting CD80/86, seek to reduce
the effectiveness of the immune system by preventing the activation of T cells. By
the edge effect, the specific inhibition of CD80/86 blocks the interaction between
CD80/86 and CTLA-4, which is important for Treg regulation. This approach still
has a strong interest for autoimmune diseases as it reduces ultimately the
immune response. Belatacept has shown beneficial effects on the survival of
grafts, renal and cardiovascular function, and metabolic risk with the use of
calcineurin inhibitors in the context of kidney transplants (Vincenti et al., 2010,
2012). However, in the Phase III trial with Belatacept, a fairly high rejection rate
was still observed. In addition, the product was used in combination with steroids,
which would prevent its use in the very long term.
By selectively targeting CD28, Effimune overcomes the issue of Treg cell regulation
while limiting the activation of cytotoxic T lymphocytes (Poirier et al., 2010, 2011).
In addition, this mechanism of action has been confirmed in recent discoveries,
including on the interaction between PD-L1 (another immune checkpoint) and
CD80 (Butte et al., 2007) as well as CD28 and ICOSL (Inducible T-cell Co-
Stimulator Ligand) (Yao et al., 2011). However, we will not describe these two
mechanisms in detail.

OSE Immuno, 6 July 2016 45/66 Portzamparc
FR104 and its action on lymphocytes
Source: Effimune
Effimune is developing a monoclonal monovalent antibody fragment (only binding
to a single receptor) called FR104, which specifically targets the CD28 protein to
decrease unwanted immune responses and prevent transplant rejection. For Teff
cells, blocking CD28 results in inhibition of these cells while for Treg cells,
upregulation is induced. Metaphorically, the product brakes immunity then
accelerates it.
III – 3 – b) A pegylated humanised antibody fragment?
Under the term FR104 hides a “pegylated heterodimeric humanised monovalent Fab antibody fragment”.
An antibody is a combination of different protein chains called heavy (blue in the figure) and light (yellow and green in the figure) whose role is the recognition of antigens. In the body, they are produced by B cells (also from bone marrow) and form with T cells another facet of adaptive immunity. The role of antibodies is to identify and disable any pathogen.

OSE Immuno, 6 July 2016 46/66 Portzamparc
General descriptive diagram of an antibody and FR104
Source: Effiumune, Mary et al., 2012
The term "fragment" refers to a sub-fraction of the original antibody, including the
"Fab" part - on the right of the figure - which is the combination of light chains and
part of the heavy chains. This sub-section has the same affinity for the target as
the complete antibody (Fc + Fab).
The term "humanised" describes a process for potentiating antibodies so that they
are not recognised as foreign bodies by the host.
The term "heterodimer" refers to the combination of two non-identical complexes.
In other words, the two heavy chains and two light chains are slightly different in
their composition.
Finally, the term "pegylation" is a method of adding PEG (polyethylene glycol, a
chemical compound widely used in biology) to the molecules in order to protect
or to change some of their biological properties. In this case, pegylation allows
better blood stability in the absence of modification.
III – 3 – c) Proof of concept and Phase I results
The company has conducted numerous clinical studies to demonstrate the efficacy
and prove the concept of their product both in vitro and in vivo. Effimune was able
to test its product in the context of heart (Dong et al., 2002; Dugast et al., 2008;
Jang et al., 2008), liver (Urakami et al., 2006) and renal (Laskowski and al., 2002;
Haspot et al., 2005; Poirier et al., 2010, 2012) transplantation.

OSE Immuno, 6 July 2016 47/66 Portzamparc
1 In vitro studies
In its in vitro models, the company showed selective targeting of CD28 in
addition to a much better reduction in the activity of the protein by
monovalent compounds (Fab' and FR104), thus validating their drug design
(Mary et al., 2012). Moreover, it showed selective inhibition of the binding
between CD80/86 and CD28 while preserving the CD80/86 and CTLA-4
interaction (Dilek Nahzil, PhD thresis, 2011).
CD28 targeting by FR104 in vitro
Source: Mary et al., 2012
FR104 also has a capacity for inhibiting binding between CD28 and CD275
(Poirier et al., 2012.), another receptor on the surface of certain APC cells involved
in the recruitment of T cells (Youngnak-Piboonratanakit et al., 2006).
By these processes, the molecule is able to slow the proliferation of T cells, but
also that of cytokine synthesis including gamma interferon and interleukin-2, key
molecules in the processes of cellular communication and immune regulation.
Finally, FR104 induces a Treg cell response, which causes a suppressive effect on
the T-cell response.
In summary, each in vitro study conducted by the company shows the antibody
operating mechanism via the famous CD28, CD80/CTLA-4 and 86 trio, resulting in a
double suppressive effect on the immune response to regulate negative effects on
autoimmunity and transplant rejection.

OSE Immuno, 6 July 2016 48/66 Portzamparc
FR104 effects on T-cell proliferation
Source : Mary et al., 2012
2 In vivo studies
If the results obtained in vitro are solid, it is essential before moving on to humans to perform animal tests. Through this type of testing, the company has shown, for example, that FR104 indeed inhibits graft rejection over two months in mice by modulating the expression of Treg cells (Poirier et al., 2012). The product also showed a synergistic effect with others commonly used, such as calcineurin inhibitors, and thus produces a long-term beneficial effect on the development of antibodies against the graft (Poirier et al., 2015).
FR104 efficiency in mice in the context of GvHD
Source: Poirier et al., 2012
OSE Immuno, 6 July 2016 49/66 Portzamparc
Moreover, the company recently published an article where a comparison with
Belatacept was conducted in the context of renal graft rejection in baboons. FR104
showed a complete lack of graft rejection in contrast to Belatacept, which showed
four rejections in five transplants (Ville et al., 2016). This last result is particularly
interesting because it clearly demonstrates the superiority of the mechanism of
action described by the company for this type of pathology.
Outside the field of transplantation, Effimune also conducted trials in autoimmune
disease models including encephalomyelitis (Haanstra et al., 2015), rheumatoid
arthritis (Vierboom et al., 2015, 2016), uveitis (an eye disorder; Silver et al., 2000)
and psoriasis (Raychaudhuri et al., 2008) with a beneficial effect of FR104 shown
in each case.
In conclusion, animal studies confirm the therapeutic effect of FR104 in
autoimmune diseases and in transplant rejection. Although seldom relevant to
humans, these results in animals and all molecular studies strongly reassure of its
use in humans.
3 Clinical data
The Phase I trial that determines the safety, pharmacokinetics (study of
the fate of a substance following administration) and pharmacodynamics
(study of the effect of a substance following administration) is still
ongoing. The study report of Phase Ia, conducted in healthy individuals,
is expected in late May/early June. According to the feedback from the
company, the preliminary results are quite satisfactory. The end of the
trial and the report will mark either the entry into Phase Ib (tolerance in
patients) or Phase II directly.
Following these results, and in the following three months, Janssen Biotech
(Johnson & Johnson group) will have to decide to exercise the license option it
currently has on the product. The decision is expected in the second half of 2016. In
connection with the license option, payments when reaching the milestones
totalling € 155M will be paid and will be accompanied by royalties approaching
10% on worldwide annual sales. Janssen Biotech should initiate Phase II, probably
in rheumatoid arthritis in first approach. It is important to note that Janssen Biotech
has already made some payments that have helped cover the R&D expenses in
FR104 in 2013 and 2014.
III – 3 – d) Competition in CD28
Based on all the biological results and already seen on allogeneic recognition and
the tripartite modulation system of CD28, CD80/86 and CTLA-4, it is not
surprising that other competitors are seeking to develop their own product
targeting CD28. This is the case especially for BMS with Lulizumab Pegol and
TAB08 developed by TheraMAB. Unlike TAB08, Lulizumab is a direct competitor
of FR104. Indeed, TAB08 is, unlike the other two products, an agonist of the CD28
receptor, that is to say that its role is not to inhibit receptor function, but to
promote it. The response is the inverse of that sought by FR104 and Lulizumab
although the biological target is exactly the same.
1 Lulizumab Pegol
The product is currently being tested in Phase II versus placebo in America
(North and South), Europe, Lebanon and Russia in the treatment of systemic
lupus erythaematosus. The product is fairly close to the FR104 structure

OSE Immuno, 6 July 2016 50/66 Portzamparc
consisting of a conjugated antibody protected by polyethylene glycol (Yang et
al., 2015).
2 TAB08
By binding to CD28 competitively, TAB08 (formerly TGN1412) strongly
activates the activity (known as a "super agonist") of cytokine release of T
cells resulting in a phenomenon that promotes inflammation. The first trials of
this product led to stopping the clinical trials immediately due to systemic
inflammatory reactions, including cytokine storms. The Russian company
TheraMAB took over the product and tested it at lower doses. It plans to
initiate Phase II in the context of chronic lymphocytic leukaemia and
rheumatoid arthritis.
Effimune is thus in a good position to develop its product. BMS remains a very
serious competitor, especially considering its liability in immunotherapy.
However, Effimune’s product still has validated high differentiating potential
shown through various preclinical studies conducted by the company.
Besides FR104, Effimune has in its portfolio two other molecules currently in the
preclinical phase, which represent growth drivers for the company.
III – 4 Effi-7: autoimmune diseases and transplantation via a different mechanism
All the immune mechanisms that we have discussed so far involve many more
molecules than those presented in this study. Interleukin-7 (IL-7), for example, is
a cytokine involved in survival, development and homeostasis (ability of a system
to maintain its balance) of T cells (Fry et al. 2001). In the presence of mutation in
the gene for IL-7, the immune system is diminished, which is called
immunodeficiency (Holm et al., 2005). Consequently, and in the same way as for
CD28, targeting IL-7 could undermine immune adverse effects to reduce the effect
of autoimmune diseases and alleviate graft rejection (Dooms, 2013).
Effect of interleukin-7 on the immune system
Source: Gao et al., 2015

OSE Immuno, 6 July 2016 51/66 Portzamparc
Expression of receptor to interleukin 7 (IL-7R) by virtually all cells except Treg
cells (Seddiki et al., 2006) confirms the therapeutic approach since a product
blocking IL-7 inhibits Teff cells but not Treg cells, thus inducing a double
suppression of the immune response.
Effi-7 is a humanised monoclonal antibody directed against IL-7R and more
particularly, against a sub-part of the interleukin: CD127. Indeed, IL-7R consists of
two protein chains, CD127 specific to IL-7R and CD132 common to other
receptors IL (IL-2R, IL-4R, IL-7R, IL-9R, IL-15R). Effi-7 therefore binds to CD127
and limits or blocks IL-7 and the bond between CD127 and CD132, making the
receptor ineffective. It is therefore an immunomodulator. The differentiating
feature of this antibody relative to others against same target is the lack of
receptor internalisation. This feature blocks Teff cells without affecting Treg cells.
Mechanism of Effi-7
Source : Effimune
The product has shown efficacy in various models, including inflammatory bowel
disease (Willis et al., 2012), type 1 diabetes, multiple sclerosis and rheumatoid
arthritis, in addition to promoting immune tolerance in the context of allo-
transplantations (May et al., 2014).
Below are presented some results on inflammatory bowel disease models
following treatment with Effi-7. The product indeed limits inflammation to bring it
back to a normal level.

OSE Immuno, 6 July 2016 52/66 Portzamparc
Effi-7 treatment in mice
The project is expected to enter the clinical phase in 2017 although nothing has
yet been officially announced.
Eff-7 has two competitors: GSE2618960 developed by GSK, but interrupted in
June 2013 due to fraudulent study data and PF-06342674 developed by Pfizer,
which causes internalization of the IL-7R receptor. It is currently in Phase I in
knowing that Phase Ib in multiple sclerosis was completed in April 2015 by
corporate strategic decision.
III – 5 Effi-DEM: a second-generation immune checkpoint inhibitor
The latest company product addresses a therapeutic facet abuzz today: the field of
immune checkpoint inhibitors.
The characteristic of the product developed by the company is that it does not
target lymphocyte receptors like most of its competitors, but receptors on the
surface of two types of cells present heavily in the tumour environment:
macrophages (TAM – tumour- associated macrophages) and myeloid cells (MDSC
or myeloid-derived suppressor cells), hence the term "second-generation immune
checkpoint". Both types of cells show immunity and Teff-cell suppressive
functions, which increasing tumour development (Chanmee et al., 2014).

OSE Immuno, 6 July 2016 53/66 Portzamparc
Immunosuppressive network of tumour by myeloid cells
Source: Kusmartsev and Vieweg, 2009
The precise target of Effi-DEM is SIRP-alpha (Signal Regulatory Protein α), a
receptor highly expressed by TAM and MDSC and thus promotes the restoration of
the immunosurveillance (Hanna et al., 2015). The company was able to
demonstrate in in vivo models, including liver, melanoma and breast cancer, that
treatment alone or in combination with other immune checkpoints allowed a
powerful and sustainable anti-tumour action. Indeed, after reimplantation of
tumour cells in treated animals, the latter showed immune defence against the
tumours.
In fact, the product can also be used in combination with other ICI, particularly
those targeting PD-1 and PD-L1, or any product stimulating the immune system to
take advantage of synergistic effects on immunity. It remains today, to our
knowledge, the only treatment aimed toward this type of cells.
Effi-DEM is now considered for use in ulcerative colitis and acute T-lymphoblastic
leukaemia. These two indications are explored through a collaborative
programme funded in part by Bpifrance and called EFFIMAB. With a total budget
amounting to € 20 million, it allows further development of the molecule until and
including Phase 2. The programme groups six French partners, including
Effimune, PX'Therapeutics, two Inserm units of Nantes, Assistance publique -
Hôpitaux de Paris-St Louis and the Regional University Hospital of Lille.
In conclusion, Effimune and therefore OSE Immunotherapeutics target many
applications through its immunotherapeutic approaches. As part of the immune
system, the targets involved in various immunological mechanisms are often the
same whatever the application, so the company covers numerous and varied
diseases. Through its merger with OSE Pharma and mechanisms of action of the
products offered by the two companies, the number of diseases covered is still
rising and we take strength from the synergy resulting from the merger.

OSE Immuno, 6 July 2016 54/66 Portzamparc
IV – Repositioning in cystic fibrosis
The OSE-1101 molecule or tritoqualine is a molecule that has been used in various
allergic diseases and has been marketed by Novartis since 1960. It is a molecule
inhibitor of histidine decarboxylase, that is to say a histamine modulator.
The goal of this programme is to improve the respiratory function of patients with
cystic fibrosis. Given the highly reliable safety profile of the molecule, established
over these many years of use in allergy, it would enter immediately into Phase II
in case of positive results in transgenic animals.
IV – 1 Cystic fibrosis
Cystic fibrosis is an inherited autosomal genetic (carried by the non-sex
chromosomes) recessive (requires that both parents provide the mutant version
of the gene to appear in the progeny) disease related to modification of a receptor
located on the surface of lung cells. This assignment is not limited to the
respiratory system, but is also found in the ORL system, digestive tract, liver,
pancreas and reproductive organs.
As part of the lung damage, genetic modification causes chronic respiratory
infections. 80% of cystic fibrosis is diagnosed in newborns. The life expectancy of
patients with this disease is 36 years.
The causative gene of cystic fibrosis is CFTR (cystic fibrosis transmembrane
conductance regulator), a transmembrane protein involved in the control of water
and chloride ion flow into and out of the lungs. Genetic modifications of the
protein cause mucociliary clearance defects (blocked protein channels) and thus
the accumulation of mucus in the airways. This obstruction then causes infection
and inflammation. The phenomenon of obstruction, inflammation and infection
then combine and form a vicious circle that ultimately leads to death of the
patient.
The incidence in Europe and North America is estimated at 1 per 2500 births
(source: CDC). Despite the advances in medicine and the overall increase in the
patient lifespan in recent decades, there is currently no treatment to cure the
disease.
IV – 2 OSE-1101 and competition
OSE-1101 arrives on a market where competition is weak. The recommended
treatments against this disease today are essentially symptomatic: prevention of
undernutrition via a high-calorie diet and prevention of respiratory infections by
common means.
The few products in development are either gene therapies where the objective is
to restore the function of the CFTR gene, or chemical molecules that target the
biological processes associated with CFTR. This is the typical case of Ivacaftor
(Kalydeco® of Vertex), which aims to promote CFTR channel opening. The latter
is used only for certain specific gene mutations.
OSE-1101 acts as an anti-inflammatory agent by reducing the level of interleukin 8
(IL8), which degrades the pulmonary epithelium and increases the symptoms of
cystic fibrosis. Thus, the molecule would be able to preserve lung function and
reduce infections.

OSE Immuno, 6 July 2016 55/66 Portzamparc
Although this molecule is an interesting growth driver for the company, we have
not factored it into our valuations since it is still in the preclinical phase. In
addition, the project seems to be suspended since the merger between OSE
Pharma and Effimune. The molecule will still be tested in chronic inflammation
models, which integrates better into the objectives of the new company.

OSE Immuno, 6 July 2016 56/66 Portzamparc
V – Patents
Product Family Expiry date Country Number of issued patents
Number of
pending patents
OSE-2101
Family 1: Memopi technology and Tedopi® product
April 2024 US, Europe, Canada, Japan, Australia
5 1
Family 2: Peptides with OSE-2101 (SMPPPGTRV)
June 2018 Europe, US
2 0
Other opening November
2034 Argentina, Taiwan, PCT
0 4
OSE-1101
Family 1: Princeps in the treatment of cystic fibrosis
April 2033 US, Europe, Israel, Canada
? ?
FR104
Family 1: CD28.3 antibody and antibody derivatives
December 2021
Europe, US, Japan, PCT
3 0
Family 2: preparing a recombinant monovalent derivative of the CD28.3 antibody
January 2030
Japan, Canada, US, PCT
1 3
Family 3: Selection procedure of a monovalent ligand of the human CD28 receptor binding to the epitope of CD28.3
October 2030
Europe, US, PCT
2 1
Family 4: Humanised antibody derived from the CD28.3 antibody
February 2031 US, Europe, Canada, Japan, PCT
1 5
Effi-7
Family 1: anti-IL-7Rα antibody antagonists
2032 Europe, US, Japan, PCT
0 4
Family 2: anti-IL-7R α antibody antagonists of the IL-7 pathway recognising the epitope on IL-7R α
2035
Europe, US, PCT
0 2
Effi-DEM Family 1 ? PCT 0 2 Family 2 ? ? 0 1
With its five-product portfolio targeting many (if not most) different indications, the
company seems to be well on its way to being a key player in the international
immunotherapy. Different intellectual fronts provide it with strong barriers for entry until
2024 at least.

OSE Immuno, 6 July 2016 57/66 Portzamparc
VI – Capital valuation methodology
Our valuation methodology is based on a series of steps to determine a company
value from the future sales of a drug candidate - they themselves are determined
from several key points: the market (s) targeted by the company, the price of the
said drug, the dates for obtaining marketing authorisation, the company’s business
model, a discount rate, a rise in sales, clinical phases success probabilities and the
company’s tax system.
Determination of the markets targeted by the company through the strategic
analysis of the latter is exposed in part I of this document. These hypotheses are
based on our own expertise and company information; they may need to evolve in
the future and are not source of absolute accuracy.
The total number of patients is generally determined either from a disease
incidence in a population and world population projections estimated by the
world population prospect, for example (incidence by the number of individuals
gives an approximation the number of patients) or from statistical projections
based on retrospective disease studies on particular populations (projections can
be more or less complex to determine the number of patients). Source: World
Population Prospect, Heart Disease and Stroke Statistics, Orpha.net, Pubmed, etc.
The price of the molecules is determined from a benchmark of products in the
same therapeutic area and in the same categories. Wherever possible and to
obtain statistically reliable results, a benchmark of 10 products is taken into
account. In the absence of such information, it is based on estimates of the
company and products more or less close to the estimated price. Source:
pharmatimes, imshealth, company reports, etc.
The price of the molecules by the number of patients then gives the market
addressable by companies. Since it is unlikely for a company to reach 100% of
patients, market share is first determined from data such as competition,
therapeutic area, type of product, safety profile, product price, etc. These shares
are usually between 10% and 30%. They will, however, not be reached for the first
marketing year, but usually after several years that represent the penetration of
the product on the relevant market. This penetration or "ramping" generally
continues for five years (15%, 25%, 50%, 75% and 100%). It obviously depends
on the product, the market and the agreements with the partner.
The company’s business model (BU) determines what will be the type of
remuneration of the latter. Two leading BU in biotechnology are the FIPCO model
(fully integrated pharmaceutical company) where the company supports the
development and marketing of the product (it is necessary to estimate operating
expenses from pre-existing data) and the CRO model (contract research
organisation) where the company does not usually support marketing, but relies
on a FIPCO type of company to market (at least) the product. For FIPCO, the
company receives all income while the CRO model is based on the achievement of
milestone payments (upfront and milestone payments) and royalties on sales of
the product (generally between 5% and 20% depending on the drug candidate's
progress during the signing of the contract). In either case, sales and operating
income are projected for the company (source: LES; Giordano-Collart & Calkins,
2007; Edwards, 2007).
The business model will also determine the tax on corporate profits. For the FIPCO
model, payment (in the case of a domicile in France) is at minimum 33.3% across
all profits while for the CRO model, payment is 15% tax (Article 219 of the CGI;
source: Impots.gouv/legifrance.gouv).

OSE Immuno, 6 July 2016 58/66 Portzamparc
The goal is then to calculate the free cash flow (FCF) from all the above
information as well as depreciation, investment and change in net working capital.
These estimates usually made over 10 years, are based on company data,
projections and comparisons with peer companies. A discount rate is then used to
update the FCF to their present value. This rate is estimated by the CAPM method
(no debt) and depends on a number of market parameters such as the β sector, the
market premium or OAT. This rate is generally between 12% and 16% (source:
Damodaran; Joseph H. Golec & John A. Vernon, 2007; Harrington et al., 2009).
A final step in our capital and valuation process is the estimation of project risk.
This risk is defined as the probability of success of the various clinical phases from
retrospective studies of success and failure for a variety of drug candidates for
various therapeutic areas. These probabilities can also rest on estimates of the
company in the absence of relevant information (source: Hay et al. 2014).
Our methodology estimates the financial flows based on clinical milestone stages
conditionally using a probability tree: In this case, the probability of obtaining the
marketing authorisation depends on the probability of success of Phase III, which
itself depends on the success of Phase II. The image below shows a generic
example for a full clinical project:
Next, the sum of discounted FCF and a normative terminal value that takes into
account flows beyond 10 years while considering the different phases of the

OSE Immuno, 6 July 2016 59/66 Portzamparc
probability of success and clinical advancement of the product are calculated:
Considering , the discount rate; β, a possible decline in the price of the molecule
(after loss of patent), , the growth rate to infinity (OAT or other), the
probability of success in the year " ", and , and the normative year, we have:
The sum of equations 4) and 5) gives the value of the company’s securities. A
sensitivity analysis can also be conducted to find the influence of key parameters
such as the discount rate, the price of molecules, market share, etc.
A peculiarity of the sum of the flows over 10 years is its weighting by the sum of
the project's total probabilities to consider the project statistical consistency in its
entirety over 10 years (the maximum success probability is 100%).
Source: Driessen et al. 2011; Harrington et al. 2009; and with the assistance of Dr Prakash Gorroochurn - assistant
professor in biostatistics department at Columbia (US).

OSE Immuno, 6 July 2016 60/66 Portzamparc
Case of Tedopi® :
2016 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 North American population (k) Lung cancer 1.5% 227 231 234 238 241 245 248 252 256 260 1.5% 227 231 234
NSCLC 86.5% 194 196 199 202 205 209 212 215 218 221 86.5% 194 196 199
HLA-A2+ 45.0% 88 90 91 92 94 95 97 98 100 101 45.0% 88 90 91
PIII/IV 75.0% 66 67 68 69 70 71 73 74 75 76 75.0% 66 67 68
North American market
66 67 68 69 70 71 73 74 75 76
66 67 68
Market share
15% 15% 15% 15% 15% 15% 15% 15% 15% 15%
15% 15% 15%
Ramp up (%)
0% 0% 0% 0% 10% 25% 50% 75% 100% 100%
0% 0% 0%
Patients treated
0 0 0 0 1 3 5 8 11 11
0 0 0
Price per year / patient ($) 70,000
70,000 Gross income per year (k €) North
America 0.9 0 0 0 0 69,300 170,100 340,200 522,900 705,600 718,200 0.9 0 0 0
Israel population (k) Lung cancer 1.5% 5 5 5 5 5 5 6 6 6 6 1.5% 5 5 5
…
Gross income per year (k €) Israel 0 0 0 0 0 1,478 3,750 7,613 11,591 15,686 15,921 0 0 0 0
EU population (k) Lung cancer 1.5% 332 337 342 347 353 358 363 369 374 380 1.5% 332 337 342
…
Gross income per year (k €) EU
0 0 0 0 58,800 147,000 298,200 453,600 613,200 625,800
0 0 0
Total gross income per year (k €)
0 0 0 0 129,742 321,267 646,859 989,379 1,336,229 1,361,690
0 0 0
Milestones 500,000 0 0 25,000 50,000 50,000 100,000 125,000 150,000 0 0 500,000 0 0 25,000
Royalties collected
0 0 0 0 15,569 38,552 90,560 158,301 213,797 245,104
0 0 0
Royalty rates 18% 0% 0% 0% 0% 12% 12% 14% 16% 16% 18% 18% 0% 0% 0%
Revenues collected by OSE (k€)
0 0 25,000 50,000 65,569 138,552 215,560 308,301 213,797 245,104
0 0 25,000
Takeda royalties 4% 0 0 -1,000 -2,000 -2,623 -5,542 -8,622 -12,332 -8,552 -9,804 4% 0 0 -1,000
Tax 15% 0 0 -3,750 -7,500 -9,835 -20,783 -32,334 -46,245 -32,069 -36,766 15% 0 0 -3,750
FCF
0 0 20,250 40,500 53,111 112,227 174,604 249,723 173,175 198,534
0 0 20,250
Discounted FCF
0 0 13,315 23,156 26,406 48,519 65,640 81,635 49,227 49,075
0 0 13,315
Probability 249% 45% 45% 45% 23% 23% 23% 23% 23% 23% 23% 249% 45% 45% 45%
FCF based on a probability
0 0 6,018 5,233 5,968 10,965 14,835 18,450 11,125 11,091
0 0 6,018
NPV Tedopi® 41,048
41,048
Terminal value 49,009
49,009
Total NPV 90,057
90,057

OSE Immuno, 6 July 2016 61/66 Portzamparc
Case of FR104:
2016 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031 2032 2033 2034 2035
North American population (k)
360 038 362 783 365 550 368 337 371 146 373 421 375 711 378 014 380 332 382 664 385 010 387 371 389 746 392 135 394 540 396 959 399 392 401 841 404 305 406 784
Rheumatoid polyarthritis population North America
0,041% 148 149 150 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167
Market share 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30% 30%
Ramp up (%) 0% 0% 0% 0% 0% 0% 0% 15% 25% 50% 75% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Patients treated 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Price per year / patient ($)
20 000
Gross income per year (k €) North America
0,90 0 0 0 0 0 0 0 126 000 210 600 423 000 639 000 856 800 862 200 867 600 873 000 878 400 883 800 889 200 894 600 900 000
Japan population (k) 126 652 126 541 126 430 126 319 125 039 124 971 124 903 124 835 124 768 124 700 124 632 124 564 124 497 124 429 124 361 124 294 124 226 124 159 124 091 117 063
Rheumatoid polyarthritis population Japan
0 52 52 52 52 51 51 51 51 51 51 51 51 51 51 51 51 51 51 51 48
…
Gross income per year (E) Japan
0% 0 0 0 0 0 0 0 41 400 68 400 138 600 207 000 275 400 275 400 275 400 275 400 275 400 275 400 275 400 275 400 259 200
EU population (k) 319 300 320 494 321 697 322 907 319 727 319 958 320 191 320 426 320 663 320 903 321 144 321 388 321 634 321 882 322 132 322 385 322 640 322 897 323 156 323 417
Rheumatoid polyarthritis population
0,041% 131 131 132 132 131 131 131 131 131 132 132 132 132 132 132 132 132 132 132 133
…
Gross income per year (E) EU 0 0 0 0 0 0 0 70 800 118 800 236 400 355 200 474 000 475 200 475 200 475 200 476 400 476 400 476 400 476 400 477 600
Total gross income per year (k €)
0 0 0 0 0 0 0 242 800 405 400 813 400 1 224
200 1 636 800
1 643 400
1 648 800
1 654 200
1 660 800
1 666 200
1 671 600
1 677 000
1 665 600
Milestones 155 000 10 000 10 000 0 20 000 0 0 25 000 25 000 30 000 35 000 0 0 0 0 0 0 0 0 0 0
Royalties collected 0 0 0 0 0 0 0 14 568 30 405 65 072 104 057 147 312 147 906 148 392 148 878 149 472 149 958 150 444 150 930 149 904
Royalty rates 9% 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Revenues collected by OSE (k€)
10 000 10 000 0 20 000 0 0 25 000 39 568 60 405 100 072 104 057 147 312 147 906 148 392 148 878 149 472 149 958 150 444 150 930 149 904
Tax 15% -1 500 -1 500 0 -3 000 0 0 -3 750 -5 935 -9 061 -15 011 -15 609 -22 097 -22 186 -22 259 -22 332 -22 421 -22 494 -22 567 -22 640 -22 486
FCF 8 500 8 500 0 17 000 0 0 21 250 33 633 51 344 85 061 88 448 125 215 125 720 126 133 126 546 127 051 127 464 127 877 128 291 127 418
Discounted FCF 7 391 6 427 0 9 720 0 0 7 989 10 995 14 595 21 026 19 011 23 404 20 433 17 826 15 552 13 577 11 845 10 333 9 014 7 785
Probability 169% 100% 30% 30% 30% 26% 26% 26% 26% 26% 26% 26% 26% 26% 26% 26% 26% 26% 26% 26% 26%
FCF based on a probability 7 391 1 928 0 2 916 0 0 2 037 2 804 3 722 5 362 4 848 5 968 5 210 4 546 3 966 3 462 3 020 2 635 2 299 1 985
NPV SCA 10 081
Terminal value 33 063
Total NPV 43 144

OSE Immuno, 6 July 2016 62/66 Portzamparc
OSE IMMUNOTHERAPEUTICS
Valuation NPV
67,8%
32,2%
1
Te dopi
FR104
Cash Flow statement 11 12 13 14 15 16e 17e 18e Cash Flow 0,0 0,0 -0,2 -2,7 -3,6 5,3 4,7 15,3 Change in WCR 0,0 0,0 0,0 0,8 -1,0 0,0 0,0 0,0 Capital expenditures 0,0 0,0 0,0 0,0 -6,2 0,0 0,0 0,0 Free Cash Flow 0,0 0,0 -0,2 -2,0 -10,8 5,3 4,7 15,3 Asset disposal 0,0 0,0 0,0 0,0 0,0 0,0 0,0 0,0 Financial investments 0,0 0,0 0,0 0,0 0,0 0,0 0,0 0,0 Dividends 0,0 0,0 0,0 0,0 0,0 0,0 0,0 0,0 Capital increase 0,0 0,0 0,0 2,8 20,2 0,0 0,0 0,0 Other 0,0 0,0 0,5 0,0 -1,1 0,0 0,0 0,0 Change in Net Cash 0,0 0,0 0,3 0,8 8,2 5,3 4,7 15,3 Net Cash position 0,0 0,0 0,3 1,1 9,3 14,7 19,4 34,7
P&L Account 11 12 13 14 15 16e 17e 18e Operating income 0,0 0,0 0,0 0,0 0,0 10,0 10,0 25,0 EBIT 0,0 0,0 -0,3 -2,8 -5,4 5,5 4,9 19,2 CIR 0,0 0,0 1,9 1,2 - - - -
R & D - - - - - - - - Cost of R&D 0,0 0,0 0,2 2,0 2,2 2,5 2,8 3,1 Declared Group net Income 0,0 0,0 -0,3 -2,8 -5,6 5,3 4,7 15,3 Cost of personnel - - - - - - - - Avg nb of staff - - - - - - - -
Fixed
Balance Sheet 11 12 13 14 15 16e 17e 18e Equity value (group's share) 0,0 0,0 -0,9 -0,8 14,5 18,5 23,2 38,5 Other 0,0 0,0 1,2 2,0 -5,0 -3,7 -3,7 -3,7 Invested Capital 0,0 0,0 0,3 1,2 9,5 14,8 19,5 34,8 Net Fixed Assets 0,0 0,0 0,0 0,1 0,1 0,1 0,1 0,1 o/w goodwill ' - - - - - - - - o/w financial assets - - - - - - - - Net Cash position 0,0 0,0 0,3 1,1 9,3 14,7 19,4 34,7 WCR - - - - - - - - Economic Asset 0,0 0,0 0,3 1,2 9,5 14,8 19,5 34,8

OSE Immuno, 6 July 2016 63/66 Portzamparc
OSE IMMUNOTHERAPEUTICS
Share Price History
janv.-16 janv.-17 janv.-18 janv.-19 janv.-20
Tedopi/Phase 3
Tedopi/AMM
FR104/Phase 1b/2
5
6
7
8
9
10
11
12
mai-15 août-15 nov.-15 févr.-16 mai-16
Data per Share 11 12 13 14 15 16e 17e 18e Net Cash / share - - 0,03 0,14 0,93 1,04 1,37 2,45 CFPS - - 0,0 -0,3 -0,4 0,4 0,3 1,1 Nb of shares (M) 0,000 0,000 8,026 8,026 10,049 14,156 14,156 14,156 Restated nb of shares ( M ) 0,000 0,000 8,026 8,026 10,049 14,156 14,156 14,156 % dilution ns ns 0,0% 0,0% 0,0% 0,0% 0,0% 0,0%
Calendar

OSE Immuno, 6 July 2016 64/66 Portzamparc
Note to the reader
All notes concerning Portzamparc research (commitment to transparency, policy for managing conflicts of interest, breakdown by recommendation, etc.) may be accessed on the www.midcaps.portzamparc.fr website (institutional clients) or obtained from your financial advisor (private clients).
This release is a general investment recommendation. This document is not intended for persons residing in any country in which specific types of offerings infringe
current laws and regulations in force. This document is not intended for persons residing in the United States of America.
This document may not be published, forwarded or released directly or indirectly outside French territory and specifically not in the United States of America, Canada, Japan or Australia. The information provided in this document has been obtained from public sources that are deemed reliable. Opinions and projected data are those of their authors. Stated assessments reflect their opinion at the publication date and may be revised at a later date. Quantified forecasts have been made according to consistent accounting standards. The transition to IFRS may result in significant modifications to estimates. The issuing company, Portzamparc and any other person shall not be held liable in any manner whatsoever for direct or indirect injury arising from the use of this document. This document may be released in the United Kingdom only to authorised persons or exempted persons, as defined by the UK 1986 Financial Services Act (or any regulation enabling said Act) or to other persons stipulated in Article 11(3) du Financial Services Act (Investment Advertisements) (Exemptions) Order 1996 (as amended). The forwarding, issue or circulation of this document (or of any duplicate of such) is prohibited in the United States of America and for any U.S. national (as defined by rule “S” of the 1993 U.S. Securities Act). Any failure to comply with said restrictions may constitute an infringement of U.S. securities law. The release of this document in other jurisdictions may be subject to legal restrictions; persons in possession of this document must obtain relevant information and comply with said restrictions. This document is neither an offer nor an invitation to acquire or subscribe to negotiable securities or other stocks. It may not serve in any way as an instrument or be used within the framework of any contract or undertaking. It is issued solely for information purposes and may not be duplicated or disclosed to a third party. In receiving this document, you undertake to comply with the restrictions referred to herein above. In its capacity as an investment service provider, Société de Bourse Portzamparc is regulated by Autorité des Marchés Financiers and is authorised by the Committee of Credit Institutions and Investment Companies. Administrative and organisational conditions intended to prevent and avert conflicts of interest concerning the production of financial analyses: Société de bourse Portzamparc has developed internal regulations incorporating measures referred to as “Great Wall of China” that describe the organisation set up to prevent undue circulation of confidential or insider information. The organisation is the responsibility of the compliance officer who sets rules and monitors their application. The organisation stipulates in particular the separation of activities that may constitute a conflict of interest: proprietary asset management, third-party asset management, value enhancement, trading, institutional sales, the assembly of financial operations and financial analysis. Financial analysts, just like all staff members in the brokerage firm, are subject to measures for managing confidential information and to restrictions applicable to investment service providers, as per articles 315-15 to 315-19 of AMF general regulations, and are required to maintain their stock accounts in the brokerage firm. The compliance officer keeps three lists of stocks up to date:
- A list of stocks prohibited for staff members, which contains all the stocks monitored by the financial analysis department and all the stocks under contract with the brokerage firm. As regards analysts in particular, they are also prohibited from intervening personally with regard to any stock in the same sector as the stocks they monitor
- A list of stocks under surveillance, which lists primarily stocks for which one or more staff members in the brokerage firm has confidential information
- A public list of prohibited stocks, which lists stocks for which a financial operation is in progress and for which property asset operations or financial analysis publications are no longer allowed.
The compliance officer monitors operations concerning stocks identified in the above lists. This applies equally to operations for clients, operations for staff members and proprietary operations. The authority, which decides whether or not to undertake financial operations, the Commitments Committee, is subject to a specific system intended to ensure complete confidentiality in discussions and decisions. In the absence of specific criteria laid down by law or regulations, the Portzamparc Group adopts a position on the eligibility or ineligibility of shares in employee shareholder programs on the basis of its interpretation of the spirit guiding the budget law. In so doing, the liability of the Portzamparc group cannot be incurred on the assumption that it may make a mistake in assessment.

OSE Immuno, 6 July 2016 65/66 Portzamparc
Disclaimer
Stock market recommendations
Our stock market recommendations reflect the absolute performance expected from a stock over a timeframe of six to twelve months. They are based on price objectives set by the analyst and include external factors relating to the market environment, which may vary significantly. The Portzamparc analysis bureau draws up its assessments based on a multi-criteria fundamental analysis approach (primarily, but not exclusively, updates of movements, multiples of comparable factors, transaction multiples, sum of parties and net asset values).
STRONG BUY (1): Expected performance over +15%
BUY (2): Expected performance between +5% and +15%
HOLD (3): Expected performance between -5% and +5%
UNDERPERFORM (4): Expected performance between -5% and -15%
SELL (5): Expected performance below -15% or lack of visibility concerning the company’s fundamentals.
12-month history of recommendation changes for the stock
Questionnaire: transparency commitment for potential conflicts of interest In accordance with AMF general regulations (articles 321-129 to 321-132), Société de Bourse Portzamparc provides information on any conflicts of interest, which may occur with the company or companies under review. 1- Analyst’s personal interest Does the analyst in charge of drawing up the analysis have a significant financial interest in one or more financial instruments under study? NO Does the analyst in charge of drawing up the analysis or one of the members of his/her household serve as an auditor, executive or member of the board of directors of the issuer under study? NO 2 - Portzamparc/Issuer conflict of interest Is there a significant conflict of interest between the issuer covered by the analysis Société de Bourse Portzamparc? NO 3 - Portzamparc/Issuer financial interests Are there any significant equity investments between Société de Bourse Portzamparc on the one hand and the issuer on the other? NO Is Société de Bourse Portzamparc on its own or with other legal entities bound to the issuer by other financial interests? NO 4 – Liquidity contract Has a liquidity contract been signed by Société de Bourse Portzamparc and the issuer? NO 5 – Investment service Has Société de Bourse Portzamparc served in the last twelve months as lead or joint lead advisor for the company or companies concerned in a public share offering? NO Have Société de Bourse Portzamparc and the issuer agreed on the provision by the former to the latter of financial analysis production and circulation services concerning the said issuer? NO 6 – Other conflicts of interest Is Société de Bourse Portzamparc aware of other significant conflicts of interest concerning the circulation of this study? NO 7 – Disclosure of the study to the issuer Has a copy of this study without price objectives and recommendations been sent to the company prior to release solely for the purpose of verifying factual data? NO Have the study’s conclusions been modified following its disclosure to the issuer and prior to general release? NO
Date New recommendation Old recommendation
05 Juillet 2016 Acheter

OSE Immuno, 6 July 2016 66/66 Portzamparc
Research
Arnaud GUERIN [email protected] Head of Financial Analysis Nicolas ROYOT, CFA [email protected] Financial Analyst Maxence DHOURY [email protected] Financial Analyst Thomas OILLIC [email protected] Financial Analyst Geoffroy MICHALET [email protected] Financial Analyst Ricky BHAJUN [email protected] Financial Analyst Maxime PRODHOMME [email protected] Analyste Financier Marion ARDIET [email protected] Analyste Financier Stéphanie MANTEIGAS [email protected] Assistant Stéphanie TASSIN [email protected] Assistant Phone 33 (0) 2 40 44 94 09 Institutional Sales
François BREDOUX 33 (0) 2 40 44 95 21 Head of Institutional Sales [email protected] Henri TASSO 33 (0) 2 40 44 95 41 Institutional Sales [email protected] Henrique CRISTINO 33 (0) 2 40 44 95 31 Institutional Sales [email protected] Nitin KHEDNAH 33 (0) 2 40 44 95 11 Institutional Sales [email protected] Alexandre LE DROGOFF 33 (0) 2 40 44 95 48 Institutional Sales [email protected] Franck JAUNET 33 (0) 2 40 44 95 26 Head of Trading, Sales Trading [email protected] Reine HASLAY 33 (0) 2 40 44 95 40 Risks and performances Analyst [email protected]
Nantes : 13 rue de la Brasserie - BP 38629 - 44186 Nantes Cedex 4 - Tél 33 (0) 2 40 44 94 00
Paris : 16 rue de Hanovre - 75002 Paris - 33 (0) 1 40 17 50 08