international registry relapsed aml 2009neu - skion - home · international registry relapsed aml...
TRANSCRIPT
International Registry
Relapsed AML 2009
Registry of children and adolescents with relapsed or refractory acute myeloid leukemia (AML)
AML-BFM-Study Group
Coordination
Dirk Reinhardt, MD, PhD Ursula Creutzig, MD, PhD
Pediatric Hematology and Oncology Pediatric Hematology and Oncology
Hannover Medical School University Children’s Hospital Münster
Carl-Neuberg-Str. 1 Albert-Schweitzer-Str. 33
D-30625 Hannover D- 48129 Münster
Tel.: +49 (0)511 532 6720 Tel.: +49 (0)511 604 66 77 or +49 (0)511 532 9123
Fax: +49 (0)511 532 9029 Fax: +49 (0)511/604 64 04 or +49 (0)511 532 9029
E-mail: [email protected] E-mail: [email protected]
Gertjan J.L. Kaspers, MD, PhD
Department of Pediatric Hematology/Oncology
VU medical center
De Boelelaan 1117
NL-1081 HV Amsterdam
The Netherlands.
Phone: +31 (0)20 444 2420
Fax: +31 (0)20 444 2422
E-mail: [email protected]
Registry center Statistician
Ursula Bernsmann Martin Zimmermann, PhD
Pediatric Hematology and Oncology Pediatric Hematology and Oncology
Hannover Medical School Hannover Medical School
Carl-Neuberg-Str. 1 Carl-Neuberg-Str. 1
D-30625 Hannover D-30625 Hannover
Tel.: +49 (0)511 532 9123 E-mail: [email protected]
Fax: +49 (0)511 532 9029
E-mail: [email protected]
International Registry AML Relapse 2009 / -June ’09 - 2 -
Addresses
Dirk Reinhardt, MD, PhD
Hannover Medical School
Pediatric Hematology and Oncology
Carl-Neuberg-Str. 1
D-30625 Hannover
Tel.: +49 (0)511 532 6720
Fax: +49 (0)511 532 9029
E-mail: [email protected]
Gertjan J.L. Kaspers, MD, PhD
Department of Pediatric Hematology/Oncology
VU medical center
De Boelelaan 1117
NL-1081 HV Amsterdam
The Netherlands.
Phone: +31 – 20 444 2420
Fax: +31 – 20 444 2422
E-mail: [email protected]
Ursula Creutzig, MD, PhD
Pediatric Hematology and Oncology
University Children’s Hospital Münster
Albert-Schweitzer-Strasse 33
D-48129 Münster
Germany
Phone: +49 (0)511 604 66 77 or +49 (0)511 532 9123
Fax: +49 (0)511/604 64 04 or +49 (0)511 532 9029
E-mail: [email protected]
Central Data Office International Statistician
Ursula Bernsmann Martin Zimmermann, PhD
Pediatric Hematology and Oncology Pediatric Hematology and Oncology
Hannover Medical School Hannover Medical School
Carl-Neuberg-Str. 1 Carl-Neuberg-Str. 1
D-30625 Hannover D-30625 Hannover
Tel.: +49 (0)51 1532 9123 E-mail: [email protected]
Fax: +49 (0)511 532 9029
E-mail: [email protected]
Geschützte Internetregistrierung: https://aml.mh-hannover.de/amlreg09/
International Registry AML Relapse 2009 / -June ’09 - 3 -
Table of Contents
Abbreviations ........................................................................................................................................ 5
Synopsis .................................................................................................................................... 6
Summary .................................................................................................................................... 7Reference List .......................................................................................................................................... 8
International Registry AML Relapse 2009 ............................................................................. 10Objectives .............................................................................................................................................. 10
Eligibility ................................................................................................................................................. 10
Requested data: ..................................................................................................................................... 10
Reference diagnostics ........................................................................................................................ 11
Material banking ................................................................................................................................. 11
Data management and registration........................................................................................................ 12
Data pooling ....................................................................................................................................... 12
Data Monitoring Committee (DMC)........................................................................................................ 12
Registration Procedure .......................................................................................................................... 12
Ethical considerations ............................................................................................................................ 13
Patient/parent information and informed consent .................................................................................. 14
Registration form .................................................................................................................................... 16
Datenweitergabe .................................................................................................................................... 17
Einwilligungserklärung zur Lagerung und Nutzung biologischen Materials........................................... 18
Recommendations for diagnostics and treatment .............................................................. 25Diagnostics............................................................................................................................................. 25
Clinical evaluation, laboratory tests and follow-up ............................................................................. 25
Criteria of response and other definitions .......................................................................................... 25
Therapy .................................................................................................................................................. 27
Schedule overview ............................................................................................................................. 27
Conditions to start treatment .................................................................................................................. 27
Contradiction for full-dose treatment .................................................................................................. 28
Background and introduction.............................................................................................................. 28
Stem cell transplantation (SCT) ............................................................................................................. 30
Conclusion .......................................................................................................................................... 31
Special measures for reinduction........................................................................................................... 32
REINDUCTION FLAG + DaunoXome® .................................................................................................. 33
2nd REINDUCTION FLAG ...................................................................................................................... 34
CONSOLIDATION - high intensity ......................................................................................................... 35
CONSOLIDATION - low intensity ....................................................................................................... 36
CNS PROPHYLAXIS AND TREATMENT ............................................................................................. 37
Prophylaxis: ........................................................................................................................................ 37
Treatment of CNS leukemia ............................................................................................................... 37
STEM CELL TRANSPLANTATION ....................................................................................................... 37
Overview drugs ...................................................................................................................................... 38
Cytarabine .......................................................................................................................................... 38
Fludarabine......................................................................................................................................... 38
Supportive Care ..................................................................................................................................... 40

International Registry AML Relapse 2009 / -June ’09 - 4 -
General measures .............................................................................................................................. 40
Hyperleukocytosis and metabolic derangement ................................................................................ 40
Prevention and treatment of infections ............................................................................................... 41
G-CSF ................................................................................................................................................ 42
Transfusion support ............................................................................................................................ 42
Cardiotoxicity monitoring .................................................................................................................... 44
Comments:Performance scales ............................................................................................................. 48
Performance scales ............................................................................................................................... 49
Lansky score: 0-16 years ................................................................................................................... 49
Karnofsky score: 16 years and older .................................................................................................. 49
International Registry AML Relapse 2009 / -June ’09 - 5 -
Abbreviations
AML acute myeloid leukemia
ara-CTP arabinosylcytosine 5’-triphosphate
CR complete remission
DNX DaunoXome®
FAB French-American-British classification
FLAG fludarabine, cytarabine and G-CSF
FS fractional shortening
HID haplo-identical donor
ITH intrathecally
IV intravenously
LP lumbar puncture
LV left ventricle
LVET left ventricular ejection time
MRD minimal residual disease
MSD matched sibling donor
MUD matched unrelated donor
NR non response
PR partial response
SC subcutaneously
SCT stem cell transplantation
SF see FS
UNL upper normal level
International Registry AML Relapse 2009 / -June '09
Wichtiger Hinweis!
Die im Register „International Registry Relapsed AML 2009“ beschriebene
Therapiemöglichkeit ist eine Empfehlung der internationalen AML-Rezidiv Studiengruppe
bzw. der AML-I-BFM Gruppe (Leiter Prof. Dr. G. J. Kaspers [Amsterdam] bzw. Dr. David
Webb [London]), basierend auf den Ergebnissen der vorherigen, abgeschlossenen Studien
zur Behandlung von Rezidiven der akuten myeloischen Leukämie (AML) bei Kindern und
Jugendlichen.
Die Durchführung dieser Therapie empfiehlt sich nur an erfahrenen kinderonkologischen
Zentren mit intensivmedizinischer Behandlungsmöglichkeit (Behandlungszentren mit >20
kinderonkologischen Neuerkrankungen pro Jahr, Erfahrungen mit Hyperleukozytose) und an
Zentren mit Erfahrung in der Behandlung von refraktärer und rezidivierter AML im Kindes-
und Jugendalter bzw. Knochenmarktransplantationszentren.
Gemäß der publizierten Ergebnisse und der eigenen Erfahrungen zum Einsatz von
liposomalem Daunorubicin, Fludarabin in Kombination mit Cytarabin und/oder Anthrazyklinen
besteht eine relevante Gefahr für akute, subakute und chronische opportunistische
Infektionen, was Erfahrung in der Diagnostik und Therapie dieser Komplikationen und eine
Langzeitnachbetreuung der Patienten an einem erfahrenen kinderonkologischen Zentrum
erfordert.
Die Erstellung der Therapieempfehlung erfolgte mit größter Sorgfalt, dennoch können
mögliche Fehler nicht vollständig ausgeschlossen werden. Fehler oder Unklarheiten zur
Protokolldurchführung bitten wir umgehend zu melden.
Hiermit wird darauf hingewiesen, dass die Leitung des Registers keine juristische
Verantwortung für mögliche, aus der Anwendung der Therapie resultierende Folgen
übernimmt und der jeweils behandelnde Arzt allein für die Therapie verantwortlich ist.
International Registry AML Relapse 2009 / -June ’09 - 6 -
Synopsis
COORDINATOR Dr. med. Dirk Reinhardt, MD, PhD Pediatric Hematology and Oncology Hannover Medical School Carl-Neuberg-Str.1, 30625 Hannover +495115326720 / FAX +495115329029
Gertjan J.L. Kaspers, MD PhD Department of Pediatric Hematology/Oncology VU medical center De Boelelaan 1117 NL-1081 HV Amsterdam The Netherlands. Phone: +31 – 20 444 2420 Fax: +31 – 20 444 2422 E-mail: [email protected]
located Hannover Medical School, Germany
Registry International Registry Relapsed AML 2009
Registry of relapsed and refractory acute myeloid leukemia (AML) in children and adolescents
CONDITION Relapsed or refractory AML in children and adolescants
OBJECTIVE(S) To register all children and adolescents with relapsed or refractory acute
myeloid leukemia
- incidence and frequency of relapsed and refractory AML
- background for clinical advisement and recommendation
- Data for biological studies concerning
o Diagnosis
o Prognosis
INTERVENTION (S) none
ELIGIBILTY Children and adolescents (age<18 years at diagnosis) with refractory AML or
relapse of AML
OUTCOME(S) Not applicable
TYPE registry
STATISTICAL ANALYSIS Descriptive statistics:
- Incidence of AML relapses
- Biological characteristics
- Prognostics factors
Rational Refractory and relapse AML is rare. The registration of all children and
adolescents with relapsed or refractory AML will assure profound expect advice
concerning diagnostics, prognostic factors, therapy, treatment response and
complications. Central reference diagnostics will improve the quality of diagnosis.
Biological research could be supported with patient’s material and correlated to
clinical course of disease.
SAMPLE SIZE 100 patients per year
DURATION The registry will be closed if any Phase III clinical trial will be open for this patient
group.
International Registry AML Relapse 2009 / -June ’09 - 7 -
Summary
Children and adolescents with relapsed or refractory AML still have an unfavorable prognosis.
Internationally several clinical trials confirmed the efficacy and feasibility of an combined chemotherapy
with anthracyclines and cytarabine (or derivates).
In postremission the need of an allogenic stem cell transplantation is generally accepted. Only in specific
cases (very late relapse and lack of matched donor, insufficient first line therapy) and autologous stem
cell transplantation or even chemotherapy only could be considered. Following prognostic factors of
relapsed AML have been identified:
Duration of first remission, cytogenetics and response to the first re-induction element (analyzed at day
28 by morphology).
In Germany, Austria and the Czech Republic since 1997 different combinations of anthracyclines and
cytarabine have been successfully studied. Both, liposomal daunorubicin and cytarabine (AML Rezidiv
97) and the idarubicin combined with fludarabine, cytarabine and G-SCF showed encouraging efficacy
and limited toxicity1-3. Comparable results have been reported by other groups in children and adults4-15.
The results were the basic for the international Relapsed AML 2001/01 trial. Although the preliminary
analysis of the randomised comparison of L-DNR-FLAG versus FLAG showed no significant advantage
of the overall survival, improved remission and less toxicity supported a benefit of L-DNR/FLAG16-20.
After finishing the international Relapsed AML 2001/01 trial, the patients should be registered to the
“International Registry Relapsed AML 2009”.
The aims are to evaluate the incidence and frequency of relapsed and refractory AML in children and
adolescents, assurance of substantial advisement for therapy, identification of biological and prognostic
factors and the support of associated research projects.
The expected number of patients will be between 25 and 35 (Germany, Austria and Czech Republic).
Zusammenfassung
Rezidivierte und refraktäre akute myeloische Leukämien (AML) bei Kindern und Jugendlichen sind
selten und haben eine ungünstige Prognose. In den letzten Jahren wurden verschiedene Kombinationen
von Chemotherapie in Therapieoptimierungsstudien getestet. Der Einsatz von Antracyclinen kombiniert
mit Cytarabin bzw. Cytarabinderivaten hat dabei in verschiedenen Studien bei Kindern und Jugendlichen
die besten Remissionsraten und Überlebenschancen ergeben. Allgemein akzeptiert ist die
Notwendigkeit der allogenen Stammzelltransplantation als Postremissiontherapie. Unter bestimmten
Umständen wie z.B. einem sehr späten Rezidiv und fehlendem gut passenden Spender kommen auch
autologe Stammzelltransplantation oder nur chemotherapeutischen Ansätze infrage.
Als prognostische Faktoren für ein Rezidiv der AML gelten: Dauer der 1. Remission; Zytogenetik und
insbesondere das Ansprechen auf die Reinduktionstherapie (Blasten % an Tag 28).
In Deutschland, Österreich und der Tschechischen Republik wurden seit 1997 verschiedene Ansätze
untersucht. Dieses waren einmal der Einsatz des liposomal formulierten Daunorubicin (DaunoXome, L-
DNR) in Kombination mit Cytarabin sowie Idarubicin mit Fludarabin, Cytarabin und G-CSF (FLAG) 1-3.
Ähnliche Ergebnisse wurden auch von anderen Gruppen bei Kindern und Erwachsenen berichtet 4-15.
Die ermutigenden Ergebnisse waren Grundlage der international AML Relapse 2001/01 Studie 16-20.
International Registry AML Relapse 2009 / -June ’09 - 8 -
Hier konnte bei einer großen Anzahl von Patienten die Effizienz und vertretbare Toxizität der
Kombination von L-DNR und FLAG dokumentiert werden. Obwohl in bezug auf das Gesamtüberleben
bei den vorläufigen Ergebnissen bislang keine signifikanter Vorteil bewiesen werden konnte, weisen
eine bessere Remissionsrate bei gleicher oder verminderter Toxizität auf einen eventuellen Vorteil des
Zusatzes von L-DNR im Vergleich zur Therapie nur mit FLAG hin.
Nach Abschluss der internationalen Rezidivstudie wird deshalb diese Kombination zur Behandlung von
Rezidiven bei Kindern und Jugendlichen empfohlen.
Gleichzeitig werden alle Rezidive und refraktären AML in dem Register Relapsed AML 2009 erfasst.
Ziele des Registers sind die Erfassung der Häufigkeit und Inzidenz der Rezidive, Sicherstellung der
umfassenden und fundierten Therapieberatung, Identifikation prognostischer Faktoren, Entwicklung
diagnostischer Methodik und die Unterstützung biologischer und klinischer Forschungsprojekte.
Die erwartete Patientenaufnahme in das Register beträgt pro Jahr 25 bis 35 Patienten (Deutschland,
Österreich, Tschechische Republik).
Reference List
(1) Fleischhack G, Hasan C, Graf N, Mann G, Bode U. IDA-FLAG (idarubicin, fludarabine, cytarabine, G-CSF), an
effective remission-induction therapy for poor-prognosis AML of childhood prior to allogeneic or autologous bone marrow
transplantation: experiences of a phase II trial. Br J Haematol. 1998;102:647-655.
(2) Fleischhack G, Graf N, Hasan C, Ackermann M, Breu H, Zernikow B, Bode U. [IDA-FLAG (idarubicin,
fludarabine, high dosage cytarabine and G-CSF)--an effective therapy regimen in treatment of recurrent acute myelocytic leukemia
in children and adolescents. Initial results of a pilot study]. Klin Padiatr. 1996;208:229-235.
(3) Reinhardt D, Hempel G, Fleischhack G, Schulz A, Boos J, Creutzig U. [Liposomal daunorubicine combined
with cytarabine in the treatment of relapsed/refractory acute myeloid leukemia in children]. Klin Padiatr. 2002;214:188-194.
(4) Yavuz S, Paydas S, Disel U, Sahin B. IDA-FLAG regimen for the therapy of primary refractory and relapse
acute leukemia: a single-center experience. Am J Ther. 2006;13:389-393.
(5) Viniou NA, Vassilakopoulos TP, Giakoumi X, Mantzouranis M, Pangalis GA. Ida-FLAG plus imatinib mesylate-
induced molecular remission in a patient with chemoresistant Ph1+ acute myeloid leukemia. Eur J Haematol. 2004;72:58-60.
(6) de la RJ, Regadera A, Martin G, Cervera J, Sanz G, Martinez J, Jarque I, Garcia I, Andreu R, Moscardo F,
Jimenez C, Molla S, Benlloch L, Sanz M. FLAG-IDA regimen (fludarabine, cytarabine, idarubicin and G-CSF) in the treatment of
patients with high-risk myeloid malignancies. Leuk Res. 2002;26:725-730.
(7) Luczynski W, Muszynska-Roslan K, Krawczuk-Rybak M, Kuzmicz M, Iwaszkiewicz-Pawlowska A, Kaliszewski
J. Results of IDA-FLAG programme in the treatment of recurrent acute myeloblastic leukaemia--preliminary report. Med Sci Monit.
2001;7:125-129.
(8) Steinmetz HT, Schulz A, Staib P, Scheid C, Glasmacher A, Neufang A, Franklin J, Tesch H, Diehl V, Dias WP.
Phase-II trial of idarubicin, fludarabine, cytosine arabinoside, and filgrastim (Ida-FLAG) for treatment of refractory, relapsed, and
secondary AML. Ann Hematol. 1999;78:418-425.
(9) Latagliata R, Breccia M, Fazi P, Iacobelli S, Martinelli G, Di Raimondo F, Sborgia M, Fabbiano F, Pirrotta MT,
Zaccaria A, Amadori S, Caramatti C, Falzetti F, Candoni A, Mattei D, Morselli M, Alimena G, Vignetti M, Baccarani M, Mandelli F.
Liposomal daunorubicin versus standard daunorubicin: long term follow-up of the GIMEMA GSI 103 AMLE randomized trial in
patients older than 60 years with acute myelogenous leukaemia. Br J Haematol. 2008;143:681-689.
(10) Camera A, Rinaldi CR, Palmieri S, Cantore N, Mele G, Mettivier V, Miraglia E, Mastrullo L, Grimaldi F, Luciano
L, Guerriero A, Rotoli B, Ferrara F. Sequential continuous infusion of fludarabine and cytarabine associated with liposomal
daunorubicin (DaunoXome) (FLAD) in primary refractory or relapsed adult acute myeloid leukemia patients. Ann Hematol.
2009;88:151-158.
(11) Fassas A, Anagnostopoulos A. The use of liposomal daunorubicin (DaunoXome) in acute myeloid leukemia.
Leuk Lymphoma. 2005;46:795-802.
(12) Clavio M, Venturino C, Pierri I, Garrone A, Miglino M, Canepa L, Balleari E, Balocco M, Michelis GL, Ballerini
F, Gobbi M. Combination of liposomal daunorubicin (DaunoXome), fludarabine, and cytarabine (FLAD) in patients with poor-risk
acute leukemia. Ann Hematol. 2004;83:696-703.
International Registry AML Relapse 2009 / -June ’09 - 9 -
(13) Russo D, Piccaluga PP, Michieli M, Michelutti T, Visani G, Gugliotta L, Bonini A, Pierri I, Gobbi M, Tiribelli M,
Fanin R, Piccolrovazzi S, Baccarani M. Liposomal daunorubicin (DaunoXome) for treatment of poor-risk acute leukemia. Ann
Hematol. 2002;81:462-466.
(14) Piccaluga PP, Visani G, Martinelli G, Isidori A, Malagola M, Rondoni M, Baccarani M, Tura S. Liposomal
daunorubicin (DaunoXome) for treatment of relapsed meningeal acute myeloid leukemia. Leukemia. 2002;16:1880-1881.
(15) Muggia FM. Liposomal encapsulated anthracyclines: new therapeutic horizons. Curr Oncol Rep. 2001;3:156-
162.
(16) Kaspers GJ, Zimmermann M, Fleischhack G, Tamminga R, Gibson B, Armendariz H et al. Relapsed Acute
Myeloid Leukemia in Children and Adolescents: Interim Results of the International Randomised Phase III Study Relapsed AML
2001/01. 5th Bi-annual Symposium on Childhood Leukemia, Noordwijkerhout, The Netherlands: 2006.
(17) Kaspers GJ, Zimmerman M, Fleischhack G et al. Relapsed Acute Myeloid Leukemia in Children and
Adolescents: Interim Report of the International Randomised Phase III Study Relapsed AML 2001/01 [abstract]. Blood.
2006;108:570a.
(18) Kaspers GJ, Zimmermann M, Reinhardt D et al. Prognostic Significance of Early Treatment Response in
Pediatric Relapsed Acute Myeloid Leukemia: Results from the International Study Relapsed AML 2001/01 [abstract]. Blood.
2007;110:546a.
(19) Kaspers GJL, Zimmermann M, Reinhardt D et al. Clinical Relevance of Early Treatment Response in Pediatric
Relapsed Acute Myeloid Leukemia (AML): Study Relapsed AML 2001/01 [abstract]. Ann Hematol. 2008;87:S2.
(20) Kaspers GJL, Zimmermann M, Reinhardt D et al. Prognostic Significance of Time to Relapse in Pediatric AML:
Results from the International Randomised Phase III Study Relapsed AML 2001/01 [abstract]. Blood. 2008;112:1022-1023.

International Registry AML Relapse 2009 / -June ’09 - 10 -
International Registry AML Relapse 2009
Newly diagnosed acute myeloid leukemia (AML) is a rare disease in children and adolescents. The
prognosis has improved using intensive chemotherapy with or without stem cell transplantation.
However, 5-10% of patients do not achieve first complete remission (CR) due to resistant disease
(primary refractory AML), and 30-50% of CR patients relapse. Primary refractory AML and relapsed AML
have a poor prognosis, with an overall survival of less than 25%. For first relapse disease, the prognosis
mainly depends on the time of relapse. If early (duration of 1st remission less than 1 year) the 2nd CR
rate is about 50%, and overall survival 10% or less. If late, the second CR rate is 80-90% and the overall
survival up to 40%. Multiple relapsed AML has an even worse prognosis. Several treatment schedules
have been studied recently, and progress seems feasible.
Within the German BFM group between 1997 and 2001 two clinical trials demonstrated the feasibility
and efficacy of combinations of anthracyclines (idarubicine / liposomal daunorubicin) and
cytarabine/fludarabine in childhood relapsed AML. The encouraging results were the fundament of the
International Relapsed AML 2001/01 Study, recruiting more than 500 patients (2001 to 2009).
As the Relapsed AML 2001/01 was finished in 3/2009, there is still a need to register all children and
adolescents with refractory or relapsed AML. This should allow evaluating the incidence, to identify new
diagnostic procedures and prognostics factors, improve diagnostic security by central reference
diagnostics, and assure qualified expert advice concerning prognosis, therapy, response and
complications. In addition, central material banking will supply selected research projects with patients’
material and enable correlating biological results with clinical data.
Objectives
To register all children and adolescents with relapsed or refractory acute myeloid leukemia
- incidence and frequency of relapsed and refractory AML
- basis for profound clinical advisement and recommendation
- Data for biological studies concerning
o Diagnosis
o Prognosis
Eligibility
All children and adolescents with relapsed or refractory AML younger than 18 years at diagnosis
Requested data:
Patient´s characteristics
Biological and Features of the AML
Registration form

Reference diagnostics
- central morphology
- central immunophenotyping
- cytogenetics / molecular genetics
Material banking
Material which is not required for diagnostics will be stored according to the following algorithm.
At diagnosis:
Basic Diagnostics
Morphology 6 unstained smears BM/PB
Immunophenotyping 11x 70µl heparinized BM / PB
Cytogenetic 4 ml heparinized BM / PB
Molecular genetics (Fusion genes, FLT3 ITD, NPM1) 5µg DNA
Mononuclear cells (ficoll) 1 to5*106cells (back up) ( ~2 5ml)
Research:
Isolation of leukemic blasts (sorting); purity > 95% X ml available
Non leukemic cells storage
Leukemic blasts 5*106cells per ( ~10ml)
DNA 10µg per ( ~ 1ml)
RNA 5µg per ( ~ 2ml)
Leukemic stem cells (if possible: sorting strategy pending) 0.01 0.3%
DNA
RNA
Follow up (time point 1 to 6):
Morphology unstained smears BM/PB
Immunophenotyping 5x 100µl heparinized BM / PB
Mononuclear cells (ficoll) 1 *106cells (back up) ( ~2ml)
DNA 5µg per ( ~ 1ml)
RNA 1 to5µg per ( ~ 2ml)
The material is available for research projects according the priority list of the registry committee.
The priority list is based on the reviews of the international reviewers and the feasibility to provide
adequate material.
International Registry AML Relapse 2009 / -June ’09 - 11 -
International Registry AML Relapse 2009 / -June ’09 - 12 -
Data management and registration
Each participating group will refer to their clinical contact person and to the usual network of clinical
centers, data center and experts (statistician, laboratories, etc) for the application of this registry. The
international coordinator will act as a co-ordination unit for the monitoring and exchange of information
and for the pooling of the data.
The set of data to be collected and pooled by the participants. Each group may:
Toxicity collection after each course should be done using the common form
Centralize the forms for quality checks in its own data center, according to the approach routinely
used in the group.
decide whether to input data in their own data base and send data as a file for pooling (at least every
6 months) or to send each checked and corrected forms to the operating center in Hannover
In summary, the major requirements that each group will have to ask to each of its clinical oncology
centers are:
1. To register at the data center each patient with relapsed or refractory AML. Registration should be
done as soon as possible after diagnosis; entry on this registry can only be done with informed
consent.
2. To send at least every 6 months the forms on diagnosis, response, treatment, toxicity and events as
soon as they can be completed, to the central data office (see addresses).
Data pooling
A common coding system and format has been made, for use by the data managers and/or
statisticians, in order to minimize mistakes in data exchange. This coding system is defined for the
purpose of data pooling only: it is required that a data set including each registered patient is prepared
with this format by the data managers and/or statisticians of each group. The data have to be sent every
6 months for pooling to the operating center, in a file structured according to a file that will be forwarded
separately to the data managers/statisticians, or on forms. The operating center, in collaboration with the
clinical contact person and the data manager/statistician of each group, pools the data and circulates a
report on these data.
Data Monitoring Committee (DMC)
Such a committee (two clinicians and one statistician) will be installed. Members of the DMC are
experienced researchers not involved in the trial who will be responsible for providing the principal
investigators with guidance on the trial conduction and, in case of problems, on whether the trial should
be stopped, modified or continued.
Registration Procedure
There will be a continuous possibility (7 days/week, 24 hours/day) of computerized registration. The
local/national representatives for data management will be instructed by the central data office (Martin
Zimmermann) about the procedure. After that, these local data managers will distribute login names and
passwords to all participating centers of their group. Then, each individual center will have the possibility
International Registry AML Relapse 2009 / -June ’09 - 13 -
to register a new patient using the internet. Alternatively, the registration can be done centrally by the
local group/national data manager, or the central data office in Hannover.
There will be a back-up procedure if the internet system is not available. In these circumstances, please
consult your local representative for data management, or if not available the central data office for this
study in Hannover.
Publication and other policies
Authors on abstracts and manuscripts:
- Final main publications to be written by international coordinators
- Members of the writing committee will be included
- Clinical contact persons of each of the participating groups, if a total of at least 2 patients has been
included from that group in the International Registry Relapsed AML 2009, will be included
- International statistician
- Manuscripts concerning add-on studies only will include those who made a significant contribution to
that particular study, according to international guidelines for authorship
Other guidelines:
- Participating groups are obliged to send all required patient data every 6 months to the central data
office in Hannover. Groups who fail to do so will loose their status as collaborating group.
Ethical considerations
All patients with a refractory or relapsed AML should be registered. Due to the rareness of the disease,
sufficient data to analyse incidence and prognostic factors could only be generated in a collaborative
European registry. Diagnostics will be improved by a central reference diagnostics. In addition, all
patients will benefit from an expect advice based on the response data of the treated patients, potential
side effects or complications.
Coordinated add-on studies, using left material and correlated to the clinical course of disease will
generate new insights to leukemogenesis, new diagnostics or prognostic factors.
The treatment recommendation is based on several clinical trials in adults and children and could be
state as “best available option”.
International Registry AML Relapse 2009 / -June ’09 - 14a -
Patient/parent information and informed consent
Information Sheets
Dear Parent / Guardian,
We would like to invite your child to be registered to an International Registry Relapsed AML 2009.
Before you decide whether you would like your child to take part it is important for you to understand
why the registry is being done and what it will involve. Please take time to read the following information
carefully and discuss it with others if you wish. Ask us if there is anything that is not clear or if you would
like more information. Take time to decide whether or not you wish your child to take part.
1. What is the purpose of the registry? AML relapses in children or adolescents are rare. To learn more about incidence, prognostics
factors or new diagnostic markers, an European collaboration is necessary. Central reference
diagnostics will improve the diagnostically security. The analysis of given treatment, response, side
effects and complication from all children and adolescents enables a profound expert advice in all
patients, especially in case or rare events.
2. Which kind of data will be transferred? The registry aimed to gather and analyze data on:
patients characteristics / symptoms
features of the leukemic blasts
treatment response
side effects
severe complications
3. Are there any risks? There are no risks expected
4. Are there any benefits? The individual patient will benefit from improved diagnostics and the opportunity of qualified advice
5. What will happen, if new knowledge is available? If a new clinical trial will be started, the patients are eligible.
6. Will taking part in this study be kept confidential? All data will be handled confidential
Thank you for reading this information
International Registry AML Relapse 2009 / June 2009 - 14b -
Patienteninformation
International Registry Relapsed AML 2009
Name, Vorname des Patienten:................................................................................Geb.-Datum:...............................................................................................................Sorgeberechtigter/Gesprächspartner:.........................................................................................................................................................................................................Ärztin/Arzt....................................................................................................................
Lieber Patient, liebe Eltern,bei Ihnen bzw. Ihrem Kind wurde ein Rückfall der akuten myeloischen Leukämie (AML) festgestellt. Auch wenn Sie bzw. Ihr Kind bereits in der vorangegangenen Therapie viele in der Behandlung der AML wirksame zytostatische Medikamente erhalten haben, gibt es auch beim Rückfall der Erkrankung (Rezidiv) erneut die Möglichkeit einer Behandlung. Die Erfahrungen in der Behandlung von Rückfällen der akuten myeloischen Leukämie (AML) im Kindes- und Jugendalter sind begrenzt. Es liegen jedoch Ergebnisse mehrerer Studien in Deutschland, Europa und den USA vor. In diesen Untersuchungen konnte bei mehr als 50% der behandelten Kinder eine erneute Remission, d.h. das erneute Verschwinden der Leukämiezellen erreicht werden. Danach sollte sich dann eine Knochenmarktransplantation anschließen, um ein langfristiges Überleben zu erreichen.
Durch diese Maßnahmen überlebten insgesamt etwa ein Drittel der Patienten die nächsten 5 Jahre, ohne dass es Hinweise für einen erneuten Rückfall gegeben hat. Allerdings sind die Chancen in Abhängigkeit von einer Reihe von Risikofaktoren unterschiedlich (Dauer zwischen der Ersterkrankung und dem Rückfall, genetische Eigenschaften der AML, Ansprechen auf die erneute Therapie).
Aufgrund der bisherigen Erfahrungen aus nationalen und internationalen Studien (Int. Relapsed AML 2001/01) wird eine intensive Chemotherapie mit der Kombination von liposomalem Daunorubicin (L-DNR), Fludarabin, Cytarabin und der Gabe des Wachstumsfaktors G-CSF empfohlen. Wenn eine erneute Remission erreicht wird, sollte eine Stammzelltransplantation angeschlossen werden, bevorzugt von einem guten passend Geschwisterkind oder einem Fremdspender.
Das liposomale Daunorubicin ist ein Anthracyclin, das mit einer „Hülle aus Fetten verpackt“ ist. Hierdurch sollen mögliche Schädigungen des Herzens, die bei der Behandlung mit hohen Dosierungen auftreten könnten, vermindert werden
Erläuterungen zur Therapie und den NebenwirkungenDas "L-DNR/FLAG“ oder „FLAG"-Schema sind Therapien, die über einen Zeitraum von 4 Tagen verabreicht werden und sich aus den drei Medikamenten (Zytostatika) Daunorubicin, Cytarabin und Fludarabin bzw. Cytarabin und Fludarabin zusammensetzen. Diese Medikamente greifen in unterschiedlicher Weise die sich teilenden Leukämiezellen an und bewirken so deren Vernichtung. Cytarabin ist Ihnen möglicherweise bereits bekannt, da Sie bzw. Ihr Kind es bereits in der Vorbehandlung der AML in anderer Kombination erhalten haben. Die Wirksamkeit ist in vielen nationalen und internationalen AML-Studien des Kindes- und Erwachsenenalters belegt. Das Medikament Fludarabin ist bisher nur in begrenztem Umfang bei Kindern, aber umfangreicher bei erwachsenen Patienten erfolgreich in der AML-Rezidivbehandlung eingesetzt worden. Zusätzlich zu diesen Medikamenten wird bereits vor Start der Therapie und ab Tag 15 täglich bis zur Blutbilderholung ein Wachstumsfaktor für weiße Zellen (Leukozyten) eingesetzt, der sogenannte „Granulozyten-Kolonien stimulierende Faktor“ (G-CSF). Dieser Faktor soll
International Registry AML Relapse 2009 / June 2009 - 14b -
einerseits zu Beginn der Therapie mehr Leukämiezellen aus der ruhenden Phase in die Teilungsphase bringen, um so die Wirksamkeit der Behandlung zu verbessern.
In der Erstbehandlung der AML haben Sie bzw. Ihr Kind bereits die sogenannten Anthrazykline erhalten. Diese Medikamente können bei einigen Patienten möglicherweise Schädigungen des Herzen verursachen. Das Risiko, dass eine solche Schädigung auftritt, hängt direkt mit der gegebenen Gesamtmenge dieser Medikamente zusammen. Andererseits sind die Anthrazykline gerade gegen Leukämiezellen der AML sehr wirksam. Seit einiger Zeit gibt es das Anthrazyklin „Daunorubicin“ in einer Fetthülle (so genannten Liposomen) verkapselt, das auch in dieser Form als so genanntes "liposomales Daunorubicin" (L-DNR) wirksam ist. Untersuchungen ergaben Hinweise, dass bei Verwendung des Medikaments in dieser Form die Schädigung des Herzens seltener ist.
Bei Ansprechen auf diese Therapie (Kontrollen erfolgen wie in der Ersttherapie durch Knochenmarkpunktionen und ggf. Liquorpunktionen) wird der behandelnder Arzt Sie über weitere Therapiemöglichkeiten informieren. Im Rahmen des Registers empfehlen wir, dass nach erreichen einer Remission (Verschwinden der sichtbaren Leukämiezellen) eine Knochenmarktransplantation/ Stammzelltransplantation durchgeführt wird. Ziel der Transplantation ist es, das mit dem "DNX-FLAG / FLAG"-Schema erreichte Ergebnis zu festigen und die Langzeitprognose zu verbessern. In Abhängigkeit vom zeitlichen Ablauf ist eine Behandlung mit Cytarabin und Thioguanin zur Überbrückung vorgesehen. Sollte eine Knochenmarktransplantation erst nach einem längeren Zeitraum möglich sein, so wird die intensivere Behandlung mit Cytarabin und Etoposid empfohlen. Bei der Knochenmarktransplantation kommt in erster Linie ein Familienangehöriger (Geschwister), infrage, der/die weitgehend übereinstimmende Gewebemerkmale aufweist (HLA-identisch). Sollte es in der Familie keinen Spender geben, wird ein fremder Spender gesucht, der gleiche Gewebemerkmale wie Ihr Kind aufweist (HLA identisch).
Nebenwirkungen: Wie Ihnen bereits aus den vorangegangenen Behandlungen bekannt ist, greifen die zytostatischen Medikamente leider auch alle gesunden, schnell wachsenden Zellen in unserem Organismus an. Kurzzeitige Nebenwirkungen neben Übelkeit, Erbrechen, Fieber und Kopfschmerzen können daher vorübergehender Haarausfall, Entzündungen der Darm- und Mundschleimhaut sowie Blutbildveränderungen sein. Die Blutbildveränderungen können dabei die bereits durch die Leukämie bedingten Veränderungen wie Verminderung der roten Blutzellen, der weißen Blutzellen und der Blutplättchen noch verstärken, wodurch eine hohe Blutungsgefahr und Infektionsgefahr besteht. Bluttransfusionen sind daher unvermeidbar. Bei Fieber sind intravenöse Antibiotika-Gaben erforderlich. Des Weiteren kann es durch diese Therapie oder durch infektiöse Komplikationen auch zu Organschäden, insbesondere zur Schädigung des Herzen, seltener der Lunge, Leber oder Niere, oder zu neurologischen Störungen kommen. Langfristig können das Wachstum und die Fortpflanzungsfähigkeit beeinträchtigt sein, und es besteht ein höheres Risiko für das spätere Entstehen einer zweiten bösartigen Erkrankung. Schwerwiegende Infektionen oder Organschädigungen können auch zum Tod führen.
Die Durchführung der Therapie ist nur unter stationären Bedingungen möglich. Da die zu erwartenden Blutbildveränderungen relativ lange anhalten und die damit verbundene Gefahr von Komplikationen durch Blutungen oder Infektionen hoch ist, ist in der Regel auch für die weitere Behandlung bis zur Blutbilderholung ein Krankenhausaufenthalt erforderlich.
Wissenschaftliche Begleituntersuchungen Parallel zur Durchführung dieser Therapie sind wissenschaftliche Begleituntersuchungen zur Untersuchung der Biologie und des Verhaltens der Leukämiezellen im Blut und Knochenmark (Untersuchungen zur Charakterisierung der Leukämiezellen / Untersuchungen zur minimalen Resterkrankung [(MRD]) wie in der Erstbehandlung der AML vorgesehen. Diese erfolgen parallel zu anderen Routineuntersuchungen und bedeuten keine zusätzlichen Blut- oder Knochenmarkentnahmen. Diese Untersuchungen können insbesondere bei Optimierungen der Therapie zukünftiger Patienten behilflich sein (siehe Einwilligung Materialübertragung).
International Registry AML Relapse 2009 / June 2009 - 14b -
Weitergabe von patientenbezogenen Daten Im Rahmen des Registers ist die Erfassung der patientenbezogenen Daten (Name, Vorname, Geb.-Datum, Diagnose, Befunde, Therapie, Verlauf) zur medizinischen Dokumentation vorgesehen. Dadurch wird einerseits eine Zusammenarbeit zwischen verschiedenen Kliniken möglich und andererseits ist es die Voraussetzung für die genauere Diagnosestellung und die Überwachung der Therapie.
Alle Personen, die Daten erfassen oder Einblick in die gespeicherten Daten haben, unterliegen der Schweigepflicht und sind zur Wahrung des Datengeheimnisses entsprechend dem §40 des Bundesdatenschutzgesetzes verpflichtet. Alle erhobenen oder gespeicherten personenbezogenen Daten werden ausschließlich zum Zwecke der wissenschaftlichen Forschung verarbeitet und genutzt und anonymisiert, sobald das in der Auswertung möglich ist. Die personenbezogenen Daten werden an folgende Zentren übermittelt bzw. dürfen eingesehen werden durch:
Registerleitung:
Prof. Dr. med. Dirk Reinhardt AML-BFM Studienleitung Medizinische Hochschule Hannover Pädiatrische Hämatologie und Onkologie Carl-Neuberg-Str. 1 30625 Hannover
(Form to be on Institution headed paper)
Addressogram:
PARENT/CHILD CONSENT FORM
(Version No., Date)
Title: International Relapsed AML 2009 Registry
Name of Local Researcher: Please initial boxes
1. I confirm that I have read and understood the information sheet(s),
and have had the opportunity to ask questions and had satisfactory
answers to them.
2. I understand that my child’s participation is voluntary and that I am free
to withdraw at any time, without giving any reason, without his/her medical care
or legal rights being affected.
3. I understand that information from my child’s medical notes may be looked at
and information passed on to responsible individuals from cancer research bodies,
where it is relevant to research, to the national registration bodies and to regulatory
authorities where it is relevant to my child’s participation in research.
Relevant information will be collected and held securely and kept confidential.
4. I agree for my child’s additional tissue to be collected, stored and used for
ethically-approved research.
5. I agree for my child to be registered in the
International Relapsed AML 2009 Registry
Name of patient
Name of parent/guardian Date Signature
Name of parent/guardian Date Signature
Researcher Date Signature
International Registry AML Relapse 2009 / -June ’09 - 15 -
Registration form
ONLY TO BE USED IF THE INTERNET PROCEDURE IS NOT AVAILABLE
Whenever possible, please use the internet for registration:
https://aml.mh-hannover.de/amlreg09/
To: Local Data Office for the International Registry Relapsed AML 2009
FAX nr: E-mail:
or:
To Int. Registry Relapsed AML 2009
Pediatric Hematology and Oncology
Hannover Medical School
Carl-Neuberg-Str. 1
30625 Hannover, Germany
FAX +49 511 532 9029 Tel +49 511 532 9123
I declare that the patient I will include is eligible for the Registry Relapsed AML 2009 for relapsed or
refractory AML. I have obtained formal written informed consent, which I will forward soon.
Treating Pediatric Oncologist:
Name:
Center:
Phone: Fax:
E-mail:
Patient data: a) primary refractory disease
(please b) refractory to other reinduction protocol after relapse
encircle) b) first relapse 1) early 2) late
c) subsequent relapse
Initials:
Date of birth:
PLEASE CONTACT YOUR LOCAL OR THE INTERNATIONAL DATA OFFICE FOR
REGISTRATION IN CASE THE INTERNET PROCEDURE IS NOT AVAILABLE
International Registry AML Relapse 2009 / -June ’09 - 16 -
International Registry AML Relapse 2009 / -June ’09 - 17 -
Datenweitergabe
Einwilligungserklärung zur Weitergabe und Verarbeitung der Patientendaten
im Rahmen des Registers “AML Rezidiv 2009” / “Registry Relapsed AML 2009”
Ich erkläre mich damit einverstanden, dass personenbezogenen Daten (Name, Geburtsdatum, Wohnort,
Diagnose mit Befunderhebung, Verlauf usw.) die meines Sohnes/meiner Tochter
....................................................................................................................................................
Name, Vorname Geb.-Datum
verarbeitet werden (Speicherung, Übermittlung, Veränderung, Löschen). Das Verarbeiten der Daten
dient der medizinischen Dokumentation im Rahmen der Zusammenarbeit mehrerer Kliniken um eine
bessere Erarbeitung der Diagnosen und eine Überwachung der Therapie in den einzelnen Kliniken zu
gewährleisten. Diese Dokumentation ist für eine Bewertung des Behandlungserfolgs im Rahmen desRegisters unerlässlich. Die Daten werden an folgendes Zentrum übermittelt
Abteilung für Hämatologie und Onkologie der Medizinische Hochschule Hannover, Carl-Neuberg-Str. 1,
30625 Hannover (= Prof. Dr. Reinhardt, Leitung des Int. Registers für AML-Rezidive 2009).
Alle Personen, die Einblick in die gespeicherten Daten haben, sind zur Wahrung des
Datengeheimnisses verpflichtet. Sie werden um Ihr Einverständnis zur Verarbeitung dieser Daten
gebeten.
Datum: -- / -- /----
_______________________________ _________________________________
Sorgeberechtigte/r Sorgeberechtigte/r
Gesprächsführende/r Ärztin/Arzt: ...............................................................................
Datum /Unterschrift
Zeugin/Zeuge: .............................................................................................................
Datum / Unterschrift
International Registry AML Relapse 2009 / -June ’09 - 18 -
Material
Einwilligungserklärung zur Lagerung und Nutzung biologischen Materials
Bei den notwendigen Untersuchungen bei Diagnose und im Verlauf der Behandlung (Knochenmark/
Blutentnahmen) können von den entnommenen Material Restmengen übrig bleiben, die nicht mehr für
die Diagnosestellung oder Verlaufskontrolle erforderlich sind. Diese Leukämiezellen/Blutzellen meines
Kindes können zur Erforschung der akuten myeloischen Leukämie in ihren molekularen, genetischen,
immunologischen und anderen, mit der Krankheit direkt verbundenen Merkmalen, untersucht und
gegebenenfalls für die Entwicklung neuer Behandlungsverfahren eingesetzt werden.
Die Entnahme des Blutes/Knochenmarks ist nicht mit zusätzlichen Schmerzen oder
Risiken verbunden, sie erfolgt im Rahmen der notwendigen Blut- oder Knochenmarkentnahme bei
Diagnosestellung oder im Verlauf.
Auf diese Weise sollen die Diagnosestellung sicherer gemacht werden, das biologische Verständnis der
Erkrankung verbessert und neue therapeutische Ansätze gefunden werden.
Für Studien, die eine zusätzliche Probenentnahme (Anzahl/ Menge) erfordern, sind gesonderte
Einwilligungen erforderlich.
Die Verwendung des Materials kann nur nach Beschluss einer wissenschaftlichen Kommission(1)
erfolgen.
Eine kommerzielle Nutzung des Materials wird ausgeschlossen.
Die Lagerung des Materials erfolgt in den Referenzlaboren der AML-BFM Studiengruppe.
Medizinische Hochschule Hannover; Pädiatrische Hämatologie/Onkologie (Prof. Dr. Reinhardt)
Ich lehne die Weiterverwendung von gewonnenen Materialien für Forschungszwecke ab
Ich stimme der Verwendung in
(1) anonymisierter 5
(2) pseudonymisierter 1 oder (3) nicht anonymisierter Form für konkrete Studienfragen zu.
In den Fällen (2) und (3) wird die Verwendung
für alle Studienmöglichkeiten erlaubt für alle Studien erlaubt, die im Kontext der Fragestellung stehen, für die ursprünglich das
Material gespendet wurde.
eine Kontaktaufnahme für die Zustimmung zur Verwendung in weiteren Studien erlaubt. eine Kontaktaufnahme für die Zustimmung zur Verwendung in weiteren Studien nicht erlaubt.
1Bei der Pseudonymisierung werden die Angaben, die die Identifikation des Patienten ermöglichen (Name, Geburtsdatum,
Herkunft) durch einen Code ersetzt, der ausschließlich von der Studienleitung entschlüsselt werden kann. Dadurch haben zum
einen die beteiligten Forschungsgruppen keine Möglichkeit, einen Patienten zu identifizieren, in dringenden Fällen (z.B. wenn ein
Forschungsergebnis direkt dem individuellen Patienten nützen könnte) kann aber die Studienleitung den Patienten identifizieren.
Bei der Anonymisierung ist keine Rückverfolgung oder Identifikation des Patienten möglich.
International Registry AML Relapse 2009 / -June ’09 - 19 -
Übereignung
Ich übereigne die meinem Kind entnommenen Blut- bzw. Gewebeproben hiermit an die oben genannte
Institution bzw. Person.
Unentgeltlichkeit
Ich bin mir bewusst, dass ich/mein Kind für die Spende der Blut- bzw. Gewebeprobe kein Entgelt
erhalte/erhält. Ich bin mir bewusst, keinerlei Ansprüche auf Vergütung, Tantieme oder sonstige
Beteiligung an finanziellen Vorteilen und Gewinnen zu haben, die möglicherweise auf der Basis der
Forschung mit der Blut- bzw. Gewebeprobe meines Kindes erlangt werden.
Widerruf der Zustimmung zur Probenverwendung
Ich weiß, dass ich meine Zustimmung zur Verwendung der Blut- bzw. Gewebeprobe meines Kindes
jederzeit und ohne Angabe von Gründen gegenüber der oben genannten Institution / Person widerrufen
kann und dass dies keinen Einfluss auf etwaige weitere ärztliche Behandlung meines Kindes hat.
Im Falle des Widerrufs bin ich damit einverstanden, dass die Blut- bzw. Gewebeprobe zu
Kontrollzwecken weiter aufbewahrt wird. Ich habe das Recht, deren Vernichtung zu verlangen, sofern
gesetzliche Bestimmungen der Vernichtung nicht entgegenstehen.
Ich bin mir bewußt, dass eine Vernichtung der Blut- bzw. Gewebeprobe auf meinen Wunsch nicht
möglich ist, wenn sie anonymisiert aufbewahrt wird.
Ort, Datum ................., ...............................
Unterschriften
...................................... .........................................
Sorgeberechtigte/Mutter Sorgeberechtigter/Vater
...................................... ..........................................
Patient/in zuständiger Arzt/Ärztin
(1) Kommission: Von dem Beratungsgremium des Registers Int. AML-Relapse 2009 werden 3-5
Wissenschaftler (z. Zt. Prof. Dr. Serve, Frankfurt, Prof. S. Izraeli, Tel Aviv, Prof. P. Vyas, Oxford) gewählt, die die
Qualität wissenschaftlicher Projekte und die Antragsteller prüfen und begutachten. Das
Beratungsgremium legt dann eine Prioritätenliste für die Weitergabe von Material fest.
International Registry AML Relapse 2009 / -June ’09 - 20 -
Please fax or mail to the appropriate coordination office! Or
+49 511 532 9029
International Registry Relapsed AML 2009: Registration
Identification number : |___________________________________________|
Surname / Initials: |___________________________________________|
Date of Birth |__|__|__|__|__|__| Gender |__| male |__| female
dd/mm/yr
Enters registry: |__| no |__| yes Informed consent: |__| no |__| yes
Date of initial diagnosis: |__|__|__|__|__|__| Date of relapse: |__|__|__|__|__|__|
dd/mm/yy dd/mm/yy
Number of relapse: |__| first |__| second |__| third or more
Resistant disease: |__| at initial diagnosis |__| at 1st relapse |__| at 2nd relapse
FAB type at initial diagnosis: _____ Auer rods |__| no |__| yes M4 eo |__| no |__| yes
Cytogenetics at initial diagnosis:
|__| no result
|__| examined, no result
|__| not examined
|__| no data
|__| normal karyotype
|__| t(9;22), Philad.-Chrom.
|__| 11q23 ( t(4;11),t(9;11), etc)
|__| t(1;19)
|__| t(4;11)
|__| t(8;14) / der (8q24)
|__| 14q11-aberrations
|__| del (6q)
|__| der (9p)
|__| der (12p)
|__| >50 (hyperdiploid)
|__| t(8;21)
|__| t(15;17)
|__| inv(16)
|__| t(9;11)
|__| t(6;9)
|__| der(3q)
|__| +4
|__| +8
|__| +9
|__| -5/5q-
|__| -7/7q-
|__| missing X-
chromosome
|__| +12
|__| 17q
|__| t(1;22)
|__| other aberrations
Molecular aberration (specify):____ (e.g. AML1/ETO etc) Results neg |__|pos. |__|
Liver enlargement: |__| no |__| yes ______ cm below costal margin in MCL
Spleen enlargement: |__| no |__| yes ______ cm below costal margin in MCL
Leukocytes : |__| |__|__|__| |__|__|__| x 109/l Platelets |__| |__|__|__| |__|__|__| x 109/l
Blasts % peripheral blood: |__|__|__| Blasts % BM: |__|__|__| LDH (U/l): |__|__|__|__|__|
CNS disease at initial diagnosis
|__| no |__| yes, blasts in the spinal fluid Cells in the spinal fluid at day 0: |_|_|_|/mm³
|__| yes, with symptoms (white blood cells)
(cranial nerve dysfunction, CNS mass, retinal infiltration, etc.)
Artificial contamination of spinal fluid with blood: |__| no |__| yes
International Registry AML Relapse 2009 / -June ’09 - 21 -
Pat. ID ____________________ International Registry Relapsed AML 2009
Data at Relapse - investigations
FAB type: __________ Auer rods |__| no |__| yes M4 Eo |__| no |__| yes
Cytogenetics at relapse:
|__| no result
|__| examined, no result
|__| not examined
|__| no data
|__| normal karyotype
|__| t(9;22), Philad.-Chrom.
|__| 11q23 ( t(4;11),t(9;11), etc)
|__| t(1;19)
|__| t(4;11)
|__| t(8;14) / der (8q24)
|__| 14q11-aberrations
|__| del (6q)
|__| der (9p)
|__| der (12p)
|__| >50 (hyperdiploid)
|__| t(8;21)
|__| t(15;17)
|__| inv(16)
|__| t(9;11)
|__| t(6;9)
|__| der(3q)
|__| +4
|__| +8
|__| +9
|__| -5/5q-
|__| -7/7q-
|__| missing X-chromosome
|__| +12
|__| 17q
|__| t(1;22)
|__| other aberrations
DATA AT RELAPSE, continued
Molecular aberration:________ (e.g. AML1/ETO, CBF/MYH11, MLL/AF9)
Results: |__| neg |__| pos
Bone marrow involv. |__| no |__| yes CNS involvement |__| no |__| yes
Gonadal involv. |__| no |__| yes Other localisations |__| no |__| yes
Liver enlargement: |__| no |__| yes ______ cm below costal margin in MCL
Spleen enlargement: |__| no |__| yes ______ cm below costal margin in MCL
Leukocytes : |__| |__|__|__| |__|__|__| x 109/l Platelets: |__| |__|__|__| |__|__|__| x 109/l
Blast % peripheral blood: |__|__|__| Blast % BM: |__|__|__| LDH (U/l): |__|__|__|__|__|__|
CNS disease at relapse:
|__| no |__| yes, blasts in the spinal fluid Cells in the spinal fluid at day 0: |_|_|_|/mm³
_| yes, with symptoms (white blood cells)
(cranial nerve dysfunction, CNS mass, retinal infiltration, etc)
Artificial contamination of spinal fluid with blood: |__| no |__| yes Weight [kg] |__|__| Height [cm] |__|__|__| Information submitted by:
Signature:_____________________________________ Date: __________________________
Tel/FAX no.: _____________________________
International Registry Relapsed AML 2009
Acute events
To: International Data Office
FAX: +49 – 511 532 9029
E-mail: [email protected]
And to: Local Data Office of the Own Group
FAX:
E-mail:
Date:
This is to inform you that we have observed a serious adverse event in a patient with relapsed or
refractory AML.
Identification number : _____________________|
Surname / Initials: ________________________|
Date of Birth |__|__|__|__|__|__| Gender |__| male |__| female
dd/mm/yr
Reporting pediatric oncologist/treating physician:
Name:
Center:
Phone:
Fax:
E-mail:
Please indicate:
- death Y/N
- life-threatening Y/N
- permanently disabling Y/N
Comments:
International Registry AML Relapse 2009 / June ’09
Prof. Dr. D. Reinhardt
Pediatric Hematological laboratory (K10)
Hannover Medical School
Carl-Neuberg-Str. 1
Tel.: +49/ 511/ 532 9019 30625 Hannover
fax: +49/ 511/ 532 9029 Germany
requested
Morphology
Immunophenotyping
Cytogenetics1 / Molecular genetics
Hospital: Patient: (label)
Address: ........................................... Name: .....................................
……………........................................ Prename: ................................
……………........................................ date of birth: ......../........../...........
Telephone: (.................)....................
Diagnosis: ................................(FAB)..... Date:......./......../................
Relapse: � yes Refractory: � yes Secondary malignancy: � yes
Cytogenetics at de-novo AML: ______________
Immunological data: .........................................................(immunophenotype, if available)
Last treatment block: ......................
Start: ....../....../....... til ....../......../........
Peripheral blood Bone marrow
� smears (at least 6; unstained) � smears (at least 6; unstained)
� PB (2x10ml, heparinized) � Bone marrow (3x10ml, heparinized)
� Ficoll isolated nucleated cells � Ficoll isolated nucleated cells
BMA: .......................... (date)
hemoglobin: ........ g/dl WBC: ............x109/l platelets: ..............x109/l
BM-blasts: ............. %
Send to :1 Institut für Zell- und Molekularpathologie
Prof. Dr. D. Reinhardt Professorin Dr. B. SchlegelbergerHematological laboratory MHH (OE 5120) Pediatric Hematology/Oncology Carl-Neuberg-Str. 1Hannover Medical School D-30625 HannoverCarl-Neuberg-Str. 1 30625 Hannover
Germany
International Registry AML Relapse 2009 / -June ’09 - 22 -
International Registry AML Relapse 2009 / -June ’09 - 23 -
Group representatives for clinical and data management
Clinical Data management
AIEOP Carmelo Rizzari Roberto Rondelli
e-mail [email protected] [email protected]
phone +39 – 39 233 3513 +39 – 51 636 4667
fax +39 – 39 230 1646 +39 – 51 34 5759
AML-BFM-G Dirk Reinhardt J.E. Müller
e-mail [email protected] [email protected]
phone +49 – 511 532 6720 +49 – 511 532 9123
fax +49 – 511 532 9029 +49 – 511 532 9029
BFM-A: Michael Dworzak Nora Muehlegger
e-mail [email protected] [email protected]
phone +43 – 1 40170 480 +43 – 1 40170 4390
fax +43 – 1 40170 481 +43 – 1 40170 7430
CWPGH Petr Smisek Alena Vrzalova
e-mail [email protected] [email protected]
phone +420 – 2 2443 2201/2251/2232 +420 – 2 2443 2243
fax +420 – 2 2443 2220 +420 – 2 2443 2220
DCOG Gertjan J.L. Kaspers Karin van der Pal-de Bruin
e-mail [email protected] [email protected]
(new e-mail address)
phone +31 – 20 444 2420 +31 – 70 367 4545
fax +31 – 20 444 2422 +31 – 70 367 0868
EORTC-CLCG/FRALLE Noel Philippe Noel Philippe
e-mail [email protected] [email protected]
phone +33 – 4 7238 5780 +33 – 4 7238 5780
fax +33 – 4 7238 5503 +33 – 4 7238 5503
GATLA Hortensia Armendariz Francisco J. Lastiri
e-mail [email protected] [email protected]
phone +54 – 221 451 4641 +54 – 11 4806 8457
fax +54 – 221 457 5209 +54 – 11 4806 8457
Hong Kong S.Y. Ha S.Y. Ha
e-mail [email protected] [email protected]
phone +852 - 2855 3453 +852 - 2855 3453
fax +852 - 3005 7808 +852 - 3005 7808
International Registry AML Relapse 2009 / -June ’09 - 24 -
Hungary E. Magyarosy E. Magyarosy
e-mail [email protected] [email protected]
phone +36 – 1 459 9108 +36 – 1 459 9108
fax +36 – 1 459 9154 +36 – 1 459 9154
Israel Batia Stark David Steinberg
e-mail [email protected] [email protected]
phone +972 – 3 925 3669 +972 – 3 640 8035/8036
fax +972 – 3 925 3042 +972 – 3 640 9357
Moscow-Minsk Alexei Maschan Alexei Maschan
e-mail [email protected] [email protected]
phone +7 – 095 936 9423/935 6656 +7 – 095 936 9423/935 6656
fax +7 – 095 935 5510 +7 – 095 935 5510
MRC Owen Smith Rachael Clack
e-mail [email protected] [email protected]
phone +35 3 – 1 416 2014/2953 +44 – 1865 40 4861
fax +353 – 1 410 3475 +44 – 1865 40 4849
NOPHO Liisa Hovi Göran Gustafsson
e-mail [email protected] [email protected]
phone +358 – 9 4717 2720 +46 – 8 5177 2484
fax +358 – 9 4717 4707 +46 – 8 5177 3184
PINDA J. Quintana J. Quintana
e-mail [email protected] [email protected]
phone +56 – 2 210 4073 +56 – 2 210 4073
fax +56 – 2 210 4075 +56 – 2 210 4075
St. Jude Raul C. Ribeiro Annette Stone, R.H.I.A.
e-mail [email protected] [email protected]
phone +1 – 901 495 3694 +1 – 901 495 3192
fax +1 – 901 495 3122 +1 – 901 495 2405
SHOP Amparo Verdeguer Dainora Jaloveckas
e-mail [email protected] [email protected]
phone +34 - 96 398 7727 +34 - 93 458 3800
fax +34 - 96 398 7727 +34 - 93 459 0997
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 25 -
Recommendations for diagnostics and treatment
Diagnostics
Clinical evaluation, laboratory tests and follow-up
Send unstained smears (BM and PB; 6 each) and heparinised BM (2x 10ml) to your reference
laboratory for central diagnosis, and if possible send material for research studies in order to be
able to address the additional objectives of the study.
Before the start of the treatment the following parameters need to be obtained:
- medical history and physical examination
- performance status (depending on age, either the Karnofsky or Lansky Performance scale)
- ophthalmologic finding (retinal infiltration)
- complete blood count (hemoglobin, platelets, white blood cell count and differentiation). This
should be determined within 2 days prior to the first reinduction course.
- serum chemistry: creatinine, sodium, potassium, calcium, phosphate, ALAT, bilirubin, uric
acid, LDH, CK, glucose, total protein, albumin; clotting (APTT, PT, fibrinogen).
- HLA typing (if not done previously)
- recent information on the viral serology (antibodies: EBV, HSV, CMV, PVB19, HAV, HBV,
HCV, HIV; PCR: CMV, HCV) and IgG and IgA levels should be available.
- bone marrow examination (marrow cellularity and percentage of blasts). Perform a biopsy in
case of a dry tap. This should be performed within 3 days prior to the first reinduction course.
Bone marrow should also be sent to the reference laboratory for confirmation of the
diagnosis, and should be studied for immunophenotype and cytogenetics. Please consider to
participate in research studies.
- lumbar puncture (quantification of cells and protein, pathological examination), also to be
done within 3 days from the start of reinduction chemotherapy.
- urine (protein, glucose, ery’s)
- Chest X-Ray
- Abdominal ultrasound
- MRI (=NMR) of the brain in case of (the suspicion on) localized symptomatic CNS disease
- Electrocardiogram
- Echocardiography (please refer to the more comprehensive guidelines below)
- Lung function test (optional)
Criteria of response and other definitions
CNS disease
5 white blood cells/mm3 (ie, 5/ l, or 15/3 l) and unequivocal evidence of blasts on
cytospin examination, and/or clinical (seizures, cranial nerve palsy and symptoms of
increased cranial pressure or other signs/symptoms not readily explained by another
disease) and/or radiological evidence of leukemic infiltration in the central nervous
system. In all of the symptomatic cases, a MRI should be made. CSF not evaluable in
case of >50/3 erythrocytes.
Complete remission
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 26 -
5% leukaemic blasts in the bone marrow with signs in the BM of normal haematopoiesis
and with clear signs of regeneration of normal blood cell production in the peripheral
blood (platelets > 50x109/l without transfusions, neutrophils >1.0x109/l), and no leukaemic
cells in the PB or anywhere else.
Death, early
Death during the first 2 months of treatment (ie, before the time that complete remission
could have been documented). The cause of death (disease, therapy or both) should be
recorded as well as the last known percentage of blasts in the BM.
Death, toxic
Death due to treatment-related complications, and not caused by the leukemia itself
Partial remission
No complete remission, BM blasts > 5 20% and/or no regeneration
Refractory disease = non-responder
More than 20% of blasts in the bone marrow after 1 or 2 complete blocks of
chemotherapy, and/or elsewhere documented leukemic cells after 2 complete blocks of
chemotherapy
Relapse
After a documented complete remission, the recurrence of 10% unequivocal leukemic
cells (occasionally, 10-20% blasts in the BM does not represent a relapse!) in a
representative bone marrow, and/or evidence of leukemic infiltration or recurrence at any
site. CSF with <5 cells/mm3 but with blasts on the cytospin examination should be
investigated repeatedly, as should the BM in case of >5<10% leukemic cells and in case
of doubt otherwise.
Relapse, early first
Relapse within 1 year from initial diagnosis
Relapse, late first
Relapse occurring 1 year or later from initial diagnosis
Serious adverse event
Death, life-threatening or permanently disabling event, or grade 3 or 4 cardiotoxicity.
Therapy
This registry aims to evaluate the incidence and frequency of AML relapses in children and
adolescents. Further, a central reference diagnostics for the participating hospitals is offered. The
coordination center of the registry will provide clinical advice concerning diagnostics, treatment,
prognosis and alternative therapies.
To assure an informed advisory service, the administered therapy, treatment response and side
effects should be documented.
Based on the previous studies and the preliminary results from the international Relapsed AML
2001/01 trial, the registry committee recommended the following schedule:
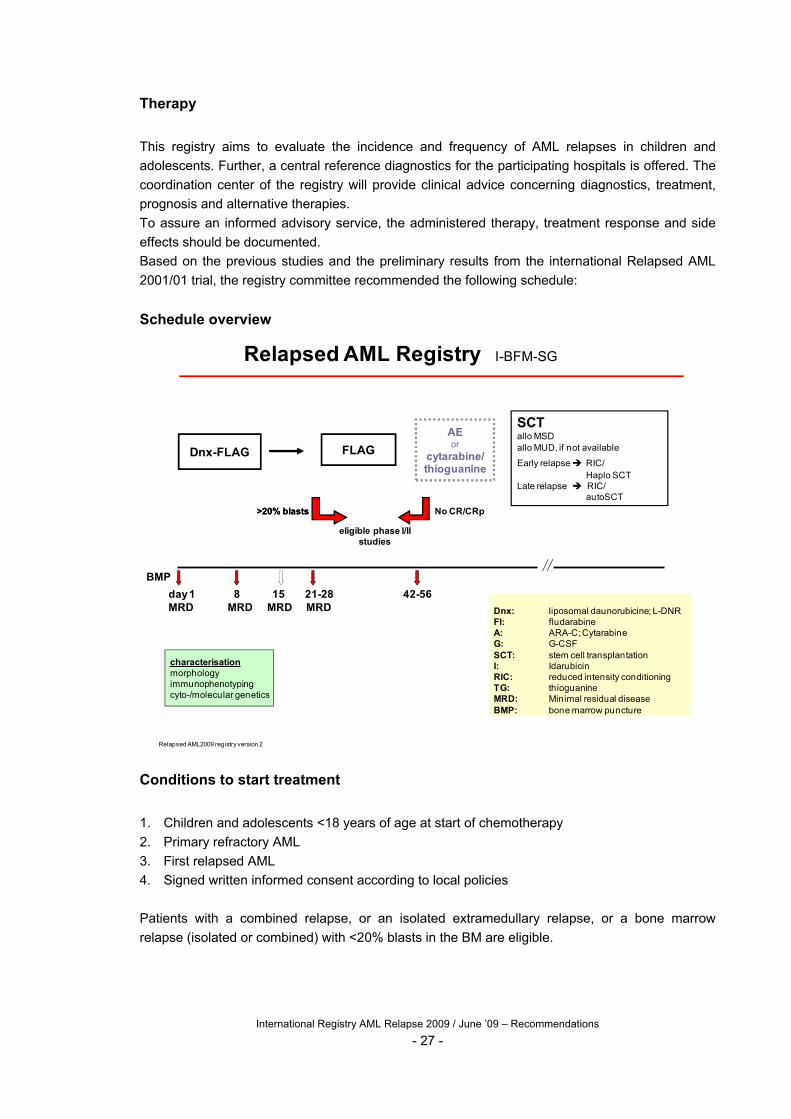
Schedule overview
Relapsed AML Registry I-BFM-SG
BMP
day 1 8 15 21-28 42-56 MRD MRD MRD MRD
FLAG
Relapsed AML2009 registry version 2
Dnx: liposomal daunorubicine; L-DNRFl: fludarabineA: ARA-C; CytarabineG: G-CSFSCT: stem cell transplantationI: IdarubicinRIC: reduced intensity conditioningTG: thioguanineMRD: Minimal residual diseaseBMP: bone marrow puncture
Dnx-FLAG
>20% blasts
eligible phase I/II studies
SCTallo MSDallo MUD, if not available
Early relapse RIC/Haplo SCT
Late relapse RIC/autoSCT
AEor
cytarabine/thioguanine
characterisationmorphologyimmunophenotypingcyto-/molecular genetics
No CR/CRp>20% blasts
Conditions to start treatment
1. Children and adolescents <18 years of age at start of chemotherapy
2. Primary refractory AML
3. First relapsed AML
4. Signed written informed consent according to local policies
Patients with a combined relapse, or an isolated extramedullary relapse, or a bone marrow
relapse (isolated or combined) with <20% blasts in the BM are eligible.
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 27 -
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 28 -
Contradiction for full-dose treatment
1. Symptomatic cardiac dysfunction (CTC grade 3 or 4) and/or a Fractional Shortening at
echocardiography below 29%
2. A Karnofsky performance status <40% (children >=16 years) or an Lanksy performance
status of <40% (children < 16 years) before start of chemotherapy
3. Any other organ dysfunction (CTC grade 4) that will interfere with the administration of the
therapy according to this protocol (e.g. transaminases >10 times the UNL)
4. Inability to potentially complete the treatment protocol for any other reason
5. FAB type M3 (please refer to your local group for one of the treatment alternatives)
Background and introduction
Newly diagnosed acute myeloid leukemia (AML) is a rare disease in children. The prognosis has
improved using intensive chemotherapy with or without stem cell transplantation. However, 5-10%
of patients do not achieve first complete remission (CR) due to resistant disease (primary
refractory AML), and 30-50% of CR patients relapse. Primary refractory AML and relapsed AML
have a poor prognosis, with an overall survival of less than 25%. For first relapse disease, the
prognosis mainly depends on the time of relapse. If early, defined as within 1-1.5 years from initial
diagnosis, the second CR rate is about 50%, and overall survival 10% or less. If late, defined as
after 1-1.5 years from diagnosis, the second CR rate is 80-90% and the overall survival up to
40%. Multiple relapsed AML has an even worse prognosis. Several treatment schedules have
been studied recently, and progress seems feasible using new drugs and new drug combinations.
The currently available alternatives are described below.
Liposomal daunorubicin (DaunoXome®)
Daunorubicin is a well-known anthracycline with proven efficacy in AML. Anthracyclines are
intensely used in first-line treatment, which limits its use in case of refractory or relapsed disease,
because of its cardiotoxicity. This cardiotoxicity is dose-related, and becomes an increasing
problem in case of higher cumulative doses (Lipshultz 1991). Such cumulative doses have
normally been given in first-line treatment. Another cumbersome side-effect of anthracyclines is
mucositis. DaunoXome® is a combination of daunorubicin and a unilamellar liposomal transport
system. Because of the chemical formula, the compound is relatively stable in the plasma.
Because of the preferential release of free daunorubicin intracellularly, the plasma level of free
daunorubicin is lower than in case of infusion with daunorubicin itself. In a mouse model,
liposomal doxorubicin had no cardiotoxicity like in saline-treated controls, but did have significant
antileukemic activity (Forssen 1981). In an isolated perfused rat model, DaunoXome® had no
cardiotoxicity in contrast to free daunorubicin (Pouna 1996). DaunoXome® had a relatively low
incorporation in heart muscle as compared to tumor cells (Forssen 1992). The above may explain
the absence of cardiotoxicity of DaunoXome® in 277 AIDS patients with Kaposi’s sarcoma, who
received cumulative doses of DaunoXome® of up to 1700 mg/m2, >600 mg/m2 in 53 patients at a
total group mean cumulative dose of 481 mg/m2 (Gill 1996). Out of 979 Kaposi’s sarcoma patients
treated with DaunoXome®, 1 patient developed cardiotoxicity with clinical symptoms (Summary of
Product Characteristics, Gilead Sciences, 5 June 2001). In general, liposomal anthracyclines
cause less cardiotoxicity at higher cumulative doses than conventional anthracyclines (Levitt
1999). Animal solid tumor studies showed that at equivalent daunorubicin dosages, DaunoXome®
had significantly increased antitumor activity and less toxicity as compared to free daunorubicin
(Corbett 1978, Forssen 1994). Significant penetration of DaunoXome® into the cerebrospinal fluid
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 29 -
and brain is unlikely, since liposomes cross the blood-brain barrier poorly, if at all (Tökés 1980).
This is also the case for free anthracyclines. However, the penetration may be different in e.g.
brain tumors (Zucchetti 1999). A clinical study of the AML-BFM group (Creutzig et al., unpublished
data) is in progress, in which DaunoXome® is given in combination with cytarabine in relapsed
AML patients. Initially, DaunoXome® at 60 mg/m2/day was given on days 1 and 5 of a course
including 4 days of continuously iv cytarabine (500 mg/m2/day for 4 days), which course was
repeated after 4-5 weeks. Because of limited toxicity, the current cohort of patients is being
treated with an extra infusion of DaunoXome® on day 3 of each of the 2 courses. No
cardiotoxicity has been seen sofar, but follow-up is short. Based on these data, it was decided to
include DaunoXome® in this treatment protocol.
FLAG +/- Idarubicin
The favorable effect of combining fludarabine and cytarabine, leading to an increased
arabinosylcytosine 5’-triphosphate (ara-CTP) accumulation as compared to that achieved by
cytarabine alone, was initially described by Gandhi et al. (1993). In addition, it has been reported
that G-CSF combined with cytarabine may render AML cells more sensitive to the latter drug
(Tafuri 1990), which may be explained by the increased ara-CTP accumulation - associated with
increased deoxycytidine kinase activity – in case of pre-exposure to G-CSF as reported by Braess
et al. (2000). Finally, Gandhi et al. (1995) reported that G-CSF significantly increased the
accumulation of the active metabolite of fludarabine. Thus, the combination of fludarabine,
cytarabine and G-CSF (FLAG) emerged, although the role of G-CSF has been questioned (Estey
1994). Several colleagues in the UK used FLAG for reinduction of relapsed AML. Retrospectively,
data on 40 patients were obtained using a questionnary (Gibson et al., unpublished data), with
subsequent CR in 21/30 (70%) relapse patients and CR in 3/7 primary refractory patients. One
patient died of pneumocystis carinii pneumonia. Grade 4 hematological toxicity was the rule.
Fleischhack et al. (1998) treated 38 (update: 44) relapsed AML patients with IDA-FLAG, ie,
idarubicin added to FLAG, followed by again IDA-FLAG or FLAG. Three patients received FLAG
only. Toxicity was marked. Numbers were small, but the time of myelosuppression was shorter
after FLAG than after IDA-FLAG. Except for grade 4 hematological toxicity, infections with often
pulmonary involvement was a relatively frequent complication, and were more often seen after
IDA-FLAG than after FLAG. CR rates were 56% and 75% in early and late relapses respectively
(updated but not published data: 58% and 78% respectively). This protocol applies the FLAG
schedule with G-CSF starting 1 day before and to be continued during chemotherapy, based on
the above summarised studies.
FLAG + DaunoXome®
Fleischhack et al. (Bonn, unpublished data) have piloted this regimen in 10 patients with relapsed
AML. Toxicity was tolerable and similar as with IDA-FLAG. Five patients had mild mucositis, eight
fever of unknown origin, one gram-positive bacteremia, and one a pneumonia. Five patients
achieved CR and proceeded to SCT, two patients were partial responders and three patients did
not respond and died. This pilot study shows that FLAG in combination with DaunoXome® is
feasible and has antileukemic activity. However, 2 consecutive courses of FLAG + DaunoXome®
(3 x 60 mg/m2/day) is anticipated to be too toxic.
Other reinduction chemotherapy regimens
Cytarabine or other agents have been studied in combination with well-known drugs such as
etoposide and amsacrine, with significant antileukemic activity (Miller 1991, Ozkaynak 1998,
Steuber 1996, Whitlock 1997, Baruchel unpublished). Data on the use of new agents such as

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 30 -
topotecan in children have not been reported yet. Cladribine® (2-chloro-deoxyadenosine) has
been studied in relapsed AML as well. The response rate in 17 children was 59%, including a CR
rate of 47% (Santana 1992). However, these investigators subsequently investigated this drug in
93 children with newly diagnosed AML or myelodysplastic syndrome (MDS), and found that at an
overall CR rate of 40% after 2 courses of cladribine®, patients with FAB type M5 responded
significantly better than non-M5 patients, with CR rates of 71% and 24% respectively. Therefore,
cladribine does not seem very active in non-FAB M5 type cases.
CNS prophylaxis and treatment
Overt CNS leukemia is relatively rare in AML. This protocol applies high-dose chemotherapy, with
an anticipated CNS prophylactic effect as well. This is also true for the conditioning regimen (see
later), that all children are supposed to get. There is virtually no literature available on CNS
prophylaxis and treatment in this patient-group to further refine or substantiate the
recommendations given in this protocol, which were therefore extensively discussed and agreed
upon.
Consolidation chemotherapy
To consolidate an achieved CR, and to have time to prepare a transplant if not available
immediately, further chemotherapy seems indicated. Whether this is really necessary and if so,
which drugs should be used, is essentially unknown. Yet, in these high-risk patients, further
intensive treatment seems justified. Therefore, a schedule of VP16 and cytarabine given by
continuous infusion has emerged. In case of a delayed SCT and a contra-indication for this high-
intensity consolidation regimen, a low-intensive combination of orally thioguanine and cytarabine
subcutaneously is proposed. Extensive experience with this regimen has been obtained within the
BFM-AML protocols.
Stem cell transplantation (SCT)
Allogeneic SCT is associated with major morbidity and mortality. Therefore, allogeneic SCT
should be considered in the context of the prognosis with chemotherapy only. In patients with
primary refractory and relapsed AML, this prognosis is very poor. Moreover, few long-term
survivors have been described after chemotherapy only for this particular disease, in contrast to
chemotherapy followed by SCT. Although not proven in properly designed randomised clinical
trials, allogeneic SCT may have a bigger impact on the prognosis than autologous SCT, because:
1) a graft-versus-leukemia effect may be present in the allogeneic, but not (or less) in the
autologous setting, and 2) the autologous transplant is likely to contain minimal residual leukemia
cells, which may cause a relapse. On the other hand, allogeneic SCT may be complicated by
graft-versus-host-disease. We do recommend allogeneic SCT for all patients who achieve CR,
preferably using a matched sibling donor (MSD), or if not available, a matched unrelated (MUD)
donor. Patients with refractory disease or early relapse and lack of a matched donor might be
eligible for an alternative or experimental allogeneic SCT. In late relapses without a matched
donor, autologous SCT may be used. There are several proposals for the conditioning regimen,
including a combination of busulfan, cyclophosphamide and melphalan. Experiences using this
regimen in children with myelodysplastic syndrome were good (Locatelli 1994). Depending on the
type of donor, additional immunosuppression may be required in conditioning. Patients who were
not irradiated previously and who will have a SCT for the 1st time should have for instance
TBI/cyclophosphamide (also depending on age) as conditioning instead of busulfan,
cyclophosphamide and melphalan.

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 31 -
Conclusion
The above summary shows that the DNX-FLAG regimen seems relatively effective with tolerable
toxicity. Another point of concern is the cardiotoxicity of anthracyclines, which is a major potential
problem in these patients because of their initial treatment leading to high cumulative doses of
these drugs already. However, anthracyclines are among the most effective drugs in AML.
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 32 -
Special measures for reinduction
High cell counts
Patients with high peripheral blast counts (>50-100x109/l) and significant organomegaly have
increased problems related to metabolic abnormalities, bleeding, and hyperviscosity. Platelets
should be transfused if < 15-30x109/l; in this phase, hemoglobin should not be raised above 6
mmol/l (= 9,6 g/dl); treatment of coagulation disorders is required. The use of leukopheresis,
exchange transfusion, or hemodialysis may be necessary. To prevent tumor lysis syndrome, the
patient should be well hydrated, alkalinized and get allopurinol before start of therapy:
Allopurinol: 200-300 mg/m2 p.o. divided q 8-12 hours; give at least 2 doses prior to
initiation of therapy (alternatively, uricozyme may be used)
Hydration: 2400-3000 ml/m2/day; be careful with potassium containing solutions;
electrolyte substitions only based on laboratory results; check fluid balance
NaHCO3: 4 g/m2/day (= 50 mEq/m2/day) to maintain urine pH 7-8
High dose ARA-C
During cytarabine and for 24-48 hours after completion, dexamethasone ophthalmic solution or
isotears (q 6 hours) should be used to prevent cytarabine induced conjunctivitis.
Because of the association of streptococcus viridans infection and high dose cytarabine, penicillin
prophylaxis is recommended from completion of cytarabine administration until neutrophil
recovery.
Nurses and doctors should be aware of the relatively high (up to 15%) incidence of neurotoxicity,
which may necessitate to interrupt or stop high-dose cytarabine administration.
Pyridoxine (300 mg/m2/day in 2 doses) might ameliorate cytarabine-induced mucositis.
Granulocyte colony stimulating factor
G-CSF will be used as part of the FLAG regimen (please refer to “background and introduction”).
After discontinuation at day 6 it is recommended to restart G-CSF at day 15 of each reinduction
course in order to shorten the period of neutropenia in these patients who all are at high risk for
severe infections, of which the occurrence is correlated with the duration of neutropenia. G-CSF
can be stopped again upon neutrophil recovery, as locally defined. The use of G-CSF for
prevention or treatment of chemotherapy induced fever and neutropenia before day 15 is
considered useless.
Irradiation of blood products
Mainly due to fludarabine and body irradiation, profound and long term lymphocytopenia can be
expected to occur. Therefore, cellular blood products should be irradiated with 25 Gy to prevent
transfusion related graft versus host disease, at least up to 6 months after the last fludarabine
administration. Of course, all blood products should be leukocyte-depleted as well. Similarly,
irradiation and leukocyte-depletion of the blood products is required at least up to 6 months after
SCT.
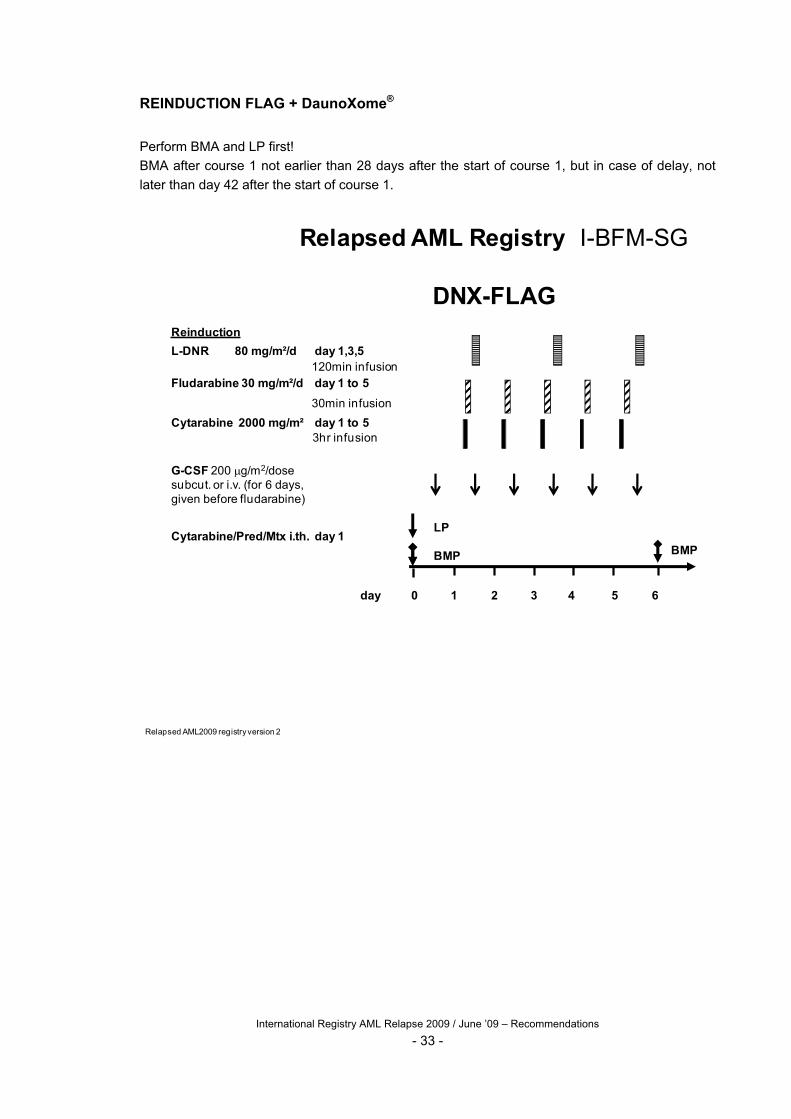
REINDUCTION FLAG + DaunoXome®
Perform BMA and LP first!
BMA after course 1 not earlier than 28 days after the start of course 1, but in case of delay, not
later than day 42 after the start of course 1.
Relapsed AML Registry I-BFM-SG
DNX-FLAGReinduction
L-DNR 80 mg/m²/d day 1,3,5120min infusion
Fludarabine 30 mg/m²/d day 1 to 5
30min infusion
Cytarabine 2000 mg/m² day 1 to 53hr infusion
G-CSF 200 g/m2/dosesubcut. or i.v. (for 6 days,given before fludarabine)
Cytarabine/Pred/Mtx i.th. day 1
day
LP
BMP BMP
0 1 2 3 4 5 6
Relapsed AML2009 registryversion 2
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 33 -

2nd REINDUCTION FLAG
Course 2 may start not earlier than 28 days after the start of course 1, and only in case of good
clinical condition, platelets > 50x109/l (without transfusions) and neutrophils > 1.0x109/l. An
exception are patients with partial remission after course 1, who retain too low neutrophils and/or
platelets, likely to be due to residual leukemia. These patients – if in good enough clinical
condition – may continue treatment irrespective of the blood counts, after BMA.
FLAGReinduction
G-CSF 200µg/m²/d SC/IV day 0 to 5
Fludarabine 30 mg/m²/d day 1 to 530 min IV infusion, after G-CSF
Cytarabine 2000 mg/m²/d day 1 to 53hr IV infusion, begin 4 h after start of Fludarabine
Cytarabine/Pred/MTX day 1
IT bolus injection, age related dosage
day
LP
BMP
0 1 2 3 4 5
In case of a body weight <12 kg, calculate dose according to weight as follows: [weight (kg) x dose (per m2)] /30.
10 mg8 mg6 mg4 mgPred
12 mg10 mg8 mg6 mgMTX
30 mg26 mg20 mg16 mgAraC
3 year2<3year1<2year<1 year
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 34 -
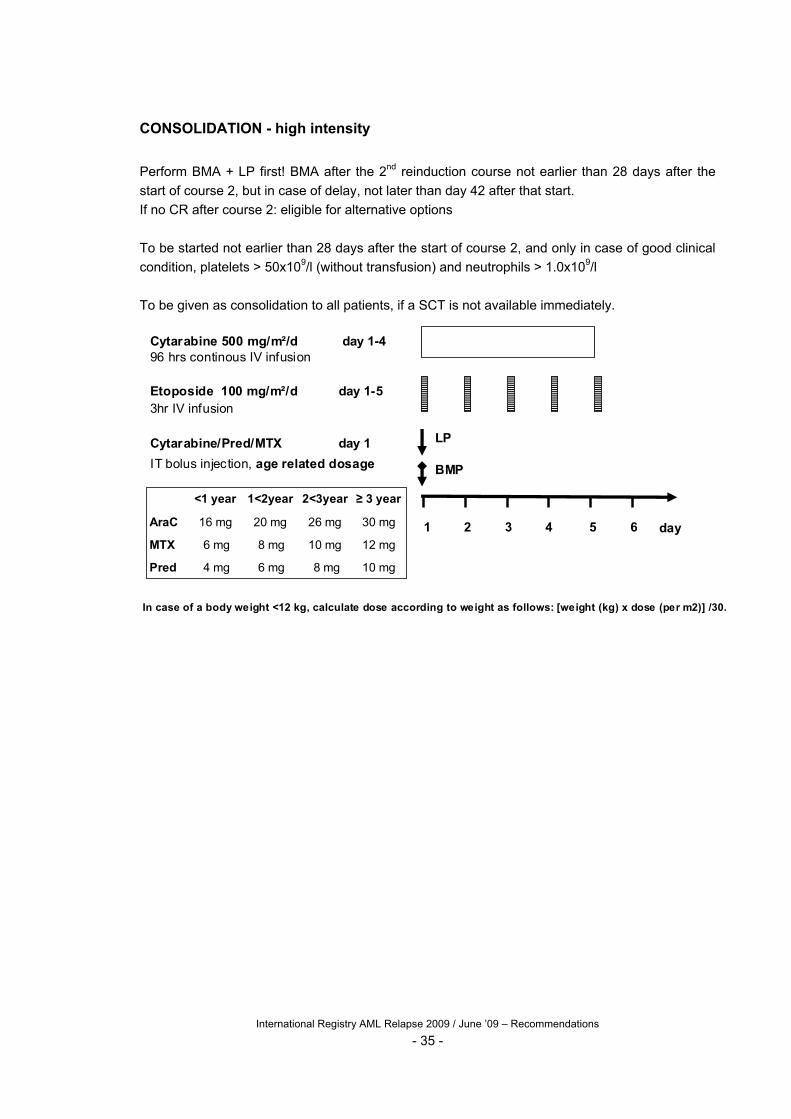
CONSOLIDATION - high intensity
Perform BMA + LP first! BMA after the 2nd reinduction course not earlier than 28 days after the
start of course 2, but in case of delay, not later than day 42 after that start.
If no CR after course 2: eligible for alternative options
To be started not earlier than 28 days after the start of course 2, and only in case of good clinical
condition, platelets > 50x109/l (without transfusion) and neutrophils > 1.0x109/l
To be given as consolidation to all patients, if a SCT is not available immediately.
Cytarabine 500 mg/m²/d day 1-496 hrs continous IV infusion
Etoposide 100 mg/m²/d day 1-5 3hr IV infusion
Cytarabine/Pred/MTX day 1
IT bolus injection, age related dosage
LP
BMP
1 2 3 4 5 6
10 mg8 mg6 mg4 mgPred
12 mg10 mg8 mg6 mgMTX
30 mg26 mg20 mg16 mgAraC
3 year2<3year1<2year<1 year
day
In case of a body weight <12 kg, calculate dose according to weight as follows: [weight (kg) x dose (per m2)] /30.
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 35 -
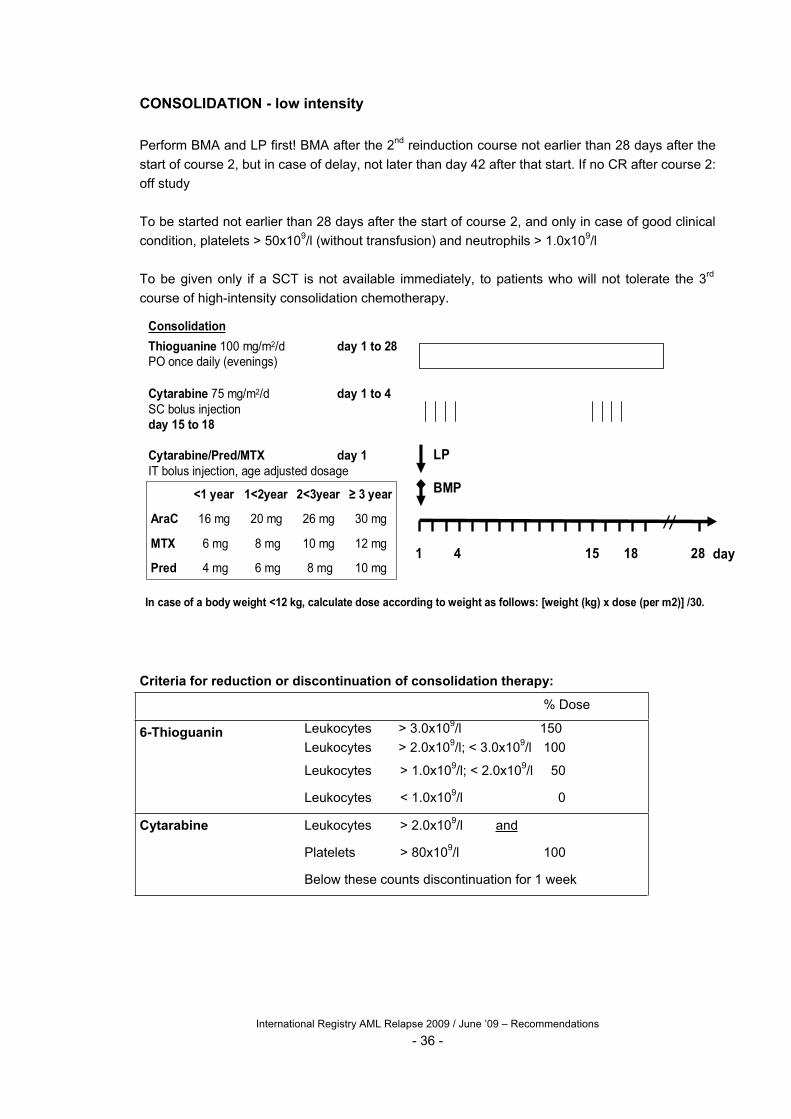
CONSOLIDATION - low intensity
Perform BMA and LP first! BMA after the 2nd reinduction course not earlier than 28 days after the
start of course 2, but in case of delay, not later than day 42 after that start. If no CR after course 2:
off study
To be started not earlier than 28 days after the start of course 2, and only in case of good clinical
condition, platelets > 50x109/l (without transfusion) and neutrophils > 1.0x109/l
To be given only if a SCT is not available immediately, to patients who will not tolerate the 3rd
course of high-intensity consolidation chemotherapy.
Consolidation
Thioguanine 100 mg/m2/d day 1 to 28PO once daily (evenings)
Cytarabine 75 mg/m2/d day 1 to 4SC bolus injectionday 15 to 18
Cytarabine/Pred/MTX day 1IT bolus injection, age adjusted dosage
LP
BMP
1 4 15 18 28 day10 mg8 mg6 mg4 mgPred
12 mg10 mg8 mg6 mgMTX
30 mg26 mg20 mg16 mgAraC
3 year2<3year1<2year<1 year
In case of a body weight <12 kg, calculate dose according to weight as follows: [weight (kg) x dose (per m2)] /30.
Criteria for reduction or discontinuation of consolidation therapy:
% Dose
6-Thioguanin Leukocytes > 3.0x109/l 150
Leukocytes > 2.0x109/l; < 3.0x109/l 100
Leukocytes > 1.0x109/l; < 2.0x109/l 50
Leukocytes < 1.0x109/l 0
Cytarabine Leukocytes > 2.0x109/l and
Platelets > 80x109/l 100
Below these counts discontinuation for 1 week
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 36 -
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 37 -
CNS PROPHYLAXIS AND TREATMENT
Prophylaxis:
There should be no evidence of CNS leukemia (see below).
Cytarabine/ methotrexate/ prednisolone should be administered three times, intrathecally at age-
adjusted doses (Table), via a lumbar puncture (LP). Give the first and second dose one day
before the start of reinduction course 1 and 2 respectively (not simultaneously with high dose
cytarabine). Give the third dose at the start of consolidation treatment. Cranial irradiation is not
recommended.
Table. Intrathecal medication (LP) in case of CNS prophylaxis
Age
mg/dose mg/dose
Cytarabine Methotrexate Prednisolone
mg/dose
<1 year 16 6 4
1<2 year 20 8 6
2<3 year 26 10 8
3 years 30 12 10
Treatment of CNS leukemia
CNS leukemia is defined on page 31. Triple intrathecal medication at age-adjusted doses (Table),
by LP. The first dose should be given immediately before the start of reinduction course 1. The
second and subsequent doses should be given every 7 days until 1 week after complete
clearance of the CSF of leukemic blasts. Then, 2 more doses must be given, one immediately
before the start of the second reinduction course, and the other at the start of consolidation
treatment.
Table. CNS leukemia: Intrathecal medication via lumbar puncture or reservoir; to be given every
week until 1 week after complete blast clearance of the CSF.
Age Cytarabine
mg/dose, every week
Methotrexate
mg/dose, every week
Prednisolone
mg/dose, every week
<1 year 16 6 4
1<2 year 20 8 6
2<3 year 26 10 8
3 years 30 12 10
Cranial irradiation is not recommended, but may be considered in those patients who do achieve
complete remission but who will not undergo SCT, and who did not receive cranial irradiation in
the past.
STEM CELL TRANSPLANTATION
All patients should be treated according to the AML-SCT synopsis (see attachment)
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 38 -
Overview drugs
Cytarabine
This nucleoside analogue (pyrimidine antagonist) is an antimetabolite that is mainly metabolised
in the liver. It may cause myelosuppression, hepatotoxicity, exanthema, malaise, and gastro-
intestinal toxicity such as nausea, vomiting, stomatitis, and ileus. At high doses, fever, severe
diarrhea, central nervous system disturbances such as somnolence, cerebellar ataxia and
nystagmus, keratitis, veno-occlusive disease, pneumonitis and adult respiratory distress
syndrome with streptococcus viridans infection are possible. Intrathecal administration has been
associated with headache, fever, vomiting, and pleiocytosis, rarely with aseptic meningitis or
central nervous system disturbances. To prevent keratitis, indifferent or corticoid eye drops every
4-6 hours are recommended during and until 12 hours after stopping cytarabine. Prolonged
corticoid eye drops have side-effects as well, such as infection. Conjunctivitis should be treated
with corticoid eye drops. To prevent streptococcal infection, penicilline prophylaxis may be
considered starting as soon as neutropenia develops after high-dose cytarabine until neutrophils
> 0.5x109/l. Patients who developed grade 3 or 4 neurotoxicity following high-dose cytarabine
should not receive further high-dose cytarabine, but are eligible for continuous lower-dose
cytarabine.
Fludarabine
This nucleoside analogue (purine antagonist) is an antimetabolite that is excreted mainly in the
urine. After phosphorylation, it is less susceptible to deamination than cytarabine. Main side-
effects are myelosuppression, fever, chills, malaise, nausea, and vomiting. More rare are auto-
immune phenomena (hemolytic anemia), pneumonitis, and CNS symptoms such as agitation.
Since it causes profound and long-term lymphocytopenia, irradiation of blood products to prevent
graft-versus-host disease and antifungal prophylaxis is strongly recommended, from the start of
treatment until 6 months after SCT or if SCT is not being perfomed until 6 months after the last
administration of fludarabine.
G-CSF
This is a drug produced in E. coli by recombinant DNA technology that stimulates the production
of neutrophils in the bone marrow. Side-effects occur occasionally, and concern beside local
irritation mainly bone pain, vasculitis and thrombocytopenia. G-GSF can be administered both
subcutaneously and i.v., but for the latter administration special attention has to be given to the
instructions for dilution and administration.
Liposomal daunorubicin (DaunoXome®)
This drug is the combination of an anthracycline with a unilamellar liposomal transport system.
Daunorubicin is released slowly, and then mainly excreted in the bile, less so in the urine.
Daunorubicin itself is metabolised to daunorubicinol, which is again mainly excreted in the urine
and in the bile. The drug should be soluted in dextrose 5% only, because of agglutination in other
solutions! Although not reported for DaunoXome®, the concomitant use of daunorubicin with
heparin or dexamethasone i.v. is complicated by precipitation. Therefore, these drugs should not
be used simultaneously i.v. with DaunoXome®. Because of its composition, care should be taken
when using DaunoXome® concomitantly with parenteral nutritional lipid solutions or other
liposmal products. Side-effects that have been described were nausea, vomiting, mucositis,
hepatotoxicity and the dose-limiting toxicity is myelosuppression. Cardiotoxicity is rare, but has
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 39 -
been documented both without (decreased left ventricular ejection fraction) and with clinical
symptoms (congestive heart failure).
In case of a fractional shortening at echocardiography below 29%, DaunoXome® should not be
given, at least not as part of this register. Another relative contra-indication is a previous serious
hypersensitivity reaction to DaunoXome® or any of its constituents.
In case of hepatic disturbances before the first administration of DaunoXome®, a reduction for all
three doses is recommended:
Transaminases >3-5 times upper normal limit (UNL): reduction of 25%.
Transaminases >5-10 times UNL: reduction of 50%
Transaminases >10 times UNL: not eligible
All three doses of DaunoXome® should be similar, in other words, no further reductions after the
first dose.
Thioguanine
This purine antagonist is an antimetabolite that is metabolised rapidly and then excreted renally. It
may cause myelosuppression, nausea, vomiting, anorexia, mucositis, diarrhea, hepatotoxicity,
and veno-occlusive disease.

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 40 -
Supportive Care
The treatment to be given is aggressive and immunosuppressive. Therefore, meticulous care is
required in the management of patients entering the study (Riley 1999).
General measures
* Venous access: placement of a double lumen central venous catheter for administration of
chemotherapy, nutrients, antibiotics and blood products is strongly advised.
* Tumor lysis prevention: to prevent tumor lysis syndrome, the patient should be well hydrated,
alkalinized and placed on allopurinol (or uricozyme) before initiation of therapy (see also page 14)
* Nutrition: the combination of chemotherapy induced vomiting, mucositis, infection, and
hemorrhage may result in significant weight loss. Progressive weight loss should be treated
aggressively with supplemental enteral or parenteral nutrition; enteral feedings are preferred to
parenteral; adjustment of the diet (p.e. no lactose or semi elementary) may be beneficial. Because
melphalan competes with phenylalanine for cellular uptake, amino acids as part of parenteral
nutrition should not be given one day before and two days following melphalan
* Nill-by-mouth: when enteral feedings must be withheld, protection of the gastric mucosa should
be initiated
* Antiemetics: prophylactic antiemetic therapy should be instituted to prevent chemotherapy
induced nausea and vomiting. Steroids should not be used in case of (suspected) fungal
infections.
* Mucositis: meticulous oral hygiene is required; tooth brushing, hydrogen peroxide, saline and
bicarbonate rinses; chlorhexidine solution; liberal use of pain medication for this condition is
encouraged. Stomatitis due to herpes virus may be confused with drug induced mucositis;
therefore, viral cultures should be obtained frequently. Anti-herpetic and anti-fungal therapy
should be given as indicated.
* Conjunctivitis prophylaxis: during cytarabine and for 24-48 hours after completion,
dexamethasone ophthalmic solution or isotears (q 6 hours) should be used to prevent cytarabine
induced conjunctivitis.
* Suppression of menstruation: menstruating females should receive depo-provera or another
suppressant during the entire course of the protocol until the platelet count is >40-50x109/l without
transfusion support.
* Vaccinations: these should be postponed till after completion of treatment
* Physical therapy: timely exercises for preventing and maintaining optimal motor skills are
recommended
* Psychosocioeconomic support: recommended
* Prevention and treatment of pain: according to local guidelines
Hyperleukocytosis and metabolic derangement
Patients with high peripheral blast counts (>50-100x109/l) and significant organomegaly have
increased problems related to metabolic abnormalities, bleeding, and hyperviscosity. Therefore,
special measures for reinduction are indicated and are described on page 14.

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 41 -
Prevention and treatment of infections
Prevention:
* mandatory hospitalization during and after treatment courses until the absolute neutrophil count
is rising (and depending on the clinical condition)
* barrier nursing
* HEPA air filtration in the nursing room if available
* oral hygiene (see above)
* treatment of infectious foci before initiating therapy: ENT, dental prior to initiating therapy;
multiple dental extractions may be necessary.
* surveillance cultures may be considered, according to local guidelines; routine culture of throat
to detect the presence of penicillin-resistant streptococcus
* test for toxoplasmosis, hepatitis viruses, CMV, varicella and HSV antibodies
* bowel decontamination may be considered, according to local guidelines (Guiot 1983)
* prophylactic antibiotics in case of bacteriaemia causing operations
* pneumocystis carinii prophylaxis with trimethoprim-sulfamethoxazole, e.g. 150/750 mg/m2/day
for 3 consecutive days every week (Hughes 1987); alternatives: dapsone or aerosolized
pentamidine
* because of the association of streptococcus viridans infection and high dose cytarabine,
penicillin prophylaxis is recommended from completion of cytarabine administration until
neutrophil recovery
* prophylactic treatment of fungal (including aspergillus) infections is recommended: e.g. with oral
itraconazole (liquid!, 5-10 mg/kg/day in 1-2 doses, maximum 600 mg/day)
* at the time of stem cell transplantation, prophylactic acyclovir for patients with positive HSV titers
* administration of zoster hyper immune globulin within 48 hours after a real varicella contact
* Restarting G-CSF at day 15 of each of both reinduction courses is recommended to reduce the
duration of neutropenia. G-CSF should be stopped again upon neutrophil recovery, as defined by
local guidelines.
Treatment in case of fever and neutropenia:
Because of the high risk of serious infectious complications, patients developing fever should be
treated for presumed sepsis with broad spectrum antibiotics. Because of the association of high
dose cytarabine with streptococcus viridans infection and because of the possibility of a
contaminated central venous line (staphylococci) the antibiotic regimen should include drugs
specific for the treatment of an infection with gram-positive bacteria (vancomycin, teicoplanin).
Antifungal therapy, such as amphotericin B should be administered when defervescence does not
occur within 3-5 days.
AML treatment is associated with a high risk of pulmonary aspergillus; however,
pulmonary infiltrates can also be caused by bacteria, virus (CMV), legionella and PCP; therefore,
agressive diagnostic measures including (repeated) high resolution CT scans, bronchoscopy with
biopsy or bronchoalveolar lavage, and open lung biopsy, should timely be contemplated.
G-CSF, if not given already, may be considered to reduce the duration of neutropenia, in
patients with life-threatening bacterial or fungal infections.
Treatment in case of a documented infection:
The empiric treatment may be adjusted when a specific cause for the infectious symptoms is
found, although broad-spectrum antibiotics remain (at least initially) indicated in case of
neutropenia.
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 42 -
G-CSF
Granulocyte colony stimulating factor (G-CSF) will be used as part of the FLAG regimen from the
day before starting fludarabine until the first day after fludarabine (for a total of 6 days). Adding G-
CSF to FLA has been decided because the pilot-studies were done with FLAG and because of
several papers describing favorable interactions of G-CSF with fludarabine and cytarabine
(Braess 2000, Gandhi 1995; see also “background and introduction”). After the discontinuation it
is recommended to restart G-CSF at day 15 of each reinduction course in order to shorten the
period of neutropenia in these patients at high risk for severe infections, of which the occurrence
is correlated with the duration of neutropenia. G-CSF appears safe in that it had no negative
impact on the prognosis of adult AML in 2 large randomised studies (Godwin 1998, Heil 1997),
and its use reduced duration of neutropenia, fever, hospitalisation, and use of antibiotics and
antifungals (Chen 1998, Godwin 1998, Heil 1997). G-CSF should be stopped again upon
neutrophil recovery, as locally defined. The use of G-CSF before day 15 of each course for
prevention or treatment of chemotherapy induced fever and neutropenia is considered useless,
although this has not been studied in this particular setting.
Transfusion support
* Bleeding due to thrombocytopenia should be treated promptly; during the induction period and
throughout admissions for fever and neutropenia, it is recommended that the platelet count be
maintained >15-30x109/l. Higher tresholds may be indicated, for instance in case of lumbar
punctures and surgery.
* Packed red blood cell transfusions should be used to correct hypovolemia from blood loss or
pre-existing anemia (Hb < 5 mmol/l = 8,0 g/dl). Higher threshold levels may be indicated in case
of pneumonitis or (imminent) bleeding or other causes of a compromised clinical condition.
* The blood products should be leukocyte-depleted to prevent HLA sensibilization; leukocyte-
depleted blood products can be considered CMV-safe.
* To prevent transfusion related graft versus host disease, cellular blood products should be
irradiated (25 Gy) during and at least till 6 months after fludarabine, in case of (imminent)
lymphopenia (< 500/ml), and from 2 weeks before till at least 6 months after stem cell
transplantation.
* In case of allo-immunization HLA-matched platelets may be required.
2. During initial treatment, i.e. the 1st course, to monitor the disease:
- At least twice weekly a complete hematological count and serum chemistry are needed as
described above
- a twice or more weekly physical examination is performed
- at day +15 after the start of reinduction treatment a bone marrow sample is obtained to
determine early clinical response, which may be different between both treatment arms and
which may have prognostic significance. Slides should also be send to the reference
laboratory for morphological (and flowcytometrical) examination, together with peripheral
blood slides.
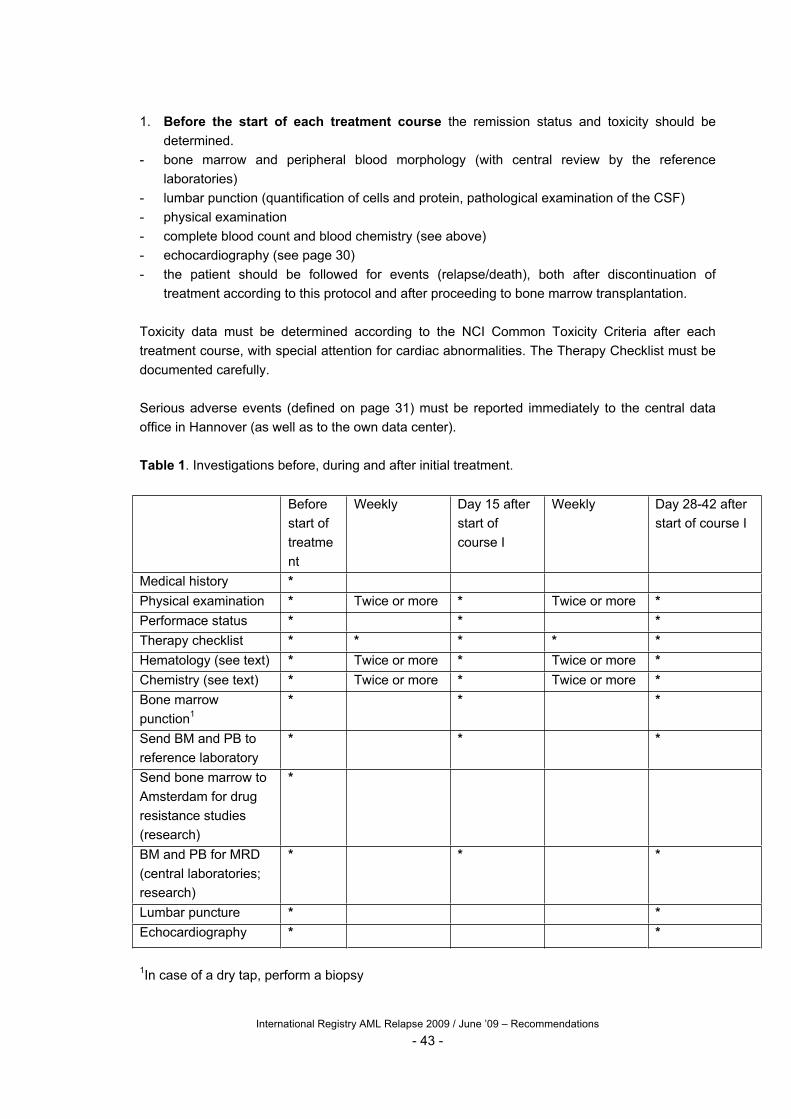
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 43 -
1. Before the start of each treatment course the remission status and toxicity should be
determined.
- bone marrow and peripheral blood morphology (with central review by the reference
laboratories)
- lumbar punction (quantification of cells and protein, pathological examination of the CSF)
- physical examination
- complete blood count and blood chemistry (see above)
- echocardiography (see page 30)
- the patient should be followed for events (relapse/death), both after discontinuation of
treatment according to this protocol and after proceeding to bone marrow transplantation.
Toxicity data must be determined according to the NCI Common Toxicity Criteria after each
treatment course, with special attention for cardiac abnormalities. The Therapy Checklist must be
documented carefully.
Serious adverse events (defined on page 31) must be reported immediately to the central data
office in Hannover (as well as to the own data center).
Table 1. Investigations before, during and after initial treatment.
Before
start of
treatme
nt
Weekly Day 15 after
start of
course I
Weekly Day 28-42 after
start of course I
Medical history *
Physical examination * Twice or more * Twice or more *
Performace status * * *
Therapy checklist * * * * *
Hematology (see text) * Twice or more * Twice or more *
Chemistry (see text) * Twice or more * Twice or more *
Bone marrow
punction1
* * *
Send BM and PB to
reference laboratory
* * *
Send bone marrow to
Amsterdam for drug
resistance studies
(research)
*
BM and PB for MRD
(central laboratories;
research)
* * *
Lumbar puncture * *
Echocardiography * *
1In case of a dry tap, perform a biopsy
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 44 -
Cardiotoxicity monitoring
Why: to determine possible short- and long-term cardiotoxicity, and to detect any differences in
the incidence and severity of cardiotoxicity in patients who did or did not receive liposomal
daunorubicin.
When: Echocardiography should be performed within 1 week before start of reinduction
treatment, within 1 week prior to the second course (FLAG), within 1 week prior to the
conditioning regimen as part of SCT, and 6 months after SCT. In case of a normal FS of >28%,
then repeat echocardiography every 3 years (earlier if clinically indicated). In case of an abnormal
FS, then repeat echocardiography at least every year. Additional echocardiography (and other
monitoring) may be indicated in case of growth spurt, involvement in regular strenuous exercise,
growth hormone and/or sex hormone replacement therapy and in case of pregnancy.
How: M-mode echo measurements according to the American Heart Association guidelines.
Whenever possible, the patient should be afebrile and have a normal haemoglobin (>9 g/dl, >5.6
mmol/l). If an ECG is not recorded simultaneously with M-mode echo, greatest and least LV
dimensions should be used for diastolic and systolic measurements respectively. Please note the
date of each scan, along with the height, body weight, and three blood pressure measurements
(preferably obtained during the last part or immediately after the echo; ensure that the cuff is in
place before starting the echocardiography), as well as initials, gender, race, and identification
number.
Please save all the information of one patient on one (or more) tape (VHS/S-VHS) to allow central
review at a later stage. At least, save the recordings on tape, and note which type of echo-
machine was used.
What:
- Attach ECG
- Baseline echocardiogram: apical 4 chamber view
apical 5 chamber view (with aorta)
short axis left ventricle (papillary muscle level)
short axis left ventricule (aortic valve/pulmonary
artery level)
- Baseline colour Doppler: apical 4 chamber (mitral, tricuspid, aortic flows)
- Pulsed Doppler: aortic flow (measurement of LVET)
mitral valve (tips of mitral valve leaflets)
- M-mode: left ventricle – parasternal long axis
M-mode cursor perpendicular to interventricular septum in a plane where the mitral valve and
aorta (aortic valve) are visible
M-mode cursor immediately below tips of mitral valve
Confirm on tape that the M-mode cursor is positioned correctly
M-mode recording of aortic valve opening (for LVET) if aortic Doppler was not obtained (see
above)
Record a minimum of 10 good quality cardiac cycles
Record blood pressure (see above)
Fractional Shortening will be used as main measurement of cardiac function.

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 45 -
References
Bernstein ID. Monoclonal antibodies to the myeloid stem cells: therapeutic implications of CMA-676, a humanized anti-
CD33 antibody calicheamicin conjugate. Leukemia 2000, 14: 474-475
Bernstein ID, Singer JW, Andrews RG, Keating A, Powell JS, Bjornson BH, Cuttner J, Najfeld V, Reaman G, Raskind W.
Treatment of acute myeloid leukemia cells in vitro with a monoclonal antibody recognizing a myeloid differentiation antigen
allows normal progenitor cells to be expressed. J Clin Invest 1987, 79: 1153-1159
Braess J, Wegendt C, Jahns-Streubel G, Kern W, Keye S, Unterhalt M, Schleyer E, Hiddemann W. Succesful modulation
of high-dose cytosine arabinoside metabolism in acute myeloid leukaemia by haematopietic growth factors: no effect of
ribonucleotide reductase inhibitors fludarabine and gemcitabine. Br J Haematol 2000, 109: 388-395
Chen S-H, Liang D-C, Liu H-C. High-dose cytarabine-containing chemotherapy with or without granulocyte colony-
stimulating factor for children with acute leukemia. Am J Hematol 1998, 58 : 20-23
Corbett TH, Griswold DP Jr, Roberts BJ, Peckham JC, Schabel EM Jr. Biology and therapeutic response of a mouse
mammary adenocarcinoma (16/C) and its potential as a model for surgical adjuvant chemotherapy. Cancer Treat Rep
1978, 62: 1471-1488
Creutzig U, Ritter J, Schellong G, for the AML-BFM Study Group. Identification of two risk groups in childhood acute
myelogenous leukemia after therapy intensification in study AML-BFM-83 as compared with study AML-BFM-78. AML-
BFM Study Group. Blood 1990, 75: 1932-1940
Creutzig U, Harbott J, Sperling C, Ritter J, Zimmermann M, Loffler H, Riehm H, Schellong G, Ludwig WD. Clinical
significance of surface antigen expression in children with acute myeloid leukemia: results of study AML-BFM-87. Blood
1995, 86: 3097-3108
Estey E, Thall P, Andreeff M, Beran M, Kantarjian H, O’Brien S, Escudier S, Robertson LE, Koller C, Kornblau S, Pierce
S, Freireich EJ, Deisseroth A, Keating MJ. Use of granulocyte colony-stimulating factor before, during and after
fludarabine plus cytarabine induction therapy of newly diagnosed acute myelogenous leukemia or myelodysplastic
syndromes: comparison with fludarabine plus cytarabine without granulocyte colony-stimulating factor. J Clin Oncol 1994,
12: 671-678
Fleischhack G, Hasan C, Graf N, Mann G, Bode U. IDA-FLAG (idarubicin, fludarabine, cytarabine, G-CSF): an effective
remission-induction therapy for poor-prognosis AML of childhood prior to allogeneic or autologous bone marrow
transplantation. Experiences of a phase II trial. Br J Haematol 1998, 102: 647-655
Forssen EA, Coulter DM, Proffitt RT. Selective in vivo localization of daunorubicin small unilamellar vesicles in solid
tumors. Cancer Res 1992, 52: 3255-3261
Forssen EA, Ross ME. DaunoXome® treatment of solid tumors: preclinical and clinical investigations. J Liposome Res
1994, 4: 481-512
Gandhi V, Estey E, Keating MJ, Plunkett W. Fludarabine potentiates metabolism of cytarabine in patients with acute
myelogenous leukemia during therapy. J Clin Oncol 1993, 11: 116-124
Gandhi V, Estey E, Du M, Nowak B, Keating MJ, Plunkett W. Modulation of the cllular metabolism of cytarabine and
fludarabine by granulocyte-colony-stimulating factor during therapy of acute myelogenous leukemia. Clin Cancer res 1995,
1: 169-178
Gill PS, Wernz J, Scadden DT, Cohen P, Mukwaya GM, Von Roenn JH, Jacobs M, Kempin S, Silverberg I, Gonzales G,
Rarick MU, Myers AM, Shepherd F, Sawka C, Pike MC, Ross ME. Randomized phase III trial of liposomal daunorubicin
versus doxorubicin, bleomycin, and vincristine in AIDS-related Kaposi’s sarcoma. J Clin Oncol 1996, 14: 2353-2364
Godwin JE, Kopecky KJ, Head DR, Willman CL, Leith CP, Hynes HE, Balcerzak SP, Appelbaum FR. A double-blind-
placebo-controlled trial of granulocyte colony-stimulating factor in elderly patients with previously untreated acute myeloid
leukemia: a Southwest Oncology Group study (9031). Blood 1998, 91: 3607-3615
Guiot HF, Van Den Broek PJ, Van Der Meer JW, Van Furth R. Selective antimicrobial modulation of the intestinal flora of
patients with acute nonlymphocytic leukemia: a double-blind, placebo-controlled study. J Infect Dis 1983, 147: 615-623
Heil G, Hoelzer D, Sanz MA, and 9 others, for the International Acute Myeloid Leukemia Study group. A randomized,
double-blind, plecabo-controlled, phase III study of Filgrastim in remission induction and consolidation therapy for adults
with de novo acute myeloid leukemia. Blood 1997, 90: 4710-4718

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 46 -
Hinman LM, Hamann PR, Wallace R, Menendez AT, Durr FE, Upeslacis J. Preparation and characterization of
monoclonal antibody conjugates of the calicheamicins: a novel and potent family of antitumor antibiotics. Cancer Res
1993, 53: 3336-3342
Hughes WT, Rivera GK, Schell MJ, Thornton D, Lott L. Successful intermittent chemoprophylaxis for Pneumocystis carinii
pneumonitis. N Engl J Med. 1987, 316: 1627-1632
Kaspers GJL, Zwaan ChM, Veerman AJP, Rots MG, Pieters R, Bucsky P, Domula M, Göbel U, Graf N, Havers W, Jorch
N, Kabisch K, Spaar HJ, Ritter J, Creutzig U. Cellular drug resistance in acute myeloid leukemia: literature review and
preliminary analysis of an ongoing collaborative study. Klin Padiatr 1999, 211: 239-244
Klumper E, Pieters R, Kaspers GJL, Huismans DR, Loonen AH, Rottier MMA, Van Wering ER, Van Der Does-Van Den
Berg A, Hählen K, Creutzig U, Veerman AJP. In vitro chemosensitivity assessed with the MTT assay in childhood acute
non-lymphoblastic leukemia. Leukemia 1995, 9: 1864-1869
Levitt GA. Cardioprotection. Br J Haematol 1999, 106: 860-869
Lipshultz SE, Colan SD, Gelber RD, Perez-Atayde AR, Sallan SE, Sanders SP. Late cardiac effects of doxorubicin therapy
for acute lymphoblastic leukemia in children. N Engl J Med 1991, 324: 808-815
Locatelli F, Pession A, Bonetti F, Maserati E, Prete L, Pedrazzoli E, Zecca M, Prete A, Paoluci P, Cazzola M. Busulfan,
cyclophosphamide and melphalan as conditioning regimen for bone marrow transplantation in children with
myelodysplastic syndrome. Leukemia 1994, 8: 844-849
McCarthy AJ, Pitcher LA, Hann IM, Oakhill A. FLAG (Fludarabine, high-dose cytarabine, and G-CSF) for refractory and
high-risk acute leukemia in children. Med Pediatr Oncol 1999, 32: 411-415
Ravindranath Y, Yeager AM, Chang MN, Steuber CP, Krischer J, Graham-Pole J, Carroll A, Inoue S, Camitta B, Weinstein
HJ, for the Pediatric Oncology Group. Autologous bone marrow transplantation versus intensive consolidation
chemotherapy for acute myeloid leukemia in childhood. N Engl J Med 1996, 334: 1428-1434
Ribeiro R, Santana VM, Head DR, Jayawardene D, Srivastava AK, Raimondi SC, Hurwitz CA, Mahmoud H, Krance R.
Factors associated with hematologic response to 2-chlorodeoxyadenosine (2-CDA) in de novo pediatric acute myeloid
leukemia. Blood 1996, 88 (Suppl.1): 219a, abstract 866
Riley LC, Hann IM, Wheatley K, Stevens RF. Treatment-related deaths during induction and first remission of acute
myeloid leukaemia in children treated on the Tenth Medical Research Council acute myeloid leukaemia trial (MRC
AML10). The MCR Childhood Leukaemia Working Party. Br J Haematol 1999, 106: 436-444
Santana VM, Hurwitz CA, Blakley RL, Crom WR, Luo X, Roberts WM, Ribeiro R, Mahmoud H, Krance RA. Complete
hematologic remissions induced by 2-chlorodeoxyadenosine in children with newly diagnosed acute myeloid leukemia.
Blood 1994, 84: 1237-1242
Santana VM, Mirro JJ, Harwood FC, Cherrie J, Schell M, Kalwinsky D, Blakley RL. A phase I clinical trial of 2-
chlorodeoxyadenosine in pediatric patients with acute leukemia. J Clin Oncol 1991, 9: 416-422
Sievers EL. Clinical studies of new "biologic" approaches to therapy of acute myeloid leukemia with monoclonal antibodies
and immunoconjugates. Curr Opin Oncol 2000, 12: 30-35
Sievers EL, Larson RA, Stadtmauer EA, Estey E, Lowenberg B, Dombret H, Karanes C, Theobald M, Bennett JM,
Sherman ML, Berger MS, Eten C, Loken MR, Van Dongen JJM, Bernstein ID, Appelbaum FR, Mylotarg Study Group.
Efficacy and safety of gemtuzumab ozogamicin in patients with CD33-positive acute myeloid leukemia in first relapse. J
Clin Oncol 2001, 19: 3244-3254
Stahnke K, Boos J, Bender-Götze C, Ritter J, Zimmermann M, Creutzig U. Duration of first remission predicts remission
rates and long-term survival in children with relapsed acute myelogenous leukemia. Leukemia 1998, 12: 1534-1538
Stevens RF, Hann IM, Wheatley K, Gray RG, on behalf of the MRC Childhood Leukaemia Working Party. Marked
improvements in outcome with chemotherapy alone in paediatric acute myeloid leukemia: results of the United Kingdom
Medical Research Council's 10th AML trial. Br J Haematol 1998, 101: 130-140
Tafuri A, Andreeff M. Kinetic rationale for cytokine-induced recruitment of myeloblastic leukemia followed by cell-cycle
specific chemotherapy in vitro. Leukemia 1990, 4: 826-834
Tökés ZA, St. Peteri AK, Todd JA. Availability of liposome content to the nervous system. Liposomes and the blood-brain
barrier. Brain Res 1980, 188: 282-286
Webb DKH. Management of relapsed acyte myeloid leukaemia. Br J Haematol 1999, 106: 851-859

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 47 -
Webb DK, Wheatley K, Harrison G, Stevens RF, Hann IM, for the MRC Childhood Leukaemia Working Party. Outcome for
children with relapsed acute myeloid leukaemia following initial therapy in the Medical Research Council (MRC) AML 10
trial. MRC Childhood Leukaemia Working Party. Leukemia 1999, 13: 25-31
Whitlock JA, Wells RJ, Hord JD, Janco RL, Greer JP, Gay JC, Edwards JR, McCurley TL, Lukens JN. High-dose cytosine
arabinoside and etoposide: an effective regimen without anthracyclines for refractory chlidhood acute non-lymphocytic
leukemia. Leukemia 1997, 11: 185-189
Woods WG, Kobrinsky N, Buckley JD, Lee JW , Sanders J, Neudorf S, Gold S, Barnard DR, DeSwarte J, Dusenbery K,
Kalousek D, Arthur DC, Lange BJ. Timed-sequential induction therapy improves postremission outcome in acute myeloid
leukemia: a report from the Children's Cancer Group. Blood 1996, 87: 4979-4989
Woods WG, Neudorf S, Gold S, Sanders J, Buckley JD, Barnard DR, Dusenbery K, DeSwarte J, Arthur DC, Lange BJ,
Kobrinsky NL. A comparison of allogeneic bone marrow transplantation, autologous bone marrow transplantation, and
aggressive chemotherapy in children with acute myeloid leukemia in remission: a report from the Children’s Cancer Group.
Blood 2001, 97: 56-62
Zucchetti M, Boiardi A, Silvani A, Parisi I, Piccolrovazzi S, D’Incalci M. Distribution of daunorubicin and daunorubicinol in
human glioma tumors after administration of liposmal daunorubicin. Cancer Chemother Pharmacol 1999, 44: 173-176
Zwaan ChM, Kaspers GJL, Pieters R, Ramakers-Van Woerden NL, Den Boer ML, Wünsche R, Rottier MMA, Hählen K,
Van Wering E.R., Janka-Schaub GE, Creutzig U, Veerman AJP. Cellular drug resistance profiles in childhood acute
myeloid leukemia: differences between FAB types and comparison with acute lymphoblastic leukemia. Blood 2000, 96:
2879-2886

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 48 -
Acute event form
To: International Data Office
FAX: +49 – 511 532 9029
E-mail: [email protected]
And to: Local Data Office of the Own Group
FAX:
E-mail:
Date:
This is to inform you that we have observed a serious adverse event in a patient with relapsed or
refractory AML
Reporting pediatric oncologist/treating physician:
Name:
Center:
Phone:
Fax:
E-mail:
Please indicate:
- death Y/N
- life-threatening Y/N
- permanently disabling Y/N
Comments:
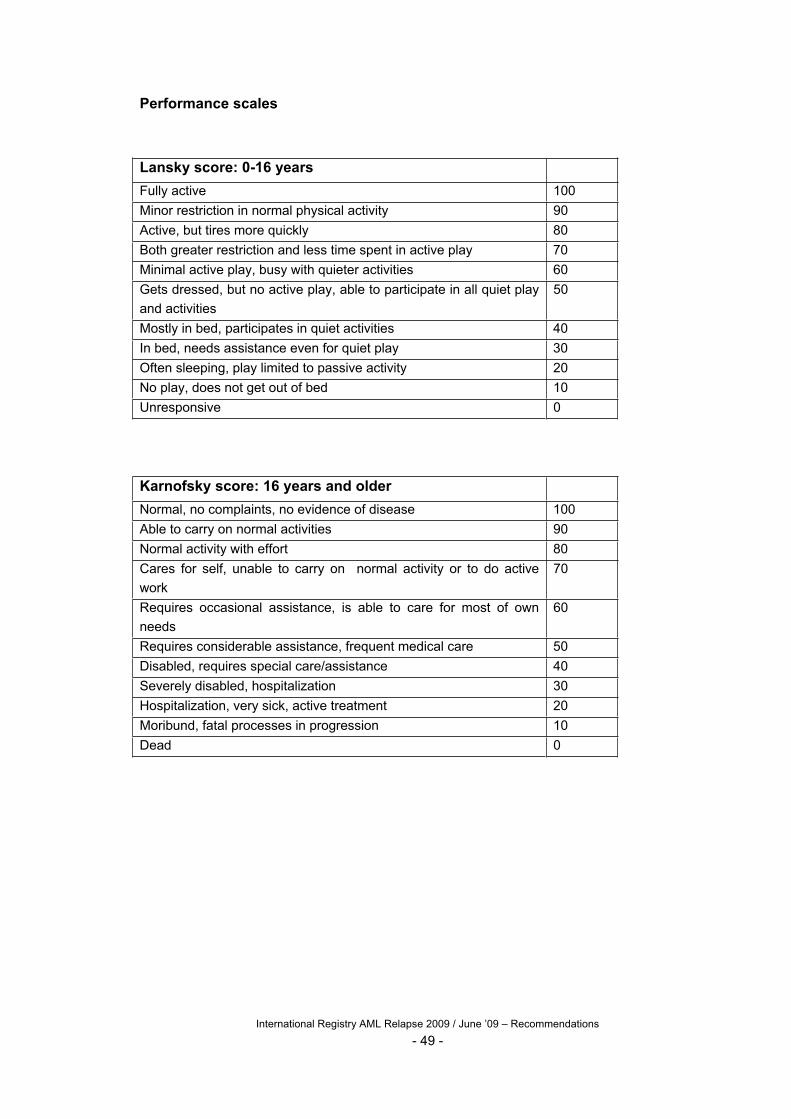
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 49 -
Performance scales
Lansky score: 0-16 years
Fully active 100
Minor restriction in normal physical activity 90
Active, but tires more quickly 80
Both greater restriction and less time spent in active play 70
Minimal active play, busy with quieter activities 60
Gets dressed, but no active play, able to participate in all quiet play
and activities
50
Mostly in bed, participates in quiet activities 40
In bed, needs assistance even for quiet play 30
Often sleeping, play limited to passive activity 20
No play, does not get out of bed 10
Unresponsive 0
Karnofsky score: 16 years and older
Normal, no complaints, no evidence of disease 100
Able to carry on normal activities 90
Normal activity with effort 80
Cares for self, unable to carry on normal activity or to do active
work
70
Requires occasional assistance, is able to care for most of own
needs
60
Requires considerable assistance, frequent medical care 50
Disabled, requires special care/assistance 40
Severely disabled, hospitalization 30
Hospitalization, very sick, active treatment 20
Moribund, fatal processes in progression 10
Dead 0
International Registry AML Relapse 2009 / June ’09 – Recommendations
- 50 -
Reference List
1. Fleischhack G, Hasan C, Graf N, Mann G, Bode U. IDA-FLAG (idarubicin, fludarabine,
cytarabine, G-CSF), an effective remission-induction therapy for poor-prognosis AML of
childhood prior to allogeneic or autologous bone marrow transplantation: experiences of a phase II
trial. Br J Haematol. 1998;102:647-655.
2. Fleischhack G, Graf N, Hasan C, Ackermann M, Breu H, Zernikow B, Bode U. [IDA-FLAG
(idarubicin, fludarabine, high dosage cytarabine and G-CSF)--an effective therapy regimen in
treatment of recurrent acute myelocytic leukemia in children and adolescents. Initial results of a
pilot study]. Klin Padiatr. 1996;208:229-235.
3. Reinhardt D, Hempel G, Fleischhack G, Schulz A, Boos J, Creutzig U. [Liposomal daunorubicine
combined with cytarabine in the treatment of relapsed/refractory acute myeloid leukemia in
children]. Klin Padiatr. 2002;214:188-194.
4. Yavuz S, Paydas S, Disel U, Sahin B. IDA-FLAG regimen for the therapy of primary refractory
and relapse acute leukemia: a single-center experience. Am J Ther. 2006;13:389-393.
5. Viniou NA, Vassilakopoulos TP, Giakoumi X, Mantzouranis M, Pangalis GA. Ida-FLAG plus
imatinib mesylate-induced molecular remission in a patient with chemoresistant Ph1+ acute
myeloid leukemia. Eur J Haematol. 2004;72:58-60.
6. de la RJ, Regadera A, Martin G, Cervera J, Sanz G, Martinez J, Jarque I, Garcia I, Andreu R,
Moscardo F, Jimenez C, Molla S, Benlloch L, Sanz M. FLAG-IDA regimen (fludarabine,
cytarabine, idarubicin and G-CSF) in the treatment of patients with high-risk myeloid
malignancies. Leuk Res. 2002;26:725-730.
7. Luczynski W, Muszynska-Roslan K, Krawczuk-Rybak M, Kuzmicz M, Iwaszkiewicz-Pawlowska
A, Kaliszewski J. Results of IDA-FLAG programme in the treatment of recurrent acute
myeloblastic leukaemia--preliminary report. Med Sci Monit. 2001;7:125-129.
8. Steinmetz HT, Schulz A, Staib P, Scheid C, Glasmacher A, Neufang A, Franklin J, Tesch H, Diehl
V, Dias WP. Phase-II trial of idarubicin, fludarabine, cytosine arabinoside, and filgrastim (Ida-
FLAG) for treatment of refractory, relapsed, and secondary AML. Ann Hematol. 1999;78:418-425.
9. Latagliata R, Breccia M, Fazi P, Iacobelli S, Martinelli G, Di Raimondo F, Sborgia M, Fabbiano F,
Pirrotta MT, Zaccaria A, Amadori S, Caramatti C, Falzetti F, Candoni A, Mattei D, Morselli M,
Alimena G, Vignetti M, Baccarani M, Mandelli F. Liposomal daunorubicin versus standard
daunorubicin: long term follow-up of the GIMEMA GSI 103 AMLE randomized trial in patients
older than 60 years with acute myelogenous leukaemia. Br J Haematol. 2008;143:681-689.
10. Camera A, Rinaldi CR, Palmieri S, Cantore N, Mele G, Mettivier V, Miraglia E, Mastrullo L,
Grimaldi F, Luciano L, Guerriero A, Rotoli B, Ferrara F. Sequential continuous infusion of
fludarabine and cytarabine associated with liposomal daunorubicin (DaunoXome) (FLAD) in
primary refractory or relapsed adult acute myeloid leukemia patients. Ann Hematol. 2009;88:151-
158.
11. Fassas A, Anagnostopoulos A. The use of liposomal daunorubicin (DaunoXome) in acute myeloid
leukemia. Leuk Lymphoma. 2005;46:795-802.
12. Clavio M, Venturino C, Pierri I, Garrone A, Miglino M, Canepa L, Balleari E, Balocco M,
Michelis GL, Ballerini F, Gobbi M. Combination of liposomal daunorubicin (DaunoXome),
fludarabine, and cytarabine (FLAD) in patients with poor-risk acute leukemia. Ann Hematol.
2004;83:696-703.
13. Russo D, Piccaluga PP, Michieli M, Michelutti T, Visani G, Gugliotta L, Bonini A, Pierri I, Gobbi
M, Tiribelli M, Fanin R, Piccolrovazzi S, Baccarani M. Liposomal daunorubicin (DaunoXome) for
treatment of poor-risk acute leukemia. Ann Hematol. 2002;81:462-466.
14. Piccaluga PP, Visani G, Martinelli G, Isidori A, Malagola M, Rondoni M, Baccarani M, Tura S.
Liposomal daunorubicin (DaunoXome) for treatment of relapsed meningeal acute myeloid
leukemia. Leukemia. 2002;16:1880-1881.
15. Muggia FM. Liposomal encapsulated anthracyclines: new therapeutic horizons. Curr Oncol Rep.
2001;3:156-162.
16. Kaspers GJ, Zimmermann M, Fleischhack G, Tamminga R, Gibson B, Armendariz H et al.
Relapsed Acute Myeloid Leukemia in Children and Adolescents: Interim Results of the
International Randomised Phase III Study Relapsed AML 2001/01. 5th Bi-annual Symposium on
Childhood Leukemia, Noordwijkerhout, The Netherlands: 2006.

International Registry AML Relapse 2009 / June ’09 – Recommendations
- 51 -
17. Kaspers GJ, Zimmerman M, Fleischhack G et al. Relapsed Acute Myeloid Leukemia in Children
and Adolescents: Interim Report of the International Randomised Phase III Study Relapsed AML
2001/01 [abstract]. Blood. 2006;108:570a.
18. Kaspers GJ, Zimmermann M, Reinhardt D et al. Prognostic Significance of Early Treatment
Response in Pediatric Relapsed Acute Myeloid Leukemia: Results from the International Study
Relapsed AML 2001/01 [abstract]. Blood. 2007;110:546a.
19. Kaspers GJL, Zimmermann M, Reinhardt D et al. Clinical Relevance of Early Treatment Response
in Pediatric Relapsed Acute Myeloid Leukemia (AML): Study Relapsed AML 2001/01 [abstract].
Ann Hematol. 2008;87:S2.
20. Kaspers GJL, Zimmermann M, Reinhardt D et al. Prognostic Significance of Time to Relapse in
Pediatric AML: Results from the International Randomised Phase III Study Relapsed AML
2001/01 [abstract]. Blood. 2008;112:1022-1023.
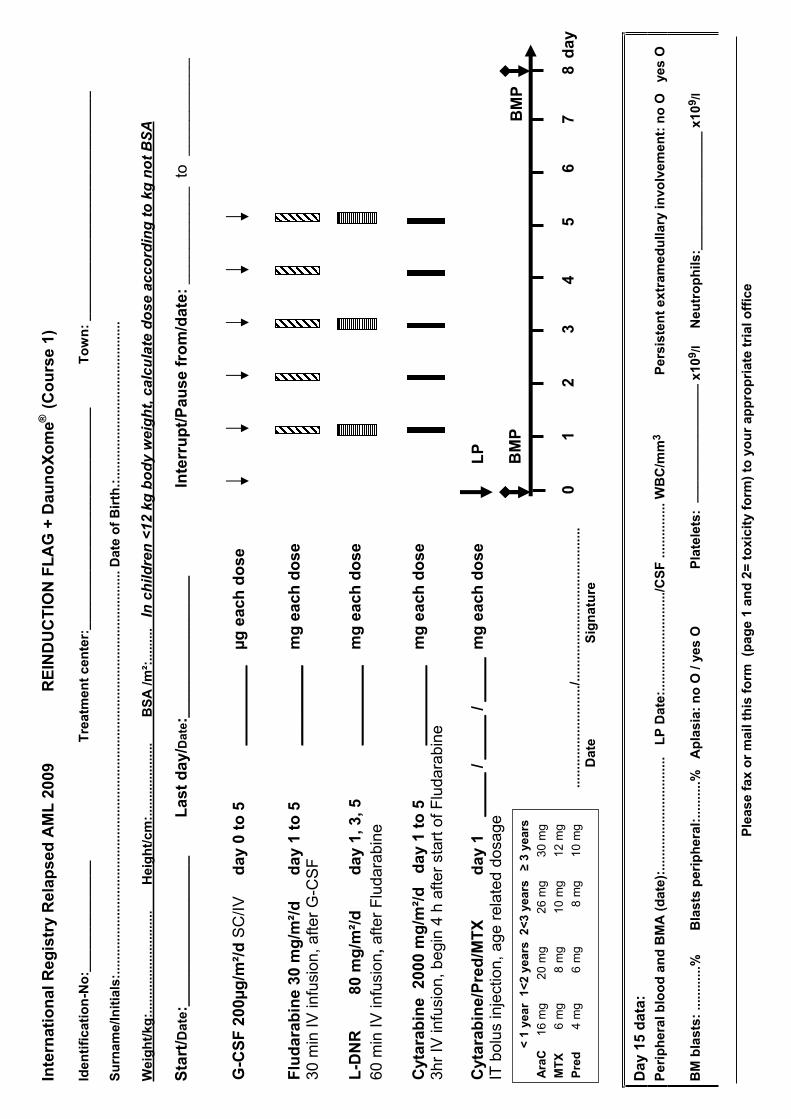
Ple
ase f
ax o
r m
ail
this
fo
rm (
pag
e 1
an
d 2
= t
oxic
ity
form
) to
yo
ur
ap
pro
pri
ate
tri
al o
ffic
e
Inte
rna
tio
na
l R
eg
istr
y R
ela
ps
ed
AM
L 2
00
9
RE
IND
UC
TIO
N F
LA
G +
Da
un
oX
om
e®(C
ou
rse
1)
Ide
nti
fic
ati
on
-No
:__
__
__
__
__
__
__
_T
rea
tme
nt
ce
nte
r:_
__
__
__
__
__
__
__
__
__
__
__
__
__
__
_
To
wn
: _
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
Su
rnam
e/In
itia
ls:.
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
. Dat
e o
f B
irth
.:...
......
......
......
......
......
......
....
Wei
gh
t/kg
:....
......
......
......
......
Hei
gh
t/cm
:....
......
......
....
B
SA
/m²:
......
...In
ch
ild
ren
<1
2 k
g b
od
y w
eig
ht,
ca
lcu
late
do
se
ac
co
rdin
g t
o k
g n
ot
BS
A
Sta
rt/D
ate
:___
____
____
____
__
Las
t d
ay/D
ate:
________________
Inte
rru
pt/
Pau
se f
rom
/date
: ___________
to
___________
Da
y 1
5 d
ata
: P
eri
ph
era
l blo
od
an
d B
MA
(d
ate)
:....
......
......
......
......
...L
P D
ate:
......
......
......
......
.../C
SF
.....
......
.... W
BC
/mm
3P
ers
iste
nt
extr
am
ed
ullary
invo
lvem
en
t: n
o O
ye
s O
BM
bla
sts:
.....
......
.%
Bla
sts
per
iph
eral
:....
......
%A
pla
sia:
no
O /
yes
O
Pla
tele
ts:
__
__
__
__
__
__
__
__
x10
9/l
Ne
utr
op
hil
s:_
__
__
__
__
__
__
__
_ x
10
9/l
day
LP
BM
P
0
1
2
3
4
5
6
7
8
BM
P
G-C
SF
20
0µ
g/m
²/d
SC
/IV
da
y 0
to
5
__
__
__
__
_ µ
g e
ach
do
se
Flu
da
rab
ine
30
mg
/m²/
d
d
ay
1 t
o 5
_
__
__
__
__
mg
each
do
se
30
min
IV
infu
sio
n,
aft
er
G-C
SF
L-D
NR
80
mg
/m²/
d
d
ay
1,
3,
5
__
__
__
__
_ m
g e
ach
do
se
60 m
in I
V in
fusi
on,
after
Flu
dara
bin
e
Cyt
ara
bin
e
20
00
mg
/m²/
d
da
y 1
to
5
__
__
__
__
_ m
g e
ach
do
se
3h
r IV
infu
sio
n,
be
gin
4 h
aft
er
sta
rt o
f F
lud
ara
bin
e
Cyt
ara
bin
e/P
red
/MT
X
d
ay
1
_
__
__
/ _
__
__
/ _
__
__
mg
each
do
se
IT b
olu
s in
ject
ion,
age r
ela
ted d
osa
ge
...
......
......
......
......
./....
......
......
......
......
......
......
..
D
ate
Sig
nat
ure
< 1
ye
ar
1<
2 y
ea
rs
2<
3 y
ea
rs
3
yea
rs
Ara
C
16 m
g
20 m
g
26 m
g
30 m
g
MT
X
6 m
g
8 m
g
10 m
g
12 m
g
Pre
d
4 m
g
6 m
g
8 m
g
10 m
g
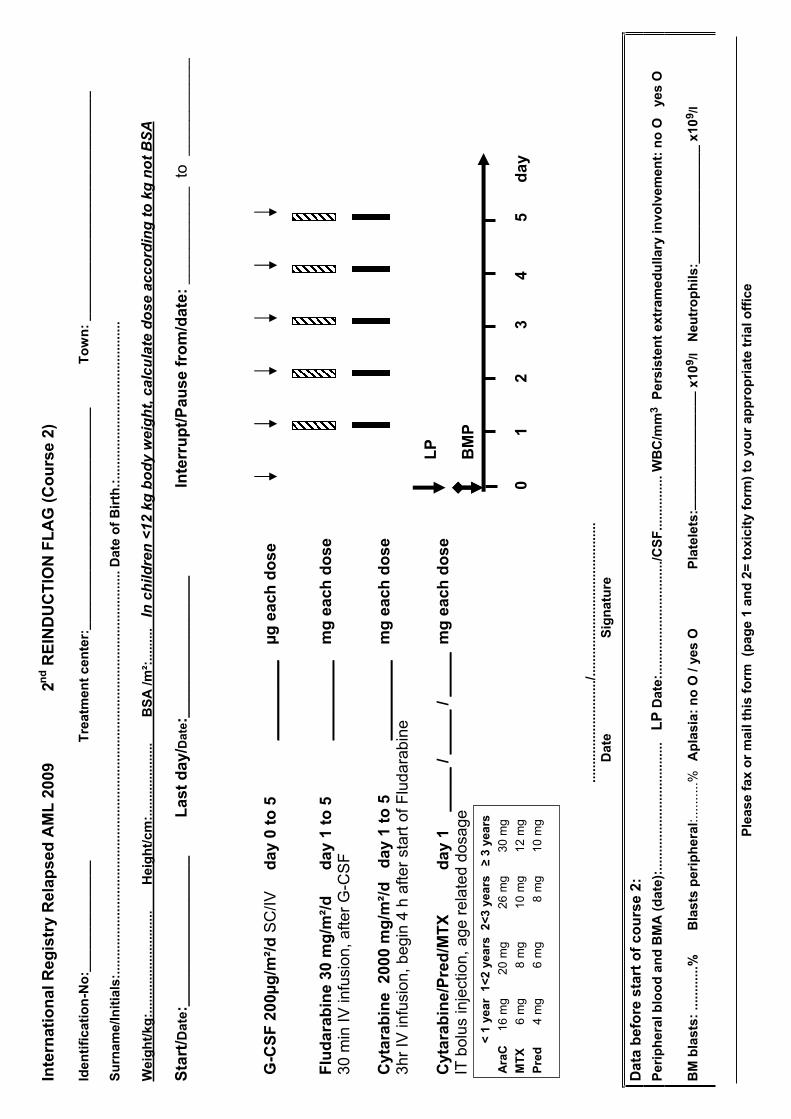
Ple
ase f
ax o
r m
ail
this
fo
rm (
pag
e 1
an
d 2
= t
oxic
ity
form
) to
yo
ur
ap
pro
pri
ate
tri
al o
ffic
e
Inte
rna
tio
na
l R
eg
istr
y R
ela
ps
ed
AM
L 2
00
9
2n
d R
EIN
DU
CT
ION
FL
AG
(C
ou
rse 2
)
Ide
nti
fic
ati
on
-No
:__
__
__
__
__
__
__
_T
rea
tme
nt
ce
nte
r:_
__
__
__
__
__
__
__
__
__
__
__
__
__
__
_
To
wn
: _
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
Su
rnam
e/In
itia
ls:.
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
. Dat
e o
f B
irth
.:...
......
......
......
......
......
......
....
Wei
gh
t/kg
:....
......
......
......
......
Hei
gh
t/cm
:....
......
......
....
B
SA
/m²:
......
...In
ch
ild
ren
<1
2 k
g b
od
y w
eig
ht,
ca
lcu
late
do
se
ac
co
rdin
g t
o k
g n
ot
BS
A
Sta
rt/D
ate
:___
____
____
____
__
Las
t d
ay/D
ate:
________________
Inte
rru
pt/
Pau
se f
rom
/date
: ___________
to
___________
Da
ta b
efo
re s
tart
of
co
urs
e 2
:
Per
iph
eral
blo
od
an
d B
MA
(d
ate
):...
......
......
......
......
......
..L
P D
ate:
......
......
......
......
......
./CS
F...
......
......
WB
C/m
m3
Pers
iste
nt
extr
am
ed
ullary
invo
lvem
en
t: n
o O
ye
s O
BM
bla
sts:
.....
......
.%
Bla
sts
per
iph
eral
:..........%
Ap
lasia
: n
o O
/ ye
s O
P
late
lets
:__
__
__
__
__
__
__
__
x10
9/l
Neu
tro
ph
ils:_
_______________ x
10
9/l
0
1
2
3
4
5
d
ay
LP
BM
P
G-C
SF
20
0µ
g/m
²/d
SC
/IV
da
y 0
to
5
__
__
__
__
_ µ
g e
ach
do
se
Flu
da
rab
ine
30
mg
/m²/
d
d
ay
1 t
o 5
_
__
__
__
__
mg
each
do
se
30
min
IV
infu
sio
n,
aft
er
G-C
SF
Cyt
ara
bin
e
20
00
mg
/m²/
d
da
y 1
to
5
__
__
__
__
_ m
g e
ach
do
se
3h
r IV
infu
sio
n,
be
gin
4 h
aft
er
sta
rt o
f F
lud
ara
bin
e
Cyt
ara
bin
e/P
red
/MT
X
d
ay
1
_
__
__
/ _
__
__
/ _
__
__
mg
each
do
se
IT b
olu
s in
ject
ion,
age r
ela
ted d
osa
ge
...
......
......
......
......
./....
......
......
......
......
......
......
..
D
ate
Sig
nat
ure
< 1
ye
ar
1<
2 y
ea
rs
2<
3 y
ea
rs
3
yea
rs
Ara
C
16 m
g
20 m
g
26 m
g
30 m
g
MT
X
6 m
g
8 m
g
10 m
g
12 m
g
Pre
d
4 m
g
6 m
g
8 m
g
10 m
g

Ple
ase f
ax o
r m
ail
this
fo
rm (
pag
e 1
an
d 2
= t
oxic
ity
form
) to
yo
ur
ap
pro
pri
ate
tri
al o
ffic
e
Inte
rna
tio
na
l R
eg
istr
y R
ela
ps
ed
AM
L 2
00
9
C
ON
SO
LID
AT
ION
- h
igh
in
ten
sit
y
Ide
nti
fic
ati
on
-No
:__
__
__
__
__
__
__
_T
rea
tme
nt
ce
nte
r:_
__
__
__
__
__
__
__
__
__
__
__
__
__
__
_
To
wn
: _
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
Su
rnam
e/In
itia
ls:.
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
. Dat
e o
f B
irth
.:...
......
......
......
......
......
......
....
Wei
gh
t/kg
:....
......
......
......
......
Hei
gh
t/cm
:....
......
......
....
B
SA
/m²:
......
...In
ch
ild
ren
<1
2 k
g b
od
y w
eig
ht,
ca
lcu
late
do
se
ac
co
rdin
g t
o k
g n
ot
BS
A
Sta
rt/D
ate
:___
____
____
____
__
Las
t d
ay//D
ate:
________________
Inte
rru
pt/
Pau
se f
rom
/date
: ___________
to
___________
No
te:
Sta
rt n
ot
ea
rlie
r th
an
28
d a
fte
r s
tart
of
rein
du
cti
on
co
urs
e 2
, a
nd
on
ly i
f C
R i
s a
ch
iev
ed
, o
the
rwis
e:
off
stu
dy!
Co
nd
itio
ns
: g
oo
d c
lin
ica
l c
on
dit
ion
, p
late
lets
>5
0 x
109
/l,
ne
utr
op
hil
s >
1,0
x 1
09/l
.P
erf
orm
BM
A a
nd
LP
fir
st!
Da
ta b
efo
re s
tart
of
co
ns
oli
da
tio
n:
Peri
ph
era
l blo
od
an
d B
MA
(d
ate
):...
......
......
......
......
......
LP
Dat
e:...
......
......
......
......
..../
CS
F...
......
......
WB
C/m
m3
Pers
iste
nt
extr
am
ed
ullary
invo
lv.:
no
O y
es O
BM
bla
sts:
.....
......
.%
Bla
sts
per
iph
eral
:..........%
Ap
lasia
: n
o O
/ ye
s O
P
late
lets
: _
__
__
__
__
__
__
__
_x
10
9/l
N
eu
tro
ph
ils:_
_______________ x
10
9/l
LP
BM
P
1
2
3
4
5
6
da
y
Cyt
ara
bin
e 5
00 m
g/m
²/d
d
ay
1 t
o 4
_________
mg
ea
ch
da
y 3
0 m
in I
V in
fusi
on
, a
fte
r G
-CS
F96 h
rs c
ontin
ous
IV in
fusi
on
Eto
po
sid
e
100 m
g/m
²/d
d
ay
1 t
o 5
_________
mg
each
do
se
30
min
IV
infu
sio
n,
aft
er
G-C
SF
3hr
IV in
fusi
on
Cyt
ara
bin
e/P
red
/MT
X
da
y 1
__
__
_ /
__
__
_ /
__
__
_ m
g e
ach
do
se
IT b
olu
s in
ject
ion,
age r
ela
ted d
osa
ge
...
......
......
......
......
./....
......
......
......
......
......
......
..
D
ate
Sig
nat
ure
< 1
ye
ar
1<
2 y
ea
rs
2<
3 y
ea
rs
3
yea
rs
Ara
C
16 m
g
20 m
g
26 m
g
30 m
g
MT
X
6 m
g
8 m
g
10 m
g
12 m
g
Pre
d
4 m
g
6 m
g
8 m
g
10 m
g
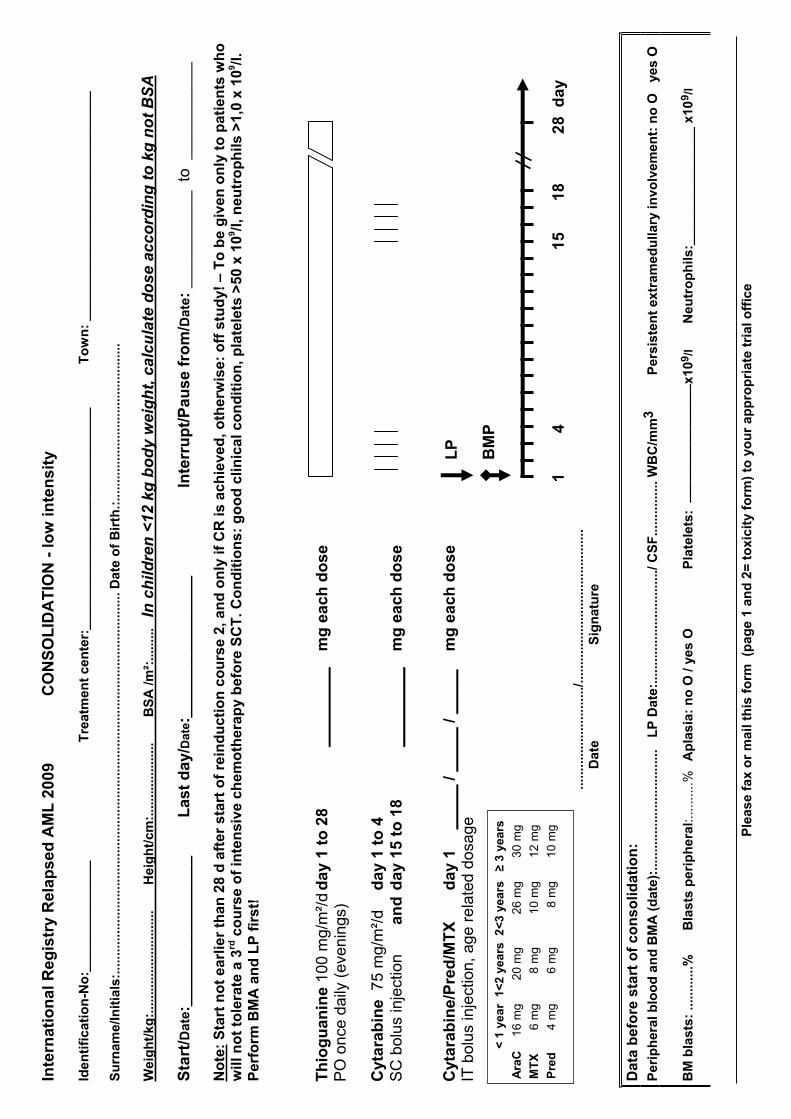
Ple
ase f
ax o
r m
ail
this
fo
rm (
pag
e 1
an
d 2
= t
oxic
ity
form
) to
yo
ur
ap
pro
pri
ate
tri
al o
ffic
e
Inte
rna
tio
na
l R
eg
istr
y R
ela
ps
ed
AM
L 2
00
9
CO
NS
OL
IDA
TIO
N -
lo
w i
nte
ns
ity
Ide
nti
fic
ati
on
-No
:__
__
__
__
__
__
__
_T
rea
tme
nt
ce
nte
r:_
__
__
__
__
__
__
__
__
__
__
__
__
__
__
_
To
wn
: _
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
Su
rnam
e/In
itia
ls:.
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
.Dat
eo
f B
irth
.:...
......
......
......
......
......
......
....
Wei
gh
t/kg
:....
......
......
......
......
Hei
gh
t/cm
:....
......
......
....
B
SA
/m²:
......
... I
n c
hil
dre
n <
12
kg
bo
dy
we
igh
t, c
alc
ula
te d
os
e a
cc
ord
ing
to
kg
no
t B
SA
Sta
rt/D
ate
:___
____
____
____
__
Las
t d
ay/D
ate:
________________
Inte
rru
pt/
Pau
se f
rom
/Da
te:
___________
to
___________
No
te:
Sta
rt n
ot
ea
rlie
r th
an
28
d a
fte
r s
tart
of
rein
du
cti
on
co
urs
e 2
, a
nd
on
ly i
f C
R i
s a
ch
iev
ed
, o
the
rwis
e:
off
stu
dy!
– T
o b
e g
ive
n o
nly
to
pa
tie
nts
wh
o
wil
l n
ot
tole
rate
a 3
rd c
ou
rse
of
inte
ns
ive
ch
em
oth
era
py
be
fore
SC
T.
Co
nd
itio
ns
: g
oo
d c
lin
ica
l c
on
dit
ion
, p
late
lets
>5
0 x
109
/l,
ne
utr
op
hil
s >
1,0
x 1
09/l
.P
erf
orm
BM
A a
nd
LP
fir
st!
Da
ta b
efo
re s
tart
of
co
ns
oli
da
tio
n:
Peri
ph
era
l blo
od
an
d B
MA
(d
ate
):...
......
......
......
......
......
LP
Dat
e:...
......
......
......
......
..../
CS
F...
......
......
WB
C/m
m3
Pers
iste
nt
extr
am
ed
ullary
invo
lvem
en
t: n
o O
ye
s O
BM
bla
sts:
.....
......
.%
Bla
sts
per
iph
eral
:..........%
Ap
lasia
: n
o O
/ ye
s O
P
late
lets
: _
__
__
__
__
__
__
__
_x
10
9/l
N
eu
tro
ph
ils:_
_______________ x
10
9/l
Th
iog
ua
nin
e1
00
mg
/m²/
d d
ay 1
to
28
__
____
___
mg
each
do
se
PO
once
daily
(eve
nin
gs)
Cyt
ara
bin
e
75
mg
/m²/
d
day
1 t
o 4
S
C b
olu
s in
ject
ion
a
nd
day
15 t
o 1
8
_________
mg
each
do
se
Cyt
ara
bin
e/P
red
/MT
X
da
y 1
__
__
_ /
__
__
_ /
__
__
_ m
g e
ach
do
se
IT b
olu
s in
ject
ion,
age r
ela
ted d
osa
ge
...
......
......
......
......
./....
......
......
......
......
......
......
..
D
ate
Sig
nat
ure
< 1
ye
ar
1<
2 y
ea
rs
2<
3 y
ea
rs
3
yea
rs
Ara
C
16 m
g
20 m
g
26 m
g
30 m
g
MT
X
6 m
g
8 m
g
10 m
g
12 m
g
Pre
d
4 m
g
6 m
g
8 m
g
10 m
g
LP
BM
P
1
4
1
5
18
2
8
da
y
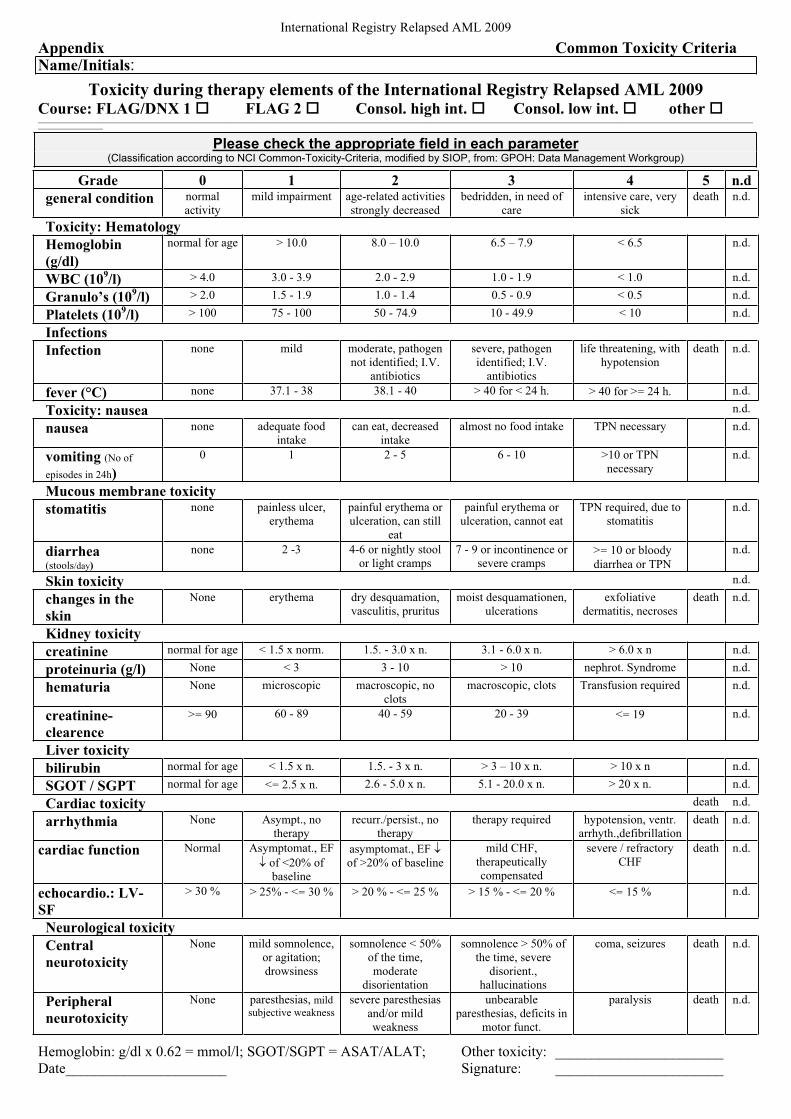
International Registry Relapsed AML 2009
Appendix Common Toxicity Criteria Name/Initials:
Toxicity during therapy elements of the International Registry Relapsed AML 2009 Course: FLAG/DNX 1 FLAG 2 Consol. high int. Consol. low int. other ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Please check the appropriate field in each parameter(Classification according to NCI Common-Toxicity-Criteria, modified by SIOP, from: GPOH: Data Management Workgroup)
Grade 0 1 2 3 4 5 n.d
general condition normal
activity
mild impairment age-related activities
strongly decreased
bedridden, in need of
care
intensive care, very
sick
death n.d.
Toxicity: Hematology
Hemoglobin
(g/dl)
normal for age > 10.0 8.0 – 10.0 6.5 – 7.9 < 6.5 n.d.
WBC (109/l) > 4.0 3.0 - 3.9 2.0 - 2.9 1.0 - 1.9 < 1.0 n.d.
Granulo’s (109/l) > 2.0 1.5 - 1.9 1.0 - 1.4 0.5 - 0.9 < 0.5 n.d.
Platelets (109/l) > 100 75 - 100 50 - 74.9 10 - 49.9 < 10 n.d.
Infections
Infection none mild moderate, pathogen
not identified; I.V.
antibiotics
severe, pathogen
identified; I.V.
antibiotics
life threatening, with
hypotension
death n.d.
fever (°C) none 37.1 - 38 38.1 - 40 > 40 for < 24 h. > 40 for >= 24 h. n.d.
Toxicity: nausea n.d.
nausea none adequate food
intake
can eat, decreased
intake
almost no food intake TPN necessary n.d.
vomiting (No of
episodes in 24h)
0 1 2 - 5 6 - 10 >10 or TPN
necessary
n.d.
Mucous membrane toxicity
stomatitis none painless ulcer,
erythema
painful erythema or
ulceration, can still
eat
painful erythema or
ulceration, cannot eat
TPN required, due to
stomatitis
n.d.
diarrhea(stools/day)
none 2 -3 4-6 or nightly stool
or light cramps
7 - 9 or incontinence or
severe cramps >= 10 or bloody
diarrhea or TPN
n.d.
Skin toxicity n.d.
changes in the
skin
None erythema dry desquamation,
vasculitis, pruritus
moist desquamationen,
ulcerations
exfoliative
dermatitis, necroses
death n.d.
Kidney toxicity
creatinine normal for age < 1.5 x norm. 1.5. - 3.0 x n. 3.1 - 6.0 x n. > 6.0 x n n.d.
proteinuria (g/l) None < 3 3 - 10 > 10 nephrot. Syndrome n.d.
hematuria None microscopic macroscopic, no
clots
macroscopic, clots Transfusion required n.d.
creatinine-
clearence
>= 90 60 - 89 40 - 59 20 - 39 <= 19 n.d.
Liver toxicity
bilirubin normal for age < 1.5 x n. 1.5. - 3 x n. > 3 – 10 x n. > 10 x n n.d.
SGOT / SGPT normal for age <= 2.5 x n. 2.6 - 5.0 x n. 5.1 - 20.0 x n. > 20 x n. n.d.
Cardiac toxicity death n.d.
arrhythmia None Asympt., no
therapy
recurr./persist., no
therapy
therapy required hypotension, ventr.
arrhyth.,defibrillation
death n.d.
cardiac function Normal Asymptomat., EF
of <20% of
baseline
asymptomat., EF
of >20% of baseline
mild CHF,
therapeutically
compensated
severe / refractory
CHF
death n.d.
echocardio.: LV-
SF
> 30 % > 25% - <= 30 % > 20 % - <= 25 % > 15 % - <= 20 % <= 15 % n.d.
Neurological toxicity
Central
neurotoxicity
None mild somnolence,
or agitation;
drowsiness
somnolence < 50%
of the time,
moderate
disorientation
somnolence > 50% of
the time, severe
disorient.,
hallucinations
coma, seizures death n.d.
Peripheral
neurotoxicity
None paresthesias, mild
subjective weakness
severe paresthesias
and/or mild
weakness
unbearable
paresthesias, deficits in
motor funct.
paralysis death n.d.
Hemoglobin: g/dl x 0.62 = mmol/l; SGOT/SGPT = ASAT/ALAT; Other toxicity: _______________________
Date______________________ Signature: _______________________
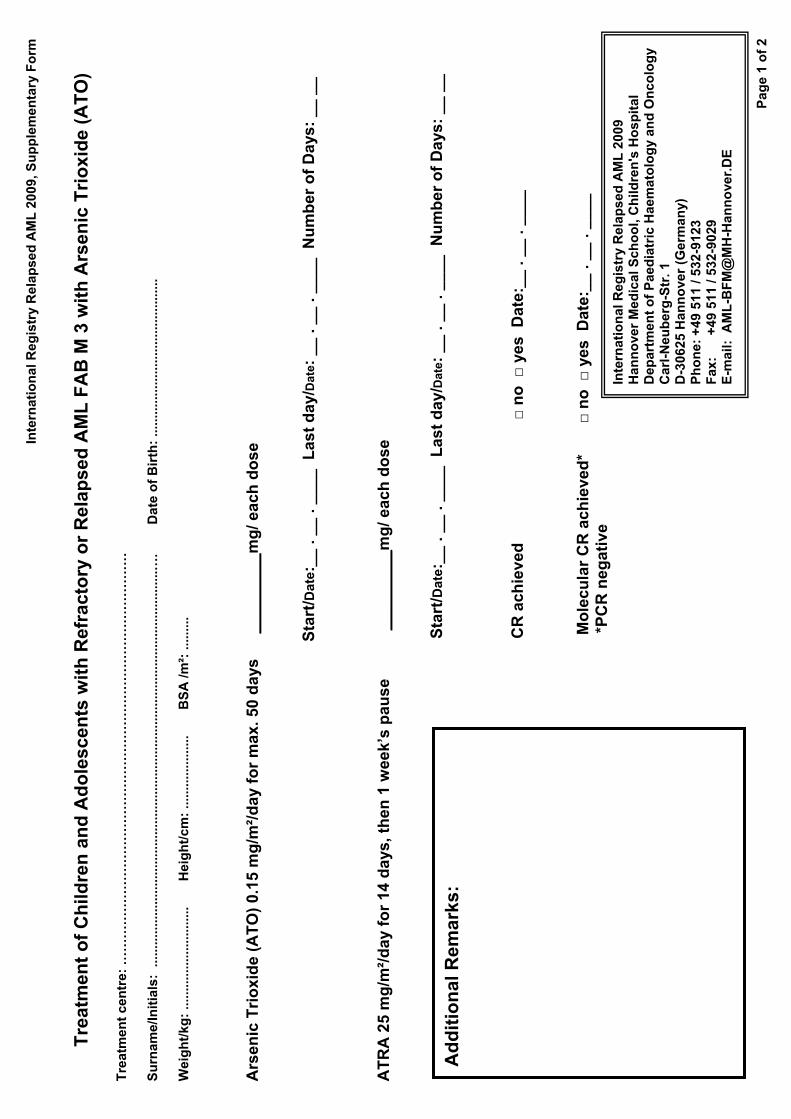
Inte
rnati
on
al R
eg
istr
y R
ela
psed
AM
L 2
009, S
up
ple
men
tary
Fo
rm
Pag
e 1
of
2
Tre
atm
en
t o
f C
hil
dre
n a
nd
Ad
ole
sc
en
ts w
ith
Re
fra
cto
ry o
r R
ela
ps
ed
AM
L F
AB
M 3
wit
h A
rse
nic
Tri
ox
ide
(A
TO
)
Tre
atm
en
t cen
tre:
……
……
……
……
……
……
……
……
……
……
……
……
……
……
……
…
Su
rnam
e/In
itia
ls:
.....
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
.….
Da
te o
f B
irth
: ...
......
......
......
......
......
......
....
Wei
gh
t/kg
: ...
......
......
......
......
. H
eig
ht/
cm:
......
......
......
..
B
SA
/m²:
.....
....
Ars
en
ic T
rio
xid
e (
AT
O)
0.1
5 m
g/m
²/d
ay
for
ma
x.
50
da
ys_
__
__
__
__m
g/
ea
ch
do
se
Sta
rt/ D
ate
:__
. _
_ .
__
__
L
as
t d
ay/
Dat
e: _
_ .
__
. _
__
_
Nu
mb
er
of
Da
ys:
__
__
AT
RA
25
mg
/m²/
da
y fo
r 1
4 d
ays
, th
en
1 w
ee
k’s
pa
us
e
__
__
__
__
_ mg
/ e
ac
h d
os
e
S
tart
/Da
te:_
_ .
__
. _
__
_
La
st
da
y/D
ate:
__
. _
_ .
__
__
N
um
be
r o
f D
ays
: _
_ _
_
CR
ac
hie
ve
d
no
yes
Da
te:_
_ .
__
. _
__
_
Mo
lecu
lar
CR
ach
ieved
* n
o y
esD
ate
:__
. _
_ .
__
__
*P
CR
ne
ga
tiv
e
Ad
dit
ion
al
Re
ma
rks
:
Inte
rnati
on
al R
eg
istr
y R
ela
psed
AM
L 2
009
Han
no
ver
Med
ical S
ch
oo
l, C
hild
ren
's H
osp
ital
Dep
art
men
t o
f P
aed
iatr
ic H
aem
ato
log
y an
d O
nco
log
y C
arl
-Ne
ub
erg
-Str
. 1
D-3
06
25
Ha
nn
ove
r (G
erm
an
y)
Ph
on
e:
+4
9 5
11
/ 5
32
-91
23
Fax:
+
49 5
11 /
532-9
029
E-m
ail:
AM
L-B
FM
@M
H-H
an
no
ver.
DE
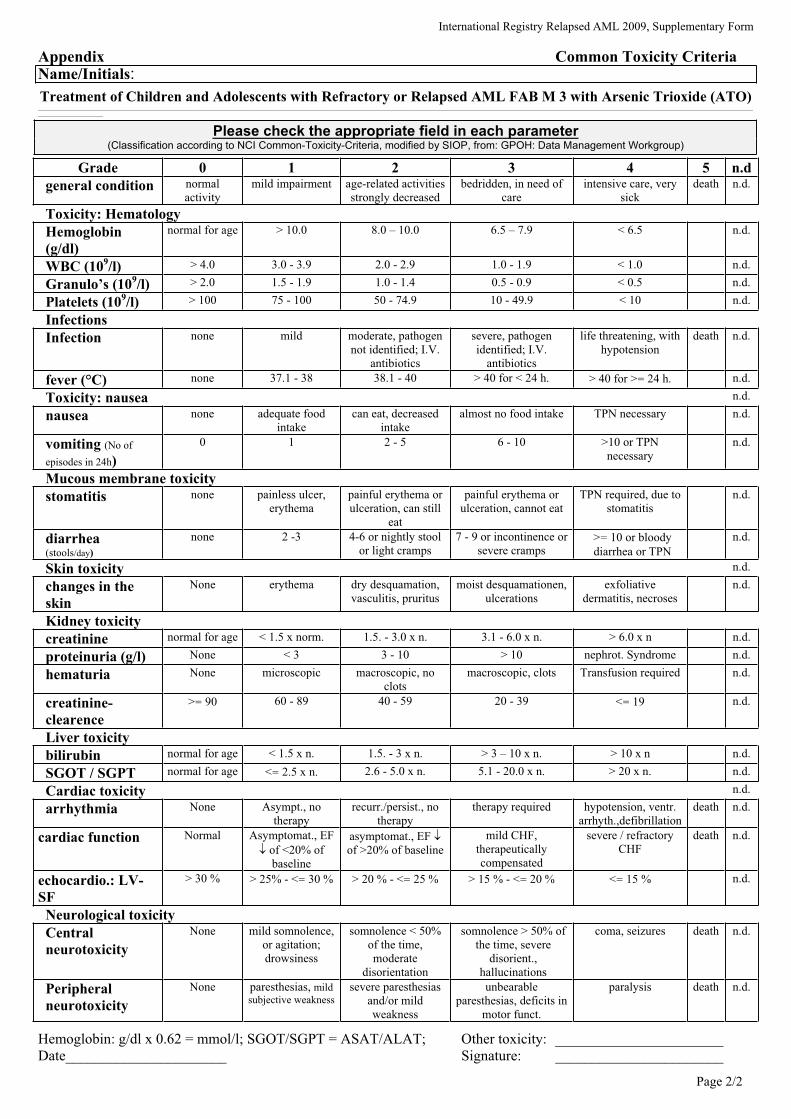
International Registry Relapsed AML 2009, Supplementary Form
Page 2/2
Appendix Common Toxicity Criteria Name/Initials:
Treatment of Children and Adolescents with Refractory or Relapsed AML FAB M 3 with Arsenic Trioxide (ATO)________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Please check the appropriate field in each parameter(Classification according to NCI Common-Toxicity-Criteria, modified by SIOP, from: GPOH: Data Management Workgroup)
Grade 0 1 2 3 4 5 n.d
general condition normal
activity
mild impairment age-related activities
strongly decreased
bedridden, in need of
care
intensive care, very
sick
death n.d.
Toxicity: Hematology
Hemoglobin
(g/dl)
normal for age > 10.0 8.0 – 10.0 6.5 – 7.9 < 6.5 n.d.
WBC (109/l) > 4.0 3.0 - 3.9 2.0 - 2.9 1.0 - 1.9 < 1.0 n.d.
Granulo’s (109/l) > 2.0 1.5 - 1.9 1.0 - 1.4 0.5 - 0.9 < 0.5 n.d.
Platelets (109/l) > 100 75 - 100 50 - 74.9 10 - 49.9 < 10 n.d.
Infections
Infection none mild moderate, pathogen
not identified; I.V.
antibiotics
severe, pathogen
identified; I.V.
antibiotics
life threatening, with
hypotension
death n.d.
fever (°C) none 37.1 - 38 38.1 - 40 > 40 for < 24 h. > 40 for >= 24 h. n.d.
Toxicity: nausea n.d.
nausea none adequate food
intake
can eat, decreased
intake
almost no food intake TPN necessary n.d.
vomiting (No of
episodes in 24h)
0 1 2 - 5 6 - 10 >10 or TPN
necessary
n.d.
Mucous membrane toxicity
stomatitis none painless ulcer,
erythema
painful erythema or
ulceration, can still
eat
painful erythema or
ulceration, cannot eat
TPN required, due to
stomatitis
n.d.
diarrhea(stools/day)
none 2 -3 4-6 or nightly stool
or light cramps
7 - 9 or incontinence or
severe cramps >= 10 or bloody
diarrhea or TPN
n.d.
Skin toxicity n.d.
changes in the
skin
None erythema dry desquamation,
vasculitis, pruritus
moist desquamationen,
ulcerations
exfoliative
dermatitis, necroses
n.d.
Kidney toxicity
creatinine normal for age < 1.5 x norm. 1.5. - 3.0 x n. 3.1 - 6.0 x n. > 6.0 x n n.d.
proteinuria (g/l) None < 3 3 - 10 > 10 nephrot. Syndrome n.d.
hematuria None microscopic macroscopic, no
clots
macroscopic, clots Transfusion required n.d.
creatinine-
clearence
>= 90 60 - 89 40 - 59 20 - 39 <= 19 n.d.
Liver toxicity
bilirubin normal for age < 1.5 x n. 1.5. - 3 x n. > 3 – 10 x n. > 10 x n n.d.
SGOT / SGPT normal for age <= 2.5 x n. 2.6 - 5.0 x n. 5.1 - 20.0 x n. > 20 x n. n.d.
Cardiac toxicity n.d.
arrhythmia None Asympt., no
therapy
recurr./persist., no
therapy
therapy required hypotension, ventr.
arrhyth.,defibrillation
death n.d.
cardiac function Normal Asymptomat., EF
of <20% of
baseline
asymptomat., EF
of >20% of baseline
mild CHF,
therapeutically
compensated
severe / refractory
CHF
death n.d.
echocardio.: LV-
SF
> 30 % > 25% - <= 30 % > 20 % - <= 25 % > 15 % - <= 20 % <= 15 % n.d.
Neurological toxicity
Central
neurotoxicity
None mild somnolence,
or agitation;
drowsiness
somnolence < 50%
of the time,
moderate
disorientation
somnolence > 50% of
the time, severe
disorient.,
hallucinations
coma, seizures death n.d.
Peripheral
neurotoxicity
None paresthesias, mild
subjective weakness
severe paresthesias
and/or mild
weakness
unbearable
paresthesias, deficits in
motor funct.
paralysis death n.d.
Hemoglobin: g/dl x 0.62 = mmol/l; SGOT/SGPT = ASAT/ALAT; Other toxicity: _______________________
Date______________________ Signature: _______________________