innovations in elder care - ihi home pageapp.ihi.org/.../document-6045/c2_presentation.pdf ·...
TRANSCRIPT

12/10/2012
1
Innovations in Elder Care
Jennie Chin Hansen, CEO, RN, MS, FAAN
American Geriatrics Society
Warren Wong, MD, FACP
National Medicare Strategy, Kaiser
Permanente
Session C2
The presenters have nothing to disclose
12/11/2012
1:30 PM
Session Objectives
Be able to describe initiatives that emphasize alternatives to traditional patient and disease focused care delivery.
Provide perspective on a shared and actionable vision for Older Adults with Complex Needs.
Plan activities within their own work environments

12/10/2012
2
Evolving Directions in Framing Health and Care of Older Adults
A directional shift from reimbursement of volume towards outcome.
Focus on improving quality, safety and value.
Recognize the importance of addressing cost outliers.
There are more concrete population health initiatives that go beyond the hospital and facility settings
Health care payors and providers are learning to expand their consideration of “patient” to “older adult”
Examples of Innovative Practices
Long Term Quality Alliance
Coalition with example of best practices
CMS-Center for Innovations and Other ACA Enabled Efforts
Partnership for Patients
Independence at Home
ACA Section 3024
Hospital at Home
Stanford Coordinated Care
Chronic Care, Employer Based Systems

12/10/2012
3
Long Term Quality Alliance (LTQA)
Begun late 2010
Influenced by December 2010 article published in the Stanford Social Innovation Review (Winter 2011) explored a new “Collective Impact”(Kania and Kramer) approach to community change
Cross sector membership committed to quality of care transitions and stewarding resources
LTQA Initial Best Practices
Cathedral Square Corporation (Housing Corporation)
• Evolved from landlord role to advocate monitoring health and
coordinating services help resident stability-
• 1 year outcome-22% falls reduction, 19% reduced risk reduction of
those of moderate risk; physically inactive residents reduced by
10%
• July 2011-112 housing projects added
• Estimated $40million w health care
Savings to Medicare

12/10/2012
4
LTQA Initial Best Practices
Community Resource Identification and Coordination to ease
transitions form home to hospital-
Created NC Alliance for effective Care Transitions-30 org
stakeholders to coordinate aging and long term care services and
supports
1. 6 counties assisted for CC Transitions Program
2. Coordination of Aging and Disability Resource Centers (ADRCs)
3. Support for 14 films-”Caring Matters” for caregivers
Carol Woods Retirement Community
The Triple Aimfor the Older Adult
Better Care
Better
Health Lower Costs
Maintain best function and
engagement in home and
community: prevention, self
care, coordination
Hospital-Quality and Safety
•ACE-Acute Care for Elders
•Transitions Programs-Naylor,
Coleman, Boost, Project Red
•NICHE
•Value Based Purchasing
•Partnership for Patients
Save $$$ for
consumer/family, payors,
society-Medicare,
Medicaid

12/10/2012
5
Community Based Care Transitions Program (CCTP)-Section 3026
Provide Payment for Care Transitions Services to Improve Health and Reduce Readmissions
An Engine & Asset to Connect Hospitals and Communities to Help Patients
47 Sites in Place with Many More on the Way
Buttressed by HENs, QIOs, AAAs, ADRCs and Many Other Resources to Reduce Readmissions
The Community-Based Care Transitions Program (CCTP, ACA Section 3026)
Now 47 Sites: CBOs with 200+ hospitals
serving 185,500 beneficiaries in 21 states

12/10/2012
6
There has never been a time like this in U.S. Health Care: unique confluence of forces for change
1. There is unprecedented Federal action and coordination, including CMS payment reform and innovation.
2. Physicians and other health professionals need to be front and center in these efforts: We need your more active involvement to get this right.
Council of Medical Specialty Societies: McGann and Wagner Nov 2012 CMS
Partnership for PatientsTen Priority Areas of Focus
1. Adverse Drug Events
2. Catheter-Associated Urinary Tract Infections
3. Central Line Associated Blood Stream Infections
4. Injuries from Falls and Immobility
5. Obstetrical Adverse Events *
6. Pressure Ulcers
7. Surgical Site Infections
8. Venous Thromboembolism
9. Ventilator-Associated Pneumonia
10. Reducing ReadmissionsSource: CMMS 2012
* Only area that would not relate to older adults

12/10/2012
7
Innovation Center PortfolioLong-Term Care Involvement in Many Areas
Primary Care Transformation●●●● Comprehensive Primary Care Initiative (CPC)●●●● Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration●●●● Federally Qualified Health Center (FQHC) Advanced Primary Care Practice Demonstration●●●● Independence at Home Demonstration●●●● Graduate Nursing Education Demonstration
ACOs●●●● Medicare Shared Savings Program●●●● Pioneer ACO Model●●●● Advance Payment ACO Model●●●● PGP Transition Demonstration
Bundled Payment for Care Improvement●●●● Model1: Retrospective Acute Care ●●●● Model 2: Retrospective Acute Care Episode & Post Acute●●●● Model 3: Retrospective Post Acute Care●●●● Model 4: Prospective Acute Care
c ●●●● Partnership for Patients
●●●● Community-Based Care Transitions●●●● Million Hearts ●●●● Innovation Advisors Program● Health Care Innovation Challenge
Initiatives Focused on the Medicaid Population●●●● Medicaid Emergency Psychiatric Demonstration●●●● Medicaid Incentives for Prevention of Chronic Diseases●●●● Strong Start Initiative
Dual Eligible Beneficiaries●●●● State Demonstration to Integrate Care for Dual Eligible Individuals●●●● Financial Models to Support State Efforts to Integrate Care●●●● Demonstration to Reduce Avoidable Hospitalizations of Nursing Facility Residents
Source: CMMS 2012
There has never been a time like this in U.S. Health Care: unique confluence of forces for change
1. There is unprecedented Federal action and coordination, including CMS payment reform and innovation.
2. Physicians and other health professionals need to be front and center in these efforts: We need your more active involvement to get this right.
Council of Medical Specialty Societies: McGann and Wagner Nov 2012 CMS

12/10/2012
8
Header
Hospital at Home®: Disseminating an Innovative Health
Service Delivery Model into Practice
Bruce Leff, MDProfessor of MedicineJohns Hopkins University Schools of Medicine & Public Health
Hospital at Home slides source: Bruce Leff, MD 2012
Hospital Safety Pre IOM
Hospitalat Home®
16

12/10/2012
9
Hospitalat Home®
Hospital Safety Over Time – Post IOM
� 10 NC hospitals, annual review of charts ‘02 to ‘07, n=2341� 588 harms = Rate: 25.1 / 100 admits
� Harms:
� 2.9% permanent
� 8.5% life threatening
� 2.4% caused or contributed to death
� Harms from procedures, medications, nosocomial infections, other therapies, diagnostic evaluations, falls
� No change over time in rate of harms
NEJM 2010;363:2124
• 61% chose HAH care• HaH is feasible and efficacious• High-quality care• Fewer complications• Higher satisfaction • Lower costs of care
Ann Intern Med. 143:798-808, 2005. J Am Geriatr Soc. 54:1355-1363, 2006. J Am
Geriatr Soc. 2008;56(1):117-23. Am J Manag Care. 15:49-56, 2009. J Am Geriatr
Soc. 2009;57(2):273-8. Medical Care, 47(9):979-85, 2009.
Less CG stress
Better function
High provider satisfaction
Hospitalat Home®

12/10/2012
10
HaH at Presbyterian Health SystemHaH for PHS health plan pts1st year of HaH
4 diagnoses, 125 patients10/08 – 4/12: 582 patients1/1/09 – 12/31/10
323 patients93% acceptance rate
Care ProvisionMean MD visits 3.5 (SD 2.8)Mean RN visits 6.4 (SD 3.2)2.5% return to hospital to complete admissionAfter-hours, unplanned visits
15 RN, 3 MD
� LOS
� HaH 3.3, median 3, 1-31
� Hospital 4.5, median 4, 1-50� 2.5% transfer to hospital to complete
admission� Mortality during admission
� 0.93% HaH v 3.4% hospital � Satisfaction – Press Ganey CAHPS
adapted to HaH� 90.7 HaH v 83.9 hospital
� Readmission 30d� 10.8 HaH v 10.5% hospital
Scaling HaH into a Nationwide Model is the New Frontier
Goal: to transform the site of acute health care from the hospital to the home with a nationally scaled health services delivery organization
Australian example
Key decision 1994: reimburse HaH as inpatient service. Led to units being based in hospitals
2009: 32K admissions = 2.3% all inpatient admissions & 5% all bed days
Hospitalat Home®
20
MJA 2010;193:598
12/10/2012
11
Independence at Home (IAH)
� 2009 HB 2560 (Markey) + S 1131 (Wyden)� 2010 ACA section 3024� Medically-led interdisciplinary team (MD or NP)
� House calls, with technology�Portable diagnostics, telemedicine
� 24-7-365 availability� Electronic health record� Expertise and experience with model
� Keep + use existing Medicare benefits (A,B)� Savings (gain-sharing)
� First 5% � Medicare; then 80% � IAH� 10,000 beneficiary cap in current demo
Why Independence At Home (IAH)
Immobile, complex population is better served at home
Patient and family centered
Better insight into illness and needs, better care plan
More timely response when getting sick
Real opportunity for near term cost savings
Targets highest cost subset with a viable solution that people prefer

12/10/2012
12
Cost Savings Evidence
VA HBPC (large cohort before and after) ~ 24%
Savings relative to HCC-modeled costs
Naylor post-hospital transitional care (RCT) ~ 50%
GRACE (RCT) ~ 30% in high cost subset, year 2
ElderPAC (AAA + house calls; case control) ~ 50%
VCUHS Transitional Care (pre-post) ~ 50%
Many examples with reported positive impacts
Mount Sinai, Inspiris (acquired by United HC), Clinic Without Walls, etc
IAH Patient Selection
� Multiple chronic diseases (at least 2)�Ones that directly cause disability (not HTN)
� Functional deficit (2 or more ADLs)�Requiring human help
� One or more non-elective inpatient hospital stays within 12 months
� Post-acute care�HHA, SNF, IP Rehab (all report ADLs)
� High cost – higher is better ($50,000 +)

12/10/2012
13
IAH Demontration Project
Under Office of Research and Demonstration, now in CMMI
RFA released 12-20-11; August 2012-18 sites
Minimal IAH site size = 200 patients
Maximum number for demo (currently) is 10,000 nationally, all sites
3 options: single site, part of national pool, regional consortium of programs
3 years
IAH Attributes
� Voluntary
� Advanced mobile medical team = access
� Medical leader = adjusts to condition changes
� Longitudinal, continuous, comprehensive
� Where you want it, when you need it
� Less ER, hospital time = better, safer
� Incents medical providers to engage in model
� Funded from savings = accountable� Minimal initial investment
� Immediate savings (1 to 2 years) - $billions

12/10/2012
14
Stanford Coordinated Care
“Tools, Training and Teams to Achieve the Triple Aim”
Alan Glaseroff, MD
Sept 2012
Adapting a Trend-Bending Care Model:

12/10/2012
15
A Costly Health System Failure
• Avoidable Hospital Admissions 2x more likely for asthma and diabetes in US
vs. average of 30 developed countries in Organization for Economic
Cooperation and Development
“The United States does not do well in preventing costly hospital admissions
for chronic conditions, such as asthma or complications from diabetes,
which should normally be managed through proper primary care.”
(Organization for Economic Cooperation and Development. Expensive
healthcare is not always the best healthcare, says OECD’s Health at a Glance
[Internet]. Paris: OECD; 2009 Aug [cited 2010 Jan 3)]).
vs.
1.Panel Management 2. Care Management for 3. Complex Case Management
Chronic Disease
•Registries
•Gaps in Care
•Planned Visits
•Self Management
Support
•Patient Education
•Patient Activation
•Care Coordination
•Problem Solving
•Linking with
Community Resources
•Empowerment and
Education
Modest Potential Value Gain from
std Medical Home
Large Potential Value Gain from
Intensified Medical Home
Where’s the Leverage on Trend?

12/10/2012
16
Take away themes
Treating segments of population with the most appropriate health and health care in settings that are most conducive to effectiveness
Consider the whole environment of the person as an asset to health and chronicity maintenance
Engagement and capacity of the person/patient toward health and well being
Enlargement of the caring provider roles-i.e. not just the professionally licensed
Current Practice Model
DM & CRF
DM & HTN
COPD
CVA & HTN
DM & CAD
DM & Alz & AF
BPH
Physician
HTN

12/10/2012
17
Segmentation-Based Practice Model
33
Segment 1
Healthy, Robust
Segment 2
Chronic Conditions
Segment 3
Advanced Illness
Segment 4
Severe Frailty
End-of-life
Segment Specific Interventions
• benefit from palliative care, hospice care and high touch programs• use health care services erratically partly due to poor access to care
• have chronic illness and benefit most from disease management approaches • use health care services, mostly outpatient, regularly
• have multiple complex issues• frequent ER visits and hospital admissions
• largest benefit is from disease prevention, screening and health promotion• use health care services periodically
Features
of each
segmentSegment 1
Robust
Segment 2
Chronic
Conditions
Segment 3
Advanced
Illness
Segment 4
Severe Frailty/
End of life

12/10/2012
18
What is the Optimal Process to Segment Older Adults??
•Self report yields important domains
of information but is logistically
intensive and prone to inaccuracy
over time.
•Provider report is arduous and prone
to inconsistency.
The Senior Segmentation Algorithm was initially developed
with a group of physicians based on empirical derivation,
clinical reasoning, & workflow choices. It incorporates a
combination of diagnosis, a utilization prediction tool, and
specific data points available from administrative data and
the EMR.
15-20% 10-15%
Per Member per month Cost Ratio:
1X 2-3X 5-8X
5-7%
Estimated %
Medicare
Members:
60-65%
Healthy
15-20X
Chronic Conditions
Advanced Illness
Frailty
End of life
Overall cost of
care per segment
based on
membership and
cost ratio:
PMPM Cost x
percentage
/total costs
5% 45% 30% 20%
What is the Cost of Care in Each Segment??

12/10/2012
19
Segmentation Findings
Most members remain in the same segment over a year’s period of time
Those that change segments generally move to a “higher” segment
1/1/2010 As of 12/1/2010
As of 1/1/2010
Starting Pop Seg 1 Seg 2 Seg 3 Seg 4
Seg 1 14.0% 68.4% 29.4% 1.5% 0.7%
Seg 2 63.1% 2.6% 88.2% 7.0% 2.1%
Seg 3 15.0% 0.2% 9.5% 80.1% 10.3%
Seg 4 7.9% 0.2% 5.5% 13.7% 80.6%
Mortality Risk Increases from Segment to Segment
Segment @ 1/1/10
Members % Deceased 6/30/10
% Deceased 12/31/10
Segment 1 8563 0.4% 0.6%
Segment 2 38629 0.5% 1.2%
Segment 3 9175 2.6% 5.5%
Segment 4 4822 15.2% 28.0%
• Determining and implementing optimal system
design features for each segment.
• Is there VARIATION in segment sizes in various health
systems?
• Is there variation in health system practices for
specific segments?
• Is there variation in migration from segment to
segment and can the rate of migration be impacted?
•Segmentation is a TOOL, not an outcome
•Segmentation and PERSON CENTERED care go hand in
hand
How Can Segmentation be Used?
12/10/2012
20
A nation's greatness is
measured by how it treats
its weakest members."
Mahatma Ghandi
Achieving the Triple Aim
for Older Adults with
Complex Conditions
Patients age 85 and over account for 10.2
% of all hospital days in the United states
while accounting for 1.7% of the
population
Only 41% of these patients are discharged
home, while 33% are sent to institutional
care
http://www.cdc.gov/nchs/data/series/sr_
13/sr13_165.pdf
Achieving the Triple Aim for
Older Adults with Complex Conditions
I. Core Conceptual Framework
II. System Design
III. Critical Factors for Success
A goal beyond the capability of the
system will not be reached. You will
get whatever the system will deliver.
W E Demming

12/10/2012
21
Core Concept A: Older Adults benefit from a comprehensive whole person evaluation and personalized health and well-being plan.
1. What matters to you: preferences, values, priorities, preferences, attachments, concerns and social milieu.
2. Tell us about yourself: Emotional, social, cognitive and physical well-being, functional status.
3. Common conditions in older adults/geriatric syndrome.
4. The evaluation should be done routinely akin to a well child check.
5. The evaluation should be the basis of a health and well-being plan.
NOT TYPICAL PRACTICE NOW
Core Concept B: Care must be integrated
and coordinated across settings
• Within the entire Health Care Delivery
system.
•Between the health care system and
community services.
•Coordinated with caregivers. Most care
occurs in the home.
NOT TYPICAL PRACTICE NOW

12/10/2012
22
Core Concept C: Functional Status
should be a cornerstone of care.
•Primary importance for independence.
•Key indicator of reserve capacity,
prognosis and health care utilization.
•Variable and fluctuates but overall
decline over time occurs in the older
adult.
NOT A CORE TENENT OF PRACTICE
Core Concept D: With progressive functional decline,
disease based model of care becomes of less and less
value.•SLIGHT DECLINE: “linked” to desirable services such as transportation
services and meals on wheels.
•MODERATE DECLINE: patient should remain in the primary care setting but
there is more emphasis on “well-coordinated” care in which community
based and home based services play an increasing role and are partners in
care. At this point, these services provide strong support to the patient,
unpaid caregivers as well as to the primary care team.
•SEVERE DECLINE: transitions to special programs of care such as hospice,
home visit program or nursing home care. Non physician services become
more important and physician services less.
NOT TYPICAL PRACTICE NOW

12/10/2012
23
Frailty Care SettingsHospital-based Services
Clinic-based Services
Geriatrics principles embedded in all services and programs
Connected by an integrated, informed, accurate, and available information system
System measurement and monitoring across the continuum of care
Status: Robust
Linked Services
Status: Progressive Frailty
Coordinated Services
Status: End of Life
Fully Integrated Services
Frailty Care Services (at home)
Home and Community-based Services
System Features Enabling Older Adults with
Complex Conditions to Live at Home
A Report from Primary Care
Comparison of Needed vs Available Elements of Care
For Older Adults with Complex Needs
Very or Extremely Likely to improve Care & reduce costs
Occurs most of the time or always
Occurs sometimesOr rarely
Element
Case Management
Assessment of psychosocial needs
Plan of Care
Home visit by MD or NP
88 %
81 %
69 %
63 %
13 %
27 %
27 %
20 %
80 %
73 %
73 %
80 %
12/10/2012
24
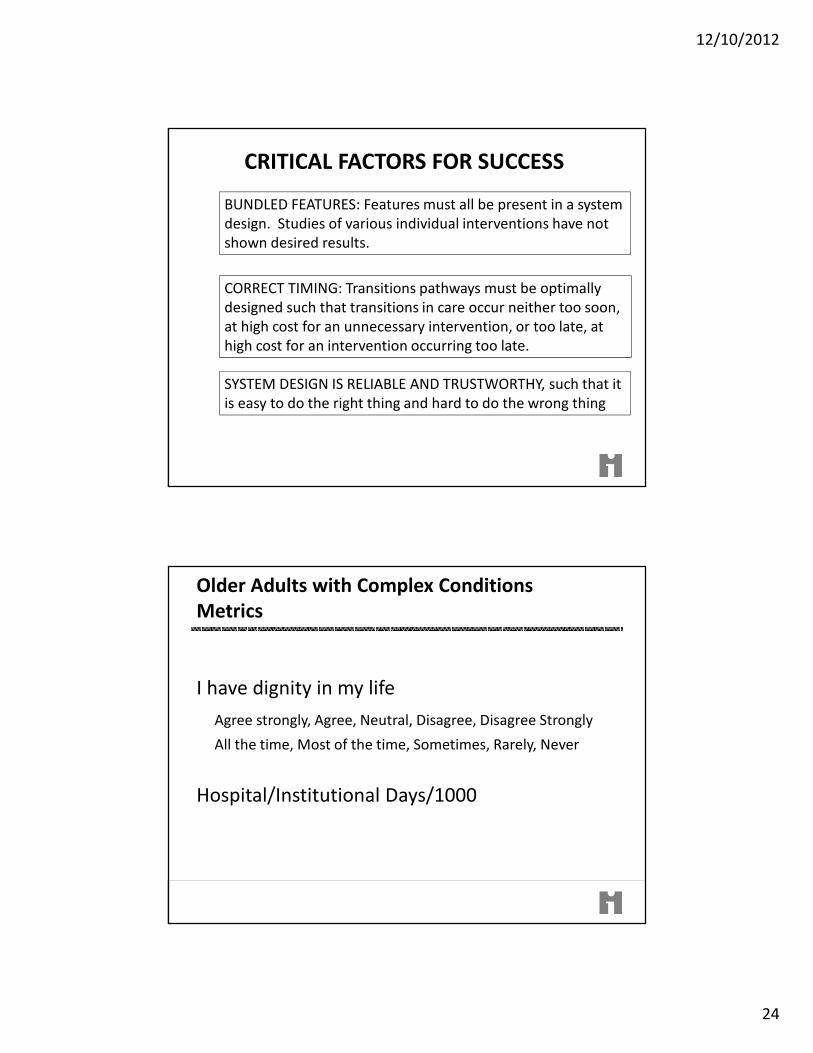
CRITICAL FACTORS FOR SUCCESS
BUNDLED FEATURES: Features must all be present in a system
design. Studies of various individual interventions have not
shown desired results.
CORRECT TIMING: Transitions pathways must be optimally
designed such that transitions in care occur neither too soon,
at high cost for an unnecessary intervention, or too late, at
high cost for an intervention occurring too late.
SYSTEM DESIGN IS RELIABLE AND TRUSTWORTHY, such that it
is easy to do the right thing and hard to do the wrong thing
Older Adults with Complex Conditions
Metrics
I have dignity in my life
Agree strongly, Agree, Neutral, Disagree, Disagree Strongly
All the time, Most of the time, Sometimes, Rarely, Never
Hospital/Institutional Days/1000

12/10/2012
25
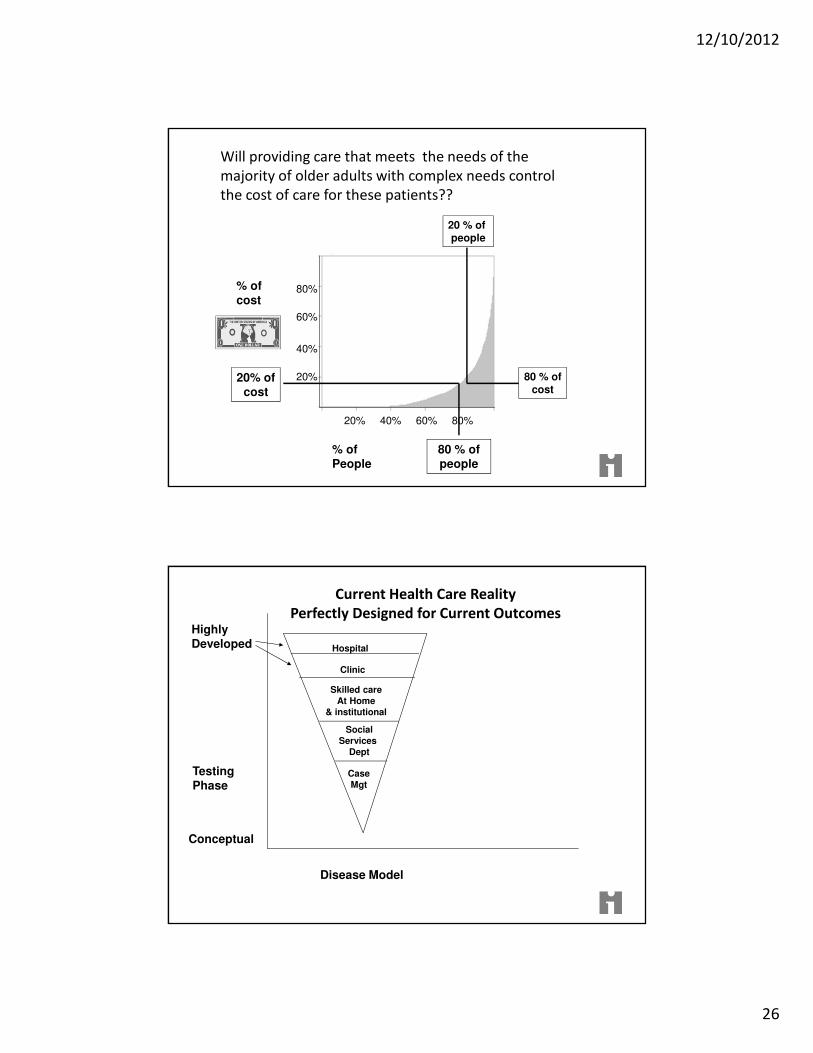
Will providing care that meets the needs of the
majority of older adults with complex needs control
the cost of care for these patients??
% of People
Will providing care that meets the needs
of the majority of older adults with complex needs
control the cost of care for these patients??
20%
40%
60%
80%
20% 40% 60% 80%
% ofcost
�
12/10/2012
26
% of People
Will providing care that meets the needs of the
majority of older adults with complex needs control
the cost of care for these patients??
20%
40%
60%
80%
20% 40% 60% 80%
% ofcost
� 80 % of people
20% ofcost
80 % ofcost
20 % of people
Current Health Care Reality
Perfectly Designed for Current OutcomesHighly Developed
TestingPhase
Conceptual
Disease Model
Hospital
Clinic
Skilled careAt Home
& institutional
SocialServices
Dept
CaseMgt

12/10/2012
27
Population Health, One of the Triple Aims,
is largely at the conceptual stage
Highly Developed
TestingPhase
Conceptual
Disease Model Population Health Model
patient
person
Dz““““Family””””Existing community
infrastructure
Community health workers
Self help Villages
Community ActivationSocial Movements
Social Policy
Hospital
Clinic
Skilled careAt Home
& institutional
SocialServices
Dept
CaseMgt
““““Public Health””””
patient
person
Dz““““Family””””Existing community
infrastructure
Community health workers
Self help Villages
““““Public Health””””Community ActivationSocial MovementsSocial Policy
Hospital
Clinic
Skilled careAt Home
& institutional
SocialServices
Dept
CaseMgt
Highly Developed
TestingPhase
Conceptual
Creating Change in Health Care Reality
PUSH PULL
TOOLS
Disease management tools
Care Plans
Segmentationmodels
Personal Navigators
Information Tech
Social Networks
Big Data
Community Integration
Disease Model Population Health Model

12/10/2012
28
Jennie Chin Hansen, RN, MS, FAANCEO, American Geriatrics [email protected]
Warren Wong, MD, FACP, Physician Lead, Medicare Transformation, Kaiser [email protected]
Thank You