injectable alginate hydrogels for cell delivery in tissue ... · tions or homeostasis are...
TRANSCRIPT

Acta Biomaterialia 10 (2014) 1646–1662
Contents lists available at ScienceDirect
Acta Biomaterialia
journal homepage: www.elsevier .com/locate /ac tabiomat
Review
Injectable alginate hydrogels for cell delivery in tissue engineering q
1742-7061/$ - see front matter � 2013 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.actbio.2013.12.006
q Part of the Special Issue on Biological Materials, edited by Professors Thomas H.Barker and Sarah C. Heilshorn⇑ Corresponding author. Tel.: +351 226074900; fax: +351 226094567.
E-mail addresses: [email protected] (S.J. Bidarra), [email protected](C.C. Barrias), [email protected] (P.L. Granja).
Sílvia J. Bidarra a,⇑, Cristina C. Barrias a, Pedro L. Granja a,b,c
a INEB – Instituto de Engenharia Biomédica, Universidade do Porto, Rua do Campo Alegre, 823, 4150-180 Porto, Portugalb FEUP – Faculdade de Engenharia da Universidade do Porto, Departamento de Engenharia Metalúrgica e de Materiais, Rua Dr. Roberto Frias, s/n, 4200-465 Porto, Portugalc ICBAS – Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto, Rua de Jorge Viterbo Ferreira, 228, 4050-313 Porto, Portugal
a r t i c l e i n f o
Article history:Available online 12 December 2013
Keywords:Tissue engineeringRegenerationCell deliveryInjectableAlginate
a b s t r a c t
Alginate hydrogels are extremely versatile and adaptable biomaterials, with great potential for use in bio-medical applications. Their extracellular matrix-like features have been key factors for their choice asvehicles for cell delivery strategies aimed at tissue regeneration. A variety of strategies to decorate themwith biofunctional moieties and to modulate their biophysical properties have been developed recently,which further allow their tailoring to the desired application. Additionally, their potential use as inject-able materials offers several advantages over preformed scaffold-based approaches, namely: easy incor-poration of therapeutic agents, such as cells, under mild conditions; minimally invasive local delivery;and high contourability, which is essential for filling in irregular defects. Alginate hydrogels have alreadybeen explored as cell delivery systems to enhance regeneration in different tissues and organs. Here, thein vitro and in vivo potential of injectable alginate hydrogels to deliver cells in a targeted fashion isreviewed. In each example, the selected crosslinking approach, the cell type, the target tissue and themain findings of the study are highlighted.
� 2013 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
1. Injectable cell delivery systems
In many clinical scenarios, where normal physiological condi-tions or homeostasis are compromised, there is a need for tissuetransplantation or implantation. The ideal paradigm in tissue engi-neering consists in introducing cells or tissues grafts, native to theinjured area, to foster the regenerative process. In this context, cell-based therapeutic approaches can thus be considered a vital tool inregenerative medicine strategies. They rely on the successful deliv-ery of living cells to the target location, where they can produce adesired therapeutic effect by paracrine delivery of biomolecules(growth factors, cytokines, hormones, etc.) or replace lost cellswith donor cells that can integrate and regenerate the damagedtissues [1,2]. Cells used for cellular therapies can be previouslymanipulated to produce a missing substance, such as a specificprotein that is absent in a metabolic disease [3].
To ensure that an adequate number of cells reach the target tis-sue, cell-based approaches have usually been based on the deliveryof high-density single-cell suspensions to the site of injury throughinjection. However, such direct cell injection often has a poor out-come due to large and rapid loss of cell viability (thus requiring
high cell densities, which makes it technically complex and alsoextremely expensive), reduced engraftment of delivered cells andlimited control over cell fate, in terms of both site-specificity (withcells eventually migrating and affecting other sites) and cell differ-entiation [4–6]. Therefore, more effective cell transplantationmethods, capable of sustaining the survival of implanted cellswhile maintaining their function and enhancing their incorpora-tion into the host, are mandatory. One strategy to achieve this goalrelies on the delivery of transplanted cells via a temporary supportmade of biocompatible materials that can be further biochemicallyand physically modified to improve cell delivery [7,8]. This strategywill provide cell protection, prolonged retention at the injury siteand a more physiological three-dimensional (3-D) environment.Moreover, many studies have pointed to the importance of strate-gies that promote cell–cell and cell–matrix interactions, which im-pact considerably on cell morphology, viability and function [5,9].For instance, for anchorage-dependent cells, these interactions de-fine cell shape and organization, which in turn will regulate cellbehavior, namely survival, differentiation, proliferation and migra-tion [10]. Hydrogels are candidates of choice to mediate cell deliv-ery and accommodate cells in a 3-D microenvironment due to theirnatural similarities to the extracellular matrix (ECM). One paradig-matic example is alginate, a tunable and versatile natural inject-able hydrogel with huge potential as an artificial 3-D cellularmatrix, which has already been explored in a myriad of studiesas an injectable cell delivery system for a broad variety of biomed-ical applications [11].

S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1647
For clinical applications, cell delivery through injectable materi-als may be a desirable method, since these systems offer specificadvantages over preformed scaffold-based approaches. On theone hand, they can be applied using minimally invasive tech-niques, improving patient compliance and comfort, and eventuallyleading to faster recovery and hence lower healthcare costs. On theother hand, they present several additional appealing features,namely: (i) easy incorporation of therapeutic agents, such as pro-teins or cells, and their subsequent localized delivery; (ii) simplic-ity of implantation by injection; (iii) high contourability, providingadaptable filling of defects with irregular shapes and sizes; and (iv)site specificity as well as confined delivery [12–22]. A key requisiteof cell delivery vehicles is the maintenance of cell viabilitythroughout the injection procedure. For instance, when flowingthrough a syringe needle, cells can experience three types ofmechanical forces that can lead to cell disruption: (i) a pressuredrop across the cell; (ii) shearing forces due to linear shear flow;and (iii) stretching forces due to extensional flow [23]. Therefore,an injectable matrix is also required to exhibit adequate mechani-cal properties to protect injected cells and thereby ensure theirsurvival [23,24].
Injectable cell-based systems can be prepared with differentconfigurations, depending on the type of application. Distinct andoften conflicting terms exist to designate these systems. In thepresent review, we propose a classification (Fig. 1) in which sys-tems have been divided into four main categories: (1) surfaceattachment with a preformed microcarrier, where cells are at-tached to the outside surface of microcarriers or even to the surfaceof inner pores; (2) microencapsulation, where cells are dispersed ina liquid contained within a polymeric membrane or capsule(mainly used for immunoisolation); (3) matrix entrapment, wherecells are embedded in a hydrogel matrix that creates a 3-D envi-ronment, which can be formed in situ or ex situ (as in the case ofmicroparticles); and (4) multicellular aggregates, where cellsself-aggregate spontaneously or upon induction (due to matrixproperties) to present some integrity, despite sometimes being‘‘scaffold-free’’, and can be manipulated as ‘‘microparticles’’ dueto their size. These multicellular aggregates can be further injected
Fig. 1. Cell immobilization strategies for injectable cell-based therapies. Several strategieuse in injectable cell-based therapies. Here, the different approaches were divided into foentrapment; and (4) multicellular aggregation. The bottom images correspond to injecultured for 5 days on the surface of calcium titanium phosphate microspheres, under sta(F-actin) and counterstained with propidium iodide (DNA). (B) Human mesenchymal smicrospheres in basal conditions. (C) hMSCs entrapped and cultured for 8 days inside 2 wAlexa-fluor 488-phalloidin (F-actin) and counterstained with DAPI (DNA). (D) Mouse mwere stained for E-cadherin (red) and counterstained with DAPI (DNA). Adapted from R
using a hydrogel-based vehicle [5]. Although alginate hydrogelshave been employed in all of these types of systems, this reviewwill mainly focus on applications belonging to category 3, thusthe term ‘‘entrapment’’ will be used throughout the text. The mainpurpose of this review is to demonstrate the alginates potential asan adequate 3-D microenvironment for cell delivery, in which cellsare kept in direct contact with this synthetic ECM and, after trans-plantation, might become incorporated in the host tissue and ac-tively participate in the regeneration process. Therefore,categories 1, 2 and 4 above will be described no further in this re-view. In strategy 1, cells are actually in a 2-D rather than a true 3-Denvironment; strategy 2 aims at isolating cells from the host envi-ronment that will most likely not be incorporated in the host; andin strategy 4 the 3-D environment is a result of the natural cellularaggregation and is not necessarily provided by the matrix.
The present review focuses mainly on strategies where cell-la-den alginate-based systems were designed to be delivered in aminimally invasive way and, after injection, allow the transplantedcells to be integrated in the host’s damaged tissue and actively par-ticipate in the regeneration process.
2. Hydrogels in tissue engineering
Hydrogels are 3-D hydrophilic, cross-linked polymeric net-works capable of absorbing a significant amount of water or bio-logical fluids [27]. Chain crosslinking can be achieved bychemical or physical methods, and the large variety of crosslinkingreaction schemes make it possible to control the gelation kineticsand the subsequent hydrogel properties [28]. Hydrogels are com-pliant and permeable structures, mostly constituted of water,which resemble the native ECM, providing an ideal 3-D microenvi-ronment for culturing cells. As a consequence, hydrogels haveemerged as a valuable platform for examining the effects of ECMproperties on cell behavior [9,29–33]. Additionally, they can be fur-ther modified to improve their mechanical and biochemical prop-erties, to better mimic the native ECMs, via physicochemicalmodifications of the gel-forming polymers and/or crosslinking
s and carrier materials can be used for cell immobilization. These can be adapted forur major categories: (1) surface immobilization; (2) microencapsulation; (3) matrixctable alginate-based systems incorporating cells. (A) Bone marrow stromal cellsndard osteoinductive conditions. Cells were stained with Alexa-fluor 488-phalloidintem cells (hMSCs) entrapped and cultured for 21 days inside 2 wt.% RGD–alginatet.% PVGLIG/RGD–alginate hydrogels under basal conditions. Cells were stained withammary epithelial cell line (EpH-4) within 2 wt.% RGD–alginate after 7 days. Cellsefs. [25,26].

1648 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
compounds [14,24,34–40]. Furthermore, many hydrogels can beformed under mild conditions, creating the adequate conditionsfor cytocompatible cell entrapment.
In situ forming hydrogels present the added benefit of injecta-bility, and have been widely studied as cell carriers for in vivo tis-sue engineering [41]. As previously pointed out, injectablehydrogels offer several advantages for cell entrapment and subse-quent delivery, for which purpose they should ideally combine anumber of requisites, such as: (i) be in a sufficiently fluid state dur-ing administration, like a low-viscosity solution, or undergo shearthinning before administration; (ii) gelation should start or becompleted shortly after injection; (iii) be biocompatible and biode-gradable, and their products bioresorbable; and (iv) fulfill specificrequirements according to the application envisaged (e.g. cell-adhesive capability for entrapment of anchorage-dependent cells).
Injectable hydrogels can be obtained from either natural or syn-thetic polymers [42,43]. Naturally derived polymers are frequentlyselected since these hydrogels either include components of theextracellular matrix (e.g. collagen, fribronectin, fribrinogen) orpresent a chemical structure similar to natural glycosaminoglycans(e.g. alginate, hyaluronic acid, chitosan), offering an intrinsicadvantage over synthetic hydrogels [33]. Since they are derivedfrom natural sources, many of them contain cellular binding do-mains, thus allowing cell adhesion and/or present soluble signalingfactors to become intrinsically bioactive and capable of regulatecellular behavior. However, they may exhibit batch-to-batch vari-ations and, in some cases, it is difficult to modulate their usuallypoor mechanical properties [33,44]. Additionally, natural hydro-gels may be inherently immunogenic or give rise to some immuno-genicity due to the presence of contaminates, like proteins andendotoxins. In contrast with natural polymers, synthetic polymersallow better control over and reproducibility of their mechanicalproperties and chemistry [45]. On the other hand, they may pres-ent a low degradation rate in physiological conditions and, in somecases, their preparation involves the use of toxic chemicals. Amongthese, polyethylene glycol (PEG)-based polymers are widely usedas injectable hydrogels for cell delivery, and considerable effortshave been made in order to improve their features, including incor-poration of cell adhesion ligands or biodegradable units suscepti-ble to cell proteolytic activity, making them viable alternatives[38–40].
3. Alginate hydrogels
Alginates are natural anionic biopolymers typically extractedfrom brown seaweeds. They are unbranched polysaccharides con-sisting of 1,4-linked b-D mannuronic acid (M) and a-L-guluronicacid (G) units, which are covalently linked together in differentnumber and sequence distributions along the polymer chain,depending on the alginate source [46]. The functional propertiesof alginate depend on its monomer composition (M/G) ratio andsequence [47]. For example, MG blocks (MGMGMGM) form themost flexible chains and G blocks (GGGGGGG) form stiff chains.Moreover, alginate can be prepared with a wide range of molecularweights (typically 101–103 kDa) [24,47].
Alginates are already used in several clinical applications, e.g.for treatment of heartburn and acid reflux (Gaviscon�, Bisodol�,Asilone™), as wound dressing materials (Algicell�, AlgiSite M™,Comfeel� Plus, Kaltostat�, Sorbsan� and Tegagen™) and as anappetite suppressant for long-term weight loss [48–50]. Alginateis further being currently assessed in several clinical trials, namelyas an agent for weight control, in the treatment of type I diabetesand as temporary acellular scaffolds to attenuate adverse cardiacremodeling [51]. Additionally, tissue engineering alginate productsare commercially available for 3-D cell culture, such as AlgiMatrix
from Invitrogen and NOVATACH peptide-coupled alginates fromFMC Biopolymers.
Alginate is considered to be non-immunogenic and has showngreat potential as a cell delivery vehicle [46,50,52–54]. In Fig. 2several examples of alginate as a cell delivery system are depicted.It is possible to visualize that alginate matrices allow the outwardmigration of different cell types, in this case human umbilical veinendothelial cells (HUVECs) (Fig. 2A and B) and human mesenchy-mal stem cells (hMSCs) (Fig. 2C and D), in different scenariosin vitro (Fig. 2A), ex vivo (Fig. 2B) and in vivo (Fig. 2C and D). Cellmigration from the matrix is a vital process when a cell deliverystrategy is envisaged.
As previously pointed out, an adequate vehicle must providecell protection during injection. Alginate has been shown to havea shielding effect on cells during ejection from a syringe needle.Aguado et al. [23]tested 1 wt.% alginate with three different molec-ular weights on four different cell types (HUVECs, rat MSCs, humanadipose stem cells and mouse neural progenitor cells), and havedemonstrated the protective effect of alginate hydrogels with opti-mized mechanical properties (G0 � 30 Pa). The authors showed thatHUVECs in phosphate-buffered saline (PBS) or in non-crosslinkedalginate have a significantly lower cell viability compared to incrosslinked alginates. Moreover, for all the studied cells, therewas a significantly higher viability in alginate with G0 � 30 Pa thanin PBS or in alginate with a higher modulus. In an earlier study byKong and colleagues [24], the authors showed that it is possible tomaintain the alginate’s gel-forming ability by adjusting its molec-ular weight, while decreasing its viscosity and thus better preserv-ing cell viability (cell viability �80% within 2 and 3.5 wt.% alginatehydrogels). To obtain different molecular weights, the alginate wasirradiated, resulting in solutions with different viscosities and deg-radation rates [47].
Alginate presents a number of benefits for general use in bio-medical applications, coupled with a set of unique advantages forcell encapsulation and entrapment. Alginate allows the formationof hydrogels (with water) in situ, and the gelling process can becarried out using non-toxic solvents and under physiological con-ditions (namely in terms of pH and temperature), which provideeasy cell encapsulation and entrapment. These hydrogels possessa soft nature, making them physically similar to most native tis-sues. Additionally, alginate mechanical properties can be tunedin order to encompass a range of stiffnesses that cover a varietyof tissues. For example, the compression modulus of alginatehydrogels can range from 1 to 1000 kPa and the shear modulusfrom 0.02 to 40 kPa [55]. Alginate mechanical properties can becontrolled by changing different parameters, such as the polymersource, molecular weight, concentration and chemical modifica-tions, and/or the type and density of the crosslinking [46]. Becausethey are transparent, alginate hydrogels allow the routine analysisof entrapped cells using standard microscopical techniques andthey further enable easy cell recovery without cell damage.Regarding batch-to-batch variation and immunogenic response,both can be avoided through the use of highly purified and well-characterized alginates (concerning the molecular weight and theG/C ratio) that are currently commercially available. For instance,highly purified or ultrapure alginate contains low levels of residualendotoxin, lower than 100 EU g�1, and has been shown not to in-duce any severe foreign body reaction when implanted into ani-mals [53]. As major drawbacks for these applications, alginate isslowly biodegradable and is not cell-interactive. However, thesecan be easily overcome by a number of chemical and biochemicalmodifications [14,15,35,56].
Although alginate chains cannot be cleaved by mammalian en-zymes, ionically crosslinked alginate hydrogels disintegrate pro-gressively in vivo due to the exchange between monovalentcations, such as Na+, present in the surrounding milieu and the

Fig. 2. Outward cell migration from alginate hydrogels. In vitro: HUVECs migrating out from an alginate–RGD hydrogel disk and (A) adhering to the bottom of a TCPS cultureplate. Ex vivo: (B) forming tubular-like structures that sprout into Matrigel. In vivo: an hMSC-laden alginate–RGD–PVGLIG hydrogel after subcutaneous implantation in ansevere combined immunodeficiency (SCID) mice, showing (C) a paraffin section stained with safranin/light green (alginate stains in orange and the host tissue and entrappedcells stain in blue) where transplanted hMSC (arrows) can be observed within the disk, and (D) a paraffin section immunolabelled with an anti-human specific monoclonalantibody showing an hMSC still inside the hydrogel (dashed arrow) and another one at the hydrogel periphery (solid arrow), in close proximity with the host mice cells(autofluorescence green staining) (⁄ alginate; orange line – alginate matrix boundary).
S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1649
divalent cations that crosslink the hydrogel. Additionally, alginatecan be modified to become degradable in physiological conditionsby partial oxidation of alginate chains using sodium periodate [56].The periodate oxidation cleaves the carbon–carbon bond of thecis-diol group in the uronate residue and alters the chain conforma-tion to an upon-chain adduct, which behaves similar to an acetalgroup susceptible to hydrolysis. The degradation rate can be fur-ther regulated by adjusting the molecular weight distribution ofoxidized alginates without varying the number of oxidized uronicacids, chain inflexibility and gel-forming ability [35]. The molecu-lar weight can be modified by c-irradiation, which breaks the algi-nate chain [47]. The oxidized binary hydrogels improved theformation of bone tissue compared to non-modified alginate, sincea faster degradation occurs that facilitates the formation of newbone tissues [35]. Additionally, alginates are chemically versatile,allowing the easy incorporation of biochemical cues to engineerspecific cell responses. For example, as cells have no specific recep-tors for binding to alginate, several methods to promote cellattachment to alginate matrices have been developed. These in-clude the coupling of ECM proteins such as laminin, collagen andfibronectin [57–59]. However, since the coupling of an entire pro-tein is difficult to control, can lead to non-specific interactions, mayelicit an immune response and proteins are subject to proteolyticdegradation [60], the decoration of biomaterials with cell recogni-tion motifs, such as small immobilized peptides, has becomepopular. The arginine–glycine–aspartic acid (RGD) sequence wasone of the first peptides to be used to promote cell adhesion on abiomaterial and is still one of the most widely employed. This tri-peptide motif corresponds to the minimal essential cell adhesionpeptide sequence identified in many ECM proteins, such as fibro-nectin, collagen, laminin, osteopontin and vitronectin, which areassociated with integrins in cell surface membranes [60]. Topromote cell adhesion, alginate can be functionalized with thispeptide using the aqueous carbodiimide chemistry, as demon-
strated by Rowley et al. [34]. In this case, RGD peptides are linkedvia a stable covalent amide bond and this reaction occurs betweenthe carboxyl group of the alginate and the N-terminus of the peptide.
Several other combined modifications have been investigated toimprove alginate properties. For instance, the same chemical ap-proach was used to further tailor alginate hydrogels to a moresophisticated ECM-like 3-D cellular microenvironment. Alginatewas grafted not only with RGD but also with a protease-labilecrosslinking peptide (proline–valine–glycine–leucine–isoleucine–glycine, PVGLIG) that is cleavable by metalloproteinases (MMPs)produced by cells [14,15]. The resultant MMP-sensitive hydrogelscan be partially remodeled by cell-driven proteolytic mechanisms,leading to increased cellular evasion/invasion, and are particularlyappealing vehicles for cell-delivery strategies. In another example,alginate was chemically functionalized with cell signaling moietiessuch as galactose to improve hepatocyte cell recognition [61,62].Since hepatocytes have a specific receptor that recognizes this li-gand, cells entrapped within alginate bearing galactose residuespresent higher functionality and survival rate. Also, to mimic therheological behavior of the nucleus pulposus in the intervertebraldisk, Leone et al. [63]have covalently crosslinked alginate by amidebond formation, after activation of the carboxylic groups and theirconversion into amide moieties. They were able to attain arheological behavior very similar to the one of the human nucleuspulposus and, when chondrocytes were added, they were able toproliferate and produce ECM proteins.
According to the aim of the strategy, several other alginatemodifications have been proposed to improve its behavior. Severalalginate derivatives, their properties and possible applications aredescribed in detail in a recent review by Pawar and Edgar [64].One of the greatest potentials of alginate is its mild and diversegel-forming capacity. As described below, alginate hydrogels canbe prepared by various crosslinking methods, which give rise todifferent delivery strategies with equally different outcomes.
1650 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
3.1. Formation of alginate hydrogels
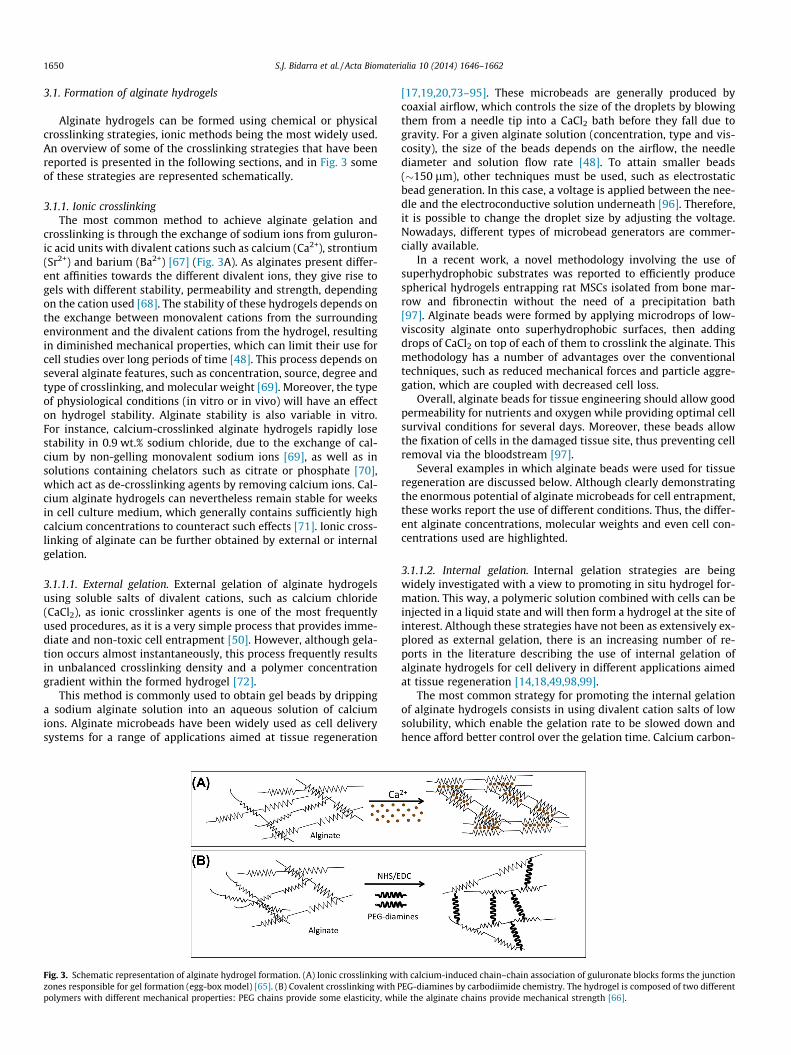
Alginate hydrogels can be formed using chemical or physicalcrosslinking strategies, ionic methods being the most widely used.An overview of some of the crosslinking strategies that have beenreported is presented in the following sections, and in Fig. 3 someof these strategies are represented schematically.
3.1.1. Ionic crosslinkingThe most common method to achieve alginate gelation and
crosslinking is through the exchange of sodium ions from guluron-ic acid units with divalent cations such as calcium (Ca2+), strontium(Sr2+) and barium (Ba2+) [67] (Fig. 3A). As alginates present differ-ent affinities towards the different divalent ions, they give rise togels with different stability, permeability and strength, dependingon the cation used [68]. The stability of these hydrogels depends onthe exchange between monovalent cations from the surroundingenvironment and the divalent cations from the hydrogel, resultingin diminished mechanical properties, which can limit their use forcell studies over long periods of time [48]. This process depends onseveral alginate features, such as concentration, source, degree andtype of crosslinking, and molecular weight [69]. Moreover, the typeof physiological conditions (in vitro or in vivo) will have an effecton hydrogel stability. Alginate stability is also variable in vitro.For instance, calcium-crosslinked alginate hydrogels rapidly losestability in 0.9 wt.% sodium chloride, due to the exchange of cal-cium by non-gelling monovalent sodium ions [69], as well as insolutions containing chelators such as citrate or phosphate [70],which act as de-crosslinking agents by removing calcium ions. Cal-cium alginate hydrogels can nevertheless remain stable for weeksin cell culture medium, which generally contains sufficiently highcalcium concentrations to counteract such effects [71]. Ionic cross-linking of alginate can be further obtained by external or internalgelation.
3.1.1.1. External gelation. External gelation of alginate hydrogelsusing soluble salts of divalent cations, such as calcium chloride(CaCl2), as ionic crosslinker agents is one of the most frequentlyused procedures, as it is a very simple process that provides imme-diate and non-toxic cell entrapment [50]. However, although gela-tion occurs almost instantaneously, this process frequently resultsin unbalanced crosslinking density and a polymer concentrationgradient within the formed hydrogel [72].
This method is commonly used to obtain gel beads by drippinga sodium alginate solution into an aqueous solution of calciumions. Alginate microbeads have been widely used as cell deliverysystems for a range of applications aimed at tissue regeneration
Fig. 3. Schematic representation of alginate hydrogel formation. (A) Ionic crosslinking wizones responsible for gel formation (egg-box model) [65]. (B) Covalent crosslinking with Ppolymers with different mechanical properties: PEG chains provide some elasticity, whi
[17,19,20,73–95]. These microbeads are generally produced bycoaxial airflow, which controls the size of the droplets by blowingthem from a needle tip into a CaCl2 bath before they fall due togravity. For a given alginate solution (concentration, type and vis-cosity), the size of the beads depends on the airflow, the needlediameter and solution flow rate [48]. To attain smaller beads(�150 lm), other techniques must be used, such as electrostaticbead generation. In this case, a voltage is applied between the nee-dle and the electroconductive solution underneath [96]. Therefore,it is possible to change the droplet size by adjusting the voltage.Nowadays, different types of microbead generators are commer-cially available.
In a recent work, a novel methodology involving the use ofsuperhydrophobic substrates was reported to efficiently producespherical hydrogels entrapping rat MSCs isolated from bone mar-row and fibronectin without the need of a precipitation bath[97]. Alginate beads were formed by applying microdrops of low-viscosity alginate onto superhydrophobic surfaces, then addingdrops of CaCl2 on top of each of them to crosslink the alginate. Thismethodology has a number of advantages over the conventionaltechniques, such as reduced mechanical forces and particle aggre-gation, which are coupled with decreased cell loss.
Overall, alginate beads for tissue engineering should allow goodpermeability for nutrients and oxygen while providing optimal cellsurvival conditions for several days. Moreover, these beads allowthe fixation of cells in the damaged tissue site, thus preventing cellremoval via the bloodstream [97].
Several examples in which alginate beads were used for tissueregeneration are discussed below. Although clearly demonstratingthe enormous potential of alginate microbeads for cell entrapment,these works report the use of different conditions. Thus, the differ-ent alginate concentrations, molecular weights and even cell con-centrations used are highlighted.
3.1.1.2. Internal gelation. Internal gelation strategies are beingwidely investigated with a view to promoting in situ hydrogel for-mation. This way, a polymeric solution combined with cells can beinjected in a liquid state and will then form a hydrogel at the site ofinterest. Although these strategies have not been as extensively ex-plored as external gelation, there is an increasing number of re-ports in the literature describing the use of internal gelation ofalginate hydrogels for cell delivery in different applications aimedat tissue regeneration [14,18,49,98,99].
The most common strategy for promoting the internal gelationof alginate hydrogels consists in using divalent cation salts of lowsolubility, which enable the gelation rate to be slowed down andhence afford better control over the gelation time. Calcium carbon-
th calcium-induced chain–chain association of guluronate blocks forms the junctionEG-diamines by carbodiimide chemistry. The hydrogel is composed of two differentle the alginate chains provide mechanical strength [66].

S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1651
ate (CaCO3) and calcium sulfate (CaSO4) have been widely used forthis purpose. They have low solubility in pure water at neutral pH,but are soluble under acidic conditions, allowing its uniform distri-bution in the alginate solution before gelation occurs [72,100]. Freecalcium ions can later be released from these salts by slightlydecreasing the pH with glucone-d-lactone (GDL), thereby allowinggradual gelation. In the case of CaCO3, the CaCO3/GDL molar ratiocan be set at 0.5 to yield a neutral pH [14,72]. It is notable that,although there is a slight decrease in pH, the cell viability is not af-fected [14,18].
As an alternative to GDL, a photoacid generator (PAG) has beenproposed that dissociates under UV light, releasing H+ ions, whichwill react with CaCO3 to create Ca2+ [101]. Despite the great poten-tial of these light-derived hydrogels as cell delivery systems forseveral biomedical applications, their cytocompatibility needs tobe investigated further. Another way to promote photoactivatedinternal gelation consists in the use of water-soluble Ca2+ chelators(‘‘cages’’), which can be mixed with alginate solutions and, uponlight exposure, will undergo an irreversible molecular change thatdecreases their affinity to Ca2+. This will result in the release ofCa2+, which will subsequently trigger crosslinking [102]. In con-trast to the use of insoluble calcium salts, this methodology allowshomogeneous alginate hydrogels to be obtained even in concen-trated alginate solutions (e.g. 10 wt.%). Using this method,improvements in mechanical properties and homogeneity havebeen observed over comparable alginate concentrations.
3.1.2. Covalent crosslinkingCovalent crosslinking of alginate hydrogels can be achieved by a
variety of different methods, and usually provides more stable andmechanically stronger gels than ionic crosslinking. It is beyond thescope of the present article to review them all; instead, we focus onthe strategies used for cell entrapment and delivery. Generally,once a material is covalently crosslinked, it no longer meets theinjectability criteria. There are, however, a few exceptions, suchas photocrosslinking alginates [103] and shape-memory alginatescaffolds [104], which will be explained later on. The major disad-vantages of these methods are their increased complexity and theeventual toxicity of the reagents used.
Covalently crosslinked alginate hydrogels can be synthesizedwith a wide range of mechanical properties using, for example,PEG-diamine molecules with different molecular weights as cross-linkers [66] (Fig. 3B). The elastic modulus of the crosslinked algi-nate changes according to the molecular weight of the PEGmolecules. The hydrogel properties can be further regulated bymultifunctional crosslinking molecules, which provide a widerrange and tighter control over degradation rates and mechanicalstiffness, as demonstrated by Lee et al. [105]. In their work, PAGhydrogels were formed with either poly(acrylamide-co-hydrazide)as a multifunctional crosslinking molecule or adipic acid dihydra-zide (AAD) as a bifunctional crosslinking molecule. This multi-crosslinking strategy led to the formation of stronger hydrogels.
3.1.2.1. Photocrosslinking. Injectable photocrosslinkable alginateshave been proposed for tissue engineering applications and havebeen designed to allow better control over mechanical properties,swelling ratios and degradation rates than ionically crosslinkedalginates [50,103,106,107]. Their cell-signaling ability can also betailored by incorporating biochemical signals such as growth fac-tors and cell adhesive peptides [108,109].
Photocrosslinkable alginate can be delivered in a minimallyinvasive way and then rapidly crosslinked in physiological condi-tions in situ following a brief exposure to ultraviolet (UV) light[110]. This process occurs under mild conditions and thereforecan be performed in direct contact with cells. For that purpose,alginate was modified with 2-aminoethyl methacrylate using
carbodiimide chemistry and these methacrylated alginates weresubsequently photocrosslinked using UV light with a photoiniti-ator [103]. Photocrosslinkable alginate with controlled degradationand cell adhesive properties have attracted great interest with re-gard ton tissue engineering applications [103,109,111,112],although they are still relatively new and seem to require furtherstudies to assess their effectiveness.
3.1.2.2. Shape-memory alginate scaffolds. A novel type of covalentlycrosslinked alginate, capable of retaining its shape and forming amacroporous structure, has been developed. The concept involvesa hydrogel that allows control over its size and shape. Basically, ahydrogel is formed into the desired shape, then is collapsedin vitro for storage and handling purposes and, finally, is reformedin its original shape in vivo by rehydration [6,104]. It is noteworthythat, although these covalently cross-linked alginate hydrogelspresent great potential as injectable bulking agents, they exhibitless contourability than other alginate hydrogels. On the otherhand, they display greater shape definition, with a wider range ofphysical and mechanical properties.
To obtain these shape-memory scaffolds, alginate was cova-lently crosslinked with AAD and the hydrogels were formed bystandard carbodiimide chemistry using 1-ethyl-(dimethyl amino-propyl) carbodiimide, 1-hydroxybenzotriazole and AAD[104,113]. Thornton et al. [104]were able to produce macroporousalginate hydrogel scaffolds with a predefined geometry, whichwere then dehydrated and compressed into small, temporaryforms. The compressed scaffolds were then minimally invasivelydelivered to the dorsal subcutaneous space of a mouse through acatheter. Next, they were successfully rehydrated in situ by theinjection of PBS. Overall, this work demonstrated the potential ofthese covalently crosslinked hydrogels as an injectable deliverysystem.
More recently, Wang and colleagues [6] showed that theseshape-memory scaffolds have the potential to serve as a syntheticmatrix for skeletal muscle cell survival, proliferation and migra-tion. These results confirm the potential of these shape-memoryalginate scaffolds as cell delivery systems for tissue regeneration,although this strategy needs further exploration.
4. Alginate-based injectable cell delivery systems
4.1. Bone regeneration
In the fields of orthopedics and oral and maxillofacial surgery,bone regeneration remains a clinical challenge, despite the intro-duction of various bone augmentation techniques and bone graftmaterials. The current standard treatment is based on the use ofbone graft materials that are divided into two major groups: natu-ral and synthetic bone grafts [114]. Natural bone grafts includeauto-, allo- (human donors) and xenografts (other species). Autol-ogous bone graft is considered the ‘‘gold standard’’ for bone repairand regeneration by many surgeons, mainly due to lack of immu-nogenic reaction and optimal biological performance in terms ofosteogenicity, osteoinductivity and osteoconductivity [115]. How-ever, such bone grafts present several limitations, namely limitedavailability, the risks associated with harvesting, the additionalsurgical procedure required, donor site morbidity, post-operativepain and infection. On the other hand, allografts and xenograftsare widely available and there is no need for additional surgery.However, with both types of graft there is the risk of immunoreac-tion and, since they undergo several processing techniques, theirosteoinductive and osteoconductive potentials are reduced [115–117]. To overcome the above-mentioned limitations of naturalgrafting, a large number of synthetic grafts have been designed

1652 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
over the past decades. These materials present several advantages,such as wide availability, lack of antigenic response and easy tai-loring to a specific application. However, their biological perfor-mance regarding the induction and support of bone growth isinferior to those of natural grafts [115]. One way to overcome thisis to add cells and/or growth factors to the materials, to producemore biologically effective systems capable of restoring, maintain-ing or improving bone function [118].
In the subsequent paragraphs several promising alternativestrategies to the current therapies are described in which inject-able alginate-based cell delivery systems have been used withthe aim of promoting bone regeneration (Table 1).
The first studies to report the culture of bone cells in a 3-D algi-nate-based microenvironment were carried out using unmodifiedhydrogels and committed cell types, such as the mouse calvarial-3T3 osteoblastic cell line (MC3T3) or primary chick embryo osteo-blasts. In one of the first reports, Majmudar et al. [122]observedthat osteoblasts were kept viable for as long as 8 months withinalginate beads. Using an in situ gelling strategy, Kuo and Ma[72]were able to control the gelation rate of alginate hydrogels,and successfully entrapped MC3T3 pre-osteoblastic cells.
Due to the importance of cell–ECM interactions in cell adhesion,proliferation and differentiation, Alsberg et al. [119]explored forthe first time the use of RGD-modified alginate for the entrapmentof MC3T3-E1. They observed that RGD–alginate enhanced in vivobone formation after 16 and 24 weeks compared to unmodifiedalginate. Later, Evangelista et al. [20]demonstrated the importanceof these peptides not only in promoting cell adhesion but also inenhancing osteogenic differentiation.
MSCs or bone marrow stromal cells (BMSCs) are an importantcell population, being a mandatory first element for an unimpededbone repair process, so have shown great potential in bone tissueengineering [123]. Markusen et al. [124]demonstrated that hMSCsisolated from bone marrow could be entrapped within alginate-GRGDY (glycine-arginine-gycine-aspartic acid-tyrosine) beadswith viability higher than 80%. Duggal et al. [125] later investigatedthe phenotype and gene expression of hMSC from bone marrowand adipose tissue in a 3-D RGD–alginate system as compared toa 2-D culture. They observed that hMSCs within the beads acquireda compact morphology, maintained high cell viability and almostceased their proliferation. They also observed that hMSCs in 3-DRGD–alginate matrices presented more similarities with hMSCscultured in two dimensions than with uncultured freshly isolated
Table 1Examples of injectable alginate hydrogels proposed for cell delivery in bone tissue engine
Alginate supplier Alginate characteristics Alginateconcentration (w
Sigma–Aldrich n/a 1.2FMC BioPolymer Ultrapure n/aFMC BioPolymer;
SigmaUltrapure MVG; with RGD 2
FMC BioPolymer MVG Protonal LF20/40, HMW and LMW,oxidized with RGD
2
FMC BioPolymer MVG Protonal LF20/40, HMW and LMW,oxidized with RGD
2
FMC BioPolymer MVG with RGD 2
FMC BioPolymer MVG Protonal LF20/40,HMW and LMW,oxidized with RGD
2
FMC BioPolymer MVG irradiated with RGD 2FMC BioPolymer Pronova SLG 100 1.2Sigma–Aldrich n/a 2.5Sigma Aldrich Intermediate guluronic content 1.5
ATSC, adipose tissue stromal cells; BMSC, bone marrow stromal cells; EG, external gelatioHMW, high molecular weight; HOC, human osteoprogenitor cells; HUVEC, human umbiliavailable; PDLSC, periodontal ligament stem cells.
hMSCs by studying gene expression through a microarray analysis(an Affymetrix GeneChip Human Gnome U133A 2.0 Array plat-form, which contains 22,000 probes that represent 14,500 genesassociated with early development, intracellular signaling, cellshape and differentiation). This study demonstrated that 3-D cul-ture within RGD–alginate did not present the same gene expres-sion profile as their cells of origin. In the search for a bone tissueengineering application, Bidarra et al. [17]reported the successfulentrapment of bone marrow-derived hMSCs within 2 wt.% RGD-modified alginate microbeads cultured under dynamic conditionsfor 21 days, as shown in Fig. 4. Upon osteogenic stimulation, thehMSCs were able to differentiate along the osteoblastic lineageand also to stimulate neighboring endothelial cells to form tube-like structures on matrigel, thus demonstrating their pro-angio-genic ability. To assess this ability, hMSCs within RGD–alginatebeads were entrapped within matrigel and, after matrigel gelation,endothelial cells were added on top. After 48 h, tube-like struc-tures were counted and compared to those formed by endothelialcells seeded on matrigel alone.
The combination of stem cells with growth factors within a ma-trix may lead to increased bone formation. To explore this possibil-ity, Simmons et al. [120]investigated whether BMSCs entrappedwithin 2 wt.% irradiated alginate with RGD could enhance boneregeneration, in the absence or presence of bone morphogeneticprotein (BMP)-2 and/or transforming growth factor (TGF)-b3. Theauthors observed that only BMSCs transplanted in the presenceof both factors produced significant bone tissue. Therefore, theentrapment of progenitor cells and growth factors in a singledegradable matrix may provide a more potent strategy for bonetissue formation.
To amplify the MSCs potential, in some cases, these cells havebeen genetically modified with genes that codifiy for factors thathave a crucial role in bone regeneration, such as BMP-2. Rat bonemarrow-derived MSCs containing a BMP-2 transgene, when in-jected directly into articular osteotomies in nude rats, were capa-ble of accelerating bone healing compared to MSCs without theBMP-2 gene or MSCs with BMP-2 injected within alginate [121].In this example, the authors observed that the alginate carriers in-duced the formation of a chondroid mass that impeded bone heal-ing, therefore suggesting that alginate may not be a favorablevehicle for these genetically modified MSCs. It is noteworthy thata high molecular weight alginate without cell adhesion peptideswas used in this study, and no other formulations were tested,
ering applications (these data are not intended to be all-inclusive).
t.%)Hydrogel formation (beaddiameter, lm)
Cell type (cell density,�105 cells ml�1)
Refs.
EG with CaCl2 (352) Rabbit MSC (10) [74]EG with CaCl2 (2000) Human PDLSC and GMSC (10) [75]IG with CaSO4 Swine MSC (50) [98]
EG with CaCl2 (700) hMSC (200) [17]
EG with CaCl2 (200–500) HOC and HUVEC (200) [19]
EG with CaCl2 (1400)IG with CaSO4
MC3T3 (in vitro, 220)(in vivo, 315)
[119]
EG with CaCl2 (1000) MC3T3 (200) [20]
IG with CaSO4 BMSCs (200) [120]EG Rat MSC (0.5) [121]EG with CaCl2 Rabbit MSC (10) [77]EG with CaCl2 (300) Murine ATSC (10) [78]
n; GMSC, gingival mesenchymal stem cells; hMSC, human mesenchymal stem cells;cal vein endothelial cells; IG, internal gelation; LMW, low molecular weight; n/a, not

Fig. 4. Osteogenic differentiation of hMSCs inside alginate hydrogel microspheres: (A) hMSCs within 2 wt.% RGD–alginate microspheres with a cell density of2 � 107 cells ml�1 remain with a high viability after 21 days in culture, (B) as demostrated by the Live/Dead assay (viable cells stain green), (C) express high levels of ALP (acommon osteogenic marker; ALP + cells stain pink) activity when cultured under standard osteoinductive conditions [17].
Fig. 5. Effect of human osteoprogenitors and endothelial cells co-immobilizedwithin RGD–alginate microspheres on mineralization in a bone defect. Bone defectswere performed in the femoral metaphysis of nude mice, and RGD–alginatemicrospheres containing no cells, only human osteoprogenitors (HOPs) or HOPs co-immobilized with HUVECs were implanted. Quantification of mineralizationrevealed by von Kossa staining 3 and 6 weeks post-implantation. After implantationfor 6 weeks, mineralization of co-immobilized HOPs and HUVECs was significantlyhigher than with HOPs immobilized alone. ⁄p 6 0.05; ⁄⁄p 6 0.01 [19]. Copyright2009 Elsevier Ltd.
S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1653
which could presumably yield more favorable results. In anotherstudy, using miniature swine bone marrow-derived MSCs express-ing BMP-2, the authors compared three different types of alginates(regular alginate, ultrapure alginate and RGD-modified alginate)and also collagen type I as injectable cell delivery systems [126].The crosslinking of the alginate–cell suspension was achieved byinternal gelation with CaSO4. The authors reported a significantlybetter behavior of collagen type I, although detailed experimentalinformation is not available, such as the molecular weight of thealginate, the concentration of RGD or even the source of alginate.Moreover, the alginate was not modified to improve its biodegrad-ability, such as recurring to alginate oxidation, which alters chainconformation to an upon-chain adduct that is susceptible to hydro-lysis in physiological conditions.
Due to their flexibility, alginate beads with cells can also beformed in the presence of antibiotics, giving rise to a delivery sys-tem that is simultaneously capable of helping in the treatment ofinfected defects. For example, Ueng and colleagues [77] entrappedrabbit bone marrow-derived MSC with vancomycin within2.5 wt.% alginate for the treatment and prevention of surgical boneinfections. They were able to demonstrate the sustained release ofvancomycin over 14 days in vitro and the released concentrationexceeded the minimum inhibitory concentration against Staphylo-coccus aureus (determined by an antibiotic disk diffusion methodapplied to the nutrient broth). Moreover, when alginate beadsloaded with vancomycin and rabbit MSCs were implanted in bonecavities created in rabbit lateral femoral condyles, they were ableto contribute to the newly formed bone and a substantial mineraldeposition occurred. Nevertheless, as highlighted by the authors,further studies need to be performed in order to specifically inves-tigate the effect of the antibiotic in the combined system using aninfected bone model.
In more recent years interesting new cell sources have beenattracting attention in the tissue engineering field. For example,using adipose-derived cells from mice, Abbah et al. [78] observed,in vitro, more cell proliferation and alkaline phosphatase (ALP)activity within 1.5 wt.% alginate than in cells growing in a mono-layer. It is noteworthy that this is one of the few studies where sig-nificant cell proliferation in three dimensions was observed, withthe cell number almost doubling during the first week in culture.Other authors used adipose-derived cells and platelet-rich plasma(PRP) from rabbits within 1.2 wt.% alginate to produce beads. Theyobserved that these cells were capable of enhancing vasculariza-tion and mineralization in vivo [74].
To assess the possibility of using dental-derived stem cells forcraniofacial applications, since they might be more likely to differ-entiate into craniofacial tissues, Moshaverinia and colleagues [75]explored the potential of two such types of stem cells (human peri-odontal ligament stem cells and human gingival MSC) entrappedwithin 1 wt.% oxidized alginate beads. They demonstrated for thefirst time that these cells were able to differentiate, in vitro, into
osteogenic and adipogenic lineages, thus providing a promisingstrategy for bone tissue engineering.
Another strategy to enhance bone regeneration relies on the useof co-cultures of bone cells and endothelial cells. In this regard,Grellier et al. [19]entrapped primary human osteoprogenitor cellstogether with primary HUVECs within 2 wt.% RGD-modified algi-nate microbeads and showed that the co-transplantation of thesetwo cell types in femoral defects of mice promoted a significant in-crease in mineralization after 6 weeks of implantation, as depictedin Fig. 5.
4.2. Cartilage regeneration
Adult articular cartilage has a very limited reparative capacity,hence, in adults, cartilage defects do not regenerate. Efforts toachieve repair of these lesions have been limited by the challengeof stimulating the resident cells to form new cartilage. Among themany different clinical strategies to induce the formation of carti-laginous tissue, the implantation of autologous chondrocytes andstem cells have been explored in the pursuit of cartilage repair[127,128]. There are many examples of strategies involving theuse of alginate as a cell delivery vehicle for cartilage regeneration.Regarding the presence of adhesion peptides in the alginate matrix,it has already been demonstrated that these motifs support chon-drocyte and MSC adhesion, but in a 3-D environment MSC-inducedchondrogenesis may be inhibited when cells interacted with RGDpeptides [129]. This study points to the importance of designing

Table 2Examples of injectable alginate hydrogels proposed for cell delivery in cartilage tissue engineering applications (these data are not intended to be all-inclusive).
Alginate supplier Alginate characteristics Alginateconcentration (wt.%)
Hydrogel formation(bead diameter, lm)
Cell type (cell density,�105 cells ml�1)
Refs.
FMC BioPolymer LMW (150 kDa) 2 EG with CaCl2 ASCs (250) [79]FMC BioPolymer LMW (150 kDa) 2 EG with CaCl2 ASCs (250) [80]n/a n/a 1.2 EG with CaCl2 TGF-b3 CHOs (100) [130]Sigma–Aldrich Low viscosity 1.2 EG with CaCl2 CHOs and MSCs (5) [82]Sigma–Aldrich n/a 1.2 EG with CaCl2 Rabbit MSCs (10) [83]Sigma–Aldrich n/a 1.2 EG with CaCl2 IGF-I/FGF-2 rabbit CHOs (40) [84]Sigma–Aldrich n/a 1.2 EG with CaCl2 Synovium MSCs (70) [85]FMC BioPolymer LF 20/40 Protonal; low viscosity
M/G = 0.49; medium viscosity M/G = 1.61.5 and 2 EG with CaCl2 (800) Calf CHOs (330) [90]
FMC Biopolymer LF 20/40 Protonal; 19,600 g mol–1 2 Photocrosslinked Bovine CHOs (100) [109]Sea Matrix M/G ratio = 1–1.4; ultrapure 1 EG with CaCl2 Rabbit BMSCs (250) [86]n/a M/G ratio = 1.56; 75,000–100,000 g mol–1;
viscosity = 0.25 Pa s1.2 EG with CaCl2 (676) Human CSP (120) [131]
FMC BioPolymer LF 20/40 Protonal; 19,600 g mol–1 2 Photocrosslinked Bovine CHOs (100) [103]Fluka n/a 1 EG with CaCl2 (2000) Rat CHOs (5) [88]FMC BioPolymer n/a 2 EG with CaCl2 Human CHOs (200) [132]FMC BioPolymer n/a 0.8, 1.2 and 2 EG with CaCl2 (3000) Calf CHOs (25,000 and 100,000 cells per bead) [89]Sigma–Aldrich n/a 1.2 EG with CaCl2 FGF-2 rabbit CHOs (20) [133]Sigma–Aldrich n/a 1.2 EG with CaCl2 IGF-I rabbit CHOs (20) [134]Sigma–Aldrich n/a 1.2 EG with CaCl2 Rabbit CHOs (20) [135]
ASC, adipose stem cells; BMSC, bone stromal marrow cells; CHO, chondrocytes; CSP, mesenchymal progenitor cells from the subchondral bone marrow; EG, external gelation;FGF-1, fibroblast growth factor 1; G, guluronic acid; HMW, high molecular weight; IG, internal gelation; IGF-1, insulin-like growth factor 1; LMW, low molecular weight; M,mannuronic acid; MSC, mesenchymal stem cells; n/a, not available.
1654 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
appropriate scaffolds and biomaterials for cartilage engineeringapplications. In fact, the majority of the studies with MSCs forchondrogenesis do not use modified alginate, which is in agree-ment with the fact that they are not anchorage-dependent cells.
In the majority of the studies published, cells are delivered inalginate beads (Table 2). It is noteworthy that one major parameterthat differs between studies is the cell source used by the authors.Independently of the cell source, alginate has shown great poten-tial in cartilage regeneration. Therefore, the following examplesare discussed considering the cell origin.
Several studies report the use of fully differentiated chondro-cytes entrapped within an alginate matrix. For instance, primaryrat articular chondrocytes entrapped within 1 wt.% alginate wereable to proliferate and maintain their phenotype [88]. In fact, thesecells showed a significantly higher proliferation rate in 3-D than in2-D cultures, and showed continued growth for 40 days. For carti-lage regeneration, alginate hydrogels seem to provide an adequateenvironment since chondrocytes are not anchorage-dependentcells and their natural microenvironment consists in a hydratedmatrix.
Dobratz and colleagues [132] prepared an injectable in situcrosslinking system to produce an engineered cartilage by injectinga CaCl2 solution immediately after mixing a 2 wt.% alginate solu-tion with primary perichondrium-derived human chondrocytes.This minimally invasive system allowed for an in vivo molding thatmaintained its shape for at least 38 weeks after injection.
Jeon and co-authors [103,109]developed a photocrosslinkable,biodegradable alginate system with controlled cell adhesive prop-erties in which bovine articular chondrocytes were successfully en-trapped. In this study, chondrocytes within RGD–alginateexhibited a higher proliferation rate and greater chondrogenic dif-ferentiation compared to the cells entrapped within unmodifiedhydrogels. It is noteworthy that these hydrogels contained TGF-b1. This new photocrosslinkable biomaterial constitutes a promis-ing approach to cartilage tissue engineering.
In an attempt to overcome some of the limitations of chondro-cyte transplantation, cells are being genetically modified toenhance repair. For instance, porcine TGF-b3-secreting chondro-cytes combined with porcine synovial-derived MSCs within algi-nate beads were able not only to induce MSCs differentiation, butalso to prevent chondrocyte dedifferentiation [130]. In addition,
the combination of both types of cell presented the highest levelof chondrogenesis in vivo. In other examples, rabbit chondrocyteswere modified to overexpress two growth factors simultaneouslyor separately, namely insulin-like growth factor (IGF)-I and fibro-blast growth factor (FGF)-2 [84,133–135]. In these works, the1.2 wt.% alginate beads entrapping these genetically modified cellspromoted important cartilage repair in vivo. IGF-I is an anabolicgrowth factor of chondrocytes that has been shown to stimulatethe production of proteins from the cartilage ECM (e.g. collagentype II and proteoglycans), whereas FGF-2 is mitogenic for articularchondrocytes [136]. Normal chondrocytes produce IGF-I and, in the3-D alginate environment, these cells continue to produce this fac-tor [89]. Moreover, Yoon et al. [89]demonstrated that the associa-tion of higher cell densities and higher matrix concentrations leadsto an enhancement in IGF-I production, since IGF-I expression bycalf chondrocytes was increased with smaller cell-to-cell distances(higher cells densities).
MSCs have been explored as an alternative cell source in carti-lage regeneration strategies. The chondrogenic potential of hMSCsisolated from subchondral bone marrow was assessed after entrap-ment within 1.2 wt.% alginate beads and under chondrogenic stim-ulation [87]. Although further in vivo studies are necessary, theauthors demonstrated the relevance of the calcium–alginate sys-tem for stem cell injection by obtaining full chondrogenic differen-tiation within the alginate matrix. The chondrogenic potential ofbone marrow stem cells isolated from rabbits was also assessedby entrapping these cells and comparing their behavior in ultra-pure (UP) and commercial grade sodium alginate [86]. The authorsobserved a significant enhancement of cell proliferation and differ-entiation in the UP compared to the commercial grade alginate.When UP beads with cells were implanted, a significant improve-ment in cartilage repair was observed compared to commercialgrade alginate, which points to the importance of purification algi-nate in such applications. Dashtdar et al. [83]demonstrated that,independently of their state of differentiation, transplanted rabbitbone marrow-derived MSCs entrapped within 1.2 wt.% alginatebeads promoted greater healing compared to untreated controlsin articular cartilage defects in rabbit. In a comparative analysis,the effectiveness of rabbit allogeneic MSCs was evaluated againstthat of autologous chondrocytes in repairing focal cartilage defectsin an in vivo rabbit model [82]. When transplanted within 1.2 wt.%

S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1655
alginate beads, the two cell types promoted similar chondrogenicdifferentiation and produced selective up-regulation of cartilage-specific genes. These results support the potential use of MSCsfor articular cartilage repair. In other studies, MSCs were modifiedwith the purpose of producing TGF-b3 – a commonly used growthfactor to induce MSCs chondrogenesis – and simultaneously sup-pressing collagen type I expression [85,136,137]. Although furtherstudies are needed to optimize the efficiency of this strategy,encouraging in vitro results were obtained when these cells wereentrapped within 1.2 wt.% alginate.
Overall, the treatment of articular cartilage defects with stemcells of mesenchymal origin has achieved satisfactory outcomesand MSCs seem to present several advantages compared to chon-drocytes, which have limited proliferation capacity and, in somecases, even seem to lose their cartilaginous phenotype duringexpansion [82]. However, although adult stem cells reveal suchgreat potential, the majority of the studies in cartilage regenerationhave used differentiated chondrocytes as the cell source[81,90,138,139] and, despite their limitations, most of the clinicaltrials that use these cells have good repair outcomes (i.e. the cellswere able to form new cartilage).
Adipose-derived stem cells (ASCs) have emerged as anotherpromising adult cell source for cartilage regeneration because oftheir easy accessibility and chondrogenic potential [140]. Addition-ally, ASCs have demonstrated the ability to secrete a wide range oftrophic factors that can stimulate endogenous cartilage regenera-tion. Lee and co-authors [79,80] optimized the cell culture condi-tions for entrapped rat ASCs within alginate microbeads and,after implantation in a focal cartilage repair site, tissue infiltrationand perichondrium were observed.
4.3. Intervertebral disk regeneration
Intervertebral disk (IVD) degeneration is a major health concernworldwide. Replacement of the nucleus pulposus (NP) of the IVD, anatural hydrated structure, with injectable biomaterials representsa potential treatment strategy for IVD degeneration. Naturally de-rived materials such as alginate have been used as models to studythe behavior of NP cells in a 3-D environment [141–146]. In severalstudies, NP cells were cultured in 3-D alginate beads to assess theirbehavior under the influence of different conditions [147–150]. Forinstance, when bovine NP cells within 1.2 wt.% beads were cul-tured in the presence of bovine lactoferricin there was a decreasein inflammatory mediators involved in degenerative disk disease(cytokine interleukin-1 and endotoxin lipolysaccharide) that medi-ate the suppression of prostaglandin (PG) accumulation [147]. As aconsequence, there was an up-regulation of PG synthesis, aggrecanexpression and pericellular matrix formation. In another example,alginate beads with NP cells were used as a model to evaluate thetoxicity of some compounds commonly used in spinal surgery[148,149]. In a different study, the influence of different mediumcompositions, one with human PRP and another with TGF-b1, onchondrogenic differentiation of hMSCs comparison with NP cellswas investigated [150]. In comparison with TGF-b1, PRP did not in-duce adequate chondrogenic differentiation. These types of studiesare key for better understanding how cell biology influences diskdegeneration and how this process could be manipulated. For in-stance, Stephan et al. [142]evaluated a range of cell densities en-trapped in alginate under different culture conditions (standardculture conditions with 3.15 g l�1 glucose and 10% serum or with-out glucose and/or 20% serum), and demonstrated that NP cellgrowth and survival were both influenced by cell density and theavailability of serum or nutrients such as glucose. For instance,additional serum (20%) promoted cell proliferation and the forma-tion of large cell clusters, and even larger cell clusters were createdwithout glucose. Additionally, lower cell densities led to higher cell
proliferation and cluster formation. Bron and colleagues [143] ana-lyzed the effect of different alginate concentrations (2, 4 and6 wt.%) and preparation conditions (external and internal gelation)on the gene expression of components of the IVD’s ECM. Theyfound that 2 wt.% alginate disks prepared by external gelation clo-sely matched the viscoelastic properties of the nucleus pulposus. Itis noteworthy that alginate was not modified to promote cell adhe-sion, hence cells were not able to actively respond to matrix stiff-ness via focal adhesion sites. Therefore, no pronounced effect ofmatrix stiffness was observed on ECM synthesis.
Using an alternative crosslinking approach, Chou et al.[111]studied the potential of photocrosslinked alginate for NP cellencapsulation and in vivo repair, and further compared it with ion-ically crosslinked alginate. Photocrosslinked alginate maintainedstructural integrity, as illustrated in Fig. 6, and presented a highernumber of NP cells producing ECM components (type II collagenand chondroitin sulfate proteoglycan) compared to ionically cross-linked alginate in vitro. Additionally, increases in gene expression(type II collagen and aggrecan) and ECM accumulation (type II col-lagen and sulfated glycosaminoglycan) were obtained by photo-crosslinked alginate after 8 weeks in vivo. At this time thematrices presented an equilibrium Young’s modulus of around4.31 kPa, which is close to the native NP equilibrium modulus re-ported in other studies [183,184] that employed a similar uncon-fined compression testing protocol (5–6.7 kPa).
Generally, these studies underscore the potential of alginate asa synthetic ECM for IVD engineering.
4.4. Adipose tissue regeneration
Contour defects due to loss of soft tissue, largely composed ofsubcutaneous adipose tissue, are associated with tumor resection,trauma and congenital abnormalities. Current treatment for softtissue reconstruction use autologous fat transplantation, alloplasticimplants and autologous tissue flaps, which present a number ofchallenges and limitations, such as donor site morbidity and vol-ume loss over time, implant migration and foreign body reaction[49,151]. Several studies have tried to overcome these limitationsthrough the use of human adipose stem cells (hADSCs) in an at-tempt to engineer adipose tissue in vivo. hADSCs have severalattractive features, including a high expansion potential in culture,the ability to be readily induced to differentiate into adipocytesin vitro, easy isolation and isolation in large quantities. The feasi-bility of using an injectable hydrogel such as alginate as a deliveryvehicle for these cells for contour improvement has been demon-strated in a few studies (Table 3).
Kang and co-authors [99] showed that an RGD-modified algi-nate matrix enhanced adipogenic differentiation, demonstratingthat the RGD peptides function not only as cell adhesion sites,but also as adipogenic stimulator for ADSCs. In another study,the behavior of hADSC was analyzed within alginate matrices pre-pared using two different crosslinking agents: calcium chlorideand calcium gluconate [151]. Both matrices maintained cell viabil-ity (higher than 80%) and supported adipogenic differentiation (po-sitive staining for neutral lipid accumulation and increased levelsof perilipin expression). It is noteworthy that an enhancement ofbiological performance was detected in the case of alginate cross-linked with calcium gluconate, which could be explained by thelarger pore sizes, as qualitatively observed by scanning electronmicroscopy. In contrast to calcium chloride, calcium gluconate pro-vides the slow release of small amounts of Ca2+, and this leads tothe formation of a more homogeneous matrix with larger pores.This type of matrix probably promotes a more efficient diffusionof oxygen and nutrients within the alginate matrix while allowinga higher cell–cell contact, and thus might present advantages forapplication in adipose tissue engineering. In another example,

Fig. 6. Methacrylate alginate hydrogels after 4 weeks in vivo: (A) ionically and (B) photocrosslinked hydrogels. After 4 weeks in vivo, all hydrogels were encapsulated in a thinfibrous capsule consistent with a mild foreign body response. However, ionically crosslinked alginate hydrogels underwent dissolution while photocrosslinked hydrogelsremained intact, with no apparent changes in structural integrity and shape. Arrows indicate location of the hydrogel [111]. Copyright 2009 Elsevier Ltd.
Table 3Examples of injectable alginate hydrogels proposed for cell delivery in adipose tissue engineering applications (these data are not intended to be all-inclusive).
Alginatesupplier
Alginate characteristics Alginateconcentration(wt.%)
Hydrogel formation(bead diameter, lm)
Cell type (celldensity,�105 cells ml�1)
Ref.
FMCBioPolymer
Ultrapure MVG; 40% M/60% G;Irradiated,oxidized and RGD modified; 3LMW:1HMW
2 IG with CaSO4 hADSC (20) [49]
n/a LMW 1 EG with CaCl2 and calciumgluconate (thin layer)
hADSCs (n/a) [151]
FMCBioPolymer
200,000–300,000 g mol–1 RGDmodified
2 IG with CaSO4 (disks, 8 mm diameter and 1 mmthickness)
hADSCs (5) [99]
FMCBioPolymer
LF 10/60 Protonal RGD modified 3 Photocrosslinked APC (3T3-L1 cells) [112]
n/a Low viscosity 1.2 EG with CaCl2 Mice ADSCs (20) [152]
ADSCs, adipose-derived stem cells; APC, adipose progenitor cells; EG, external gelation; G, guluronic acid; HMW, high molecular weight; IG, internal gelation; LMW, lowmolecular weight; M, mannuronic acid; n/a, not available.
1656 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
photocrosslinked methacrylated RGD–alginates with differentmechanical properties were investigated as 3-D hydrogel matricesfor a mouse pre-adipocytic cell line (3T3-L1) [112]. Hydrogels withdifferent stiffness were obtained, with representative elastic mod-uli of different physiological conditions: 3.3 (physiological), 7.9(intermediate) and 12.4 kPa (pathological). The authors observedthat increased matrix rigidity enhanced cell proliferation andangiogenic capacity, while adipose differentiation was inhibited.Collectively, the obtained results highlight the role of matrix stiff-ness in the design of biomaterial scaffolds for adipose tissueengineering.
Jing and co-workers [152] isolated ADSCs from mice that weredifferentiated into the adipogenic lineage in vitro and then en-trapped within 1.2 wt.% alginate crosslinked with calcium chloride.The cells–alginate system was then implanted subcutaneously andnew adipose tissue was formed after 8 weeks, demonstrating thepotential of combining predifferentiated cells and alginate for adi-pose tissue engineering. Kim et al. [49]further demonstrated thepotential of cryopreserved hADSCs entrapped within 2 wt.%RGD–alginate hydrogel to produce living adipose tissue in vivovia a minimally invasive way, since crosslinking occurred in situdue to the presence of CaSO4.
4.5. Cardiac regeneration
Cardiovascular disease is one of the most common causes ofdeath in the world [153]. In the majority of cases heart failure,
and consequently death, are due to myocardial infarction (MI)associated with the left ventricle (LV) [154]. In this clinical area,cardiac tissue engineering offers promising post-MI treatments,based on the use of injectable alginate hydrogels [155,156].
In 2008, Landa et al. [157]demonstrated for the first time that insitu forming 1 wt.% alginate hydrogel improves left ventricularremodeling and function in a rat model of recent and old infarcts.This group later tested the same system in a large animal model ofMI (swine) [158]. They were able to show that an intracoronaryinjection of a calcium crosslinked alginate solution was feasiblein a larger infarcted area, and that alginate diffuses from the leakycoronary microvasculature and deposits in the infarcted myocar-dium. In an attempt to improve alginate function, alginate wasfurther modified with adhesion peptides (RGD and YIGSR (tyro-sine-isoleucine-glycine-serine-arginine)) [159]. However, when in-jected, a reduction in the beneficial effect of the alginate in theinfarcted area was observed. A possible explanation for this maylie in the possible physical changes that occurred due to alginatemodification (e.g. increased viscosity leading to reduced biomate-rial spreading).
Using a different in situ approach, Yu et al. [160]were able todeliver 1.5 wt.% alginate, grafted or not with RGD and calciumchloride using a Duploject (Baxter) applicator, which provided asimultaneous mixing and delivery of both components into the in-farcted area of the LV, in a chronic rodent model of ischemic car-diomyopathy. The authors observed that both alginates (modifiedand unmodified) could reshape the aneurysmal LV (as illustrated

Fig. 7. Effect of injected alginate in a chronic rat infarct model. Trichrome staining at 5 weeks post-injection. (A) PBS-injected and (B) alginate-injected heart. The trichromestaining demonstrated that the aneurysmal LV geometry of alginate-treated animals resembled normal control hearts, in contrast to the thin-walled, dilated LV of the PBS-treated animals. The black arrow in (B) indicates residual alginate in situ. Scale bar = 1 mm [160]. Copyright 2008 Elsevier Ltd.
S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1657
in Fig. 7) and improve LV function, and that RGD–alginate couldparticularly enhance angiogenesis. This group later adopted a dif-ferent strategy by developing a cell delivery system where hMSCswere entrapped and then injected within RGD–alginate micro-beads smaller than 100 lm [51,161]. The RGD–alginate micro-spheres induced angiogenesis and delayed the negativeremodeling of the LV by preventing the infarct wall thinning andchamber dilation after an infarct. Moreover, RGD–alginate micro-beads were able to enhance the retention and survival of trans-planted stem cells. Interestingly, the authors were unable toobserve in vivo any differences between RGD–alginate alone andwith cells. It is noteworthy that they observed hMSCs withinRGD–alginate microspheres in the MI after 1 week, demonstratingthe effectiveness of these microspheres for the delivery of cells tothe myocardium.
In this context it is worth mentioning that, following theencouraging results in animal models, an alginate hydrogel has be-come the first injectable acellular biomaterial to enter clinical trialsfor treating MI. In fact, the ongoing clinical trial using this bioma-terial, with the market name of IK-5001, is currently recruiting pa-tients to a phase II clinical trial [51].
4.6. Regeneration of other tissues and organs
Alginate hydrogels are also being investigated for their ability toenhance regeneration in other tissues and organs. However, theirapplication as injectable cell delivery vehicles is still poorlyexplored.
In the central nervous system, the benefits of other hydrogels(matrigel, collagen, fibrin, agarose) to deliver cells has already beendemonstrated in comparison with preformed scaffolds and cellsalone [2,162]. However, only few studies using alginate have beenreported to date. For example, alginate microbeads have been ex-plored as an entrapment system to facilitate the neuronal differen-tiation of embryonic stem cells (ESCs), which could be furtherscaled up for the production of large numbers of differentiatingcells [163]. For that purpose, a range of alginate concentrations(1.2, 1.7, 2.2 and 2.5 wt.%), with a final cell concentration of5 � 106 cells ml�1, were evaluated. With the right stimuli, theauthors found that 2.2 wt.% alginate was the most conducive toESC differentiation into astrocytes and neuronal lineage cells. Inanother example, Schwann cells over-expressing brain-derivedneurotrophic factor (BDNF) entrapped in alginate beads were ableto increase auditory neuron survival when transplanted into thecochlea of a deaf guinea pig [164]. This cell-based neurotrophintreatment could be considered a valuable option for the deliveryof neurotrophic factors to reduce or prevent auditory neurondegeneration in sensorineural hearing loss. In a similar approach,
fibroblasts engineered to produce BDNF survived, grew and ex-pressed bioactive BDNF while entrapped within alginate microcap-sules, and were shown to be capable of successfully guiding theneurite growth of dorsal root ganglia [165]. In a different strategy,highly anisotropic alginate-based capillary hydrogels, introducedin a spinal cord lesion, were able to induce directed nerve regrowthwithout a major inflammatory response [57].
As previously mentioned, one of the first applications of algi-nate hydrogels in tissue engineering involved immunoisolation –more specifically, the transplantation of encapsulated pancreaticislets in an effort to cure type I diabetes. The purpose of these sys-tems was to isolate the cells from the surrounding environmentwhile producing insulin in diabetic patients. Despite its great clin-ical interest, these systems have not been deemed suitable for clin-ical applications yet due to several problems, mainly related withimmunogenicity [166]. Since the 1970s several efforts to improvethis type of system have been made, namely in what concernsthe alginate composition and purity, the use of different coatingmaterials and cell sources, as well as the site of implantation[166–168].
Recently, 3-D alginate matrices have demonstrated great poten-tial in the development of a bioartificial liver [169]. Cells from a hu-man-derived liver cell line (HepG2) were entrapped in 2 wt.%alginate and cultured in a fluidized bed bioreactor. Cells were re-ported to remain viable at high cell densities and proliferate toform compact cell spheroids with extensive cell-to-cell contactsand adequate cell function (lactate production, glucose and oxygenconsumption, gene and protein expression). The authors hypothe-sized that HepG2 cultured in an optimized form could be used totemporarily improve the function of deficient liver to allow enoughtime for its repair or for transplantation. In another study, alginatematrices were used to evaluate the effect of matrix stiffness on thebehavior of a human hepatocyte cell line, C3A [170]. As demon-strated, hepatocytes stopped growing and de differentiated in stiffhydrogels (3 wt.% alginate), whereas in soft hydrogels (0.7 wt.%alginate) cells maintained their differentiated phenotype, express-ing higher xenobiotic metabolism and increased albumin secre-tion. Overall, the understanding of the 3-D mechanical effects ofthe microenvironment on C3A cells may provide a platform forthe future design of liver tissue engineering. Other cells from a hu-man hepatoma cell line (Huh-7) were successfully immobilizedwithin alginate beads for 7 days, and throughout this period cellsproliferated and organized into aggregates [91]. Hepatocytesestablished a 3-D architecture with cell polarity, cell junctionsand bile canaliculi. The functionality of these cells was assessedby the production of albumin and the exhibition of CYP1A (oneof the major drug metabolizing enzymes). Moreover, the authorsobserved the expression of specific receptors of hepatitis C virus,

1658 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
which suggests that this system could be further used for thedevelopment of a physiologically relevant model for in vitro viralstudies.
RGD–alginate scaffolds have also been explored in the field ofskeletal muscle tissue engineering as vehicles for myoblasts[171,172]. Although not injectable, these multifunctional scaffoldswere able to release cells and growth factors simultaneously, andconsequently accelerate the muscle regeneration process. In an-other example, a covalently crosslinked shape-memory alginatescaffold combined with IGF-1 and skeletal muscle cells alsoshowed great potential for cell and growth factor delivery by aminimally invasive technique for the regeneration of skeletal mus-cle [6]. Scaffolds were able to release IGF-1 over several daysin vitro and allowed skeletal muscle cells to survive, proliferateand migrate outwards over 28 days.
Alginate hydrogels combined with cells have also been investi-gated for skin regeneration strategies. Since skin is composed oftwo different layers, one rich in keratinocytes (epidermis) andthe other rich in fibroblasts (dermis), a bilayered structure shouldoffer a more effective treatment. Considering this, Hunt and col-leagues [95]immobilized fibroblasts within alginate beads andthen keratinocytes were cultured on the surface, forming a bilay-ered composition. On the one hand, the viable fibroblasts withinthe matrix did not proliferate but were able to secrete ECM, whichwould be able to replace the alginate matrix after degradation. Onthe other hand, keratinocytes were able to grow uninhibited byfibroblast overgrowth to form a stratified epidermal layer.Although in vivo studies need to be addressed, this study revealsthe potential of alginate for skin regeneration.
In a more general approach, due to their immunomodulatorycapacity, MSCs entrapped in alginate were able to preserve theiranti-inflammatory function and provide a controlled delivery vehi-cle to attenuate inflammation and, consequently, promote tissuerepair in vivo [173–176].
4.7. Vascularization
In attempting to achieve long-term clinical success of engi-neered tissues, it is now widely recognized that vascularizationshould be promoted [177]. In point of fact, to mimic the function-ality and complexity of natural tissues, such as the heart, liver, kid-ney, muscle, nerve and bone, therapeutic stimulation of vesselgrowth is important during the regeneration process. However,this is still ignored in many tissue engineering approaches. Theuse of alginate-based strategies for therapeutic vascularization
Fig. 8. Endothelial cells within alginate hydrogels. HUVECs were immobilized with 1 wpetides and (B) with RGD peptides 48 h post-immobilization. Cells were stained with Alexvisualized under a Leica SP2 AOBS SE laser scanning confocal microscope (Leica Microsy
has been recently reviewed by Gandhi and colleagues [178], andsome of the previously mentioned studies with injectable alginatematrices have taken this into account with good outcomes [17,74].
One of the approaches proposed focused on stimulating vascu-larization via cell-released soluble factors. For example, the localdelivery of MSCs in alginate microspheres per se enhanced the vas-cularization of tissue engineered constructs, since these cells se-creted different angiogenic factors that were able to diffuse outof the matrix into the surrounding environment [179]. hMSCsdelivered using this technology were shown to augment the resto-ration of vascular supply in ischemic tissue, highlighting the poten-tial of alginate-entrapped hMSCs as a strategy to enhanceparacrine-mediated vascular recovery after hindlimb ischemia[179]. In another study, a subpopulation of mouse bone marrow-derived cells encapsulated in 1.5 wt.% alginate was able to influ-ence venular remodeling in a mouse dorsal window chamber skin-fold model (a circle of tissue that is dissected and covered with around coverslip) [93]. Moreover, the in vivo delivery of rabbit bonemarrow-derived MSCs entrapped in 2 wt.% alginate was demon-strated to improve hindlimb perfusion in an endovascular modelof peripheral arterial disease [92].
An alternative strategy has been the use of alginate matrices asvehicles for endothelial-like cells that can themselves be incorpo-rated into new blood vessels. In fact, the use of cell-based therapiesinvolving the use of mature endothelial cells or progenitor endo-thelial cells has proven to be instrumental in the treatment of car-diac infarction, for example, as well as in other situations wherevascularization is deficient [153,180,181]. Although these cellsources have not yet been fully explored in alginate-based systems,a few studies have been performed with encouraging outcomes.For example, an in situ formed 1 wt.% RGD–alginate hydrogel ma-trix with a bimodal distribution of high and low molecular weightand low stiffness was shown to recreate an adequate 3-D microen-vironment for vascular cells, survival, migration and proliferationin vitro. As depicted in Fig. 8, cells within RGD–alginate were ableto spread and form a cellular network, in contrast to cells withinunmodified alginate [18]. Moreover, this specific matrix promotedthe organization of cells in 3-D networks, which constitutes a stepforward in the development of an injectable strategy to enhancevascularization. In a more complex approach, the co-entrapmentof different cell types might be even more effective. In a recentin vitro study, the co-entrapment of endothelial cells with othercell types, namely ADSCs, in a photocrosslinked RGD–alginate wereshown to be capable of accelerating vascularization. This effect wasexplained by the increasing proliferation and tube-like structure
t.% alginate with a cell density of 2 � 107 cells ml�1 of alginate: (A) without RGDa-fluor 488-phalloidin (F-actin) and counterstained with Hoechst 33342 (blue), andstems). The images represent an overlay of different plans [18].

S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1659
formation of endothelial cells in response to the elevated concen-tration of pro-angiogenic factors (e.g. vascular endothelial growthfactor) secreted by the co-cultured cells [112].
In in vivo studies, Silva et al. [4,182]used RGD–alginate scaffoldsto create a depot of human vascular progenitor cells for the treat-ment of ischemic murine hindlimb musculature. The authors ob-served a reverse hindlimb ischemia and an increase in thenumber of vessels compared to direct cell injection. These resultsdemonstrate the importance of the delivery approach to the sus-tained release and repopulation of the surrounding tissue,although the system was not injectable.
5. Conclusions and perspectives
Despite the recent advances and promising results of cell-basedtherapies, substantial challenges remain in controlling the fate oftransplanted cells. The success of these strategies might be signif-icantly improved with the use of adequate cell carriers. Alginate-based matrices stand out as ideal materials for such applications.Alginate can form tunable and versatile hydrogels that are partic-ularly attractive due to their easy and mild gelation, attained viaa variety of crosslinking approaches. These highly hydrated andpermeable matrices offer unique advantages for the developmentof 3-D cellular microenvironments. To increase their ECM-like fea-tures, alginates that are intrinsically ‘‘bioinert’’ can be modifiedwith a variety of biological cues to promote cell–matrix interac-tions. Another distinguishing characteristic of these materials istheir potential injectability, essential to deliver cells directly intothe site of injury through a minimally invasive approach. Aspointed out, injectable alginate systems are already having aremarkable impact in many biomedical applications. The examplesdescribed in this review illustrate their potential for therapeuticcell delivery, in different areas of the tissue-engineering field. Insome of the studies, the success of this strategy has been clearlydemonstrated. In this context, alginate hydrogels play two impor-tant roles: they not only provide a protective vehicle for transport-ing cells into the body, but also provide a temporary ECM-likesupportive matrix that guides 3-D cell organization and might evenmodulate cell fate, promoting cellular integration and conse-quently tissue repair and regeneration.
Despite these promising insights, it is also clear that alginate-based materials still have to evolve considerably to become theideal matrix for tissue regeneration. The alginate hydrogels pres-ently used clinically for wound healing, heat burns, acid refluxand weight control applications play quite a passive role. Although,in tissue regeneration, important steps are being made in the fieldof cardiac regeneration, in the other areas described there is still aconsiderable gap between research and the clinical application.One of the aspects that could contribute to decreasing this gapwould be better characterization of the alginate sources for bettercomparison between studies. There were several relevant worksavailable where the alginate used has not been characterized interms of molecular weight, amount of G and M units, endotoxinscontent, peptide concentration or even alginate concentration.
In line with the development of the field itself, a burgeoningnumber of cutting-edge discoveries are leading to the design of im-proved alginate hydrogels, with several interesting properties interms of injectability, in situ crosslinking strategies, mechanicalproperties, biodegradability and biomimetic behavior. At the sametime, there has been an important investment in the exploration ofnew cell sources and complex cell–cell and/or cell–drug combina-tions. All of these efforts and their achievements will certainly con-tribute to improving the current status of cellular therapies in thenear future.
Acknowledgements
This work was financed by FEDER funds through the ProgramaOperacional Factores de Competitividade – COMPETE, and by Por-tuguese funds through FCT – Fundação para a Ciência e a Tecnolo-gia, in the framework of the projects Pest-C/SAU/LA0002/2011 andBIOMATRIX (PTDC/SAU-BEB/101235/2008 and FCOMP-01-0124-FEDER-010915). S.B. is the recipient of a post-doctoral fellowshipfrom FCT-POPH (SFRH/BPD/80571/2011). C.B. has a research posi-tion funded by FCT-POPH-FSE (Ciência 2008).
Appendix A. Figures with essential colour discrimination
Certain figures in this article, particularly Figs. 1–4, 6–8, are dif-ficult to interpret in black and white. The full colour images can befound in the on-line version, at http://dx.doi.org/10.1016/j.actbio.2013.12.006
References
[1] Wang C, Varshney RR, Wang D-A. Therapeutic cell delivery and fate control inhydrogels and hydrogel hybrids. Adv Drug Deliv Rev 2010;62:699–710.
[2] Pakulska MM, Ballios BG, Shoichet MS. Injectable hydrogels for centralnervous system therapy. Biomed Mater 2012;7:024101.
[3] Place ES, Evans ND, Stevens MM. Complexity in biomaterials for tissueengineering. Nat Mater 2009;8:457–70.
[4] Silva EA, Kim E-S, Kong HJ, Mooney DJ. Material-based deployment enhancesefficacy of endothelial progenitor cells. Proc Natl Acad Sci U S A2008;105:14347–52.
[5] Bayoussef Z, Dixon JE, Stolnik S, Shakesheff KM. Aggregation promotes cellviability, proliferation, and differentiation in an in vitro model of injection celltherapy. J Tissue Eng Regen Med 2012;6:e61–73.
[6] Wang L, Shansky J, Borselli C, Mooney D, Vandenburgh H. Design andfabrication of a biodegradable, covalently crosslinked shape-memory alginatescaffold for cell and growth factor delivery. Tissue Eng A 2012;18:2000–7.
[7] Ventre M, Causa F, Netti PA. Determinants of cell–material crosstalk at theinterface: towards engineering of cell instructive materials. J R Soc Interface2012;9:2017–32.
[8] Chung S, King MW. Design concepts and strategies for tissue engineeringscaffolds. Biotechnol Appl Biochem 2011;58:423–38.
[9] Hunt NC, Grover L. Cell encapsulation using biopolymer gels for regenerativemedicine. Biotechnol Lett 2010;32:733–42.
[10] Baker BM, Chen CS. Deconstructing the third dimension: how 3D culturemicroenvironments alter cellular cues. J Cell Sci 2012;125:3015–24.
[11] Giri T, Thakur D, Alexander A, Ajazuddin, Badwaik H, Tripathi D. Alginatebased hydrogel as a potential biopolymeric carrier for drug delivery and celldelivery systems: present status and applications. Curr Drug Deliv2012;9:539–55.
[12] Salgado CL, Sanchez EMS, Zavaglia CAC, Almeida AB, Granja PL. Injectablebiodegradable polycaprolactone-sebacic acid gels for bone tissueengineering. Tissue Eng A 2012;18:137–46.
[13] Salgado CL, Sanchez EMS, Zavaglia CAC, Granja PL. Biocompatibility andbiodegradation of polycaprolactone-sebacic acid blended gels. J BiomedMater Res A 2012;100A:243–51.
[14] Fonseca K, Bidarra SJ, Oliveira MJ, Granja PL, Barrias CC. Molecularly-designedalginate hydrogels susceptible to local proteolysis as 3D cellularmicroenvironments. Acta Biomater 2011;7:1674–82.
[15] Fonseca KB, Maia FR, Cuz FA, Andrade D, Juliano MA, Granja PL, et al.Enzymatic, physiocochemical and biological properties of MMP-sensitivealginate hydrogels. Soft Matter 2013;9:3283–92.
[16] Munarin F, Guerreiro SG, Grellier MA, Tanzi MC, Barbosa MA, Petrini P, et al.Pectin-based injectable biomaterials for bone tissue engineering.Biomacromolecules 2011;12:568–77.
[17] Bidarra SJ, Barrias CC, Barbosa MA, Soares R, Granja PL. Immobilization ofhuman mesenchymal stem cells within RGD-grafted alginate microspheresand assessment of their angiogenic potential. Biomacromolecules2010;11:1956–64.
[18] Bidarra SJ, Barrias CC, Fonseca KB, Barbosa MA, Soares RA, Granja PL.Injectable in situ crosslinkable RGD-modified alginate matrix for endothelialcells delivery. Biomaterials 2011;32:7897–904.
[19] Grellier M, Granja PL, Fricain J-C, Bidarra SJ, Renard M, Bareille R, et al. Theeffect of the co-immobilization of human osteoprogenitors and endothelialcells within alginate microspheres on mineralization in a bone defect.Biomaterials 2009;30:3271–8.
[20] Evangelista MB, Hsiong SX, Fernandes R, Sampaio P, Kong H-J, Barrias CC,et al. Upregulation of bone cell differentiation through immobilization withina synthetic extracellular matrix. Biomaterials 2007;28:3644–55.
[21] Barrias CC, Lamghari M, Granja PL, Sá Miranda MC, Barbosa MA. Biologicalevaluation of calcium alginate microspheres as a vehicle for the localizeddelivery of a therapeutic enzyme. J Biomed Mater Res A 2005;74A:545–52.

1660 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
[22] Ribeiro CC, Barrias CC, Barbosa MA. Calcium phosphate–alginatemicrospheres as enzyme delivery matrices. Biomaterials 2004;25:4363–73.
[23] Aguado BA, Mulyasasmita W, Su J, Lampe KJ, Heilshorn SC. Improvingviability of stem cells during syringe needle flow through the design ofhydrogel cell carriers. Tissue Eng A 2012;18:806–15.
[24] Kong HJ, Smith MK, Mooney DJ. Designing alginate hydrogels to maintainviability of immobilized cells. Biomaterials 2003;24:4023–9.
[25] Pilkington PH, Margaritis A, Mensour NA, Russell I. Fundamentals ofimmobilised yeast cells for continuous beer fermentation: a review. J InstBrew 1998;104:19–31.
[26] Karel SF, Libicki SB, Robertson CR. The immobilization of whole cells:engineering principles. Chem Eng Sci 1985;40:1321–54.
[27] Ratner BR, Hoffman AS, Schoen FJ, Lemons JE. Biomaterials science, anintroduction to materials in medicine. 2nd ed. San Diego, CA: ElsevierAcademic Press; 2004.
[28] Yu L, Ding J. Injectable hydrogels as unique biomedical materials. Chem SocRev 2008;37:1473–81.
[29] Nicodemus GD, Bryant SJ. Cell encapsulation in biodegradable hydrogels fortissue engineering applications. Tissue Eng B Rev 2008;14:149–65.
[30] Nguyen MK, Lee DS. Injectable biodegradable hydrogels. Macromol Biosci2010;10:563–79.
[31] Jen AC, Wake MC, Mikos AG. Review: hydrogels for cell immobilization.Biotechnol Bioeng 1996;50:357–64.
[32] Tibbitt MW, Anseth KS. Hydrogels as extracellular matrix mimics for 3D cellculture. Biotechnol Bioeng 2009;103:655–63.
[33] DeVolder R, Kong H-J. Hydrogels for in vivo-like three-dimensional cellularstudies. Wiley Interdiscip Rev Syst Biol Med 2012;4:351–65.
[34] Rowley JA, Madlambayan G, Mooney DJ. Alginate hydrogels as syntheticextracellular matrix materials. Biomaterials 1999;20:45–53.
[35] Kong H, Kaigler D, Kim K, Mooney D. Controlling rigidity and degradation ofalginate hydrogels via molecular weight distribution. Biomacromolecules2004;5:1720–7.
[36] Jeong SI, Jeon O, Krebs MD, Hill MC, Alsberg E. Biodegradable photo-crosslinkable alginate nanofibre scaffolds with tuneable physical properties,cell adhesivity and growth factors release. Eur Cells Mater 2012;24:331–43.
[37] Nakaoka R, Hirano Y, Mooney D, Tsuchiya T, Matsuoka A. Study on thepotential of RGD- and PHSRN-modified alginates as artificial extracellularmatrices for engineering bone. J Artif Organs 2013:1–10.
[38] Lin C-C, Anseth KS. PEG hydrogels for the controlled release of biomoleculesin regenerative medicine. Pharm Res 2009;26:631–43.
[39] Raeber GP, Lutolf MP, Hubbell JA. Molecularly engineered PEG hydrogels: anovel model system for proteolytically mediated cell migration. Biophys J2005;89:1374–88.
[40] Lutolf M, Lauer-Fields J, Schmoekel H, Metters A, Weber F, Fields G, et al.Synthetic matrix metalloproteinase-sensitive hydrogels for the conduction oftissue regeneration: engineering cell-invasion characteristics. Proc Natl AcadSci U S A 2003;100:5413–8.
[41] Wang F, Li Z, Khan M, Tamama K, Kuppusamy P, Wagner WR, et al. Injectable,rapid gelling and highly flexible hydrogel composites as growth factor andcell carriers. Acta Biomater 2010;6:1978–91.
[42] Seliktar D. Designing cell-compatible hydrogels for biomedical applications.Science 2012;336:1124–8.
[43] Li Y, Rodrigues J, Tomas H. Injectable and biodegradable hydrogels: gelation,biodegradation and biomedical applications. Chem Soc Rev2011;41:2193–221.
[44] Lee K, Mooney D. Hydrogels for tissue engineering. Chem Rev2001;101:1869–79.
[45] Drury JL, Mooney DJ. Hydrogels for tissue engineering: scaffold designvariables and applications. Biomaterials 2003;24:4337–51.
[46] Augst AD, Kong HJ, Mooney DJ. Alginate hydrogels as biomaterials. MacromolBiosci 2006;6:623–33.
[47] Lee D, Choi W, Byun M, Park H, Yu Y, Lee C. Effect of gamma-irradiation ondegradation of alginate. J Agric Food Chem 2003;51:4819–23.
[48] Smidsrod O, Skjak-Braek G. Alginate as immobilization matrix for cells.Trends Biotechnol 1990;8:71–8.
[49] Kim WS, Mooney DJ, Arany PR, Lee K, Huebsch N, Kim J. Adipose tissueengineering using injectable, oxidized alginate hydrogels. Tissue Eng A2012;18:737–43.
[50] Lee KY, Mooney DJ. Alginate: properties and biomedical applications. ProgPolym Sci 2012;37:106–26.
[51] http://clinicaltrials.gov.[52] Ménard M, Dusseault J, Langlois G, Baille WE, Tam SK, Yahia LH, et al. Role of
protein contaminants in the immunogenicity of alginates. J Biomed Mater ResB Appl Biomater 2010;93B:333–40.
[53] Orive G, Ponce S, Hernández RM, Gascón AR, Igartua M, Pedraz JL.Biocompatibility of microcapsules for cell immobilization elaborated withdifferent type of alginates. Biomaterials 2002;23:3825–31.
[54] Zimmermann U, Klock G, Federlin K, Hanning K, Kowalski M, Bretzel RG, et al.Production of mitogen-contamination free alginates with variable ratios ofmannuronic acid to guluronic acid by free flow electrophoresis.Electrophoresis 1992;13:269–74.
[55] Drury JL, Dennis RG, Mooney DJ. The tensile properties of alginate hydrogels.Biomaterials 2004;25:3187–99.
[56] Bouhadir K, Lee K, Alsberg E, Damm K, Anderson K, Mooney D. Degradation ofpartially oxidized alginate and its potential application for tissue engineering.Biotechnol Prog 2001;17:945–50.
[57] Prang P, Muller R, Eljaouhari A, Heckmann K, Kunz W, Weber T, et al. Thepromotion of oriented axonal regrowth in the injured spinal cord by alginate-based anisotropic capillary hydrogels. Biomaterials 2006;27:3560–9.
[58] Dhoot NO, Tobias CA, Fischer I, Wheatley MA. Peptide-modified alginatesurfaces as a growth permissive substrate for neurite outgrowth. J BiomedMater Res A 2004;71A:191–200.
[59] Mosahebi A, Wiberg M, Terenghi G. Addition of fibronectin to alginate matriximproves peripheral nerve regeneration in tissue-engineered conduits. TissueEng 2003;9:209–18.
[60] Hersel U, Dahmen C, Kessler H. RGD modified polymers: biomaterials forstimulated cell adhesion and beyond. Biomaterials 2003;24:4385–415.
[61] Donati I, Coslovi A, Gamini A, Vetere A, Campa C, Paoletti S. Galactose-substituted alginate. 2. Conformational aspects. Biomacromolecules2004;5:186–96.
[62] Donati I, Vetere A, Gamini A, Coslovi A, Campa C, Paoletti S. Galactose-substituted alginate: preliminary characterization and study of gellingproperties. Biomacromolecules 2003;4:624–31.
[63] Leone G, Torricelli P, Chiumiento A, Facchini A, Barbucci R. Amidic alginatehydrogel for nucleus pulposus replacement. J Biomed Mater Res A2008;84A:391–401.
[64] Pawar SN, Edgar KJ. Alginate derivatization: a review of chemistry, propertiesand applications. Biomaterials 2012;33:3279–305.
[65] Braccini I, Pérez S. Molecular basis of (Ca2+)-induced gelation in alginates andpectins: the egg-box model revisited. Biomacromolecules 2001;2:1089–96.
[66] Eiselt P, Lee KY, Mooney DJ. Rigidity of two-component hydrogels preparedfrom alginate and poly(ethylene glycol)-diamines. Macromolecules1999;32:5561–6.
[67] Gombotz WR, Wee S. Protein release from alginate matrices. Adv Drug DelivRev 1998;31:267–85.
[68] Morch YA, Donati I, Strand BL. Effect of Ca2+, Ba2+, and Sr2+ on alginatemicrobeads. Biomacromolecules 2006;7:1471–80.
[69] Martinsen A, Skjåk-Bræk G, Smidsrød O. Alginate as immobilization material.I. Correlation between chemical and physical properties of alginate gel beads.Biotechnol Bioeng 1989;33:79–89.
[70] Shoichet MS, Li RH, White ML, Winn SR. Stability of hydrogels used in cellencapsulation: an in vitro comparison of alginate and agarose. BiotechnolBioeng 1996;50:374–81.
[71] Kuhtreiber WM, Lanza RP, Chick WL, Chang TMS. Cell encapsulationtechnology and therapeutics (Tissue Engineering). Boston, MA: Birkhauser;1999.
[72] Kuo CK, Ma PX. Ionically crosslinked alginate hydrogels as scaffolds for tissueengineering. Part 1. Structure, gelation rate and mechanical properties.Biomaterials 2001;22:511–21.
[73] Moyer H, Kinney R, Singh K, Williams J, Schwartz Z, Boyan B. Alginatemicroencapsulation technology for the percutaneous delivery of adipose-derived stem cells. Ann Plast Surg 2010;65:497–503.
[74] Man Y, Wang P, Guo Y, Xiang L, Yang Y, Qu Y, et al. Angiogenic and osteogenicpotential of platelet-rich plasma and adipose-derived stem cell laden alginatemicrospheres. Biomaterials 2012;33:8802–11.
[75] Moshaverinia A, Chen C, Akiyama K, Ansari S, Xu X, Chee W, et al. Alginatehydrogel as a promising scaffold for dental-derived stem cells: an in vitrostudy. J Mater Sci Mater Med 2012;23:3041–51.
[76] Abbah S, Lu W, Chan D, Cheung K, Liu W, Zhao F, et al. Osteogenic behavior ofalginate encapsulated bone marrow stromal cells: an in vitro study. J MaterSci Mater Med 2008;19:2113–9.
[77] Ueng SWN, Lee MS, Lin SS, Chan E-C, Liu S-J. Development of a biodegradablealginate carrier system for antibiotics and bone cells. J Orthop Res2007;25:62–72.
[78] Abbah SA, Lu WW, Chan D, Cheung KMC, Liu WG, Zhao F, et al. In vitroevaluation of alginate encapsulated adipose-tissue stromal cells for use asinjectable bone graft substitute. Biochem Biophys Res Commun2006;347:185–91.
[79] Lee CSD, Watkins E, Burnsed OA, Schwartz Z, Boyan BD. Tailoring adiposestem cell trophic factor production with differentiation medium componentsto regenerate chondral defects. Tissue Eng A 2013;19:1451–64.
[80] Lee CSD, Burnsed OA, Raghuram V, Kalisvaart J, Boyan BD, Schwartz Z.Adipose stem cells can secrete angiogenic factors that inhibit hyalinecartilage regeneration. Stem Cell Res Ther 2012;3:35.
[81] Coates E, Fisher JP. Gene expression of alginate-embedded chondrocytesubpopulations and their response to exogenous IGF-1 delivery. J Tissue EngRegen Med 2012;6:179–92.
[82] Tay LX, Ahmad RE, Dashtdar H, Tay KW, Masjuddin T, Ab-Rahim S, et al.Treatment outcomes of alginate-embedded allogenic mesenchymal stemcells vs. autologous chondrocytes for the repair of focal articular cartilagedefects in a rabbit model. Am J Sports Med 2012;40:83–90.
[83] Dashtdar H, Rothan HA, Tay T, Ahmad RE, Ali R, Tay LX, et al. Apreliminary study comparing the use of allogenic chondrogenic pre-differentiated and undifferentiated mesenchymal stem cells for the repairof full thickness articular cartilage defects in rabbits. J Orthop Res2011;29:1336–42.
[84] Orth P, Kaul G, Cucchiarini M, Zurakowski D, Menger M, Kohn D, et al.Transplanted articular chondrocytes co-overexpressing IGF-I and FGF-2stimulate cartilage repair in vivo. Knee Surg Sports Traumatol Arthrosc2011;19:2119–30.
[85] Zhang F, Yao Y, Zhou R, Su K, Citra F, Wang D-A. Optimal construction anddelivery of dual-functioning lentiviral vectors for type I collagen-suppressed

S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662 1661
chondrogenesis in synovium-derived mesenchymal stem cells. Pharm Res2011;28:1338–48.
[86] Igarashi T, Iwasaki N, Kasahara Y, Minami A. A cellular implantation systemusing an injectable ultra-purified alginate gel for repair of osteochondraldefects in a rabbit model. J Biomed Mater Res A 2010;94A:844–55.
[87] Endres M, Wenda N, Woehlecke H, Neumann K, Ringe J, Erggelet C, et al.Microencapsulation and chondrogenic differentiation of humanmesenchymal progenitor cells from subchondral bone marrow in Ca-alginate for cell injection. Acta Biomater 2010;6:436–44.
[88] Eslaminejad M, Taghiyar L, Falahi F. Quantitative analysis of the proliferationand differentiation of rat articular chondrocytes in alginate 3D culture. IranBiomed J 2009;13:153–60.
[89] Yoon DM, Hawkins EC, Francke-Carroll S, Fisher JP. Effect of constructproperties on encapsulated chondrocyte expression of insulin-like growthfactor-1. Biomaterials 2007;28:299–306.
[90] Stojkovska J, Bugarski B, Obradovic B. Evaluation of alginate hydrogels underin vivo-like bioreactor conditions for cartilage tissue engineering. J Mater SciMater Med 2010;21:2869–79.
[91] Tran NM, Dufresne M, Duverlie G, Castelain S, Defarge C, Paullier P, et al. Anappropriate selection of a 3D alginate culture model for hepatic Huh-7 cellline encapsulation intended for viral studies. Tissue Eng A 2013;19:103–13.
[92] Kedziorek DA, Hofmann LV, Fu Y, Gilson WD, Cosby KM, Kohl B, et al. X-ray-visible microcapsules containing mesenchymal stem cells improve hind limbperfusion in a rabbit model of peripheral arterial disease. Stem Cells2012;30:1286–96.
[93] Doyle M, Perley J, Skalak T. Bone marrow-derived progenitor cells augmentvenous remodeling in a mouse dorsal skinfold chamber model. PLoS One2012;7:e32815.
[94] Ruvinov E, Leor J, Cohen S. The promotion of myocardial repair by thesequential delivery of IGF-1 and HGF from an injectable alginate biomaterialin a model of acute myocardial infarction. Biomaterials 2011;32:565–78.
[95] Hunt NC, Shelton RM, Grover L. An alginate hydrogel matrix for the localiseddelivery of a fibroblast/keratinocyte co-culture. Biotechnol J 2009;4:730–7.
[96] Klokk TI, Melvik JE. Controlling the size of alginate gel beads by use of a highelectrostatic potential. J Microencapsul 2002;19:415–24.
[97] Lima AC, Batista P, Valente TAM, Silva AS, Correia IJ, Mano JF. Novelmethodology based on biomimetic superhydrophobic substrates toimmobilize cells and proteins in hydrogel spheres for applications in boneregeneration. Tissue Eng A 2013;19:1175–87.
[98] Chang SCN, Chung H-Y, Tai C-L, Chen PKT, Lin T-M, Jeng L-B. Repair of largecranial defects by hBMP-2 expressing bone marrow stromal cells:comparison between alginate and collagen type I systems. J Biomed MaterRes A 2012;94A:433–41.
[99] Kang SW, Cha BH, Park H, Park KS, Lee KY, Lee SH. The effect of conjugatingRGD into 3D alginate hydrogels on adipogenic differentiation of humanadipose-derived stromal cells. Macromol Biosci 2011;11:673–9.
[100] Oliveira SM, Barrias CC, Almeida IF, Costa PC, Ferreira MRP, Bahia MF, et al.Injectability of a bone filler system based on hydroxyapatite microspheresand a vehicle with in situ gel-forming ability. J Biomed Mater Res B ApplBiomater 2008;87B:49–58.
[101] Javvaji V, Baradwaj AG, Payne GF, Raghavan SR. Light-activated ionic gelationof common biopolymers. Langmuir 2011;27:12591–6.
[102] Cui J, Wang M, Zheng Y, Rodriguez Muniz GM, del Campo A. Light-triggeredcross-linking of alginates with caged Ca2+. Biomacromolecules 2013;14(5):1251–6.
[103] Jeon O, Bouhadir KH, Mansour JM, Alsberg E. Photocrosslinked alginatehydrogels with tunable biodegradation rates and mechanical properties.Biomaterials 2009;30:2724–34.
[104] Thornton AJ, Alsberg E, Hill EE, Mooney DJ. Shape retaining injectablehydrogels for minimally invasive bulking. J Urol 2004;172:763–8.
[105] Lee KY, Bouhadir KH, Mooney DJ. Controlled degradation of hydrogels usingmulti-functional cross-linking molecules. Biomaterials 2004;25:2461–6.
[106] Jeon O, Alt DS, Ahmed SM, Alsberg E. The effect of oxidation on thedegradation of photocrosslinkable alginate hydrogels. Biomaterials 2012;33:3503–14.
[107] Rouillard AD, Berglund CM, Lee JY, Polacheck WJ, Tsui Y, Bonassar LJ, et al.Methods for photocrosslinking alginate hydrogel scaffolds with high cellviability. Tissue Eng C Methods 2011;17:173–9.
[108] Jeon O, Alsberg E. Photofunctionalization of alginate hydrogels to promoteadhesion and proliferation of human mesenchymal stem cells. Tissue Eng A2013;19:1424–32.
[109] Jeon O, Powell C, Ahmed SM, Alsberg E. Biodegradable, photocrosslinkedalginate hydrogels with independently tailorable physical properties and celladhesivity. Tissue Eng A 2010;16:2915–25.
[110] Smeds KA, Grinstaff MW. Photocrosslinkable polysaccharides for in situhydrogel formation. J Biomed Mater Res 2001;54:115–21.
[111] Chou AI, Akintoye SO, Nicoll SB. Photo-crosslinked alginate hydrogels supportenhanced matrix accumulation by nucleus pulposus cells in vivo.Osteoarthritis Cartilage 2009;17:1377–84.
[112] Chandler EM, Berglund CM, Lee JS, Polacheck WJ, Gleghorn JP, Kirby BJ, et al.Stiffness of photocrosslinked RGD–alginate gels regulates adipose progenitorcell behavior. Biotechnol Bioeng 2011;108:1683–92.
[113] Lee KY, Rowley JA, Eiselt P, Moy EM, Bouhadir KH, Mooney DJ. Controllingmechanical and swelling properties of alginate hydrogels independently bycross-linker type and cross-linking density. Macromolecules 2000;33:4291–4.
[114] Stevens B, Yang Y, Mohandas A, Stucker B, Nguyen KT. A review of materials,fabrication methods, and strategies used to enhance bone regeneration inengineered bone tissues. J Biomed Mater Res B Appl Biomater2008;85B:573–82.
[115] Habibovic P, de Groot K. Osteoinductive biomaterials – properties andrelevance in bone repair. J Tissue Eng Regen Med 2007;1:25–32.
[116] Bauer TW, Muschler GF. Bone graft materials: an overview of the basicscience. Clin Orthop Relat Res 2000;371:10–27.
[117] Rosa AL, de Oliveira PT, Beloti MM. Macroporous scaffolds associated withcells to construct a hybrid biomaterial for bone tissue engineering. Expert RevMed Devices 2008;5:719–28.
[118] Dawson JI, Oreffo ROC. Bridging the regeneration gap: stem cells,biomaterials and clinical translation in bone tissue engineering. ArchBiochem Biophys 2008;473:124–31.
[119] Alsberg E, Anderson K, Albeiruti A, Franceschi R, Mooney D. Cell-interactive alginate hydrogels for bone tissue engineering. J Dent Res2001;80:2025–9.
[120] Simmons C, Alsberg E, Hsiong S, Kim W, Mooney D. Dual growth factordelivery and controlled scaffold degradation enhance in vivo bone formationby transplanted bone marrow stromal cells. Bone 2004;35:562–9.
[121] Zachos T, Diggs A, Weisbrode S, Bartlett J, Bertone A. Mesenchymal stem cell-mediated gene delivery of bone morphogenetic protein-2 in an articularfracture model. Mol Ther 2007;15:1543–50.
[122] Majmudar G, Bole D, Goldstein SA, Bonadio J. Bone cell culture in a three-dimensional polymer bead stabilizes the differentiated phenotype andprovides evidence that osteoblastic cells synthesize type III collagen andfibronectin. J Bone Miner Res 1991;6:869–81.
[123] Giannoudis PV, Einhorn TA, Marsh D. Fracture healing: the diamond concept.Injury 2007;38:S3–6.
[124] Markusen JF, Mason C, Hull DA, Town MA, Tabor AB, Clements M, et al.Behavior of adult human mesenchymal stem cells entrapped in alginate–GRGDY beads. Tissue Eng 2006;12:821–30.
[125] Duggal S, Fronsdal KB, Szoke K, Shahdadfar A, Melvik JE, Brinchmann JE.Phenotype and gene expression of human mesenchymal stem cells inalginate scaffolds. Tissue Eng A 2009;15:1763–73.
[126] Chang SCN, Chung H-Y, Tai C-L, Chen PKT, Lin T-M, Jeng L-B. Repair of largecranial defects by hBMP-2 expressing bone marrow stromal cells:comparison between alginate and collagen type I systems. J Biomed MaterRes A 2010;94A:433–41.
[127] Huey D, Hu J, Athanasiou K. Unlike bone, cartilage regeneration remainselusive. Science 2012;338:917–21.
[128] Oldershaw RA. Cell sources for the regeneration of articular cartilage: thepast, the horizon and the future. Int J Exp Pathol 2012;93:389–400.
[129] Connelly JT, Garcia AJ, Levenston ME. Inhibition of in vitro chondrogenesis inRGD-modified three-dimensional alginate gels. Biomaterials 2007;28:1071–83.
[130] Zhang F, Su K, Fang Y, Sandhya S, Wang D-A. A mixed co-culture ofmesenchymal stem cells and transgenic chondrocytes in alginate hydrogelfor cartilage tissue engineering. J Tissue Eng Regen Med 2012.
[131] Endres M, Wenda N, Woehlecke H, Neumann K, Ringe J, Erggelet C, et al.Microencapsulation and chondrogenic differentiation of humanmesenchymal progenitor cells from subchondral bone marrow in Ca-alginate for cell injection. Acta Biomater 2010;6:436–44.
[132] Dobratz E, Kim S, Voglewede A, Park SS. Injectable cartilage: using alginateand human chondrocytes. Arch Facial Plast Surg 2009;11:40–7.
[133] Kaul G, Cucchiarini M, Arntzen D, Zurakowski D, Menger MD, Kohn D, et al.Local stimulation of articular cartilage repair by transplantation ofencapsulated chondrocytes overexpressing human fibroblast growth factor2 (FGF-2) in vivo. J Gene Med 2006;8:100–11.
[134] Madry H, Kaul G, Cucchiarini M, Stein U, Zurakowski D, Remberger K, et al.Enhanced repair of articular cartilage defects in vivo by transplantedchondrocytes overexpressing insulin-like growth factor I (IGF-I). Gene Ther2005;12:1171–9.
[135] Madry H, Cucchiarini M, Stein U, Remberger K, Menger MD, Kohn D, et al.Sustained transgene expression in cartilage defects in vivo aftertransplantation of articular chondrocytes modified by lipid-mediated genetransfer in a gel suspension delivery system. J Gene Med 2003;5:502–9.
[136] Puetzer J, Petitte J, Loboa E. Comparative review of growth factors forinduction of three-dimensional in vitro chondrogenesis in humanmesenchymal stem cells isolated from bone marrow and adipose tissue.Tissue Eng B 2010;16:435–44.
[137] Augello A, De Bari C. The regulation of differentiation in mesenchymal stemcells. Hum Gene Ther 2010;21:1–13.
[138] Madry H, Cucchiarini M. Clinical potential and challenges of using geneticallymodified cells for articular cartilage repair. Croat Med J 2011;52:245–61.
[139] Mierisch C, Wilson H, Turner M, Milbrandt T, Berthoux L, Hammarskjöld M,et al. Chondrocyte transplantation into articular cartilage defects with use ofcalcium alginate: the fate of the cells. J Bone Joint Surg Am 2003;85-A:1757–67.
[140] Wu L, Cai X, Zhang S, Karperien M, Lin Y. Regeneration of articularcartilage by adipose tissue derived mesenchymal stem cells: perspectivesfrom stem cell biology and molecular medicine. J Cell Physiol2013;228:938–44.
[141] Gantenbein-Ritter B, Chan SW. The evolutionary importance of cell ratiobetween notochordal and nucleus pulposus cells: an experimental 3-D co-culture study. Eur Spine J 2012;21:819–25.
1662 S.J. Bidarra et al. / Acta Biomaterialia 10 (2014) 1646–1662
[142] Stephan S, Johnson W, Roberts S. The influence of nutrient supply and celldensity on the growth and survival of intervertebral disc cells in 3D culture.Eur Cell Mater 2011;5:97–108.
[143] Bron JL, Vonk LA, Smit TH, Koenderink GH. Engineering alginate forintervertebral disc repair. J Mech Behav Biomed Mater 2011;4:1196–205.
[144] Baer AE, Wang JY, Kraus VB, Setton LA. Collagen gene expression andmechanical properties of intervertebral disc cell–alginate cultures. J OrthopRes 2001;19:2–10.
[145] Chiba K, Andersson G, Masuda K, Thonar E. Metabolism of the extracellularmatrix formed by intervertebral disc cells cultured in alginate. Spine1997;15:2885–93.
[146] Wang JY, Baer AE, Kraus VB, Setton LA. Intervertebral disc cells exhibitdifferences in gene expression in alginate and monolayer culture. Spine2001;26:1747–51.
[147] Kim J-S, Ellman MB, Yan D, An HS, Kc R, Li X, et al. Lactoferricin mediates anti-inflammatory and anti-catabolic effects via inhibition of IL-1 and LPS activityin the intervertebral disc. J Cell Physiol 2013;228(9):1884–96.
[148] Kim K-H, Kim Y-S, Kuh S-U, Park H-S, Park J-Y, Chin D-K, et al. Time- anddose-dependent cytotoxicities of ioxitalamate and indigocarmine in humannucleus pulposus cells. Spine J 2013;13(5):564–71.
[149] Moon J-H, Kuh S-U, Park H-S, Kim K-H, Park J-Y, Chin D-K, et al.Triamcinolone decreases bupivacaine toxicity to intervertebral disc cellin vitro. Spine J 2012;12:665–73.
[150] Mietsch A, Neidlinger-Wilke C, Schrezenmeier H, Mauer UM, Friemert B,Wilke H-J, et al. Evaluation of platelet-rich plasma and hydrostatic pressureregarding cell differentiation in nucleus pulposus tissue engineering. J TissueEng Regen Med 2013;7:244–52.
[151] Galateanu B, Dimonie D, Vasile E, Nae S, Cimpean A, Costache M. Layer-shaped alginate hydrogels enhance the biological performance of humanadipose-derived stem cells. BMC Biotechnol 2012;12:1–14.
[152] Jing W, Lin Y, Wu L, Li X, Nie X, Liu L, et al. Ectopic adipogenesis ofpreconditioned adipose-derived stromal cells in an alginate system. CellTissue Res 2007;330:567–72.
[153] Venugopal JR, Prabhakaran MP, Mukherjee S, Ravichandran R, Dan K,Ramakrishna S. Biomaterial strategies for alleviation of myocardialinfarction. J Royal Soc Interface 2012;9:1–19.
[154] Johnson TD, Christman KL. Injectable hydrogel therapies and their deliverystrategies for treating myocardial infarction. Expert Opin Drug Deliv2013;10:59–72.
[155] Christman KL, Lee RJ. Biomaterials for the treatment of myocardial infarction.J Am Coll Cardiol 2006;48:907–13.
[156] Davis ME, Hsieh PCH, Grodzinsky AJ, Lee RT. Custom design of the cardiacmicroenvironment with biomaterials. Circ Res 2005;97:8–15.
[157] Landa N, Miller L, Feinberg MS, Holbova R, Shachar M, Freeman I, et al. Effectof injectable alginate implant on cardiac remodeling and function after recentand old infarcts in rat. Circulation 2008;117:1388–96.
[158] Leor J, Tuvia S, Guetta V, Manczur F, Castel D, Willenz U, et al. Intracoronaryinjection of in situ forming alginate hydrogel reverses left ventricularremodeling after myocardial infarction in swine. J Am Coll Cardiol2009;54:1014–23.
[159] Tsur-Gang O, Ruvinov E, Landa N, Holbova R, Feinberg MS, Leor J, et al. Theeffects of peptide-based modification of alginate on left ventricularremodeling and function after myocardial infarction. Biomaterials2009;30:189–95.
[160] Yu J, Gu Y, Du KT, Mihardja S, Sievers RE, Lee RJ. The effect of injected RGDmodified alginate on angiogenesis and left ventricular function in a chronicrat infarct model. Biomaterials 2009;30:751–6.
[161] Yu J, Du KT, Fang Q, Gu Y, Mihardja SS, Sievers RE, et al. The use of humanmesenchymal stem cells encapsulated in RGD modified alginatemicrospheres in the repair of myocardial infarction in the rat. Biomaterials2010;31:7012–20.
[162] Perale G, Rossi F, Sundstrom E, Bacchiega S, Masi M, Forloni G, et al.Hydrogels in spinal cord injury repair strategies. ACS Chem Neurosci2011;2:336–45.
[163] Li L, Davidovich AE, Schloss JM, Chippada U, Schloss RR, Langrana NA, et al.Neural lineage differentiation of embryonic stem cells within alginatemicrobeads. Biomaterials 2011;32:4489–97.
[164] Pettingill L, Wise A, Geaney M, Shepherd R. Enhanced auditory neuronsurvival following cell-based BDNF treatment in the deaf guinea pig. PLoSOne 2011;6:e18733.
[165] Francis NL, Shanbhag MS, Fischer I, Wheatley MA. Influence of alginate cross-linking method on neurite response to microencapsulated neurotrophin-producing fibroblasts. J Microencapsul 2011;28:353–62.
[166] Weir GC. Islet encapsulation: advances and obstacles. Diabetologia 2013:1–4.[167] Kendall WF, Darrabie MD, El-Shewy HM, Opara EC. Effect of alginate
composition and purity on alginate microspheres. J Microencapsul2004;21:821–8.
[168] Rezania A, Bruin JE, Riedel MJ, Mojibian M, Asadi A, Xu J, et al. Maturation ofhuman embryonic stem cell derived pancreatic progenitors into functionalislets capable of treating pre-existing diabetes in mice. Diabetes2012;61:2016–29.
[169] Erro E, Bundy J, Massie I, Chalmers S, Gautier A, Gerontas S, et al.Bioengineering the liver: scale-up and cool chain delivery of the liver cellbiomass for clinical targeting in a bioartificial liver support system. BioresOpen Acess 2013;2:1–11.
[170] Huang X, Hang R, Wang X, Lin N, Zhang X, Tang B. Matrix stiffness in three-dimensional systems effects on the behavior of C3A cells. Artif Organs2013;37:166–74.
[171] Hill E, Boontheekul T, Mooney DJ. Designing scaffolds to enhancetransplanted myoblast survival and migration. Tissue Eng2006;12:1295–304.
[172] Borselli C, Cezar CA, Shvartsman D, Vandenburgh HH, Mooney DJ. The role ofmultifunctional delivery scaffold in the ability of cultured myoblasts topromote muscle regeneration. Biomaterials 2011;32:8905–14.
[173] Barminko J, Kim JH, Otsuka S, Gray A, Schloss R, Grumet M, et al.Encapsulated mesenchymal stromal cells for in vivo transplantation.Biotechnol Bioeng 2011;108:2747–58.
[174] Le Blanc K, Ringdén O. Immunomodulation by mesenchymal stem cells andclinical experience. J Intern Med 2007;262:509–25.
[175] Goren A, Dahan N, Goren E, Baruch L, Machluf M. Encapsulated humanmesenchymal stem cells: a unique hypoimmunogenic platform for long-termcellular therapy. FASEB J 2010;24:22–31.
[176] Garate A, Murua A, Orive G, Hernandez RM, Pedraz JL. Stem cells in alginatebioscaffolds. Ther Deliv 2012;3:761–74.
[177] Jain R, Au P, Tam J, Duda D, Fukumura D. Engineering vascularized tissue. NatBiotechnol 2005;23:821–3.
[178] Gandhi JK, Opara EC, Brey EM. Alginate-based strategies for therapeuticvascularization. Ther Deliv 2013;4:327–41.
[179] Landázuri N, Levit RD, Joseph G, Ortega-Legaspi JM, Flores CA, Weiss D, et al.Alginate microencapsulation of human mesenchymal stem cells as a strategyto enhance paracrine-mediated vascular recovery after hindlimb ischaemia. JTissue Eng Regen Med 2012.
[180] Segers V, Lee R. Stem-cell therapy for cardiac disease. Nature2008;451:937–42.
[181] Baiguera S, Ribatti D. Endothelialization approaches for viable engineeredtissues. Angiogenesis 2013;16:1–14.
[182] Vacharathit V, Silva EA, Mooney DJ. Viability and functionality of cellsdelivered from peptide conjugated scaffolds. Biomaterials 2011;32:3721–8.
[183] Cloyd Jordan M, Malhotra Neil R, Weng Lihui, Chen Weiliam, Mauck Robert L,Elliott Dawn M. Material properties in unconfined compression of humannucleus pulposus, injectable hyaluronic acid-based hydrogels and tissueengineering scaffolds. Eur Spine J 2007;16(11):1892–8.
[184] Umehara S, Tadano S, Abumi K, Katagiri K, Kaneda K, Ukai T. Effects ofdegeneration on the elastic modulus distribution in the lumbar intervertebraldisc. Spine 1996;21(7):811–9.