joseph roberts, md gastroenterology gastrointestinal clinic
TRANSCRIPT

Fall CME EventOctober 27, 2020
Joseph Roberts, MDGastroenterology
Gastrointestinal Clinic

Incidentalomas of the GI Tract
• Review overview of pancreatic cysts and next steps in management
• Evaluation of the asymptomatic dilated bile duct

Pancreatic Cysts• Pancreatic cysts are incidentally
found on up to 13% of abdominal imaging performed for non-pancreatic reasons1
• Incidence of pancreatic cysts increases with age >70 (as high as 40%), however pooled studies showed an incidence of cysts >2cm of 0.8%1
• Overall incidence rates of pancreatic cancer remains stable, so increased incidence rates of pancreatic cysts are likely due to increased use of advanced abdominal imaging2

Potential for Malignancy• Primary concern with regard to
pancreatic cysts is the malignant transformation rate, which overall is low (0.25%/yr)3
• However, retrospective surgical studies show rates of high grade dysplasia or malignancy as high as 15-70% for surgically resected cysts3
• Despite that, not all pancreatic cysts harbor malignant potential, so identifying type of cysts becomes incredibly important3


Further Evaluation• Evaluation and screening of
pancreatic cystic lesions should only be performed in patient who are fit to undergo surgery
• Patients with “high risk features” should be referred for pancreatic resection
• Lesions that don’t warrant immediate resection should undergo evaluation with EUS and/or imaging surveillance (indications vary)


High Risk Features

Secondary High Risk Features• Upstream pancreatic
atrophy• Elevated CA 19-9 (European
Guidelines)• Patulous Ampulla (fish
mouth sign)• New onset Diabetes
Mellitus• Acute Pancreatitis
unexplained by common causes


Additional EUS Benefit: Fluid Analysis
• Fine needle aspiration allows for fluid acquisition and further testing
• Testing for amylase, carcinoembryonic antigen (CEA), cytology, and mutational analysis– High CEA portends mucinous tumor, generally higher risk– High amylase suggests inflammatory or PD involvement– Cytology low yield as fluid tends to be acellular– Mutational analysis: KRAS and GNAS

Why EUS?• For patients with 1 HRF,
addition of EUS to imaging increased both sensitivity and sensitivity for malignant and high risk lesions (p<.0003)
• Additionally, for patients with 1 HRF, EUS downgraded 30% of cysts to SCA or pseudocysts, not necessitating any follow up.

Main Take Aways• Cumulative yearly progression of high
risk pancreatic to cysts remains low, but even low risk lesions can progress to malignancy
• Current guidelines favor either a conservative or aggressive approach to surveillance and follow up for lesions of low or indeterminate risk, without a clear impact on morbidity and mortality
• Further possible areas of study include risk stratification by cyst fluid genetic analysis, tumor markers, TTN laser endomicroscopy, TTN endobiopsy
• Low risk and non-low risk cystic neoplasms can progress to pancreatic malignancy, and appears to be in a linear fashion (0.6-0.8%/yr)
• Given the risk of late progression to pancreatic cancer, some guidelines advocate for ongoing screening for IPMN, contrary to the AGA recommendations.


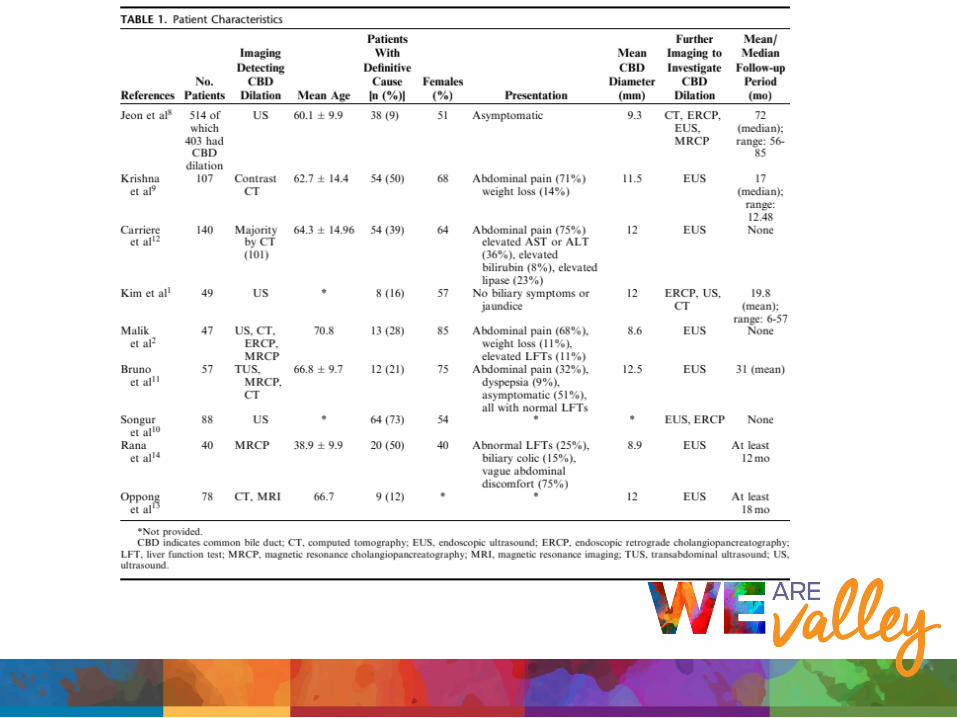
Biliary Duct Dilation • As with Pancreatic Cysts,
with increased abdominal imaging, incidental appreciation of dilation of the common bile duct is frequently observed
• Unfortunately, few studies regarding the yield of further diagnostic work up
• Occult malignancy may be 1.8-5%

Basic Anatomy

How big is too big?• No clear consensus for
normal size of CBD• Common rule: 1mm per
decade of life• Gallbladder in or out?
– How much to you add?
• Generally: >7mm is considered abnormal

Asymptomatic Differential• Choledocholithiasis• Chronic pancreatitis• Ampullary adenoma• Periampullary Diverticulum• Choledochocyst• Distal Biliary stricture• Papillary stenosis
(sphincter of oddidysfunction)
• Cholangiocarcinoma/pancreatic cancer



Risks for Significant Pathology
• Age• Abnormal LFTs (jaundice) • Abdominal Pain• Unexplained pancreatitis• Coincident PD dilation• Intrahepatic duct dilation in addition to CBD

Take Aways
• CBD diameter itself is not correlated with specific pathology
• 9-73% of the time a cause is found• Rate of malignancy is low• Concomitant LFT abnormalities associated
with higher causative lesion found on EUS
What to do?
• No consensus in the GI literature about further work up
• Long term outcomes across populations is not well defined
• EUS was highest yield for providing diagnosis, and generally less invasive than ERCP
• Low risk individual, monitor clinically/labs• Higher risk, or symptoms/labs develop, EUS

Referrals and Location• Referral to GI is the best way to get a patient in to see us, and if marked
urgent gets flagged for our triage nurse to review within 24-48hr. If any concern, can page the on-call provider or send a staff message
• Joseph Roberts, MD– Interventional and Therapeutic Gastroenterology– UW Valley Medical Center– 4011 Talbot Road South, Suite 500, Renton, WA 98055
• Office: 425.690.3488• Fax: 425.690.9088• Cell:425.269.3878