intraoperative endodontic applications of cone-beam ... of... · intraoperative endodontic...
TRANSCRIPT

Case Report/Clinical Techniques
Intraoperative Endodontic Applications of Cone-BeamComputed TomographyRandy L. Ball, DMD, Joao V. Barbizam, DDS, MS, PhD, and Nestor Cohenca, DDS
Abstract
Introduction: The use of cone-beam computed tomog-raphy (CBCT) in endodontics for diagnosis, treatmentplanning, and follow-up has been extensively reportedin the literature. Compared with the traditional spiralcomputed tomography, high-resolution limited CBCTresults in a fraction of the effective absorbed dose ofradiation. However, it should be prescribed only afterweighing the cost of radiation exposure with the benefitof the diagnostic information that can be obtained fromthe scan. Methods: The purpose of this article is todiscuss the application and advantages of intraoperativeCBCT in endodontics, while reducing radiation exposureduring complex endodontic procedures. Results: Incases of increased difficulty or intraoperative complica-tions such as complex anatomy, dystrophic calcifica-tions, root resorptions, perforations, and rootfractures, it is prudent to consider the use of CBCTwith its inherent diagnostic value and limited radiationexposure. Conclusions: The benefits of the added diag-nostic information provided by intraoperative CBCTimages in select cases justify the risk associated withthe limited level of radiation exposure. (J Endod2013;39:548–557)Key WordsCBCT, cone-beam computed tomography, diagnosis, in-traoperative, root canal treatment
From the Department of Endodontics and PediatricDentistry, School of Dentistry, University of Washington, Seat-tle, Washington.
Address requests for reprints to Dr Nestor Cohenca, Depart-ment of Endodontics, University of Washington, Box 357448,Seattle, WA 98195-7448. E-mail address: [email protected]/$ - see front matter
Copyright ª 2013 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2012.11.038
548 Ball et al.
Since the first cone-beam volumetric tomography unit was approved for dental use inthe United States in 2000 (1), numerous endodontic applications of this technology,
along with cone-beam computed tomography (CBCT), have been described in the liter-ature. Most of these applications are focused on preoperative assessment and treatmentplanning and include diagnosis and canal morphology (2–4), assessment of internal(2, 4, 5) and external root resorption (4, 6, 7), treatment planning and assessmentof traumatic dental injuries (7, 8), assessment of root fractures (2, 9), presurgicalanatomic assessment (2, 4), and treatment planning for tooth anomalies such asdens invaginatus (10, 11). Comparison studies have shown CBCT to be moreaccurate than conventional periapical radiographs in measurement of the length ofroot fillings (12) and diagnosing the presence of resorption lesions (13–15),periapical bone defects (16–20), root fractures (21–23), and perforations (24). Thesestudies underscore the potential benefits of CBCT in diagnosis and treatment ofendodontic problems.
In 2011, the American Association of Endodontists (AAE) and the AmericanAcademy of Oral andMaxillofacial Radiology (AAOMR) issued a joint position statementregarding the use of CBCT in endodontics (25). The statement emphasizes that the useof CBCT should be prescribed only after weighing the risks of radiation exposure withthe benefit of the diagnostic information that can be obtained from the scan. Also, CBCTshould never be routinely used in every case with every patient, and its prescriptionshould only occur after a thorough clinical examination. In certain circumstances,however, use of limited field of view (FOV) CBCT may actually reduce the potential radi-ation exposure of the patient during the course of endodontic treatment. The statementnotes that the ‘‘use of limited field of view CBCT systems can provide images of severalteeth from approximately the same radiation dose as two periapical radiographs, andthey may provide a dose savings over multiple traditional images in complex cases’’(25). Situations occur during the course of endodontic treatment that may require addi-tional diagnostic information to provide the best outcome for the patient. Use of CBCT inplace of multiple periapical radiographs to obtain this needed information not onlyprovides more accurate assessment but also reduces patient exposure to radiation.
One indication cited in the joint position statement of the AAE and AAOMR for theuse of CBCT in endodontics was ‘‘intra- or post-operative assessment of endodontictreatment complications, such as overextended root canal obturation material, sepa-rated endodontic instruments, calcified canal identification, and localization of perfo-rations’’ (25). Such intraoperative use of CBCT aids in avoidance of iatrogenic mishaps,which greatly influence the outcome of endodontic treatment. The overall prognosis ofendodontically treated teeth has been shown to decrease because of perforations (26–29), presence of periradicular radiolucency (29–31), and overfill or underfill ofobturation materials (32, 33). Fracture resistance of endodontically treated teeth hasalso been shown to decrease when excessive tooth structure has been removedduring endodontic treatment (34). Judicious use of intraoperative limited FOV CBCTimages may prevent the occurrence of iatrogenic mishaps and reduce removal ofhealthy tooth structure when anatomy of the tooth is not fully apparent on standard peri-apical radiographs.
Intraoperative applications of CBCT include the following: location of calcifiedcanals, evaluation of unexpected anatomic findings, evaluation of missed canals inendodontic retreatment, evaluation of root resorption and root fractures, and assess-ment of iatrogenic errors such as perforation, fractured instruments, and extrudedobturation materials. The purpose of this article is to discuss the application and
JOE — Volume 39, Number 4, April 2013

Figure 1. (A) Preoperative periapical radiograph of maxillary right second molar depicts radiolucent lesions around the P and buccal roots. (B and C) Intra-operative CBCT demonstrates absence of MB2 in MB root (arrows) in both axial and coronal planes. (D) Postoperative periapical radiograph of nonsurgical rootcanal treatment.
Case Report/Clinical Techniques
advantages of intraoperative CBCT in endodontics, while reducing radi-ation exposure during complex endodontic procedures.
Interpretation of Root Canal AnatomyCase 1: Determination of Second Mesiobuccal Canal inMaxillary Second Molar
A 41-year-old woman was referred for consultation and treatmentof her maxillary right second molar. Clinical and radiographic exami-nation was performed, and a diagnosis of pulp necrosis and symptom-atic apical periodontitis was obtained. Initial radiographic examinationwas performed with RVG 6100 digital sensors (Carestream, Atlanta, GA)and included 2 periapical radiographs and a bite-wing radiograph.Periapical radiolucencies were evident around the palatal (P) and dis-tobuccal (DB) root apices (Fig. 1A). On access, the mesiobuccal (MB),DB, and P canals were located by using a dental operating microscope(DOM), and working lengths were obtained. Mueller burs (BrasselerUSA, Savannah, GA) and ProUltra Endo Tip #2 (Dentsply Tulsa, TulsaOK) were then used to trace the MB groove in an attempt to localizethe second MB (MB2) canal. Despite all clinical efforts, no MB2 wasidentified. The tooth was sealed by using Cavit (3M ESPE, Seefeld,Germany), rubber dam was removed, and the patient was scannedwith limited FOV CBCT at 76 mm (Kodak 9000; Carestream) (Fig. 1Band C). Careful examination of the CBCT study revealed that MB2 wasnot present. Periradicular radiolucencies were confirmed at the apicesof MB, DB, and P canals. Nonsurgical root canal treatment wascompleted on #2 (Fig. 1D).
Figure 2. (A and B) Preoperative periapical and bite-wing radiographs of maxiincluding a deep furcation and large pulp chamber. Distal caries were noted on b
JOE — Volume 39, Number 4, April 2013
Case 2: TaurodontismA 34-year-old man was referred for consultation and treatment of
the maxillary right first molar. The patient’s chief complaint wasdiscomfort in the maxillary right posterior quadrant with cold sensitivityduring the past few weeks. Clinical and radiographic examination wasperformed, and a diagnosis of symptomatic irreversible pulpitis andsymptomatic apical periodontitis was obtained. Initial radiographicexamination was performed with RVG 6100 digital sensors (Care-stream) and included 2 periapical radiographs and a bite-wing radio-graph (Fig. 2A and B). The periapical radiograph revealed a deepfurcation consistent with a taurodontism. On isolation and access,caries was removed, and the pulp chamber was exposed. A C-shapedroot canal anatomy was initially diagnosed with 4 root canal orifices.However, patency was not achieved in all canals. At this point, theneed for intraoperative CBCT was indicated to further evaluate theroot canal morphology and possible intracanal and intercanal connec-tions. The patient was informed, and consent was obtained. The toothwas then temporarily sealed by using Cavit, rubber dam was removed,and the patient was scanned with limited field of view CBCT at 76 mm(Kodak 9000) (Fig. 3).
Analysis of the CBCT scan confirmed the anatomy of taurodontism(Fig. 3A) as well as the presence of maxillary mucositis in relationshipwith the maxillary right first molar (Fig. 3B and C). Axial cuts showedthe presence of 4 canals (Fig. 3D) with fusion of the DB and P roots,creating the C-shape anatomy (Fig. 3D). With this information, thenonsurgical therapy was successfully completed (Fig. 4A), and a perma-nent core buildup was performed (Fig. 4B).
llary right first molar depict anatomic pattern consistent with taurodontism,oth images.
Intraoperative Endodontic Applications of CBCT 549
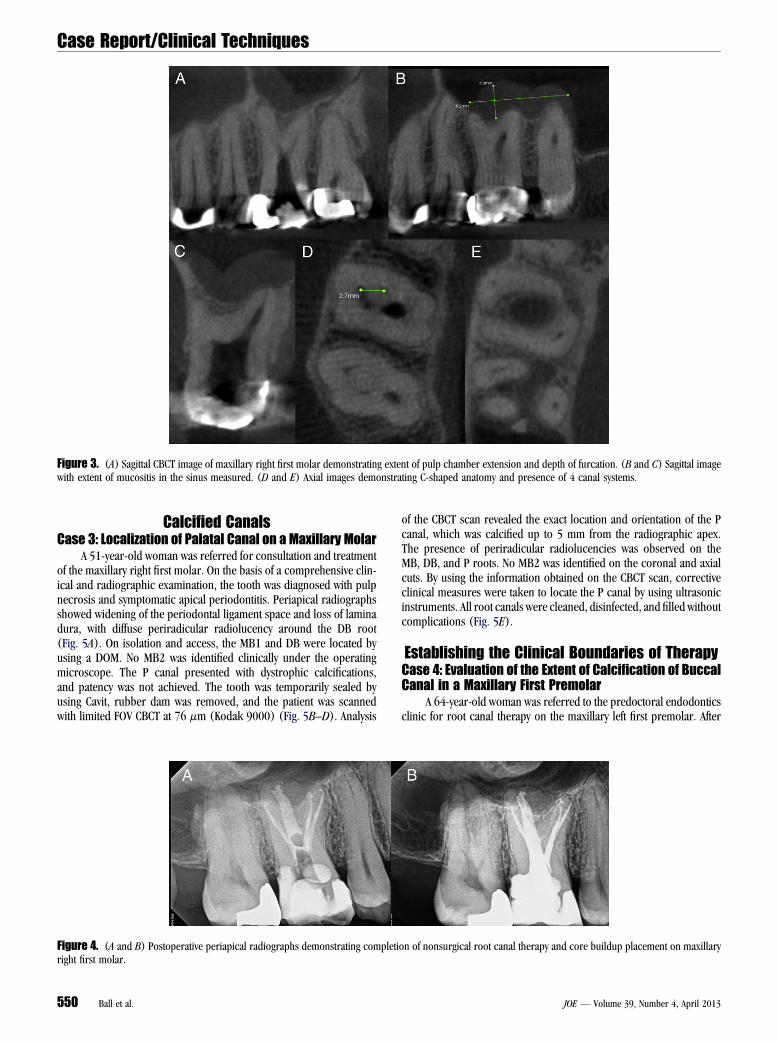
Figure 3. (A) Sagittal CBCT image of maxillary right first molar demonstrating extent of pulp chamber extension and depth of furcation. (B and C) Sagittal imagewith extent of mucositis in the sinus measured. (D and E) Axial images demonstrating C-shaped anatomy and presence of 4 canal systems.
Case Report/Clinical Techniques
Calcified CanalsCase 3: Localization of Palatal Canal on a Maxillary Molar
A 51-year-old woman was referred for consultation and treatmentof the maxillary right first molar. On the basis of a comprehensive clin-ical and radiographic examination, the tooth was diagnosed with pulpnecrosis and symptomatic apical periodontitis. Periapical radiographsshowed widening of the periodontal ligament space and loss of laminadura, with diffuse periradicular radiolucency around the DB root(Fig. 5A). On isolation and access, the MB1 and DB were located byusing a DOM. No MB2 was identified clinically under the operatingmicroscope. The P canal presented with dystrophic calcifications,and patency was not achieved. The tooth was temporarily sealed byusing Cavit, rubber dam was removed, and the patient was scannedwith limited FOV CBCT at 76 mm (Kodak 9000) (Fig. 5B–D). Analysis
Figure 4. (A and B) Postoperative periapical radiographs demonstrating completiright first molar.
550 Ball et al.
of the CBCT scan revealed the exact location and orientation of the Pcanal, which was calcified up to 5 mm from the radiographic apex.The presence of periradicular radiolucencies was observed on theMB, DB, and P roots. No MB2 was identified on the coronal and axialcuts. By using the information obtained on the CBCT scan, correctiveclinical measures were taken to locate the P canal by using ultrasonicinstruments. All root canals were cleaned, disinfected, and filled withoutcomplications (Fig. 5E).
Establishing the Clinical Boundaries of TherapyCase 4: Evaluation of the Extent of Calcification of BuccalCanal in a Maxillary First Premolar
A 64-year-old woman was referred to the predoctoral endodonticsclinic for root canal therapy on the maxillary left first premolar. After
on of nonsurgical root canal therapy and core buildup placement on maxillary
JOE — Volume 39, Number 4, April 2013

Figure 5. (A) Preoperative periapical radiograph #3. (B–D) Intraoperative CBCT images confirming the presence of P canal associated with periradicular radio-lucency. Arrows indicate the level and orientation of access achieved by the operator. (E) Postoperative periapical radiograph depicting completion of endodontictreatment #3 and obturation of P root.
Case Report/Clinical Techniques
clinical tests were performed and periapical radiographs were taken(Fig. 6A), a diagnosis of pulp necrosis with normal apical tissues wasgiven. Upon access and caries removal, the P canal was located, butthe dental student was unable to locate the buccal canal, and the casewas referred to the graduate endodontic clinic. An intraoperative limitedFOV CBCT scan at 76mm (Kodak 9000) was taken and analyzed (Fig. 6Band C). The axial and coronal cuts revealed the location of the buccalroot, but no evidence of a patent canal was noted along the length ofthe buccal root. The decision was made to treat the lingual canal onlyand leave the buccal root intact, thereby avoiding unnecessary removal
Figure 6. (A) Preoperative periapical radiograph #12 depicts large carious lesionscan demonstrates complete obliteration of buccal canal (arrows). (D) Postoperat
JOE — Volume 39, Number 4, April 2013
of tooth structure and/or perforation. Nonsurgical root canal treatmentwas completed on the lingual root of the maxillary left first premolar(Fig. 6D).
Root ResorptionCase 5: Diagnosis of External Inflammatory RootResorption and Extent of Crown Root Fracture
A 61-year-old woman was referred for consultation and treatmentof the maxillary right first molar. Her dental history included
beneath existing gold onlay and calcified canals. (B and C) Intraoperative CBCTive periapical radiograph of nonsurgical root canal treatment of lingual canal.
Intraoperative Endodontic Applications of CBCT 551

Case Report/Clinical Techniques
orthognathic surgery 43 years prior and endodontic access of the maxil-lary right first molar 2 months prior. Clinical examination revealed noresponse to thermal tests, with tenderness to palpation, percussion, andbiting. During the periodontal examination a localized 5-mm pocketwas probed on the mesial aspect of the maxillary right first molar. Allother probing depths were less than 3 mm. There was no evidence ofsinus tracts or soft tissue swelling. Preoperative radiographs were takenwith digital sensors (Kodak RVG 6100) and included 2 periapical and 1bite-wing radiographs (Fig. 7D). Loss of lamina dura and widened peri-odontal ligament space were noted on the MB and DB roots, witha diffuse periradicular radiolucency of 3 mm in diameter around thedistal root. The P and DB roots were shortened and had the radio-graphic appearance of external inflammatory root resorption. Themaxillary right first molar was diagnosed as previously initiated therapyand asymptomatic apical periodontitis. On access, 4 canal orifices wereidentified (MB1, MB2, DB, and P) by using a DOM. An intracoronalcrack was also noted that extended down the mesial and distal aspectsbeneath an existing amalgam restoration (Fig. 7A and B). The amalgamrestoration was removed, and it appeared that the cracks did not extendbeyond the level of the canal orifice, although the 5-mm mesial peri-odontal pocket indicated possible crack propagation. Patency of allcanals was confirmed with an electronic apex locator, and a periapicalradiograph with patency files in all 4 canals was taken (Fig. 7E). Thefiles in the mesial canals appeared 2–3 mm short of the radiographicapex, and the file in the P canal appeared 3–4 mm short of the radio-graphic apex. An intraoperative CBCT scan was taken to evaluate extentof fracture as well as the accuracy of the working lengths (Fig. 7G–J).Mesial crestal bone loss was not noted on the CBCT scan. Also, theforamina of the mesial canals exited short and both buccal and lingualto the anatomic apex by 2–3 mm. Progressive external root resorptionwas apparent at the apex of the P canal, and the foramen exited 3–4 mmFigure 7. (A and B) Intraoperative photographs depicting crack lines (arrows)demonstrating composite resin core buildup and orthodontic band cemented inDB and P roots and radiolucent lesions around DB and MB roots. (E) Intraoperain the mesial and palatal canals are several millimeters short of the radiographic apment. (G and H) Intraoperative CBCT scan demonstrating extent of P root resorption(arrows). (J) No evidence of crestal bone loss caused by fractures.
552 Ball et al.
coronal to the apical extent of the P root, possibly because of the resorp-tion. These findings explained the discrepancy in the patency file lengthsfrom the radiographic apices of themesial and P roots. Nonsurgical rootcanal treatment was completed on the maxillary right first molar,a composite resin core buildup was placed in the access, and an ortho-dontic band was placed around the tooth as a temporary measure toprevent further propagation of the crack (Fig. 7C and F). The patientwas referred back to her primary care dentist with a recommendationfor full cuspal coverage restoration.
Separated InstrumentsCase 6: Determining the Location of a SeparateInstrument to Enable Bypass and Removal
A 38-year-old man presented for evaluation and treatment of hismandibular right first molar. Dental history revealed a previous attemptto perform a root canal retreatment 1 week prior. The endodontist ac-cessed the tooth and attempted to loosen the separated instrument in theMB canal by using ultrasonics tips and files without positive outcome. Atthis point, the endodontist sealed the access with Cavit (Fig. 8A) andreferred the case to a different endodontist. On initial consultation,the patient was symptomatic and frustrated with the fact that the instru-ment was not removed. A CBCT scan was prescribed to (1) determinepossible spaces for ultrasonic activation without risks of stripping orperforation, (2) evaluate the location of the mental foramen to deter-mine the feasibility of apical surgery in case the file was deemed unre-trievable, and (3) diagnose the size and location of the apicalresorption. Analysis of the scan revealed a clear space between theinstrument and the lingual wall of the MB canal (Fig. 8A–D). Inciden-tally, a clear intracanal root resorption, presumably inflammatory, wasalso observed. With this information available, the second endodontist
on mesial and distal aspects of pulp chamber. (C) Postoperative photographplace. (D) Preoperative periapical radiograph demonstrating resorption oftive periapical radiograph demonstrating patency files in all canals. The filesices. (F) Postoperative radiograph demonstrating completed endodontic treat-(arrows) and (I) apical foramen of MB canals exiting short of anatomic apex
JOE — Volume 39, Number 4, April 2013

Figure 8. (A) Preoperative periapical radiograph of mandibular right first molar depicting separated instrument in MB canal. (B–D) Intraoperative axial, sagittal,and coronal CBCT images demonstrate location of separated instrument and location of apical internal resorptive defect (arrows). (E) Postoperative periapicalradiograph of nonsurgical root canal treatment performed on mandibular right first molar, including obturation of apical resorptive defect. (F) Periapical radio-graph taken at 3-month recall visit showing evidence of apical healing.
Case Report/Clinical Techniques
accessed the tooth and bypassed and removed the instrument. Once thisobstruction was removed, all efforts were aimed at debriding and dis-infecting the resorptive defect at the apical third to achieve disinfectionof this niche. Failure to do so would have likely affected the outcome ofthe root canal retreatment, despite the successful removal of the sepa-rated instrument. The nonsurgical root canal retreatment was thensuccessfully completed (Fig. 8E), and the patient returned asymptom-atic at the 3-month follow-up, with radiographic evidence of healing inprocess (Fig. 8F).
Vertical Root FractureCase 7: Differential Diagnosis of Vertical Root Fracture
A 67-year-old woman presented for examination andendodontic treatment of her maxillary right second premolar.The patient was complaining of dull pain in the maxillary rightposterior quadrant that started 2 weeks prior. Patient reportedhaving endodontic therapy on the maxillary right second premolarmore than 20 years ago. Clinical examination revealed no responseto thermal tests, with tenderness to palpation, percussion, andbiting. Periodontal examination was within normal limits, with noprobing depths of more than 3 mm. There was no evidence of sinustracts or soft tissue swelling. Preoperative periapical radiographswere taken with RVG 6100 digital sensors (Fig. 9A and B). Lossof lamina dura and widened periodontal ligament space were notedwith diffuse periradicular radiolucency. Accordingly, the maxillaryright second premolar was diagnosed as previously treated withsymptomatic apical periodontitis. The existing full crown restora-tion was passively lifted, and the silver cones were removed by
JOE — Volume 39, Number 4, April 2013
using ultrasonic and Hedstrom files. Working length was obtained,and canals were irrigated. Under the DOM, a possible fracture onthe palatal aspect of the buccal root was noted. The canal wasstained with methylene blue, but no definitive diagnosis waspossible. The tooth was temporarily sealed by using Cavit, rubberdam was removed, and the patient was scanned with limited FOVCBCT at 76 mm (Kodak 9000) (Fig. 9C and D). Analysis of thestudy confirmed the presence of a root fracture on the buccalroot of the maxillary right second premolar. The patient wasreferred for extraction and rehabilitation.
Case 8: Differential Diagnosis of Additional Canals orVertical Root Fracture
A 64-year-old woman presented for examination and endodontictreatment of her maxillary right second premolar. Comprehensive clin-ical and radiographic examination was performed, and the tooth wasdiagnosed as previously treated with symptomatic apical periodontitis(Fig. 10A and B). No deep periodontal pockets were diagnosed. Onaccess, the root canal filling was removed, and a lingual projectionwas observed; the possibility of a second canal or root was discussedwith the patient. The tooth was temporarily sealed by using Cavit, rubberdam was removed, and the patient was scanned with limited FOV CBCTat 76 mm (Kodak 9000) (Fig. 10C–E). Careful interpretation of theCBCT images revealed the presence of a vertical bone loss along thelingual aspect of the root (Fig. 10C) and a root fracture on the lingualside of the maxillary right second premolar (Fig. 10D). The endodonticprocedure was not completed, and the patient was referred for extrac-tion and rehabilitation.
Intraoperative Endodontic Applications of CBCT 553

Figure 9. (A and B) Preoperative periapical radiographs of maxillary right second premolar showing presence of silver points on root canals and presence ofperiradicular radiolucency. (C and D) Intraoperative coronal and axial slides after silver point removal confirming presence of root fracture on buccal root(arrows).
Case Report/Clinical Techniques
Management of Iatrogenic Root PerforationCase 9: Location of Mesiolingual Perforation and MBRoot Canal in a Mandibular Second Molar
A 73-year-old womanwas referred for consultation and endodontictreatment of the mandibular right second molar. Clinical and radio-graphic examination was performed, and the tooth was given a pulpaland periradicular diagnosis of symptomatic irreversible pulpitis andsymptomatic apical periodontitis (Fig. 11A). There was no evidence ofsinus tracts or soft tissue swelling, and all periodontal probing depthswere less than 3 mm. Endodontic treatment was initiated, and occlusalaccess was performed. The distal canal and 1 mesial canal were located.A lingual perforation occurred while searching for the second mesialcanal, and a periapical radiograph was immediately taken to confirmthe perforation (Fig. 11B). A small amount of mineral trioxide aggregate(MTA) (Pro Root; Dentsply, Tulsa Dental, Johnson City, TN) was placedover the perforation to seal it and prevent further contamination. Theaccess was temporarily sealed, and an intraoperative CBCT scan (Kodak9000) was taken to evaluate the location of the perforation as well as thelocation of the secondmesial canal (Fig. 11C–F). By using the intraoper-ative CBCT images, the location and relationship of the perforation withthe crestal bone were determined, and the precise location of the MBcanal was identified. Taking into consideration the location of the perfo-ration, the MTA seal was removed, and the perforation was repaired withGeristore (Denmat, Santa Maria, CA). The root canal was then completedwithout further complications (Fig. 11G).
DiscussionAccurate diagnostic imaging is an essential part of endodontic
evaluation and treatment. Conventional two-dimensional radiographs
554 Ball et al.
are still the most widely accepted and used imaging modality inendodontics. This is despite the fact that classic and current literaturehas highlighted the limitations of conventional radiographs (16, 35–37). These limitations arise primarily because of the inherentprojection of a three-dimensional anatomy into a two-dimensionalview, which leads to geometric distortion and, consequently, misinter-pretation and/or misdiagnosis. It has been shown that CBCT is not sub-jected to the same limitations because of the production of accuratethree-dimensional images (16). Current literature has demonstratedthat preoperative CBCT images precisely reproducemaxillofacial tissues(2–4), elucidate the presence of periapical lesions more accuratelythan conventional radiographs (16–20), and display the location andextension of perforations (24), traumatic injuries (8), and resorptivedefects (7, 14–16). Despite the myriad advantages that CBCT offerscompared with conventional radiographs, its use for preoperativeendodontic examination should carefully be considered on the basisof the as low as reasonably achievable protocol concerning radiationlevels to expose patients to the least amount of radiation possible,while still gaining the most useful information for proper diagnosis.
To date, the intraoperative use of limited FOV CBCT has not beenreported in the literature, despite the fact that it is not unusual toencounter internal root canal anatomy that was not completely revealedby traditional preoperative radiographs. The cases outlined in thisarticle exemplified clinical situations that might benefit from furtherimaging information to provide the best clinical care. Furthermore,they underscore the value of taking intraoperative CBCT images to facil-itate safe and effective endodontic treatment and to contribute todecision-making in cases in which it may be prudent to set the bound-aries and evaluate the benefit/risk ratio that will be in the best interest ofthe patient’s care. A good example of this clinical situation would be the
JOE — Volume 39, Number 4, April 2013
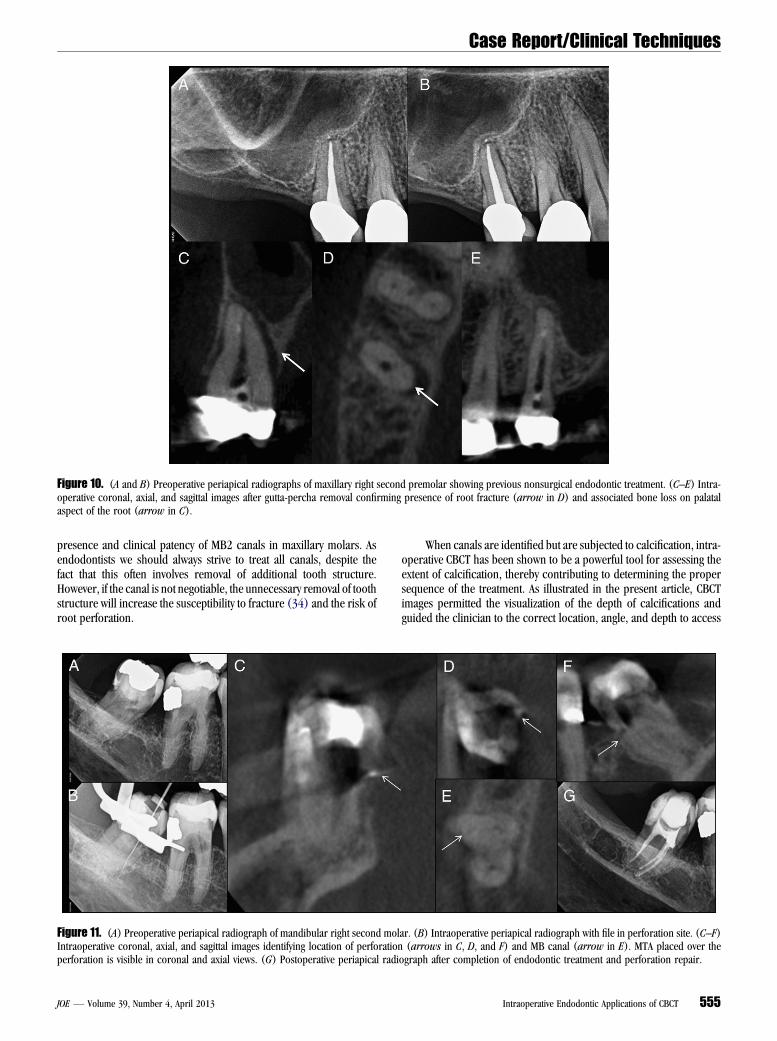
Figure 10. (A and B) Preoperative periapical radiographs of maxillary right second premolar showing previous nonsurgical endodontic treatment. (C–E) Intra-operative coronal, axial, and sagittal images after gutta-percha removal confirming presence of root fracture (arrow in D) and associated bone loss on palatalaspect of the root (arrow in C).
Case Report/Clinical Techniques
presence and clinical patency of MB2 canals in maxillary molars. Asendodontists we should always strive to treat all canals, despite thefact that this often involves removal of additional tooth structure.However, if the canal is not negotiable, the unnecessary removal of toothstructure will increase the susceptibility to fracture (34) and the risk ofroot perforation.
Figure 11. (A) Preoperative periapical radiograph of mandibular right second molIntraoperative coronal, axial, and sagittal images identifying location of perforationperforation is visible in coronal and axial views. (G) Postoperative periapical radi
JOE — Volume 39, Number 4, April 2013
When canals are identified but are subjected to calcification, intra-operative CBCT has been shown to be a powerful tool for assessing theextent of calcification, thereby contributing to determining the propersequence of the treatment. As illustrated in the present article, CBCTimages permitted the visualization of the depth of calcifications andguided the clinician to the correct location, angle, and depth to access
ar. (B) Intraoperative periapical radiograph with file in perforation site. (C–F)(arrows in C, D, and F) and MB canal (arrow in E). MTA placed over the
ograph after completion of endodontic treatment and perforation repair.
Intraoperative Endodontic Applications of CBCT 555

Case Report/Clinical Techniques
the patent portion of the canals. On the basis of accurate measurementof the length and width of canal walls and distance from importantanatomic structures provided by the CBCT scan, the canals were foundand properly treated. On the other hand, when complete calcificationswere detected, the intraoperative CBCT scan provided the critical infor-mation that led to the decision of preserving dental structures, particu-larly when apical pathosis is not present and the risks of attempting toexpose a completely calcified canal are unjustifiable.Vertical root fractures can be one of the most challenging diag-nostic situations in endodontics. The cases illustrated in the presentarticle have demonstrated the advantage of using CBCT intraoperativelyafter removal of obturation materials to diagnose root fractures. Incases in which preoperative scans are taken, artifacts created by theroot canal fillingmaterials would havemade definitive diagnosis of theseconditions challenging. Vertical root fractures are also rarely visualizedon traditional preoperative periapical radiographs.
Precise identification of the location of a perforation can helpdictate the type of repair material used. In the case presented in thisarticle, the location of the perforation was identified at the height ofthe crestal bone by using intraoperative CBCT images. The intraopera-tive periapical radiograph with the file in the perforation site was notable to provide this information. A bondable repair material (Geristore)was chosen for final repair to prevent washout, which might haveoccurred with MTA. Also, placement of a small amount of MTA overthe perforation before intraoperative CBCT enabled exact location ofthe perforation site. Accurate location of the perforation was criticalin determining management in this case.
From the clinical point of view, the case series presented follows theAAE/AAOMR recommendations of using CBCT for the assessment ofendodontic complications such as those previouslymentioned. By relyingon the intraoperative CBCT images, it was possible to elucidate toothmorphology, determine the boundaries and risks for attempting rootcanal treatment in cases of calcified canals, and use them as a guidefor localization and understanding of complex endodontic anatomy. Inaddition, the intraoperative CBCT scanwas an important tool for detectingperiapical pathosis, resorptive defects, extension of crack propagation,root perforation, and vertical root fractures in cases in which the diag-nosis or treatment was compromised by the limitations of radiographs.
In conclusion, the patient always has the right to an informed deci-sion, especially when other diagnostic means are inconclusive. In cases ofincreased difficulty or intraoperative complications, it is prudent toconsider the use of limited FOV CBCT with its inherent accurate diagnosticvalue and limited radiation exposure. In essence, the benefits of the addeddiagnostic information provided by intraoperative CBCT in select casesjustify the risk associated with the limited level of radiation exposure.
AcknowledgmentsThe authors acknowledge Dr Jordan West, Blake McRay, Steven
Kwan, Lindsay Posner, Harrison Nguyen, and David Mortenson fortheir contribution to this manuscript.
This article was written with LCDR Randy Ball, DC, USN whilehe was a resident at the University of Washington training inendodontics. The views expressed in this article are those of theauthor and do not reflect the official policy or position of theDepartment of the Navy, Department of Defense, or the UnitedStates Government.
The authors deny any conflicts of interest related to this study.
References1. Danforth RA. Cone beam volume tomography: a new digital imaging option for
dentistry. J Calif Dent Assoc 2003;31:814–5.
556 Ball et al.
2. Cotton TP, Geisler TM, Holden DT, et al. Endodontic applications of cone-beamvolumetric tomography. J Endod 2007;33:1121–32.
3. Tyndall DA, Rathore S. Cone-beam CT diagnostic applications: caries, periodontalbone assessment, and endodontic applications. Dent Clin North Am 2008;52:825–41. vii.
4. Tyndall DA, Kohltfarber H. Application of cone beam volumetric tomography inendodontics. Aust Dent J 2012;57(Suppl 1):72–81.
5. Patel S, Ricucci D, Durak C, Tay F. Internal root resorption: a review. J Endod 2010;36:1107–21.
6. Patel S, Dawood A. The use of cone beam computed tomography in the managementof external cervical resorption lesions. Int Endod J 2007;40:730–7.
7. Cohenca N, Simon JH, Mathur A, Malfaz JM. Clinical indications for digital imagingin dento-alveolar trauma: part 2—root resorption. Dent Traumatol 2007;23:105–13.
8. Cohenca N, Simon JH, Roges R, et al. Clinical indications for digital imaging indento-alveolar trauma: part 1—traumatic injuries. Dent Traumatol 2007;23:95–104.
9. Hassan B, Metska ME, Ozok AR, et al. Comparison of five cone beam computedtomography systems for the detection of vertical root fractures. J Endod 2010;36:126–9.
10. Patel S. The use of cone beam computed tomography in the conservative manage-ment of dens invaginatus: a case report. Int Endod J 2010;43:707–13.
11. Durack C, Patel S. The use of cone beam computed tomography in the managementof dens invaginatus affecting a strategic tooth in a patient affected by hypodontia:a case report. Int Endod J 2011;44:474–83.
12. Liang YH, Li G, Wesselink PR, Wu MK. Endodontic outcome predictors identifiedwith periapical radiographs and cone-beam computed tomography scans.J Endod 2011;37:326–31.
13. Patel S, Dawood A, Wilson R, et al. The detection and management of root resorptionlesions using intraoral radiography and cone beam computed tomography: anin vivo investigation. Int Endod J 2009;42:831–8.
14. Kamburoglu K, Kursun S, Yuksel S, Oztas B. Observer ability to detect ex vivo simu-lated internal or external cervical root resorption. J Endod 2011;37:168–75.
15. Durack C, Patel S, Davies J, et al. Diagnostic accuracy of small volume cone beamcomputed tomography and intraoral periapical radiography for the detection ofsimulated external inflammatory root resorption. Int Endod J 2011;44:136–47.
16. Patel S, Dawood A, Mannocci F, et al. Detection of periapical bone defects in humanjaws using cone beam computed tomography and intraoral radiography. Int Endod J2009;42:507–15.
17. Huumonen S, Kvist T, Grondahl K, Molander A. Diagnostic value of computedtomography in re-treatment of root fillings in maxillary molars. Int Endod J2006;39:827–33.
18. Lofthag-Hansen S, Huumonen S, Grondahl K, Grondahl HG. Limited cone-beam CTand intraoral radiography for the diagnosis of periapical pathology. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2007;103:114–9.
19. Jorge EG, Tanomaru-Filho M, Goncalves M, Tanomaru JM. Detection of periapicallesion development by conventional radiography or computed tomography. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2008;106:e56–61.
20. de Paula-Silva FW, Wu MK, Leonardo MR, et al. Accuracy of periapical radiog-raphy and cone-beam computed tomography scans in diagnosing apical peri-odontitis using histopathological findings as a gold standard. J Endod 2009;35:1009–12.
21. Ozer SY. Detection of vertical root fractures of different thicknesses in endodonti-cally enlarged teeth by cone beam computed tomography versus digital radiography.J Endod 2010;36:1245–9.
22. Bernardes RA, de Moraes IG, Hungaro Duarte MA, et al. Use of cone-beam volu-metric tomography in the diagnosis of root fractures. Oral Surg Oral Med OralPathol Oral Radiol Endod 2009;108:270–7.
23. Hassan B, Metska ME, Ozok AR, et al. Detection of vertical root fractures inendodontically treated teeth by a cone beam computed tomography scan.J Endod 2009;35:719–22.
24. Shemesh H, Cristescu RC, Wesselink PR, Wu MK. The use of cone-beam computedtomography and digital periapical radiographs to diagnose root perforations.J Endod 2011;37:513–6.
25. Joint Position Statement of the American Association of Endodontists and the Amer-ican Academy of Oral and Maxillofacial Radiology. Use of cone-beam computedtomography in endodontics. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2011;111:234–7.
26. Mente J, Hage N, Pfefferle T, et al. Treatment outcome of mineral trioxide aggregate:repair of root perforations. J Endod 2010;36:208–13.
27. Zadik Y, Sandler V, Bechor R, Salehrabi R. Analysis of factors related to extraction ofendodontically treated teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2008;106:e31–5.
28. Marquis VL, Dao T, Farzaneh M, et al. Treatment outcome in endodontics: the Tor-onto Study—phase III: initial treatment. J Endod 2006;32:299–306.
JOE — Volume 39, Number 4, April 2013

Case Report/Clinical Techniques
29. de Chevigny C, Dao TT, Basrani BR, et al. Treatment outcome in endodon-tics: the Toronto study—phase 4: initial treatment. J Endod 2008;34:258–63.
30. Ng YL, Mann V, Rahbaran S, et al. Outcome of primary root canal treatment: system-atic review of the literature—part 2: influence of clinical factors. Int Endod J 2008;41:6–31.
31. Chugal NM, Clive JM, Spangberg LS. A prognostic model for assessment ofthe outcome of endodontic treatment: effect of biologic and diagnosticvariables. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:342–52.
32. Schaeffer MA, White RR, Walton RE. Determining the optimal obturation length:a meta-analysis of literature. J Endod 2005;31:271–4.
JOE — Volume 39, Number 4, April 2013
33. Chugal NM, Clive JM, Spangberg LS. Endodontic infection: some biologic and treat-ment factors associated with outcome. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;96:81–90.
34. Tang W, Wu Y, Smales RJ. Identifying and reducing risks for potential fractures inendodontically treated teeth. J Endod 2010;36:609–17.
35. Bender IB, Seltzer S. Roentgenographic and direct observation of experimentallesions in bone: II, 1961. J Endod 2003;29:707–12.
36. Bender IB, Seltzer S. Roentgenographic and direct observation of experimentallesions in bone: I, 1961. J Endod 2003;29:702–6.
37. Green TL, Walton RE, Taylor JK, Merrell P. Radiographic and histologic periapicalfindings of root canal treated teeth in cadaver. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1997;83:707–11.
Intraoperative Endodontic Applications of CBCT 557