l features related to fetal alcohol syndrome in 5-year-old
TRANSCRIPT

Are Low-to-Moderate Average Alcohol Consumption and Isolated Episodes of Binge Drinking in Early Pregnancy Associated with Facial Features Related to Fetal Alcohol Syndrome in 5-Year-Old Children?
Ulrik Schiøler Kesmodel, Siv Steffen Nygaard, Erik Lykke Mortensen, Jacquelyn Bertrand, Clark H. Denny, Alex Glidewell, Susan Astley HemingwayDepartment of Obstetrics and Gynecology, (USK, SSN), Herlev University Hospital, Herlev, Denmark; Department of Clinical Medicine, (USK), University of Copenhagen, Copenhagen, Denmark; Center for Healthy Aging, (ELM), Institute of Public Health, University of Copenhagen, Copenhagen, Denmark; Centers for Disease Control and Prevention (CDC), (JB, CHD), Atlanta, Georgia; University of Washington, (AG), Seattle, Washington; and Departments of Epidemiology and Pediatrics, (SAH), University of Washington, Seattle, Washington.
Abstract
Background: Fetal alcohol syndrome (FAS) typically is observed among individuals with high
prenatal alcohol exposures (PAE), but exposure histories obtained in clinical diagnostic settings
are often inaccurate. The present analysis used the Lifestyle During Pregnancy Study (LDPS) to
assess the potential effects of low-to-moderate average weekly alcohol consumption and binge
drinking in early pregnancy on facial features associated with FAS among children 5 years of age.
Methods: The analysis is a prospective follow-up study of 670 women and their children
sampled from the LDPS cohort based on maternal alcohol consumption during pregnancy. The 4-
Digit Code FAS Facial Photographic Analysis Software was used to measure the magnitude of
expression of the 3 diagnostic facial features of FAS from standardized digital photographs.
Logistic regression was used to estimate the odds of presenting with the FAS/partial fetal alcohol
syndrome (PFAS) facial phenotypes relative to different patterns of prenatal alcohol exposure.
Results: Ten children presented with the FAS/PFAS facial phenotypes. None of the children
sampled met the central nervous system (CNS) criteria for FAS or PFAS at age 5 years. All
remained at risk for PFAS since some types of CNS dysfunction associated with this diagnosis
Reprint requests: Ulrik Schiøler Kesmodel, Department of Obstetrics and Gynecology, Herlev University Hospital, PhD, University of Copenhagen, Herlev Ringvej 75, Herlev, Denmark; Tel.: +45 3020 6850; [email protected].
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
CONFLICT OF INTERESTNone.
ETHICSThe LDPS was approved by the DNBC Board of Directors, the DNBC Steering Committee, the Regional Ethics Committee, the Danish Data Protection Agency, and the Institutional Review Board at the Centers for Disease Control and Prevention. Signed informed consent was obtained for the LDPS. The current analyses were approved by the DNBC Steering Committee and the Danish Data Protection Agency.
HHS Public AccessAuthor manuscriptAlcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Published in final edited form as:Alcohol Clin Exp Res. 2019 June ; 43(6): 1199–1212. doi:10.1111/acer.14047.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by CDC Stacks
may only be assessed at older ages. The FAS/PFAS facial phenotypes were 8.5-fold more likely
among children exposed to an average of 1 to 4 drinks/wk and 2.5-fold more likely among
children with a single binge exposure in gestational weeks 3 to 4 compared to children with no
such exposures. The magnitude of expression of the FAS facial phenotype was significantly
correlated with all other diagnostic features of FAS: growth deficiency, microcephaly, and
measures of CNS dysfunction.
Conclusions: These findings suggest that low-to-moderate levels of PAE or isolated binge
exposures may place some fetuses at risk for FAS/PFAS. Thus, conservative advice is still for
women to abstain from alcohol consumption during pregnancy.
Keywords
Alcohol; Alcohol Binge Drinking; Pregnancy; Fetal Alcohol Syndrome; Fetal Alcohol Spectrum Disorders
Fetal alcohol syndrome (fas) is a permanent birth defect and developmental disability caused
by in utero exposure to alcohol. FAS is characterized by growth deficiency, a unique
constellation of minor facial anomalies, and structural, neurological, or functional central
nervous system (CNS) abnormalities (Astley and Clarren, 2000; Bertrand et al., 2004;
Stratton et al., 1996). Not all individuals exposed to and damaged by prenatal alcohol
exposure have FAS, the most involved diagnosis under the umbrella of fetal alcohol
spectrum disorders (FASDs). Prenatal exposure to alcohol can also result in more subtle
adverse effects and diagnoses. The growth, facial, and CNS abnormalities can all present
along separate continua from mild to severe (Stratton et al., 1996).
A number of FASD diagnostic schemes have been posed and applied worldwide (Astley,
2004; Bertrand et al., 2004; Bower and Elliott, 2016; Cook et al., 2016; American
Psychiatric Association, 2013; Hoyme et al., 2016). All promote an interdisciplinary
approach to diagnosis and broadly agree that FASDs are characterized by growth, facial, and
CNS abnormalities. But, the specific criteria used to define each diagnosis under the
umbrella of FASDs do differ across the diagnostic systems (Astley, 2011; Astley et al., 2017;
Coles et al., 2016). It should be noted that all schemes assess facial features for an FAS
diagnosis since these features reflect anomalies in prenatal brain development. The current
analysis used criteria as outlined in Astley (2004), also known as the 4-Digit Code. Briefly,
these criteria require all of the following:
1. Growth deficiency: prenatal and/or postnatal height and/or weight at or below the
10th percentile;
2. Facial dysmorphia: all 3 of the following: (i) short palpebral fissure lengths
(PFLs; less than or equal to third percentile); (ii) smooth philtrum (Rank 4 or 5
on the University of Washington Lip-Philtrum Guide); and (iii) thin upper lip
(Rank 4 or 5 on the University of Washington Lip-Philtrum Guide);
3. Evidence of severe CNS structural, neurological, and/or functional
abnormalities;
Schiøler Kesmodel et al. Page 2
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

4. Prenatal alcohol exposure: a confirmed or unknown history of exposure. FAS can
be diagnosed in the absence of a confirmed prenatal alcohol exposure history if
the 3 facial features (as defined by the Rank 4 facial phenotypes in the 4-Digit
Code) are present. Empirical evidence confirms the Rank 4 facial phenotypes are
so highly specific to (caused only by) prenatal alcohol exposure. Its presence can
be used to confirm exposure when an exposure history is unavailable (Astley,
2013).
The FAS facial phenotype is not simply present or absent. It presents along a clinically
meaningful continuum from mild to moderate to severe (Astley and Clarren, 2000). The
magnitude of expression of the FAS facial phenotype not only increases with increasing
prenatal alcohol exposure, but also correlates significantly with increasing severity of growth
deficiency, microcephaly, and CNS dysfunction (Astley, 2013). These significant
correlations serve to validate a causal association between prenatal alcohol exposure and the
growth, facial, and CNS abnormalities currently used to define FAS (Astley, 2013; Astley
and Clarren, 2001).
FAS is typically observed among individuals with reportedly high prenatal alcohol
exposures (PAE; ≥6 drinks/d or 5 to 6 drinks within a short period of time) (O’Leary and
Bower, 2012), but exposure histories obtained in clinical diagnostic settings often are
inaccurate. For example, the average reported exposure among 154 individuals diagnosed
with FAS or partial fetal alcohol syndrome (PFAS) at the University of Washington FAS
Diagnostic & Prevention Network (FASDPN) using the 4-Digit Code was 8 to 12 drinks per
drinking occasion, 5 to 6 days per week (Astley, 2010). This average exposure pattern,
however, spanned a wide range. At the low end of the range, 1 of every 14 children with
FAS or PFAS had a reported exposure of no more than 1 drink/d. Are these 1 in 14 cases
especially vulnerable to the adverse effects of prenatal alcohol exposure, or were their lower
exposures inaccurately reported? The Lifestyle During Pregnancy Study (LDPS) (Kesmodel
et al., 2010, 2012) provided just such a dataset that addressed this issue by collecting
prenatal alcohol exposure history during early pregnancy and using standardized measures
of growth, face, and CNS.
The LDPS has previously provided data on the association between low-to-moderate alcohol
intake and alcohol binge drinking and neuropsychological development, including
intelligence, attention, psychomotor function, executive function, and behavior (Bay et al.,
2012; Kesmodel et al., 2010, 2012, 2013). The objective of the present analysis was to use
the LDPS to assess the potential effects of low-to-moderate average weekly alcohol
consumption and binge drinking in early pregnancy on facial features associated with FAS
among children 5 years of age. Specifically, we (i) document the occurrence of the
individual FAS facial features and overall FAS facial phenotype in the study sample; (ii)
assess the association between prenatal alcohol exposure and the magnitude of expression of
the FAS facial features and phenotype; and (iii) assess the association between the
magnitude of expression of the FAS facial phenotype and other diagnostic features of FAS,
including cognitive impact, reduced head circumference, and growth deficiency.
Schiøler Kesmodel et al. Page 3
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

MATERIALS AND METHODS
Study Sample
This study was part of the LDPS, which has been described in detail elsewhere (Kesmodel et
al., 2010, 2012). Briefly, the study is a prospective follow-up study based on a subsample
from the Danish National Birth Cohort (DNBC; Olsen et al., 2001).
A total of 1,628 mother–child pairs participated in the follow-up. Inclusion was based on a
stratified sample with oversampling of women with low-to-moderate alcohol intake and
binge drinking (Kesmodel et al., 2010, 2012). Exclusion criteria were inability to speak
Danish, impaired hearing or vision causing inability to complete the cognitive tests, multiple
pregnancies, and congenital diseases likely to cause mental retardation (Kesmodel et al.,
2010). Data collection for the follow-up study took place from September 2003 to June 2008
(Kesmodel et al., 2010).
Of the 1,628 participants’ images available for measurement, 670 met the inclusion criteria
for this study and had at least 1 of the 3 facial features measured (see details in Appendix).
Exposure Assessment
Information on alcohol intake during pregnancy was derived from the first prenatal DNBC
interview. Among the subsample of women participating in the follow-up, the median week
of gestation for completing the prenatal interview was 17 weeks (range: 7 to 39 weeks).
During the interview, the women were asked about their average number of beers, glasses of
wine, and glasses of spirits they currently consumed at the time of the interview over the
course of a week, and based on this information, the total number of weekly drinks was
calculated. These alcohol exposure questions have been shown to yield valid estimates of
alcohol consumption throughout pregnancy (relative to other methods) and reliable
information among pregnant Danish women (Kesmodel and Olsen, 2001). Information on
binge drinking during pregnancy included data on the number of binge episodes (defined as
intake of ≥5 drinks on a single occasion) and the timing (gestational week) of these episodes
(Kes-model, 2001) up until the time of the interview. A number of women in the current
sample reported 1 or more binge episodes during early weeks of pregnancy, although their
average number of drinks per week at the time of interview was zero (Kesmodel et al.,
2012). These women were classified accordingly as consuming zero average drinks per
week during pregnancy, but with 1 or more previous binge episodes. The definition of a
drink followed the definition from the Danish National Board of Health, with 1 standard
drink being equal to 12 g of pure alcohol. The sampling stratification for average weekly
consumption and binge consumption in the first trimester has been described previously
(Kesmodel et al., 2010, 2012). This stratification resulted in 5 sampling categories used in
this analysis.
Outcome Measures
Facial Features.—The follow-up assessments were conducted at 4 sites located in
Copenhagen, Aarhus, Odense, and Aalborg. The assessment comprised a comprehensive
Schiøler Kesmodel et al. Page 4
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

neuropsychological test battery which is described in detail elsewhere (Kesmodel et al.,
2010, 2012).
Following the test session, standardized digital facial photographs were taken of each mother
and child to allow subsequent measurement of (dysmorphic) facial features, including the
philtrum, the upper lip, and PFL. Specific procedures for taking and coding photographs are
described in Appendix. All testers were blind to the exposure status of the participants, and
all tests were administered in Danish.
Briefly, the University of Washington FAS Facial Photographic Analysis Software (Astley,
2016) was used to measure the magnitude of expression of each of the 3 diagnostic facial
features of FAS (short PFLs: 2 or more standard deviations (SD) below the mean; smooth
philtrum (Rank 4 or 5 on the University of Washington Lip-Philtrum Guide) and thin upper
lip (Rank 4 or 5 on the Lip-Philtrum Guide (Fig. 1), lip circularity ≥75.5) as defined by the
University of Washington FASD 4-Digit Code (Astley, 2016). For the 366 children with
photographs of sufficient quality to allow accurate measurement of all 3 facial features, the
magnitude of expression of the overall FAS facial phenotype (Face Rank) was ranked on a 4-
point Likert scale (Rank 1: normal phenotype; Rank 2: mild FAS phenotype; Rank 3:
moderate FAS phenotype; and Rank 4: severe FAS phenotype) in accordance with the FASD
4-Digit Code (Astley, 2004). The Scandinavian PFL growth charts (Stromland et al., 1999)
and University of Washington Lip-Philtrum Guide 1 were used for this Danish population.
Cognitive Function.—Child intelligence was assessed using the Wechsler Preschool and
Primary Scale of Intelligence-Revised (WPPSI-R) (Wechsler, 1990) covering the age span 3
to 7 years. The WPPSI-R includes 5 verbal and 5 performance subtests that are used to
calculate an overall verbal intelligence quotient (VIQ), overall performance IQ (PIQ), and
full-scale IQ (FSIQ). In this test battery, only 3 of the verbal (arithmetic, information, and
vocabulary) and 3 of the performance (block design, geometric design, and object assembly)
subtests were carried out to facilitate the child’s cooperation throughout the testing. Standard
procedures were used to prorate scores from the shortened test.
Child attention was assessed with the Test of Everyday Attention for Children at Five
(TEACh-5; Underbjerg et al., 2012, 2013) covering the age span 5 years to 5 years and 3
months. For this study, 2 subtests assessing selective attention (“Great Balloon Hunt” and
“Hide and Seek II”) and 2 subtests assessing sustained attention (“Barking” and “Draw a
line”) were used. Each subtest score was standardized to a mean of 0 and a SD of 1. To
calculate composite scores for overall, selective, and sustained attention, the means of the
respective standardized subtest scores for each individual were calculated and restandardized
to a mean of 0 and SD of 1.
Executive function was assessed using the Behavior Rating Inventory of Executive Function
(BRIEF) questionnaire (Gioia et al., 2000) covering the age span 5 to 18 years. The
questionnaire consists of 2 versions, 1 for parents and 1 for teachers. The parent version was
used for these analyses because of higher participation. Each questionnaire evaluates 8
domains of executive functioning and forms the Global Executive Composite (GEC). Three
of the 8 domains form the Behavioral Regulation Index (BRI), and 5 of the domains form
Schiøler Kesmodel et al. Page 5
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
the Metacognition Index (MI). Since the 8 domains do not follow a normal distribution, we
performed a normalizing t-score transformation to standardize each domain to a mean of 50
and SD of 10. To compute the GEC, BRI, and MI, the means of the respective domains for
each individual were calculated and restandardized to a mean of 50 and SD of 10. For all
BRIEF scores, a higher score indicates more executive function difficulties.
Covariates
Factors demonstrated in previous research to influence child neurodevelopment were
selected as covariates. The following covariates were obtained in the prenatal interview and
subsequently coded as follows: parity (0, 1, ≥2); prenatal smoking (yes/no); and maternal
prepregnancy body mass index (BMI) (weight in kg/[height in m]2). At the time of the 5-
year follow-up, the following variables were recorded: maternal marital status (single at
either the prenatal interview or follow-up/with partner at both times) and parental education
in years (total duration of attained education averaged for both parents or maternal only if
information on the father was missing). Additional information on collection of covariate
information is provided elsewhere (Kesmodel, 2012; Kesmodel et al., 2010).
Maternal age was obtained from the unique Danish personal identification number, as were
sex and age of the child. Birthweight in grams, head circumference, and gestational age in
days were obtained from the Danish Medical Birth Registry (Bliddal et al., 2018).
Data Analysis
Descriptive statistics (i.e., means, SDs, and proportions) were used to profile the
sociodemographics of the study population, the maternal drinking patterns, and the
magnitude of expression of the FAS facial features and phenotype. Logistic regression was
used to document the odds of presenting with the FAS/PFAS facial phenotype (Face Rank 3
or 4), short PFLs (ABC-Score = C, 2 or more SDs below the mean), smooth philtrum (Rank
4 or 5), or thin upper lip (Rank 4 or 5) relative to 4 different patterns of prenatal alcohol
exposure: (i) average number of drinks/week during pregnancy (0, 1 to 4, ≥5), (ii) binge
drinking (yes/no), (iii) number of binge drinking episodes (0, 1, 2 ≥ 3), and (iv) gestational
timing of the single binge drinking episode (no binge, weeks 1 to 2, weeks 3 to 4, weeks 5+;
multiple episodes). Odds ratios were adjusted for predefined covariates (parity; prenatal
smoking; maternal prepregnancy BMI; maternal marital status; parental education in years;
maternal age at the birth of the index child; sex and age of the child).
Not all photographs were of sufficient quality (e.g., facial expression, rotation, and focus) to
generate accurate measures of all 3 facial features. As a result, participants were divided into
2 groups. Group A (N = 366) consisted of children whose photographs were of sufficient
quality to measure all 3 facial features. Group B (N = 670) consisted of children whose
photographs were of sufficient quality to measure 1 to all 3 of the facial features. Group A is
a subset of Group B. Group B was used for analyses focused on the individual facial
features. Group A was used for analyses focused on the overall facial phenotype.
All analyses were conducted in SAS and Stata 12 (StataCorp LP, College Station, TX, USA)
and weighted by sampling probabilities. Statistical tests were 2-sided and deemed significant
at the 5% level. Estimates are accompanied by 95% confidence intervals.
Schiøler Kesmodel et al. Page 6
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

RESULTS
Sample Characteristics
Although the 2 subsets, Group A and Group B, were not randomly selected from the 1,628,
the sociodemographic profiles (Table 1) and maternal drinking patterns (Table 2) confirm
that both subgroups were highly reflective of one another and highly representative of the
1,628 participants from which they were drawn. Of the 366 women in Group A, 308 (84%)
reported, on average, low-to-moderate alcohol consumption with isolated episodes of binge
drinking, and 58 reported no alcohol consumption during pregnancy. Of the 670 women in
Group B, 561 (84%) reported, on average, low-to-moderate alcohol consumption with
isolated episodes of binge drinking, and 109 reported no alcohol consumption during
pregnancy (Table 2).
Occurrence of the FAS and PFAS Facial Phenotypes
Among the 366 participants with all 3 facial features measured, 308 had confirmed exposure
to alcohol. Nine of the 308 (2.9%) met the 4-Digit Code criteria for the moderate expression
of the FAS facial phenotype (Face Rank 3), and 1(0.3%) met the criteria for the severe
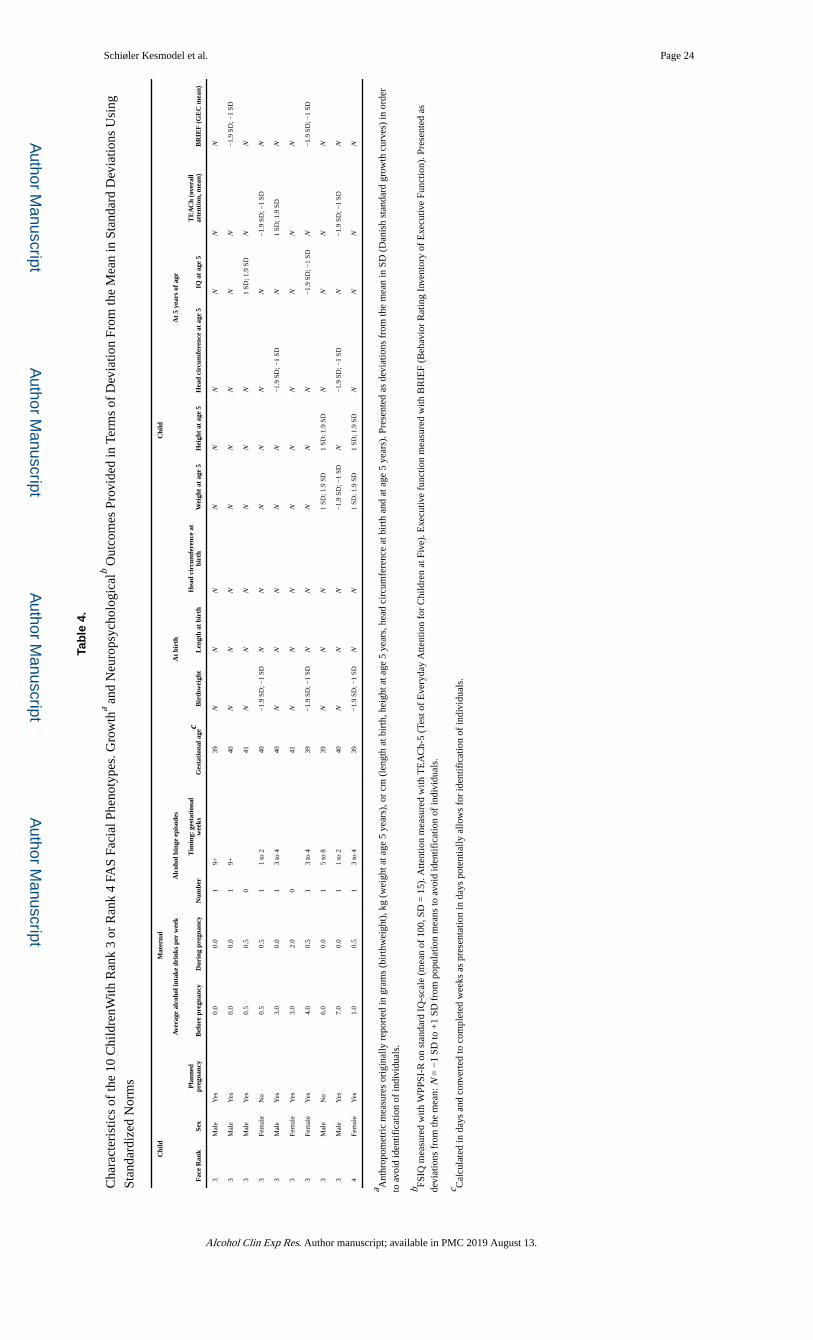
expression of the FAS facial phenotype (Face Rank 4) (Table 3). Measures of growth, CNS
structure and function, and maternal drinking patterns are presented in Table 4 to document
whether any of these 10 children met the diagnostic criteria for FAS or PFAS in accordance
with the FASD 4-Digit Code. All children were alcohol-exposed. Their mothers reported an
average intake of 0 to 7 drinks/wk before pregnancy, 0 to 2 drinks on average per week
during pregnancy, and a maximum of 1 binge episode during the first 20 weeks of
pregnancy. All children were born at term. Five of the 10 presented with growth, head
circumference, and/or IQ measures between 1 and 2 SDs below the mean. None of the
children presented with growth measures at or below the 10th percentile. One child
presented with a head circumference at the 10th percentile. In the absence of microcephaly
(head circumference less than or equal to third percentile), FAS and PFAS require evidence
of brain dysfunction. The level of brain dysfunction required for FAS or PFAS (CNS Rank
3) is defined by the 4-Digit Code as 3 or more domains of brain function, 2 or more SDs
below the mean based on a comprehensive assessment of language, memory, executive
function, cognition, motor, attention, and adaptation, using validated instruments
administered by clinical professionals (Astley, 2004). To confirm or rule out this level of
brain dysfunction, these assessments must be administered when a child is old enough
(typically >8 years) to engage in assessments of more complex, mature brain function
(Astley, 2004). None of the 10 children met the above criteria for brain dysfunction based on
the WPPSI-R IQ test. Thus, at 5 years of age, none of the 10 children met the 4-Digit Code
CNS criteria for FAS or PFAS, but all remain at risk for PFAS because CNS dysfunction
(CNS Rank 3) cannot be confirmed or ruled out at this young age.
Among the 304 children in which only 1 or 2 facial features could be measured, the full FAS
facial phenotype (Face Rank 4) could effectively be ruled out in 96% and the moderate
expression of FAS facial phenotype (Face Rank 3) could be ruled out in 77%. When
combined with the facial outcomes of the 366 children with all 3 facial features measured,
Schiøler Kesmodel et al. Page 7
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
the FAS/PFAS facial phenotypes (Face Ranks 3 to 4) could be ruled out in 96.7% of the 670
children.
Occurrence of the Individual FAS Facial Features
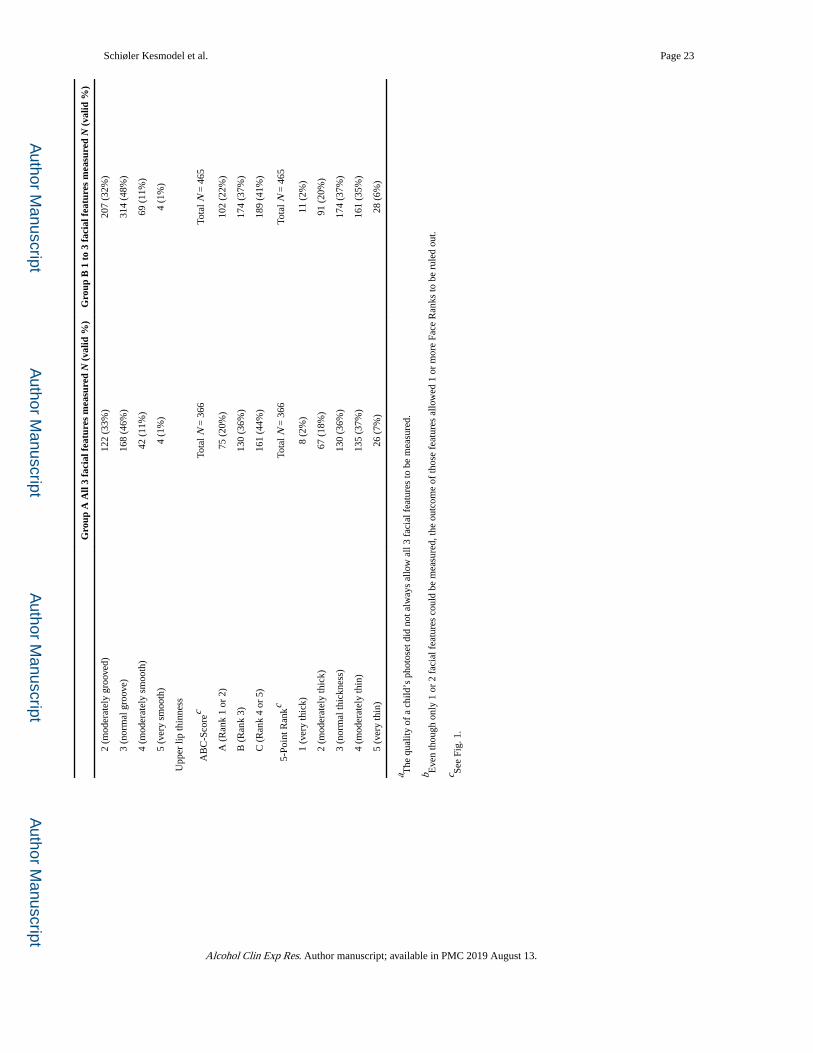
Among the 670 participants with 1, 2, or all 3 of the facial features measured, 4% presented
with PFLs 2 or more SDs below the mean (PFL ABC-Score = C), 11% presented with
moderately-to-completely smooth philtrums (Philtrum Ranks 4 and 5; ABC-Score = C), and
41% presented with moderately-to-severely thin upper lips (Lip Ranks 4 and 5; ABC-Score
= C; Table 3; Fig. 1). The prevalence of each FAS facial feature was nearly identical in the
smaller subset of 366 participants that had all 3 facial features measured.
Association Between FAS/PFAS Facial Features and Prenatal Alcohol Exposure
Table 5 shows the odds of presenting with the FAS/PFAS facial phenotypes (Face Rank 3 or
4) across different patterns of quantity, frequency, and timing of prenatal alcohol exposure.
Exposure to 1 to 4 drinks/wk on average during gestation was associated with a significant
8.5-fold increased odds for presenting with the FAS/PFAS facial phenotypes compared to
participants with no average drinks per week. Exposure to a single binge drinking episode
was associated with a significant 1.9-fold increased odds for the FAS/PFAS facial
phenotypes. When the timing of the single binge exposure was in gestational weeks 3 to 4,
participants were 2.5-fold more likely to present with the FAS/PFAS facial phenotypes than
participants with no binge exposure. Single binge exposures occurring before or after
gestational weeks 3 to 4 did not result in a significantly increased odds of the FAS/ PFAS
facial phenotypes.
Table 5 also presents the odds of presenting with each of the individual facial features of
FAS (short PFL: ≤−2 SDs, ABC-Score = C), smooth philtrum (Rank 4 or 5, ABC-Score =
C), and thin upper lip (Rank 4 or 5, ABC-Score = C) across the different patterns of prenatal
alcohol exposure.
PFL.—The odds of presenting with short PFLs (ABC-Score = C) increased significantly
from 1.8-fold to 3.7-fold as the average number of drinks per week during pregnancy
increased from 1 to 4 to ≥5. The odds of short PFLs increased significantly as the timing of
binge exposure occurred earlier in gestation. The odds were highest when binge(s) occurred
in weeks 1 to 2 and lowest when binge(s) occurred during or after gestational week 5,
although not statistically significant. The odds of short PFLs was highest with a single binge
exposure and significantly lower with 2 or more binge episodes.
Philtrum.—Odds of a smooth philtrum (ABC-Score = C) appeared to be more dependent
on the timing of binge exposure than the number of binge exposures. The odds were
significant and highest (1.3-fold higher) when binge drinking occurred in weeks 1 to 2. Odds
decreased linearly as binge drinking occurred later in gestation. Intake of 1 to 4 drinks/ wk
on average and 2 binge episodes in early pregnancy were associated with significantly lower
odds of a smooth philtrum.
Schiøler Kesmodel et al. Page 8
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Lip.—Odds of upper lip thinness (ABC-Score = C) also appeared to be more dependent on
the timing of binge exposure rather than the number of binge exposures. Participants with 1
binge exposure were at significantly higher odds (Odds ratios [OR] 1.19) for thin upper lip
than participants with no binge exposures. When binge exposure occurred in weeks 3 to 4,
odds of a thin upper lip was greatest (OR 1.66). When binge exposure occurred in week 5 or
later, children were significantly less likely to present with a thin upper lip (OR 0.83).
Associations Between the Magnitude of Expression of the FAS Facial Phenotype and Other Diagnostic Features of FASD
Individuals with short PFLs (≤−2 SDs) had significantly lower mean FSIQ and PIQ scores
(5 to 7 points lower) than the reference group with normal PFLs (>−1 SD) (Table 6).
Individuals with smooth philtrums (Rank 4or 5) had significantly lower mean FSIQ and VIQ
scores (3 to 4 points lower) than individuals with deep philtrums (Rank 1 or 2). Individuals
with thin upper lip (Rank 4 or 5) had a significantly higher mean VIQ score (2.5 points
higher) than individuals with thicker upper lips (Ranks 1 and 2). When the 3 facial features
were assessed together, individuals with the Rank 3 or 4 FAS/PFAS facial phenotypes
presented with mean FSIQ and PIQ scores that were 4 to 7 points lower than the individuals
with normal facial phenotypes (Ranks 1 and 2). Although the magnitude and direction of
association were equivalent to those observed for the individual facial features, the contrasts
were not statistically significant. The smaller sample sizes resulted in insufficient power
(<80%) to identify the 4 to 7 point contrasts as statistically significant.
We found no significant or clinically relevant differences between children with different
facial phenotypes or different measures of individual facial features and executive function
and attention (data not presented).
Mean birthweight, birth length, and birth head circumference decreased significantly with
increasing magnitude of expression of the FAS facial phenotype (Face Ranks 1 to 4) among
the 366 participants in Group A (Fig. 2).
DISCUSSION
Summary
There were 3 core findings in this study with a sample of 670 children in which 109 had no
prenatal alcohol exposure and 561 had low-to-moderate exposure with isolated binge
episodes. First, 10 children presented with the FAS/PFAS facial phenotypes (Face Rank 3 or
4). All 10 were alcohol-exposed. None met the diagnostic criteria for FAS or PFAS at 5
years of age. All 10, however, remain at risk for PFAS because they were too young at age 5
years to engage in the battery of neuropsychological assessments required to confirm or rule
out brain dysfunction. Second, children exposed to 1 to 4 drinks/wk were 8.5-fold more
likely to present with the FAS/PFAS facial phenotypes (Rank 3 or 4) than children with no
prenatal alcohol exposure. Risk of the FAS/PFAS facial phenotypes was also significantly
increased (2.5-fold) among children with a single binge exposure in gestational weeks 3 to 4
compared to children with no binge exposures. And third, the magnitude of expression of the
FAS facial phenotype was significantly correlated with all other diagnostic features of FAS:
Schiøler Kesmodel et al. Page 9
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
growth deficiency, microcephaly, and measures of CNS dysfunction, even if measures of
these features were within the normal range in this sample.
A primary objective of this study was to determine whether adverse outcomes typically
observed among populations with high PAE could be found in a population with much lower
exposure. Since the facial features that define FAS/PFAS were measured using the same
software (Astley, 2016), personnel, and FASD diagnostic system (Astley, 2004) used to
measure facial features in the University of Washington FASDPN clinical population,
relevant comparisons can be made between the 2 populations. The FASDPN dataset includes
over 3,000 individuals with prenatal alcohol exposure who received an interdisciplinary
FASD diagnostic evaluation using the FASD 4-Digit Diagnostic Code (Astley, 2010). The
alcohol exposures reported in the current study population (83% reported no more than 1 to
8 drinks/wk and/or isolated binge episode [drinking categories 1a to 4c; Table 1]) were
considerably lower than the alcohol exposures reported in the FASDPN clinical population
(76% report greater than 1 to 8 drinks/wk; average exposure is 7 to 9 drinks per occasion, 4
to 5 d/wk) (Astley, 2010).
Prevalence of FAS Facial Features and Correlation with Prenatal Alcohol Exposure
In the current study population with low-to-moderate prenatal alcohol exposure, 3.2%
(10/308) presented with the FAS/PFAS facial phenotypes (Rank 3 or 4). All were exposed to
no more than 7 drinks/wk and no more than a single episode of binge drinking. In contrast, a
much higher proportion of individuals (19%) present with the FAS/PFAS facial phenotypes
in the FASDPN patient population (Astley, 2010). Although individuals in the FASDPN
patient population are, on average, highly exposed, 1 of every 14 diagnosed with FAS/PFAS
has a reported exposure of no more than 7 drinks/wk. This is similar to the 10 children with
the FAS/PFAS facial phenotypes in the current study. Although prenatal alcohol exposure
may have been underreported for these 1 in 14 cases, it is also possible that these children
are particularly vulnerable to lower levels of exposure. Future research may want to examine
this possibility. The outcomes in the current study suggest that lower exposures may, in fact,
be sufficient to produce the FAS/PFAS facial phenotypes in a small proportion of children.
Timing of exposure also appears to be important. Perhaps one of the most compelling
findings in the current study was a significant 2.5-fold increased odds of the FAS/PFAS
facial phenotypes among children with a single binge exposure in gestational weeks 3 to 4.
Gestational weeks 3 and 4 reflect the primitive streak and gastrulation stage of
embryogenesis—a critical period of induction of alcohol-induced craniofacial alterations
(Astley, 2013; Astley et al., 1999; Sulik, 1984).
FAS and PFAS require more than just the Rank 3 or 4 facial phenotype. Although 10
children in the current study presented with the Rank 3 or 4 FAS/PFAS facial phenotypes,
none met the diagnostic criteria for FAS or PFAS (in accordance with the 4-Digit Code) at
the young age of 5 years. FAS is defined by growth ≤10th percentile, a Rank 4 facial
phenotype, and microcephaly (less than or equal to third percentile) and/or brain dysfunction
(3 or more domains of brain function 2 or more SDs below the mean) (Astley, 2004). PFAS
is defined by normal growth, a Rank 3 or 4 facial phenotype, and microcephaly and/or brain
dysfunction (3 or more domains of brain function 2 or more SDs below the mean). Since no
Schiøler Kesmodel et al. Page 10
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
child presented with growth ≤10th percentile, no child met the criteria for FAS. In contrast,
all 10 children met the growth and facial criteria for PFAS. None of them presented with
microcephaly; therefore, CNS dysfunction would be required to meet the CNS criteria for
PFAS. Nevertheless, at 5 years of age, all were too young to participate in the battery of
assessments required to confirm or rule out CNS dysfunction. As documented in the
FASDPN clinical population, most children with FAS or PFAS do not present with severe
brain dysfunction until later in childhood. For example, among 87 children ≤5 years of age
at the time of their FAS/PFAS diagnosis at the FASDPN, only 24% met the criteria for
severe CNS dysfunction (3 or more domains of function 2 or more SDs below the mean).
Among 152 children >5 years of age at the time of their FAS/PFAS diagnosis, 84% met the
criteria for severe CNS dysfunction. In addition, recent research (Astley et al., 2016)
documents that 67 and 70% of young children with prenatal alcohol exposure that present
with the Rank 3 or 4 FAS facial phenotypes, respectively, will present with severe CNS
dysfunction (3 or more domains of brain function 2 or more SDs below the mean) when they
are old enough (>8 years of age) to engage in more sophisticated assessments of brain
function. Thus, if any of the 10 children with the Rank 3 or 4 FAS/PFAS facial phenotypes
present with brain dysfunction (3 or more domains of brain function 2 or more SDs below
the mean) later in childhood, they would meet the diagnostic criteria for PFAS.
Prenatal alcohol exposure was significantly correlated with the FAS facial phenotype and the
3 individual features that comprise the FAS facial phenotype. The strongest correlations with
alcohol (ORs of 1.9 to 8.5) were observed when the 3 features appeared together to produce
the Rank 3 or 4 FAS/PFAS facial phenotypes (Table 5). Since the Rank 4 FAS facial
phenotype is confirmed to be highly specific to prenatal alcohol exposure (Astley, 2013;
Astley and Clarren, 1996), it is highly likely that the FAS/PFAS facial phenotypes observed
in these 10 children were caused by their prenatal alcohol exposure. Weaker, but statistically
significant, correlations (ORs of 1.2 to 3.7) were observed between prenatal alcohol
exposure and each individual FAS facial feature. This would be expected since alcohol is not
the only factor influencing the length of a palpebral fissure, the depth of a philtrum, or the
thickness of an upper lip. Perhaps one of the strongest factors other than alcohol influencing
the physical presentation of these 3 facial features is familial genetics. A unique strength of
the current study was the opportunity to measure the birth mothers’ facial features. Among
the 10 children who presented with the Rank 3 or 4 FAS facial phenotypes, all of their birth
mothers presented with normal facial phenotypes (Face Ranks 1 and 2).
Correlations Between the FAS Facial Phenotype and Growth Deficiency, Microcephaly, and CNS Dysfunction
The correlations between face, growth, and CNS abnormalities observed in the current study
(Fig. 2) are nearly identical to those documented in the FASDPN clinical population (figures
8 and 9 in Astley, 2013). This study extends understanding of these correlations to a
population of children with low-to-moderate prenatal alcohol exposure.
Strengths
The sample of women and children used for this study form part of a well-described,
prospective cohort (Kesmodel et al., 2010; Olsen et al., 2001). While information bias is
Schiøler Kesmodel et al. Page 11
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

always a potential problem in observational studies (Kesmodel, 2018), the risk of
information bias was minimized. Information on alcohol drinking patterns was collected
directly from the birth mothers during pregnancy using validated instruments (Kesmodel,
2001; Kesmodel and Olsen, 2001), and all facial measures were performed by the inventor
of the software system (Astley, 2016) used in this paper, thereby eliminating any
interobserver variability and reducing the likelihood of measurement error. Further, facial
measurements were taken blind to the child’s exposure history. Because of the detailed
information available on all participants, confounding could be addressed by adjusting for a
priori selected potential confounders (Howards, 2018), following the same criteria as
previous papers based on this cohort (Kesmodel et al., 2012). Also, it has previously been
shown that despite selection problems in the DNBC, the external validity of measures of
association seems to be good (Nohr and Liew, 2018).
Weaknesses
The DNBC represents only approximately 30% of all Danish pregnant women and hence is
not a representative sample (Olsen et al., 2001). Further, the LDPS sample is a stratified
sample within the DNBC (Kesmodel et al., 2010), making the current sample even less
representative of the background population. While such selection may make the sample less
suitable for firm statements about the overall prevalence of specific traits, inferences based
on measures of association have been shown to be valid within the cohort (Nohr and Liew,
2018). Finally, since only 10 children presented with the Rank 3 to 4 facial phenotypes, the
representativeness of this small group may be limited, but the statistical power was sufficient
to identify significant associations with level and timing of prenatal alcohol exposure.
CONCLUSION
In conclusion, we found that approximately 3% (10/308) of the children whose mothers
reported low-to-moderate alcohol intake, not usually associated with the full FAS, met the
criteria for moderate-to-severe expression of the FAS facial phenotypes, Face Ranks 3 to 4.
None met the diagnostic criteria for FAS or PFAS at 5 years of age. However, all 10 remain
at risk for PFAS because they were too young at age 5 years to engage in the battery of
neuropsychological assessments required to confirm or rule out severe brain dysfunction.
The risk of FAS/PFAS facial phenotypes (Ranks 3 to 4) was significantly increased among
both women with average alcohol intake of 1 to 4 drinks/wk and women with isolated
episodes of binge drinking, particularly during gestational weeks 3 to 4. These findings
suggest that low-to-moderate levels of prenatal alcohol exposure or isolated binge exposures
may place some fetuses at risk for FAS, PFAS, or other FASDs. Thus, conservative advice is
still for women to abstain from alcohol consumption during pregnancy.
ACKNOWLEDGMENTS
Primary support for this study was provided by the Centers for Disease Control and Prevention (CDC), Atlanta, Georgia, USA. The Danish National Research Foundation has established the Danish Epidemiology Science Centre that initiated and created the DNBC. The cohort was furthermore a result of a major grant from this Foundation. Additional support for the DNBC was obtained from the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Augustinus Foundation, and the Health Foundation. The authors would like to thank all the participants for their time and efforts.
Schiøler Kesmodel et al. Page 12
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

APPENDIX: DETAILED PROCEDURES FOR TAKING AND SELECTING
PHOTOGRAPHS FOR FACIAL CODING:
To examine the association between facial features used to diagnose FAS/PFAS and low-to-
moderate prenatal alcohol exposure, digital photographs were obtained, selected, and
categorized for FAS/PFAS criteria according to the FASD 4-Digit Code (Astley, 2004).
Details of these procedures are described in this appendix.
Taking Digital Photographs
Each participant had a standardized frontal, oblique, and lateral digital facial photograph
taken in accordance with the FAS Facial Photographic Analysis Software instructions
(Astley, 2016). Briefly, the child had a relaxed facial expression (no smile, lips gently
closed, eyes fully open with no eyeglasses), and the digital images had proper rotation,
exposure, and focus. A 19.05-mm-diameter round paper sticker was placed between the
participant’s eyebrows as an internal measure of scale. Photographs were taken according to
the protocol outlined in Astley (2016), and lead psychologists received in-person training on
how to take the photographs by SA.
Selection of Photographs for Facial Coding
Resources and photograph quality did not permit the complete analysis of all 1,628
participants’ photographs. Thus, a stepwise approach was used to identify those children
with clear or suggestive indication of facial dysmorphia for further measurement. The goal
was to identify all individuals that presented with 1, 2, or all 3 of the FAS facial features as
defined above. The photographs were measured by authors AG and SA in a 2-step process,
masked to the participant’s alcohol exposure.
• Step 1: AG measured the PFLs and lip circularities of all 1,628 participants
regardless of the quality of the feature in the photograph (e.g., the eyes were not
fully open, the child was smiling, or the sticker curled). If the eyes are not fully
open, the child is smiling, or the sticker is slightly curled, the direction of error
will always be in 1 direction; the PFLs will be shorter, the lip thinner, and the
philtrum smoother than they truly are. SA reviewed the subset from Step 1 that
appeared to have short PFLs ≤−1.5 SDs and/or thin upper lips (lip circularities
≥70) and identified the subset that had sufficient image quality to ensure the PFL
and lip circularity measures could be accurately measured. SA then remeasured
the PFLs and lip circularities of this subset to ensure the highest level of
consistency and accuracy across all facial measures.
• Step 2: SA also reviewed the philtrum of all 1,628 participants and ranked only
the subset with philtrum images of sufficient image quality and met criteria for
Rank 4 or 5.
Schiøler Kesmodel et al. Page 13
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Final FAS/PFAS Determination
For all viable photographs, whenever a participant was identified as having at least 1 facial
feature in the FAS range, the other 2 facial features were also measured if the quality of the
image was sufficient. Once measurement of the 3 facial features was complete, the software
generated a 4-Digit Code Facial ABC-Score and Face Rank (Fig. 1). For example, if a child
presented with PFLs 2.6 SDs below the mean, a Rank 3 philtrum, and a Rank 2 upper lip,
they would receive a Facial ABC-Score of CBA and a Face Rank of 2 (mild). If 1 or 2 of the
3 facial features could not be measured, an “X” was placed in the ABC-Score to signify its
absence (e.g., the ABC-Score XCA signifies that the PFL could not be measured, but the
philtrum was a “C” and the lip was an “A” [see Fig. 1B]). A Face Rank could not be
generated if 1 or 2 of the 3 features could not be measured, but Facial ABC-Scores with 1 or
2 missing features could be used to accurately rule out 1 or more of Face Ranks 1 to 4. For
example, if a Facial ABC-Score was XXA, Face Ranks 3 and 4 can be accurately ruled out
despite not knowing the outcome of the PFL or philtrum, because neither can include a
feature with a Rank A.
REFERENCES
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorder. 5th ed. American Psychiatric Association, Arlington, VA 10.1176/appi.books.9780890425596.
Astley SJ (2004) Diagnostic Guide for Fetal Alcohol Spectrum Disorders: The 4-Digit Diagnostic Code, 3rd ed. University of Washington Publication Services, Seattle, WA.
Astley S (2010) Profile of the first 1,400 patients receiving diagnostic evaluations for fetal alcohol spectrum disorder at the Washington State Fetal Alcohol Syndrome Diagnostic & Prevention Network Can J Clin Pharmacol 17:e132–e164. Science Publishers Ltd, Potomac, MD. [PubMed: 20335648]
Astley SJ (2013) Validation of the fetal alcohol spectrum disorder (FASD) 4-Digit Diagnostic Code. J Popul Ther Clin Pharmacol 20:e416–e467. [PubMed: 24323701]
Astley SJ (2016) FAS Facial Photographic Analysis Software Instruction Manual. Version 2.1. University of Washington. http://depts.washington.edu/fasdpn/pdfs/FAS_Instruction_Manual_v2.1.0-050616.pdf
Astley SJ, Bledsoe JM, Davies JK (2016) The essential role of growth deficiency in the diagnosis of fetal alcohol spectrum disorder. Adv Pediatr Res 3(3):1–20. 10.12715/apr.2016.3.9.
Astley SJ, Bledsoe JM, Davies JK, Thorne JC (2017) Comparison of the FASD 4-digit code and Hoyme et al. 2016 FASD diagnostic guidelines. Adv Pediatric Res 4(3):1–26.
Astley SJ, Clarren SK (1996) A case definition and photographic screening tool for the facial phenotype of fetal alcohol syndrome. J Pediatr 129:33–41. [PubMed: 8757560]
Astley SJ, Clarren SK (2000) Diagnosing the full spectrum of fetal alcohol exposed individuals: introducing the 4-digit diagnostic code. Alcohol Alcohol 35:400–410. [PubMed: 10906009]
Astley SJ, Clarren SK (2001) Measuring the facial phenotype of individuals with prenatal alcohol exposure: correlations with brain dysfunction. Alcohol Alcohol 36:147–159. [PubMed: 11259212]
Astley SJ, Magnuson SI, Omnell LM, Clarren SK (1999) Fetal alcohol syndrome: changes in craniofacial form with age, cognition, and timing of ethanol exposure in the macaque. Teratology 59:163–172. [PubMed: 10194807]
Bay B, Støvring H, Wimberley T, Denny CH, Mortensen EL, Eriksen H-LF, Kesmodel US (2012) Low to moderate alcohol intake during pregnancy and risk of psychomotor deficits. Alcohol Clin Exp Res 36:807–814. [PubMed: 21995343]
Bertrand J, Floyd RL, Weber MK, O’Connor M, Riley EP, Johnson KA, Cohen DE, National Task Force on FAS/FAE (2004) Fetal Alcohol Syndrome: Guideline for Referral and Diagnosis. Centers for Disease Control and Prevention, Atlanta, GA.
Schiøler Kesmodel et al. Page 14
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Bliddal M, Broe A, Pottegård A, Olsen J, Langhoff-Roos J (2018) The Danish Medical Birth Register. Eur J Epidemiol 33:27–36. [PubMed: 29349587]
Bower C, Elliott EJ, On Behalf of the Steering Group (2016) Report to the Australian Government Department of Health: “Australian Guide to the diagnosis of Fetal Alcohol Spectrum Disorder (FASD)”.
Coles CD, Gailey AR, Mulle JG, Kable JA, Lynch ME, Jones KL (2016) A comparison among 5 methods for the clinical diagnosis of fetal alcohol spectrum disorders. Alcohol Clin Exp Res 40:1000–1009. [PubMed: 27028727]
Cook JL, Green CR, Lilley CM, Anderson SM, Baldwin ME, Chudley AE, Conry JL, LeBlanc N, Loock CA, Lutke J, Mallon BF, McFarlane AA, Temple VK, Rosales T; Canada Fetal Alcohol Spectrum Disorder Research Network (2016) Fetal alcohol spectrum disorder: a guideline for diagnosis across the lifespan. Can Med Assoc J 188:191–197. [PubMed: 26668194]
Gioia GA, Isquith PK, Guy SC, Kenworthy L (2000) Behavior Rating Inventory of Executive Function. Child Neuropsychol 6:235–238. [PubMed: 11419452]
Howards PP (2018) An overview of confounding. Part 1: the concept and how to address it. Acta Obstet Gynecol Scand 97(4), 394–399. [PubMed: 29341103]
Hoyme HE, Kalberg WO, Elliott AJ, Blankenship J, Buckley D, Marais AS, Manning MA, Robinson LK, Adam MP, Abdul-Rahman O, Jewett T, Coles CD, Chambers C, Jones KL, Adnams CM, Shah PE, Riley EP, Charness ME, Warren KR, May PA (2016) Updated clinical guidelines for diagnosing fetal alcohol spectrum disorders. Pediatrics 138:e20154256. [PubMed: 27464676]
Kesmodel U (2001) Binge drinking in pregnancy—frequency and methodology. Am J Epidemiol 154:777–782. [PubMed: 11590091]
Kesmodel US (2018) Information bias in epidemiological studies with a special focus on obstetrics and gynecology. Acta Obstet Gynecol Scand 97:417–423. [PubMed: 29453880]
Kesmodel US, Bay B, Wimberley T, Eriksen H-LF, Mortensen EL (2013) Does binge drinking during early pregnancy increase the risk of psychomotor deficits? Alcohol Clin Exp Res 37:1204–1212. [PubMed: 23414523]
Kesmodel US, Bertrand J, Støvring H, Skarpness B, Denny C, Mortensen EL, Lifestyle During Pregnancy Study Group (2012) The effect of different alcohol drinking patterns in early to mid-pregnancy on child’s intelligence, attention and executive function. BJOG 119:1180–1190. [PubMed: 22712700]
Kesmodel U, Olsen SF (2001) Self-reported alcohol intake in pregnancy: comparison between four methods. J Epidemiol Community Health 55:738–745. [PubMed: 11553658]
Kesmodel US, Underbjerg M, Kilburn TR, Bakketeig L, Mortensen EL, Landrø NI, Schendel D, Bertrand J, Grove J, Ebrahim S, Thorsen P (2010) Lifestyle during pregnancy: neurodevelopmental effects at age 5 years of age. The design and implementation of a prospective follow-up study. Scand J Public Health 38:208–219. [PubMed: 20064917]
Nohr EA, Liew Z (2018) How to investigate and adjust for selection bias in cohort studies. Acta Obstet Gynecol Scand 97:407–416. [PubMed: 29415329]
O’Leary CM, Bower C (2012) Guidelines for pregnancy: what’s an acceptable risk, and how is the evidence (finally) shaping up? Drug Alcohol Rev 31:170–183. [PubMed: 21955332]
Olsen J, Melbye M, Olsen SF, Sorensen TI, Aaby P, Andersen AM, Taxbol D, Hansen KD, Juhl M, Schow TB, Sorensen HT, Andresen J, Mortensen EL, Olesen AW, Sondergaard C (2001) The Danish National Birth Cohort–its background, structure and aim. Scand J Public Health 29:300–307. [PubMed: 11775787]
Stratton K, Howe C, Battaglia F (1996) Fetal Alcohol Syndrome: Diagnosis Epidemiology Prevention and Treatment Institute of Medicine, National Academy Press, Washington, DC.
Stromland K, Chen Y, Norberg T, Wennerstrom K, Michael G (1999) Reference values of facial features in scandinavian children measured with a range-camera technique. Scand J Plast Reconstr Surg Hand Surg 33:59–65. [PubMed: 10207966]
Sulik KK (1984) Critical periods for alcohol teratogenesis in mice, with special reference to the gastrulation stage of embryogenesis, in Mechanisms of Alcohol Damage in Utero. Pitman, London, Ciba Foundation Symposium. Vol. 105, pp 124–141. [PubMed: 6563984]
Schiøler Kesmodel et al. Page 15
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Underbjerg M, George MS, Thorsen P, Kesmodel US, Mortensen EL, Manly T (2013) Separable sustained and selective attention factors are apparent in 5-year-old children. PLoS ONE 8:e82843. [PubMed: 24376591]
Underbjerg M, Kesmodel US, Landrø NI, Bakketeig L, Grove J, Wimberley T, Kilburn TR, Sværke C, Thorsen P, Mortensen EL (2012) The effects of low to moderate alcohol consumption and binge drinking in early pregnancy on selective and sustained attention in five-year-old children. BJOG 119:1211–1221. [PubMed: 22712829]
Wechsler D (1990) Manual for the Wechsler Preschool and Primary Scale of Intelligence—Revised. The Psychological Corporation, Sidcup, Kent.
Schiøler Kesmodel et al. Page 16
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Fig. 1. (A) University of Washington Lip-Philtrum Guide 1 used to rank lip thinness and philtrum
smoothness on 5-point Likert scales. (B) The face tables on the backside of the Lip-Philtrum
Guide outline how the magnitude of expression of the FAS facial phenotype is ranked on a
4-point scale (Rank 1: normal; Rank 2: mild; Rank 3: moderate; and Rank 4: severe) (Astley,
2004). Copyright Susan Astley Hemingway. Reprinted by permission.
Schiøler Kesmodel et al. Page 17
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Fig. 2. Mean birthweight, birth length, and birth head circumference decreased significantly with
increasing magnitude of expression of the FAS facial phenotype (Face Ranks: 1, normal; 2,
mild; 3, moderate; and 4, severe) among the 366 participants in Group A. Error bars reflect
95% CIs. One-way ANOVA test for linear trend p-values: birth length 0.04, and birth-weight
and head circumference 0.001.
Schiøler Kesmodel et al. Page 18
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 19
Tab
le 1
.
Sam
ple
Cha
ract
eris
tics
of th
e C
urre
nt S
tudy
Pop
ulat
ions
and
the
Ori
gina
l LD
PS P
opul
atio
n fr
om W
hich
The
y W
ere
Dra
wn
LD
PS
2012
stu
dy p
arti
cipa
nts
Mot
her
and
child
pai
rs f
rom
alc
ohol
sam
plin
g ca
tego
ries
1 t
o 5
Cur
rent
201
8 st
udy
part
icip
ants
Chi
ldre
n fr
om t
he L
DP
S w
ith
Gro
up A
All
3 fa
cial
fea
ture
s m
easu
red
Gro
up B
1 t
o 3
faci
al f
eatu
res
mea
sure
d
Sam
ple
char
acte
rist
ics
n
1,62
836
667
0
Sa
mpl
ing
frac
tion
(med
ian,
10t
h/90
th p
erce
ntile
)9.
7 (1
.5/4
9.6)
9.7
(1.5
/49.
6)9.
7 (1
.2/4
9.6)
T
imin
g of
inte
rvie
w, g
esta
tiona
l wee
k (m
edia
n, 1
0th/
90th
per
cent
ile)
17 (
13/2
4)17
(13
/23)
17 (
13/2
3)
Fam
ily c
hara
cter
istic
s
M
ater
nal a
ge, y
ears
(m
ean
± S
D)
Pari
ty30
.9 ±
4.4
30.9
± 4
.330
.9 ±
4.3
0 (%
)50
.148
.949
.1
1 (%
)32
.231
.732
.1
≥2 (
%)
17.8
19.4
18.8
M
ater
nal B
MI
(bef
ore
preg
nanc
y), k
g/m
2 (m
edia
n, 1
0th/
90th
per
cent
ile)
22.6
(19
.6/2
8.7)
22.5
(19
.7/2
9.3)
22.6
(19
.6/2
9.1)
M
ater
nal m
arita
l sta
tus:
sin
gle
(%)
12.1
12.0
11.0
Pa
rent
al e
duca
tion,
yea
rs (
med
ian,
10t
h/90
th p
erce
ntile
)13
.0 (
11.0
/16.
0)12
.5 (
11.0
/16.
0)13
.0 (
11.0
/16.
0)
Fa
mily
hom
e in
dex:
sub
optim
al (
%)
18.7
20.8
18.6
M
ater
nal I
Q (
mea
n ±
SD
)10
0.0
± 1
5.0
100
± 1
4.8
M
ater
nal s
mok
ing
duri
ng p
regn
ancy
(%
)31
.433
.932
.2
Pa
rent
al p
ostn
atal
sm
okin
g (%
)31
.933
.331
.1
M
ater
nal b
inge
dri
nkin
g in
pre
gnan
cy (
%)
69.6
70.8
67.6
M
edia
n nu
mbe
r of
dri
nks
per
wee
k du
ring
pre
gnan
cy (
med
ian,
10t
h/90
th
perc
entil
e)0.
5 (0
/5)
0.5
(0/5
)0,
5 (0
/5)
Chi
ld c
hara
cter
istic
s
M
ale
sex
(%)
52.0
46.5
48.5
A
ge a
t tes
ting,
yea
rs (
med
ian,
10t
h/90
th p
erce
ntile
)5.
2 (5
.1/5
.3)
5.2
(5.1
/5.3
)5.
2 (5
.1/5
.3)
B
irth
wei
ght,
gram
s (m
ean
± S
D)
3601
.9 ±
516
.13,
600
± 5
07.3
3613
.6 ±
521
.4
G
esta
tiona
l age
, day
s (m
edia
n, 1
0th/
90th
per
cent
ile)
281
(267
/293
)28
1 (2
67/2
93)
282
(269
/293
)
M
edic
al c
ondi
tion
or m
edic
atio
n (%
)3.
31.
62.
4
Im
pair
ed h
eari
ng a
bilit
ies
(%)
4.7
4.4
4.8
Im
pair
ed v
isio
n ab
ilitie
s (%
)2.
92.
52.
7
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 20
Tab
le 2
.
Dis
trib
utio
n of
Mat
erna
l Dri
nkin
g Pa
ttern
s in
the
Ori
gina
l LD
PS 2
012
Stud
y an
d th
e C
urre
nt 2
018
Stud
y
Ave
rage
sta
ndar
d dr
inks
per
wee
kB
inge
a dri
nkin
gL
DP
S201
2bC
urre
nt 2
018
Fac
ial S
tudy
Ges
tati
onal
wee
ksP
arti
cipa
nts
Gro
up A
All
3 fa
cial
fea
ture
s m
easu
red
Gro
up B
1 t
o 3
faci
al f
eatu
res
mea
sure
d
Dur
ing
preg
nanc
y1
to 2
3 to
45
to 8
≥9N
= 1
,622
NN
=36
6 N
(%
of
LD
PS)
N =
670
N (
%of
LD
PS)
0N
oN
oN
oN
o25
758
(23
)10
9 (4
2)
0Y
esN
oN
oN
o11
328
(25
)47
(42
)
0N
oY
esN
oN
o10
425
(24
)42
(40
)
0N
oN
oY
esN
o10
924
(22
)55
(50
)
0N
oN
oN
oY
es94
21 (
22)
38 (
40)
Tota
l 677
Tota
l 156
(23
)To
tal 2
91 (
43)
1 to
4N
oN
oN
oN
o15
530
(19
)72
(46
)
1 to
4Y
esN
oN
oN
o11
330
(27
)43
(38
)
1 to
4N
oY
esN
oN
o12
023
(19
)43
(36
)
1 to
4N
oN
oY
esN
o93
28 (
30)
45 (
48)
1 to
4N
oN
oN
oY
es11
421
(18
)39
(34
)
Tota
l 595
Tota
l 132
(22
)To
tal 2
42 (
41)
0Y
es in
at l
east
281
21 (
26)
33 (
41)
1 to
8Y
es in
at l
east
282
15 (
18)
28 (
34)
1 to
3 to
≥5To
tal 1
63To
tal 3
6 (2
2)To
tal 6
1 (3
7)
24
5 to
8N
oN
oN
o79
17 (
22)
35 (
44)
5 to
8Y
esN
oN
o11
1 (9
)1
(9)
5 to
8N
oY
esN
o37
7 (1
9)15
(41
)
5 to
8N
oN
oY
es40
12 (
30)
18 (
45)
≥9N
oN
oN
o15
4 (2
7)5
(33)
≥9Y
es in
at l
east
25
1 (2
0)2
(40)
Tota
l 187
Tota
l 42
(22)
Tota
l 76
(41)
No.
of
bing
e dr
inki
ng e
piso
des
duri
ng p
regn
ancy
049
510
7 (2
2)21
7 (4
4)
178
318
2 (2
3)31
2 (4
0)
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 21
Ave
rage
sta
ndar
d dr
inks
per
wee
kB
inge
a dri
nkin
gL
DP
S201
2bC
urre
nt 2
018
Fac
ial S
tudy
Ges
tati
onal
wee
ksP
arti
cipa
nts
Gro
up A
All
3 fa
cial
fea
ture
s m
easu
red
Gro
up B
1 t
o 3
faci
al f
eatu
res
mea
sure
d
Dur
ing
preg
nanc
y1
to 2
3 to
45
to 8
≥9N
= 1
,622
NN
=36
6 N
(%
of
LD
PS)
N =
670
N (
%of
LD
PS)
222
547
(21
)95
(42
)
3 to
12
114
30 (
26)
46 (
40)
a Def
ined
as
an in
take
of
5 or
mor
e st
anda
rd d
rink
s on
one
occ
asio
n.
b Lif
esty
le D
urin
g Pr
egna
ncy
Stud
y 20
12.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 22
Tab
le 3
.
Dis
trib
utio
n of
the
FAS
Faci
al F
eatu
res
in th
e 2
Stud
y Po
pula
tions
Gro
up A
All
3 fa
cial
fea
ture
s m
easu
red
N (
valid
%)
Gro
up B
1 t
o 3
faci
al f
eatu
res
mea
sure
d N
(va
lid %
)
Num
ber
of f
acia
l fea
ture
s m
easu
reda
Tota
l N =
366
Tota
l N =
670
O
nly
10
(0%
)10
2 (1
5%)
2
of th
e 3
0 (0
%)
202
(30%
)
A
ll 3
366
(100
%)
366
(55%
)
FAS
face
ran
k
N
orm
al: R
ank
117
2 (4
7%)
172
M
ild: R
ank
218
4 (5
0%)
184
M
oder
ate:
Ran
k39
(2%
)9
Se
vere
: Ran
k41
(< 1
%)
1
A
mon
g th
e 30
4 w
ith o
nly
1 or
2 f
eatu
res
mea
sure
dbTo
tal N
= 3
04
Ran
k 1
rule
d ou
tN
/A12
(4%
)
Ran
k 4
rule
d ou
tN
/A38
(12
%)
Ran
ks 1
and
4 r
uled
out
N/A
20 (
7%)
Ran
ks 3
and
4 r
uled
out
N/A
211
(69%
)
Ran
ks 1
, 3, a
nd 4
rul
ed o
utN
/A23
(8%
)
PFL
Tota
l N =
366
Tota
l N =
491
A
BC
-Sco
rec
A(>
−1
SD)
298
(81%
)41
1 (8
4%)
B (
>−
2 SD
s &
≤−
1 SD
)50
(14
%)
58 (
12%
)
C (
≤−2
SDs)
18 (
5%)
22 (
4%)
Philt
rum
sm
ooth
ness
A
BC
-Sco
rec
Tota
l N =
366
Tota
l N =
648
A (
Ran
k 1
or 2
)15
2 (4
1%)
261
(40%
)
B (
Ran
k 3)
168
(46%
)31
4 (4
9%)
C (
Ran
k 4
or 5
)46
(13
%)
73 (
11%
)
5-
Poin
t Ran
kcTo
tal N
= 3
66To
tal N
= 6
48
1 (d
eepl
y gr
oove
d)30
(8%
)54
(8%
)
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 23
Gro
up A
All
3 fa
cial
fea
ture
s m
easu
red
N (
valid
%)
Gro
up B
1 t
o 3
faci
al f
eatu
res
mea
sure
d N
(va
lid %
)
2 (m
oder
atel
y gr
oove
d)12
2 (3
3%)
207
(32%
)
3 (n
orm
al g
roov
e)16
8 (4
6%)
314
(48%
)
4 (m
oder
atel
y sm
ooth
)42
(11
%)
69 (
11%
)
5 (v
ery
smoo
th)
4 (1
%)
4 (1
%)
Upp
er li
p th
inne
ss
A
BC
-Sco
rec
Tota
l N =
366
Tota
l N =
465
A (
Ran
k 1
or 2
)75
(20
%)
102
(22%
)
B (
Ran
k 3)
130
(36%
)17
4 (3
7%)
C (
Ran
k 4
or 5
)16
1 (4
4%)
189
(41%
)
5-
Poin
t Ran
kcTo
tal N
= 3
66To
tal N
= 4
65
1 (v
ery
thic
k)8
(2%
)11
(2%
)
2 (m
oder
atel
y th
ick)
67 (
18%
)91
(20
%)
3 (n
orm
al th
ickn
ess)
130
(36%
)17
4 (3
7%)
4 (m
oder
atel
y th
in)
135
(37%
)16
1 (3
5%)
5 (v
ery
thin
)26
(7%
)28
(6%
)
a The
qua
lity
of a
chi
ld’s
pho
tose
t did
not
alw
ays
allo
w a
ll 3
faci
al f
eatu
res
to b
e m
easu
red.
b Eve
n th
ough
onl
y 1
or 2
fac
ial f
eatu
res
coul
d be
mea
sure
d, th
e ou
tcom
e of
thos
e fe
atur
es a
llow
ed 1
or
mor
e Fa
ce R
anks
to b
e ru
led
out.
c See
Fig.
1.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 24
Tab
le 4
.
Cha
ract
eris
tics
of th
e 10
Chi
ldre
nWith
Ran
k 3
or R
ank
4 FA
S Fa
cial
Phe
noty
pes.
Gro
wth
a and
Neu
rops
ycho
logi
calb O
utco
mes
Pro
vide
d in
Ter
ms
of D
evia
tion
From
the
Mea
n in
Sta
ndar
d D
evia
tions
Usi
ng
Stan
dard
ized
Nor
ms
Chi
ldM
ater
nal
Chi
ld
Ave
rage
alc
ohol
inta
ke d
rink
s pe
r w
eek
Alc
ohol
bin
ge e
piso
des
At
birt
hA
t 5
year
s of
age
Fac
e R
ank
Sex
Pla
nned
pr
egna
ncy
Bef
ore
preg
nanc
yD
urin
g pr
egna
ncy
Num
ber
Tim
ing:
ges
tati
onal
w
eeks
Ges
tati
onal
age
cB
irth
wei
ght
Len
gth
at b
irth
Hea
d ci
rcum
fere
nce
at
birt
hW
eigh
t at
age
5H
eigh
t at
age
5H
ead
circ
umfe
renc
e at
age
5IQ
at
age
5T
EA
Ch
(ove
rall
atte
ntio
n, m
ean)
BR
IEF
(G
EC
mea
n)
3M
ale
Yes
0.0
0.0
19+
39N
NN
NN
NN
NN
3M
ale
Yes
0.0
0.0
19+
40N
NN
NN
NN
N−
1.9
SD; −
1 SD
3M
ale
Yes
0.5
0.5
041
NN
NN
NN
1 SD
; 1.9
SD
NN
3Fe
mal
eN
o0.
50.
51
1 to
240
−1.
9 SD
; −1
SDN
NN
NN
N−
1.9
SD; −
1 SD
N
3M
ale
Yes
3.0
0.0
13
to 4
40N
NN
NN
−1.
9 SD
; −1
SDN
1 SD
; 1.9
SD
N
3Fe
mal
eY
es3.
02.
00
41N
NN
NN
NN
NN
3Fe
mal
eY
es4.
00.
51
3 to
439
−1.
9 SD
; −1
SDN
NN
NN
−1.
9 SD
; −1
SDN
−1.
9 SD
; −1
SD
3M
ale
No
6.0
0.0
15
to 8
39N
NN
1 SD
; 1.9
SD
1 SD
; 1.9
SD
NN
NN
3M
ale
Yes
7.0
0.0
11
to 2
40N
NN
−1.
9 SD
; −1
SDN
−1.
9 SD
; −1
SDN
−1.
9 SD
; −1
SDN
4Fe
mal
eY
es1.
00.
51
3 to
439
−1.
9 SD
; −1
SDN
N1
SD; 1
.9 S
D1
SD; 1
.9 S
DN
NN
N
a Ant
hrop
omet
ric
mea
sure
s or
igin
ally
rep
orte
d in
gra
ms
(bir
thw
eigh
t), k
g (w
eigh
t at a
ge 5
yea
rs),
or
cm (
leng
th a
t bir
th, h
eigh
t at a
ge 5
yea
rs, h
ead
circ
umfe
renc
e at
bir
th a
nd a
t age
5 y
ears
). P
rese
nted
as
devi
atio
ns f
rom
the
mea
n in
SD
(D
anis
h st
anda
rd g
row
th c
urve
s) in
ord
er
to a
void
iden
tific
atio
n of
indi
vidu
als.
b FSIQ
mea
sure
d w
ith W
PPSI
-R o
n st
anda
rd I
Q-s
cale
(m
ean
of 1
00, S
D =
15)
. Atte
ntio
n m
easu
red
with
TE
AC
h-5
(Tes
t of
Eve
ryda
y A
ttent
ion
for
Chi
ldre
n at
Fiv
e). E
xecu
tive
func
tion
mea
sure
d w
ith B
RIE
F (B
ehav
ior
Rat
ing
Inve
ntor
y of
Exe
cutiv
e Fu
nctio
n). P
rese
nted
as
devi
atio
ns f
rom
the
mea
n: N
= −
1 SD
to +
1 SD
fro
m p
opul
atio
n m
eans
to a
void
iden
tific
atio
n of
indi
vidu
als.
c Cal
cula
ted
in d
ays
and
conv
erte
d to
com
plet
ed w
eeks
as
pres
enta
tion
in d
ays
pote
ntia
lly a
llow
s fo
r id
entif
icat
ion
of in
divi
dual
s.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 25
Tab
le 5
.
Odd
s R
atio
sa for
Dys
mor
phic
Fac
ial F
eatu
res
Am
ong
the
366
Chi
ldre
n fr
om G
RO
UP
AW
ith a
ll 3
Faci
al F
eatu
res
Mea
sure
d an
d th
e 67
0 C
hild
ren
From
Gro
up B
With
1 to
3 F
acia
l Fea
ture
s M
easu
red
in R
elat
ion
to P
atte
rn o
f M
ater
nal A
lcoh
ol C
onsu
mpt
ion
Dur
ing
Preg
nanc
y
Alc
ohol
pat
tern
Fac
e ra
nks
3 to
4 v
ersu
s 1
to 2
N =
10
vers
us n
= 3
56F
rom
Gro
up A
: N
= 3
66O
R (
95%
CI)
PF
L A
BC
-Sco
resb
C v
ersu
s A
BN
= 2
2 ve
rsus
N =
469
Fro
m G
roup
B:
N =
670
OR
(95
% C
I)
Phi
ltru
m A
BC
-Sco
resb
C v
ersu
s A
BN
= 7
3 ve
rsus
N =
575
Fro
m G
roup
B:
N =
670
OR
(95
% C
I)
Upp
er li
p A
BC
-Sco
resb
C v
ersu
s A
BN
= 1
89 v
ersu
s N
= 2
76F
rom
Gro
up B
: N
= 6
70O
R (
95%
CI)
Ave
rage
num
ber
of d
rink
s pe
r w
eek
duri
ng p
regn
ancy
0
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
1
to 4
8.50
(6.
03 to
12.
0)1.
76 (
1.42
to 2
.16)
0.87
(0.
79 to
0.9
6)0.
97 (
0.90
to 1
.05)
≥5
No
rank
3 to
4 fa
ces
in th
is c
ateg
ory
3.71
(2.
15 to
6.4
0)0.
76 (
0.47
to 1
.24)
1.16
(0.
85 to
1.5
8)
p-
Val
uec
<0.
001
<0.
001
0.01
0.46
Bin
ge d
rink
ing
in p
regn
ancy
N
oR
efer
ence
dR
efer
ence
Ref
eren
ceR
efer
ence
Y
es1.
36 (
1.03
to 1
.78)
0.85
(0.
67 to
1.0
8)0.
92 (
0.82
to 1
.03)
1.08
(0.
99 to
1.1
8)
p-
Val
ue0.
030.
190.
150.
07
Num
ber
of b
inge
dri
nkin
g ep
isod
es in
pre
gnan
cy
0
Ref
eren
ceR
efer
ence
cR
efer
ence
Ref
eren
ce
1
1.94
(1.
48 to
2.5
4)1.
20 (
0.94
to 1
.54)
1.00
(0.
87 to
1.1
4)1.
19(1
.08
to 1
.31)
2
No
rank
3 to
4 fa
ces
in th
is c
ateg
ory
0.11
(0.
03 to
0.3
5)0.
71 (
0.57
to 0
.89)
0.86
(0.
74 to
0.9
9)
≥3
No
rank
3 to
4 fa
ces
in th
is c
ateg
ory
0.44
(0.
21 to
0.9
6)0.
96 (
0.70
to 1
.31)
1.08
(0.
87 to
1.3
5)
p-
Val
ue<
0.00
1<
0.00
10.
020.
93
Tim
ing
of b
inge
dri
nkin
g ep
isod
es in
pre
gnan
cy (
gest
atio
nal w
eek)
N
o bi
nge
Ref
eren
ceR
efer
ence
Ref
eren
ceR
efer
ence
W
eeks
1 to
2 o
nly
1.46
(0.
90 to
2.3
5)1.
13 (
0.76
to 1
.69)
1.32
(1.
08 to
1.6
2)1.
12 (
0.95
to 1
.31)
W
eeks
3 to
4 o
nly
2.47
(1.
79 to
3.4
1)1.
10 (
0.78
to 1
.56)
0.91
(0.
76 to
1.0
8)1.
66 (
1.46
to 1
.90)
W
eek
>5
only
0.80
(0.
43 to
1.4
9)0.
99 (
0.66
to 1
.48)
0.87
(0.
69 to
1.0
8)0.
83 (
0.71
to 0
.98)
M
ultip
le e
piso
des
No
rank
3 to
4 fa
ces
in th
is c
ateg
ory
No
rank
C P
FLs
in th
is c
ateg
ory
0.79
(0.
62 to
1.0
1)1.
05 (
0.89
to 1
.24)
p-
Val
ue<
0.00
1<
0.00
10.
007
<0.
001
a OR
adj
uste
d fo
r so
ciod
emog
raph
ic a
nd s
ampl
ing
fact
ors.
95%
conf
iden
ce in
terv
als
that
do
not s
pan
1.0
are
stat
istic
ally
sig
nifi
cant
at p
< 0
.05.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 26b Fa
cial
AB
C-S
core
s fr
om th
e FA
SD 4
-Dig
it C
ode
are
defi
ned
in F
ig. 1
.
c p-V
alue
for
the
hypo
thes
is o
f no
dif
fere
nce
in f
acia
l fet
aure
s ac
ross
leve
ls o
f al
coho
l int
ake.
d The
ref
eren
ce g
roup
s ha
ve z
ero
expo
sure
onl
y fo
r th
e ty
pe o
f ex
posu
re p
atte
rn b
eing
ass
esse
d, b
ut h
ave
the
full
rang
e of
exp
osur
e ba
sed
on th
e ot
her
patte
rns.
For
exa
mpl
e, th
is r
efer
ence
gro
up o
f 10
9 pa
rtic
ipan
ts h
as z
ero
bing
e ep
isod
es o
f ex
posu
re, b
ut 3
0 (2
8%)
wer
e ex
pose
d to
an
aver
age
of 1
to 4
dri
nks/
wk
duri
ng p
regn
ancy
and
21
(19%
) w
ere
expo
sed
to a
n av
erag
e of
5 o
r m
ore
drin
ks/w
k du
ring
pr
egna
ncy.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Schiøler Kesmodel et al. Page 27
Tab
le 6
.
Ass
ocia
tion
Bet
wee
n Fa
cial
Fea
ture
s an
d C
hild
IQ
a
Inte
llige
nce
Ful
l-sc
ale
IQ (
stan
dard
sco
re)
Per
form
ance
IQ
(st
anda
rd s
core
)V
erba
l IQ
(st
anda
rd s
core
)
Mea
nM
ean
diff
eren
ce95
% C
Ip-
Val
ueM
ean
Mea
n di
ffer
ence
95%
CI
p-V
alue
Mea
nM
ean
diff
eren
ce95
% C
Ip-
Val
ue
Faci
al f
eatu
res
mea
sure
b
Fa
cial
phe
noty
pe r
ank
Ran
ks 1
and
2 (N
= 3
55)
106.
7R
efer
ence
107.
4R
efer
ence
104.
8R
efer
ence
Ran
ks 3
and
4 (N
= 1
0)10
2.5
−4.
2−
11.7
, 3.3
0.26
910
0.6
−6.
8−
16.6
,3.0
0.17
510
3.6
−1.
2−
7.6,
5.3
0.72
4
PF
L A
BC
-Sco
re
A (
>—
1 SD
) (N
= 4
10)
107.
2R
efer
ence
107.
7R
efer
ence
105.
2R
efer
ence
B (
>−
2 SD
& ≤
−1
SD)
(N =
57
)10
3.9
−3.
3−
6.6,
0.0
60.
055
102.
4−
5.3
−9.
6, −
1.0
0.01
510
4.4
−0.
9−
3.7,
2.0
0.55
3
C (
≤−2
SD)
(N =
22)
101.
3−
5.9
−11
.0, −
0.7
0.02
510
0.4
−7.
3−
13.8
, −0.
80.
027
102.
0−
3.2
−7.
7, 1
.30.
160
Ph
iltru
m A
BC
-Sco
re
A (
Ran
k 1
or 2
) {N
= 2
60)
107.
8R
efer
ence
107.
9R
efer
ence
106.
1R
efer
ence
B (
Ran
k 3)
(N=
314)
105.
5−
2.3
−4.
4, −
0.2
0.03
410
5.6
−2.
2−
5.0,
0.5
0.11
510
4.3
−1.
8−
3.6,
−0.
070.
041
C (
Ran
k 4
or 5
) (N
= 7
3)10
4.1
−3.
5−
6.9,
−0.
10.
042
104.
3−
3.4
−7.
6, 0
.80.
116
103
−2.
9−
5.8,
−0.
030.
048
U
pper
Lip
AB
C-S
core
A (
Ran
k 1
or 2
)(N
= 10
2)10
5.9
Ref
eren
ce10
7.3
Ref
eren
ce10
3.4
Ref
eren
ce
B (
Ran
k 3)
(N =
174
)10
6.0
0.1
−3.
2, 3
.40.
950
106.
7−
0.7
−4.
9, 3
.50.
757
104.
10.
7−
2.0,
3.4
0.61
3
C (
Ran
k 4
or 5
) (N
= 1
88)
107.
21.
3−
1.7,
4.3
0.38
810
6.9
−0.
5−
4.4,
3.4
0.81
010
6.0
2.5
0.06
, 5.0
0.04
5
PFL
, pal
pebr
al f
issu
re le
ngth
.
a IQ m
easu
red
with
WPP
SI-R
.
b Face
Ran
ks a
nd A
BC
-Sco
res
desc
ribe
d in
Fig
. 1.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2019 August 13.