islhd procedure cover sheet - medfromtheshed.com.au · sepsis pathway should be followed where:...
TRANSCRIPT
INTERNAL ONLY
ISLHD PROCEDURE
COVER SHEET
COMPLIANCE WITH THIS DOCUMENT IS MANDATORY Feedback about this document can be sent to [email protected]
NAME OF DOCUMENT
Sepsis Pathway – Emergency Department
TYPE OF DOCUMENT
Procedure
DOCUMENT NUMBER
ISLHD CLIN PROC 137
DATE OF PUBLICATION
October 2016
RISK RATING
Medium
REVIEW DATE
October 2018
FORMER REFERENCE(S)
Nil
EXECUTIVE SPONSOR or
EXECUTIVE CLINICAL SPONSOR
Director of Medical Services
AUTHOR
Robert Marco - Inpatient Sepsis Project Manager
Sarah Dwyer - Senior Nurse Educator- Wollongong Hospital
KEY TERMS
Emergency, sepsis, antibiotics, guideline, escalation, auditing
SUMMARY
This document is to act as a guideline for staff who suspect patients to have sepsis.
The procedure includes the Clinical Excellence Commissions’ (CEC) sepsis pathway and antibiotics guidelines

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 1 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
1. POLICY STATEMENT
The Emergency Department (ED) Sepsis Pathway is based on the CEC Sepsis ED
guidelines and aims to guide the recognition and management of emergency patients
who are suspected of severe sepsis.
Clinicians are required to refer to the Sepsis pathway when they recognise a patient’s
clinical condition is deteriorating. Where signs and/or symptoms of sepsis are
identified the Sepsis Pathway must be followed until the AMO determines that sepsis
is not the cause of deterioration.
Quick administration of antibiotics and resuscitation fluids is vital in the management
of the patient with sepsis. The goal is to commence antibiotic therapy within the first
hour of recognition and diagnosis of sepsis.
The guideline is based on the Therapeutic Guidelines: Antibiotic Version 15 and
incorporates best available evidence and the principles of appropriate use of
antibiotics. The selection of appropriate antimicrobial therapy in sepsis management is
complex and this guideline is not intended to cover all possible scenarios.
AIMS of the Sepsis Pathway
Recognise sepsis early and escalate appropriately.
Initiate appropriate management: Give IV antibiotics and fluids within one hour of
identification.
Provide appropriate follow up management to ensure sepsis is treated adequately
or pathway is ceased if not required.
2. BACKGROUND
Sepsis is a medical condition where the immune system goes into overdrive. This process
releases chemicals into the blood to combat infection and trigger widespread
inflammation. If the body is unable to control this immune response, it then overwhelms
normal blood processes. This progression can lead to severe sepsis and septic shock
which leads to organ dysfunction, hypotension, or hypoperfusion to one or more organs1.
INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 2 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
3. RESPONSIBILITIES
This guideline applies to all medical, nursing and allied health staff who attend to the care
and treatment of hospital inpatients.
4. PROCEDURE
4.1 Procedure for Milton Hospital, Shellharbour Hospital, Shoalhaven District Hospital and Wollongong Hospital
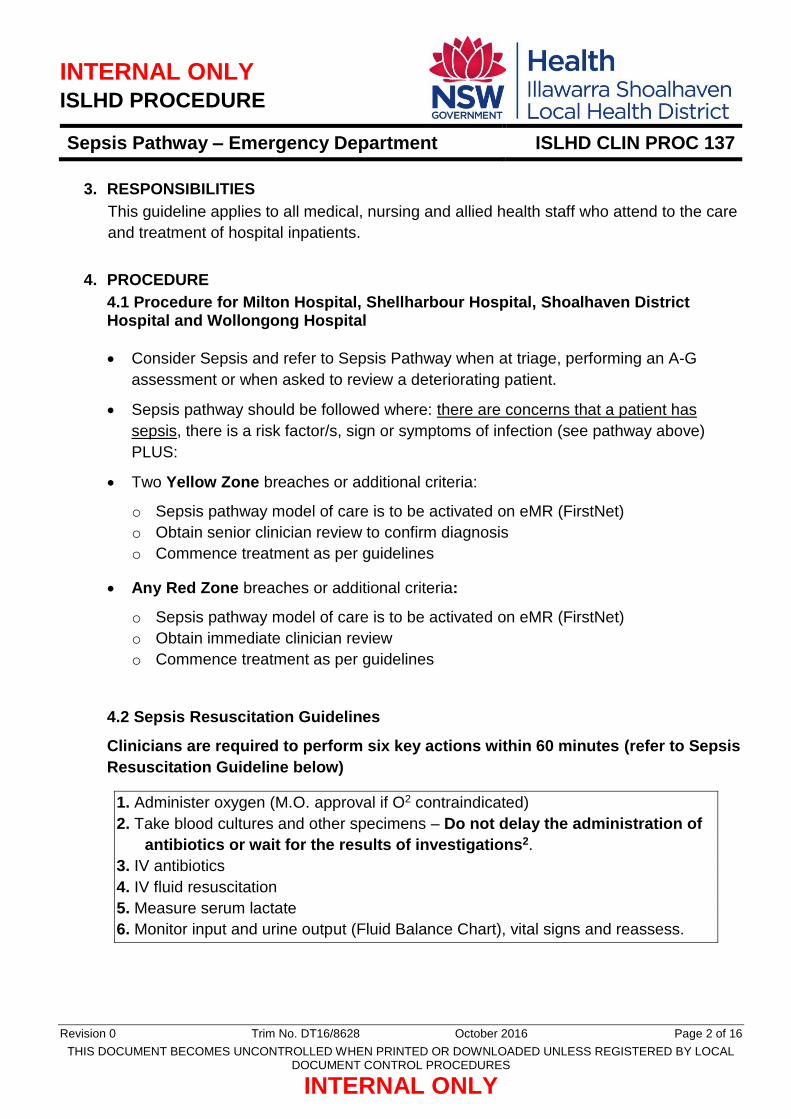
Consider Sepsis and refer to Sepsis Pathway when at triage, performing an A-G
assessment or when asked to review a deteriorating patient.
Sepsis pathway should be followed where: there are concerns that a patient has
sepsis, there is a risk factor/s, sign or symptoms of infection (see pathway above)
PLUS:
Two Yellow Zone breaches or additional criteria:
o Sepsis pathway model of care is to be activated on eMR (FirstNet)
o Obtain senior clinician review to confirm diagnosis
o Commence treatment as per guidelines
Any Red Zone breaches or additional criteria:
o Sepsis pathway model of care is to be activated on eMR (FirstNet)
o Obtain immediate clinician review
o Commence treatment as per guidelines
4.2 Sepsis Resuscitation Guidelines
Clinicians are required to perform six key actions within 60 minutes (refer to Sepsis
Resuscitation Guideline below)
1. Administer oxygen (M.O. approval if O2 contraindicated)
2. Take blood cultures and other specimens – Do not delay the administration of
antibiotics or wait for the results of investigations2.
3. IV antibiotics
4. IV fluid resuscitation
5. Measure serum lactate
6. Monitor input and urine output (Fluid Balance Chart), vital signs and reassess.
INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 3 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
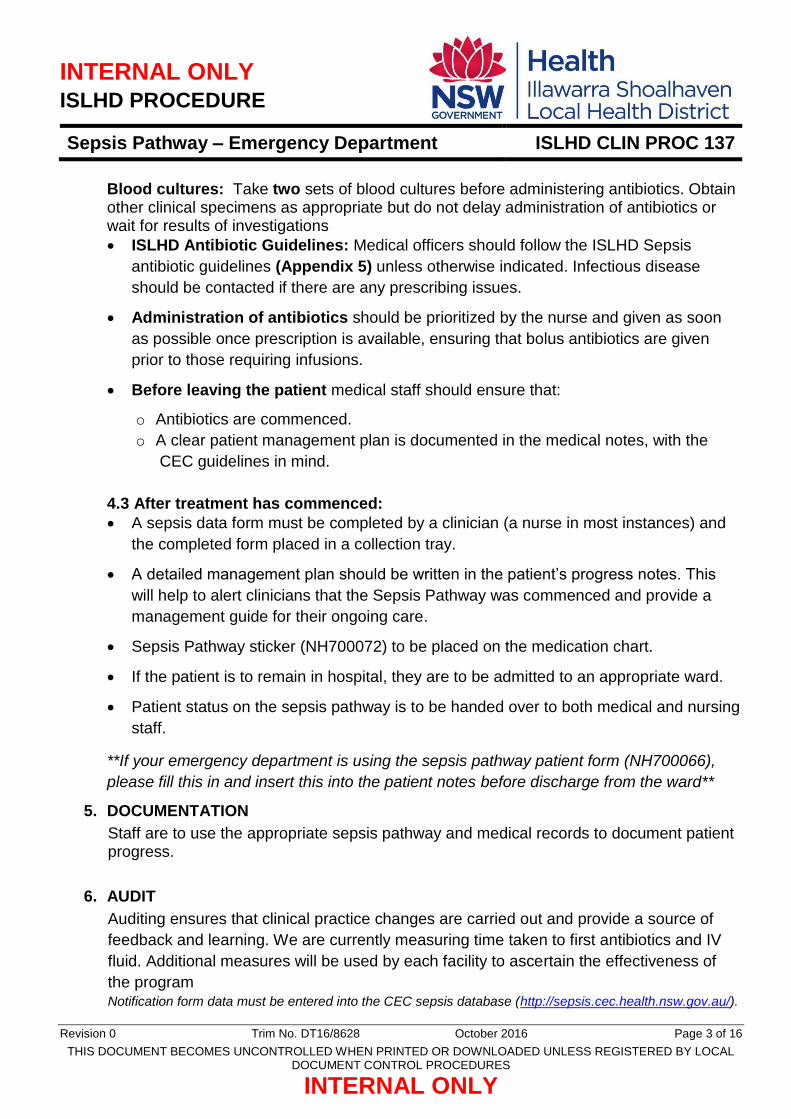
Blood cultures: Take two sets of blood cultures before administering antibiotics. Obtain other clinical specimens as appropriate but do not delay administration of antibiotics or wait for results of investigations
ISLHD Antibiotic Guidelines: Medical officers should follow the ISLHD Sepsis
antibiotic guidelines (Appendix 5) unless otherwise indicated. Infectious disease
should be contacted if there are any prescribing issues.
Administration of antibiotics should be prioritized by the nurse and given as soon
as possible once prescription is available, ensuring that bolus antibiotics are given
prior to those requiring infusions.
Before leaving the patient medical staff should ensure that:
o Antibiotics are commenced.
o A clear patient management plan is documented in the medical notes, with the
CEC guidelines in mind.
4.3 After treatment has commenced:
A sepsis data form must be completed by a clinician (a nurse in most instances) and
the completed form placed in a collection tray.
A detailed management plan should be written in the patient’s progress notes. This
will help to alert clinicians that the Sepsis Pathway was commenced and provide a
management guide for their ongoing care.
Sepsis Pathway sticker (NH700072) to be placed on the medication chart.
If the patient is to remain in hospital, they are to be admitted to an appropriate ward.
Patient status on the sepsis pathway is to be handed over to both medical and nursing
staff.
**If your emergency department is using the sepsis pathway patient form (NH700066),
please fill this in and insert this into the patient notes before discharge from the ward**
5. DOCUMENTATION
Staff are to use the appropriate sepsis pathway and medical records to document patient progress.
6. AUDIT
Auditing ensures that clinical practice changes are carried out and provide a source of
feedback and learning. We are currently measuring time taken to first antibiotics and IV
fluid. Additional measures will be used by each facility to ascertain the effectiveness of
the program Notification form data must be entered into the CEC sepsis database (http://sepsis.cec.health.nsw.gov.au/).

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 4 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
7. REFERENCES
Internal:
ISLHD CLIN PD 86 – Sepsis Management
ISLHD CLIN PROC 136 – Sepsis Pathway - Inpatient
ISLHD CLIN PROC 95 - Transfer to Higher Level Care
ISLHD CLIN PD 52- Between the Flags (BTF) - Patient with Acute Condition for Escalation (PACE) - Management of Clinical Deterioration:
ISLHD CLIN PD 54 - Emergency Department Admission Process External: 1. Chang, H, Lynm, C & Glass, R, 2012, ‘Sepsis’, Journal of the American Medical
Association, vol. 304, no. 16, pp.1813. Available from: http://jama.jamanetwork.com/data/Journals/JAMA/4534/jpg1027_1856_1856.pdf
2. Australian Commission on Safety and Quality in Health Care. Antimicrobial Stewardship Clinical Care Standard. Sydney: ACSQHC, 2014
3. Antibiotic Expert Group. Therapeutic Guidelines: Antibiotic Version 15 Melbourne: Therapeutic Guidelines Limited; 2014 Accesses through eTG complete (via CIAP)
4. Burridge N (ed). Australian Injectable Drugs Handbook (5th Ed). The society of Hospital Pharmacists Australia; 2011
8. REVISION AND APPROVAL HISTORY
Date Revision No. Author and Approval
October 2016
0 Robert Marco - Inpatient Sepsis/VTE Project Manager
Draft for comment February 2016
Endorsed ISLHD Drug & Therapeutics June 2016
IV Antibiotic Guideline Update and Pathway Updates August 2016
Distributed to Divisional Co-directors August 2016
Approved Clinical Governance Council October 2016

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 5 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
Sepsis pathways should not be printed from this procedure. For the most up to date pathway please check via the following link: http://cec.health.nsw.gov.au/patient-safety-programs/adult-patient-safety/sepsis-kills/sepsis-tools
Appendix 1 – Adult Sepsis Pathway

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 6 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
Appendix 2 – Paediatric Sepsis Pathway

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 7 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
Appendix 3 – Maternal Sepsis Pathway

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 8 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
Appendix 4 – Newborn Sepsis Pathway

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 9 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
APPENDIX 5 – Antibiotic Prescribing Guide
ADULT SEVERE SEPSIS INTRAVENOUS ANTIBIOTIC GUIDELINE (Review after 24 hours)
Sepsis = Infection + SIRS (Temp <36/ >38, RR > 24, HR >90, WCC < 4/ > 12) SEVERE SEPSIS= Sepsis + Deteriorating Organ Function
ACTIONS (For ALL Sepsis) 1. Lactate 2. Blood cultures 3. IV antibiotics 4. Fluid Resus
Follow the sepsis pathway in conjunction with your local BTF RED & YELLOW Zone escalation procedures.
Source not covered below, recent travel, or HIGH risk of multi-resistant organisms? Antimicrobial stewardship (AMS) hotlines: 3838 (TWH, SHH, SDMH, CDH); #2828 (BDH, MUH); 3535 (PKH)
For patients already on antibiotics: Contact AMO or ID (AMS hotline or switchboard) for advice.
For sepsis in renal patients (e.g. PD peritonitis), contact the renal team via switchboard.
Doses below are for SEVERE sepsis and SEPTIC SHOCK. For non-severe sepsis doses, refer to the Therapeutic Guidelines
Likely source of SEVERE sepsis
Preferred regimen Penicillin allergy (NOT anaphylaxis)
Penicillin/cephalosporin allergy (anaphylaxis)
Severe sepsis of unknown origin
OR intravascular device source
OR surgical site source
Flucloxacillin 2g 6-hourly PLUS
gentamicin 7mg/kg IDEAL body weight
PLUS vancomycin 25-30mg/kg
ACTUAL body weight
If gentamicin contraindicated, use piperacillin/tazobactam
4.5g 6-hourly instead of flucloxacillin and gentamicin
Cefazolin 2g 6-hourly PLUS
gentamicin 7mg/kg IDEAL body weight
PLUS vancomycin 25-30mg/kg
ACTUAL body weight
If gentamicin contraindicated, use meropenem 2g 8-hourly
instead of cefazolin and gentamicin
Gentamicin 7mg/kg IDEAL body weight
PLUS vancomycin 25-30mg/kg
ACTUAL body weight
If gentamicin contraindicated,
call AMS/ID for advice
Severe sepsis due to community-acquired
pneumonia
Ceftriaxone 1g 12-hourly PLUS
azithromycin 500mg daily
Ceftriaxone 1g 12-hourly PLUS
azithromycin 500mg daily
Moxifloxacin 400mg daily
Severe sepsis due to hospital acquired
pneumonia - low risk of MRO
(no recent intubation)
Ceftriaxone 1g 12-hourly PLUS
metronidazole 500mg 12-hourly
Ceftriaxone 1g 12-hourly PLUS
metronidazole 500mg 12-hourly
Moxifloxacin 400mg daily
Severe sepsis due to hospital acquired
pneumonia - high risk of MRO (recent intubation,
prior infection,
Piperacillin-tazobactam 4.5g 6-hourly
If risk of MRSA, ADD vancomycin 25-30mg/kg
ACTUAL bodyweight
Cefepime 2g 8-hourly
If risk of MRSA, ADD vancomycin 25-30mg/kg
ACTUAL bodyweight
Call AMS/ID for advice
Consider vancomycin if Staphylococcal pneumonia suspected (recent ‘flu, cavitation, rapid progression)

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 10 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
colonised)
Severe sepsis with skin source
Flucloxacillin 2g 6-hourly PLUS
vancomycin 25-30mg/kg ACTUAL bodyweight
Cefazolin 2g 8-hourly PLUS
vancomycin 25-30mg/kg ACTUAL bodyweight
Vancomycin 25-30mg/kg ACTUAL body weight
Severe sepsis with urinary source
(If recent TRUS
biopsy, call AMS/ID for advice)
Gentamicin 7mg/kg IDEAL bodyweight
PLUS ^ampicillin 2g 6-hourly
If gentamicin contraindicated, use ceftriaxone 1g 12-hourly
Gentamicin 7mg/kg IDEAL bodyweight
If gentamicin contraindicated, use ceftriaxone 1g 12-hourly
Gentamicin 7mg/kg IDEAL bodyweight
If gentamicin contraindicated, call AMS/ID for advice
Biliary or gastrointestinal
source
Gentamicin 7mg/kg IDEAL bodyweight
PLUS ^ampicillin 2g 6-hourly
PLUS metronidazole
500mg 12-hourly
If gentamicin contraindicated, use piperacillin/tazobactam
4.5g 6-hourly
Ceftriaxone 1g 12-hourly PLUS
metronidazole 500mg 12-hourly
Call AMS/ID for advice
Peri- or post-partum severe sepsis
(See maternal sepsis pathway for ongoing
therapy)
Piperacillin-tazobactam 4.5g 6-hourly
If patient meets toxic shock criteria, ADD
clindamycin 600mg 8-hourly
Ceftriaxone 1g 12-hourly PLUS
metronidazole 500mg 12-hourly
If patient meets toxic shock criteria, ADD
clindamycin 600mg 8-hourly
Call AMS/ID for advice
Severe sepsis with neurological source
(organism or susceptibility
unknown)
Ceftriaxone 2g 12-hourly PLUS
vancomycin 25-30mg/kg ACTUAL bodyweight
If risk of listeria ADD
benzylpenicillin 2.4g 4-hourly
Moxifloxacin 400mg daily PLUS
vancomycin 25-30mg/kg ACTUAL bodyweight
If risk of listeria,
call AMS/ID for advice.
Moxifloxacin 400mg daily PLUS
vancomycin 25-30mg/kg ACTUAL bodyweight
If risk of listeria,
call AMS/ID for advice.
If post-neurosurgical, give meropenem 2g 8-hourly PLUS vancomycin 25-30mg/kg ACTUAL body weight
Intravenous dexamethasone may be required before antibiotics – refer to Therapeutic Guidelines

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 11 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
Severe sepsis due to diabetic foot infection
Piperacillin-tazobactam 4.5g 6-hourly
PLUS vancomycin 25-30mg/kg
ACTUAL bodyweight
Ciprofloxacin 400mg 12-hourly PLUS
clindamycin 600mg 8-hourly PLUS
vancomycin 25-30mg/kg ACTUAL bodyweight
Ciprofloxacin 400mg 12-hourly PLUS
clindamycin 600mg 8-hourly PLUS
vancomycin 25-30mg/kg ACTUAL bodyweight
Febrile neutropenia
(refer to local protocol)
Piperacillin-tazobactam 4.5g 6-hourly
AND refer to local protocol
Cefepime 2g 8-hourly AND refer to local protocol
Call AMS/ID for advice
Once prescribed, enter antibiotic approval/s in Guidance MS.
^If ampicillin unavailable use benzylpenicillin 2.4 grams 6-hourly.

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 12 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
TABLE 2: ANTIBIOTIC ADMINISTRATION
Reconstitute antibiotics with sterile water for injection (WFI) unless stated otherwise.
If further dilution is required for IV injection or infusion, use sterile sodium chloride 0.9% or sterile glucose 5% unless stated
otherwise.
Where possible use separate dedicated lines for resuscitation fluid and for medications. When injecting antibiotics directly
into an IV injection port which has resuscitation fluid running:
- clamp the infusion fluid line and flush with 20 mL sterile sodium chloride 0.9% solution
- administer antibiotic over the required time
- flush the line with 20 mL sterile sodium chloride 0.9% solution and recommence resuscitation fluid.
For detailed information refer to the SHPA injectable handbook via CIAP:
http://aidh.hcn.com.au/index.php/section-one/drug-monographs-a-z?view=alphacontent
Antibiotic Presentation
(adult)
Recon fluid
/volume
Final
volume
Minimum
admin time
Notes
Ampicillin Vial 1g 10 mL NS 10-20 mL 3-5 min Penicillin class antibiotic
Azithromycin Vial 500mg 4.8mL WFI 250mL 60 min 250mL sodium chloride 0.9%
Benzylpenicillin Vial 1.2g 3.2mL WFI 10mL 5-10 min Penicillin class antibiotic. Do no inject
faster than 300mg/min
Cefepime Vial 1 g 10 mL NS 10 mL 3-5 min
Cephalosporin class antibiotic
Doses ≥ 2 g infused over 20 min
Ceftriaxone Vial 1 g 10 mL WFI 10 mL 2–4 min Cephalosporin antibiotic incompatible
with calcium containing solutions,
flush before and after with sodium
chloride 0.9%
Cefazolin Vial 1 g 10 mL WFI 10 mL 3–5 min Cephalosporin class antibiotic
Ciprofloxacin Infusion bag
400mg/200mL
N/A 200mL 60 min May induce seizures in epileptics
Flucloxacillin Vial 1 g 5 mL WFI 10 mL 3-5 min
(1 g)
Penicillin class antibiotic
Repeated doses of 2 g via a
peripheral line should be further
diluted and infused over 30 min
Gentamicin
Ampoule
80 mg/2 mL
N/A 10- 20 mL ≤ 240mg
3–5 min
Refer to notes for Gentamicin
50 mL or
100 mL
> 240mg
30 min
Clindamycin Amp 600mg N/A 50mL 20 min Do not give as bolus injection
Metronidazole Infusion bag
500mg/100mL
N/A 100mL 20 min

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 13 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
Meropenem 1g vial 10 mL WFI 50-250 mL 30-60 min
Moxifloxacin Infusion bag
400 mg/ 250 mL
N/A 250mL 60 min May prolong QT interval and lead to
ventricular arrhythmias.
May induce seizures in epileptics
Piperacillin-
tazobactam
Vial 4 g/0.5 g 20 mL WFI 50 mL 30 min Penicillin class antibiotic
Vancomycin Vial 500 mg 10 mL WFI **5mg/mL
peripheral
Max
10 mg/min
Infusion related effects are common,
decrease infusion rate and monitor
closely
INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 14 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
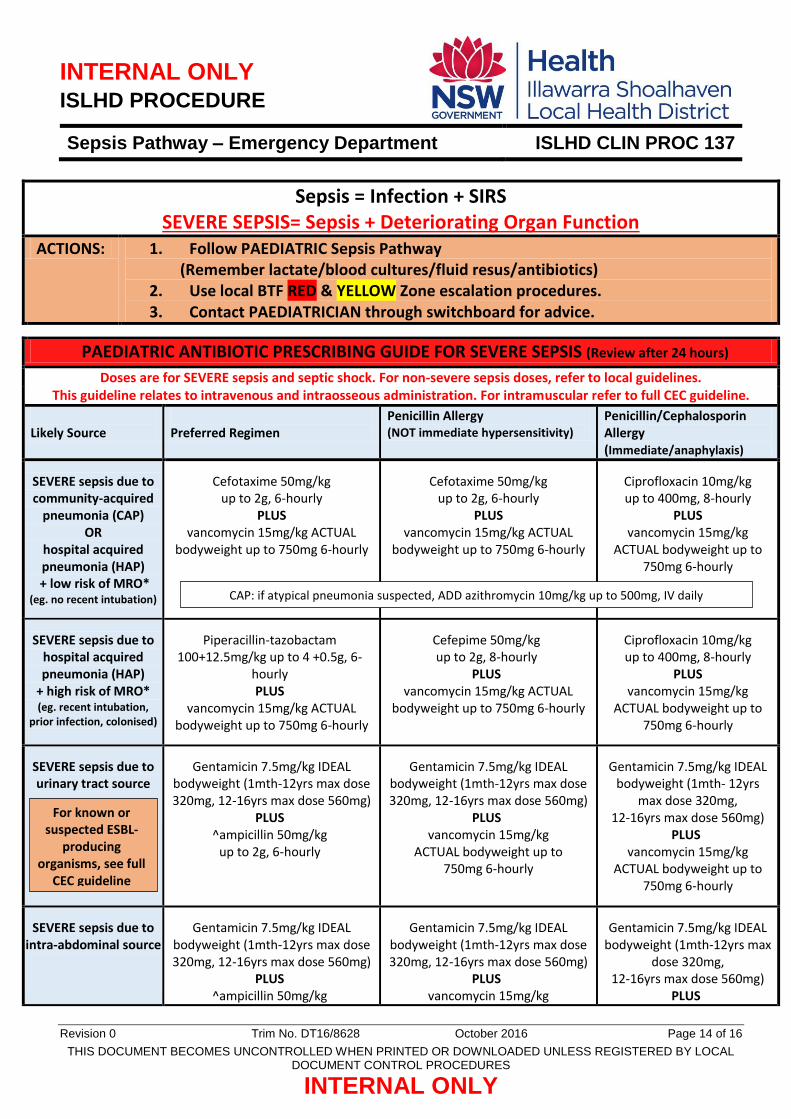
Sepsis = Infection + SIRS SEVERE SEPSIS= Sepsis + Deteriorating Organ Function
ACTIONS: 1. Follow PAEDIATRIC Sepsis Pathway (Remember lactate/blood cultures/fluid resus/antibiotics)
2. Use local BTF RED & YELLOW Zone escalation procedures. 3. Contact PAEDIATRICIAN through switchboard for advice.
PAEDIATRIC ANTIBIOTIC PRESCRIBING GUIDE FOR SEVERE SEPSIS (Review after 24 hours)
Doses are for SEVERE sepsis and septic shock. For non-severe sepsis doses, refer to local guidelines. This guideline relates to intravenous and intraosseous administration. For intramuscular refer to full CEC guideline.
Likely Source
Preferred Regimen
Penicillin Allergy (NOT immediate hypersensitivity)
Penicillin/Cephalosporin Allergy (Immediate/anaphylaxis)
SEVERE sepsis due to community-acquired
pneumonia (CAP) OR
hospital acquired pneumonia (HAP)
+ low risk of MRO* (eg. no recent intubation)
Cefotaxime 50mg/kg up to 2g, 6-hourly
PLUS vancomycin 15mg/kg ACTUAL
bodyweight up to 750mg 6-hourly
Cefotaxime 50mg/kg up to 2g, 6-hourly
PLUS vancomycin 15mg/kg ACTUAL
bodyweight up to 750mg 6-hourly
Ciprofloxacin 10mg/kg up to 400mg, 8-hourly
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
SEVERE sepsis due to hospital acquired pneumonia (HAP)
+ high risk of MRO* (eg. recent intubation,
prior infection, colonised)
Piperacillin-tazobactam 100+12.5mg/kg up to 4 +0.5g, 6-
hourly PLUS
vancomycin 15mg/kg ACTUAL bodyweight up to 750mg 6-hourly
Cefepime 50mg/kg up to 2g, 8-hourly
PLUS vancomycin 15mg/kg ACTUAL
bodyweight up to 750mg 6-hourly
Ciprofloxacin 10mg/kg up to 400mg, 8-hourly
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
SEVERE sepsis due to urinary tract source
Gentamicin 7.5mg/kg IDEAL bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS ^ampicillin 50mg/kg
up to 2g, 6-hourly
Gentamicin 7.5mg/kg IDEAL bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
Gentamicin 7.5mg/kg IDEAL bodyweight (1mth- 12yrs
max dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
SEVERE sepsis due to intra-abdominal source
Gentamicin 7.5mg/kg IDEAL bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS ^ampicillin 50mg/kg
Gentamicin 7.5mg/kg IDEAL bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg
Gentamicin 7.5mg/kg IDEAL bodyweight (1mth-12yrs max
dose 320mg, 12-16yrs max dose 560mg)
PLUS
CAP: if atypical pneumonia suspected, ADD azithromycin 10mg/kg up to 500mg, IV daily
For known or suspected ESBL-
producing organisms, see full
CEC guideline

INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 15 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
up to 2g, 6-hourly PLUS
metronidazole 12.5mg/kg up to 500mg, 12-hourly
ACTUAL bodyweight up to 750mg 6-hourly
PLUS metronidazole 12.5mg/kg
up to 500mg, 12-hourly
vancomycin 15mg/kg ACTUAL bodyweight up to
750mg 6-hourly PLUS
metronidazole 12.5mg/kg up to 500mg, 12-hourly
Likely Source
Preferred Regimen
Penicillin Allergy (NOT immediate hypersensitivity)
Penicillin/Cephalosporin Allergy
(Immediate/anaphylaxis)
SEVERE sepsis due to skin infection
Flucloxacillin 50mg/kg up to 2g, 6-hourly
PLUS vancomycin 15mg/kg ACTUAL
bodyweight up to 750mg 6-hourly
Cefazolin 50mg/kg up to 2 g, 8-hourly
PLUS vancomycin 15mg/kg ACTUAL
bodyweight up to 750mg 6-hourly
Vancomycin 15mg/kg ACTUAL bodyweight up to
750mg 6-hourly
SEVERE sepsis due to intravascular device (eg. venous access device, permanent
pacemaker or defib, endovascular
prostheses such as stents)
Flucloxacillin 50mg/kg up to 2g, 6-hourly
PLUS gentamicin 7.5mg/kg IDEAL
bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
Cefazolin 50mg/kg up to 2 g, 8-hourly
PLUS gentamicin 7.5mg/kg IDEAL
bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
Gentamicin 7.5mg/kg IDEAL bodyweight (1mth-12yrs max
dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
SEVERE sepsis due to
meningitis/ encephalitis
Cefotaxime 50mg/kg up to 2g, 6-hourly
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
If risk of Listeria, ADD ampicillin
50mg/kg up to 2g, 6-hourly
Cefotaxime 50mg/kg up to 2g, 6-hourly
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
If risk of Listeria, seek advice.
Vancomycin 15mg/kg ACTUAL bodyweight up to
750mg 6-hourly PLUS
ciprofloxacin 10mg/kg up to 400mg, 8-hourly
If risk of Listeria, seek advice.
Dexamethasone may be given before antibiotics: 0.15mg/kg up to 10mg, then 6-hourly for 4 days (If serious concern of encephalitis, do not give dexamethasone.)
If signs of encephalitis, ADD: 1mth - 5 yrs aciclovir 20mg/kg, 8-hourly; ≥5 years 15mg/kg, 8-hourly
For water-related infections, see full
CEC guideline)
INTERNAL ONLY ISLHD PROCEDURE
Sepsis Pathway – Emergency Department ISLHD CLIN PROC 137
Revision 0 Trim No. DT16/8628 October 2016 Page 16 of 16
THIS DOCUMENT BECOMES UNCONTROLLED WHEN PRINTED OR DOWNLOADED UNLESS REGISTERED BY LOCAL DOCUMENT CONTROL PROCEDURES
INTERNAL ONLY
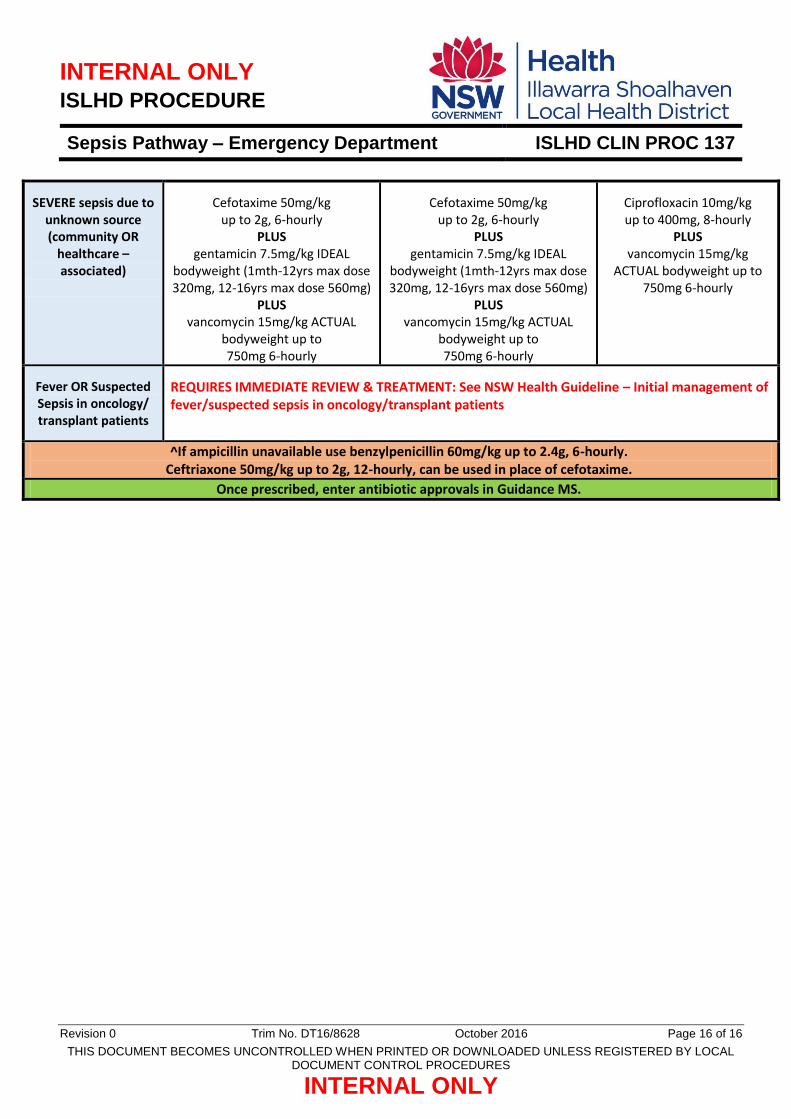
SEVERE sepsis due to unknown source (community OR
healthcare – associated)
Cefotaxime 50mg/kg up to 2g, 6-hourly
PLUS gentamicin 7.5mg/kg IDEAL
bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg ACTUAL
bodyweight up to 750mg 6-hourly
Cefotaxime 50mg/kg up to 2g, 6-hourly
PLUS gentamicin 7.5mg/kg IDEAL
bodyweight (1mth-12yrs max dose 320mg, 12-16yrs max dose 560mg)
PLUS vancomycin 15mg/kg ACTUAL
bodyweight up to 750mg 6-hourly
Ciprofloxacin 10mg/kg up to 400mg, 8-hourly
PLUS vancomycin 15mg/kg
ACTUAL bodyweight up to 750mg 6-hourly
Fever OR Suspected Sepsis in oncology/ transplant patients
REQUIRES IMMEDIATE REVIEW & TREATMENT: See NSW Health Guideline – Initial management of fever/suspected sepsis in oncology/transplant patients
^If ampicillin unavailable use benzylpenicillin 60mg/kg up to 2.4g, 6-hourly. Ceftriaxone 50mg/kg up to 2g, 12-hourly, can be used in place of cefotaxime.
Once prescribed, enter antibiotic approvals in Guidance MS.