la nefrologia tra passato,presente e futuro · la nefrologia tra passato,presente e futuro ......
TRANSCRIPT

La Nefrologia tra passato,presente e
futuro
Antonio Santoro
Nephrology, Dialysis and Hypertension Unit
Sant’Orsola-Malpighi Hospital
Bologna - ITALY
University Hospital



• The ultimate goal of a nephrologist is to maintain renal
function and to treat kidney diseases,manage
associated metabolic changes and prolong time till
dialysis.
• Nephrologist perform hemodialysis,PD, and other
extracorporeal depuration techniques.
• Nephrologists manage Acute Renal Failure and provide
lifesaving Continuous and intermittent Renal
Replacement Therapy (CRRT).
• Nephrologists are specialists in electrolyte, fluid
balance, acid/base, anemia assoc renal disease,
metabolic bone disease, hypertension management
and renal trasplantation.
The nephrologist
J. Stewart Cameron 1982



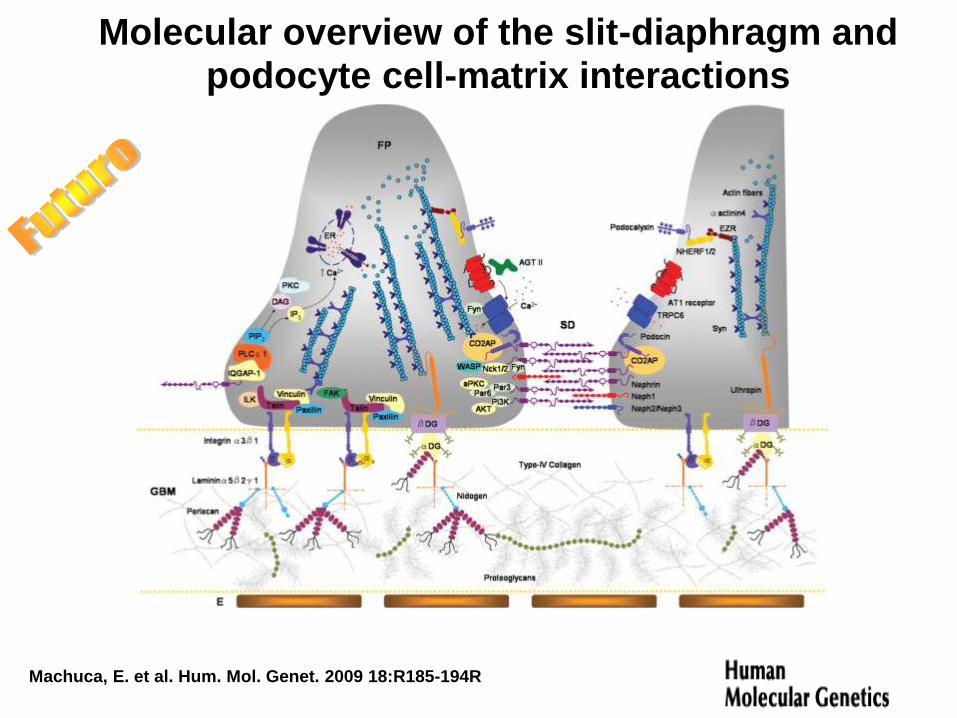
Machuca, E. et al. Hum. Mol. Genet. 2009 18:R185-194R
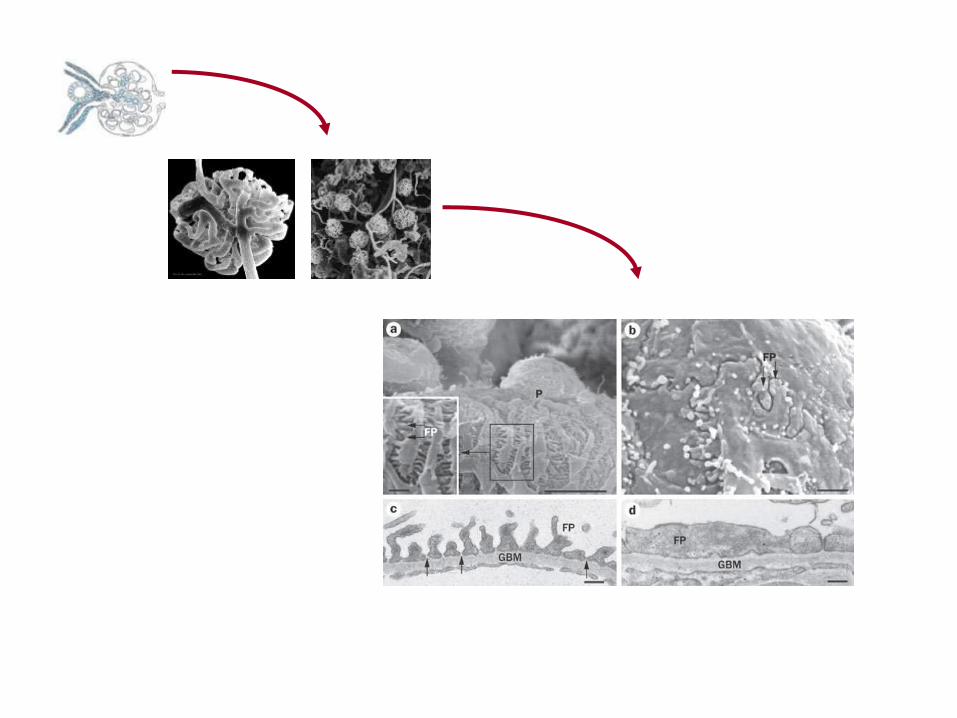
Glomerular filtration barrier structure
Machuca, E. et al. Hum. Mol. Genet. 2009 18:R185-194R
Molecular overview of the slit-diaphragm and podocyte cell-matrix interactions
Various molecules having diverse functions at the glomerular filtration
barrier may be affected by mutations in genetic forms of NS.
However, recent findings have indicated that different pathogenetic
mechanisms have converging lines in that the rearrangement of the
podocyte’s actin cytoskeleton has been identified as a common
denominator of a variety of inherited glomerular disorders.
It has also become evident that the molecular sieve formed by the
glomerular filtration barrier is not a static structure. In fact, the podocyte
layer has emerged as a particularly dynamic network of
interacting cells that contain an actin-based contractile apparatus.
It seems likely that the podocytes’ ability to continuously sense
and adapt to environmental changes is critical for preserving
glomerular permselectivity. Notably, there is emerging evidence that also
podocyte injury of non-genetic cause may involve the same
pathogenetic pathways, as it is associated with reorganization of the slit
diaphragm and of the foot process structur

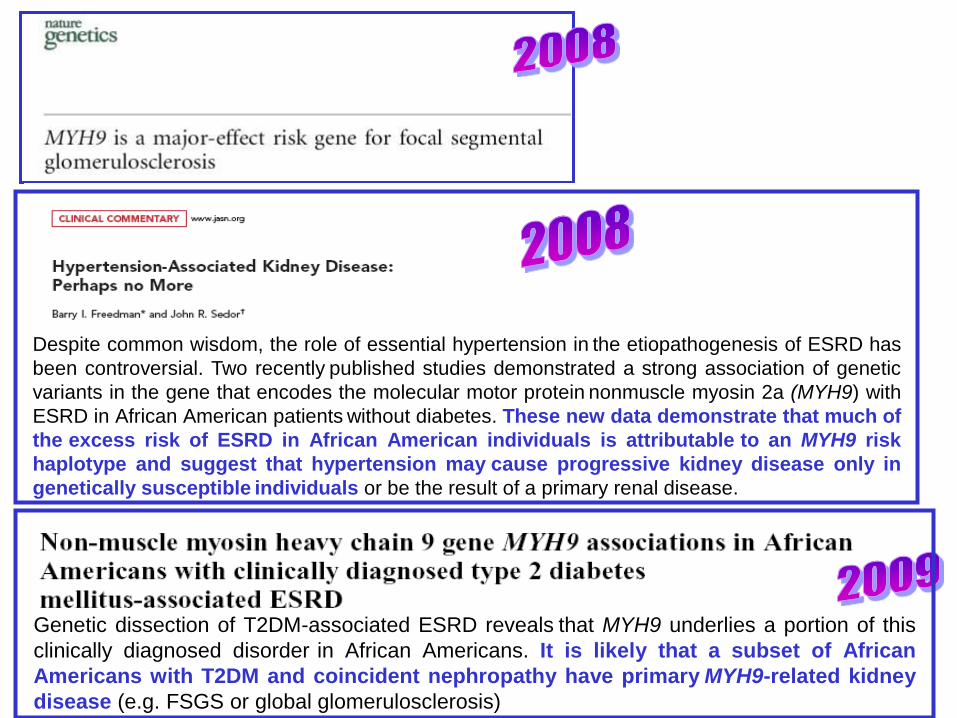
Despite common wisdom, the role of essential hypertension in the etiopathogenesis of ESRD has
been controversial. Two recently published studies demonstrated a strong association of genetic
variants in the gene that encodes the molecular motor protein nonmuscle myosin 2a (MYH9) with
ESRD in African American patients without diabetes. These new data demonstrate that much of
the excess risk of ESRD in African American individuals is attributable to an MYH9 risk
haplotype and suggest that hypertension may cause progressive kidney disease only in
genetically susceptible individuals or be the result of a primary renal disease.
Genetic dissection of T2DM-associated ESRD reveals that MYH9 underlies a portion of this
clinically diagnosed disorder in African Americans. It is likely that a subset of African
Americans with T2DM and coincident nephropathy have primary MYH9-related kidney
disease (e.g. FSGS or global glomerulosclerosis)

… altri contributi della genetica ….
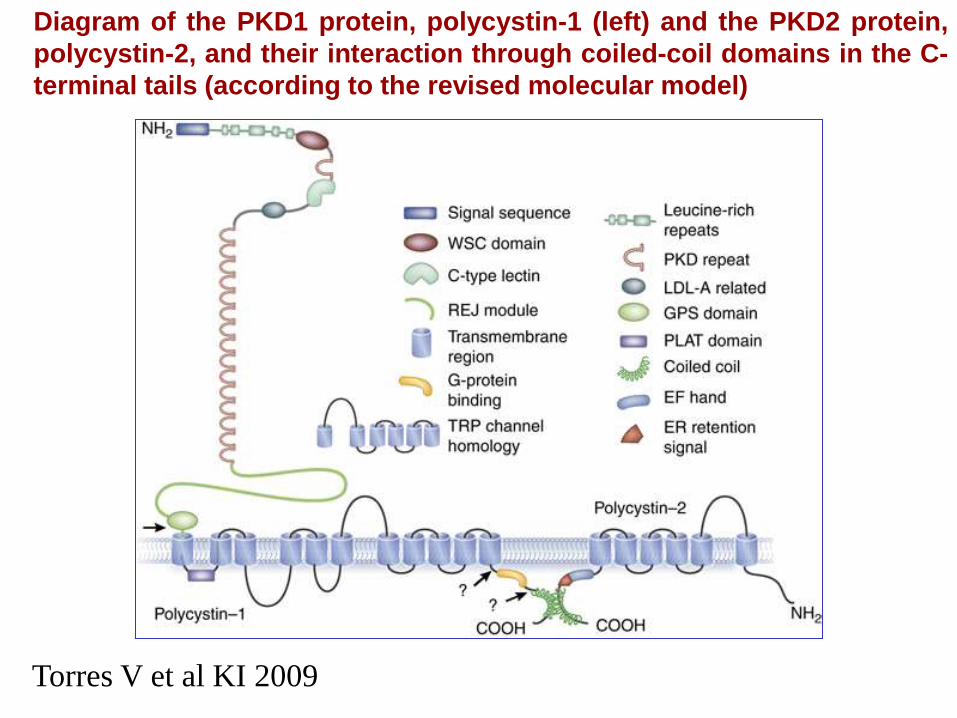
Diagram of the PKD1 protein, polycystin-1 (left) and the PKD2 protein,
polycystin-2, and their interaction through coiled-coil domains in the C-
terminal tails (according to the revised molecular model)
Torres V et al KI 2009
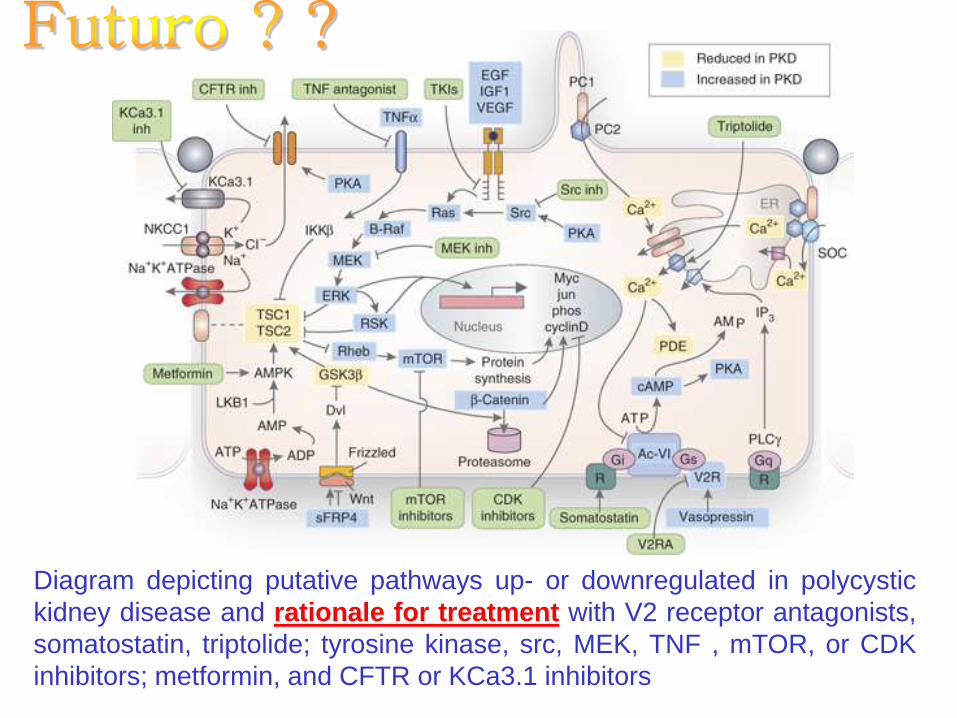
Diagram depicting putative pathways up- or downregulated in polycystic
kidney disease and rationale for treatment with V2 receptor antagonists,
somatostatin, triptolide; tyrosine kinase, src, MEK, TNF , mTOR, or CDK
inhibitors; metformin, and CFTR or KCa3.1 inhibitors

Clin JASN 2008
NDT 2009
2008

CURRENTLY ACTIVE TRIALs for ADPKD
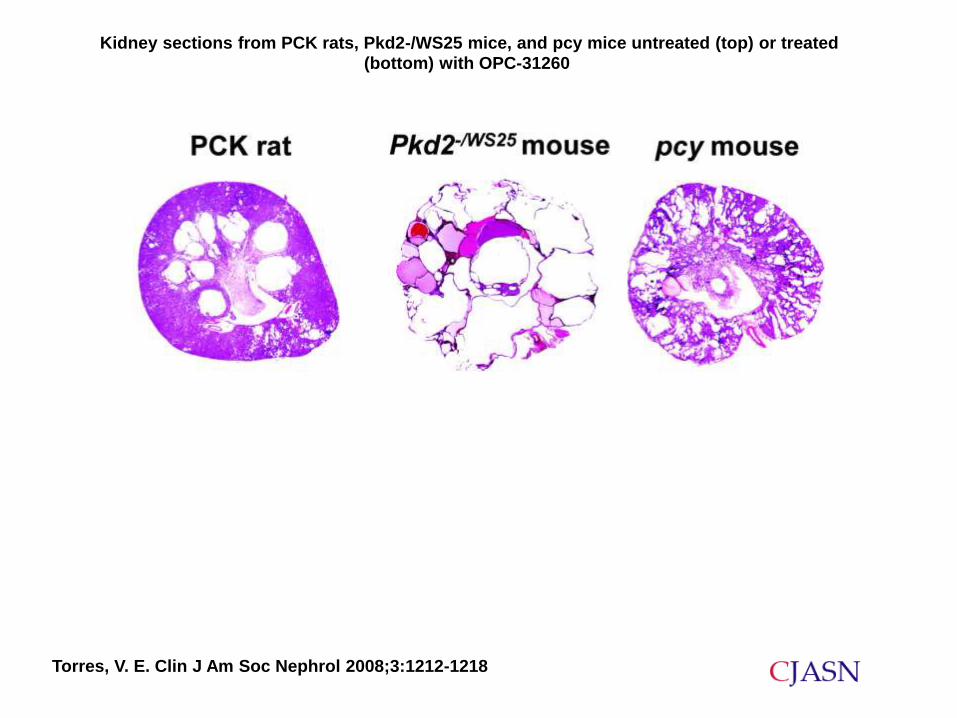
Torres, V. E. Clin J Am Soc Nephrol 2008;3:1212-1218
Kidney sections from PCK rats, Pkd2-/WS25 mice, and pcy mice untreated (top) or treated
(bottom) with OPC-31260

Diagnostic tools

1960 1970 1980 1990 2000
Chest X Ray
ECG
Nuclear Medicine
Echo
Angiography
CT
Doppler Echo
TEE
MRI
PET
MDCT
Chest x ray
SPECT
CT
MRI
PET
MDCT
Echography
Coronary angiography
TEE
IVUS
Diagnostic tools
EBCT
$
Spectroscopy

Multidetector CT
evolution or revolution? (Rubin G, Radiology 2000)


Cellule staminali

Ronconi, E. et al. J Am Soc Nephrol 2009;20:322-332
Schematic representation of the hierarchical distribution of CD133+CD24+PDX- and CD133+CD24+PDX+ cells within human
glomeruli

Ronconi, E. et al. J Am Soc Nephrol 2009;20:322-332
Heterogeneous expression of renal progenitors and podocytes markers by cells of Bowman's capsule in adult human kidney

Urinary proteomics
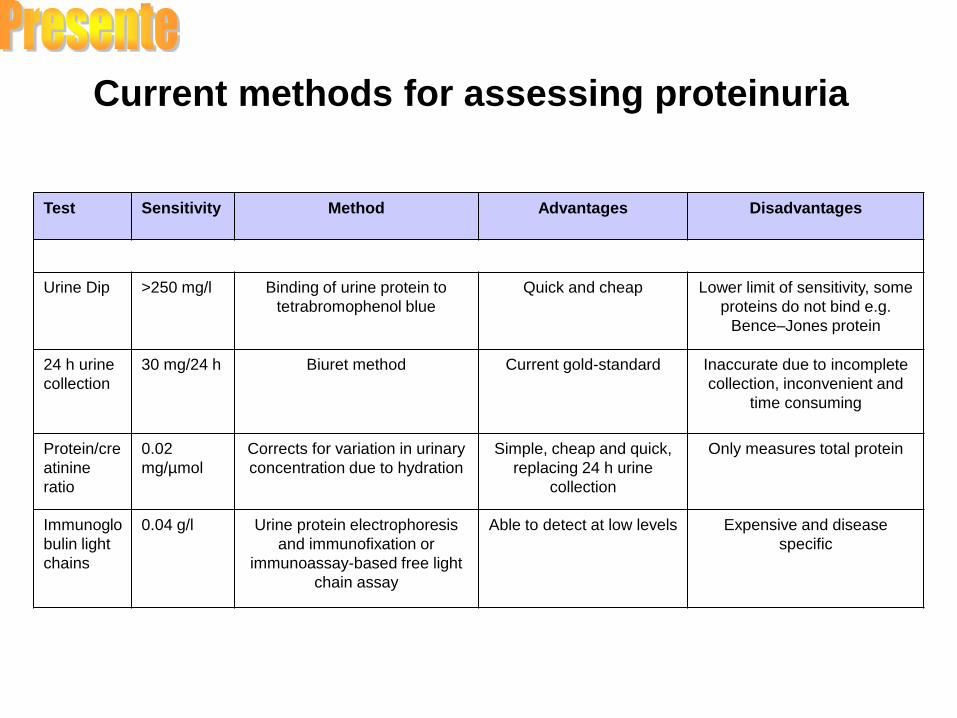
Test Sensitivity Method Advantages Disadvantages
Urine Dip >250 mg/l Binding of urine protein to
tetrabromophenol blue
Quick and cheap Lower limit of sensitivity, some
proteins do not bind e.g.
Bence–Jones protein
24 h urine
collection
30 mg/24 h Biuret method Current gold-standard Inaccurate due to incomplete
collection, inconvenient and
time consuming
Protein/cre
atinine
ratio
0.02
mg/µmol
Corrects for variation in urinary
concentration due to hydration
Simple, cheap and quick,
replacing 24 h urine
collection
Only measures total protein
Immunoglo
bulin light
chains
0.04 g/l Urine protein electrophoresis
and immunofixation or
immunoassay-based free light
chain assay
Able to detect at low levels Expensive and disease
specific
Current methods for assessing proteinuria

Bramham, K. et al. QJM 2009 102:523-538
Schema of translation of urinary proteomics into clinical practice

Recent developments in proteomic techniques promise exciting insight
into normal renal physiology and renal disease processes, allowing
precise definition of the disease proteome. In turn this will enable
diagnosis, prognosis and prediction of response to treatment of
individuals. …………………………………............…
Expanding knowledge in recent years and the rapidly advancing
field of proteomics will facilitate studies of renal physiology and
pathophysiology and ultimately should make redundant the
traditional renal biopsy.
QJM 2009 102(8):523-538

Characterization of Diabetic Nephropathy by Urinary Proteomic
Analysis: Identification of a Processed Ubiquitin Form as a Differentially
Excreted Protein in Diabetic Nephropathy Patients Hassan Dihazi et al. Clinical Chemistry 2007; 53: 1636-1645
Ubiquitin degradation assay
In summary, in this pilot study we identified 3 different proteins that were differentially excreted in the urine of
diabetic nephropathy patients compared with the other groups. A processed form of ubiquitin with m/z 6188
was missed in the urine of diabetic nephropathy patients.
This ubiquitin form could be used as a prognosis marker for DM-NP. Quantification of this protein
during the progressive disease course in the DM-NP patients will give interesting information on the
development of the diseases and serve as a good marker for prognosis.

1854: The Scientific Basis for Dialysis
Script of Graham´s Bakerian Lecture, 1854
Thomas Graham
1805 - 1869 “... might be
applied to
medicine ...”

1913: A First “Artificial Kidney”
Abel JJ, Rowntree LG, Turner BB: On the removal of
diffusible substances from the circulating blood by
means of dialysis. Trans Ass Am Physicians 28:51, 1913
John Jacob Abel
1857 - 1939
"... by which the blood of a living animal may be submitted to
dialysis outside the body, and again returned to the natural
circulation without exposure to air, infection by micro-organisms or
any alteration which would necessarily prejudicial to life."
burette with hirudin solution
1913 - 1937: Anticoagulation as a Major Problem
Before 1916 hirudin extracted from the salvia
of leeches was the only practical
anticoagulant. Insufficient purification caused
major side effects and allergic reactions.
Hirudin was first identified in 1884.
In 1916 McLean isolated heparin as a
naturally occurring mammalian anticoagulant.
Haas (see next slide) used heparin in animal
experiments.
Use of heparin in human medicine became
a standard after appropriate purification
technology was available in 1937 (Murray et.
al).
Recombinant hirudin currently experiences a
come-back.

1945: The First Surviving Patient (1)
Willem Kolff Kolff´s rotating drum
dialyzer (1943, Kampen,
Netherlands)

Timeline: Major Achievements in Hemodialysis
1850 1860 1870 1880 1890 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000
Diffusive membrane
transport
First anticoagulant
(hirudin)
First animal
dialysis
First human
dialysis
First patient
surviving
due to
dialysis
First chronic
HD program
First high flux
dialyzer & related
machine
First single pass
machine for all
types of dialyzers
EPO
Polysulfone®
Natural occurring
mammalian anticoagulant
(heparin) for medical
application

Possibili usi del Personal Computer in una divisione di nefrologia e dialisi.
Santoro A. et. Al.
Attualità nefrologiche e dialitiche San Carlo 1984
– Patient archiving for administrative
purposes
– Computerised monitoring of
dialysis parameters
– Computerised clinical records
– Modelling and simulation
– Computerised control of dialysis
equipment

Automazione in dialisi
L’automazione come
informatizzazione di dati clinici e dati
macchina
L’informatica come controllo di
processi
L’ informatica nella gestione della
terapia dialitica : I biofeedbacks

Networking and connectivity
PC03 PC02 H
U
B
Local Network
Physician
Hospital Dialysis Centre Router 1
Router 2
Limited Care Centre
SERVER
PC01

Possibilità Attuali di
Monitoraggio della
Dialisi
• WHY ?
• WHEN
?
• HOW ? …. and what kind of results ?

Il monitoraggio in tempo reale
permette :
• di mantenere sotto continuo controllo
parametri fisiologici,biochimici ed
emodinamici
• di prevenire situazioni critiche
• di modificare in anello aperto o con
feedback automatici attuatori dialitici

PARAMETRI SUSCETTIBILI DI
MONITOROGGIO ON-LINE
Efficienza dialitica (Kt/V)
Volume Ematico
Stabilità pressoria
Ricircolo dell’accesso
Bilancio termico

Controllo automatico dei parametri fisiologici ... Un “pilota automatico” per l’emodialisi
HD
system
Dialysate
sensors
Blood
sensors
Patient
sensors
Modules
Monitor
Hydraulics
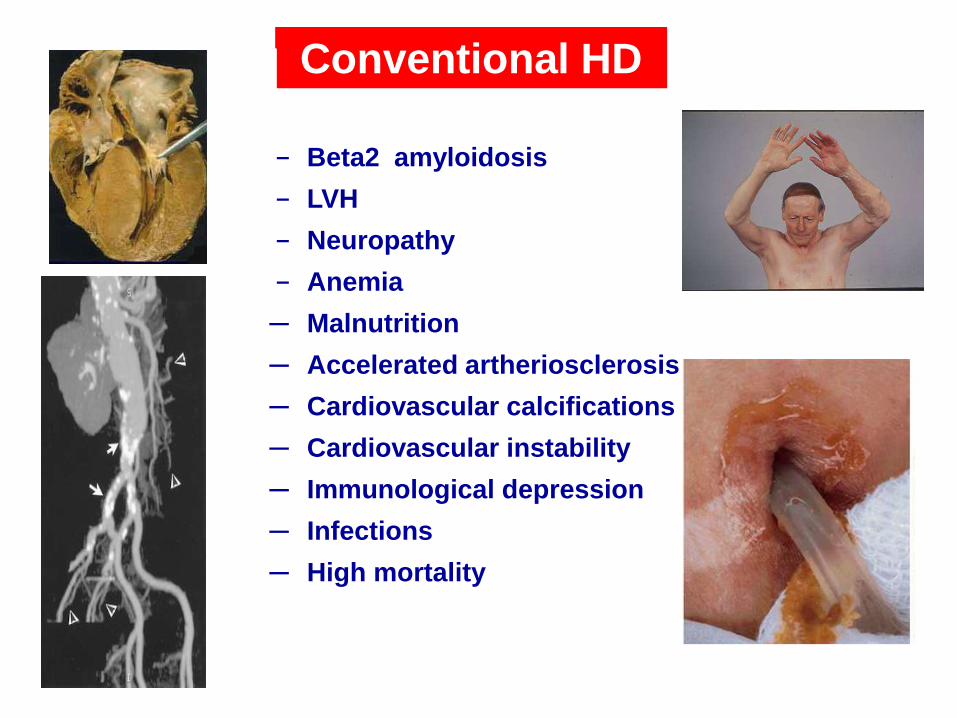
─ Beta2 amyloidosis
─ LVH
─ Neuropathy
─ Anemia
─ Malnutrition
─ Accelerated artheriosclerosis
─ Cardiovascular calcifications
─ Cardiovascular instability
─ Immunological depression
─ Infections
─ High mortality
Conventional HD

DIALYSIS MEMBRANE EVOLUTION
• Low-flux membranes
• High-flux membranes (pore size & water permeability)
• removal of MM
• removal of low MW proteins
• Superflux or Protein-leaking membranes • clearance for low MW prteins & small prrotein-bound
solutes (Homocystein, AGEP…)

High Cut-Off membrane
Cut-off ≈ 60.000 Dalton Increase in:
pore size
homogeneous pore distribution
Increase in membrane permeability
Transfer of protein-bound solutes

SUPERFLUX DIALYZERS
MAXIMISATITON OF THE CONVECTIVE
TRANSPORT BY INCREASING THE PRESSURE
DROP ALONG THE FIBERS
INCREASE IN PORE SIZE
INCREASE IN THE HOMOGENEOUS DISTRIBUTION
OF PORES
INCREASE THE MEMBRANE PERMEABILITY
TRANSFER OF LARGE TOXINS (PROTEIN-BOUND)

Dialyzer characteristics
Low-flux
polysulphone
(F60)
Low-flux triacetate
(Sureflux 150L)
High-flux triacetate
(FB-150U)
Super-flux
triacetate
(Sureflux 150FH)
Super-flux
polysulphone
(F500S)
Effective surface
area m2 1.3 1.5 1.5 1.5 1.2
Inner diameter, m 200 200 200 185 155
Membrane
thickness, m 40 15 15 15 35
Pore size, A 50 70 78
Ratio of open pores,
% 63 70 84
Sieving coefficient
2MG
0.65 0.36 0.88 1 0.9
UF coeff,
ml/mmHg,h 40 19 30 67 300 (H2O)

Van Tellingen A et al NDT 2004
25
20
15
10
5
0
-5
-10
-15
-20
-25
Plasma leptin
(ng/ml)
Week 1 week 12 week 1 week 12 week 1 week 12 week 1 week 12
F 6HPS TRICEA 15 G F 60S F 500S
Superflux dialyzers on leptin levels
Superflux
F500S
MW 160000 D

INFLAMMATORY MEDIATORS IN CONVENTIONAL CVVH
Mediator Molecular Weight (daltons)
Sieving Coefficient Clearance (ml/min)
Bradykinin 1,100
Endothelin 2,500 0.19
C3a / C5a 11,000 0.11-0.77
Factor D 24,000
LPS 67,000
LPS fragments < 1000 – 20,000
TNF- 50,000 0-0.2 3.6
sTNFr 30,000 – 50,000 <0.1
IL-1 17,500 0.07-0.42
IL-1ra 24,000 0.28-0.45 13.2
IL-6 22,000 1.2
IL-8 8,000 0-0.48 4.4
IL-10 18,000 0
INF- 20,000

Morgera S et al. Crit Care 2006
HIGH-CUTOFF HEMOFILTRATION IN
SEPSIS
0
200
400
600
800
1000
0
200
400
600
800
1000
0
1000
2000
3000
0
1000
2000
3000
p=0.0465
High cut off hemofilter (P2SH) Conventional hemofilter (PF 11S)
p=0.5506
p=0.0014 p=0.7789
Inte
rleu
kin
-6 [
pg/m
l]
Inte
rleu
kin
-1ra
[p
g/m
l]
Inte
rleu
kin
-1ra
[p
g/m
l]
Inte
rleu
kin
-6 [
pg/m
l]
High cut off hemofilter (P2SH)
Conventional hemofilter(PF 11S)
0 0
0 0 48
48 48
48
Time (hours)
Time (hours) Time (hours)
Time (hours)

SUPERFLUX FILTERS IN RHABDOMYOLYSIS
Naka T. Critical Care 2005,
Filter type UFR (L/h) Myoglobin Myoglobin
UF conc (g/L) removal (g/day)
Conventional 2 23.003 1.1
Superflux 2 >100.000 >4.8
Superflux 3 60.912 4.4
Superflux 4 53.527 5.

Meyer T W et al. Kidney Int 2004
Effect of protein binding on dialyzer solute clearance

REMOVAL OF FREE CIRCULATING LIGHT CHAINS (LC) BY
A HIGH CUT-OFF MEMBRANE: DIFFERENT DIALYSIS STRATEGIES
Sonia Pasquali , Elena Mancini, Antonio Santoro
and Collaborative Study Group on TheraliteTM HCO1100 in Myeloma.
Nephrology, Dialysis and Hypertension, Policlinico S.Orsola-Malpighi,
Bologna, Italy.
Eleven MM patients with high serum FLC levels (6 lambda/5 kappa; FLC=8,9±5,5 g/L),
were enrolled in an acute study where every patient was his/her own control.
HD HDF
Duration (h) 8 8
Filter Theralite HCO1100TM
QB (ml/min) 200 200
QD (ml/min) 500 500
QINF (ml/min) 0 33
Vascular Access Artero-venous fistula or dual lumen catheter (13F)
Heparin strategy Initial bolus, then continuous inrfusion, flow rate adjusted to
achieve the desired activated coagulation time (ACT, HemocronR)
Assessment of serum
and dialysate FLC
(FreeliteTM assay)
Basal, after 30, 60, 120, 240, 480 mins. and after 60 mins after end
of treatment.

Ultrafiltration Diffusion Convection Adsorbtion Plasmafiltration
BLOOD PURIFICATION PROCESS & THERAPIES
SCUF CVVHD CVVH PEX HP
CVVHDF
CPFA
Selective Plasmapheresis
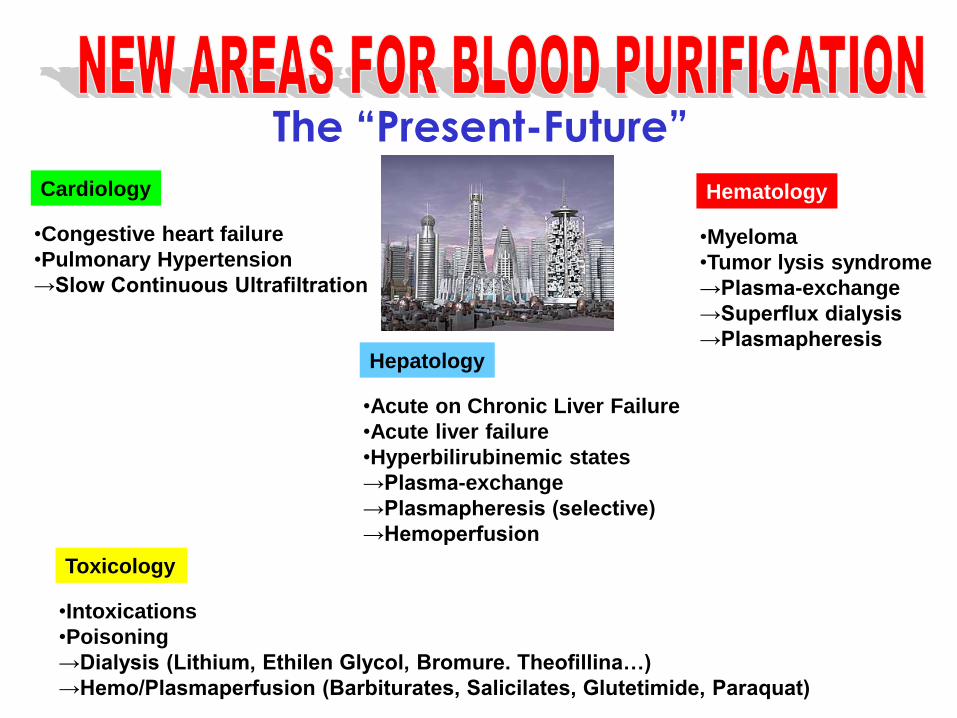
Cardiology
•Congestive heart failure
•Pulmonary Hypertension
→Slow Continuous Ultrafiltration
Hematology
•Myeloma
•Tumor lysis syndrome
→Plasma-exchange
→Superflux dialysis
→Plasmapheresis Hepatology
•Acute on Chronic Liver Failure
•Acute liver failure
•Hyperbilirubinemic states
→Plasma-exchange
→Plasmapheresis (selective)
→Hemoperfusion
Toxicology
•Intoxications
•Poisoning
→Dialysis (Lithium, Ethilen Glycol, Bromure. Theofillina…)
→Hemo/Plasmaperfusion (Barbiturates, Salicilates, Glutetimide, Paraquat)
The “Present-Future”

Pathways to Renal Replacement Therapy
Undiagnosed
Community
CKD
Known
Community
CKD
Kidney
Care
CKD or AKI in
Secondary Care
Centre/Satellite
HD/HDF/HF
Home HD
PD
Conservative
Care
Late
Referral
Timely
Referral
AKI
Trasplant
Conv. HD
Nocturnal
HD
Daily HD
6 times/week
HD (4 hrs.)
6 times/week
HD (8 hours)
3 times/wek
8 hours
WAK

The universe of innovations in dialysis
Different HD
schedules:
Frequency, Duration
Dialysis location:
In-center? Satellites ?
At home? WAK ?
Diffusion? Convection?
How much convection?
Absorption

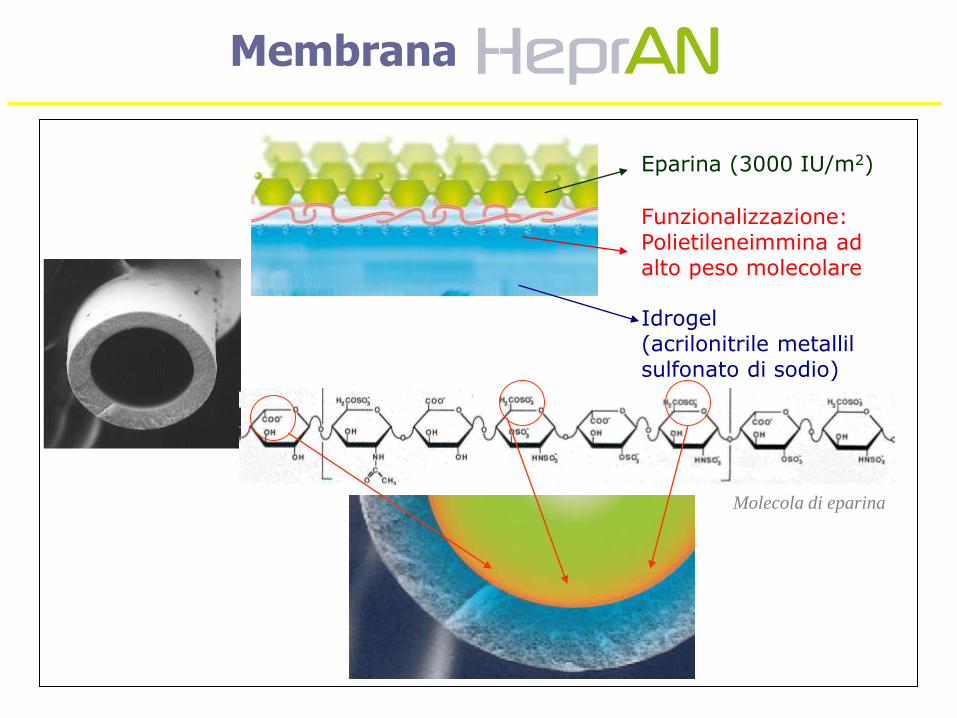
Molecola di eparina
Idrogel (acrilonitrile metallil sulfonato di sodio)
Eparina (3000 IU/m2)
Funzionalizzazione: Polietileneimmina ad alto peso molecolare
Membrana

• Attività anticoagulante mantenuta durante l’intera
sessione di dialisi (reversibilità dell’affinità eparina-TAT): – L’eparina esercita la sua attività anticoagulante legandosi
all’ATIII (anti-trombina III) – La configurazione di ATIII viene modificata dall’eparina – Si forma il complesso TAT che viene rilasciato nel circolo ematico – L’eparina rimane fissata alla membrana (alta affinità)
Bioattività dell’eparina graffata:
Membrana

CELL THERAPY, THE BIOARTIFICIAL
KIDNEY (BAK)
Tulim et al. JASN 2008

• Immunoregulatory role of tubule cells:
– Glutathione peroxidase synthesis
– Glutathione reclamation
– Activation of Vit D3
• Immunological actions of proxymal tubular cells:
– Antigen-presenting cells
– Synthesis and process of inflammatory cytokines
Propensity of patients with ARF to develop SIRS and sepsis
Renal tubule cell therapy: potential mechanisms of
action in ARF
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
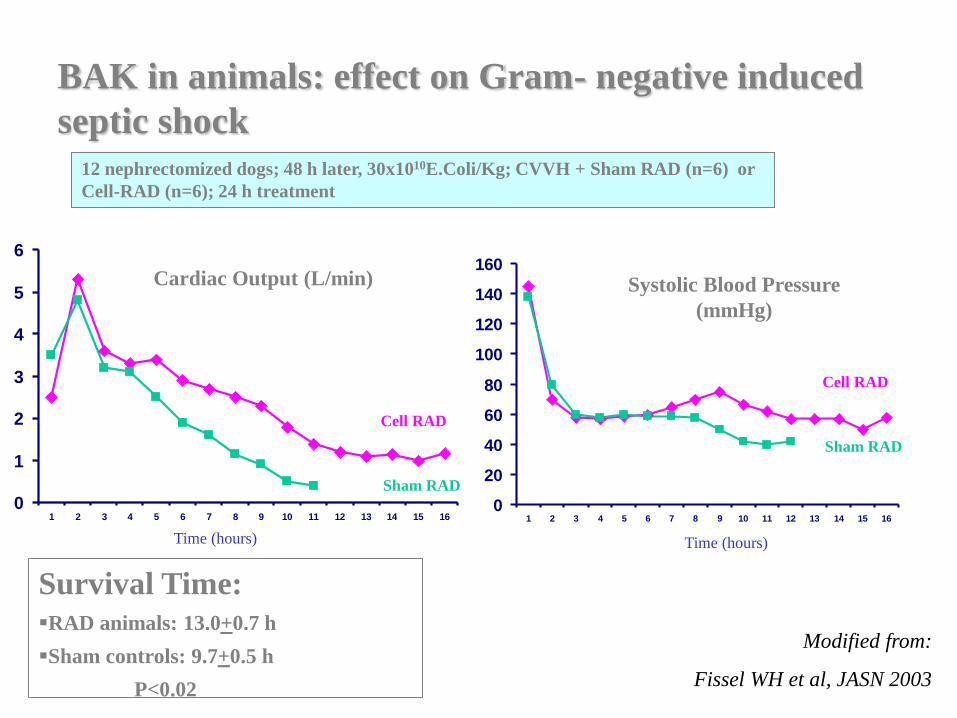
BAK in animals: effect on Gram- negative induced
septic shock
12 nephrectomized dogs; 48 h later, 30x1010E.Coli/Kg; CVVH + Sham RAD (n=6) or
Cell-RAD (n=6); 24 h treatment
Survival Time:
RAD animals: 13.0+0.7 h
Sham controls: 9.7+0.5 h
P<0.02
Time (hours)
Cardiac Output (L/min)
Cell RAD
Sham RAD
0
20
40
60
80
100
120
140
160
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Time (hours)
Systolic Blood Pressure
(mmHg)
Cell RAD
Sham RAD
Modified from:
Fissel WH et al, JASN 2003
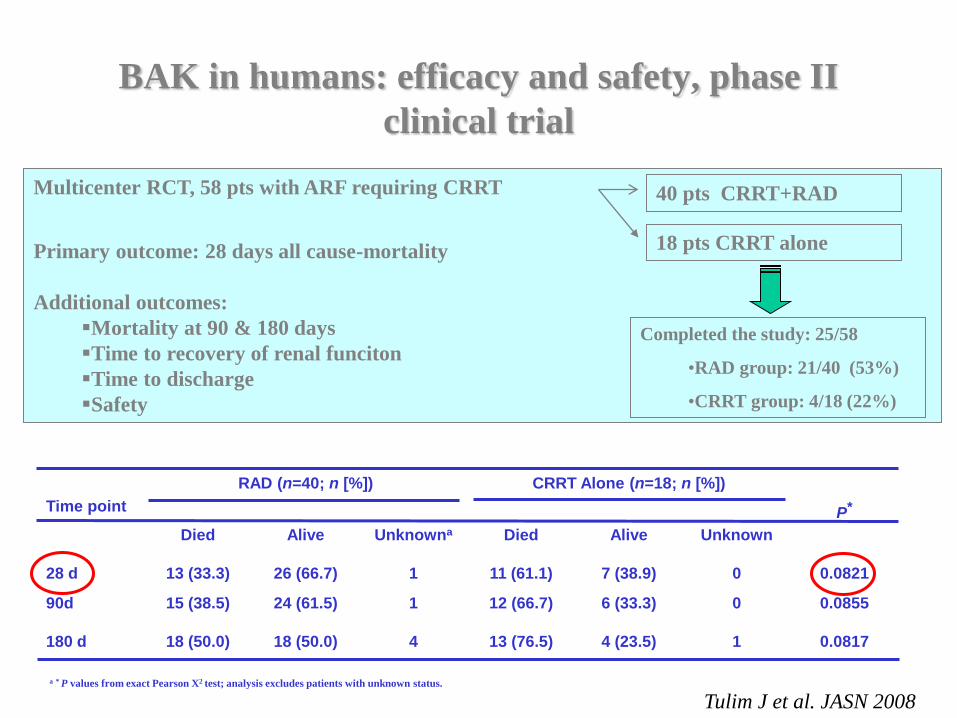
Tulim J et al. JASN 2008
BAK in humans: efficacy and safety, phase II
clinical trial
Multicenter RCT, 58 pts with ARF requiring CRRT
Primary outcome: 28 days all cause-mortality
Additional outcomes:
Mortality at 90 & 180 days
Time to recovery of renal funciton
Time to discharge
Safety
40 pts CRRT+RAD
18 pts CRRT alone
Completed the study: 25/58
•RAD group: 21/40 (53%)
•CRRT group: 4/18 (22%)
Time point
RAD (n=40; n [%]) CRRT Alone (n=18; n [%])
P* Died Alive Unknowna Died Alive Unknown
28 d 13 (33.3) 26 (66.7) 1 11 (61.1) 7 (38.9) 0 0.0821
90d 15 (38.5) 24 (61.5) 1 12 (66.7) 6 (33.3) 0 0.0855
180 d 18 (50.0) 18 (50.0) 4 13 (76.5) 4 (23.5) 1 0.0817
a * P values from exact Pearson X2 test; analysis excludes patients with unknown status.

Tulim J et al. JASN 2008
BAK in humans: survival
HR for death, adjusted for disease cause:
RAD group vs CRRT alone:
0.481 (CI 0.23-0.99)

La Dialisi Peritoneale è una DIALISI
DOMICILIARE
Può essere eseguita con modalita’
manuale (CAPD)
automatizzata (APD)
E’ rivolta a :
Pazienti in grado gestire autonomamente
il trattamento
Pazienti affiancati da un partner
efficiente LA DIALISI PERITONEALE PRESUPPONE LA
PRESENZA DI GRANDE AUTONOMIA
GESTIONALE
GRANDE CONTROLLO
CENTRALE

1. L’ icodestrina è un polimero del glucosio che viene
idrolizzato a maltosio a livello intraperitoneale.
2. Capacità di ultrafiltrazione elevata e prolungata nel
tempo, grazie ad una ridotta back-diffusion dalla cavità
peritoneale alla circolazione sanguigna
3. Basso contenuto di glucosio e conseguentemente ridotta
produzione di prodotti di degradazione del glucosio
4. Monoscambio quotidiano, con notevole riduzione dei
rischi legati alla manovra per se
L’ICODESTRINA

1200
900
600
300
0
UF netta (ml)
1,5% 4,25% 7,5% 7,5%
Paz. con alta UF
Paz. con bassa UF
Pannekeet MM et al, KI 1996;50:979-986
Glucosio
Icodestrina

Years Years
Years
2 4 6 8 10 0
20%
0%
40%
60%
80%
100%
1981 - 1985
Graft Survival by Era
Kidney trasplantation

73
Trapianto di Rene e Rigetto Acuto
Zand M, Seminars in Dialysis, 2005
0
40
80
100
%
‘60 ‘65 ‘70 ‘75 ‘80 ‘85 ‘90 ‘95 ‘00 ‘05
Years
20
60
Rejection < 12 mo

74
Immunosoppressione Clinica e Trapianto
Steroidi
Azatioprina
Abs Policlonali
Ciclosporina
OKT3
Tacrolimus
Micofenolato
Rapamicina
Everolimus
Ab Monoclonali
Thymoglobulne
1955 1960 1970 1980 1990 1995 2000
Myfortic
Advagraf
CP 690-550
FTY 720
Alemtuzumab
Rituximab
Belatacept
AEB
……..
2004 2008
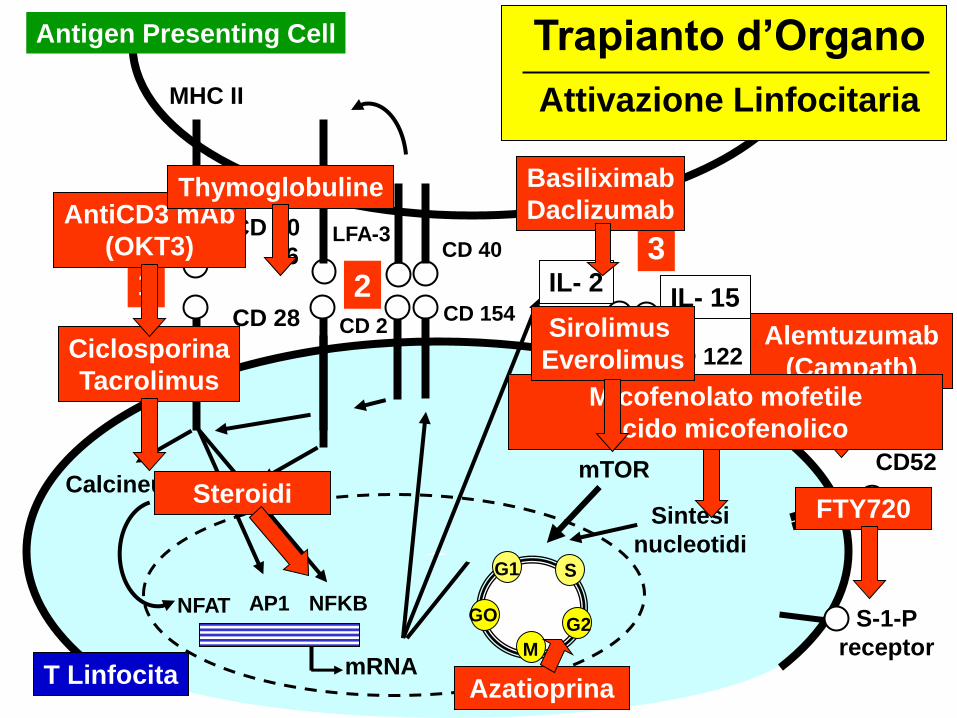
Antigen Presenting Cell
MHC II
T Linfocita
mTOR
CD 40 CD 80
86
CD 3
G1
M
G2
S
GO AP1 NFKB
mRNA
Calcineurina
CD 28 CD 154
IL- 2 IL- 15
CD 25
NFAT
CD52 JAK3
1 3
2
S-1-P
receptor
CD 122
Sintesi
nucleotidi
PKC Steroidi
LFA-3
CD 2
Azatioprina
Ciclosporina
Tacrolimus
AntiCD3 mAb
(OKT3)
Basiliximab
Daclizumab
Alemtuzumab
(Campath)
FTY720
Micofenolato mofetile
Acido micofenolico
Sirolimus
Everolimus
Thymoglobuline
Trapianto d’Organo
Attivazione Linfocitaria

Nanoscienza
Biomimetica
Nanotecnologia
Nanomedicina
Nanostrutture

La nanotecnologia è un ramo della scienza applicata e
della tecnologia che si occupa del controllo della
materia su scala dimensionale inferiore al micrometro
(in genere tra 1 e 100 nanometri) e della progettazione
e realizzazione di dispositivi in tale scala.
Il termine "nanotecnologia" indica genericamente la
manipolazione della materia a livello atomico e
molecolare.
Rappresentazione al
computer di un "ingranaggio"
di dimensione nanometrica

J Biolog Chem, 2005
Shen LJ, Int J Nanom, 2007
Panchapakesan U, Int J Nanom, 2007
Pickup J, Diab Metab researc Rev, 2008


Realistic Perspectives
Cli
nic
al E
ffecti
ven
ess
Acceptable range
Minumum
standard
Cost
Achievable based on local
resource and priorities
Best practice: optimum clinical
and cost effectiveness
Gold standard: maximal clinical
but reduced cost effectiveness