introduction to risk adjustment - chima · introduction to risk adjustment & hccs ... the...
TRANSCRIPT
4/28/2016
1
CHIMA Annual Meeting
Introduction to Risk Adjustment & HCCs
CHIMA Annual MeetingMay 6, 2016
Kathryn DeVault, MSL, RHIA, CCS, CCS‐P, FAHIMAUnited Audit Solutions, Inc.
Objectives
• Discuss the meaning of risk adjustment
• Discuss the meaning of hierarchical condition categories (HCC)
• Review the history of HCCs and how they’re used in population health management and value based purchasing
• Review documentation requirements for accurate HCC capture
• Review case exampleReview case example
4/28/2016
2
Risk Adjustment Factor (RAF)
• Risk adjustment is calculated using an actuarial tool developed toRisk adjustment is calculated using an actuarial tool developed to predict the cost of healthcare for covered beneficiaries/enrollees
• A risk adjustment score is determined by using a combination of demographic information along with disease information to predict future healthcare costs for enrollees
• The score is highest for the sickest patients as determined by a• The score is highest for the sickest patients as determined by a combination of factors
4/28/2016
3
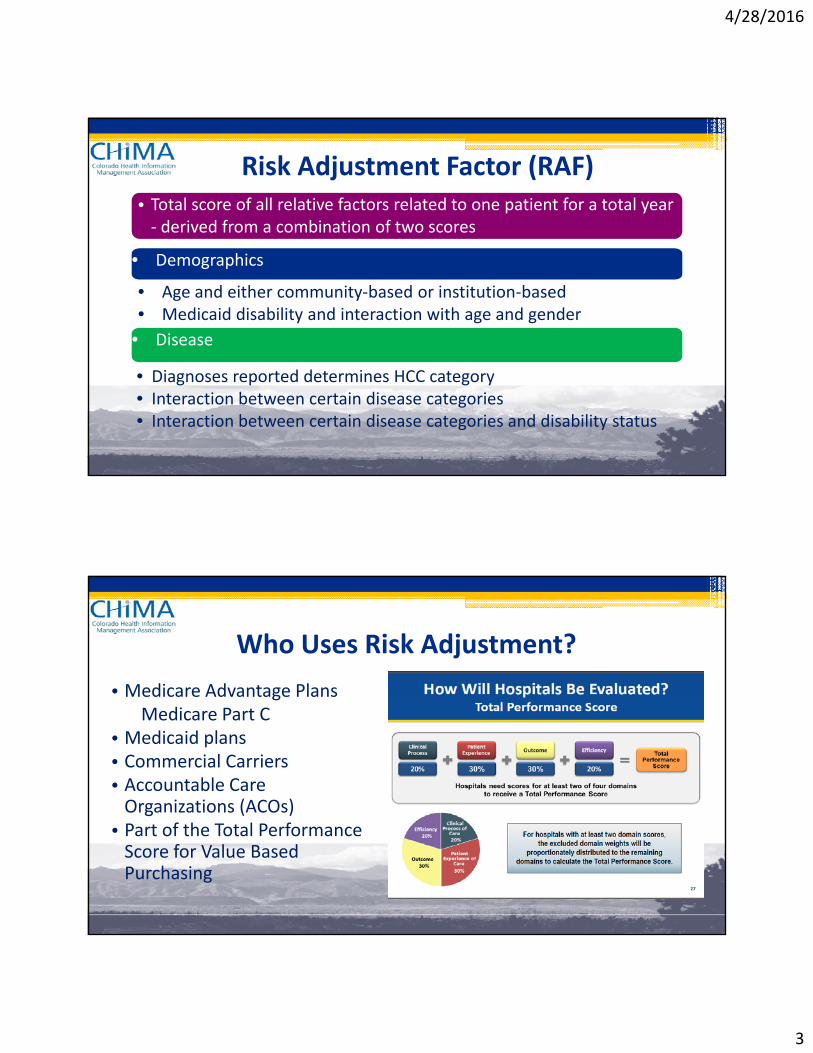
Risk Adjustment Factor (RAF)• Total score of all relative factors related to one patient for a total year ‐ derived from a combination of two scores
• Demographics
• Age and either community‐based or institution‐based• Medicaid disability and interaction with age and gender
• Disease
• Diagnoses reported determines HCC category• Interaction between certain disease categories• Interaction between certain disease categories and disability status
Who Uses Risk Adjustment?
• Medicare Advantage PlansMedicare Advantage PlansMedicare Part C
• Medicaid plans • Commercial Carriers • Accountable Care Organizations (ACOs)g ( )• Part of the Total Performance Score for Value Based Purchasing
4/28/2016
4
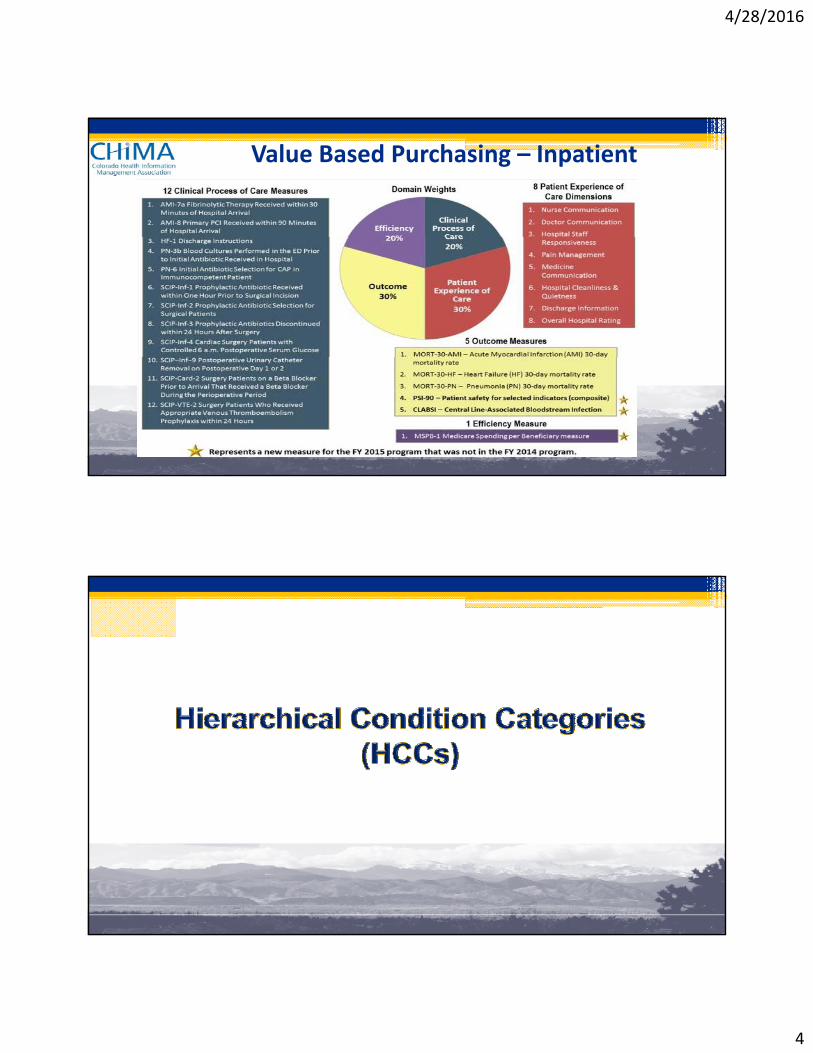
Value Based Purchasing – Inpatient
4/28/2016
5
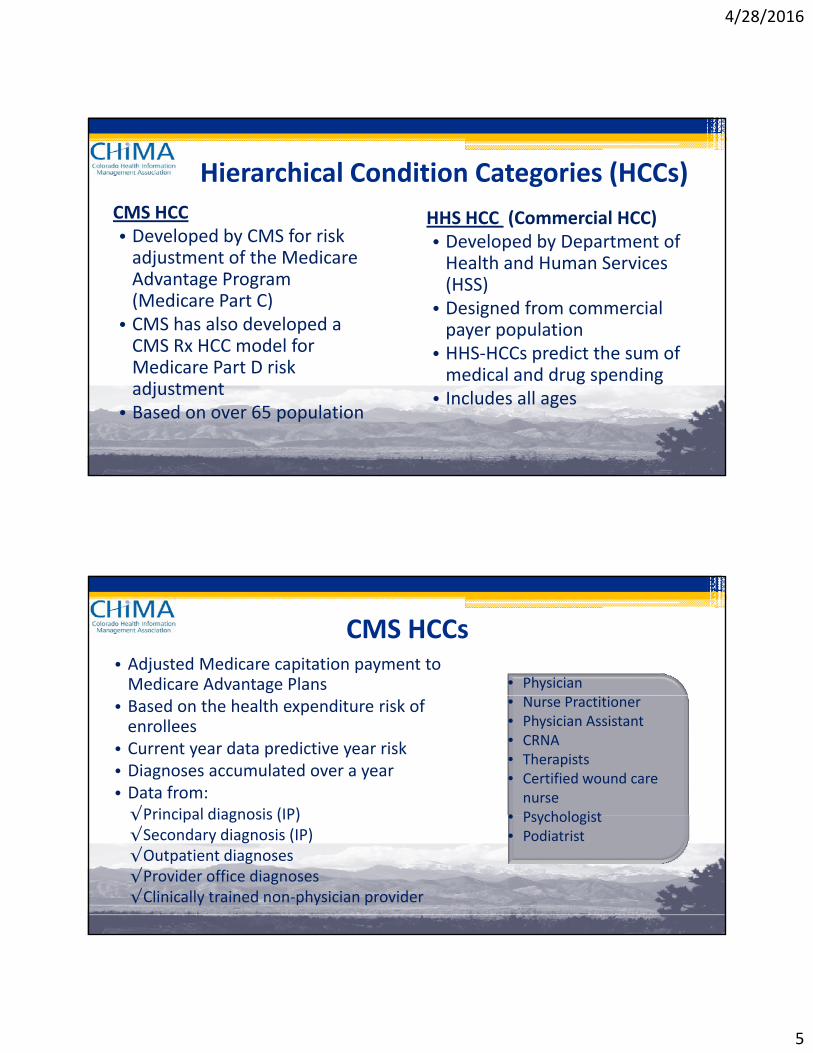
Hierarchical Condition Categories (HCCs)
CMS HCC• Developed by CMS for risk
HHS HCC (Commercial HCC)D l d b D t t f• Developed by CMS for risk
adjustment of the Medicare Advantage Program (Medicare Part C)• CMS has also developed a CMS Rx HCC model for
• Developed by Department of Health and Human Services (HSS)• Designed from commercial payer population• HHS‐HCCs predict the sum of
Medicare Part D risk adjustment• Based on over 65 population
HHS HCCs predict the sum of medical and drug spending • Includes all ages
CMS HCCs• Adjusted Medicare capitation payment to Medicare Advantage Plans • Physician
• Based on the health expenditure risk of enrollees• Current year data predictive year risk• Diagnoses accumulated over a year • Data from:√Principal diagnosis (IP)
• Nurse Practitioner• Physician Assistant• CRNA• Therapists• Certified wound care nurse
• Psychologist√Principal diagnosis (IP)√Secondary diagnosis (IP)√Outpatient diagnoses√Provider office diagnoses √Clinically trained non‐physician provider
• Psychologist• Podiatrist
4/28/2016
6
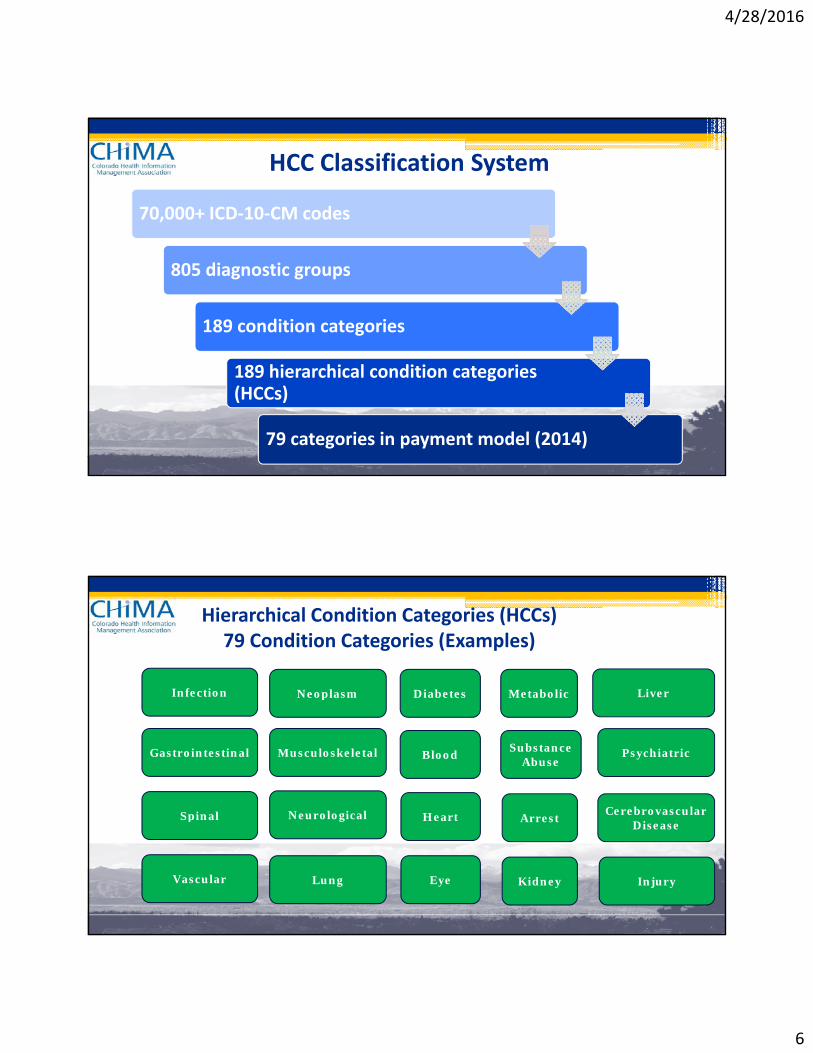
HCC Classification System
70,000+ ICD‐10‐CM codes
805 diagnostic groups
189 condition categories
189 hierarchical condition categories (HCCs)
79 categories in payment model (2014)
Hierarchical Condition Categories (HCCs)79 Condition Categories (Examples)
Infection Neoplasm Diabetes Metabolic Liver Infection
Gastrointestinal
Spinal
Neoplasm
Musculoskeletal
Neurological
Diabetes
Blood
Heart
Metabolic
Substance Abuse
A t
Liver
Psychiatric
Cerebrovascular Spinal
Vascular
Neurological
Lung
Heart
Eye
Arrest
Kidney
Ce eb o ascu a Disease
Injury
4/28/2016
7
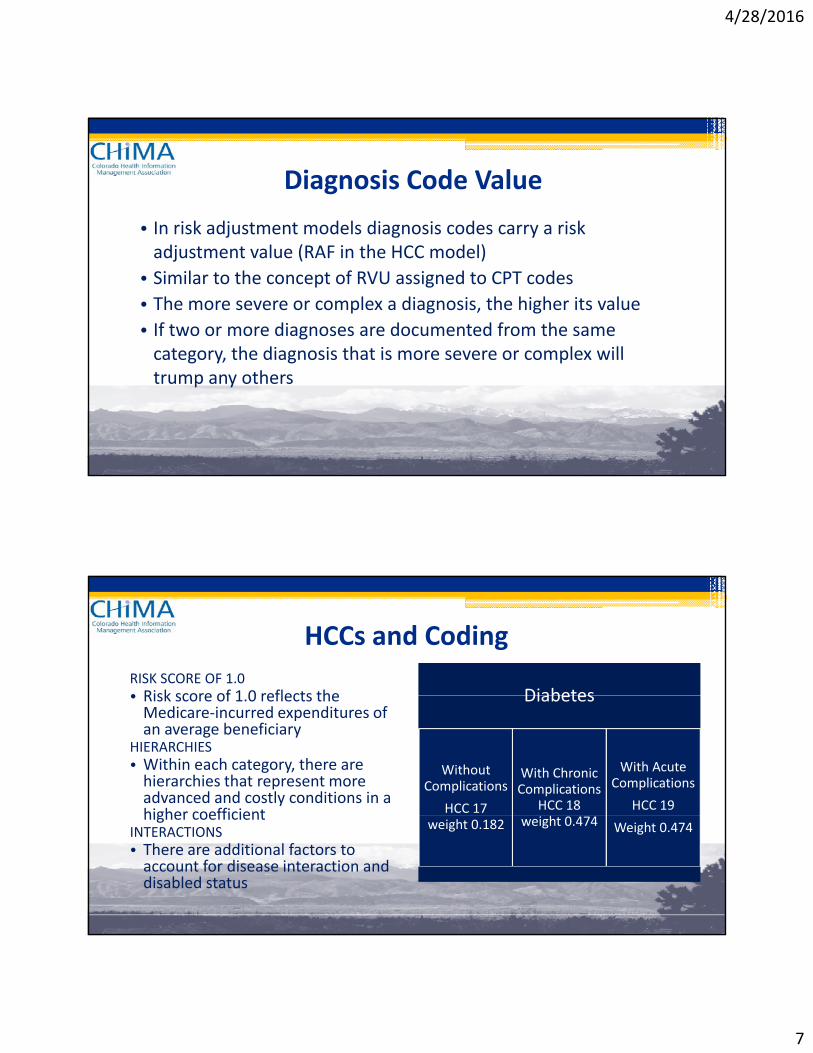
Diagnosis Code Value
• In risk adjustment models diagnosis codes carry a risk j g yadjustment value (RAF in the HCC model)
• Similar to the concept of RVU assigned to CPT codes
• The more severe or complex a diagnosis, the higher its value
• If two or more diagnoses are documented from the same category the diagnosis that is more severe or complex willcategory, the diagnosis that is more severe or complex will trump any others
HCCs and Coding
RISK SCORE OF 1.0• Risk score of 1 0 reflects the Diabetes• Risk score of 1.0 reflects the Medicare‐incurred expenditures of an average beneficiary
HIERARCHIES• Within each category, there are hierarchies that represent more advanced and costly conditions in a higher coefficient
Diabetes
Without Complications
HCC 17
With Chronic Complications
HCC 18
With Acute Complications
HCC 19higher coefficient
INTERACTIONS• There are additional factors to account for disease interaction and disabled status
weight 0.182 weight 0.474 Weight 0.474
4/28/2016
8
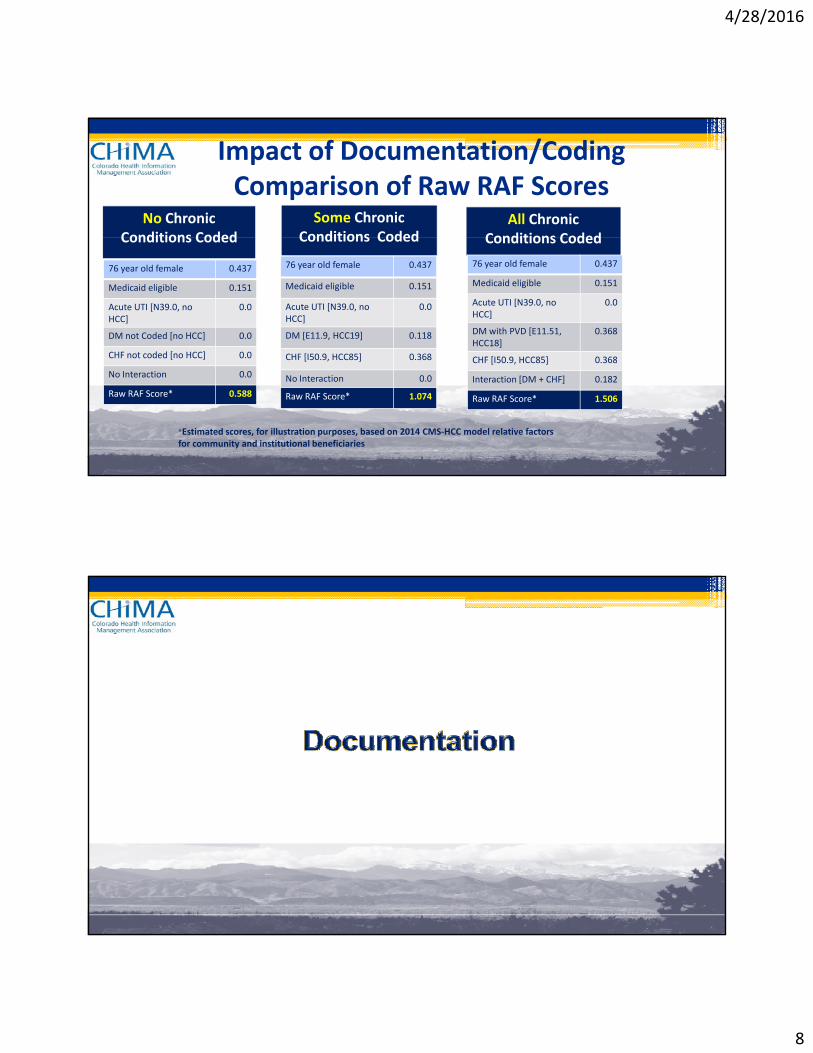
Impact of Documentation/CodingComparison of Raw RAF Scores
No Chronic Conditions Coded
Some Chronic Conditions Coded
All Chronic Conditions Coded
76 year old female 0.437
Medicaid eligible 0.151
Acute UTI [N39.0, no HCC]
0.0
DM not Coded [no HCC] 0.0
CHF not coded [no HCC] 0 0
Conditions Coded Conditions Coded
76 year old female 0.437
Medicaid eligible 0.151
Acute UTI [N39.0, no HCC]
0.0
DM [E11.9, HCC19] 0.118
CHF [I50 9 HCC85] 0 368
Conditions Coded
76 year old female 0.437
Medicaid eligible 0.151
Acute UTI [N39.0, no HCC]
0.0
DM with PVD [E11.51, HCC18]
0.368
CHF [I50 9 HCC85] 0 368CHF not coded [no HCC] 0.0
No Interaction 0.0
Raw RAF Score* 0.588
CHF [I50.9, HCC85] 0.368
No Interaction 0.0
Raw RAF Score* 1.074
CHF [I50.9, HCC85] 0.368
Interaction [DM + CHF] 0.182
Raw RAF Score* 1.506
*Estimated scores, for illustration purposes, based on 2014 CMS‐HCC model relative factors for community and institutional beneficiaries
4/28/2016
9
Documentation Requirements • Diagnoses must be captured in a face‐to‐face setting• Diagnoses must be documented in the health record appropriate identification, date, and provider signature• Example of specific reporting rules:√Chronic diseases can continue to be reported on an on‐going bases as long as receiving treatment and care for the condition
√Diagnoses that receive care and management during the encounter can be reported
√Diagnoses that have resolved or are no longer treated should not be listed
√Malignancy can be reported as long as receiving active treatment√Be careful using problem list diagnoses that have been resolved
Disease Specific Requirements• Cancer reportingp g√Primary malignancy that has been eradicated or excised is report as history once treatment is completed
√Secondary malignancy currently receiving treatment can be reported by site of the metastasis
√Leukemia is reported by type and acuity with ‘in remission’ included on the lilist
√Personal history of malignancies, leukemia and lymphoma can be reported
4/28/2016
10
Disease Specific Requirements
• Complications or manifestations of a disease process must be clearly linked to that condition
• Substance use is reported as Use, Abuse or Dependence√Dependence can be reported as ‘in remission’
Detailed Documentation is Key Reason for the Encounter Include Results and FindingsPreventive Screenings ImmunizationsRecommendationsTreatment PlanReferrals
Preventive vs. Sick VisitCC: F/U or RefillsNon-Standard AbbreviationsAcute vs. ChronicActive vs. ResolvedDiagnoses without a PlanPending TestsReferrals
Medications RefilledFollow up visits
Pending TestsMissing Exams Incomplete Notes
4/28/2016
11
Documentation Tips
• Document all cause and effect relationships
l d ll d f h d l
21
• Include all current diagnoses as part of the current medical decision making and make note of them in the note on every visit
• Each note needs date, signature and credentials• Document history of heart attack, status codes, etc.
• Only document diagnoses as “history of” or “PMH” when they no longer exist or are not a current condition
Significance to Providers
• Using specific ICD‐10 diagnosis codes will help convey the true
22
g p g p yseriousness of the conditions being addressed on each visit
• Documenting these involves:
1. Identifying the diagnosis as a current or ongoing problem, as opposed to a past medical history or previous condition
2 Choosing the most specific diagnosis code while also being sure2. Choosing the most specific diagnosis code while also being sure that is supported in documentation
4/28/2016
12
Coding from CC or HPI
• All documented diagnoses should be coded ‐ review chief complaint and HPI documentation carefully
23
and HPI documentation carefully
• Physician’s specific wording determines whether a condition is current for the particular encounter
• A “history of” statement can be interpreted as historical only and no longer existing, or as a current ongoing problem that has been
t f l tipresent for a long time
• Do not code conditions noted only in the problem list or medical history unless the condition meets the TAMPER criteria
Documentation for Coding
• Chronic conditions affect the management of the patient, even when th ti t i ti ith t i htf d ill th t ld
24
the patient is presenting with a straightforward illness that would appear unrelated to the chronic condition
• “History of” conditions are informational unless it’s documented how the patient’s care was impacted by that history
• Conditions can only be coded/reported if there is documentation that the condition has affected the patient’s treatment and management on that particular encounter
4/28/2016
13
TAMPER Documentation
• Ensure there is at least one element of TAMPER documented for
25
each coded condition
T = Treatment
A = Assessment
M = Monitor/Medicate
P = Plan E = Evaluate R = Referral
• TAMPER can be found in any section of the patient record
Documentation Goals• For each patient:
Report all c rrent diagnoses at the highest le el of specificit▫ Report all current diagnoses at the highest level of specificity based on physician documentation
▫ The more categories of diagnoses reported over a year creates a higher risk score
▫ Only one diagnosis per category is used in the risk score l lcalculation
If both angina and AMI are reported in one year, only the AMI is scored as it is at a higher level of specificity within the Heart category
4/28/2016
14
HCC Audits
Audit Example 200 Providers/2000 Records ….issues identified: Incomplete or illegible recordsIncomplete or illegible recordsCoding from a super billCoding from a problem listReporting only primary diagnosisUse of generic or unspecified codesCoding history of as currentCoding history of as currentNot linking manifestations and complicationsOverlooking chronic conditions
4/28/2016
15
Case ExampleChief Complaint: Routine physicalHPI: The patient is a 63 year old white male who comes to HPI: The patient is a 63 year old white male who comes to the office for his wellness exam. H/O gout, takes no medication. Refers to having visual problems for the last 5 months. Lifestyle modification discussed at length with the patient that include 1.5 sodium daily diet, daily exercise, smoking y , y , gcessation, balanced diet. If symptoms worsen to return for further eval.
Case Example, continued Physical ExaminationConstitutional: General appearance: well-developed, well-nourished, well-groomed, normal habitus, no obvious deformities noted. No acute distress.Neurological: Alert and oriented to person, place, time and condition. Mini-mental status exam unremarkable. Cranial nerves II-XII grossly intact by direct confrontation. Motor 5/5 strength throughout with good tone. Sensory intact throughout to pain, light touch, vibratory. Gait is symmetrical and balanced. Romberg is negative. Reflexes 2+ symmetrical with negative Babinski. No asterixis. Psychiatric: Normal affect and mood. Responds to questions appropriately. No suicidal thoughts or ideation suicidal thoughts or ideation. HEENT and Neck: Abnormalities: Mouth – Cavities, dental (aside from above listed, all others normal)Thorax and Lungs: Chest: symmetrical with equal expansion. No pain, tenderness, or masses upon palpation. Lungs: clear to auscultation and percussion. Breath sounds equal bilaterally. No wheezes, rales (crackles), or rhonchi. No dullness to percussion.
4/28/2016
16
Case Example, continued Physical ExaminationHeart, Pressures, and Pulses: Cardiovascular – Normal S1 and S2. Absent of S3 and S4. Regular rate without murmurs, rubs, heaves, or thrills. Peripheral pulses symmetrical and 2+ throughout. Breasts and Axillae: DeferredAbdomen: Abnormalities: on inguinal area had redness coloration compatible with fungus. Back: Straight and symmetrical. No abnormal spinal curvatures notes. No costovertebral angle tenderness. Anus and Rectum: DeferredExtremities: No clubbing, cyanosis or edema. Pulses 2+ bilaterallyMusculoskeletal: Upper and lower extremities symmetrical, full range of motion noted without joint tenderness, swelling or deformities noted.
Case Example, continued Today’s Diagnosis and Assessment:• 110.1 Onychomycosisy y• 274.9 Gout, unspecified• V70.0 Routine Medical Exam• 715.98 Osteoarthritis unspecified other sites (chronic
condition)• 790.29 Other abnormal glucose • V85.1 BMI between 19-24 Adult
• Do you agree based on the documentation?