leaks and obstruction after gastric resection
TRANSCRIPT

Leaks and Obstruction After Gastric Resection
Wahwd Ahmad, MD, Louisville, Kentucky
Phil J. Ha&m&t, MD, Louisville, Kentucky
Hiram C. Polk, Jr., MD, Louisville, Kentucky
There has been a decrease in the use of gastric resection for the treatment of peptic ulcer disease. Less frequent occurrence of the disease and the widespread use of HZ receptor antagonists [I] may be responsible in part, but the type of primary oper- ation has also changed since the introduction of various kinds of vagotomies [2,3]. Despite these changes, gastric resection is still a proved modality for the treatment of recalcitrant peptic ulcer disease and of neoplasms of the stomach. Leaks and ob- structions are dreaded complications of gastric re- section [4,5] but are seldom described in the current literature. In addition, what is found in the older literature is often controversial. Herein, we present a review of these complications of gastric resection to update the literature and to clarify some of the controversial issues.
Material and Methods
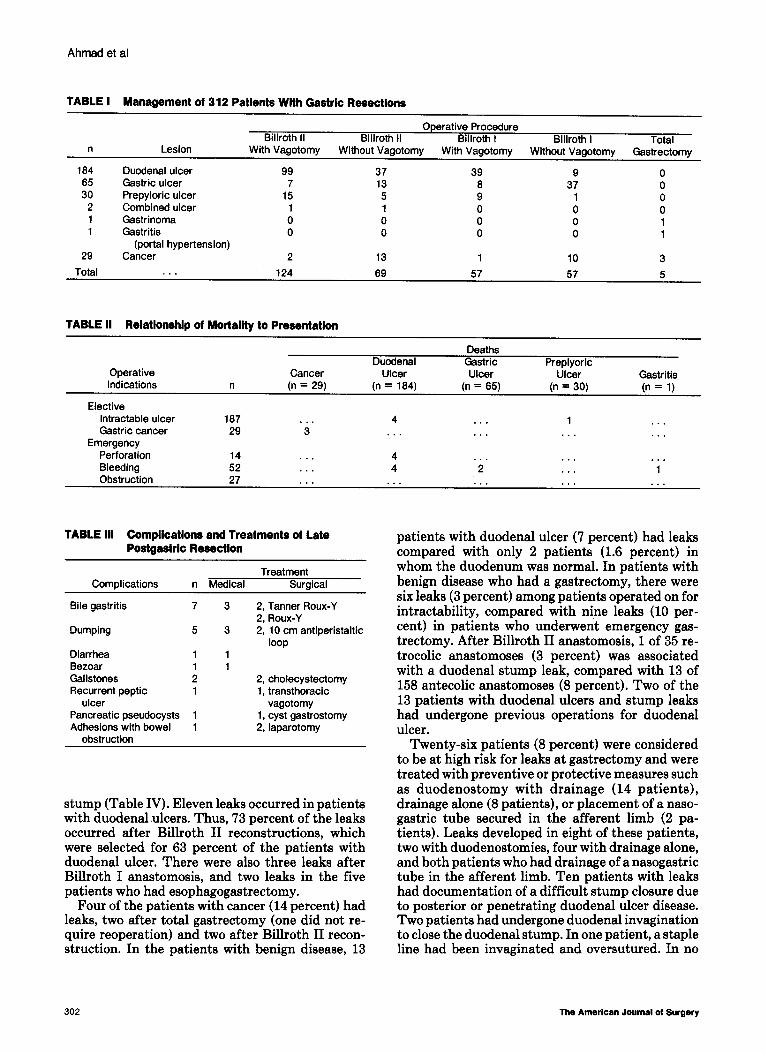
A retrospective review was undertaken at the Veterans Administration Medical Center in Louisville, Kentucky, to study 312 gastric resections (307 partial and 5 total) performed between 1968 and 1978. All patients were men, and their ages ranged from 30 to 70 years. Operative data are summarized in Table I.
Of these 312 gastric resections, the most frequent indications (listed in order) were duodenal ulcer, gastric ulcer, prepyloric ulcer, and gastric cancer. Vagotomy was performed in 181 patients, and conti- nuity was restored with a Billroth II anastomosis in 193 patients, a Billroth I anastomosis in 114 pa-
From the Department of Surgery, University of Louisville School of Medi- cine, Louisville, Kentucky.
Requests for reprints should be addressed to Waheed Ahmad, MD, Department of Surgery, Ambulatory Care Building, University of Louisville, Louisville. Kentucky 40292.
tients, and esophagojejunostomy in 5 patients. Bill- roth II reconstructions were associated with vagoto- my in 64 percent of the patients. The Hoffmeister modification was often used and was placed in the antecolic position in 82 percent of the patients. Bill- roth I reconstructions were divided equally into those with and without vagotomy. In most in- stances, the Shoemaker modification was used.
Indications for gastric resection in patients with duodenal ulcers were perforation (11 patients), ob- struction (23 patients), bleeding (26 patients), and intractability (124 patients); for patients with gas- tric ulcers, obstruction (1 patient), perforation (2 patients), bleeding (15 patients), and intractability (16 patients); and for patients with prepyloric ul- cers, perforation (1 patient), obstruction (3 pa- tients), bleeding (10 patients), and intractability (16 patients). Mortality rates were highest when resec- tion was necessitated by cancer (10 percent), bleed- ing (15 percent), and perforation (28 percent) (Ta- ble II). The mortality rate for elective operations in patients with benign duodenal ulcers was 3.2 per- cent, and it was exactly half that for elective opera- tions on benign gastric and prepyloric ulcers when the duodenum appeared normal. The mortality rate for emergency resections for benign disease was 12 percent.
Early complications after gastric resection in- cluded leaks in 19 patients; obstruction in 12 pa- tients; pneumonia, myocardial infarction, peritoni- tis, and intraperitoneal bleeding in 3 patients each; splenic injury in 2 patients; and gastrointestinal bleeding and gastrocolic fistula in 1 patient each. Late postoperative complications and treatments required are listed in Table III.
Leaks: Nineteen leaks (6 percent) were observed after gastric resection, 14 of which occurred after Billroth II anastomosis and were from the duodenal
Volume 152, September 1986 301
Ahmad et al
TABLE I Management of 312 Patients With Gastric Resections
n Lesion Billroth II
With Vagotomy
Operative Procedure Billroth II Billroth I Billroth I Total
Without Vagotomy With Vagotomy Without Vagotomy Gastrectomy
184 Duodenal ulcer 99 37 39 9 0 65 Gastric ulcer 7 13 8 37 0 30 Prepyloric ulcer 15 5 9 1 0
2 Combined ulcer 1 1 0 0 0 1 Gastrinoma 0 0 0 0 1 1 Gastritis 0 0 0 0 1
(portal hypertension)
29 Cancer 2 13 1 10 3
Total . . 124 69 57 57 5
TABLE II Relatlonshlp ot Mortality to Presentation
Operative Indications
Deaths Duodenal Gastric Preplyoric
Cancer Ulcer Ulcer Ulcer Gastritis n (n = 29) (n = 184) (n = 65) (n = 30) (n= 1)
Elective Intractable ulcer Gastric cancer
Emergency Perforation Bleeding Obstruction
187 . . . 4 . . . 1 . . . 29 3 . . . . . . . . . .
14 . . . 4 . . . . . . . . 52 . . 4 2 . . . 1 27 . . . . . . . . . . . . . .
TABLE Ill Complications and Treatments ol Late Postgastric Resection
Complications
Bile gastritis
n -
7
Dumping 5
Diarrhea Bezoar Gallstones Recurrent peptic
ulcer Pancreatic pseudocysts Adhesions with bowel
obstruction
Treatment Medical Surgical
3 2, Tanner Roux-Y 2, Roux-Y
3 2, 10 cm antiperistaltic loop
1 1
2, cholecystectomy 1, transthoracic
vagotomy 1, cyst gastrostomy 2, laparotomy
stump (Table IV). Eleven leaks occurred in patients with duodenal ulcers. Thus, 73 percent of the leaks occurred after Billroth II reconstructions, which were selected for 63 percent of the patients with duodenal ulcer. There were also three leaks after Billroth I anastomosis, and two leaks in the five patients who had esophagogastrectomy.
Four of the patients with cancer (14 percent) had leaks, two after total gastrectomy (one did not re- quire reoperation) and two after Billroth II recon- struction. In the patients with benign disease, 13
patients with duodenal ulcer (7 percent) had leaks compared with only 2 patients (1.6 percent) in whom the duodenum was normal. In patients with benign disease who had a gastrectomy, there were six leaks (3 percent) among patients operated on for intractability, compared with nine leaks (10 per- cent) in patients who underwent emergency gas- trectomy. After Billroth II anastomosis, 1 of 35 re- trocolic anastomoses (3 percent) was associated with a duodenal stump leak, compared with 13 of 158 antecolic anastomoses (8 percent). Two of the 13 patients with duodenal ulcers and stump leaks had undergone previous operations for duodenal ulcer.
Twenty-six patients (8 percent) were considered to be at high risk for leaks at gastrectomy and were treated with preventive or protective measures such as duodenostomy with drainage (14 patients), drainage alone (8 patients), or placement of a naso- gastric tube secured in the afferent limb (2 pa- tients). Leaks developed in eight of these patients, two with duodenostomies, four with drainage alone, and both patients who had drainage of a nasogastric tube in the afferent limb. Ten patients with leaks had documentation of a difficult stump closure due to posterior or penetrating duodenal ulcer disease. Two patients had undergone duodenal invagination to close the duodenal stump. In one patient, a staple line had been invaginated and oversutured. In no
302 The American Journal of Surgery

Leaks and Obstruction After Gastric Resection
TABLE IV Relationshlp of Leaks to Operatlve Procedure and Inltlal Disease’
Procedure Performed
Operative Pts Bilkoth II Billroth I Total Gastrectomies
Indications (n) Leaks Procedures Leaks Procedures Leaks Procedures
Duodenal ulcer Elective 124 5 84 0 40 . . ~ . Emergency 60 6 52 2 a . . . . . .
Gastric ulcer Elective 47 0 16 1 31 . . , . . Emergency 18 0 4 0 14 . . . . . .
Prepyloric ulcer Elective 16 0 11 0 5 . . , . Emergency 14 1 9 0 5 . . .
Cancer Elective 29 2 26 * . . . . . 2 3
l No leaks were found after operations for combined ulcers in two patients, gastrinoma in one patient, and gastritis in one patient.
patient was a mechanical defect identified at the termination of the afferent limb.
Evidence of the leak occurred within 5 to 21 days in 18 patients (average 10 days). Curiously, one patient presented 1 year later with a subphrenic abscess at the duodenal stump which represented chronic leakage. In 14 patients, the presenting symptoms were high fever, leukocytosis, and ab- dominal pain. Pleural effusion was the initial sign in three patients, and jaundice was the initial sign in one patient. One patient with an esophagojejunos- tomy had a controlled leak that was treated conser- vatively, and the patient recovered. The other 18 patients all needed drainage or improvement of drainage, and 6 needed more than one reoperation. Two patients had a duodenostomy in addition to external drainage.
The total duration of hospital stay for surviving patients was 1 to 2 months for 12 patients and more than 2 months for 2 patients. Five of the patients with leaks (26 percent) died as a result of uncon- trolled sepsis, and these accounted for one fourth of the postoperative deaths after gastrectomy. Two of the surviving patients had persistent duodenal fis- tulas which needed excision at later elective opera- tion. Data regarding the 19 patients with leaks are listed in Table V.
Gastric retention and obstruction: Twelve cases of postoperative gastric outlet obstruction [6-8] were observed for an overall incidence of 4 percent (Table VI). Four obstructions occurred af- ter Billroth I reconstruction without vagotomy, four after Billroth I reconstruction with vagotomy, and four after Billroth II reconstruction with vagotomy. There was no incidence of obstruction after Billroth II reconstruction without vagotomy or after total gastrectomy. All but one of the obstructions fol- lowed operation for duodenal ulcer. Four patients had emergency operations.
Three of four patients with obstruction after Bill- roth II reconstruction with vagotomy and all of the
patients with retrocolic anastomoses had a mechan- ical cause for their complications and required early reoperation. In two of the three patients, sutures from the mesocolon to the stomach had disinte- grated and the gastrojejunostomy was pulled up and twisted. Another patient was found to have a twist- ed gastrojejunostomy caused by a different mecha- nism. The fourth patient of this group with a vagot- omy and an antecolic anastomosis was conservative- ly treated, which resulted in remission.
Three of eight patients had early obstruction af- ter Billroth I anastomosis with vagotomy and re- sponded to prolonged nasogastric suction. Five oth- er patients presented at 7 months postoperatively or longer and required reoperation. Two-layer anasto- moses had previously been performed for duodenal ulcers that were not resected; in three, the anasto- moses included the edge of the ulcer and in another, the duodenum was noted as narrow. Four of these patients had conversion to a Billroth II anastomosis, and one had revision of a gastroduodenostomy.
Twenty-seven patients who previously had un- dergone operation for duodenal ulcer with preoper- ative obstruction underwent gastric resection as fol- lows: 1 Billroth I procedure, 2 Billroth I procedures with vagotomy, 7 Billroth II procedures, and 17 Billroth II procedures with vagotomy. Postopera- tive obstruction occurred in none of these patients, although vagotomy had been included in 19 of the operations.
Gastric retention and obstruction did not con- tribute to mortality in this series. All patients sur- vived and eventually improved after appropriate corrective treatment. Data regarding the 12 pa- tients with impaired gastric emptying are summa- rized in Table VII.
Comments
The use of surgery for the treatment of peptic ulcer disease was decreasing before the advent of the Hz receptor antagonists, although the latter ap-
Volume 152, September 1986 303

TA
BL
E V
D
etai
ls o
f 10
Lea
ks
in 1
9 P
atie
nts
Dia
gn
osi
s In
dic
atio
n
Op
erat
ion
C
om
men
ts
Dra
in
DD
T
ime
to L
eak
(d)
Man
agem
ent
Ou
tco
me
DU
O
bst
ruct
ion
DU
In
trac
tab
ility
RD
U
Ble
edin
g
DU
In
trac
tab
ility
DU
O
bst
ruct
ion
DU
P
erfo
rati
on
GU
In
trac
tab
ility
CA
C
A
CA
DU
DU
DU
Intr
acta
bili
ty
Intr
acta
bili
ty
Intr
acta
bili
ty
Intr
acta
bili
ty
Intr
acta
bili
ty
Bill
roth
II,
ante
colic
B
illro
th I
I, an
teco
lic
vag
oto
my
Bill
roth
II,
ante
colic
B
illro
th I
Po
ster
ior
ulc
er,
req
uir
ed N
isse
n m
aneu
ver
Sca
rrin
g,
dif
ficu
lt c
losu
re
No
Pen
rose
No
10
No
7
No
6
No
5
No
10
Ye
s 7
. . .
. . .
Bill
roth
II,
ante
colic
va
go
tom
y B
illro
th I
le
ak;
Bill
roth
II,
ante
colic
B
illro
th I
Mas
s ar
ou
nd
d
uo
den
um
D
iffi
cult
clo
sure
. .
Pen
rose
Su
mp
Dra
inag
e R
eco
vere
d
Dra
inag
e F
istu
la,
exci
sed
D
rain
age
Fis
tula
, ex
cise
d
Bill
roth
II,
Die
d f
rom
d
rain
age.
DD
fo
r le
ak
sep
sis
Dra
inag
e,
12th
rib
En
d D
D 8
d
rain
age
Rec
ove
red
Rec
ove
red
. .
No
21
R
eco
vere
d
Bill
roth
II
To
tal
gas
trec
tom
y T
ota
l g
astr
ecto
my
Bill
roth
II,
ante
colic
va
go
tom
y B
illro
th I
I, an
teco
lic
retr
oco
lic
vag
ato
my
Bill
roth
II,
ante
colic
va
go
tom
y
. . . . .
. . .
No
No
Dra
inag
e,
colo
sto
my
for
colo
n f
istu
la,
gas
tro
jeju
no
sto
my
for
ob
stru
ctio
n
Dra
inag
e D
rain
age
. .
No
E
xpec
tan
t
Dif
ficu
lt c
losu
re
Ye
s
Po
ster
ior
ulc
er,
nee
ded
Nis
sen
man
euve
r,
om
enta
l p
ou
ch
. .
Dif
ficu
lt c
losu
re,
om
enta
l co
ver
7 9 12
10
10 9
Dra
inag
e
. .
. D
rain
age,
tw
ice
Dra
inag
e tw
ice
Rec
ove
red
D
ied
Rec
ove
red
Die
d
Die
d
Rec
ove
red
DU
In
trac
tab
ility
D
U
Ob
stru
ctio
n
Bill
roth
II,
ante
colic
B
illro
th I
I, an
teco
lic
vag
oto
my
CA
PU
DU
Intr
acta
bili
ty
Ob
stru
ctio
n
Intr
acta
bili
ty
Per
fora
tio
n
Bill
roth
II,
ante
colic
va
go
tom
y B
illro
th I
I, an
teco
lic
vag
oto
my
Bill
roth
II,
ante
colic
va
go
tom
y B
illro
th I
I,
Om
enta
l co
ver,
d
iffi
cult
clo
sure
D
iffi
cult
clo
sure
Pen
rose
.
. . .
.
Su
mp
Pen
rose
. .
7 D
rain
age
Rec
ove
red
N
aso
gas
tric
7
Dra
inag
e R
eco
vere
d
tub
e, e
ffer
ent
limb
Yes
D
rain
age
Nas
og
astr
ic
limb
D
rain
age
. .
. . .
Dra
inag
e,
twic
e D
rain
age
Rec
ove
red
Rec
ove
red
Fis
tula
,
Dif
ficu
lt c
losu
re
8 7 1 yr
21
RD
U
. . .
ante
colic
va
go
tom
y
CA
=
can
cer;
DD
= d
uo
den
ost
om
y; D
U =
d
uo
den
al u
lcer
; G
U =
g
astr
ic u
lcer
; P
U =
p
rep
ylo
ric
ulc
er;
RD
U =
re
curr
ent
du
od
enal
ulc
er.

Leaks and Obstruction After Gastric Resection
TABLE VI Relationship ol Gastric Retention to Operative Procedure and lnltlal Disease*
Condition
Billroth II With Vagotomy
Patients With GR Procedures
Billroth II Without Vagotomy
Patients With GR Procedures
Billroth I With Vagotomy
Patients With GR Procedures
Billroth I Without Vagotomy
Patients With GR Procedures
Duodenal ulcer Elective 1 64 0 20 3 33 3 7
(n = 124) Emergency 2 35 0 17 1 6 1 2
(n = 60) Gastric ulcer
Elective 1 5 0 11 0 6 0 25
(n = 47) Emergency 0 2 0 2 0 2 0 12
(n = 16) Prepyloric ulcer
Elective 0 8 0 3 0 4 0 1
(n = 16) Emergency 0 7 0 2 0 5 0 0
(n = 14)
l There was no retention after operation for cancer in 29 patients, combined ulcer in 2 patients, gastrinoma in 1 patient, or gastritis in 1 pa- tient.
GR = gastric retention.
TABLE VII Details of Postoperatlve Obstructions In 12 Patients
Diagnosis Presentation Operation Time to Obstruction Treatment Comments
DU DU
DU
DU
DU
DU DU
DU DU
GU
DU
DU Intractability
Bleeding
Intractability
Intractability
Intractability
intractability Bleeding
Intractability Bleeding
Intractability
Intractability
Billroth I Billroth II,
antecolic vagotomy Billroth I
Billroth I, vagotomy
Billroth I, vagotomy
Billroth I Billroth I,
vagotomy Billroth I Billroth II,
retrocolic vagotomy Billroth II,
retrocolic vagotomy
Billroth I, vagotomy
Billroth II,
1 year Postop, poor emptying
7 months
Postop, poor emptying
6 years
7 months Postop, poor empyting
8 months Postop, obstruction
Postop, obstruction
Postop, poor emptying
Postop, obstruction
Billroth II, antecolic Nasogastric tube
Billroth II, antecolic
Nasogastric tube
Billroth I
Billroth II, antecolic Nasogastric tube
Billroth II Reoperation
Reoperation
Nasogastric tube
Reoperation
Recovered Recovered
Recovered, two-layer gastroduodenostomy
Recovered
Fibrosis
Recovered Recovered
Recovered Gastrojejunostomy
pulled up Gastrojejunostomy
pulled up and twisted, regastrojejunostomy
Recovered
Gastrojejunostomy pulled up retrocolic vagotomy
DU = duodenal ulcer; GU = gastric ulcer.
pear to have contributed to a further decrease in its use. Vagotomy and pyloroplasty have long been in competition with gastric resection as the operative treatments of choice in patients with duodenal ulcer [9]. In some centers, supraselective vagotomy is of- fered as an alternative [2,3]. These trends have de- creased the frequency of the use of gastric resection. In the presence of advanced duodenal ulcer, how- ever, vagotomy and antrectomy remain the most effective operations short of total gastrectomy. In
the presence of gastric ulcer or cancer, some form of resection is necessary. Although the overall inci- dence of complications after gastrectomy is less [6-14, it becomes necessary to ensure that the rela- tive incidence does not increase due to inattention to its problems.
Patients with gastric cancer are in a somewhat different category than those with benign peptic ulcers. Vagotomy was added to partial gastrectomy in only three such patients in our series. Duodenal
Volume 152,StqHember 1996 305

Ahmad et al
leaks developed in two of those patients after Bill- roth II anastomoses, and leaks developed in two of the three patients with cancer who received total gastrectomies. None of the cancer patients had postoperative obstruction.
The selection of operation for benign diseases reflected the opinions of the attending staff; how- ever, duodenal and prepyloric ulcers were consid- ered directly related to acid output, and vagotomy was added to the gastric resection by most surgeons. Gastric ulcer, on the other hand, was usually treated with resection without vagotomy.
Postoperative leaks accounted for approximately one fourth of the postoperative deaths and usually required one or more operations. Leaks were more common after emergency operations and occurred predominantly after difficult stump closures in op- erations for duodenal ulcer. Instances of afferent loop obstruction were not identified [IO]. The in- creased incidence of postoperative leaks after ante- colic anastomoses may be at least partially due to a preference of the staff for that type of anastomosis in difficult operations. When a high risk situation was recognized, no preventive measure was totally reliable, but duodenostomy achieved better results in 12 of 14 patients than drainage or intraluminal decompression [12,13].
No patient died from impairment of gastric emp- tying, but three patients with Billroth II procedures required early revision and five patients with Bill- roth I procedures required later revision. Obstruc- tion also occurred predominantly after resection for duodenal ulcer. Vagotomy in four patients, three of whom had Billroth I procedures, was associated with early retention that subsided with conservative treatment. However, vagotomy appeared to have no relationship to the need for reoperation in eight patients. The use of vagotomy in patients with pre- operative obstruction did not appear to adversely affect the results, although some staff members thought that vagotomy was contraindicated in such patients.
Complications in 103 patients with peptic ulcer disease who had Billroth I procedures included eight patients with obstruction, three patients with leaks, and one patient each with pneumonia, bile gastritis, dumping, and diarrhea. Three of these patients died. Complications in 178 patients with peptic ulcer disease who had Billroth II procedures included 12 patients with leaks, 6 patients with bile gastritis, 4 patients with obstruction, 2 patients each with pneumonia, splenic injury, and gallstones, and 1 patient each with recurrent ulcer and postop- erative hemorrhage. Twelve patients with this re- construction died. A comparison of these complica- tions suggests that leaks tend to occur in Billroth II procedures and obstruction tends to occur in Bill- roth I procedures [14,15]. The low incidence of su- ture line bleeding and clinically significant dumping
is noteworthy. Billroth I reconstruction was usually selected for patients with normal duodenums, and obstructions occurred only in the few patients with retained ulcers of the duodenum. A Billroth II pro- cedure was the usual choice in emergency situations and in patients with badly diseased duodenums, and these accounted for most of the mortality in this series.
The role of afferent loop obstruction in stump blowouts was recognized by the staff, and this recog- nition may have minimized the incidence of this complication. Difficult stump closure was avoided in some cases by pyloroplasty or gastrojejunostomy. When a difficult stump closure is unavoidable, the use of a tube duodenostomy through the side of the duodenum-not the closure line-is probably the best, if not an infallible, preventive measure 1131. External drainage permits earlier diagnosis but has no proved preventive value. Postoperatively, the less dramatic signs of leakage should be searched out. When a leak does occur, prompt and adequate drainage and augmentation of drainage are usually necessary, despite any previous operative precau- tions.
Summary
Postoperative gastric retention may be mini- mized by avoiding the use of the Billroth I recon- struction when a large duodenal ulcer must be re- tained. Postoperative gastric retention is more likely to remit with conservative therapy if the pro- cedure was a Billroth I reconstruction with a vagoto- my. In other instances where there is difficulty in gastric emptying, a mechanical cause should be strongly suspected. The optimum duration of a con- servative trial with suction for postoperative gastric retention may be debatable, and contrast radiogra- phy or endoscopy may be helpful; however, patience and suction are not long-term substitutes for a needed operation.
References
1. Gibson R, Hirschowitz Bi, Hutchinson G. Actions of metia- mide, an HP-histamine receptor antagonist, on gastric H+ and pepsin secretion in dogs. Gastroenterology 1974;67: 93-9.
2. Johnston D, Wilkinson AR. Highly selective vagotomy without a drainage procedure in the treatment of duodenal ulcer. Br J Surg 1970;57:289-96.
3. Sawyer JL, Scott HW Jr. Selective gastric vagotomy with antrectomy or pyioropiasty. Ann Surg 1971;174:541-7.
4. Pearce CW, Jordan GJ Jr, DeBakey ME. Intra-abdominal com- plications following distal subtotal gastrectomy for benign gastroduodenai ulceration. Surgery 1956;42:447-61.
5. Hardy JD. Problems associated with gastric surgery. A review of 604 consecutive patients with annotation. Am J Surg 1964;108:699-716.
6. Jordan GL Jr, Walker LL. Severe problems with gastric empty- ing after gastric surgery. Ann Surg 1973;177:660-6.
7. Cohen AM, Dttinger LW. Delayed gastric emptying following
306 The American Journal 01 Surgery

Leaks and Obstruction After Gastric Resection
gastrectomy. Ann Surg 1976; 184:689-96. 8. Donovan I, Alexander-Williams J. Postoperative gastric reten-
tion and delayed gastric emptying. Surg Clin North Am 1976;56:1413-9.
9. Farmer DA, Harrower HW, Smithwick RH. The choice of surgery in peptic ulcer disease. Am J Surg 1970;120: 295-305.
10. Buckberg GD. Acute obstruction of the afferent loop after gastrectomy. Am J Surg 1967;113:682-7.
11. Cooperman AM. Postgastrectomy syndromes. Surg Annu
1981;13:139-61. 12. Lamphier TA, Crooker C. Catheter duodenostomy for the
difficult duodenal stump. South Med J 1968;61:751-7. 13. Dardik I, Dardik H, Shumofsky E, Gliedman ML. Lateral T-tube
duodenostomy. Duodenal stump management and mano- metrics. Arch Surg 1973;107:89-90.
14. Jesseph JE. The trouble with Billroth II is Am J Surg 1974; 128:654-6.
15. Griffen WO Jr. Whither goest the duodenal stump blowout? Arch Surg 1973;107:11.
volume 152, -ember 1988 307