king s research portal - · pdf filedental caries involves interactions between the tooth...
TRANSCRIPT

King’s Research Portal
DOI:10.1038/nrdp.2017.30
Document VersionPeer reviewed version
Link to publication record in King's Research Portal
Citation for published version (APA):Pitts, N. B., Zero, D. T., Marsh, P. D., Ekstrand, K., Weintraub, J. A., Ramos-Gomez, F., ... Ismail, A. (2017).Dental caries. Nature Review Disease Primers, 3, [17030]. DOI: 10.1038/nrdp.2017.30
Citing this paperPlease note that where the full-text provided on King's Research Portal is the Author Accepted Manuscript or Post-Print version this maydiffer from the final Published version. If citing, it is advised that you check and use the publisher's definitive version for pagination,volume/issue, and date of publication details. And where the final published version is provided on the Research Portal, if citing you areagain advised to check the publisher's website for any subsequent corrections.
General rightsCopyright and moral rights for the publications made accessible in the Research Portal are retained by the authors and/or other copyrightowners and it is a condition of accessing publications that users recognize and abide by the legal requirements associated with these rights.
•Users may download and print one copy of any publication from the Research Portal for the purpose of private study or research.•You may not further distribute the material or use it for any profit-making activity or commercial gain•You may freely distribute the URL identifying the publication in the Research Portal
Take down policyIf you believe that this document breaches copyright please contact [email protected] providing details, and we will remove access tothe work immediately and investigate your claim.
Download date: 22. May. 2018

1
FinalsubmittedandacceptedVersionfromNigelPittsasatMarch17th2017
Dentalcaries
NigelB.Pitts1,DomenickT.Zero2,PhilD.Marsh3,KimEkstrand4,JaneA.Weintraub5,Francisco
Ramos-Gomez6,JunjiTagami7,SvanteTwetman4,GeorgiosTsakos8,AmidIsmail9
1DentalInnovationandTranslationCentre,King'sCollegeLondonDentalInstitute,Floor17TowerWing,Guy'sHospital,GreatMazePondRoad,London,SE19RT,UK.2DepartmentofCariologyOperativeDentistryandDentalPublicHealth,OralHealthResearchInstitute,IndianaUniversitySchoolofDentistry,Indianapolis,Indiana,USA.3DepartmentofOralBiology,SchoolofDentistry,UniversityofLeeds,Leeds,UK.4DepartmentofOdontology,UniversityofCopenhagen,Copenhagen,Denmark.5DepartmentofDentalEcology,UniversityofNorthCarolinaSchoolofDentistry,ChapelHill,NorthCarolina,USA6UCLACenterChildren’sOralHealth-UCCOHandSectionofPediatricDentistry,UCLASchoolofDentistry,UniversityofCaliforniaLosAngeles,LosAngeles,California,USA.7CariologyandOperativeDentistry,TokyoMedicalandDentalUniversity,Tokyo,Japan.8DepartmentofEpidemiologyandPublicHealth,UCL,London,UK.9RestorativeDentistry,MauriceH.KornbergSchoolofDentistry,TempleUniversity,Philadelphia.USA.Competinginterests:N.B.P.hasreceivedhonorariaandcorporateandsocialresponsibilitysupportfromColgate,consultationfeesfromCalcivisandholdsstockinaKingsCollegeLondonspin-out,Reminova.D.T.Z.hasreceivedcontractedresearchfundingfromJohnson&Johnson,GlaxoSmithKlein,C3-Jian,andNoveomeBiotherapeutics.P.D.M.,K.E.,J.A.W.,F.R.-G.,J.T.,S.T.,G.T.,A.I.havenoconflicts.
Authorcontributions
Introduction (N.B.P.); Epidemiology (N.B.P.); Mechanisms/pathophysiology (D.T.Z. and P.D.M.);Diagnosis,screeningandprevention(K.E.andJ.A.W.);Management(F.R.-G.,J.T.andS.T.);Qualityoflife(G.T.);Outlook(A.I.);overviewofPrimer(N.B.P.).

2
Abstract|Dentalcariesisabiofilm-mediated,sugar-driven,multifactorial,dynamicdiseaseresulting
inthephasicdemineralizationandremineralisationofdentalhardtissues.Cariescanoccur
throughoutlife,bothinprimaryandpermanentdentitions,andcandamagethetoothcrownand,in
laterlife,alsoexposedrootsurfaces.Thebalancebetweenpathologicalandprotectivefactors
influencestheinitiationandprogressionofcaries.Thisinterplaybetweenfactorsunderpinsthe
classificationofindividualsandgroupsintocariesriskcategoriesallowinganincreasinglytailored
approachtocare.Dentalcariesisanunevenlydistributed,preventablediseasewithconsiderable
economicandqualityoflifeburdens.Thedailyuseoffluoridetoothpasteisseenasthemainreason
fortheoveralldeclineofcariesworldwideoverrecentdecades.ThisPrimeraimstoprovideaglobal
overviewofcaries,acknowledgingthehistoricaleradominatedbyrestorationoftoothdecayby
surgicalmeans,butitfocussesoncurrent,progressiveandmoreholisticlong-term,patient-centred,
tooth-preservingpreventivecare.
3
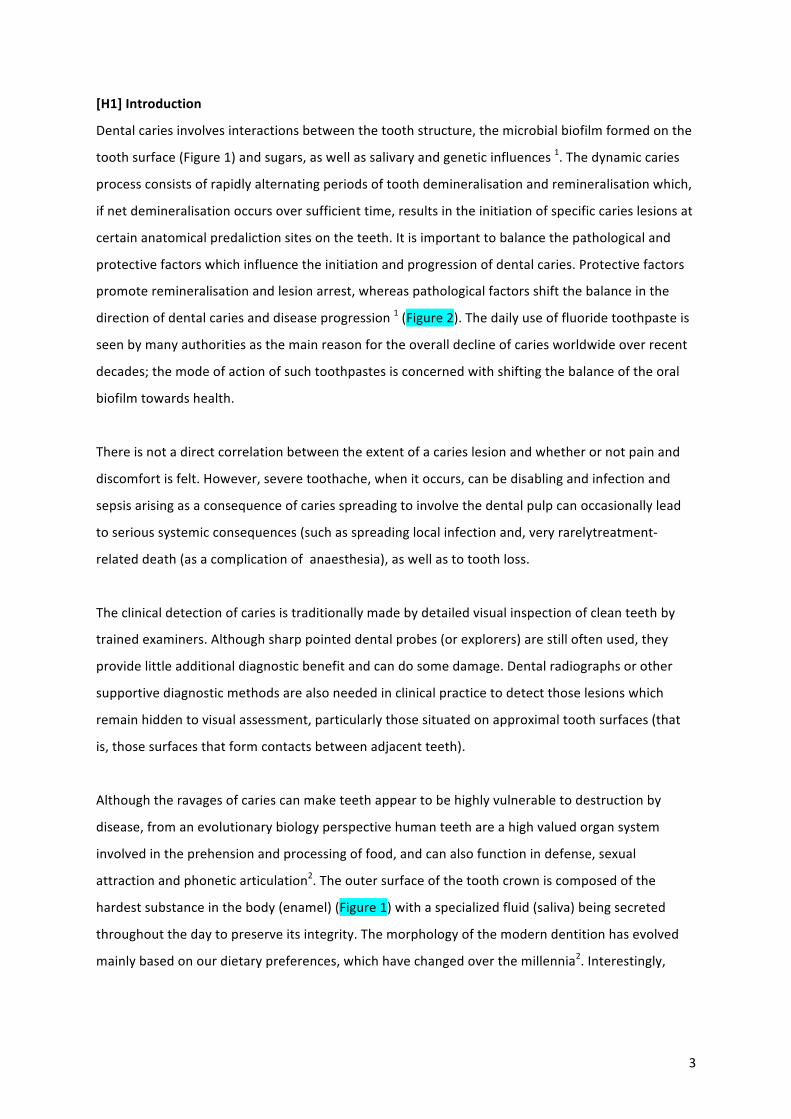
[H1]Introduction
Dentalcariesinvolvesinteractionsbetweenthetoothstructure,themicrobialbiofilmformedonthe
toothsurface(Figure1)andsugars,aswellassalivaryandgeneticinfluences1.Thedynamiccaries
processconsistsofrapidlyalternatingperiodsoftoothdemineralisationandremineralisationwhich,
ifnetdemineralisationoccursoversufficienttime,resultsintheinitiationofspecificcarieslesionsat
certainanatomicalpredalictionsitesontheteeth.Itisimportanttobalancethepathologicaland
protectivefactorswhichinfluencetheinitiationandprogressionofdentalcaries.Protectivefactors
promoteremineralisationandlesionarrest,whereaspathologicalfactorsshiftthebalanceinthe
directionofdentalcariesanddiseaseprogression1(Figure2).Thedailyuseoffluoridetoothpasteis
seenbymanyauthoritiesasthemainreasonfortheoveralldeclineofcariesworldwideoverrecent
decades;themodeofactionofsuchtoothpastesisconcernedwithshiftingthebalanceoftheoral
biofilmtowardshealth.
Thereisnotadirectcorrelationbetweentheextentofacarieslesionandwhetherornotpainand
discomfortisfelt.However,severetoothache,whenitoccurs,canbedisablingandinfectionand
sepsisarisingasaconsequenceofcariesspreadingtoinvolvethedentalpulpcanoccasionallylead
toserioussystemicconsequences(suchasspreadinglocalinfectionand,veryrarelytreatment-
relateddeath(asacomplicationofanaesthesia),aswellastotoothloss.
Theclinicaldetectionofcariesistraditionallymadebydetailedvisualinspectionofcleanteethby
trainedexaminers.Althoughsharppointeddentalprobes(orexplorers)arestilloftenused,they
providelittleadditionaldiagnosticbenefitandcandosomedamage.Dentalradiographsorother
supportivediagnosticmethodsarealsoneededinclinicalpracticetodetectthoselesionswhich
remainhiddentovisualassessment,particularlythosesituatedonapproximaltoothsurfaces(that
is,thosesurfacesthatformcontactsbetweenadjacentteeth).
Althoughtheravagesofcariescanmaketeethappeartobehighlyvulnerabletodestructionby
disease,fromanevolutionarybiologyperspectivehumanteethareahighvaluedorgansystem
involvedintheprehensionandprocessingoffood,andcanalsofunctionindefense,sexual
attractionandphoneticarticulation2.Theoutersurfaceofthetoothcrowniscomposedofthe
hardestsubstanceinthebody(enamel)(Figure1)withaspecializedfluid(saliva)beingsecreted
throughoutthedaytopreserveitsintegrity.Themorphologyofthemoderndentitionhasevolved
mainlybasedonourdietarypreferences,whichhavechangedoverthemillennia2.Interestingly,

4
dietshighinsugartendtobesoftandoftenliquid;teetharenotrequiredfortheiringestion,which
mayexplainwhyteethcanberapidlylost.
TheaimofthisPrimeristoprovideabalancedinternationaloverviewofdentalcaries,bothasa
complex,multi-factorialdiseaseandasadynamicallyfluctuatingdiseaseprocess.Thearticlecovers
thefullrangeofperspectivesfromepidemiologytoqualityoflife—viapathophysiology,diagnosis,
riskassessmentandprevention.Publichealthaspectsareanimportantcomplement,butnot
coveredindepthforreasonsofspace.Currentresearchevidenceishelpingtochartthewayforward
toamorebiologically-basedwayofplanninganddeliveringcariespreventionandcare,atboththe
populationandindividuallevels.Theseconsiderationsunderpinthedevelopmentofscience,
practiceandpolicytooptimisepatientcareandhealth.
5
[H1]Epidemiology
Epidemiological studies of caries have been undertaken formany decades and some of the data
available through WHO and other organisations gives an impression that we have plentiful
comparableglobaldata.However,inordertoevaluateandplanpolicy,epidemiologyshouldprovide
data meeting the following specification: timely, accurate and understandable data for key age
groups on the total amount of disease present (prevalence), the rate of disease progression
(incidence) and disease trends over time. In addition, information on variations in disease levels
between and within countries, including the estimates and trends in health inequalities (that is,
differences inhealthstatusbetweengroupswithinpopulations),areneeded.However,wedonot
currentlyhaveaccurate,up–to-date, clinicallymeaningful informationacross theglobe thatmeets
thesespecifications.Dentalcariesisstillaneglectedtopic,despitetheacknowledgmentoftheWHO
thatisstillamajorhealthprobleminmostindustrializedcountries,where60-90%ofchildrenand
the vastmajority of adults are affected by dental caries3. Although caries has been considered a
diseaseofchildhood,inrealityitcontinuesintoadulthood4,wherehealthinequalitiesremain5.
Dentalcariesareconsideredtobethesinglemostcommonchronicchildhooddisease,andits
prevalenceisthoughttohaveincreasedrecentlyinchildrenages2-5yearsglobally,makingthisage
groupaglobalpriorityactionarea6,7,8.Censusdatafrom2007reportedthatforUSchildrenaged2to
5,cariesprevalenceinprimaryteethshowedanincrease,fromapproximately24%to28%between
1988–1994and1999–2004withcariesratesbeinghigherinchildrenlivinginpoorhouseholdsor
thosefromethnicminorities9.InamorerecentNationalHealthandNutritionExaminationSurvey
(NHANES),from2011-2012approximately23%ofUSchildrenages2-5yearshaddentalcariesin
primaryteeth.Inaddition,thesamedatarevealedthatapproximately10%ofUSchildrenages2-5
yearshaduntreateddentalcaries.Dentalcariesprevalenceshowsmarkeddifferencesindifferent
regionsoftheUS.InarecentstudyusingtheNHANESdatafrom1999-2004,childreninLACounty,
oneofthelargestUScounties,weremorelikelytoexperiencedentalcariesthantheaverage
numberacrosstheUS.Nearly40%ofpreschoolchildrenresidinginLACountyhaddentalcariesin
primarydentitioncomparedto28%ofsameagechildrenintheUS.ChildrenresidinginLACounty
hadlessfavorableoralhealththanchildrenintheUSin1999-2004withethnicminoritieshavingthe
worst10.Earlychildhoodcaries(ECC)–averyseveretypeofcariesinchildrenisacommon
bacterially-mediatedandmultifactorialdiseasecharacterizedbymarkeddecayoftheteethof
children≤6yearsofagewhichisthoughtbysometobetransmissiblefromcaretakerstotheir
childrenbutisfullypreventable.RepresentativeinternationaldataispatchyonECC,asmost
countriesonlyreportcariesfromage5or6years.
6
Traditionally, low caries prevalence has been observed in the developing countries, whereas the
prevalenceishigher indevelopedcountries.3Thisgeographicsituationhasbecomemorecomplex
due to speed of economic development and rapid changes in habits and diet inmany countries.
Although there might be gender or ethnic differences, they are minor compared with by sugar
consumption,lifestyleandeconomicdifferences.
The traditional global index used tomeasure caries in epidemiological studies— but not clinical
practice— is theDMF (Decayed,MissingandFilled) index,which isanumerical countofaffected
teethperindividualcollectedateithertheTooth(DMFT)ortoothSurfacelevel(DMFS).Thecountof
DMFTforanindividualorgrouprecordstheircariesexperience(thatis,thetotalofbothcurrentand
past caries). The index canbeusedat thedifferentdiagnostic thresholdswhichaffectbothmean
DMFTandtheproportionofindividualsaffected11,12,13.Dependingonthecriteriaused,proportionof
15-yearoldsvariesbetween11-52%(Figure3)14.
Effortsareunderwayworldwidetoimproveourunderstandingofcariesepidemiologybyimproving
methodologies and optimising them for use in epidemiological field work, while also keeping
compatibility with systems used in a fully equipped dental practice. In epidemiology, the
InternationalCariesDetectionandAssessmentSystem(ICDAS)“Epimodifications”12,whichcanbe
usedalongsidetheWHObasicreportingcriteria13,havenowbeenused inmanycountries,15along
withthemorerecentsimplifiedmerged-codesoption16 (Figure3).ThemergedICDAScodes,which
arecloser to thoseused inclinicalpractice,considerssoundsurfacesandthreestagesofcariesas
opposedtosoundsurfacesandsixstagesofcariesinthefullcodesICDASoption.Itisalsopossibleto
combineclinicalandradiographicfindingstorevealthefullprevalenceofcaries17.Recentworkbya
numberofEuropeanorganisationshasshown—bywayofaglobalexample—thatmostofcurrent
nationalcariesdataforDMFTlevelsin12-year-oldchildrenarenotcomparableacrossEurope15.This
highlightstherealchallengesfacingepidemiologicalstudiesoncarieswhereapparentlycomparable
resultsfromacrossanumberofcountrieshave,infact,beencollectedatdifferenttime-pointswith
veryvariablelevelsoftrainingandcalibrationandrecordcariesatdifferentthresholds.
WhenoralhealthtopicswereaddedtotheongoingGlobalBurdenofDiseaseStudy18,oraldiseases
were found to be highly prevalent, affecting approximately 3.9 billion people worldwide. The
methodologyusedinthismajorstudyisusefulbecauseitallowscomparisonwithotherdiseasesin
terms of burden, but also novel from a caries epidemiology since it does not use theDMF Index

7
(whichhasbeenusedglobally for the last60years).Untreatedcaries inpermanentteethwasthe
mostprevalentconditionevaluatedacrossallmedical conditions,withaglobalprevalenceof35%
forallagescombinedwith2.4billionpeopleaffected.Notethatsomeofthesepermanentteethwill
havebeeninchildrenandadolescents.Untreatedcariesinprimaryteethinchildrenrankedthe10th
inprevalence,affecting621millionchildrenworldwide.
[H1]Mechanisms/pathophysiology
Themechanismsandpathophysiologyunderlyingthedevelopmentofdentalcariesarenow
increasinglywell-understoodandarebestconsideredfirstfromthehardtissue-relatedaspects(as
thediseaseaffectsthecalcifieddentaltissues)andthenfromthemicrobiology(biofilm)-related
aspects(astheserepresentthedriverofthecariesprocessifhomeostaticimbalanceismaintained)
(Figure1).However,becauseofthemultifacetednatureofthediseaseprocess,thesefactorsare
notindependent.Thedentalhardtissuesthatareexposedtotheoralenvironment(crownsand
laterrootsfollowinggingivalrecession)arethetargetsofthecariesdiseaseprocessandalltooth
surfacesaresusceptiblethroughoutanindividual’slifetime.However,carieswillnotoccurinthe
absenceofacariogenic(pathogenic)dentalbiofilmandfrequentexposuretodietarycarbohydrates,
mainlyfreesugars19,20,andthuscariesmustbeconsideredadietary-microbialdisease21.Amodern
conceptofcariesalsoincludesconsiderationofhowbehavioural,social,andpsychologicalfactorsas
wellasbiologicfactorsareinvolved22,23,24.Theimportanceoffluorideinmodifyingdisease
expressioncannotbeoveremphasised25(Box1).Perhapsdentalcariescanbebestdescribedasa
complexbiofilm-mediateddiseasethatcanbemostlyascribedtobehavioursinvolvingfrequent
ingestionoffermentablecarbohydrate(sugarssuchasglucose,fructose,sucrose,andmaltose)
andpoororalhygieneincombinationwithinadequatefluorideexposure.
[H2]Demineralizationandremineralization
Dentalcariestypicallystartatandbelowtheenamelsurface(theinitialdemineralisationissub-
surface)andistheresultofaprocesswherethecrystallinemineralstructureofthetoothis
demineralizedbyorganicacidsproducedbybiofilmbacteriafrommetabolismofdietary
fermentablecarbohydrates,primarilysugars.Althoughawiderangeoforganicacidscanbe
generatedbydentalbiofilmmicroorganisms,lacticacidisthepredominantendproductfromsugar
metabolism26andisconsideredtobethemainacidinvolvedincariesformation.Asacidsbuildupin
thefluidphaseofthebiofilm,thepHdropstothepointwhereconditionsatthebiofilm-enamel
interphacebecomeundersaturatedandaciddemineralizesthetoothmineralsothesurfacelayerof
thetoothispartiallydemineralized27.Thelossofmineralleadstoincreasedporosity,wideningofthe

8
spacesbetweentheenamelcrystalsandsofteningofthesurface,whichallowstheacidstodiffuse
deeperintothetoothresultingindemineralizationofthemineralbelowthesurface(sub-surface
demineralization).Thebuild-upofreactionproducts,mainlycalciumandphosphate,from
dissolutionofthesurfaceandsub-surfaceraisethedegreeofsaturationandcanpartiallyprotectthe
surfacelayerfromfurtherdemineralization.Also,thepresenceoffluoridecaninhibitthe
demineralizationofthesurfacelayer28.Oncesugarsareclearedfromthemouthbyswallowingand
salivarydilution,thebiofilmacidscanbeneutralizedbythebufferingactionofsaliva.ThepHof
biofilmfluidreturnstowardneutralityandbecomessufficientlysaturatedwithcalcium,phosphate,
andfluorideionssothatdemineralizationstopsandre-depositionofmineral(remineralization)is
favoured.Duetothedynamicnatureofthediseaseprocess,theveryearly(subclinical)stagesof
cariescanbereversedorarrestedespeciallyinthepresenceoffluoride.
Asdemineralizationprogressesintothesubsurfaceoftheenamelanddentininthecaseofroot
caries,withacontinuingacidchallengeandpHdroptherateofminerallossbecomesgreaterinthe
subsurfacethanatthesurface,resultingintheformationasubsurfacelesion.Whensufficient
mineralislost,thelesionappearsclinicallyasawhitespot.Thisisaclinicallyimportantstageofthe
cariesprocess,sincethelesioncanbearrestedorreversedbymodifyingthecausativefactorsor
applyingpreventivemeasures;however,therepairprocessistypicallymostlyrestrictedtothe
surfacelayer.
Atthisstageinitsdevelopment,initial-stagecaries(ICDAScodes1and2)areconsiderably
demineralised,theymaywithchangesinthelocalecology,dietarypracticesandfluorideavailability
arrestandremainastheyare(inactivelesionswhichdonotprogressbutremainsstillrecognisable
asascarbecauseofthechangesintheopticalpropertiesoftheenamel),remineraliseand
effectivelyheal(re-precipitationofmineralinthelesionandpossiblysomesuperficialsurfacewear
resultinginanapparentlysoundsurface),orremainactiveandprogresstoamoreextensivestageof
destruction.
Ifthecariesprocessprogressesfurther,thesurfaceporosityincreaseswiththeformationof
microcavitationsinenamel(ICDAScode3)orinrootcaries—aprogressivesofteningofthesurface
dentinelayer.Incariesofthetoothcrownthesurfacelayerofthelesionmayeventuallycollapse,
resultinginphysicalcavitation(amacroscopichole–ICDAScode5or6).Evenatthismoreextensive
stageofcariesseverity,alesionmayinoptimalcircumstancesstillarrest,althoughthebiofilm
retainingcavitywillpersist.Whenanirreversiblestageoflesionextentisreached(typicallyinmost
9
developedcountriesICDAS5&6),combinedwithsymptomsand/orconsiderationsofthefunctional
oraestheticneedsofthepatient,operativeinterventionisindicated.Ifthecariesprocesscontinues
eventuallythedentalpulpwillbecompromisedandeitherarootcanaltreatmentortooth
extractionwillbenecessary.
Foroptimaltoothhealth,themaingoalistomaintainthemineralhomeostasisoftoothsurfaces.
Sinceteetharefrequentlyexposedtoacidicconditionseitherfrombiofilmordietaryacids,the
abilitytoremineralizeisessentialtomaintainingtoothintegrity.Salivaisessentialforpreservation
oftoothhealthbyprovidingthemineralsnecessaryforremineralization.Lowlevelsoffluoride
greatlyenhancethisprocess,whichlargelyexplainstheremarkableeffectivenessoffluoridein
multipledeliveryformsinreducingdentalcaries(Box1)28.
Dentalcariesisadynamicdiseaseprocessinvolvingrepeatedcyclesofdemineralizationand
remineralizationthroughouttheday27,29.Teetharemostsusceptibletocarieswhentheyfirsteruptin
themouthandovertimebecomemoreresistanttosubsequentacidchallenge.Theclinical
implicationisthatthereshouldbegreaterfocusonmonitoringthecariesstatusofteethand
deliveringpreventivecareduringtheperiodswhenteethareerupting.
[H2]Microbiologyanddentalbiofilms
[H3]Oralmicrobiotainhealth.Themouth,suchasothersurfacesofthebody,iscolonizedfrom
birthbyadiversearrayofmicroorganisms(theoralmicrobiota)30.Themostcommongroupof
microorganismsarebacteria,butyeasts,viruses,mycoplasmas,protozoaandArchaeacanbe
present.Theoralmicrobiotahasasymbioticormutualisticrelationshipwiththehost.Theresident
oralmicroorganismsbenefitfromawarmandnutritioushabitatprovidedbythehostand,inreturn,
acttorepelinvadingmicrobes,contributetothehostdefences,andengageincross-talkwiththe
hosttodown-regulatepotentiallyexcessivepro-inflammatoryresponsestocommensalbacteria31.
Salivaplaysacriticalroleinmaintainingthisbeneficialmicrobiotabybufferingtheoralenvironment
ataneutralpH(optimalforthegrowthandmetabolismofmostoftheoralmicrobiota),while
providingproteinsandglycoproteinsasnutrients.
[H3]Dentalbiofilms.Theoralmicrobiotagrowsonsurfacesasstructurallyandfunctionally
organisedcommunitiesofinteractingspecies,termeddentalplaque32,33.Dentalplaqueisan

10
exampleofabiofilm,theformationofwhichinvolvesanumberofstages34.Toothsurfacesare
coveredbyaconditioningfilmofproteinsandglycoproteins(theacquiredpellicle)thatarederived
mainlyfromsaliva,butalsocontainscomponentsfrombacteriaandtheirproducts,gingival
crevicularfluid(thatseepsfromthejunctionbetweenthegumandthetooth),blood,andfood35
(Figure1).Theacquiredpellicleprovidesbindingsitesforadherencebyearlybacterialcolonizersof
thetoothsurfaceleadingtodentalbiofilmformation,andalsoactsasphysicalbarrierpreventing
aciddiffusion36.
Bacteriacanbeheldweaklyandreversiblynearthesurfacebylong-rangevanderWaalforces(force
thatdonotinvolvecovalentorionicbonds)betweentheexternallayersofthebacteriumandthis
conditioningfilm.Attachmentbecomesstrongerandmorepermanentifinteractionsoccurbetween
moleculesonthebacterium(adhesins)andcomplementaryreceptorsintheconditioningfilm32.
Secondarycolonisingspeciesattachtotheearlycolonisers(coadhesion),andthecomplexityofthe
biofilmincreases.Thebiofilmundergoesmaturation,andnumeroussynergisticandantagonistic
microbialinteractionsoccur37.Amatrixisformed,composedofbacterialexopolymers(polymer
secretedintheexternalenvironment),includingpolysaccharidesderivedfromsugarmetabolismand
DNA;thematrixhelpstoretainthebiofilmonthesurfaceandcaninfluencethepenetrationand
movementofmoleculeswithinthebiofilm37,38.Thebiofilmprotectthebacteriaagainstantimicrobial
agents.Thecompositionofthesebiofilmsvariesondifferentsurfacesofthetoothduetosubtle
differencesinthelocalenvironmentalconditions.
[H3]Microbialaetiologyofdentalcaries.Thenormallysynergisticrelationshipbetweenthe
residentmicrobiotaandthehostisdynamicandcanbeperturbedbychangesinlifestyleor
alterationstothebiologyofthemouth;thesechangescanpredisposesitestodisease.Riskfactors
forcariesincludethefrequentconsumptionoffermentabledietarycarbohydrates(especially
sucrose)39and/orareducedsalivaflow40.Numerouscross-sectionalandlongitudinal
epidemiologicalstudieshavereportedashiftinthebalanceofthemicrobiotaatsiteswithcaries
comparedwithsiteswithsoundsurfaces.Earlystudiesofcarieslesionsfoundhigherproportions
andincidenceofStreptococcusmutansandS.sobrinuscomparedwithsoundenamel;lactobacilli
wereisolatedfromadvancedlesions40.Theseobservationsledtotheproposalthatcariesareonly
causedbyalimitedsubsetofthemanyspeciesfoundindentalbiofilms(the‘specificplaque
hypothesis’)41.However,asmoreepidemiologicalstudieswereperformed,carieswereobservedin
11
theapparentabsenceofthesebacteria,whereastheseorganismscouldpersistonothersurfaces
thatremainedsound.
Subsequentlaboratorystudiesconfirmedthatotherbacteriafoundwithindentalbiofilmscouldalso
generatealowpHfromsugars,whereasotherscouldreducethepotentiallydamagingeffectof
lacticacidbyusingitasanutrientsourceandconvertingthemtoweakeracids,orbygenerating
alkalifromthemetabolismofarginineorureainsaliva.Thesefindingsprovidedsupportforthe
‘non-specificplaquehypothesis’,inwhichcariesisaconsequenceofthenetmetabolicactivityofthe
biofilm41.Morerecently,studiesusingclassicalcultureormolecularapproacheshavefound
associationsbetweencariesandothergroupsofacid-producingandacid-toleratingbacteria,
includingarangeofBifidobacterium,ActinomycesandPropionibacteriumspecies,andScardovia
wiggsiae.
Subsequently,alternativeconceptshavebeenproposedbasedonecologicalprinciplesthat
describetheeventsassociatedwithcaries42,43;theseecologicalplaquehypothesesarenowgenerally
accepted as the most plausible explanations of the microbial aetiology of caries (Figure 4). The
original‘ecologicalplaquehypothesis’recognizedtheconsistencyofbacterialfunction(thatis,rapid
acid production and tolerance of the acidic conditions generated) in the absence of specificity in
bacterialname,andemphasizedtheessentialrequirementofacaries-conduciveenvironment(that
is,sugar-richdietand/orlowsalivaflow).Microorganismswithtraitsthatarerelevanttocariescan
be present in biofilms on sound enamel, but at a level or activity that is too low to be clinically
relevant42.Cariesisaconsequenceofanunfavorableshiftinthebalanceoftheresidentmicrobiota
drivenbychangesinthedentalenvironment.Theregularexposureofplaquetofermentabledietary
sugars results in repeated conditions of low pH in the biofilmswhichwill favour the growth and
metabolismofacid-toleratingbacteriawhileinhibitingbeneficialorganismsthatpreferentiallygrow
atneutralpH. Implicit in thishypothesis is theconcept thatdiseasecanbecontrollednotonlyby
directly inhibiting the implicated bacteria but also by interfering with the factors that drive the
deleteriousshifts inthemicrobiota(that is, reducingtheamountandfrequencyofsugar intaketo
prevent acidic conditions, or promoting the use of snacks containing alternative sweeteners that
cannot be metabolized to acid by oral bacteria)42. The ecological plaque hypothesis has recently
been developed further to reflect the ability of some oral bacteria to adapt to acid stress during
regular andprolonged conditions of lowpH [the ‘extended caries ecological hypothesis’]43. Again,
acidificationof theplaqueacts as themain factor selectinganacid-generatingandacid-tolerating
bacterialcommunity,thedevelopmentofwhichwillincreasetheriskofcaries43.

12
Dentalcaries,therefore,isnotanexampleofaclassicinfectiousdiseasebutisa
consequenceofanecologicalshiftinthebalanceofthenormallybeneficialoralmicrobiota,driven
byachangeinlifestyleandoralenvironment.Anappreciationoftheseprinciplesopensupnew
avenuesforcariesprevention.
[H2]Environmentanddentalcaries
Althoughbiofilmformationisanaturalprocessandisanessentialstepforcariesformation,the
presenceofabiofilmonatoothsurfaceisnotinandofitselfanindicationthatdiseaseispresent.It
isonlyafteracomplexinteractionofhostfactors,includingthetoothsurface,acquiredpellicleand
saliva,andfreesugarsinthedietthatthepresenceofthedentalbiofilmcanleadtodisease
expressionovertime.
Theuniqueenvironmentalconditionsthatexistofeachtoothsiteexplainthehighlylocalizedand
complexnatureofthecariesprocesswherebycariescanoccurataspecificlocationofthetooth
surfaceandnotonanadjacenttoothsurfaceevenwhenbothappeartobecoveredbybiofilm27.
Theseincludetooth-relatedfactorsthatimpactacidsolubility(forexample,toothcomposition
(imperfectlyformedstructureasinhypoplasias)andstructure,andpre-eruptiveandpost-eruptive
fluorideexposure,post-eruptiveageofthetooth),andthosethatinfluencebiofilmthicknessand
pathogenicitybycreatingareasofplaquestagnation(forexample,toothmorphology,archform,
occlusionandtoothposition)36,37.Developmentdefects(forexample,enamelhypoplasia,a
conditioncharacterizedbythinenamel)mayleadtoincreaseacidsolubilityandlossofsurface
structurecreatingsitesofplaquestagnationandincreasedriskofcariesinprimaryteeth44.Caries
susceptibilitycanalsobeaffectedbyproximityofteethtosalivaryglandorifices,andsalivaryfilm
thicknessandvelocityatspecifictoothsites36,37.Dentalappliances(suchasorthodonticappliances
anddentures)andfaultyrestorationscanalsoincreasecariessusceptibilityatspecifictoothsitesby
creatingareasofstagnationencouragingbiofilmformation27.
13
[H1]Diagnosis,screeningandprevention
Diagnosis,riskassessment,screeningandpreventionareallvitallyimportantconsiderationsforthe
successfulunderstandingandcontrolofdentalcariesatboththeindividualandpopulationlevels.In
manycountriesscreeninghasaspecificpublichealthmeaningdiscretefromclinicalpractice,butthis
topicisbeyondthescopeofthisPrimer.Thefocushereisonwhathappensattheindividualpatient
level,wherehighnumbersofpatientsinteractwithoralhealthprofessionalsaroundtheworldona
dailybasis.Itmustbeemphasisedthat,inordertopreventandcontrolcaries,bothpublichealth
andindividuallevelinterventionsneedtobeoptimisedandaligned.
TheInternationalDentalFederation(FDI)1,45anddedicatedmeetings46havereviewedthecaries
systemsthatareavailable.Althoughexcellentworkhasbeencarriedoutinsomecountriesin
developingarangeofassessmentsystems(Box3),thereisashortageofcomprehensive,
internationallyapplicable,evidence-informed,holisticclinicalsystems,letaloneonesdevelopedby
formalconsensusprocesses.Therefore,whilstfullyacknowledgingthattherearearangeofother
systemsforundertakingsomepartsoftheclinicaltasksrequiredtoinformmoderncaries
management,wewillusetheInternationalCariesClassificationandManagementSystem(ICCMS47-
50)asaunifyingframeworktoillustratethekeypoints(Figure5).InICCMS,theelementsofcaries
riskassessmentatboththepatientandintra-orallevels,togetherwiththeclassificationofcariesby
staginglesionseverityandassessinglesionactivitybasedontheICDASsystemarebroughttogether
withdecisionmaking.Thisinformationisusedtoproduceapersonalisedcareplanwhichcanthen
beundertakenwithanemphasisontooth-preservingcariespreventionandcontrol,followedbyrisk
basedfollow-upplan(dentalrecall).47-50Thefourkeyelementsofthesystem(simplifiedforgeneral
practiceasthe“4DICCMSCariesManagement”)allowsacomprehensiveassessmentand
formulationofapersonalisedcariescareplanFigure5.
[H2]Prevention
[H3]Publichealthmanagement.Thegoalofdentalcariespreventionistopreservesound
toothstructure,preventdemineralizationofenamelandpromotenaturalhealing
processes46.Interventionscanbeimplementedatthepopulationlevelwithhealthpolicy,
legislation,regulationandpublichealthapproachestopromotehealthybehavioursand
14
impactbroadersocialdeterminantsofhealth51,52.Preventionapproachesmaytargetan
entirepopulation(forexample,waterfluoridationandsugartaxes)toassureequity,or
higher-riskgroupstoseektoincreasecost-effectiveness.Thesubjectoffluorideandcariesis
consideredinBox1,whilethereisfurtherconsiderationoffluoridesandcariesprevention
inBox2.Somecariesriskfactorsatthepopulationlevelincludelowfamilyincome,
restricteddentalcareaccess,lowfluorideexposure,loworalhealthliteracyandhighcaries
prevalence.Researchisongoingtofindthebestwaystotargethighcaries-riskindividuals.
Preventionprogrammescanbetargetedatgroupswithmedicalorspecialhealthcareneeds
suchasthosewithcompromisedimmunity(forexample,HIVandleukemia),cognitiveor
developmentaldisabilitiesthatcanmakeoralhygienedifficult,geneticdisordersthatare
associatedwithoralconditions(forexample,cleftlipandpalate,ectodermaldysplasia),
salivarydysfunctionfromSjögrensyndrome,diabetes,orfrequentuseofsomemedications
thatcausedrymouth(forexample,antihistamines).
Sincedentalcariesisamulti-factorialdisease,complementaryinterventionsmaybemoreeffective
thansingleinterventions.TheWHO’soralhealthactionplanemphasizestheneedfororalhealth
preventionprogrammestobecombinedwithotherchronicdiseasepreventionandeducational
programmesandpoliciessharingcommonriskfactors53.Inthefuturesharedelectronichealth
records,mobilesmartdevicesandsocialmediamayassistintheseefforts54.TheAlliancefora
Cavity-FreeFuture(aninternationalpublichealthadvocacycharity)haschaptersworldwide
promotingacomprehensiveagendaofactivitiesandresourcestopreventcariesinitiationand
progression.Advocacyandeducationeffortsincludeincreasingpublicawarenessandbehaviour
changetoimproveoralhygieneanddecreasesugarconsumption,advancingresearchandclinical
cariesmanagement55.56.
Manywatersuppliescontainnaturallyoccurringamountsoffluoride.Communitywaterfluoridation,
theadjustmentoffluoridetocommunitywatersuppliestoobtainoptimallevelsforcaries
prevention,isacost-effective,equitable,population-approachthatbestmeetspublichealthcriteria
andbenefitsallagegroups(Box2)57.TheUnitedStatesPublicHealthServicerecommendsthe
concentrationof0.7mg/ltomaximizecariespreventionwhileminimizingtheriskofdental
fluorosis58.Thisapproachislikelytoprovidesocietalcost-savings59.TheWHOrecommendsahigher
concentration(1.5mg/l)butflagsthattheexpectedvolumeofwaterconsumedandintakeof
fluoridefromothersourcesshouldbeconsideredwhensettingnationalstandards60.

15
Saltfluoridation,oftencombinedwithiodizedsalt,isaneffective,frequentlyusedpopulation-based
methodofcariesprevention.ItisusedprimarilyinEurope,CentralandSouthAmericawhere
fluorideinthedrinkingwaterislow,communitywaterfluoridationisnotfeasible,andotherforms
offluorideareusedlessfrequently61.Thefluorideconcentrationinsaltisusually250-300partper
million(ppm).Itistheleastexpensivemethodofcariesprevention62.Milkfluoridationprogrammes
havebeenusedinsomecountriessuchasHungaryandtheUK.63.64
Dentalsealantsareprofessionallyappliedresinmaterialbrushedontothecaries-pronepitand
fissuredgroovesoftheocclusalchewingsurfacesofchildren’smolars(backteeth)toprevent
diseaseinsoundteethorarrestprogressionofinitialnon-cavitatedcariouslesions65.Theapplication
doesnotrequirelocalanaesthesiaandsealantscanbeappliedinschool-basedprogrammeswith
portableequipment.Sealantprogrammesareaneffectivecommunityapproach66thatcanbecost-
effectivewhenappliedtochildrenathighercaries-riskorfromlow-incomefamilies67.IntheUnited
States,schoolswithmanychildrenenrolledintheFreeandReducedPriceMealProgramare
targetedforschool-basedinterventions68.
Althoughpreventivestrategiesshouldbecosteffectiveandresultinsocietalcostsaving,prevention
programmesincurmanyup-frontcosts,whereasthesavingsgainedbyaverteddiseaseand
treatmentmaytakeyearstoaccrue69.Theimpactofdentalpainandinfectiononqualityoflifealso
needstobeconsidered.Economicassessmentsofpreventivestrategiesdependonmanyfactors
includingcariesprevalence,personnelandmaterialcosts,interventioneffectivenessandtimeframe.
Examplesofresultsfromtwodifferentpopulationsfollowforcomparison(Box4)70,71.
[H3]Individualpatientlevel.Manyofthesameapproachesandtechnologiesusedatthepopulation
levelarealsoappropriateforuseinthedentalofficeorcommunitycliniclevel.Arangeofevidence
basedtoolkits72,.clinicalguidelines73,74Cochranesystematicreviews75,takentogetherwiththeWHO
Guidelineonsugarconsumption76,providearichevidencebasetosupportcariespreventionin
individualspresentingatthedentaloffice.Thisisbuiltaroundadvicetolimitamountandfrequency
ofsugarintake(alsolinkedalsotoobesityanddiabetesprevention)aswellasthefrequentuseof
fluoridecontainingtoothpastes,supplementedaccordingtocariesriskstatusbyfissuresealantsand
moreintensivepreventiveinterventions.
16
[H2]Diagnosis
[H3]Riskassessment
ThefirstelementinassessinganindividualforcariesaccordingtotheICCMSsystemistodetermine
patient-levelcariesriskbytakingacomprehensivehistoryaskingaseriesofquestionsknowntobe
associatedwith increased caries risk or caries protective factors. This includes assessment of the
medicalhistory,and the relevantsocialhistory, forexamplewhere thepatient isbornandraised,
the present residence, education level, and occupation. Finally, the patient is asked about diet
conditions intermsofamountofsugar intakeandfrequencyperday,numberof inbetweenmeal
snacks and the typeof toothpasteused; all information important to assess the caries risk at the
individuallevel77.
AwiderangeofriskassessmenttoolscanbeusedandarecompatiblewiththeICCMSSystem.One
such risk assessment is Cariogram78 , forwhich there ismore evidence than formany alternative
systems; studies have shown moderate accuracy on children and young adults79. Others include
CAMBRAandother risk factorsquestionnaires fromanumberofUniversitiesarealternatives.The
Cariogramuses9predicators in its full form:DMFT,relateddiseases,dietcontent,diet frequency,
amountofplaque,levelsofmutansstreptoccocci,fluorideuse,salivasecretion,andbuffercapacity.
A lowscore(0,1) indicatesthataparticularpredictorcontributesto lowrisk,whereasahighscore
(2,3)tohighrisk,anoverallriskcanbeestimated,ifthepatient’sprofileremainsstable78.
Theriskassessment(independentofhowit isderived)canbebuilt later intotheICCMScariesrisk
likelihoodmatrix49,50,whichcombinesclinicalcariesactivitywithrisklevelassessment.Eventually,it
ispossible toassess if thepatient is in low,moderateorhigh riskof gettingmorenew lesionsor
progressionof theexisting caries lesions,within thenext fewyears. The riskofdevelopingdental
caries can be lowered by effective dietary advice, improved plaque control and increased use of
fluoride,forexamplebyusing1450ppmfluoridatedtoothpasteinsteadof1050ppmtoothpaste80,
assumingthatthepatientiscompliant.
[H3]Clinicalassessments
Inorderto findandassessanycaries lesionson individual toothsurfaces,aclinicalexamination is
performed (thedetectandassesselementof the ICCMS4Dmethodology).Thegoal is to findany
caries lesions present and assess their severity, activity and the risk factors at the tooth level.
Assessmentscanincludesalivasecretion(andinsomecountriesbuffercapacityandthepresenceof
mutans streptococci is measured). Whilst these latter tests are deemed to have some value in
17
patientmotivation, increasing knowledge as to the complexity of thebiofilm ismaking such tests
lessclinicallyrelevant.Thelevelofplaquepresentisassessedclinicallyasithelpsinassessingcaries
activity.Professionaltoothcleaningthenallowstheidentificationofinitial-stagelesions81andlater-
stagelesionswhicharebestdetectedonclean(plaquefree)dryteeth.Locationofgingivalbleeding
duetogentleprobingisalsonotedasafurtherindicatoroflesionactivity.Clinicalexaminationalone
will, formanypatients,be insufficient inmakinga completeassessmentof caries. This isbecause
usingvisualexaminationalonethedentist/dentalhygienistsmaymissagreatnumberofinitialand
evensomemoreseverelesions(Figure6A).82,83
Thenthemouthisdriedbymeansofcottonrolls,andtheindividualtoothisexaminedbyusingthe
dentalcompressedairsyringe.Lesionseverityisthenassessedaccordingtotheclinicalappearance
ofthetoothsurfaces47,48,49,50.Althoughformanyyearsandinmanycountriesdentistshaveuseda
sharp explorer of dental probe to press into tooth fissures, it is now accepted that there is little
diagnosticbenefitfromthetactileelementanditmayconvertaninactivelesionintoanactiveone.
Anassessmentofcariesactivityofthedetectedandstagedlesionscanthenbemade.IntheICDAS
classificationsystem48,84,85,severalpredictorsareused:thelocationofthelesion(plaquestagnation
areaornot);thecolourofthelesion(whitishversusbrownish);tactilefeeling(rough,smooth)when
a blunted probe is run over the lesions, whether the lesion is matte or shiny, cavitated or non-
cavitated;andfinally,ifthelesionislocatedalongthegingivallineandwhetherthegingivableeds
afterprobingornot.Ifthelesionhasmoreofthefollowingcharacteristics(plaquestagnationarea,
whitish, rough tactile feeling, matted, cavitated, and gingiva bleeding) versus the other
characteristics,thelesioniscategorizedasactiveandthefinaldiagnosisofthelesionwillbeinitial,
moderateorextensiveactive.Ifnot,lesionsareclassifiedasinitial,moderateorextensivearrested
(inactive)47.
[H3]Radiographicassessment
Radiographicexaminationshavebeenanimportantpartofcariesassessmentseversincediagnostic
radiography became available (Figure 6B). However, there is a delicate balance to be struck in
balancingthediagnosticbenefitagainstthesmallbutrealrisksofusingionizingradiationelectively.
Thereforedecisionsas towhenandhowoften to takedental radiographs forcariesdetectionwill
dependuponfactorssuchastheresultofathoroughclinicalexamination,thepatient’scariesrisk
status,theirageandwhenradiographswerelasttaken.Theso-calledbitewingradiographprovides
18
valuableinformationforcariesinthetoothcrowns,butthesemustbesupplementedbyadditional
viewsforsomepatients.
AlthoughthedoseofionizingradiationhasreducedwithimprovementsinX-raygenerationandthe
speedandsensitivityoffilmsandsensors,thereisstillaresponsibilitytokeepexposuresaslowas
reasonably achievable and to use other diagnostic information where available to minimize
radiographic exposures. Examples of clinical indications for a radiograph could be: suspicion of a
carieslesionforasurfacethatisnoteasilyinspectedvisuallyandassessmentofthedepthofalesion
whichis,atleastpartly,visibleclinically.
Itshouldbeappreciatedthatclinicallyforsomesurfaces,particularlyapproximalsurfaceswherethe
site of caries attack cannot be visualized directly, radiographic information can be pivotal in
assessing the extent of caries lesions in terms of depth towards the dental pulp. However, this
informationhastobecombinedwithknowledgeaboutcariesactivitystatusandoverallcariesrisk
when integrating all information into a personalized care plan including decisions to treat non-
operatively or operatively (the D for Decide in the 4D System). Other situations where the
radiographic information can be invaluable include suspicious occlusal fissures where, in a high
fluorideenvironment,anapparentlysmall lesionmayonoccasionextendradiographically intothe
innerdentine.Theseexampleshighlighttheimportanceofcombiningandintegratingtheclinicaland
the radiographic information inorder tobe able tomakeaccuratediagnoses fromwhich tobuild
appropriate care plans. Recall frequency for both clinical and radiographic examination should be
decidedonanindividualisedbasis,accordingtocariesrisk.
At the end of the clinical and then the radiographic examination information on lesions visually
detectedand/orradiographicallydetectedcanbecombinedinordertomakeadiagnosis(Figure6).

19
[H1]Management
Managementofinactiveandactive(withvariousdegreeofseverityisoutlinedbelowandinFigure
7.
[H2]Initiallesions
Theinitiallesion(evenwhenactive)ismanagedthroughnon-operativecareusingremineralization
therapy,involvingbehaviouralchangesandpromotionofmineralizationoverdemineralization,
typicallybyusingfluoride-containingprocucts.1Remineralizationisaimedatstoppingprogressionof
thelesionorideally,reversingit.Aspartofthemineralizationtherapy,managementshouldinvolve
reviewingthedietaryandoralhygienebehaviours(plaquecontrol)ofthepatient,followedby
educationandencouragingbehaviouralchanges86.
Fluorideisabletoincreasetherateandmagnitudeofremineralizationofinitiallesions87,88.Fluoride
canbedeliveredtopicallyeitheraspaste,gelorvarnishbyadentalprofessionalorintheformof
toothpaste,gelormouthwashathomesettings89(Box1).Theacidulatedfluoridatedproductshave
alowpH3.0-4.0.ReducingthepHofthefluoridevehiclehasbeendemonstratedinthelaboratoryto
prolongtheingressofmineralionsintothelesionbypreventingtheblockageofsuperficialenamel
pores,precentingaccesstothedeeperareasofthelesion86,90.Ideally,fullrecoveryofaninitial
carieslesionwouldbeachievedwhencalciumandphosphatearepenetratingathighenough
concentrationsinthepresenceofslightlyelevatedconcentrationsoffluoride91.Salivaisthemost
importantsourceofionsaroundteethanditsflowcanbeenhancedthroughchewingsugar-free
gums92.Fluoridateddrinkingwaterhasprovedtobeeffectivebyincreasingthelocalconcentration
ofthisioninsalivaandplaque93.Morerecently,attemptshavebeenmadetofurtherenhancethe
remineralizationpotentialbyincorporatingwater-solublebioavailablecalciumandfluorideinto
topicalproductssuchassugar-freegums,dentalcreamsandvarnishes.Theseformulationsinclude
caseinphosphopeptide-stabilizedamorphouscalciumphosphateandphosphoryloligosaccharidesof
calciumandtheirfluoridecontainingvariations94,95,96.Earlyresearchworkssuggestthatthese
formulationsmaybeneficialanti-cariogeniceffects;however,evidenceisyettobuildup.94,95,96.
Althoughanon-surgicalapproachtothemanagementofinitiallesionsappearstobethemost
beneficial,minimalinterventiontherapycanbeusedaswell.Pitandfissuresealantshavebeen
appliedusingresinbasedmaterialandglassionomercement.Anewlydevelopedresinbased
productwithsurfacepre-reactedglass-ionomerfillerisexpectedtoreleasefluoridesustainably

20
becauseofitsabilitytorechargefluorideion97.Thesefillersreleaseotherionsenhancingtooth
mineralformation98.
Whenaninitiallesionisfound,long-termmonitoringalongwithmanagingthecariesriskfactorsis
anoptiontoconsider.Asurgicalinterventioncanbeconsideredonlyiftheinitiallesionadvances99,
100,101.
[H2]Moderatelesions
Thegoalofnon-invasivemanagementofmoderatelesions(Figure7)istoarrestfurtherprogression
andregainlostminerals.Twooptionsareavailable.
[H3]Mechanical blocking. Clinical evidence shows that non-cavitated lesions on occlusal surfaces
can be arrested with resin-based fissure sealants102. Extrinsic substrates are blocked as acids
producedbythebiofilmcannotreachtheenamelandthenumberofbacteriainthecariousdentine
isreduced.Theprocedurerequiresstrictdryconditionsandthesealantsmustberegularlychecked
andmaintained. A related technology to arrest proximal lesions is resin infiltration of the dentin
layer103.Lesionslimitedtotheouterthirdofthedentinaretreatedwitharesinthatpenetratesand
repairs subsurface pores. Although long-term results are lacking, it seems clear that the micro-
invasivetreatmentsdisplaylowerlong-termcoststhaninvasivetherapy104,105.
[H3] Fluorides. Self and professionally applied fluorides can remineralise and arrest caries lesions
(Box 1). Topically applied silver diamine fluoride is a cost-effective alternative to arrest early
childhoodcariesandrootcarieslesionsinfrailelderly,especiallywhenotheroptionsareabsent106,
107.
Inthenearfuture,novelnanotechnologiesbasedonpeptidesandhydroxyapatitecrystalstogether
withbiofilmengineeringareexpectedtoadvancethenoninvasiverestorativeoptionsformoderate
carieslesions108,109.
[H2]Extensivelesions
Extensive lesions are stillmost commonly subjected to classical standard care; the demineralized
tissuesarecompletelyremovedandreplacedwithafillingmaterial.However,thedevelopmentof
adhesive techniques without need of mechanical retention (that is, composite resins or tooth-

21
coloured mixtures of plastic and glass) has allowed dentists to adopt a more tooth-preserving
approach.Yet low-qualityevidencesuggests that resincomposites lead tohigher failure ratesand
risk of secondary caries than amalgam (metal-coloured mixture of mercury and other metals)
restorations.110
Arecentdevelopmentisthestepwiseorpartialcariesremovalinwhichonlythesuperficiallayersof
the lesions are removed. Systematic reviews have concluded that this approach reduces the
incidenceofpulpexposureandfavorcariesarrestandtertiarydentinformation(thatis,layingdown
newprotectivedentine in response to an advancing caries lesion in bothprimary andpermanent
teeth)100,111.Althoughthesetechniquesshowclinicaladvantageovercompletecariesremoval, it is
tooearlytorecommendcertainclinicalstrategies.Itmustalsobeunderlinedthatthedecayedteeth
must be vital and free from symptoms. Furthermore, the success depends on an appropriate
restorationthatcompletelysealsthetoothandkeepsremainingbacteriainthedeeperdentinlayers
dormant. A disputedmode ofmanaging advanced asymptomatic lesions in primarymolars is the
Hall-technique112.Thetoothisnotpreparedintheconventionalway,butiscoveredbyapreformed
stainless steel crown with a superior clinical performance when compared with traditional
conventionalrestorativecare113.
[H2Childrenwithaveryhighcariesrisk
Topreventcariesandhavesuccessfulmanagementoforaldiseases,perinatalandinfant
oralhealthcareareessentialaspectsofearlyintervention,whichfacilitatebehavioural
changesandallowforgoodoralhealth114.Anessentialstepistostarteducatingcaregivers
andtheirhealthcareprovidersontheimportanceofdentalcareduringpregnancyand
infancy,withthedevelopmentofchild-specificoralhealthmeasuresandmethodsto
preventoraldiseases115.ThisisespeciallyimportantforchildrenwhoareathighriskofEarly
ChildhoodCaries(ECC)development.Althoughthereisnomechanisticdifferenceinthe
pathologyandprinciplesofcarebetweenECCandotherformsofcariesinchildrenor
adults,theissuesrelatedtoECChavemoretodowithspecificbehaviouralriskfactors,most
importantlynighttimebottleusewithsugarybeveragesandjuices.Althoughanatomical
differencesbetweenprimaryandpermanentteeth(suchastheenamelismuchthinnerin
primaryteethandthuscariescanprogressfasterintodentin)exist,themechanisms,
pathophysiologyandtreatmentapproachesarenotdifferentbetweenbothtypes.However,

22
clinicalmanagementfortheyoungerpatientandtheinvolvementofcarergiversbringsits
ownchallenges.
CariesManagementbyRiskAssessment(CAMBRA)isanevidence-basedapproachadaptedtothe
specificneedsofthesubsetofthechildpopulationwithECCwhoexperienceaveryaggressivecaries
challenge.115,116CAMBRAforECCassistsprovidersinastructuredmannertofirstlyassesscariesrisk
andriskonprogressionatanearlyageinapatient-centeredapproach,basedonageanddental
statusandriskfactors;secondlytailoraspecificindividualizedcareorpreventivemanagementplan,
beforedecidingonasurgicalmodality;thirdlyformaliseafollow-upplanbasedonriskandageof
thechild;andfourthlyensurespecificguidanceforthecaretakerswithtargetedself-management
goalsbasedontheage,riskandneedofeachindividualpatientatanygiventime.Thisversionof
CAMBRAprovidestheinformationtoassesstheriskofcariesdevelopmentanddiseaseprogression
inyoungchildrenaslow,moderate,orhighrisk.
Assessmentscanalsobedonethroughtheuseofthisriskassessmenttechniqueonthreespecific
domains:riskand/orbiologicalfactorssuchascontinualbottleuse,sleepingwithabottle,frequency
andtypesofsnacks,childtakinganymedicationsandsomeotherriskfactors;protectivefactorswith
questionssuchastheuseoffluoridatedtapwater,useoffluoridatedtoothpasteortheuseofxylitol
(recommendedbysomebutwithmixedevidence)onacontinuousbasis;andclinicalfindingswhere
providerscanassessthepresenceofearlydemineralizedcariesenamelsurfaces,orcavitiesatvery
earlyage,presenceofplaquebiofilm,lackofsalivaryflow,amongothers117,118.
ThroughtheseguidelinesforchildrenprovidedbyCAMBRA,earlyinterventioncanbeconductedin
primarycaresettingsbyanyqualifiedpediatrichealthcareprovider.Furthermore,providersare
recommendedtouseminimallyinvasivetreatmentssuchasfluoridevarnish119.Athome,the
caregivershouldbeguidedandsupportedtoadoptgoodoralhealthbehavioursfortheirchildren
andthemselvesandtousefluoridatedtoothpasteassoonasthefirsttoothappearswithasmall
amountnomorethanagrainofricetoprotecttheteethfromdevelopingcaries120.Ultimately,
thesepracticeswillbenefitinthepreventionandself-managementofECCandhavethepotentialto
deliverbetterpractice,improveclinicaloutcomesandreducetheoverallburdenofdiseaseinyoung
children121.
[H2]Followup/Recall

23
The final elementof continuing caries care is toestimatewhen thepatientneeds to come to the
clinic again, and this depends on the patient’s age and actual caries-risk status. It is no longer
deemed appropriate that all patients should be recalled every sixmonths. If the risk-assessment
indicateslowrisk,thenextvisitcanbepostponedmorethanoneyearforadults,moderatetohigh
risk imply that the recall should be shorter. After a suitable risk-based recall interval the caries
managementcyclestartsagain(Figure5).
[H1]Qualityoflife
Havingconsideredthescientific,clinicalandpublichealthaspectsofcariesitisimportantto
appreciatetheimpactthatthediseasehasonqualityoflifeacrossthelife-course.Thedemographic
transitiontowardsageingsocietiesandtheoralhealthtransitionwithconsiderablymorepeople
keepingtheirnaturalteethintooldagehasresultedinarelativeshiftintheburdenofuntreated
cariestowardsadults122.Cariesisstillahighlyprevalentconditionamongadults(18-65)andolder
adults(>65)122,123,124,butalsoinchildren,evenamongveryyoungchildrenaffectingtheirprimary
dentition122,125.
Toothacheisstillprevalentamongchildrenandadolescents,andisstronglyassociatedtodental
caries,particularlyamonglowersocioeconomicpositiongroupswithanestimated5-6%increasein
probabilityoftoothacheforeachadditionalprimarytoothwithcariesexperience126.Inthemost
recentnationalstudyintheUK,18%of12-year-oldsand15%of15-year-oldsreportedtoothache127.
Despitethefactthatdentalcariescanbeasymptomatic,particularlyatitsinitialstages,cariesis
associatedwithdiminishedqualityoflifeforpeopleaffectedandtheirfamilies128.Amongchildren,
cariesisassociatedwithnegativeimpactsonarangeofdailylifeactivities129,130andthiswasthe
casealsoamongveryyoungchildrenwherecarieswasassociatedwithworseoralhealthrelated
qualityoflifeintermsofperceptionsofbothchildrenandtheirparents131.Similarly,toothacheand
toothdecayaretheconditionsmostcommonlyassociatedwithworseoralhealthrelatedqualityof
lifeonadults.AmongadultsinEngland,WalesandNorthernIreland,16%reportedfrequentand
17%severeimpactsontheirdailylifeduetotheiroralconditions,buttherespectiveprevalencefor
bothfrequentandsevereoralimpactswas24%amongthosewithdecayand38%amongthosewith
experienceofseverecariesasexpressedthroughthePUFA(pulpitis,ulceration,fistulaorabscess)
index123.Globally,untreatedcariesaccountedforalmost5milliondisabilityadjustedlifeyears
(DALYs)in2010,withafurther4.5millionDALYsattributedtoexcessivetoothloss.Caries
contributedtoDALYsacrossthedifferentagesbutmoresoforchildrenandyoungandmiddle-aged
adults.Indeed,cariesarethepredominantoralhealthcauseofDALYsamongpeopleaged≤35years.

24
Ontheotherhand,extensivetoothloss,wasprevalentandanimportantcontributortoDALYs
amongmiddleagedandolderadults18.
Theimpactofdentalcariesisnotlimitedtooralsymptomsandthedetrimentalinfluenceonthe
qualityoflife.Cariesinprimarydentitionisassociatedwithmalnutrition132;childrenwithsevere
earlychildhoodcarieshaverelativelypoornutritionalhealthforarangeofnutrientscomparedto
caries-freecontrols133,134.Otherstudieshaveshownalinkbetweencariesexperienceandpoorchild
growthandlowweightgain135-138.Theevidenceonwhethertreatmentforcariesconsiderably
enhancesgrowthisinconclusive139-142andfurthermethodologicallyrobuststudieswithlonger
follow-upperiodsareneededinthatrespect.However,treatingseveredentalcariesinchildren
resultedinsignificantlyreducedtoothacheandsepsis,andimprovedsatisfactionwithteethand
smileaswellasappetitecomparedwithchildreninwhomdentalcarieswerenottreated.142Apart
fromgrowthanddevelopment,cariesalsonegativelyaffectsschooling,aschildrenwithpooreroral
healthweremorelikelytohavehigherratesofschoolabsenceandalsoperformpoorlyinschool
comparedwithchildrenwithbetteroralhealth.143,144Finally,excessivedentalcarieshasbeenlinked
withconsiderablyincreasedriskofhospitalisationandthereforealsohascostimplications.128,145
Theaforementionedimpactsofcariesdisproportionatelyaffectthemoredeprivedgroupsinthe
society123,126,127,131,146,inlinewiththeevidenceonclearsocioeconomicinequalitieswithhigherrisk
ofcarieslesionsorexperienceamongthoseinlowersocioeconomicpositions147.Thishighlightsthe
importanceoffocussingnotonlyonbehaviouralandbiologicalriskfactorsbutalsoonthebroader
socialandenvironmentaldeterminantsofthedisease148.
[H1]Outlook
Dentalcariesremainsoneofthemostprevalentglobalchronicdiseases.9,149Foratleastacentury,
dentalcarieshasbeenmanagedsurgically.Publichealthmeasures,suchaswaterfluoridationand
topicalfluorides,havehadconsiderableimpactontheburdenofdentalcariesindeveloped
countries.However,thefailuretoeradicateorhalttheburdenofthisdiseaseinmanypartsofthe
world,aswellasvulnerablepopulationgroupsindevelopedcountries,meansthatdentalcaries
remainsamajorpublichealthproblem.

25
Intheemergingeraofhealthoutcomesandvalue-basedhealthcaresystems150,thesuccessand
paymentfortheprovisionofhealthcarewillbedeterminednotonlybythetypeandnumberof
proceduresprovidedtopatientsbutalsobythefinalhealthoutcomesachieved.Managementof
dentalcariesshouldmoveforwardtoamodelwherehealthoutcomesformthebasisfor
compensationandarethefocusofdentalcare.Accordingly,themajoroutcomeofcaries
managementclinically,personallyoratacommunitylevelisthepreservationoftoothstructureand
maintenanceofteethinahealthystate(outcome1).Asecondoutcomewouldbetocontrolinitial
stagesandarresttheirprogressionorreversethecariesprocesstowardshealth(outcome2).These
twooutcomesprecedetheoutcomeofrestoringlosttoothstructureandfunctionofdecayedteeth
(outcome3),whichisthecurrentmajoroutcomethatisbeingreimbursedbythirdpartypayersor
patientsallovertheworld.Inordertoachievethesethreeoutcomes,processoutcomesmustbe
evaluatedthroughoutthecarecycleandbereimbursedaccordingly.
Dentistsandotherdentalprofessionalsmuststagethecariesprogress,assessriskfactors(onthe
dental,medical,biological,behavioural,andsociallevel),developcomprehensivemanagement
planstopreventnewcariesbasedonriskstatusofpatients,controlinitiallesions,restorecavitated
lesions,rehabilitatethedentition,anddevelopafollow-upplan54.Assessingandreimbursing
dentiststoevaluatealltheseprocessoutcomesisasimportantasreimbursingthemforachieving
thehealthoutcomesthroughproceduresbecauseitisthroughtheseoutcomesthatdentalhealthis
achieved.Thereisnodoubtthatvaluingthenewlyproposedoutcomesrepresentsarevolutionary
changeindentalcareglobally,whichasstatedbeforehassofarbeenfocusedondeliveryof
procedures.Aprocedure-focusedsystemofreimbursementisnotobsoletebutratheritmust
becomepartofalargermodelofhealthpromotingsystemofcare.Implementationofanew
paradigmindentalpracticeandeducation,asexpected,willnotbeeasyandwilltaketime.
Fortunately,thereareafewpracticalexamplesofsuccessinchangingparadigmsofcareindentistry.
Forexample,inthe1970sand1980s,aseriesofclinicaltrialscomparednon-surgicalandsurgical
periodontaltherapiesandfoundthatformostlevelsofseverityofperiodontaldiseasesboth
modalitiesproducedsimilaroutcomes151.Whiletherewasvociferousreactionfromsupportersof
thesurgicalmodalitiesofcare,theemergenceofevidenceledtoaradicalshiftovertwodecades
towardsnon-surgicalcare.Itmaybethatsimilarchangestoalessinterventionalapproachtocaries
managementcanchangepractice152.Anotherpragmaticmodelforimplementationisthe
developmentanddisseminationofguidelinesandpoliciesthatdirectdentistsintoadoptingthe
desiredbehaviours.Dentistsareusedtoadopting,thoughwithsomehesitation,standardsdictated

26
bydentalinsurancecompanies,governmentagencies,licensingboardsorhealthauthorities.The
primeexampleofthechangeinbehaviourduetopoliciesistheadoptionofinfectioncontrol
measuresandstandardsforoccupationalhealthandradiationsafety.
Otherthanthosetwopragmaticexperiences,thereisdearthofevidenceonimplementationof
changesindentalpractice153.Continuingeducationandarticlesindentaljournals,whilenecessary,
arebythemselvesinsufficientintheireffectivenesstoinfluencechangeinpracticesofpractitioners.
Thecasetosupportthisconclusionisclearintheadoptionofpit-and-fissuresealants.Although
sealantsarebasedonthesamematerialsasresincompositefillings,theiradoptionhasbeenslower
thantherapidgrowthinuseoftoothcolouredfillingmaterials154.Thereasonforthismaybe
becausewhensealantsarepromoted,basedupontheevidence155,asaprocedureofchoicefornon-
surgicalmanagementofinitialcarieslesions,theyreplaceastandardoperativeprocedurethat
dentistshaveadoptedasthenorm.Bycontrast,tooth-colouredrestorativematerialsreplaced
amalgam“silver”fillingmaterials,whichdentistsandpatientsstartedtoabandonasanormbecause
ofconcernsabouttheexposuretomercuryandaesthetics.
Itisexpectedthattheproposedintegratedcariesmanagementsystemandvalue-baseddentalcare
requireformany,butnotall,changesinthecurrentnormsofpractice.Thewaytomoveforwardin
implementationwillrequireamulti-prongedstrategy,collectiveengagementofalldentists,
educators,andpolicymakers,andresearchstudiesthatassesstheoutcomesofthenewproposed
paradigmofcariesmanagement,andrefineitasneeded.Itshouldbeappreciatedthattimescales
andtippingpointsinimplementationarenotoriouslyunpredictable.
Theburdenofdentalcariesintheworldisconsiderableintermsofcost,lossoftimefromworkand
school,insomecasesseverefacialandsystemicinfections,andrarelydeath.Hence,itisimperative
thatthenewapproachdescribedinthisPrimerisimplementednow.Acollaborationamongdental
schools,clinics,andprofessionalandgovernmentagenciesmustbeformedtocreatealearning
organizationthatshareexperiencesandassistinconductingresearchofthepreviouslydescribed
outcomes.TheinitialstepsofthisworkareunderwaywithaconsensusproductionofaGuidein
cariesmanagementforpractitionersandeducators49.Fortunately,therearetodaynewtoolsthat
canaidandempowerchangingnormsofpracticeandcollectingoutcomedata.Theuseof
computerizedreminders,electronicauditandfeedback,andstop-and-godecisionalgorithmsin
electronichealthrecords,providenewvenuestohelpinchangingpractitionerbehaviours.Auditand
feedbackhavebeenfoundtobemodestlyeffectiveinchanginghealthcarebehaviours156.

27
Incorporationofinstantaneousauditandfeedbackinelectronichealthrecordscouldprovide
reminderstopractitionerstofollowstandardsofcareduringthecareprocess.
Thetaskaheadwillbetodevelopnewtoolsandreimbursementincentivesaswellasforma
collaborationtocoordinatetheimplementationofthenewcariesmanagementsystemacrossfields.
Thecollaborationwillalsodesignandassistpartnersinconductingresearchonoutcomesofthenew
cariesmanagementsystem.Itistimenowtostarttheprocessofmovingtowardspreservingtooth
structure,ratherthanretortingitwithartificialmaterials.

28
Textboxes
Box1|Fluorideandcaries
Thebenefitsoffluorideoncariespreventionandarrestaregenerallyacceptedbydentalresearchers
andpracticingprofessionalsworldwide.Theseincludecommunity-basedmethodsoffluoride
delivery(water,milkandsaltfluoridation)andabroadrangeoffluorideagents(paste,gel,foam,
rinse,solution,varnish,drops,tablets).Theuseoffluoridesintoothpoastesiscreditedwiththe
overallglobalreductionincariesinmanycountriesoverrecentdecadesastoothbrushingwith
toothpasteissowidelyacceptedasabehaviouralnormassociatedwithbothhealthandgrooming.
Thepreventivecontributionofthefluoridetoothpasteoutweighsthatfrombrushingperse.Flossing
ispracticedtoaveryvariableextentandtheevidenceforacariespreventiveeffectislimited.
Fluoridecancomeinvariousformulationsmainlysodiumfluoride(NaF),acidulated
fluorophosphates(APF)orstannousfluoride(SnF2).Fluoridetoothpasteisthemostwidelyused
formoffluoridedeliveryworldwide.Fluoridedentifrices(fluoridecontainingpaste)haveshownin
numerousclinicaltrialstobeeffectiveanticariesagents.Thebenefitisseentobederivedfromthe
frequentlowdoseapplications.
Topicalfluorideuseathighconcentrations(>2,500ppm)providesthedrivingforcetopenetratethe
dentalbiofilmadjacenttothetoothsurface,deliveringfluoridetotoothsurfaceandmore
importantlyconcentratesitinincipientlesions.Attheselevels,fluorideisshowntodecreaserateof
enameldemineralizationandincreasedrateofenamelremineralization.Thereisalsoarelationship
betweenhigherfluorideconcentrationandprolongedretentionoffluorideintheoralcavity.High
fluoridelevelsarenecessaryfortheformationoffluoridereservoir(calciumfluoride-likedeposits)
onthetoothsurfaceandindentalplaque.Veryhighfluoridelevelscanalsohaveatransient
bactericidaleffect,butthiswouldrequirerepeatedfrequentapplicationsofprofessionallyapplied
highconcentrationfluoridewhichisnotpractical.
ReferencesBox1:87,157-163.

29
Box2|Fluoridesandcariesprevention:evidenceandcontroversialaspects.
Fluoridehasakeyandwidespreadroleincariespreventionandcontrolwhichhasbeen
demonstratedbyarangeofevidencefordecades.Theevidenceforeffectivenessfortheprotection
andtreatmentofspecificindividualsthroughfluoridetoothpastes,gelsandvarnishesisclearand
hasbeendemonstratedconvincinglyinanumberofCochraneSystematicReviews.Useoffluoridein
thiswayislargelyuncontroversial,althoughinsomecountriesenvironmentlobbieshavevoiced
concernsataphilosophicalasopposedtoascientificlevel.
Despitethelonghistoryofsuccessfuluseofwaterfluoridationasapublichealthintervention
(wheretheconcentrationoffluorideindrinkingwateriseithermaintainedormodifiedtoalevel
between0.7mg/l1.5mg/ltomaximizecariespreventionwhileminimizingtheriskofdental
fluorosis.TheWHOrecommendsthatwatervolumeconsumedandintakefromothersources
shouldbeconsideredwhensettingnationalstandards60,butthissubjecthasinsomecountriesbeen,
andinmanycountriescontinuestobe,controversial.Incountrieswherecontroversyexists,the
centralargumentisaroundthebalancebetweenpublicbenefitononehandandtheperceived
medicationofindividualswithouttheirconsentontheother.Also,ifyoungchildrenswallowtoo
muchfluorideatanageduringwhichtheirpermanentteethareforming,thereisariskofmarks
developingonthoseteeth.Thisiscalled‘dentalfluorosis’.Mostfluorosisisverymild,withfaint
whitelinesorstreaksvisibleonlytodentistsundergoodlightingintheclinic.Morenoticeable
fluorosis,whichislesscommon,maycauseaestheticconcerns.Despitethevociferousarguments
andscarestoriesaboutthedangersofwaterfluoridation,ithasbeensupportedinmanycountries
fordecadesandisstillsupportedbyawiderangeofmedical,publichealthanddentalbodies
worldwide.Thereisapaucityofrecenthighqualitystudiesofthemagnitudeofthebenefit
achievablebywaterfluoridation–whichmaynotbeashighaswasestimatedbeforethe
widespreaduseoffluorideinthedietandintoothpastesandbeforeconsiderablelifestylechanges.
However,thebenefitisstilljudgedtobesubstantialforcariesinchildren164.Therearealso
influentialcritiquesofthesystematicreviewmethodologyusedintherecentCochranereviewthat
maintainthepotentialbenefitsofusingwidereligibilitycriteriaforstudiesinsuchreviewsinorder
toachieveafullerunderstandingoftheeffectivenessofwaterfluoridation.165Alternativesatthe
communitylevelincludebothsaltandinsomeplacesmilkfluoridation;howevertheevidencefor
theseinterventionsismorelimited.

30
Box3|Protocolstoriskassessandclassifydentalcaries
Riskassessmentprotocols:forexample,CariogramandCariesManagementbyRiskAssessment
• ResearchtoolsforexampletheNyvadcriteriaforassessingcarieswithafocusonactivity.
• Epidemiologicalcaries“indices”suchas:WHOBasicMethods,InternationalCariesDetection
andAssessment(ICDAS)andtheCariesAssessmentSpectrumandTreatment(CAST)Index.
• Operativedentistrybasedclassifications:Black’sClassificationSystem(early1900s),
AmericanDentalAssociationCariesClassificationSystem(incorporatesICDAS),Mount-Hume
ClassificationSystemandSite-Stage(SI/STA)ClassificationSystem.

31
Box4|Economicassessmentsofpreventivemeasures.
Comparedtomanydiseases,healtheconomicassessmentsofcariespreventionatboththepublic
healthandindividuallevelsarescarce.Traditionalstudieshavefocussedonshorttermcomparisons
ofdifferenttypesofrestorativematerials,orcomparingafissuresealantagainstaconventional
filling,butnottakingintoaccountthelongtermscostsandconsequencesofrepeatedreplacement
ofrestorationswhenthediseaseisnotcontrolled,norpatientpreferences.Fewrobuststudies
lookingatthecostsandbenefitsofusingbehaviouralchangetechniquestomodifycariesriskorof
usinganticipatoryguidanceormodifyingoralhealthliteracyexist.Thesetopicsneedfurther
researchacrossdisciplines–asdohealtheconomicevaluationsoftheintegrateduseofpreventive
managementsystemsattheIndividual,dentalpracticeandregionallevels.Twocasereportsare
outlinedbelow.
• Theestimatedcost-effectivenessofcariespreventionprogrammesforchildreninChile
comparedtonointerventionwereevaluatedusingeconomicmodels70.Saltfluoridation,
communitywaterfluoridationandschool-basedmilkfluoridationprovidedthemostcost-savings
fromasocietalperspective,followedbyschool-basedfluoridemouthrinseprogrammes.School-
basedprogrammesusingfluoride-gelapplication,dentalsealants,andsupervisedtoothbrushing
usingfluoridetoothpastewereeffective,butdidnotyieldsocietalsavingswithinasix-yeartime
frame.Dentalsealantprogrammeswouldbecost-savingifappliedtochildrenathighcariesrisk.
• DynamicmodellingtocomparedifferentapproachesforpreventingECCinalow-income
MedicaidenrolledpopulationinNewYork71foundnetsavingsfromcommunitywater
fluoridation,motivationalinterviewingespeciallyifimplementedforcaregiversofchildren
younger≤2years,andtoothbrushingprogramswithfluoridetoothpastewithina10-yeartime
frame.Fluoridevarnishprogrammeswererecommendedfortheyoungestchildrenathighrisk,
suchasdonebypaediatricmedicalprovidersinNorthCarolina’sIntotheMouthsofBabes
Program166.

32
Figure1:Normaltoothanatomyanddevelopingdentalbiofilm.Thetooth’shardtissueconsistsof
enamel,dentinandcementum.Enamelisahardmaterialcomposedalmostexclusivelyofmineral
(mainlycomposedofhydroxyapatite[Ca10(PO4)6(OH)2])andcoversthedentineonthecrownofthe
tooth.Cementumisabonematrixlikesubstancecomposedofmineralandcollagen;itcoversthe
rootofthetooth.Thedentalpulpformsthecentralpartandcontainsconnectivetissue,blood
vesselsandnerves.Teetharecoveredbyasalivarypelliclelayerconsistingofproteinsand
glycoproteins,whichfacilitatesbindingoftheoralmicrobiotatotheteeth;thisstructureiscalledthe
dentalbiofilm(alsoknownasdentalplaque).Thebiofilmshutsoffthesurfaceenamelfromthe
salivaandoralcavityandproducesaprotectedmicro-environmentatthetoothsurface.Gums
(gingiva)surroundtheteeth.Inhumans,primaryteetheruptaround6monthsofage;theseare
graduallyreplacedbypermanentteethfromaround6yearsofage.
Figure2:Balancingpathologicalandprotectivefactorsindentalcaries.Afocusonoptimisingthe
protectivefactors(thosefavouringhealthyteeth)willpromoteremineralisationandshiftthe
dynamicbalanceofthecariesprocessinthedirectionofhealthandlesionarrest.Afailureto
mitigatetheeffectsofthepathologicalfactorswillpromotedemineralisationandshiftthedynamic
balanceinthedirectionofdiseaseinitiationanddiseaseprogression.
Figure3: Impactofdifferentdiseasedetectionthresholdsonepidemiologicalsurveys.Whichever
classificationsystemsareused inepidemiological researchondentalcaries, resultsdependonthe
detection threshold employed. The so-called icebergmetaphor for caries is illustrated graphically.
The tipof the iceberg is representedby the11%ofchildrenwithobviouscavitateddentinedecay
(whichistheWHOBasicSurveysconvention).Aslesionswithobviousvisualdecayindentine,clinical
cavitateddecayinenamelandclinicalvisualdecayinenamelareaddedtheproportionofchildren
withdentalcariesisseentoincrease12,13 ; in thisexampleto21%,25%and52%respectively14.,Dataare
based on 15 year-old children examined in the National Child Dental Health Survey (CDHS) of
England,WalesandNorthernIrelandundertakenin201314.Radiographs(iftheycanbetaken)would
revealevenmoreofthetotalicebergofdisease17.
Figure4Ecologicalplaquehypothesistoexplaintheaetiologyofdentalcaries.Theecological
plaquehypothesisdescribesthedifferencesseeninthemicrobiotafromsoundandcarioussitesasa
consequenceofachangeinoralenvironmentalconditions.Anincreasedfrequencyoffermentable
sugarintakeresultsinthebiofilmspendingmoretimeatalowpH,whichwillselectforbacteriathat

33
growpreferentiallyunderacidicconditions.Thegrowthofbacteriaassociatedwithsoundsurfacesis
thendisadvantaged,whichovertimeresultsinanincreaseintheproportionsandactivityof
cariogenicspeciesatasiteandaheightenedriskofcaries.Thisriskisraisedinindividualswith
impairedsalivaflowandsugar-richdiet,butreducedinthosewithappropriateoralhygieneand
exposuretofluoride.
Figure 5: Overview of the ICCMSä system with its four key elements. The International Caries
ClassificationandManagementSystem (ICCMS) is ahealthoutcomes focused system thataims to
maintain health and preserve tooth structure. It uses a simple form of the “ICDAS” caries
classification model to stage caries severity and assess lesion activity in order to derive an
appropriate, personalised, preventive, risk-adjusted, tooth preservingmanagement plan. The four
keystepsinthis4Dmodelare:determinepatientlevelcariesriskthroughatargetedhistory;detect
andassesscarieslesionseverityandactivity;decideonapersonalisedcariescareplanwithelements
at both the whole patient and at the specific tooth levels; and then do the appropriate tooth-
preserving and patient level caries prevention and control interventions. The cycle then re-starts
afterarisk-basedfollow-upinterval.
Figure6:Clinicalandradiographicappearanceofthestagesofseverityoftoothdecay.Clinical
appearance(parta)andbitewingradiograph(partb)ofthesametooth.Examplesofsound
andExtensivecariessurfacesareshownonthebiting(orocclusal)surfaces,whichcontain
developmentaldepressionsandgrooves(pitsandfissures)thatcollectdentalbiofilmand
arecariespredilectionsites.Theinitialandmoderatestagelesionexamplesshow
approximalsurface(whereadjacentteethareincontact).Cariesalsodevelopsonthefree
smoothsurfaces(adjacenttocheeks,lipsandtongue).
Figure7:ICCMSäcariesmanagementplan.ICCMS™proposesacomprehensiveassessmentand
personalisedcariescareplanbasedonintegratedinformationderivedfromassessingboththecaries
lesionsandtheiractivityatatoothsurfacelevelaswellasthelikelihoodfornewcariesandforcaries
lesionprogression.Basedonlesionextent,activityandrisk,thepersonalisedcareisdividedinto
specificitemsforpreventingnewcariesonsoundsurfaces,providingnon-operative(thatis,non-
surgical)careforsomelesionstocontrolthecariesprocessandprovidingminimallyinvasivetooth
preservingoperative(surgical)careonlywherethisisunambiguouslyindicated.Riskreductionand
managementisalsoacontinuingfeatureofthecareplan.

34
References
1. PittsN.B.&Zero,D.T.WhitePaperonDentalCariesPreventionandManagement.FDIWorld
DentalFederationhttp://www.fdiworlddental.org/sites/default/files/media/documents/2016-
fdi_cpp-white_paper.pdf(2016).
2. Koussoulakou,D.S.,Margaritis,L.H.&Koussoulakos,S.L.Acurriculumvitaeofteeth:evolution,
generation,regeneration.IntJBiolSci5,226-43(2009).
3. Petersen.P-E.,Bourgeois,D.,Ogawa,H.,Estupinan-Day,S.&Ndiaye,C.Theglobalburdenof
oraldiseasesandriskstooralhealth.BulletinoftheWorldHealthOrganization.83,661-669
(2005).
4. Broadbent,J.M.,Thomson,W.M.&Poulton,R.Trajectorypatternsofdentalcariesexperiencein
thepermanentdentitiontothefourthdecadeoflife.J.Dent.Res.87,69–72(2008).
5. Pitts,N.etal.GlobalOralHeathInequalitiesDentalCariesTaskGroup-ResearchAgenda.Adv.
Dent.Res.23,98-200(2011).
6. AmericanAcademyofPediatricDentistry.AmericanAcademyofPediatricDentistryreference
manual2014-2015.Pediatr.Dent.,36(6referencemanual),1-140.(2014).
7. USDepartmentofHealthandHumanServices.OralHealthinAmerica:AReportoftheSurgeon
General.NationalInstituteofDentalandCraniofacialResearch.
https://www.nidcr.nih.gov/datastatistics/surgeongeneral/report/executivesummary.htm(2000).
8. Dye,B.A.etal.TrendsinpediatricdentalcariesbypovertystatusintheUS.Int.J.Paedi.Dent.
20(2),132-43(2010).
9. Dye,B.A.etal.Trendsinoralhealthstatus:UnitedStates,1988-1994and1999-2004.Vital
HealthStat.11(248),1-92(2007).
10. Dye,B.A.,Vargas,C.M.,Fryar,C.D.,Ramos-Gomez,F.,&Isman,R.Oralhealthstatusofchildren
inLosAngelesCountyandintheUnitedStates,1999-2004.CommunityDentOralEpidemiol.45,
135-144(2016)
11. Pitts,N.B.DiscoveringDentalPublicHealth:fromFishertotheFuture.CommunityDentalHealth
11,172-178(1994).
12. Topping,G.V.&Pitts,N.B.inMonographsinOralSciencevol21-Detection,Assessment,
DiagnosisandMonitoringofCaries:Clinicalvisualcariesdetection.(ed.Pitts,N.)15-41(2009).
13. Kühnisch,J.etal.OcclusalcariesdetectioninpermanentmolarsaccordingtoWHObasic
methods,ICDASIIandlaserfluorescencemeasurements.CommunityDent.OralEpidemiol.36
(6),475-84(2008).

35
14. Pitts,N.B.,Chadwick,B.&Anderson,T.Children’sDentalHealthSurvey2013Report2:DentalDiseaseandDamageinChildreninEngland,WalesandNorthernIreland.(London:Healthand
SocialCareInformationCentre,2015).
15. Patel,R.N.etal.VariabilityofMethodologiesUsedtoDetermineNationalMeanDMFTScoresfor
12-Year-OldChildreninEuropeanCountries.CommunityDentalHealth2016,33,286-291
(2016).
16. PittsN,MeloP,MartignonS,EkstrandK,IsmailA.Cariesriskassessment,diagnosisand
synthesisinthecontextofaEuropeanCoreCurriculuminCariology.Eur.J.Dent.Educ.15
(Suppl.1)23–31,(2011).
17. Agustsdottir,H.etal.Cariesprevalenceofpermanentteeth:anationalsurveyofchildrenin
IcelandusingICDAS.CommunityDent.OralEpidemiol.38,299-309(2010).
18. Marcenes,W.etal.Globalburdenoforalconditionsin1990-2010:asystematicanalysis.J.Dent.
Res.92,592-7(2013).
19. Moynihan,P.J.&Kelly,S.A.Effectoncariesofrestrictingsugarsintake:systematicreviewto
informWHOguidelines.J.Dent.Res.93,8-18(2014).
20. Sheiham,A.&James,W.P.DietandDentalCaries:ThePivotalRoleofFreeSugars
Reemphasized.J.Dent.Res.94(10),1341-7.(2015).
21. Zero,D.T.etal.Thebiology,prevention,diagnosisandtreatmentofdentalcaries:scientific
advancesintheUnitedStates.J.Am.Dent.Assoc.140Suppl1,25S-34S(2009).
22. Reisine,S.&Litt,M.Socialandpsychologicaltheoriesandtheirusefordentalpractice.Int.Dent.
J.43,279-87(1993).
23. Fejerskov,O.Conceptsofdentalcariesandtheirconsequencesforunderstandingthedisease.CommunityDent.OralEpidemiol.25,5-12(1997).
24. Selwitz,R.H.,Ismail,A.I.&Pitts,N.B.Dentalcaries.Lancet369,51-9(2007).
25. Zero,D.T.Sugars-thearchcriminal?CariesRes.38,277-85(2004).
26. Takahashi,N.Microbialecosystemintheoralcavity:metabolicdiversityinanecologicalniche
anditsrelationshipwithoraldiseases.(ed.WatanabeM,T.N.,TakadaH)(Elsevier,Oxford,
2005).
27. Zero,D.T.Dentalcariesprocess.Dent.Clin.NorthAm.43,635-64(1999).
28. tenCate,J.M.&Featherstone,J.D.Mechanisticaspectsoftheinteractionsbetweenfluorideand
dentalenamel.Crit.Rev.OralBiol.Med.2,283-96(1991).
29. Featherstone,J.D.Thecontinuumofdentalcaries--evidenceforadynamicdiseaseprocess.J.
Dent.Res.83,Spec.NoC,C39-42(2004).

36
30. Wilson,M.inMicrobialinhabitantsofhumans.Theirecologyandroleinhealthanddisease.
(CambridgeUniversityPress,Cambridge,2005).
31. Devine,D.A.,Marsh,P.D.&Meade,J.Modulationofhostresponsesbyoralcommensalbacteria.
J.OralMicrobiol.7,26941(2015).
32. Nobbs,A.H.,Jenkinson,H.F.&Jakubovics,N.S.Sticktoyourgums:mechanismsoforalmicrobial
adherence.J.Dent.Res.90,1271-8(2011).
33. Zijnge,V.etal.Oralbiofilmarchitectureonnaturalteeth.PLoSOne5,e9321(2010).
34. Wright,C.J.etal.Microbialinteractionsinbuildingofcommunities.Mol.OralMicrobiol.28,83-
101(2013).
35. Scannapieco,F.A.Saliva-bacteriuminteractionsinoralmicrobialecology.Crit.Rev.OralBiol.
Med.5,203-48(1994).
36. Hara,A.T.&Zero,D.T.Thecariesenvironment:saliva,pellicle,diet,andhardtissue
ultrastructure.Dent.Clin.NorthAm.54,455-67(2010).
37. Jakubovics,N.S.,Yassin,S.A.&Rickard,A.H.Communityinteractionsoforalstreptococci.Adv.
Appl.Microbiol.87,43-110(2014).
38. Klein,M.I.,Hwang,G.,Santos,P.H.,Campanella,O.H.&Koo,H.Streptococcusmutans-derived
extracellularmatrixincariogenicoralbiofilms.Front.Cell.Infect.Microbiol.5,10(2015).
39. Sheiham,A.&James,W.P.Areappraisalofthequantitativerelationshipbetweensugarintake
anddentalcaries:theneedfornewcriteriafordevelopinggoalsforsugarintake.BMCPublic
Health14,863(2014).
40. Loesche,W.J.RoleofStreptococcusmutansinhumandentaldecay.MicrobiologicalReviews50,
353-380(1986).
41. Rosier,B.T.,DeJager,M.,Zaura,E.&Krom,B.P.Historicalandcontemporaryhypothesesonthe
developmentoforaldiseases:arewethereyet?Front.Cell.Infect.Microbiol.4,92(2014).
42. Marsh,P.D.Aredentaldiseasesexamplesofecologicalcatastrophes?Microbiology149,279-294
(2003).
43. Takahashi,N.&Nyvad,B.Cariesecologyrevisited:microbialdynamicsandthecariesprocess.
CariesRes.42,409-18(2008).
44. Hong,L.,Levy,S.M.,Warren,J.J.&Broffitt,B.Associationbetweenenamelhypoplasiaand
dentalcariesinprimarysecondmolars:acohortstudy.CariesRes.43,345-53(2009).
45. Fisher,J.&Glick,M.FDIWorldDentalFederationScienceCommittee(2012).Anewmodelfor
cariesclassificationandmanagement:theFDIWorldDentalFederationcariesmatrix.J.Am.
Dent.Assoc.143(6):546–551(2012).
37
46. Ismail,A.etal.Cariesmanagementpathwayspreservedentaltissuesandpromoteoralhealth.
CommunityDentOralEpidemiol.41,e12–e40(2013).
47. Pitts,N.B.&Ekstrand,K.R.InternationalCariesDetectionandAssessmentSystem(ICDAS)andits
InternationalCariesClassificationandManagementSystem(ICCMS)-methodsforstagingofthe
cariesprocessandenablingdentiststomanagecaries.CommunityDent.OralEpidemiol.41,
e41-e52(2013).
48. ICDASFoundation.InternationalCariesDetectionandAssessmentSystem(ICDAS).Whatis
ICDAS.https://www.icdas.org/what-is-icdas(2017).
49. Pitts,N.B.etal.ICCMS™GuideforPractitionersandEducators.ICDASFoundation
https://www.icdas.org/uploads/ICCMS-Guide_Full_Guide_With_Appendices_UK.pdf(2014).
50. Ismail,A.,Pitts,N.B.&Tellez,M.Theinternationalcariesclassificationandmanagementsystem
(ICCMSTM)anexampleofacariesmanagementpathway.BMCOralHealth15,1.3Suppl.1
(2015).
51. Watt,R.G.Socialdeterminantsoforalhealthinequalities:implicationsforaction.Community
Dent.OralEpidemiol.40,Suppl2:44-8(2012).
52. Jürgensen,N.&Petersen,P.E.Promotingoralhealthofchildrenthroughschools--resultsfroma
WHOglobalsurvey.CommunityDent.Health30,204-18(2013).
53. WHOWorldHealthOrganization.Oralhealth:actionplanforpromotionandintegrateddisease
prevention.WHOIRIShttp://apps.who.int/iris/bitstream/10665/21909/1/b120_10-en.pdf
(2006).
54. Weintraub,J.A.Sustainableoralhealthinterventions.J.PublicHealthDent.71,Suppl1:S95-96
(2011).
55. Panagakos,F.Partnersinprevention:Awinningapproachforcommunitiesandcompanies.J.
Evid.BaseDent.Pract.12,58-61(2012).
56. AllianceforaCavity-FreeFuture.Aboutus.TakeacloserlookattheAlliance.TheAllianceforaCavity-FreeFuture(ACFF),www.allianceforacavityfreefuture.org/en/us/about-us(2016).
57. GuidetoCommunityPreventiveServices.DentalCaries(Cavities):CommunityWater
Fluoridation.TheCommunityGuidewww.thecommunityguide.org/oral/fluoridation.html(2013).
58. USDHHSfederalpaneloncommunitywaterfluoridation.U.S.PublicHealthService
Recommendationforfluorideconcentrationindrinkingwaterforthepreventionofdental
caries.PublicHealthReports.130,1-14(2015).
59. Griffin,S.O.,Jones,K.&Tomar,S.L.Aneconomicevaluationofcommunitywaterfluoridation.J
PublicHealthDent.61,78-86(2001).
38
60. WHOWorldHealthOrganization.Guidelinesfordrinking-waterquality,4thed.42.(World
HealthOrganization,Geneva,2011).
61. Pollick,H.F.Saltfluoridation:areview.C.D.A.J.41,395-404(2013).
62. Marthaler,T.M.Saltfluoridationandoralhealth.Acta.Med.Acad.42,140-155(2013).
63. Bánóczy,J.,Rugg-Gunn,A.&Woodward.M.Milkfluoridationforthepreventionofdentalcaries.
ActaMedAcad.42,156-167(2013).
64. Yeung,C.A.,Chong,L.Y.&Glenny,A.M.Fluoridatedmilkforpreventingdentalcaries.Cochrane
DatabaseSyst.Rev.3(9),CD003876(2015).
65. Wright,J.T.etal.Evidence-basedclinicalpracticeguidelinefortheuseofpit-and-fissure
sealants.AreportoftheAmericanDentalAssociationandtheAmericanAcademyofPediatric
Dentistry.J.Am.Dent.Assoc.147,672-682(2016).
66. GuidetoCommunityPreventiveServices.DentalCaries(Cavities):School-BasedDentalSealant
DeliveryPrograms.TheCommunityGuide
www.thecommunityguide.org/oral/schoolsealants.html(2013).
67. Griffin,S.O.etal.CentersforDiseaseControlandPrevention(CDC).UseofdentalcareandeffectivepreventiveservicesinpreventingtoothdecayamongU.S.Childrenandadolescents--
MedicalExpenditurePanelSurvey,UnitedStates,2003-2009andNationalHealthandNutrition
ExaminationSurvey,UnitedStates,2005-2010.MMWRSurveill.Summ.63,Suppl2,54-60
(2014).
68. Siegal,M.D.&Detty,A.M.Doschool-baseddentalsealantprogramsreachhigherriskchildren?
J.PublicHealthDent.70,181-7(2010).
69. Weintraub,J.A.,StearnsS.C.,Rozier,R.G.&Huang,C.C.Treatmentoutcomesandcostsofdental
sealantsamongchildrenenrolledinMedicaid.AmJPublicHealth.91,1877-1881(2001).
70. Mariño,R.,Fajardo,J.&Morgan,M.Cost-effectivenessmodelsfordentalcariesprevention
programmesamongChileanschoolchildren.CommunityDent.Health29,302-8(2012).
71. Edelstein,B.L.,Hirsch,G.,FroshM.&Kumar,J.ReducingearlychildhoodcariesinaMedicaid
population:asystemsmodelanalysis.J.Am.Dent.Assoc.146,224-32(2015).
72. PublicHealthEngland.Deliveringbetteroralhealth:anevidence-basedtoolkitforprevention-Thirdedition.(PublicHealthEngland,London,2014).
73. SIGNScottishIntercollegiateGuidelinesNetwork(SIGN).SIGN138Dentalinterventionstopreventcariesinchildren(HealthcareImprovementScotland,2015).
74. Weyant,R.J.etal.,Topicalfluorideforcariesprevention:executivesummaryoftheupdated
clinicalrecommendationsandsupportingsystematicreview.J.Am.Dent.Assoc.144(11):1279–
1291(2013).
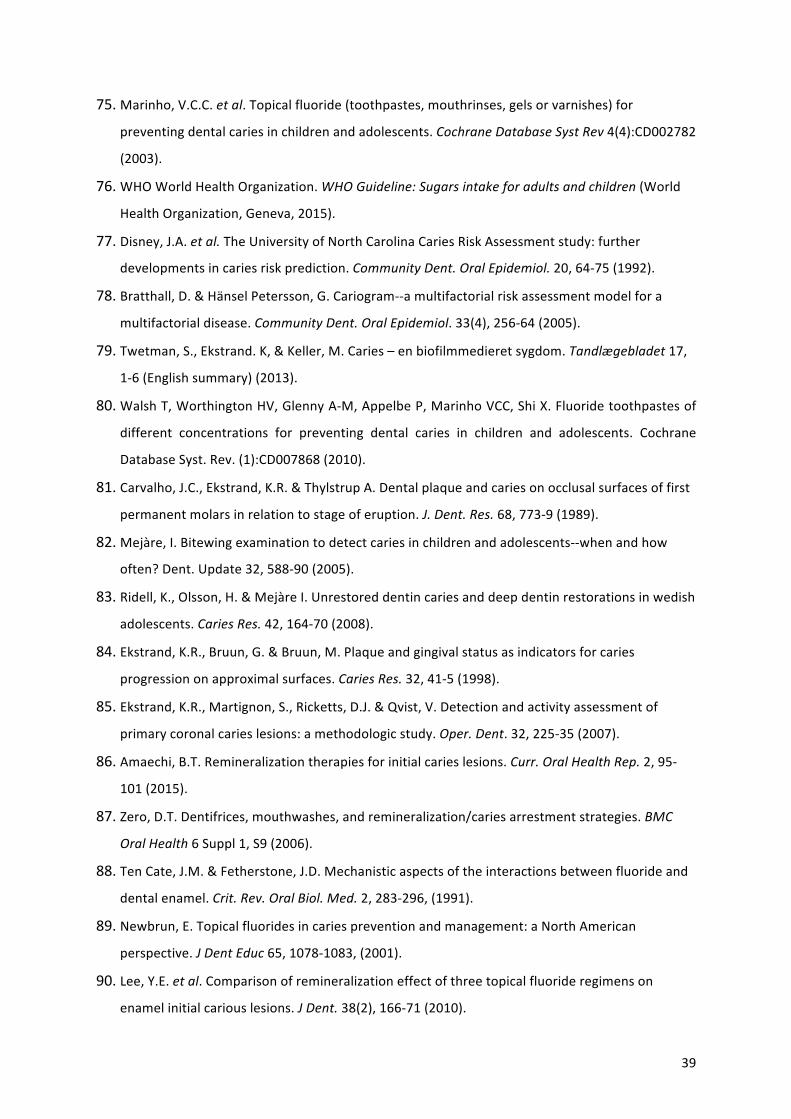
39
75. Marinho,V.C.C.etal.Topicalfluoride(toothpastes,mouthrinses,gelsorvarnishes)for
preventingdentalcariesinchildrenandadolescents.CochraneDatabaseSystRev4(4):CD002782
(2003).
76. WHOWorldHealthOrganization.WHOGuideline:Sugarsintakeforadultsandchildren(World
HealthOrganization,Geneva,2015).
77. Disney,J.A.etal.TheUniversityofNorthCarolinaCariesRiskAssessmentstudy:further
developmentsincariesriskprediction.CommunityDent.OralEpidemiol.20,64-75(1992).
78. Bratthall,D.&HänselPetersson,G.Cariogram--amultifactorialriskassessmentmodelfora
multifactorialdisease.CommunityDent.OralEpidemiol.33(4),256-64(2005).
79. Twetman,S.,Ekstrand.K,&Keller,M.Caries–enbiofilmmedieretsygdom.Tandlægebladet17,
1-6(Englishsummary)(2013).
80. WalshT,WorthingtonHV,GlennyA-M,AppelbeP,MarinhoVCC,ShiX.Fluoridetoothpastesof
different concentrations for preventing dental caries in children and adolescents. Cochrane
DatabaseSyst.Rev.(1):CD007868(2010).
81. Carvalho,J.C.,Ekstrand,K.R.&ThylstrupA.Dentalplaqueandcariesonocclusalsurfacesoffirstpermanentmolarsinrelationtostageoferuption.J.Dent.Res.68,773-9(1989).
82. Mejàre,I.Bitewingexaminationtodetectcariesinchildrenandadolescents--whenandhow
often?Dent.Update32,588-90(2005).
83. Ridell,K.,Olsson,H.&MejàreI.Unrestoreddentincariesanddeepdentinrestorationsinwedish
adolescents.CariesRes.42,164-70(2008).
84. Ekstrand,K.R.,Bruun,G.&Bruun,M.Plaqueandgingivalstatusasindicatorsforcaries
progressiononapproximalsurfaces.CariesRes.32,41-5(1998).
85. Ekstrand,K.R.,Martignon,S.,Ricketts,D.J.&Qvist,V.Detectionandactivityassessmentof
primarycoronalcarieslesions:amethodologicstudy.Oper.Dent.32,225-35(2007).
86. Amaechi,B.T.Remineralizationtherapiesforinitialcarieslesions.Curr.OralHealthRep.2,95-
101(2015).
87. Zero,D.T.Dentifrices,mouthwashes,andremineralization/cariesarrestmentstrategies.BMC
OralHealth6Suppl1,S9(2006).
88. TenCate,J.M.&Fetherstone,J.D.Mechanisticaspectsoftheinteractionsbetweenfluorideand
dentalenamel.Crit.Rev.OralBiol.Med.2,283-296,(1991).
89. Newbrun,E.Topicalfluoridesincariespreventionandmanagement:aNorthAmerican
perspective.JDentEduc65,1078-1083,(2001).
90. Lee,Y.E.etal.Comparisonofremineralizationeffectofthreetopicalfluorideregimenson
enamelinitialcariouslesions.JDent.38(2),166-71(2010).

40
91. Amaechi,B.T.&vanLoveren,C.Fluoridesandnon-fluorideremineralizationsystems.Monogr.
OralSci.23,15-26(2013).
92. Kandelman,D.&Gagnon,G.A24-monthclinicalstudyoftheincidenceandprogressionof
dentalcariesinrelationtoconsumptionofchewinggumcontainingxylitolinschoolpreventive
programs.J.Dent.Res.69,1771-1775(1990).
93. Featherstone,J.D.Preventionandreversalofdentalcaries:roleoflowlevelfluoride.Community
Dent.OralEpidemiol.27,31-40(1999).
94. Reynolds,E.C.,Cai,F.,Shen,P.&Walker,G.D.Retentioninplaqueandremineralizationof
enamellesionsbyvariousformsofcalciuminamouthrinseorsugar-freechewinggum.J.Dent.
Res.82,206-211(2003).
95. Kitasako,Y.,Sadr,A.,Hamba,H.,Ikeda,M.&TagamiJ.Gumcontainingcalciumfluoride
reinforcesenamelsubsurfacelesionsinsitu.J.Den.Res.91,370-375(2012).
96. Hamba,H.,Nikaido,T.,Inoue,G.,Sadr,A.&Tagami,J.EffectsofCPP-ACPwithsodiumfluoride
oninhibitionofbovineenameldemineralization:aquantitativeassessmentusingmicro-
computedtomography.J.Dent.39,405-13(2011).
97. Tay,F.R.etal.Theglass-ionomerphaseinpresin-basedrestorativematerials,J.Dent.Res.80,
1808-1812,(2001).
98. Ito,S.etal.Effectsofsurfacepre-reactedglass-ionomerfillersonmineralinductionby
phosphoprotein.J.Dent.39,72–9(2011).
99. Holmgren,C.,Gaucher,N.,Decerle,N.&Doméjean,S.MinimalinterventiondentistryII:part3.
Managementofnon-cavitated(initial)occlusalcarieslesions–non-invasiveapproachesthrough
remineralizationandtherapeuticsealants.Br.Dent.J.216,237-243(2014).
100. Ricketts,D.,Lamont,T.,Innes,N.P.,Kidd,E.&Clarkson,J.E.Operativecariesmanagementin
adultsandchildren.CochraneDatabaseSyst.Rev.3:CD003808(2013).
101. Kidd,E.,&Fejerskov,O.Changingconceptsincariology:fortyyearson.DentalUpdate40(4),277-286(2013).
102. Zandona,A.F.&Swift,E.J.Jr.Criticalappraisal.Evidenceforsealingversusrestorationofearlycarieslesions.J.Esthet.Restor.Dent.27(1),55-8(2015).
103. Meyer-Lueckel,H.,Bitter,K.&Paris,S.Randomizedcontrolledclinicaltrialonproximalcaries
infiltration:three-yearfollow-up.CariesRes.46,544-8(2012).
104. Schwendicke,F.,Meyer-Lueckel,H.,Stolpe,M.,Dörfer,C.E.&Paris,S.Costsandeffectivenessof
treatmentalternativesforproximalcarieslesions.PLoSOne.27,9(1):e86992(2014).
105. Schwendicke,F.,Stolpe,M.,Meyer-Lueckel,H.&Paris,S.Detectingandtreatingocclusalcaries
lesions:acost-effectivenessanalysis.J.Dent.Res.94,272-80(2015).

41
106. Wierichs,R.J.&Meyer-Lueckel,H.Systematicreviewonnoninvasivetreatmentofrootcaries
lesions.J.Dent.Res.94,261-71(2015).
107. Duangthip,D.,Jiang,M.,Chu,C.H.&LoE.C.Non-surgicaltreatmentofdentincariesinpreschool
children-systematicreview.BMCOralHealth,15:44(2015).
108. Clarkson,B.H.&Exterkate,R.A.M.Noninvasivedentistry:Adreamorreality?CariesRes.
49(suppl1),11-17(2015).
109. Marsh,P.D.,Head,D.A.&Devine,D.A.Prospectsoforaldiseasecontrolinthefuture-an
opinion.J.OralMicrobiol.6,261-76(2014).
110. RasinesAlcaraz,M.G.etal.Directcompositeresinfillingsversusamalgamfillingsforpermanent
oradultposteriorteeth.CochraneDatabaseSyst.Rev.31,3:CD005620(2014).
111. Ferreira,J.M.,Pinheiro,S.L.,Sampaio,F.C.&deMenezes,V.A.Cariesremovalinprimaryteeth--a
systematicreview.QuintessenceInt.43,e9-15(2012).
112. Innes,N.P.,Evans,D.J.&Stirrups,D.R.TheHallTechnique;arandomizedcontrolledclinicaltrial
ofanovelmethodofmanagingcariousprimarymolarsingeneraldentalpractice:acceptability
ofthetechniqueandoutcomesat23months.BMCOralHealth7:18(2007).
113. Seale,N.S.&Randall,R.Theuseofstainlesssteelcrowns:asystematicliteraturereview.Pediatr
Dent.37,145-60(2015).
114. Gajendra,S.&Kuma,J.V.,Oralhealthandpregnancy:areview.N.Y.StateDent.J.70(1),40-4,
_2004).
115. AAPDCouncilonClinicalAffairs.GuidelineonCaries-riskAssessmentandManagementfor
Infants,ChildrenandAdolescents.(AmericanAcademyofPediatricDentistry,CouncilonClinical
Affairs;2013).
116. Ramos-Gomez,F.J.Amodelforcommunity-basedpediatricoralhealth:implementationofan
infantoralcareprogram.Int.J.Dent.156821(2014).
117. Ramos-Gomez,F.&Ng,M.W.Intothefuture:keepinghealthyteethcariesfree:pediatric
CAMBRAprotocols.J.Calif.Dent.Assoc.39(10),723-33(2011).
118. InstituteofMedicine.OralHealthLiteracy.RoundtableonHealthLiteracy;BoardonPopulation
HealthandPublicHealthPractice(NationalAcademiesPress,WashingtonDC.2003).
119. Karlinsey,R.L.&Pfarrer,A.M.FluoridePlusFunctionalizedβ-TCP:APromisingCombinationfor
RobustRemineralization.(ed.tenCate,J.M.)AdvancesinDentalResearch.24(2),48-52(2012).
120. ADAReport.Fluoridetoothpasteuseforyoungchildren.TheJournaloftheAmericanDental
Association,145(2),190-191(2014).
121. Ramos-Gomez,F.&Ng,M-W.IntotheFuture:KeepingHealthyTeethCariesFree:Pediatric
CAMBRAProtocols.JournaloftheCaliforniaDentalAssociation39(10),723-733(2011).
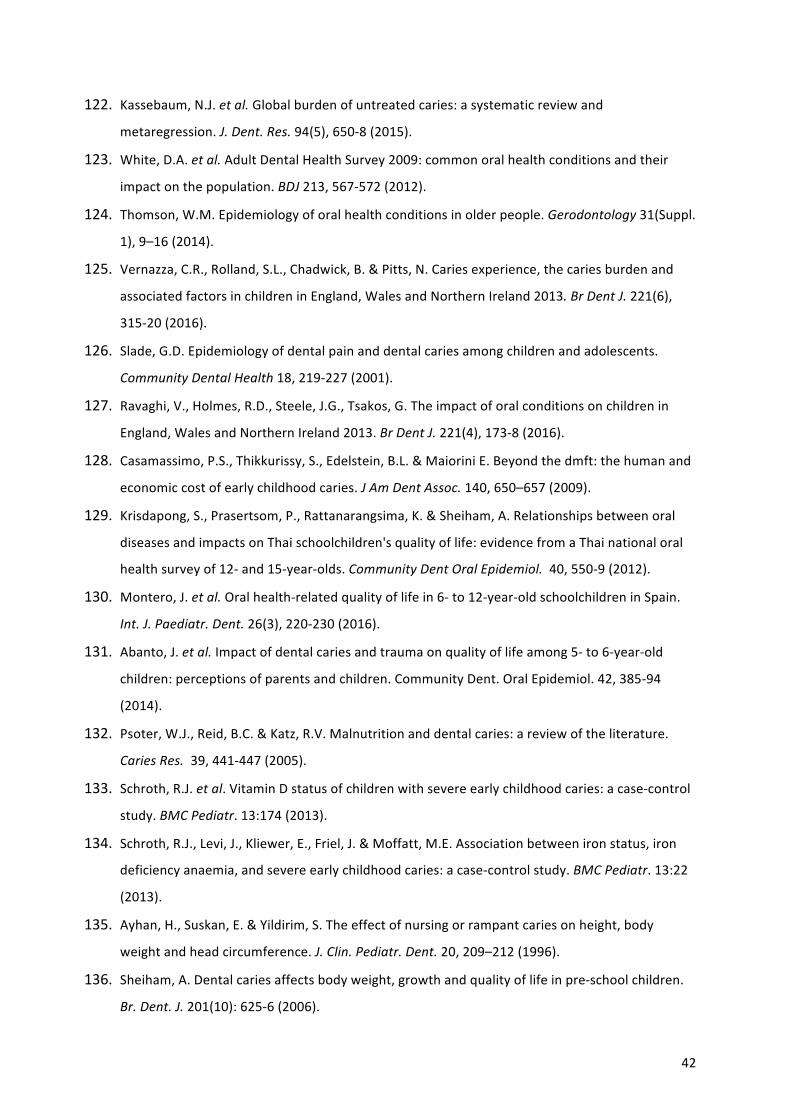
42
122. Kassebaum,N.J.etal.Globalburdenofuntreatedcaries:asystematicreviewand
metaregression.J.Dent.Res.94(5),650-8(2015).
123. White,D.A.etal.AdultDentalHealthSurvey2009:commonoralhealthconditionsandtheir
impactonthepopulation.BDJ213,567-572(2012).
124. Thomson,W.M.Epidemiologyoforalhealthconditionsinolderpeople.Gerodontology31(Suppl.
1),9–16(2014).
125. Vernazza,C.R.,Rolland,S.L.,Chadwick,B.&Pitts,N.Cariesexperience,thecariesburdenandassociatedfactorsinchildreninEngland,WalesandNorthernIreland2013.BrDentJ.221(6),
315-20(2016).
126. Slade,G.D.Epidemiologyofdentalpainanddentalcariesamongchildrenandadolescents.
CommunityDentalHealth18,219-227(2001).
127. Ravaghi,V.,Holmes,R.D.,Steele,J.G.,Tsakos,G.Theimpactoforalconditionsonchildrenin
England,WalesandNorthernIreland2013.BrDentJ.221(4),173-8(2016).
128. Casamassimo,P.S.,Thikkurissy,S.,Edelstein,B.L.&MaioriniE.Beyondthedmft:thehumanand
economiccostofearlychildhoodcaries.JAmDentAssoc.140,650–657(2009).
129. Krisdapong,S.,Prasertsom,P.,Rattanarangsima,K.&Sheiham,A.Relationshipsbetweenoral
diseasesandimpactsonThaischoolchildren'squalityoflife:evidencefromaThainationaloral
healthsurveyof12-and15-year-olds.CommunityDentOralEpidemiol.40,550-9(2012).
130. Montero,J.etal.Oralhealth-relatedqualityoflifein6-to12-year-oldschoolchildreninSpain.
Int.J.Paediatr.Dent.26(3),220-230(2016).
131. Abanto,J.etal.Impactofdentalcariesandtraumaonqualityoflifeamong5-to6-year-old
children:perceptionsofparentsandchildren.CommunityDent.OralEpidemiol.42,385-94
(2014).
132. Psoter,W.J.,Reid,B.C.&Katz,R.V.Malnutritionanddentalcaries:areviewoftheliterature.
CariesRes.39,441-447(2005).
133. Schroth,R.J.etal.VitaminDstatusofchildrenwithsevereearlychildhoodcaries:acase-control
study.BMCPediatr.13:174(2013).
134. Schroth,R.J.,Levi,J.,Kliewer,E.,Friel,J.&Moffatt,M.E.Associationbetweenironstatus,iron
deficiencyanaemia,andsevereearlychildhoodcaries:acase-controlstudy.BMCPediatr.13:22
(2013).
135. Ayhan,H.,Suskan,E.&Yildirim,S.Theeffectofnursingorrampantcariesonheight,body
weightandheadcircumference.J.Clin.Pediatr.Dent.20,209–212(1996).
136. Sheiham,A.Dentalcariesaffectsbodyweight,growthandqualityoflifeinpre-schoolchildren.
Br.Dent.J.201(10):625-6(2006).

43
137. Oliveira,L.B,Sheiham,A.&BöneckerM.Exploringtheassociationofdentalcarieswithsocial
factorsandnutritionalstatusinBrazilianpreschoolchildren.EurJOralSci116:37–43(2008).
138. Alkarimi,H.A.,Watt,R.G.,Pikhart,H.,Sheiham,A.&Tsakos,G.Dentalcariesandgrowthin
school-agechildren.Pediatrics.133:e616-23(2014).
139. Acs,G.,Shulman,R.,Ng,M.W.&Chussid,S.Theeffectofdentalrehabilitationonthebody
weightofchildrenwithearlychildhoodcaries.Pediatr.Dent.21:109–113(1999).
140. MalekMohammadi,T.,Wright,C.M.&Kay,E.J.Childhoodgrowthanddentalcaries.Community
DentHealth26,38–42(2009).
141. Gemert-Schriks,M.C.M.etal.Theinfluenceofdentalcariesonbodygrowthinprepubertal
children.ClinicalOralInvestigations15,141-149(2010).
142. Alkarimi,H.A.,etal.Impactoftreatingdentalcariesonschoolchildren'santhropometric,dental,
satisfactionandappetiteoutcomes:arandomizedcontrolledtrial.BMCPublicHealth.12,706
(2012).
143. Jackson,S.L.,Vann,W.F.Jr.,Kotch,J.B.,Pahel,B.T.&Lee,J.Y.Impactofpoororalhealthon
children'sschoolattendanceandperformance.Am.J.PublicHealth.101,1900–1906(2011).
144. Krisdapong,S.,Prasertsom,P.,Rattanarangsima,K.&Sheiham,A.Schoolabsencedueto
toothacheassociatedwithsociodemographicfactors,dentalcariesstatus,andoralhealth-
relatedqualityoflifein12-and15-year-oldThaichildren.J.PublicHealthDent.73(4),321-8
(2013).
145. Griffin,S.O.,Gooch,B.F.,Beltrán,E.,Sutherland,J.N.&Barsley,R.Dentalservices,costs,andfactorsassociatedwithhospitalizationforMedicaid-eligiblechildren,Louisiana1996-97.J.Public
HealthDent.60,21–27(2000).
146. Moles,D.Epidemicofdentalabscesses?Dentalabscesseshaveincreasedmostamongpoorer
people.B.M.J.336,1323(2008).
147. Schwendicke,F.etal.Socioeconomicinequalityandcaries:asystematicreviewandmeta-
analysis.JDentRes.94,10-8(2015).
148. Fisher-Owens,S.A.etal.Influencesonchildren'soralhealth:aconceptualmodel.Pediatrics.
120,e510-20(2007).
149. Bagramian,R.A.,Garcia-D-Gody,F.&Volpe,R.A.AmJDent.22,3-8(2009).
150. Porter,M.E.NewEngJMed.36,109-112(2009).
151. Kaldahl,W.B.,Kalkwarf,K.L.&Patil,K.D.AreviewofLongitudinalStudiesthatcompared
PeriodontalTherapies.JPeriodontol.64,243-253(1993).
152. Innes,N.&Evans,D.Associationbetweenparentalguiltandoralhealthproblemsinpreschool
children.BrDentJ.206,549-50(2009).

44
153. Eccles,M.P.etal.Developingclinicalpracticeguidelines:targetaudiences,identifyingtopicsfor
guidelines,guidelinegroupcompositionandfunctioningandconflictsofinterest.
ImplementationScience,7,60(2012).
154. Tellez,M.Gray,S.L,Gray,S.,Lim,S.&Ismail,A.I.Sealantsanddentalcaries:dentists'
perspectivesonevidence-basedrecommendations.JADA,142,1033-40(2011).
155. Beauchamp,J.etal.Evidence-basedclinicalrecommendationsfortheuseofpit-and-fissure
sealants:areportoftheAmericanDentalAssociationCouncilonScientificAffairs.Dent.Clin.
NorthAm.53(1),131-47(2009).
156. Phelan,M.P.etal..Amultifacetedinterventiontoimproveelectronichealthrecord(EHR)
nursingdocumentationforemergencydepartmentblooddraws.AcademicEmergencyMedicine,
22(5SUPPL.1),S322(2015).
157. Fejerskov,O.,Thylstrup,A.&Larsen,M.J.Rationaluseoffluoridesincariesprevention.A
conceptbasedonpossiblecariostaticmechanisms.ActaOdontol.Scand.39(4),241–249(1981).
158. FluorideRecommendationsWorkGroup.Recommendationsforusingfluoridetopreventand
controldentalcariesintheUnitedStates.CentersforDiseaseControlandPreventionMMWR
https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5014a1.htm(2001).
159. Hellwig,E.&Lennon,A.´M.SystemicversusTopicalFluoride.CariesRes.38,258–262(2004).
160. Margolis,H.C.,Moreno,E.C.&Murphy,B.J.Effectoflowlevelsoffluorideinsolutiononenamel
demineralisationinvitro.J.Dent.Res.65,23-29(1986).
161. Marinho,V.C.,Higgins,J.P.,Logan,S.&Sheiham,A.Topicalfluoride(toothpastes,mouthrinses,
gelsorvarnishes)forpreventingdentalcariesinchildrenandadolescents.CochraneDatabase
Syst.Rev.4:CD002782(2003).
162. tenCate,J.M.Currentconceptsonthetheoriesofthemechanismofactionoffluoride.Acta
Odontol.Scand.57(6),325-329(1999).
163. tenCate,J.M.&Featherstone,J.D.Mechanisticaspectsoftheinteractionsbetweenfluorideand
dentalenamel.CRCCrit.Rev.OralBiol.Med.2,283-296(1991).
164. Iheozor-Ejiofor,Z.,etal.Waterfluoridationforthepreventionofdentalcaries.Cochrane
DatabaseofSystematicReviewsIssue6,CD010856(2015).
165. Rugg-Gunn,A.J.etal.Critiqueofthereviewof'Waterfluoridationforthepreventionofdental
caries'publishedbytheCochraneCollaborationin2015.BritishDentalJournal220,335-340
(2016).
166. Pahel,B.T.,Rozier,R.G.,Stearns,S.C.&Quiñonez,R.B.EffectivenessofpreventivedentaltreatmentsbyphysiciansforyoungMedicaidenrollees.Pediatrics127,e682-e689(2011).
Author notesPlease check these figures carefully and return any comments/amendments that you might have to me as soon as possible. In particular, we would like you to check the following: • Do the figures convey the intended message?• Are all the labels accurate and in the right place?• Are all the arrows in the right place?• Are any chemical structures correct?• Have shapes and colours been used consistently and accurately throughout the figures?• Have any of the figures been previously published, or have they been supplied by a colleague(s)
who is not a named author on the article?
To mark up any corrections, please use the commenting tools in the PDF, or print and draw by hand, rather than directly editing the PDFs.
Fig 1
Nature Reviews | Disease Primers
Manuscript number NNRDP_15_048 Pitts 15|3|17
Nature Reviews | Disease Primers
Root
CrownEnamel
Dentine
Pulp chamber
Gum
Bone
Peridontal ligament
Cementum
Root canal
Nerves andblood vessels
Enamel Pellicle
Bacteria
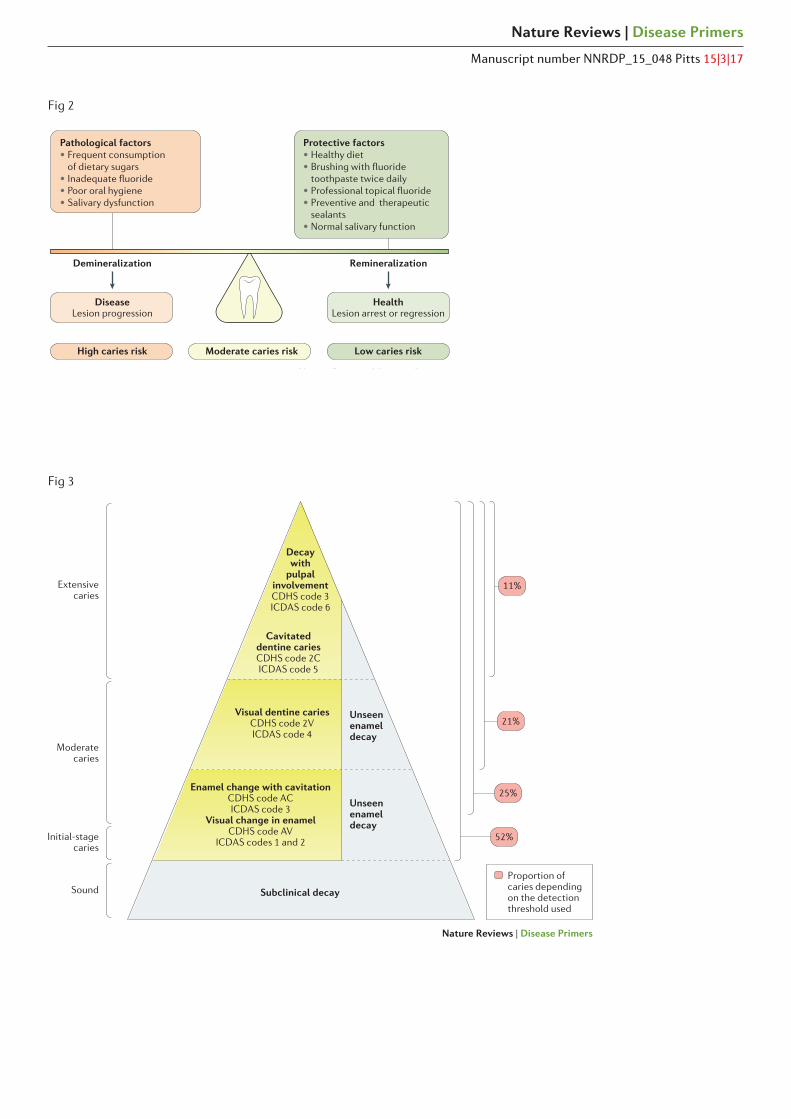
Fig 3
Fig 2
Nature Reviews | Disease Primers
Manuscript number NNRDP_15_048 Pitts 15|3|17
Nature Reviews | Disease Primers
Pathological factors• Frequent consumption of dietary sugars• nade uate uoride• Poor oral hygiene• Salivary dysfunction
Protective factors• Healthy diet• rushing with uoride toothpaste twice daily• rofessional topical uoride• Preventive and therapeutic sealants • Normal salivary function
Demineralization Remineralization
High caries risk Low caries riskModerate caries risk
DiseaseLesion progression
HealthLesion arrest or regression
Nature Reviews | Disease Primers
Decaywith
pulpalinvolvementCDHS code 3ICDAS code 6
Cavitateddentine cariesCDHS code 2CICDAS code 5
Visual dentine cariesCDHS code 2VICDAS code 4
Enamel change with cavitationCDHS code ACICDAS code 3
Visual change in enamelCDHS code AV
ICDAS codes 1 and 2
Subclinical decay
Unseenenameldecay
Unseenenameldecay
11%
21%
25%
52%
Proportion ofcaries depending on the detectionthreshold used
Sound
Moderatecaries
Extensivecaries
Initial-stagecaries

Fig 4
Fig 5
Nature Reviews | Disease Primers
Manuscript number NNRDP_15_048 Pitts 15|3|17
Nature Reviews | Disease Primers
Increasedsugar intake
Stress
NeutralpH
S. sanguinis,S. gordonii Health
CariesMutans streptococci,lactobacilli andbifidobacteria
Increasedlow pH
challenges
More frequent acid
production
Environmentalshift
Ecologicalshift
Disease
ral hygiene and uoride inta
e
ariogenic diet and low saliva
ow
Nature Reviews | Disease Primers
Risk-basedrecall
interval
DeterminePatient-level
caries risk (history)
DoAppropriate
tooth-preserving and patient-level caries
prevention and control (management)
ICCMS™ 4Dcaries management
Detect and assessCaries staging
and activity(classification and
intra-oral risk)
DecidePersonalised
care plan(decision making)

Fig 6
Fig 7
Nature Reviews | Disease Primers
Manuscript number NNRDP_15_048 Pitts 15|3|17
Nature Reviews | Disease Primers
Sound(ICDAS 0)
Initial lesion(ICDAS 1–2)
Moderate lesion(ICDAS 3–4)
Extensive lesion(ICDAS 5–6)
a
b
Nature Reviews | Disease Primers
High Moderate Low
Management of individual lesions
Sound(preventing new caries)
Tooth preservingoperative care of lesions
Non-operative careof lesions (control)
Extensiveactive caries
lesions
Moderateactive caries
lesions
Initialactive caries
lesions
Allinactive caries
lesions
Caries lesions and activity by tooth surface Likelihood for new caries and/or progression
ManagementPersonalised caries prevention;
control and tooth preserving operative care
Management at the patient level
Leads to, in most cases Leads to, in some cases
Risk management
Do