is there an association? exposure (risk factor) outcome
TRANSCRIPT

Is There An Association?Is There An
Association?
Exposure(Risk Factor) Outcome

Target Population
Study population
• Collect data• Make comparisons Is there an association?
Are the results valid?ChanceBiasConfounding
Inference
Sample
Testing Whether a Factor Is Associated With Disease
Testing Whether a Factor Is Associated With Disease

Diseased & ExposedDiseased & ExposedDiseased & non-exposed
Diseased & non-exposed
Non-diseased & non-exposed
Non-diseased & non-exposed
Non-diseased & exposed
Non-diseased & exposed
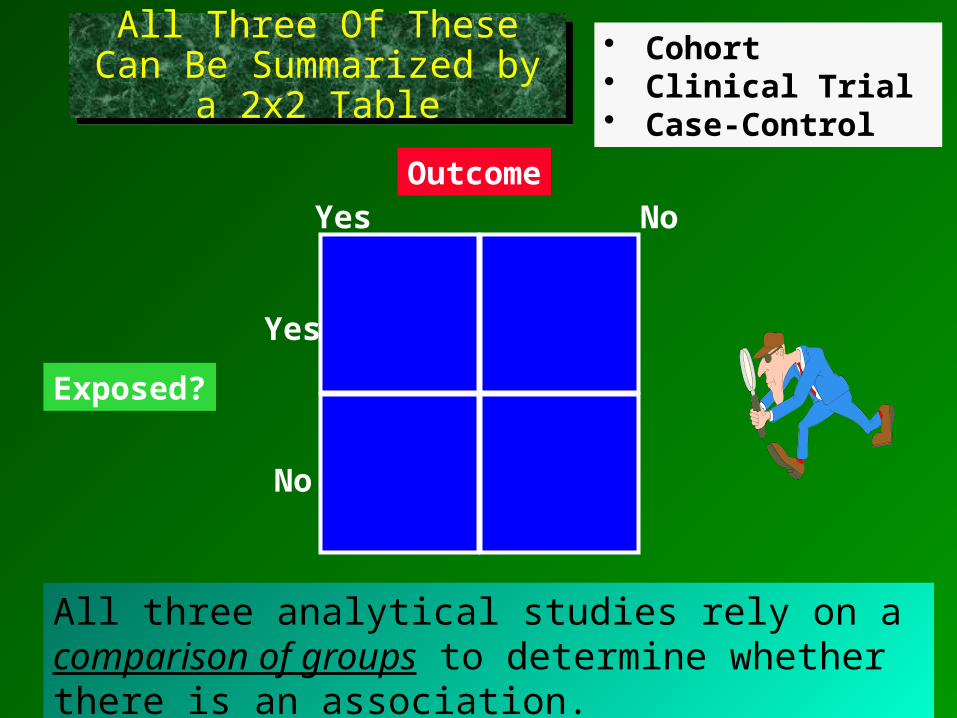
All Three Of These Can Be Summarized by a 2x2 TableAll Three Of These Can Be Summarized by a 2x2 Table
Yes No
Yes
No
Outcome
Exposed?
• Cohort• Clinical Trial • Case-Control
All three analytical studies rely on a comparison of groups to determine whether there is an association.

Wound Infection
Yes No
1 78 79
7 124 131Yes
No
Incidental Appendectomy
How many ways can we compare the groups?
How would you interpret the comparisons?

2) Calculate the difference in incidence between the two groups. (Subtract incidence in control group from the incidence in the exposed group).
Options For Comparing IncidenceOptions For Comparing Incidence
1) Calculate the ratio of the incidences for the two groups. (Divide incidence in exposed group by the incidence in the control group).
Or
Ie
I0
Ie- I0
For Cohort Type Studies

Yes No
Wound Infection
1 78 79
7 124 131 Yes
No
8 202 210 Subjects
RR = 7/131 = 5.3 = 4.2 1/79 1.3
RR = 7/131 = 5.3 = 4.2 1/79 1.3
CumulativeIncidence
5.3%
1.3%
(7/131)
(1/79)
Had IncidentalAppendectomy
Risk RatioRisk Ratio
“Risk Ratio” or “Relative Risk”

RR = =5.3%
1.3%= 4.2
Interpretation: “In this study those who had an incidental appendectomy had 4.2 times the risk compared to those who did not have appendectomy.”
Interpretation: “In this study those who had an incidental appendectomy had 4.2 times the risk compared to those who did not have appendectomy.”
5.3%
1.3%
Also had appendectomy
No appendectomy
A ratio;
no dimensions.
Risk Ratio in Appendectomy Study
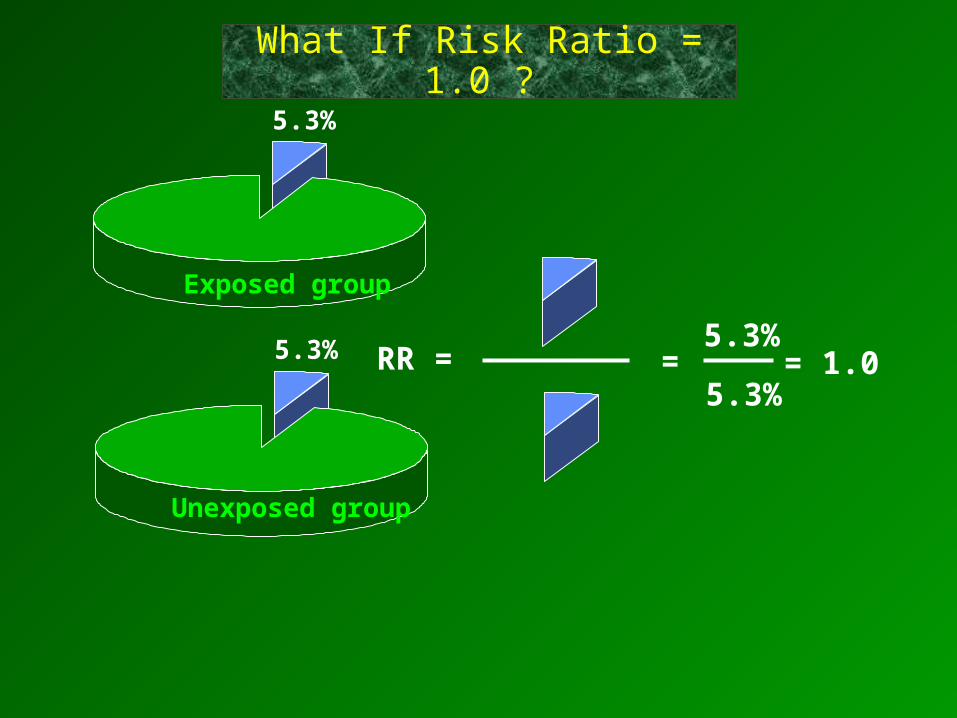
RR = =5.3%
= 1.05.3%
5.3%
5.3%
Exposed group
Unexposed group
What If Risk Ratio = 1.0 ?

Yes NoMyocardial Infarction
Yes
No
378 21,693 22,071 subjects
139 10,898 11,037 exposed
Aspirin Use
239 10,795 11,034 not exposed
RR = .0126 = 0.55 .0221
RR = .0126 = 0.55 .0221
Iexposed = 139/11,037 = .0126
Iunexposed = 239/11034 = .0221
Iexposed = 139/11,037 = .0126
Iunexposed = 239/11034 = .0221
What If Relative Risk < 1.0 ?What If Relative Risk < 1.0 ?
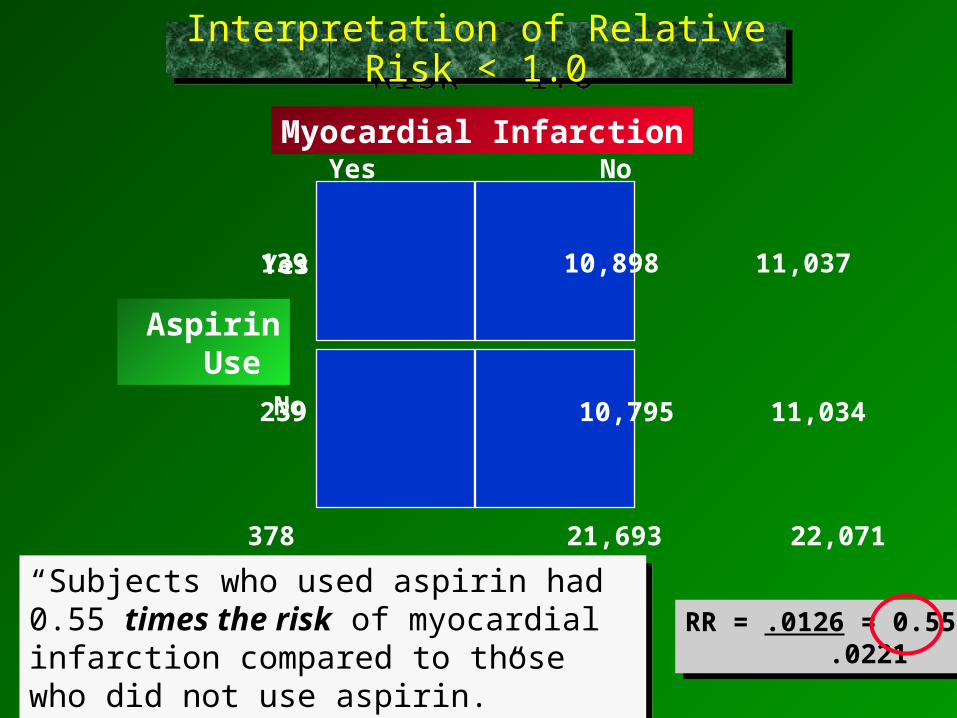
Yes NoMyocardial Infarction
Yes
No
378 21,693 22,071
139 10,898 11,037
Aspirin Use
239 10,795 11,034
RR = .0126 = 0.55 .0221
RR = .0126 = 0.55 .0221
“Subjects who used aspirin had 0.55 times the risk of myocardial infarction compared to those who did not use aspirin.”
“Subjects who used aspirin had 0.55 times the risk of myocardial infarction compared to those who did not use aspirin.”
Interpretation of Relative Risk < 1.0Interpretation of Relative Risk < 1.0

Yes No
Disease
c - PY0
a - PY1 Yes
No
IR
a/PY1
c/PY0
Total Disease-freeObs. Time
Relative risk = a/PY1
c/PY0
Relative risk = a/PY1
c/PY0
Exposure
“Rate Ratio” or “Relative Risk”
Data Summary for Incidence RateData Summary for Incidence Rate

Yes No
Coronary Artery Disease
60 - 51,477.5
30 - 54,308.7Yes
No
90 105,786.2
Person-Years of Follow Up
Incidence In treated group = 30 / 54,308.7 = 55.2 / 100,000 P-Yrs
In untreated group = 60 / 51,477.5 = 116.6 / 100,000 P-Yrs
Rate Ratio = 55.2 /100,000 P-Yr. = 55.2 = 0.47 116.6 /100,000 P-Yr. 116.6
Rate Ratio = 55.2 /100,000 P-Yr. = 55.2 = 0.47 116.6 /100,000 P-Yr. 116.6
Postmenopausal Hormones

It is more precise to say that postmenopausal women on HRT had 0.47 times the rate of coronary disease, compared to women not taking HRT.
In practice, however, many people interpret it just like a risk ratio.

Risk Ratios.0336/.0336=1.00.0415/.0336=1.23.0445/.0336=1.33
Cumulative Incidence
2,264/67,424=.0336
61/1,469 =.0415
30/674 =.0445
Low
Medium
High
Magnetic Field
Exposure
Magnetic Field
Exposure
LeukemiaNo
LeukemiaTotals
2,264 65,160 67,424
61 1,408 1,469
30 644 674
Multiple Exposure CategoriesMultiple Exposure Categories

The Nurse’s Health Study
ObesityNon-fatal MyocardialInfarction
?
# MIs(non-fatal)
41
57
56
67
85
Person-yearsof observation
177,356
194,243
155,717
148,541
99,573
Rate of MI per100,000 P-Yrs
(incidence)23.1
29.3
36.0
45.1
85.4
Rate Ratio
1.0
1.3
1.6
2.0
3.7
Multiple Exposure Categories - An “r x c” (row/column) TableMultiple Exposure Categories
- An “r x c” (row/column) Table
<21
21-23
23-25
25-29
>29
BMI:
wgt kghgt m2
?

RD = Incidence in exposed - Incidence in unexposed
Risk Difference = Ie - I0
The Risk Difference (Attributable Risk)
The Risk Difference (Attributable Risk)

Yes No
Wound Infection
1 78 79
7 124 131 Yes
No
8 202 210 subjects
Had IncidentalAppendectomy
CumulativeIncidence
5.3%
1.3%
RD = 0.053 – 0.013 = 0.04 = 4 per 100RD = 0.053 – 0.013 = 0.04 = 4 per 100
Risk Difference in Appendectomy StudyRisk Difference in Appendectomy Study

Even if appendectomy is not done, there is a risk of wound infection (1.3 per 100).
… the RD is the excess risk in those who have the factor, i.e., the risk of wound infection that can be attributed to having an appendectomy, assuming there is a cause-effect relationship.
Adding an appendectomy appears to increase the risk by (4 per 100 appendectomies), so ...
1.3/100
ExposedNot Exposed
Excess risk is
4 per 100
5.3/100
Risk Difference Gives a Different Perspective on the Same Information

Example:Incidence with appendectomy = 5.3% = 0.053Incidence without appendectomy = 1.3% = 0.013 Risk Difference = 0.040 = 40/1000
i.e., 4 per 100 incidental appendectomies or 40 per 1,000 incidental appendectomies
Interpretation:In the group that underwent incidental appendectomy there were 40 excess wound infection per 1000 subjects (or 4 per 100).
Interpretation:In the group that underwent incidental appendectomy there were 40 excess wound infection per 1000 subjects (or 4 per 100).
Convert % to convenient fractions to interpret for a group of people.
Tip #1 for Interpretation of Risk DifferenceTip #1 for Interpretation of Risk Difference

The focus is on the excess disease in the exposed group.
This implies that if incidental appendectomy were performed on another 1,000 subjects having staging surgery, we would expect 40 excess wound infections attributable to the incidental appendectomy.
Interpretation:In the group with incidental appendectomy there were 4 excess wound infections per 100 subjects.
Tip #2 for Interpretation of Risk DifferenceTip #2 for Interpretation of Risk Difference

Don’t forget to specify the time period when you are describing RD for cumulative incidence.
In the appendectomy study the time period was very brief and was implicit (“postoperatively”) it wasn’t necessary to specify the time frame. However, for most cohort studies it is important. Remember that with cumulative incidence, the time interval is described in words.
Interpretation:In the group that failed to adhere closely to the Mediterranean diet there were 120 excess deaths per 1,000 men during a two year period of observation.
Tip #3 for Interpretation of Risk DifferenceTip #3 for Interpretation of Risk Difference

85.4
23.1
# MIs(non-fatal)
41
57
56
67
85
Person-yearsof observation
177,356
194,243
155,717
148,541
99,573
Rate of MI per100,000 P-Yrs
(incidence)
29.3
36.0
45.1
Relative Risk
1.0
1.3
1.6
2.0
3.7
Risk Difference= 85.4/100,000 - 23.1/100,000 = 62.3 excess cases / 100,000 P-Y in the heaviest group
Risk Difference= 85.4/100,000 - 23.1/100,000 = 62.3 excess cases / 100,000 P-Y in the heaviest group
Rate DifferencesRate Differences
<21
21-23
23-25
25-29
>29
BMI:
wgt kghgt m2

Among the heaviest women there were 62 excess cases of heart disease per 100,000 person-years of follow up that could be attributed to their excess weight.
This suggests that if we followed 50,000 women with BMI > 29 for 2 years we might expect 62 excess myocardial infarctions due to their weight. (Or one could prevent 62 deaths by getting them to reduce their weight.)
Rate Difference InterpretationRate Difference Interpretation
If 100,000 obese women had remained lean, it would prevent 62 myocardial infarctions per year.
or

Influenza Vaccination and Reduction in Hospitalizations for Cardiac Disease and Stroke among the Elderly. Kristin Nichol et al.: NEJM 2003;348:1322-32.
These investigators used the administrative data bases of three large managed care organizations to study the impact of vaccination in the elderly on hospitalization and death. Administrative records were used to whether subjects had received influenza vaccine and whether they were hospitalized or died during the year of study. The table below summarizes findings during the 1998-1999 flu season.

Vaccinated subjects
(N=77,738)
Unvaccinated subjects
(N=62,217)Hospitalization for pneumonia or influenza
495 581
Hospitalization for cardiac disease
888 1026
Death 943 1361
Died Not Dead
Vaccinated 943 (77,738 - 943)
Not Vaccinated 1361 (62,217 – 1,361)
If the exposure is vaccination & outcome of interest is death, what is the risk difference?
RD = CIe – CIu = (943 / 77,738) - (1,361 / 62,317) = -0.0097
= - 97/10,000 over a year
77,73862,217

-97/10,000 over a year
Instead of calling it ‘excess risk’, just refer to it as a ‘risk reduction.’
Can a risk difference be a negative number?Can a risk difference be a negative number?

RR & RD Provide Different Perspectives
RR & RD Provide Different Perspectives
Relative Risk: shows the strength of the association. RR = 1.0 suggests no associationRR close to 1.0 suggests weak associationRR >> 1.0 or RR << 1.0 suggests a strong association
Risk Difference: a better measure of public health impact.How much impact would prevention have?How many people would benefit?

FOBTFOBTA large study looked at whether fecal occult blood testing (FOBT) could decrease mortality from colorectal cancer (CRC).
Relative Risk Perspective: FOBT decreased mortality from CRC by 33% !(RR = .67 for FOBT compared to no screening)
Risk Difference Perspective: FOBT decreased mortality from 9 per 1,000 people to 6 per 1,000.So, RR= 0.67 (i.e., 0.006/0.009 BUTThe risk difference was only 3 per 1,000 people screened.
The ratio of these two numbers is more impressive than the actual difference.
The ratio of these two numbers is more impressive than the actual difference.

Lung Cancer Cigarette smokers 140Non-smokers 10
Coronary Heart DiseaseCigarette smokers 669Non-smokers 413
Annual Mortality per 100,000 (CI)
RR= 14RD= 130 per 100,000
RR= 14RD= 130 per 100,000
RR= 1.6RD= 256 per 100,000
RR= 1.6RD= 256 per 100,000
Calculate RR & RD for Two DiseasesCalculate RR & RD for Two Diseases
Annual Mortality per 100,000 (CI)
Smoking is a stronger risk factor for …. ?Smoking is a bigger public health problem for …. ?

Lung Cancer Heart Disease0
100
200
300
400
500
600
700
800
No
n-s
mo
kers
Sm
oke
rs
Sm
oke
rs
No
n-s
mo
kers

MI 125.9 216.6
Aspirin Placebo RR(/10,000) (/10,000)
0.59
What should we conclude?What should we recommend?
Aspirin & MIAspirin & MI

Stroke 107.8 88.8 1.2
Ischemic 82.4 74.3 1.1
Hemorrhagic 20.8 10.9 1.9
Upper GI ulcer 153.1 125.1 1.2
with hemorrhage 34.4 19.9 1.7
Bleeding 2699.1 2037.3 1.3
Transfusion need 43.5 25.4 1.7
Aspirin Placebo RR(/10,000) (/10,000)
MI 125.9 216.6 0.59
What should we conclude?What should we recommend?
Benefits & RisksBenefits & Risks

Stroke 107.8 88.8 1.2 19
Ischemic 82.4 74.3 1.1 8
Hemorrhagic 20.8 10.9 1.9 10
Upper GI ulcer 153.1 125.1 1.2 28
with hemorrhage 34.4 19.9 1.7 15
Bleeding 2699.1 2037.3 1.3 690
Transfusion need 43.5 25.4 1.7 18
MI 125.9 216.6 0.59 -100
Aspirin Placebo RR RD(/10,000) (/10,000) (/10,000)
Benefits & Risks

If we are going to discuss rare, but serious possible complications of influenza vaccine, would it be better to look at the Risk Ratio or the Risk Difference?
Observed frequency in:Exposed people: 2 / 100,000Unexposed people: 1 / 100,000
Risk Ratio = 2; those exposed had two times the risk! (OMG!)
Risk Difference = 1 per 100,000; assuming that the exposure is a cause of the outcome, the exposed group had an excess risk of 1 case per 100,000 subjects.

The proportion (%) of disease in the exposed group that can be attributed to the exposure, i.e., the proportion of disease in the exposed group that could be prevented by eliminating the risk factor.
AR% = RD x 100
Ie
.04 x 100 = 75%
.053What % of infections in the exposed group can be attributed to having the exposure?
ExposedNot
Exposed
.013
.053.04
Interpretation: 75% of infections in the exposed group could be attributed to doing an incidental appendectomy.
Attributable Risk % - The Attributable Proportion
Attributable Risk % - The Attributable Proportion

Diseased No Disease Totals Incidence (Risk)
Exposed 500 9,500 10,000 0.050Not Exposed 900 89,100 90,000 0.010
1,400 98,600 100,000 0.014
Total risk in exposed group?
Excess risk in exposed group?
Attributable proportion in exposed group?
0.050 = 50/1,000
0.050 – 0.10 = 40/1,000 over 1 yr.
40/1,000 = 80%50/1,000
Consider this cohort study conducted over 1 year:

The Population Attributable Proportion
Diseased No Disease Totals Incidence
(Risk)
Exposed 500 9,500 10,000 0.050Not Exposed 900 89,100 90,000 0.010
1,400 98,600 100,000 0.014
Of the 1,400 diseased people, only 500 were exposed (35.7%). Of these only 80% can be attributed to the exposure. So, in the total population the fraction of cases that can be attributed to the exposure is 0.357 x 0.80 = 0.286, or 28.6%.

Measuring Association in a Case-Control Study
Measuring Association in a Case-Control Study

To calculate incidence, you need to take a group of disease-free people and measure the occurrence of disease over time.
Odds of having the risk factor prior to disease?
controls
cases
(Already have disease)
(No disease)
But in a case-control study we find diseased and non-diseased people and we measure and compare the prevalence of prior exposures.

Yes No
Wound Infection
1 78 79
7 124 131 Yes
No
Had IncidentalAppendectomy
CumulativeIncidence
5.3%
1.3%
How many exposed people did it take to generate the 7 cases in the 1st cell?
Probability that an exposed person had disease?Odds that an exposed person had disease?
Cohort Study

Yes No
Hepatitis
1 29
18 7Yes
No
19 36
Ate at Deli
Case Control
How many people had to eat at the Deli in order to generate the 18 cases in the 1st cell?
In a true case-control study, you do not know the denominators for exposure groups!
?
?
Case-Control Study

If the outcome is uncommon, the odds of exposure among non-disease subjects will be similar to the odds of exposure among the total population…
So the odds ratio will be a good estimate of the risk ratio.
(7/1,000) = Odds Ratio (7/1,007) = Risk Ratio(6/5,634) (6/5,640)
Diseased Non-diseased Total
Exposed 7 1,000 1,007
Non-exposed 6 5,634 5,640

Diseased Non-diseased Total
Exposed 7 1,000 1,007
Non-exposed 6 5,634 5,640
(7/1,000) = Odds Ratio (7/1,007) = Risk Ratio(6/5,634) (6/5,640)
(7 / 1,000)
(6 /5,634)
7x
1,000 6
5,634 (7/
(1,000
6)
/ 5,634)
7x
1,0006
5,634=
Odds of disease in ExposedOdds of disease in Unexposed
Odds of exposure in DiseaseOdds of exposure in Non-Disease
But this rearranges
algebraically:
= =
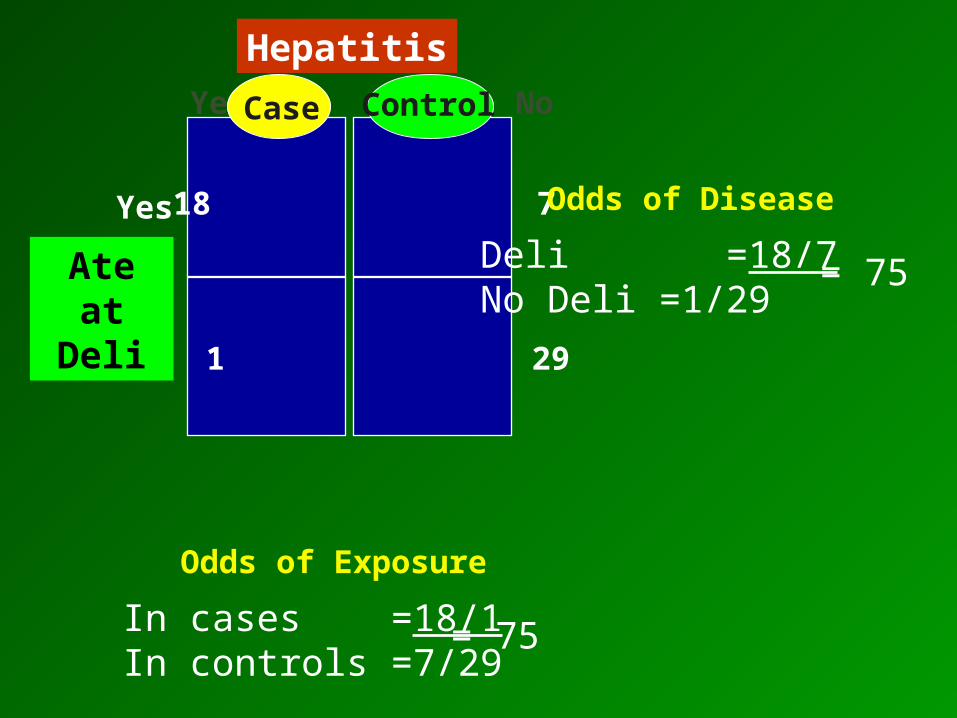
Yes No
Hepatitis
1 29
18 7Yes
No
Ate at Deli
Case Control
In cases =18/1In controls =7/29
= 75
Odds of Exposure
Deli =18/7No Deli =1/29
= 75
Odds of Disease

An Odds Ratio Is Interpreted Like Relative Risk
An Odds Ratio Is Interpreted Like Relative Risk
“Individuals who ate at the Deli had 75 times the risk of hepatitis A compared to those who did not eat at the Deli.”
An odds ratio is a good estimate of relative risk when the outcome is relatively uncommon.
The odds ratio exaggerates relative risk when the outcome is more common.

In cohort studies and clinical trials you can calculate incidence, so you can calculate either a relative risk or an odds ratio.
In a case-control study, you can only calculate an odds ratio.
You can always calculate an odds ratio, but…You can always calculate an odds ratio, but…

Yes NoGot Giardiasis
14 341 355
16 108 124 Yes
No
Exposed to Kiddy Pool
Cohort Design: Calculate RR or OR
Cohort Design: Calculate RR or OR
I can compute either RR or OR here. Why?
Compare frequencyof GiardiaNot
Kid pool

Kid pool
Not
vs.
Yes No Giardia
16 108
14 341
RiskRatio = 3.3
RiskRatio = 3.3
16 / (16+108) = 12.9%
14 / (14+341) = 3.9%
Cumulative Incidence
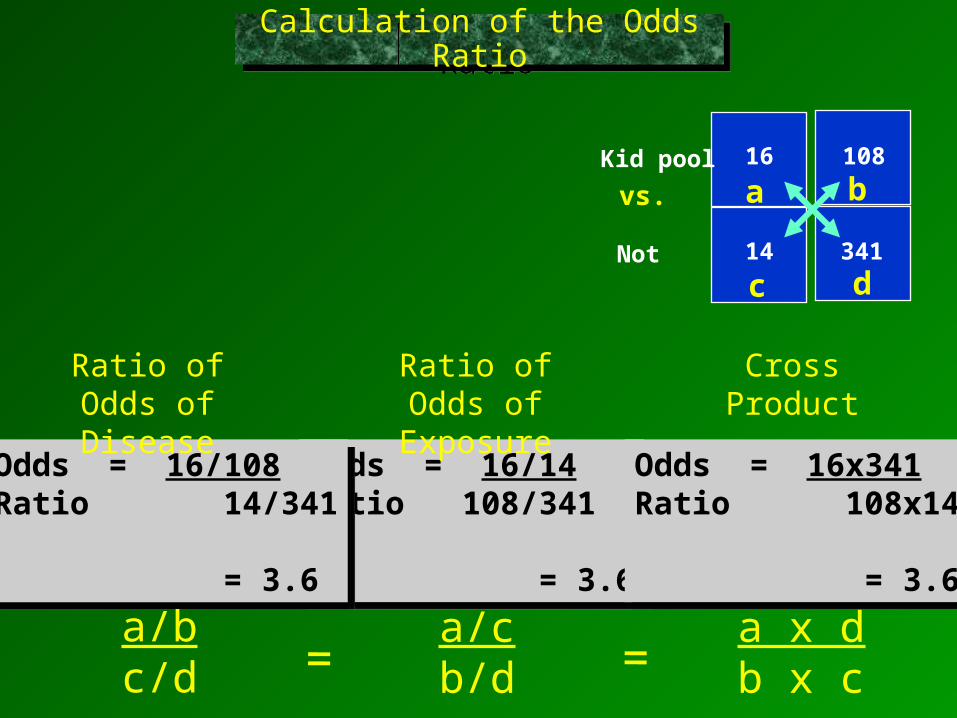
Odds = 16/14Ratio 108/341
= 3.6
Odds = 16/14Ratio 108/341
= 3.6
Odds = 16/14Ratio 108/341
= 3.6
Odds = 16/14Ratio 108/341
= 3.6
a/cb/d
a x db x c=
16 108
14 341
Kid pool
Not
vs. a b
c d
Odds = 16x341Ratio 108x14
= 3.6
Odds = 16x341Ratio 108x14
= 3.6
Calculation of the Odds RatioCalculation of the Odds Ratio
Odds = 16/108Ratio 14/341
= 3.6
Odds = 16/108Ratio 14/341
= 3.6
=a/bc/d
Ratio of Odds of Disease
Ratio of Odds of Exposure
Cross Product

With a Common Outcome OR Exaggerates RR
With a Common Outcome OR Exaggerates RR
Ie = 60 168
I0 = 45 386
Yes NoOutcome
14 341 386 unexposed
16 108 168 exposed
Yes
No
Risk Factor
16 / (16+108) 14 / (14+341)
RR = 3.3
16 / (16+108) 14 / (14+341)
RR = 3.3
RR = 16 / 108 14 / 341
OR = 3.6
16 / 108 14 / 341
OR = 3.6
OR =

With a Common Outcome OR Exaggerates RR
With a Common Outcome OR Exaggerates RR
Ie = 60 168
I0 = 45 386
Yes NoOutcome
45 341 386 unexposed
60 108 168 exposed
Yes
No
Risk Factor
60 / (60+108) 45 / (45+341)
RR = 3.06
60 / (60+108) 45 / (45+341)
RR = 3.06
RR = 60 / 108 45 / 341
OR = 4.21
60 / 108 45 / 341
OR = 4.21
OR =

You should be able to calculate these measures of disease frequency and measures of association using a simple hand calculator.
Stat Tools will also do them, and there is one question on Quiz 3 for which you are asked to hand calculate an odds ratio and then check your answer using Stat Tools.

N. Engl. J. Med.Abstract
N. Engl. J. Med.Abstract
Racial Disparities in Health CareRacial Disparities in Health Care

Yes No
Referral for Cardiac Cath
326 34 360
305 55 360 Black
White
What was the odds ratio ?
(Calculate and compare your answer with your neighbor’s.)

Yes No
Referral for Cardiac Cath
326 34 360
305 55 360 Black
White
Incidence
• What was the probability that a black patient would be referred for catheterization (cumulative incidence)?
• What was the probability that a white patient would be referred for catheterization? (Calculate and compare your answer with your neighbor’s.)

Yes No
Black
163 17 180 90.5%
163 17 180 90.5%
Referral for Cath.
White
IncidenceYes No
Black
163 17 180 90.5%
142 38 180 78.9%
Referral for Cath.
White
Incidence
What does the stratified analysis suggest?
Males Females
Stratified by GenderStratified by Gender

If you were writing the abstract for the Shulman study, how would you report the major findings?