isolation precautions for patients with confirmed or ... · pdf fileic/278/10 isolation...
TRANSCRIPT

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 1 of 37
BASINGSTOKE AND NORTH HAMPSHIRE NHS FOUNDATION TRUST
Isolation precautions for patients with confirmed or suspected infectious illness
IC/278/10
Supersedes: IC/278/07
Owner Name Hazel Gray Job Title Senior Infection Control
Nurse Final approval committee
Name Infection Control Committee
Date of meeting 23 July 2010 Authoriser Name Dr Nicki Hutchinson Job title Director Infection Prevention
and Control Signature
Date of authorisation 24.08.10 Review date (maximum 3 years from date of
authorisation) July 2013
Audience (tick all that apply) Trust staff √ NHS √ General public
Standards Standards for Better Health NHSLA The Health and Social Care Act 2008
Executive Summary It is important to minimise the risk of the spread of infection between patients. This policy outlines the measures which should be taken to prevent the spread of infection from patients who are known to be a potential source of infection.
Reviewed in accordance with The Health and Social Care Act 2008: Code of Practice for health and adult social care on the prevention and control of infections and related guidance published 16 December 2009

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 2 of 37
Implementation Plan Summary of changes
• Contact number changes • Isolation sign changes • Roles and responsibility • Education • Evaluation of policy • Standard Precautions update
Action needed and owner of action
• All staff need to be aware of which patients may need isolating and what type of isolation is necessary
• All staff need to be aware of the role they play in trying to reduce the spread of infection
• All staff need to adhere to this policy • The Infection prevention and control team IPCT will evaluate policy when
required • The IPCT will monitor infection rates via alert organism surveillance

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 3 of 37
Contents: Page 1.0 Summary 4 1.1 Roles and Responsibilities 4 1.2 Education and training 5 1.3 Evaluation of this policy 5 2.0 Introduction 5 3.0 Policy Objectives 5 4.0 Categories of isolation 6 4.1 Ring fencing 6 4.2 Source isolation 6 4.3 Protective isolation 6 5.1 Source isolation 7 5.2 Patient placement 7 5.3 Preparation of the isolation room 8 5.4 Hand Decontamination 8 5.5 What if you have cuts and breaks in your skin? 9 5.6 Hand hygiene - patient 9 5.7 Gloves 9 5.8 Aprons and gowns 9 5.9 Masks, face shields or eye protection 10 5.10 Patient care equipment 10 5.11 Environmental cleaning 10 5.12 Linen 10 5.13 Sharps Management 10 5.14 Crockery/cutlery 11 5.15 Bathing 11 5.16 Transport of infected patients 12 5.17 Visitors/patients/carers 12 6.0 References and further reading 12 Appendix 1: Diarrhoea and/or Vomiting Risk Assessment Algorithm 13 Appendix 2: Respiratory Risk Assessment 14 Appendix 3: Skin Infection Risk Assessment Algorithm 14 Appendix 4: Isolation Priorities 16 Appendix 5: Risk Assessment using the Isolation Priority Scoring
System 17
Appendix 6: Priority Scoring System: Infectious Diarrhoea 18 Appendix 7: Priority Scoring System: MRSA 19 Appendix 8: Priority Scoring System: Antimicrobial-Resistant
Bacteria 20
Appendix 9: Priority Scoring System: Respiratory Infections 21 Appendix 10: Priority Scoring System: Other Infectious Diseases /
Conditions 22
Appendix 11: Components of standard and transmission based isolation precautions
23
Appendix 12: Signage 24 Appendix 13: Cleaning Procedure for a Vacated Single Isolation
Room 27
Appendix 14: Cleaning Procedure for a Single Isolation Room 28 Appendix 15: Notifiable infectious diseases & food poisoning 29

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 4 of 37
1.0 Summary Isolation precautions are adopted to minimise the risk of spread of an infectious disease in the hospital setting. This policy is based on national guidelines that review and require assurance that there is a managed environment, which minimises the risk of infection to patients, staff and visitors. This policy is limited to the description of isolation precautions and must be supplemented by the relevant hospital policies and procedures for other aspects of infection and environmental control, occupational health, administrative and legal issues, and any other issues beyond the scope of this guideline. The policy uses a two-tier approach to isolation of patients: standard precautions, which should be used for ALL inpatients and transmission based precautions. Transmission based precautions use the likely pathogen and its’ mode of spread as the main determinant of type of precautions required. Therefore these precautions are classified by these 3 main transmission vehicles contact, droplet and air borne. The policy contains quick reference guidance attached as appendages. They are:
• Standard, airborne, droplet and contact precautions • Applications of standard precautions • Type and duration of precautions needed for selected infections • Empiric isolation precautions for clinical conditions to prevent spread pending
confirmation of diagnosis • Isolation signs • Cleaning procedure for vacated room • Daily cleaning procedure for a single isolation room • Notifiable infectious diseases (see Appendix 15)
Risk assessment should precede isolation of patients especially when single rooms are in short supply and patient isolation has to be prioritised. Some new flowcharts have been added to this document to try and help you with this process (please see Appendices 1-5). The decision to isolate a patient should always be discussed with the infection prevention and control team. The decision to isolate/close a whole ward/s will be undertaken by a Consultant Microbiologist. For further information and/or assistance contact the infection control team on extension 6774 or via bleeps. Hazel Gray } Linda Swanson } Bleep 2364 Out of hours, please contact a Consultant Microbiologist via the switchboard. 1.1 Roles and Responsibility The Executive Director of Nursing on behalf of the Chief Executive will ensure that the Clinical Directors take clinical ownership of the policy. The Clinical Directors on behalf of the executive director of nursing will ensure that:
• all health care workers comply with this policy • all healthcare workers attend mandatory infection control training

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 5 of 37
The Senior Nurses and Matrons on behalf of the Executive Director of Nursing and the Clinical Directors will ensure that:
• all health care workers comply with this policy • all healthcare workers attend mandatory training
The infection prevention and control team will:
• act as a resource for information and support • monitor the implementation of this policy within clinical areas • regularly review and update the policy
The senior nurse and doctor must ensure that all staff are aware and comply with the infection control precautions that need to be taken and follow the advice in this policy. 1.2 Education and training All staff that may come into contact with either potential or confirmed infectious patients i.e. clinical staff; porters, domestics etc must attend their annual infection control mandatory training session. 1.3 Evaluation of this policy It is important to minimise the risk of the spread of infection to and from patients and staff. This policy outlines the measures, which should be taken to prevent the spread of infection from patients who are known to be a potential source of infection. This can be monitored by:
• monitoring the trends of infections in the trust by analyzing alert organism figures
• ensuring when timely isolation of infected patients cannot occur that untoward incident forms are filled in
• monitoring that the correct signage and isolation guidelines are adhered to by all staff by undertaken ad hoc observational audits
• ensuring that non compliance to the policy is challenged
2.0 Introduction Aim of the policy is to ensure that source isolation procedures are instigated in order to minimise the risks of cross infection. The correct and timely placement of infected patients (suspected or proven) into single rooms can be very effective in reducing the overall numbers of infective patients (DH 2007). It is also a requirement of the Health Act 2008 (DH) that an evidence based isolation policy exists incorporating local risk assessment findings and measures. This policy must include indications and procedures for the infection control management of isolated patients.
3.0 Policy Objectives
• To identify patients presenting with colonisation, infection or infectious diseases that may be a risk to others.
• To take timely action to prevent the spread of potentially infectious conditions by appropriate isolation of the source patient and the appropriate use of personal protective equipment.
• To ensure that patients at high risk of infections due to immunosuppression or neutropenia are appropriately isolated and protected to minimise the acquisition of such infections. (Please see Trust Protective Isolation Policy)

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 6 of 37
• To ensure that all staff, departments and any outside agencies likely to be
involved in the care of patients care have a clear understanding of their roles and responsibilities in preventing the spread of infection.
4.0 Categories of isolation Isolation must not compromise the clinical care of the patient There are two categories of isolation (Ayliffe 2001):
• Source isolation: when a patient poses an infection risk to others • Protective isolation: when a patient is at risk from others
4.1 Ring fencing It is sometimes necessary to ring fence a high-risk area e.g. Orthopaedic or Surgical Units as a protective isolation measure. This is due to the significant implications of infections amongst these patients. When an area is ring fenced admissions are scrutinised to allow ONLY specific groups of patients sharing the same medical conditions and risk factors for infection, to be admitted to the ring fenced area. Ring fencing works as part of a complete infection control programme with active surveillance. It also allows for national targets to be met. The decision to ring fence an area should be undertaken between the Hospital Infection Control doctor, directorate leads and trust management teams. 4.2 Source isolation Source isolation is the physical separation of one patient from another, in order to prevent the spread of infection. Single room isolation will not by itself prevent the transmission of organisms; it should be used in conjunction with standard (universal) infection control precautions which must be observed at all times with all patients. Additional precautions may need to be implemented dependant on the source and mode of spread. All hospitals providing in-patient care must ensure that they are able to provide or secure the provision of adequate isolation facilities for patients sufficient to prevent or minimise the spread of Healthcare Associated Infection (DOH 2000) Hospital Trusts have a responsibility to ensure that the policy includes the potential risk of infection and the use of effective protective measures and equipment (DOH 2006) 4.3 Protective Isolation Protective isolation is the physical separation of patients who are Immunocompromised / Immunosuppressed in order to prevent the acquisition of infection from other patients, staff or visitors. (Please see separate Trust Protective Isolation Policy IC/201/10). In both categories:
• The decision to isolate a patient should be based on the infection risk to other patients, staff and visitors
• An appropriate isolation notice is required and must be placed on the outside of the door, outlining the precautions required (see appendix 1)
• In order to minimize the risks of anxiety and depression that are often experienced by many isolated patients, a full explanation of the nature of infection, including the symptoms, treatment and the rationale for the control measures should be given to the patient
• Daily assessment and evaluation of the need for ongoing isolation precautions must take place

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 7 of 37
• The infection prevention and control team is available for advice and guidance.
5.1 Source Isolation Source Isolation is indicated for conditions such as
• Pulmonary tuberculosis • Patients with diarrhoea and or vomiting clinically thought to of infectious origin • MRSA, • Clostridium difficile • Chicken Pox • Infections with Extended spectrum β lactamase producing organisms
(ESBLs) • Glycopeptide resistant enterococci including Vancomycin resistant organisms
(GRE and VRE) • Influenza and fevers from the tropics in which an infectious cause cannot be
ruled out (refer to table and specific policies for further information • Amp C producing organisms • Scabies
NB: Please note that this list is not exhaustive. If you think that a patient may have an infectious condition that will put others at risk, please discuss with the clinical team in the first instance, and consider discussion with the infection prevention and control team or microbiologist if indicated. 5.2 Patient Placement Ideally a single room should be allocated to patients with these conditions, but given the limited availability of side rooms a risk assessment needs to be undertaken. The risk assessment will include the risk factors of the other patients in isolation and the patients in the bays. Some new flowcharts have been added to this document to try and help you with this process (Please see Appendices 1-5). Appropriate patient placement is a significant component of isolation precautions. A single room is important to prevent direct- or indirect-contact transmission when the source patient has poor hygienic habits, contaminates the environment, or cannot be expected to assist in maintaining infection control precautions to limit transmission of micro organisms (i.e., infants, children, and patients with altered mental status). Where possible, a patient with highly transmissible or epidemiologically important microorganisms must be placed in a single room with hand washing and toilet facilities, to reduce opportunities for transmission of microorganisms. When a single room is not available, an infected patient could be placed with an appropriate contact. Patients infected by the same microorganism usually can share a room, provided they are not infected with other potentially transmissible microorganisms and the likelihood of re-infection with the same organism is minimal. Such sharing of rooms, also referred to as cohorting patients, is useful especially during outbreaks or when there is a shortage of side rooms. When a side room is not available and cohorting is not achievable or recommended, it is very important to consider the epidemiology and mode of transmission of the infecting pathogen and the patient population being served in determining patient placement. Under these circumstances, consultation with infection control professionals is advised before patient placement. Moreover, when an infected patient shares a room with a non-infected patient, it is also important that staff looking after the patient and visitors take precautions to prevent the spread of infection.

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 8 of 37
A single room with appropriate air handling and ventilation is particularly important for reducing the risk of transmission of microorganisms from a source patient to susceptible patients and other persons in hospitals when the microorganism is spread by airborne transmission. Some hospitals use an isolation room with an anteroom as an extra measure of precaution to prevent airborne transmission. Unfortunately the only side rooms with anterooms in the Trust are on the Oncology/Haematology unit and are for use by immunocompromised patients only. Under no circumstances should these rooms be used for any other patients An alternative to side room is to barrier nursing the patient on the general bay or cohorting of patients with the same condition. However please note that not all patients with similar symptoms e.g. diarrhoea, have the same aetiology, and cohorting should only be done following discussion with the Infection prevention and control team/or consultant microbiologist. (Out of hours number may be obtained via the switchboard). If there are no side rooms available in the immediate vicinity, consult the site team for availability on another ward if appropriate. Where a patient is nursed in a general bay all appropriate precautions must be implemented and the whole bay isolated. The infected patient should be nursed away from other patients at risk .i.e. immunocompromised patients and an appropriate sign must be displayed on the outside of the bay. Once the risk assessment has identified that the patient requires isolation the following precautions must be considered:- 5.3 Preparation of the isolation room
• All unnecessary equipment and furniture must be removed from the room to facilitate cleaning and limit the potential for contamination.
• All equipment in the room must be dedicated to the isolated patient. • The room must not be overstocked as equipment that cannot be cleaned will
need to be disposed of. • All personal belongings and equipment must be washable, cleanable or
disposable. • The patient should not keep unnecessary belongings in the room. • The source isolation poster must be placed on the door • Single use gloves and aprons must be set up outside the room. If these are
not wall mounted in the Danicenters a trolley/table/shelf must be used. This must be well stocked at all times.
• Patient notes (charts and kardex) must be kept outside the room to reduce the risk of contamination.
• A yellow plastic bag (for clinical waste) and a water soluble alginate bag and red plastic bag (for infected linen) must be available inside the isolation room.
Use Standard Precautions for the care of all patients. (Please refer to Trust Standard Precautions Policy) 5.4 Hand Decontamination
• Hands must be decontaminated before each and every episode of direct patient contact and/or the patient’s direct environment and after any activity that could potentially result in hands becoming contaminated.
• Hands that are visibly soiled with contaminated dirt or organic material, i.e. blood/body fluids must be washed immediately with liquid soap and water
IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 9 of 37
• Hands can be decontaminated, with an alcohol based hand rub unless hands are visibly contaminated, between caring for different patients and between different care activities for the same patient. (Please refer to Trust Hand Hygiene Policy)
5.5 What if you have cuts and breaks in your skin?
• Cover any existing cuts or lesions with a waterproof dressing, paying particular attention to hands and forearms.
• Any staff with chronic skin lesions to hands or forearms or persistent skin problems should avoid undertaking invasive procedures and seek advice from the dermatology and Occupational Health Department.
5.6 Hand hygiene – patient The patient is a potential source of spread of organisms to staff, visitors and the environment. He/she should be instructed to decontaminate hands before eating and after going to the toilet. Liquid soap and water should be used in these circumstances 5.7 Gloves
• Selection of protective equipment should be based on an assessment of the risk of transmission of microorganisms to the patient and the risk of contamination of the healthcare worker’s clothing and skin by patients’ blood, body fluids, secretions or excretions.
• Gloves must be worn for invasive procedures, contact with sterile sites and non-intact skin or mucous membranes and all activities that have been assessed as carrying a risk of exposure to blood, body fluids, secretions or excretions.
• Gloves must be worn as single use items. They must be put on immediately before an episode of patient contact or treatment and removed as soon as the activity is completed. Gloves must be changed between caring for different patients and between different care and treatment for the same patient.
• Gloves must be disposed of as clinical waste after every procedure/episode of care and hands decontaminated thoroughly after the gloves have been removed.
• Neither powdered nor polythene gloves should be used in healthcare activities. Any sensitivity to natural rubber latex in patients, carers and healthcare staff must be documented and alternative gloves must be available. (Please refer to Trust Glove Policy)
• Wearing gloves does not replace the need for hand washing, because gloves may have small, unapparent defects or may be torn during use, and hands can become contaminated during removal of gloves. Failure to change gloves between patient contacts is an infection control hazard. (Please refer to Trust Standard Precautions Policy and Glove Policy
5.8 Aprons and gowns
• Disposable plastic aprons should be worn where there is a risk that clothing may be exposed to blood, body fluids, secretions and excretions with the exception of sweat.
• Full body fluid repellent gowns must be worn where there is a risk of extensive splashing of blood, body fluids, secretions or excretions onto the skin or clothing of healthcare workers

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 10 of 37
• Plastic aprons and fluid repellent gowns should be worn as single use items for one procedure or episode of patient care and then discarded and disposed of as clinical waste.
• Remove a soiled gown or apron as promptly as possible and wash hands to avoid transfer of microorganisms to other patients or environments.
5.9 Masks, face shields or eye protection Wear a mask and eye protection or a face shield to protect mucous membranes of the eyes, nose, and mouth during procedures and patient-care activities that are likely to generate splashes or sprays of blood, body fluids, secretions, and excretions. 5.10 Patient care equipment Handle used patient-care equipment soiled with blood, body fluids, secretions, and excretions in a manner that prevents skin and mucous membrane exposures, contamination of clothing, and transfer of micro organisms to other patients and environments. Ensure that reusable equipment is not used for the care of another patient until it has been cleaned and reprocessed appropriately. Ensure that single-use items are not reused and are discarded of properly. 5. 11 Environmental cleaning
• There should be clear hospital procedures for the routine care, cleaning, and disinfection of environmental surfaces, beds, bedrails, bedside equipment, and other frequently touched surfaces with an audit programme to ensure that these procedures are being followed. All isolated areas should be cleaned 3 times a day with an Actichlor + solution as per Trust Cleaning Standards. (Please refer to the Hospital Cleaning Standards)
• Isolation rooms should be cleaned last; after other rooms, bays and general areas on the ward
• Single use gloves and aprons must be worn when cleaning isolation rooms and hands washed before leaving the room.
• Special attention must be given to all horizontal surfaces and frequently touched surfaces, such as door handles/door push plates, nurse call system, toilet areas and sink taps.
5.12 Linen
• Handle, transport, and process used linen soiled with blood, body fluids, secretions, and excretions in a manner that prevents skin and mucous membrane exposures and contamination of clothing and that avoids transfer of micro organisms to other patients and environments.
• Ensure that any linen contaminated with blood or body fluids is placed into a red alginate bag and then red plastic bag.
• If linen is excessively wet please ensure that this item is wrapped in another item of linen or the alginate bag may leak/split.
5.13 Sharps Management
• Sharps must not be passed directly from hand to hand and handling should be kept to a minimum
• Needles must not be resheathed, bent, broken or disassembled prior to disposal
• Always dispose of sharps at the point of use in an appropriate container. • Syringes/cartridges and needles should be disposed of intact.

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 11 of 37
• Sharps containers must comply with BS 7320 and UN3291 standards • Do not fill sharps containers above the manufacturer’s marked line, which
indicates that they are full. • Lock the used sharps container in accordance with manufacturer’s • Do not dispose of sharps with other clinical waste. • Do not place used sharps containers in yellow bags for disposal. • Ensure that sharps bins are safely positioned away from children/general
public • Ensure the temporary closure lid is in place when not in use • Do not remove sharps from the clinical setting.
NB: In the event of a sharps injury or contamination of broken skin/ mucous membranes with blood or body fluids, ensure that the Needlestick injury procedure is followed. (Please refer to Trust Sharps Contamination Policy and Safe Handling of Sharps Policy) 5.14 Crockery/cutlery
• All crockery/cutlery must be decontaminated in a dishwasher with a final
rinse temperature of 80°C. • Washing by hand is inadequate. • There is no requirement for disposable crockery and cutlery to be used.
5.15 Bathing
• To reduce the risk of cross-infection, patients with infections must be
bathed last. • The bath should be cleaned with Actichlor + (1,000 ppm) after use by the
isolated patient (this method of disinfection is adequate for use after bathing infected patients).
• If showers are used the procedure is as for baths. 5.16 Transport of Infected Patients Limiting the movement and transport of patients infected with virulent or epidemiologically important microorganisms and ensuring that such patients leave their rooms only for essential purposes reduces opportunities for transmission of microorganisms in hospitals. When patient transport is necessary, it is important that:
• Movement of infectious or potentially infectious patients should be kept to a minimum. When it is necessary to transport patients to other wards or departments, precautions to minimize the risks of transmission must continue.
• If it is possible to delay an investigation without adversely affecting the patients management this should be considered. However the presence of an infectious disease should not delay urgent clinical investigations.
• The receiving area must be informed prior to transfer to ensure that they have the appropriate precautions in place and that appropriate facilities are available.
• Patients with known or suspected infections must as far as possible be seen at the end of the list and not be left in the waiting areas. This will allow adequate cleaning of the environment and equipment following the appointment and reduce the risks to other patients.
• Check specific infection control policies for advice and guidance. • Consult the infection prevention and control team for any further advice or
guidance

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 12 of 37
5.17 Visitors/Patients/Carers
• Explain the precautions required whilst maintaining the patient’s confidentiality.
• Visitors should be advised to wash their hands with liquid soap and water in the following circumstances:
o Hands are visibly soiled; o Following close physical contact with the patient or his/her immediate
environment. o In addition, visitors should be advised to clean their hands with liquid
soap and water after removing gloves and apron (if worn, see below) and immediately before entering and leaving the isolation room(alcohol rub may be used as an alternative for hand decontamination in this instance unless the reason for source isolation is C. difficile
• Discourage visitors from having contact with other patients in the ward or hospital
• Check with specific policies regarding specific diseases to ascertain whether visitors should be excluded due to particular susceptibility.
• Visitors do not need to wear aprons and gloves unless helping with personal care or otherwise advised by Infection Control.
6.0 Post isolation/discharge/death New patients must not be admitted to the room until it has undergone a deep clean.
• A patient should be removed from isolation when he/she is no longer at risk of spreading infection to others (refer to the new LTHT alert organism/condition policy). This may be decided following consultation with a member of the infection prevention and control team or on the basis of an infection prevention and control policy (e.g. after 72 hours symptom free following gastroenteritis or C. difficile infection)
• At a minimum, daily assessment and evaluation of the patient's symptoms are therefore important
• Some specific disease policies give criteria on when isolation precautions can be stopped
• If in doubt, discuss with the infection prevention and control team • The vacated room must be cleaned thoroughly using Actichlor + solution (1
tablet to a litre of water) all equipment and belongings must be cleaned before being brought out of the room or used again. Any unused disposable items, which may be contaminated and cannot be cleaned must be disposed of (Please see Trust cleaning Standards).
7.0 References and further reading • Ayliffe GAJ, Lowbury EJL, Geddes AM and Williams JD. Control of Hospital
Infection a Practical Handbook, 3rd Edition. London: Blackwell Scientific Publications, 1988: 70.
• Horton R. Hand washing: the Fundamental Infection Control Principle. British Journal of Nursing, 1995; 4 (16): 226-233.
• Maurer IM. Hospital Hygiene, 3rd Edition. London: Edward Arnold, 1985: 50. • Lewis AM, Gammon J, Hosein I. The Pros and Cons of isolation and
Containment. Journal of Hospital Infection, 1999; 43: 19-23. • Wilson J. Theory and Practice of Isolation Nursing. Nursing Standard, 1992; 6
7): 30- 31
IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 13 of 37
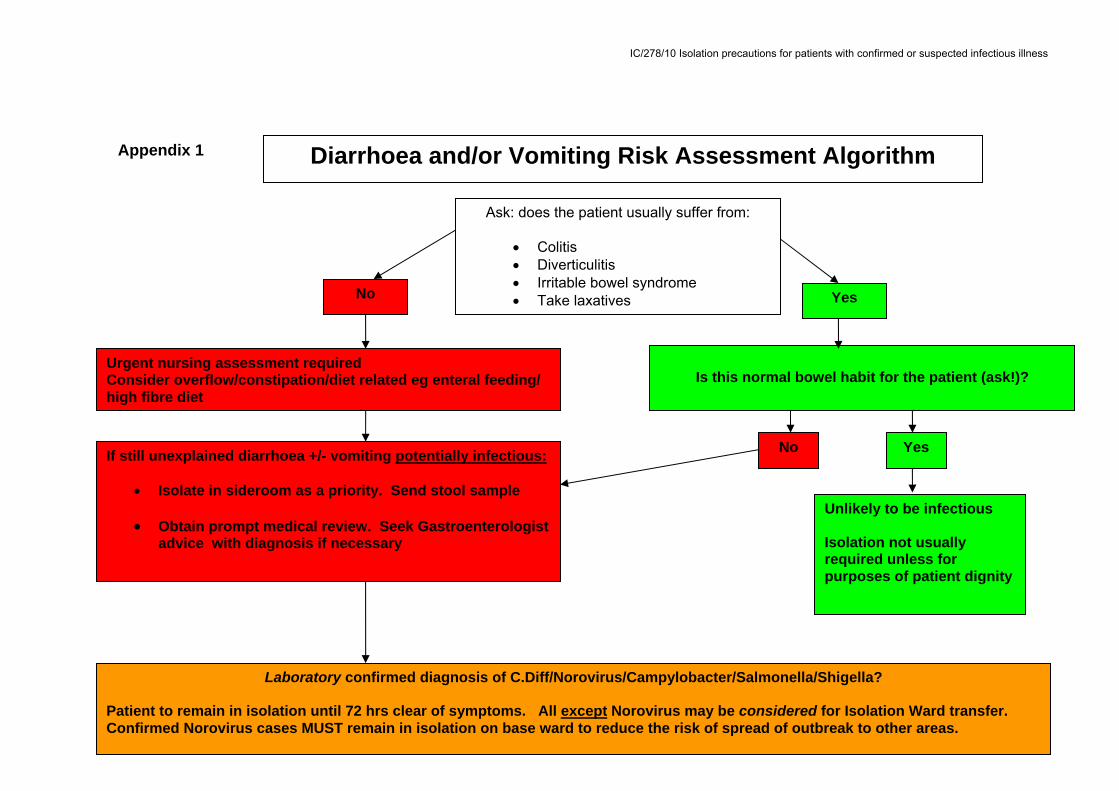
No
Urgent nursing assessment required Consider overflow/constipation/diet related eg enteral feeding/ high fibre diet
If still unexplained diarrhoea +/- vomiting potentially infectious:
• Isolate in sideroom as a priority. Send stool sample • Obtain prompt medical review. Seek Gastroenterologist
advice with diagnosis if necessary
Ask: does the patient usually suffer from:
• Colitis • Diverticulitis • Irritable bowel syndrome • Take laxatives Yes
Is this normal bowel habit for the patient (ask!)?
No Yes
Unlikely to be infectious Isolation not usually required unless for purposes of patient dignity
Laboratory confirmed diagnosis of C.Diff/Norovirus/Campylobacter/Salmonella/Shigella? Patient to remain in isolation until 72 hrs clear of symptoms. All except Norovirus may be considered for Isolation Ward transfer. Confirmed Norovirus cases MUST remain in isolation on base ward to reduce the risk of spread of outbreak to other areas.
Appendix 1 Diarrhoea and/or Vomiting Risk Assessment Algorithm

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 14 of 37
Respiratory Risk Assessment
Suspected /confirmed
H1N1/Flu A?
Suspected/confirmed Bacterial Meningitis (viral meningitis does
not require isolation)
Suspected/confirmed TB lungs/larynx? (TB in “closed sites” eg not in
lung/larynx/discharging wound does not usually require isolation).
• Respiratory isolation required*
• If multi resistant TB
suspected seek immediate duty microbiologist advice
• Respiratory isolation not required
• Use of appropriate PPE required when performing aerosol generating procedures
Yes No Yes No
• Respiratory isolation required*
• Prompt transfer to Isolation Ward E floor required
• Prompt medical review required
Respiratory isolation not
required
Respiratory isolation* required for the first 24hrs of IV Antibiotic treatment
*Respiratory isolation requires the use of aprons/gloves/ FFP2 or FFP3 mask. Please contact a member of the Infection Prevention and Control team or the Consultant Microbiologist for any specialist advice
regarding respiratory isolation. Out of hours please contact the duty Consultant Microbiologist via the hospital switchboard.
No Yes
Appendix 2

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 15 of 37
Shingles Evidence of lesions/weeping
vesicles of unknown origin
Please note in the case of shingles and chicken pox special precautions are required with certain groups of healthcare workers e.g pregnant healthcare workers. These workers and those who do not have immunity (have not previously had chicken pox) should not enter
the isolation room of these patients where at all possible. For any further advice regarding this please contact either a member of the Infection Prevention and Control Team or the Consultant
Microbiologist.
Chicken Pox
Lice Scabies
Suspected/confirmed:
Isolate into side room
until dry/healed
skin
Isolate into side room until vesicles
dry/healed
Isolate in side room until 1st treatment completed. May then be de-isolated. Patients with Norwegian
scabies need to remain in isolation
Isolate in side room until treated.
May then be de-isolated.
Isolate into side room and obtain prompt medical
review/dermatologist opinion.
Skin Infection Risk Assessment Algorithm
TB suspected in oozing/
discharging wounds?
Isolate into side room until wound
dry and completely
healed
Appendix 3

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 16 of 37
• ESBL/AMP C/Acinetobacter • GRE • RSV/Influenza • Mumps • Meningitis with cough (isolation for 24
hrs IVABX) • Strep A/Strep G on high risk areas
(isolation for first 24 hrs of IVABX) • Open weeping TB lesions to skin
• MRSA 15 or 16 post full screen and on
Mupiricin • Meningitis (undiagnosed or
meningococcal) no cough • Strep A/G (after 24 hrs IVABX) • Scabies (isolate until first treatment
completed)
HIGH Do not remove from isolation without prior
discussion with duty microbiologist/ICT
MEDIUM
LOW
• Diarrhoea and/or vomiting of unknown
origin • Suspected/confirmed Norovirus • Suspected/confirmed C.diff • Suspected/confirmed Pulmonary TB
including MDRTB. Possible MDRTB must be discussed immediately with the duty microbiologist
• Suspected/confirmed Chicken pox/Shingles/Measles
• MRSA in sputum/exudating wound/MRSA skin shedder/high mupricin resistance/MRSA 16 or 18
• E.coli 0157/Shigella/Salmonella • Norwegian scabies • Pandemic influenza • Viral haemorrhagic fever – possible
cases must be discussed with the duty microbiologist immediately
Isolation Priorities Appendix 4
NB: MRSA 16 and 18 strains can be more resistant to antibiotics and also resistant to Mupiricin 5 and 200, due to the resistance of the strain these patients cannot be placed in an open bay or with any other MRSA positive patient

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 17 of 37
Appendix 5: Risk Assessment using the Isolation Priority Scoring System The isolation priority scoring system is based on factors likely to influence the transmission of a pathogen and its impact e.g. pathogenic potential, mechanism of transmission, antibiotic resistance, susceptibility of other patients, prevalence in the hospital (see Table 2, pg11). All patients considered for admission to the Isolation Ward must be risk assessed and assigned a score using the Isolation Priority Scoring System for the relevant infectious disease/condition (see Tables 3-7, pg12 – pg16). This assessment will be guided by the nurse in charge of the Isolation Ward with the support of the Infection Control Team. The level of priority: high, medium or low, can be determined depending on the score as indicated in Table 1 Table 1: Appropriate Isolation Facility according to Level of Priority Score Priority Appropriate Isolation Facility >45 High Single room on Isolation Ward with ensuite bathroom
facilities OR If indicated, negative pressure room at a regional specialist unit (Southampton or London)
25-45 Medium Single room on Isolation Ward with ensuite bathroom facilities
<25 Low Single room on Isolation Ward, single room on general ward or Cohort bay if established
Disease-Specific Isolation Risk Assessment Priority Scoring Tables The relevant table should be used for determining the score of individual patients who are suspected or known to be colonised or infected with an infectious disease or condition. If the condition is not listed, the Infection Control Team or on-call Medical Microbiologist (out of hours) should be contacted. The risk assessment score should be reviewed and documented daily to ensure that optimal use is made of isolation facilities and to ensure that patients are not kept in isolation for longer than necessary

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 18 of 37
Appendix 6: Priority Scoring System: Infectious Diarrhoea
Table 3: Priority Scoring Table for Infectious Diarrhoea Infection Route
of spread
Evidence for spread in hospital
Antimicrobial resistance
Variable factors, e.g. patient susceptibility, dispersal risk
Risk category
Score Length of isolation
Clostridium difficile
Contact (faecal-oral)
Strong Little Profuse diarrhoea with faecal incontinence, patient confused/ Uncooperative
High >45 Until diarrhoea resolved for 72hrs
Continent and cooperative
Medium
35
Norovirus Aerosol and Contact (faecal-oral)
Strong Little To remain in isolation in base ward /area due to risk of spreading outbreak to other wards/areas
High >45 Until diarrhoea / vomiting resolved for 72hrs
E. coli 0157, Salmonella Shigella
Contact (faecal-oral)
Moderate Little Profuse diarrhoea with faecal incontinence, patient confused/ Uncooperative
High >45 Until diarrhoea resolved for 72hrs
Continent and cooperative
Medium
35

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 19 of 37
Appendix 7: Priority Scoring System: MRSA
Table 4: Priority Scoring Table for MRSA Condition or infection
Route of spread
Evidence for spread in hospital
Antimicrobial resistance
Variable factors, e.g. patient susceptibility, dispersal risk
Risk category
Score Length of isolation
MRSA15 or 16
Contact Strong Moderate Skin shedder (e.g. eczema, psoriasis), discharging wound or sputum colonised
High >45 Indefinite
>1 site colonised or uncovered wound
Medium 35
Nasal carriage only - post full screen and on mupirocin
Low 0 Continue screening, aim to clear
MRSA 17 or MRSA with high level mupirocin resistance
Contact Strong Serious Skin shedder (e.g. eczema, psoriasis), discharging wound or sputum colonised
High 50 Indefinite
Not a skin shedder High
>45

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 20 of 37
Appendix 8: Priority Scoring System: Antimicrobial-Resistant Bacteria
Table 5: Priority Scoring Table for Antimicrobial-Resistant Bacteria Condition or infection
Route of spread
Evidence for spread in hospital
Antimicrobial resistance
Variable factors, e.g. patient susceptibility, dispersal risk
Risk category
Score Length of isolation
ESBL, Acinetobacter
Contact and droplet
Moderate Serious Sputum colonised
Medium 45 Indefinite
Oncology ward, ICU
Medium 45
Glycopeptide resistant enterococci (GRE)
Contact Strong Serious Oncology ward or immuno-compromised patients
Medium >45 Indefinite
Other wards, diarrhoea
Medium 30
Other wards, faecal colonisation – no diarrhoea
Low 20

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 21 of 37
Appendix 9: Priority Scoring System: Respiratory Infections
Table 6: Priority Scoring Table for Respiratory Infections Condition or infection
Route of spread
Evidence for spread in hospital
Antimicrobial resistance
Variable factors, e.g. patient susceptibility, dispersal risk
Risk category
Score Length of isolation
Penicillin resistant Streptococcus pnemoniae
Droplet Strong Moderate Cough High 50 Until cough resolves
No cough Medium 40
Respiratory syncytial virus (RSV) / influenza
Droplet and contact
Strong N/A Non-epidemic situation
Medium 40 Until symptoms resolve
Epidemic situation
Medium 35
Pulmonary / Laryngeal Tuberculosis – ‘open’ (untreated)
Airborne Strong N/A (see below – MDRTB)
Refer to TB Policy
High 55 Refer to TB Policy
Tuberculosis lesions (weeping)
Contact Poor N/A (see below - MDRTB)
Refer to TB Policy Medium -
Low
25 Refer to TB Policy
Pulmonary Tuberculosis – multi-drug resistant
Airborne Strong Serious Refer to TB Policy
High 65 Transfer to regional specialist unit

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 22 of 37
Appendix 10: Priority Scoring System: Other Infectious Diseases / Conditions
Table 7: Priority Scoring Table for other Infectious Diseases / Conditions Condition or infection
Route of spread
Evidence for spread in hospital
Antimicrobial resistance
Variable factors, e.g. patient susceptibility, dispersal risk
Risk category
Score Length of isolation
Chicken pox (varicella) / shingles
Airborne and contact
Strong Little Antenatal, postnatal, oncology, immuno-compromised patients
High 50 Until spots/ lesions crusted
All other wards Medium 40
Measles Airborne Strong Little Antenatal, postnatal, oncology, immuno-compromised patients
High 50 14 days
All other wards Medium 40
Mumps Droplet Moderate Little Antenatal, postnatal, oncology, immuno-compromised patients
Medium 35 9 days
All other wards Medium 25
Meningitis (undiagnosed or meningococcal)
Droplet Poor Little Cough Medium 25 24 hrs with effective antibiotic therapy
No cough Low 15
Scabies Contact Strong N/A Avoid prolonged skin to skin contact
Low 20 24 hrs after treatment
Scabies – disseminated (Norwegian)
Contact Strong N/A Avoid direct contact with skin and environmental surfaces (use PPE)
High >45 Indefinite
Streptococcus Groups A and G
Droplet Strong Little Surgical wards Medium 30 24 hrs with effective antibiotic therapy
Other wards Low 20

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 23 of 37
Appendix 11: Components of standard and transmission based isolation precautions Standard Contact Droplet Airborne Hand washing
√ √ √ √
Gloves When likely to touch, blood, body fluids and contaminated items
On entering room, during care
As per standard
As per standard
Masks During procedures likely to generate contamination with blood and body fluids
As per standard
As per standard and if within 1 metre of patient
On entering if non-immune. Non-essential, susceptible people should be excluded
Eye/face protection
During procedures likely to generate contamination with blood and body fluids
As per standard
As per standard and if within 1 metre of patient
On entering if non-immune. Non essential, susceptible people should be excluded
Apron/gown During procedures likely to generate contamination with blood and body fluids
On entering if contact with patient or environment anticipated
As per standard
As per standard
Equipment √ √ √ √ Cleaning √ √ √ √ Linen √ √ √ √ Isolation room
Single room not required
Single room and minimise time outside
Single room and minimise time outside when patient may wear mask
Single room +/- negative pressure ventilation, minimise time outside and patient should wear mask, exclude non essential susceptible staff


IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 25 of 37
ALL VISITORS PLEASE: • Ask a nurse before entering so she/he can explain any precautions you need to take, such as wearing gloves, aprons or masks. • Use the alcohol gel provided before entering the room and wash your hands with soap and water before leaving the room. • Close the door behind you.
ALL STAFF PLEASE: • Wash your hands and wear appropriate protective equipment prior to contact with the patient and/or patient environment. • Wash your hands prior to leaving the room. • Close the door behind you.
Appendix 12: Signage

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 26 of 37
ALL VISITORS PLEASE: • Ask a nurse before entering so she/he can explain any precautions you need to take, such as wearing gloves, aprons or
masks. • Use the alcohol gel provided before entering the room and wash your hands with soap and water before leaving the
room. • Please do not visit if you have a cough/cold or sore throat or have been unwell within the last 7 days • Close the door behind you.
ALL STAFF PLEASE: • All Staff members entering the room MUST wear aprons and gloves • Please do not visit if you have a cough/cold or sore throat or have been unwell within the last 7 days • Please adhere to standard infection control precautions at all times • Please ensure door is closed at all times

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 27 of 37
Appendix 13: Cleaning Procedure for a Vacated Single Isolation Room Required:
• Caution sign • Yellow apron and disposable gloves • Mop and bucket • Cleaning clothes • Detergents/hypochlorite solution • Yellow bag for clinical waste • Mask & Goggles (optional depending on operators risk assessment)
Clean fixtures & Fittings:
• Remove toilet rolls if soiled with body fluids • Remove clinical and domestic waste • Clean sanitary ware and overhead bed lamps with Actichlor + solution • Note: Hand towels do not need to be thrown away if they are in the dispenser
or still wrapped Equipment use:
• Use Actichlor + hypochlorite solution to clean and disinfect items. • Remove from 'Dirty Area' to corridor clean area e.g. corridor etc • Remove/take down all curtains including door curtains and place in red
alginate bag and then Purple plastic bag • Spot clean visibly soiled area on walls • Liaise with Infection prevention and control/Estate Services if full height wall
washing is considered necessary • Clean edges, ledges, pipes and radiators thoroughly • Ensure the floor is cleaned thoroughly including corners • Cleaning is complete when the room, furniture and fittings are free from dust,
debris, spillage and moisture • Dispose of gloves and apron correctly and wash hands thoroughly • Return clean furniture to clean room. • Replace/re hang curtains correctly if hooks are loose or missing • Replenish toilet rolls and paper towels. • Replace clinical and domestic waste bin liners • Inform nursing staff that the room is now ready for use

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 28 of 37
Appendix 14: Cleaning Procedure for a Single Isolation Room
All cleaning equipment used in these rooms will be kept exclusively for use within
these rooms.
1. Floors should be cleared of debris by the use of a disposable dust control mop. The disposable strip will be removed from the head and placed in a yellow refuse bag before leaving the room.
2. A single bucket and mop handle will be kept within the room for damp
mopping of the floor.
3. Disposable yellow cloths will be used for damp dusting and washing of furniture /equipment. They will be placed in a yellow refuse bag inside the room.
4. Protective clothing will be worn as instructed.
5. Blood and blood stained body fluid spillages must be cleaned using a
hypochlorite solution as per Trust Cleaning Standards.
6. All horizontal surfaces must be wiped over with an Actichlor + solution.
7. It is not necessary to wash walls unless they are visibly soiled.
8. Dust must be kept to a minimum.
9. Clinical waste (e.g. protective clothing contaminated with body fluids) must be bagged in yellow bags.
10. Domestic waste (e.g. hand towels) must be bagged in yellow bags.
11. All waste bags for disposal must be secured with tape.
12. When room is vacated follow cleaning procedure for a vacated single isolation
room.

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 29 of 37
Appendix 15: Notifiable infectious diseases & food poisoning The statutory notification of infectious diseases has been a crucial health protection measure in this country since the late 19th century. The purpose of notification is to enable the prompt investigation, risk assessment and response to cases of infectious disease and contamination that present a significant risk to human health. Notification has the secondary benefit of providing data for use in the epidemiological surveillance of infection and contamination. Notification duties of Registered Medical Practitioners (RMPs) RMPs attending a patient are required to notify the proper officer of the local authority in which the patient resides when they have “reasonable grounds for suspecting” that the patient:
• has a notifiable disease as listed in this appendix of the Notification Regulations; or
• has an infection not included in Schedule 1 which in the view of the RMP presents, or could present, significant harm to human health (e.g. emerging or new infections); or
• is contaminated (such as with chemicals or radiation) in a manner which, in the view of the doctor presents, or could present, significant harm to human health; or
• has died with, but not necessarily because of, a notifiable disease, or other infectious disease or contamination that presents or could present, or that presented or could have presented significant harm to human health.
RMPs should not wait for laboratory confirmation or results of other investigations in order to notify a case. This will ensure prompt notification so that health protection interventions and control measures can be initiated as soon as possible. If laboratory test results refute the clinical diagnosis later, the RMP is not required to de-notify the case. However, they should contact the proper officer if they made administrative errors in the notification process. When a statutory notification is made, it is useful to mention the notification in the patient’s records. This will help to avoid duplicate notifications. When a patient is referred from one RMP to another, the first RMP who forms a clinical suspicion that a patient suffers from a notifiable disease or other infectious disease or contamination that presents, or could present, harm to human health should notify the case. This is to prevent unnecessary delay in advising or implementing public health measures Time frame for notifications The RMP should send a written notification to the proper officer of the local authority so that it is received within three days, beginning with the day on which the RMP forms the clinical suspicion or makes the clinical diagnosis. However, if the RMP considers the case requires urgent notification, they need to notify it orally – usually by telephone – as soon as reasonably practicable and follow this up with written notification within three days. It is recommended that urgent notifications are made as soon as possible after the RMP forms the clinical suspicion or makes the clinical diagnosis, and always within 24 hours. In determining whether a case is urgent or not, factors that should be considered include the:

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 30 of 37
• Nature of the suspected notifiable disease, other relevant infection or relevant
contamination including morbidity, case-fatality and epidemiology of the disease – a rare disease, or one that is re-emerging, is likely to need urgent notification.
• Ease of spread of that disease or infection, route of transmission (for example, a highly infectious respiratory disease) or potential spread of contamination.
• Ways in which the spread of the notifiable disease, other relevant infection or contamination can be prevented or controlled, for example by immunisation, disinfection, isolation or prophylactic treatment.
• Specific circumstances of the case which might represent particular risks, such as occupation, age and sex. These details have a bearing if, for example, a patient is a healthcare worker, a child attending nursery or a woman of child-bearing age.
There may be other circumstances where urgent notification is necessary, for example, if a disease appears to be a cluster of cases rather than a single case. Providing relevant information The notification by RMPs must include the following information about the patient in so far as it is known to them:
• name, date of birth and sex; • home address including postcode; • contact telephone number; • current residence (if it is not the home address); • NHS number; • occupation (if the RMP considers it relevant); • name, address and postcode of place of work or educational establishment (if
the RMP considers it relevant); • ethnicity; • relevant overseas travel history; • contact details of a parent (if the patient is a child); • disease or infection which the patient has or is suspected of having or the
nature of the patient’s contamination or suspected contamination; • date of onset of symptoms; and • date of diagnosis.
The notification should also include the name, address and telephone number of the RMP making the notification.

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 31 of 37
Alogorithm 1: The notification process
Patient
Seen by Registered Medical Practitioner (RMP)
YES
Clinically suspected or diagnosed notifiable disease
URGENT RMP considers case urgent and notifies the proper officer by telephone. It is recommended that urgent notifications are made as soon as possible after clinical suspicion or diagnosis and always within 24 hours. Oral notification needs to be followed by a written notification within three days
NON URGENT
RMP notifies the proper officer in writing
within three days
YES Proper officer considers the case to be urgent
NO
Other infection or contamination that presents, or
could be present, significant harm to human health is suspected or diagnosed
NO
No requirement to notify
NO
NON URGENT Proper officer passes on notifications specified below in writing within three
days
Proper officer receives notification
URGENT Proper officer passes on notification specified below
orally – normally be telephone – as soon as reasonably practicable. Oral notification needs to be
followed by written notification within three days
The proper officer of the local authority (LA) sends a copy of the notification to the HPA, the proper officer of the LA in whose area the patient usually resides (if different) or
proper officer of the port health authority or the LA of the patient’s port of disembarkation (if relevant)

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 32 of 37

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 33 of 37
Table 1: Notifiable diseases, with explanatory notes and guidance on the need for urgent notification NB: This table is only for guidance and each case should be considered individually. Notifiable diseases Definition/comment Likely to be urgent? Acute encephalitis No Acute meningitis Viral and bacterial Yes, if suspected bacterial
infection Acute poliomyelitis Yes Acute infectious hepatitis Close contacts of acute
hepatitis A and hepatitis B cases need rapid prophylaxis. Urgent notification will facilitate prompt laboratory testing. Hepatitis C cases known to be acute need to be followed up rapidly as this may signify recent transmission from a source that could be controlled.
Yes
Anthrax Yes Botulism Yes Brucellosis No – unless thought to be UK
acquired Cholera Yes Diptheria Yes Enteric fever (typhoid or paratyphoid fever)
Clinical diagnosis of a case before microbiological confirmation (e.g. case with fever, constipation, rose spots and travel history) would be an appropriate trigger for initial public health measures, such as exclusion of cases and contacts in high risk groups (e.g. food handlers).
Yes
Food poisoning Any disease of infectious or toxic nature caused by, or thought to be caused by consumption of food or water (definition of the Advisory Committee on the Microbiological Safety of Food)
Clusters and outbreaks, yes. For specific organisms see Table 2
Haemolytic uraemic syndrome (HUS)
Yes
Infectious bloody diarrhoea See also HUS in Schedule 1 and VTEC in Schedule 2
Yes
Invasive group A streptococcal disease and scarlet fever
Yes, if IGAS. No, if scarlet fever
Legionnaires’ disease Yes Leprosy No Malaria No, unless thought to be UK
acquired Measles Yes Meningococcal septicaemia Yes

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 34 of 37
Notifiable diseases Definition/comment Likely to be urgent? Mumps Post-exposure immunisation
(MMR or HNIG) does not provide protection for contacts
No
Plague Yes Rabies A person bitten by a
suspected rabid animal should be reported and managed urgently but if a patient is diagnosed with symptoms of rabies they will not pose a risk to human health
Yes
Rubella Post-exposure immunisation (MMR or HNIG) does not provide protection for contacts
No
SARS Yes Smallpox Yes Tetanus No, unless associated with
injecting drug use Tuberculosis No, unless healthcare worker
or suspected cluster or multi drug resistance
Typhus No Viral haemorrhagic fever (VHF)
Yes
Whooping cough Yes, if diagnosed during acute phase
Yellow fever No, unless thought to be UK acquired
NB: RMPs are also required to notify suspected cases of other infections (“other relevant infection”) or contamination (“relevant contamination”) that present, or could present, significant harm to human health (see 3.2 and 3.3).

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 35 of 37
Table 2: Causative agents, with explanatory notes and guidance on the need for urgent notification As regards urgency, the key consideration will be the likelihood that an intervention is needed to protect human health and the urgency of such an intervention. The likelihood of the diagnosis of an infection being considered urgent may also increase if it is part of a known or suspected cluster, or in someone with increased risk of transmission such as enteric infection in a food handler. NB: This table is only for guidance and each case should be considered individually. Notifiable organisms Definition/comment Likely to be urgent? Bacillus anthracis Yes Bacillus cereus Only if associated with food
poisoning No, unless part of a known cluster
Bordetella pertussis Yes, if diagnosed during acute phase
Borrelia spp No Brucella spp No, unless thought to be UK
acquired Burkholderia mallei Yes Burkholderia pseudomallei Yes Camplyobacter spp No, unless part of a known
cluster Chikungunya virus No, unless thought to be UK
acquired Chlamydophila psittaci Yes if diagnosed during
acute phase or part of a known cluster
Clostridium botulinum Yes Clostridium perfringens Only if associated with food
poisoning No, unless known to be part of a cluster
Clostridium tetani No, unless associated with injecting drug use
Corynebacterium diphtheriae Notify without delay, before results of toxigenicity tests are known
Yes
Corynebacterium ulcerans Notify without delay, before results of toxigenicity tests are known
Yes
Coxiella burnetii Yes if diagnosed during acute phase or part of a known cluster
Crimean-Congo haemorrhagic fever virus
Yes
Cryptosporidium spp No, unless part of known cluster, known food handler or evidence of increase above expected numbers
Dengue virus No, unless thought to be UK acquired
Ebola virus Yes Entamoeba histolytica No, unless known to be part
of a cluster or known food handler
Francisella tularensis Yes Giardia lamblia No, unless part of known
cluster, known food handler

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 36 of 37
or evidence of increase above expected numbers
Notifiable organisms Definition/comment Likely to be urgent? Guanarito virus Yes Haemophilus influenzae Invasive i.e. from blood,
cerebrospinal fluid or other normally sterile site
Yes
Hanta virus No, unless thought to be UK acquired
Hepatitis A, B, C, delta and E viruses
All acute and chronic cases All acute cases and any chronic cases who might represent a high risk to others, such as healthcare workers who perform exposure-prone procedures
Influenza virus No, unless known to be a new sub-type of the virus of associated with known cluster or closed communities such as care homes
Junin virus Yes Kyasanur Forest disease virus
Yes
Lassa virus Yes Legionella spp Yes Leptospira interrogans No Listeria monocytogenes Yes Machupo virus Yes Marburg virus Yes Measles virus Yes Mumps virus No Mycobacterium tuberculosis complex
No, unless healthcare worker or suspected cluster or multi- drug resistance
Neisseria meningitidis Excluding asymptomatic cases (e.g. throat carriage)
Yes
Omsk haemorrhagic fever vrius
Yes
Plasmodium falciparum, vivax, ovale, malariae, knowlesi
No, unless thought to be UK acquired
Polio virus Wild or vaccine types Yes Rabies virus Classical rabies and rabies
related lyssaviruses Yes
Rickettsia spp No, unless thought to be UK acquired
Rift Valley fever virus Yes Rubella virus No Sabia virus Yes Salmonella spp Including S. Typhi and S.
Paratyphi Yes, if S. Typhi or S. Paratyphi or suspected outbreak or food handler or closed communities such as care homes No, if sporadic cases of other Salmonella species
SARS coronavirus Yes Shigella spp Yes, except Sh. Sonnei
unless suspected outbreak or

IC/278/10 Isolation precautions for patients with confirmed or suspected infectious illness
Page 37 of 37
food handler or closed communities such as care homes
Streptococcus pneumoniae Invasive i.e. from blood, cerebrospinal fluid or other normally sterile site
No, unless part of a known cluster
Streptococcus pyogenes Invasive i.e. from blood, cerebrospinal fluid or other normally sterile site, or associated with necrotising soft tissue infection
Yes
Varicella zoster virus No Variola virus Yes Verocytotoxigenic Escherichia coli
Including E. coli O157 Yes
Vibrio cholerae Yes West Nile virus No, unless thought to be UK
acquired Yellow fever virus No, unless thought to be UK
acquired Yersinia pestis Yes