lean programme information session - nhs improvement · 6 lean programme: application to join...
TRANSCRIPT

Lean Programme Information Session
6 February 2018
Agenda
Welcome and Overview
Adam Sewell- Jones, Executive Director of
Improvement
14:00
The Application Process
Julie Fitzgerald, Head of Consultancy NHS
Improvement
14:30
Doing Lean: myths, realities
and practicalities
Bruce Gray, NHS Improvement Lean
Specialist 15:00
Our Lean Experience Louise Brennan, KPO specialist at SaTH 15:30
Questions, answers and
discussion All 16:00

Welcome and Overview
Adam Sewell-Jones
6 February 2018

The Application Process
Julie Fitzgerald
6 February 2018
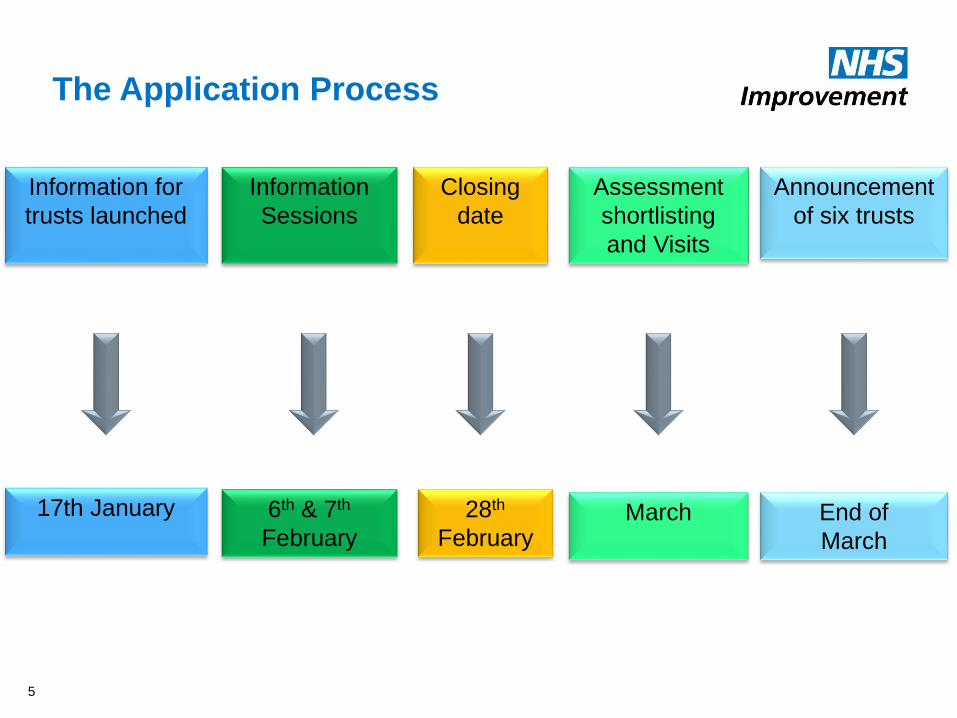
The Application Process
5
Information for
trusts launched
17th January
Information
Sessions
6th & 7th
February
Closing
date
28th
February
Assessment
shortlisting
and Visits
March
Announcement
of six trusts
End of
March

6
Lean programme: application to join cohort 1
Please fill in your details below (expanding the space below the questions to add your
answers – please try to keep each answer to 500 words maximum). Send your completed
application to [email protected] by midnight on Wednesday 28 February
2018.
Trust name:
Contact name for the programme:
Contact role:
Contact email:
Contact telephone:
Q1: Please explain why a lean approach to quality improvement is right for your trust’s development at
this time. What specifically do you want to achieve by implementing a lean management system?
A:
Circumstance of the trust
Understanding of lean
What are the drivers for implementing a lean management system
What do you perceive to be the benefits, risks and challenges of a lean management system for
your trust
Q2: Please describe the Board’s understanding of what the programme will deliver and specifically how it
will support delivery of the organisation’s existing strategy?
A:
What is the organisations’ existing strategy i.e to what extent is it built around QI
What is the Board’s understanding of a lean approach to delivering strategy
Describe the Board’s understanding of what lean transformation can deliver
Q3: Please set out how the trust Board and senior executive team will engage with the programme and
how the work will be integrated into the way the trust works. What commitment will the CEO, Executive
team and Board members make to ensure that a lean approach to management becomes the way the
organisation is run day-to-day?

7
A:
Understanding of the different management approach
Commitment to learning and adopting a different approach individually
Commitment to learning and adopting a different approach collectively
Willingness to support frontline staff in their improvement work and reduce/eliminate the barriers
that they will face
Commitment to release staff for training and improvement work
Q4: Please confirm that Executive team and Board members are able and willing to undertake the
necessary training associated with the introduction of a lean management system. We expect all
executives and non-executives to commit to leading in a different way, using lean management
techniques.
A:
Commitment to undertake training
Willingness to sponsor and get involved with RPIWs and other lean activities
Commitment to engage with Executive coaching around lean and personal effectiveness, so that
they become capable of coaching others
Understanding of implications of visible management and going to the genba
Q5: Board stability and long term commitment to the approach is a necessary condition for success.
Please describe the Board membership, non-executives’ length of time in office and remaining terms, and
any known upcoming changes, such as retirement or restructuring.
A:
Description of current state
Know or anticipated changes over next three years
Plans for changes in exec and non exec teams
Possibilities – horizon scanning
Q6: How is succession planned for both non-executive and executive members? Please describe how
commitment to a lean management system will be maintained over time.
A:
Will new recruits be asked to commit to this approach before appointment
Will lean training and induction be put in place as part of induction for new recruits
Q7: Please describe how the Board will approach securing clinical engagement and leadership in this
work?
A:
How is clinical engagement, medical and nursing secured in current work
Do you foresee any resistance from clinical colleagues and how would you plan to address this
Do you see any significant differences between current clinical engagement and that required for
lean transformation
If yes, how would you address this

8
Q8: How has the trust approached quality improvement previously, and has it had any previous
exposure to lean? What has been learnt from this and how will those lessons apply to the outcomes your
trust wants to achieve from this programme?
A: short summary
Q9: How is quality improvement work currently delivered in the trust? For example do you have a quality
improvement team in place?
A: short summary
What links are there between QI work and trust priorities/strategies
Q10: To secure long term organizational change, the trust will need to dedicate resources to operate the
management approach. What resources does the trust currently dedicate to facilitating and effecting
change? How will the trust resource the necessary requirements of the improvement and development
process?
A: short summary
Q11: If relevant, please describe how you would plan to implement lean and deliver this programme
across multiple sites.
A:
Ideas on priorities
Outline of challenges identified
Q12: Please outline any discussions the trust has had with its local health and care partners.
A: short summary
Q13: Please outline any other NHS Improvement programmes of work the trust is currently involved with.
A: short summary
Q14: Please confirm that you have included a copy of your Board-approved quality improvement
strategy.
A: attached

Doing Lean: myths, realities and practicalities
Bruce Gray
6 February 2018

Health Care – what is possible?
10
Virginia Mason Production System Success Stories
• Patient Safety Alert system
• reports used to take 3-18 months to resolve – most now processed <24hrs, as well
as increased patient safety & reduced professional liability claims.
• Nurses spend 90% with Patients Vs 35%
• Through using RPIWs to evaluate their work and make improvements
• Primary Care Achieves Positive Net Margins
• Turnaround time for lab results from 25 days for normal results to <2 days.
• Faster Revenue Cycle
• Days Revenue Outstanding in the clinic from 52.3 in 2003 to 29.4 in 2009
• (a US example, but a process is a process is a process)
• Hyperbaric Centre Increases Patient Capacity
• Used VMPS tools to design and build a new hyperbaric centre in existing hospital
space, saving $2m in construction costs and increased capacity from two to three
patients at a time, to as many as 20.
Ref: https://www.virginiamason.org/vmps#Benefits

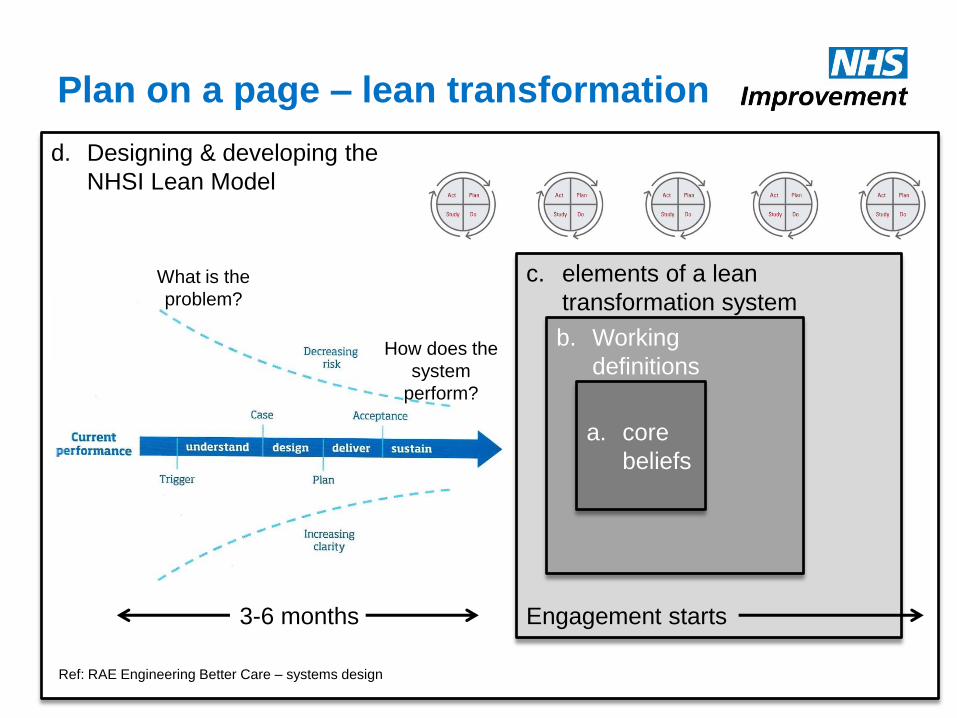
d. Designing & developing the
NHSI Lean Model
c. elements of a lean
transformation system
b. Working
definitions
Plan on a page – lean transformation
a. core
beliefs
Ref: RAE Engineering Better Care – systems design
3-6 months Engagement starts
What is the
problem?
How does the
system
perform?
a. Core beliefs
12
From Toyota Production System (TPS)
• Kaizen (practised daily) – change for the better.
• Respect for people (society & the environment).
From The Little Book of Lean – Chris Cooper
• Dissatisfaction with the status quo.
• Humility.
• A belief that Lean works wherever work is done.
• ‘Gemba’ wisdom that is valued over theoretical knowledge.
• Leadership that believes all of the above.

d. Designing & developing the
NHSI Lean Model
c. elements of a lean
transformation system
b. working
definitions
Plan on a page – lean transformation
a. core
beliefs
Ref: RAE Engineering Better Care – systems design
3-6 months Engagement starts
What is the
problem?
How does the
system
perform?

14
• Doing Lean:
– is the continuous improvement of the flow
of value via the elimination of waste by
the people who do the work, in their
workplace, under the caring guidance of
a teacher.
• Lean Transformation:
• Lean Leadership:
b. Working definitions – reflect…

Improvement will be easier and more likely to succeed by focussing
on & removing the non-value added activities (waste) than trying to
improve the value adding element
The 1st Big Idea
Typically in a process there is usually a very high proportion of wasteful activity
We often focus on the Value Adding parts because that is what we can see and measure
95% WASTE 5%
Value
Adding
Start
Identify the NeedEnd
Outcome
Non Value Adding

8 Wastes
16

17
• Doing Lean:
• Lean Transformation:
– changing the way an enterprise
approaches improvement and views its
potential, such that collectively, people
create ever-improving results and a
culture in which Lean principles are
routinely practiced and supported forever.
• Lean Leadership:
b. Working definitions – reflect…
2nd Big Idea – by the people who do the work
18

19
• Doing Lean:
• Lean Transformation:
• Lean Leadership:
– the creation of direction that results in an
environment in which every member of
the enterprise is nurtured and
encouraged to practise Lean principle-
based improvement in support of True
North goals (Human Development, Quality, Time &
Financial).
b. Working definitions – reflect…

2. Environment – Culture – Basic Thinking
5. Process
Improvement
3. People
Capacity
Capability
Development
1. Purpose and Strategy
4. Role of leaders and Mgrs.
- Management system
- Leadership behaviors
“You Don’t Understand Our Culture Here!”
Beliefs, behaviours & culture

c. Diagnostic & strategy deployment
Mission, values, guiding principles
Strategy
Diagnostic
Current State Ideal State (3-5 years)
Future State Plan for next 12-18 months
RIEs to get building
blocks of flow in place
Practising daily
improvement (PDI)
KPO
Level 3
Level 2
Level 1
Board
Staff

d. Designing & developing the
NHSI Lean Model
c. elements of a lean
transformation system
b. Working
definitions
Plan on a page – lean transformation
a. core
beliefs
Ref: RAE Engineering Better Care – systems design
3-6 months Engagement starts
What is the
problem?
How does the
system
perform?

c. Elements of a lean transformation
system
23
• Kaizen Promotion Office
– Training/coaching/leading to develop capacity and capability.
– Establishes and runs schedule of daily, weekly, monthly, quarterly, and
annual activities, e.g. Rapid Improvement Events (RIEs), A3s,
reporting.
– Establishes and maintains benefits and impact tracking.
– Co-leads RIEs – preparation, event week, 30/60/90 day follow-up.
– Improvement and Coaching ‘routines’.
– Coaches ‘Practising Daily Improvement’.
• Value stream identification and analysis
• Flow cells (1 piece flow, standard work, pull systems, 6S).
• Visual management.
• Strategy alignment and organisation-scale PDSA (level 1)

Value Stream Analysis – Current State
24

Value Stream Analysis - Future State
25
• Day 2 & 3
• Define the process vision based on their experience and lean principles
• Define the “cell building blocks” for process control and continuous improvement
• Estimate the benefits
• Define an implementation plan
• Get senior leadership endorsement

26
Future State through RIEs and daily
improvement
7 Week RIE Cycle
27

RIE week
• 1 week facilitated workshops
• Assemble cross functional team
• Deliver that week at the workplace and learn by doing
• Deliver performance improvement using Lean tools to establish cells
• Train for daily improvement – PDCA cycle
– Scientific method (develop a thesis (idea for improvement), Conduct experiment, review results, implement of successful
• Define a plan to develop the team
• Define staff and leadership standard work to sustain
Results in the week!

Q: what runs through lean like letters
through a stick of rock?
A: problem-solving…

From the patient’s perspective, value comes
not from parts, but from the whole
30

Problem-solving is closing the gap between
A & B - clinicians are partway there
31
Clinical activity for a patient
• A: what we have
– illness, exacerbations, long-
term condition etc.
– stabilise, diagnostics, root
cause via differential diagnosis
– management plan
– diagnostics + revisions
• B: what we want
– gap closed, or at least reduced
– patient condition improved

32
Clinical activity for a patient
• A: what we have
– illness, exacerbations, long-term condition etc.
– stabilise, diagnostics, root cause via differential diagnosis
– management plan
– diagnostics + revisions
• B: what we want
– gap closed, or at least reduced
– patient condition improved
Problem-solving is closing the gap between
A & B - clinicians are partway there

33
Problem-solving is closing the gap between
A & B - clinicians are partway there
Clinical activity for a patient
• A: what we have
– illness, exacerbations, long-term condition etc.
– stabilise, diagnostics, root cause via differential diagnosis
– management plan
– diagnostics + revisions
• B: what we want
– gap closed, or at least reduced
– patient condition improved
Operational activity for a process
• A: what we have
– 8 wastes (T.I.M.W.O.O.D + waste
of human creativity)
– Stabilise, diagnostics, root cause
via data analysis & small tests
– PDSA plan
– diagnostics + revisions
• B: what we want
– gap closed, or at least reduced

34
Problem-solving is closing the gap between
A & B - clinicians are partway there
Clinical activity for a patient
• A: what we have
– illness, exacerbations, long-term condition etc.
– stabilise, diagnostics, root cause via differential diagnosis
– management plan
– diagnostics + revisions
• B: what we want
– gap closed, or at least reduced
– patient condition improved
Operational activity for a process
• A: what we have
– 8 wastes (T.I.M.W.O.O.D + waste
of human creativity)
– Stabilise, diagnostics, root cause
via data analysis & small tests
– PDSA plan
– diagnostics + revisions
• B: what we want
– gap closed, or at least reduced

A3 – problem-solving method 2 3 4 5 6 7 8 9 1
Start Date: Current Date:
End Date:
Title:
Process Owner:
Sensei:
4. Gap Analysis No GoGo
Problem Statement:
Reflections:Root Cause:
5. Solution Approach
Reflections:
No GoGo
Text
Cause/Priority Solution Affecting Current State FS E C
1 O ∆2
3
4
5
6
E (ease) and C (cost) scoring
O = Easy / Low Cost, ∆ =Medium / Medium Cost, X = Hard / High Cost
6. Rapid Experiments
Reflections:
No GoGo
Text
Experiment Anticipated Effect Actual Effect Follow up Action
7. Completion Plans
Reflections:
No GoGo
Text
Action TT Owner Due RAG
8. Confirmed State
Reflections:
No GoGo
Text
9. Insights
Reflections:
No GoGo
Text
What went well?
What helped? What hindered?
Even better if…Actions:
Team Photo
1. Reason for Action
Reflections:
No Go Go
What might it look like:
a.
Business Case:
In scope:
Out of scope:
2. Initial State
Reflections:
No Go Go
Text
(a) Delivery / Timeliness
(c) Quality
(b) Cost
(d) Human
3. Target State
Reflections:
No Go Go
(a) Delivery / Timeliness (b) Cost
(c) Quality (d) Human
!Show!ME!Improvement!!
!showmeimprovement.com!
Business'improvement'you'will'see'
A3…practice, practice, practice

A system of systems, so act
on the system
36
• Do an RIE week in an Out Patient clinic
– Increases throughput by +10% (11 pts not 10)
– Over the year + 10% additions to theatre lists
– +10% to recovery, to wards, to AHPs, to discharge teams
– Understand and ‘see’ the end-to-end patient journey
– Have to work across the value stream in a coordinated way = why you need a KPO and constancy of purpose

Isolated islands of improvement, or…
Lean Leadership of org towards True North goals?
d. Designing & developing the
NHSI Lean Model
c. elements of a lean
transformation system
b. Working
definitions
Plan on a page – lean transformation
a. core
beliefs
Ref: RAE Engineering Better Care – systems design
3-6 months Engagement starts
What is the
problem?
How does the
system
perform?

39
d. Designing & developing the
NHSI Lean Transformation model
• Inputs – Interviews with lean
transformation orgs
– Developing People,
Improving Care
– Benefits defined, valued,
measured and tracked
– Transformation FMEA
– How KPO is setup & run –
‘Big Room’ ideas?
– Baseline H, Q, C/P, T
– Transactional Analysis
training for Lean team
– Social movement
knowledge
– Other QI methods (IHI-QI,
Theory of Constraints, 6
Sigma, etc.)
• Process – A guiding coalition of:
– NHSE/I
– VMI trusts
– NHS trusts/orgs that are
working on Lean & QI
– Lean orgs/leaders outside
of NHS and healthcare
– Lean ‘gurus’
– Health Foundation etc
– Royal Colleges
– Use the ‘Engineering Better
Care’ system design model
(Royal Academy of Eng.)
– Cambridge University
Engineering Dept
– Large Scale Change &
NHS Change Model
• Outputs – Training material
– Standard work
– KPO
– Leaders/staff
– Events &
– Review schedule
– Diagnostic method
– Selection of work
– Lean strategy
– Improvement & coaching
routines
– Plan across 6 trusts
– Cross-client cover
– ‘Review and improve’
schedule
– JD & PS for KPO team
members

What precisely does 200k buy?
40
• Personal commitment and leadership of programme from Executive Director of Improvement = financial input.
• Full access to tools and training materials, no on-going cost.
• 0.5 FTE per trust with consultants working across 2 trusts, but with opportunities for training etc. maximised across the cohort.
• Input from Director of Lean and Lean Specialists to coach KPO leads, as well as targeted work with CEOs, leadership teams and boards.
• Bringing CEOs, Boards, leadership teams and KPOs together for events and learning – cohort.
• Connection into trusts working in partnership with VMI and other trusts working with lean in the NHS.
• Opportunity to co-design the NHS lean transformation method.
• Support with setting up and developing programme management, stakeholder management and reporting.
• Coordination of work problem solving.
• Point of contact at NHSI.

We need to talk about money!
• Hands up if you think lean works like this.

It’s not a tool for CIP
• Reducing/removing waste does not
automatically equate to cash out of the till…

You’re all good at CIP because you've been
doing it for years
43
• But its localised saving against a single budget and not joined-up.
• There will be unintended consequences.
• You won’t know what they are because you won’t be measuring them.
• Measures of Human Development, Quality, Financial, and Time across the value stream will be impacted.
So what does Lean improvement do?
44
“There are four purposes of improvement: easier, better, faster, and cheaper. These four goals appear in the order of priority.” Shigeo Shingo (Safety is fundamental via ‘respect for people’)

So what does Lean improvement do?
Lean: easier, better, faster, cheaper.
CIP: easier, better, faster, cheaper.
Individual &
team learning
Individual &
team learning

3rd Big Idea – Two Dimensions
– Numbers • Deliver improvement in
numbers – quality, delivery, cost and happiness!
– Culture • Ensure each persons job is
aligned to provide value for the customer & a long-term future for the organisation
• Ensure staff “see abnormality & waste” and get each person to take initiative to solve problems & improve their work
Hard - Numbers
Soft - Culture
The Machine That Changed the World
Based upon MIT's five-million-dollar,
five-year study on the future of the
automobile, a ground breaking
analysis of the worldwide move from
mass production to lean production.
“The fundamentals of this system are
applicable to every industry across the
globe...[and] will have a profound
impact on human society--it will truly
change the world". --New York Times
Magazine
First published 1990

The Machine That Changed the World
Keep feeding it with: it will keep on producing:
A machine that could change our patients’, our
staff's and our organisations’ world.
• the creativity of staff
• nurturing &
encouragement
• lean leadership
• active involvement
• time
• small improvements
every day
• big improvements
regularly
• a self replicating culture
of improvement
• ever-improving value
for patients

Questions?
49
Louise Brennan – KPO Specialist
Kaizen Promotion Office
Transforming Care Institute, SaTH
February 2018

Virginia Mason Hospital 15 Year Journey
• Patients are at the heart of the improvements
• New ‘management method’ led clinically from top
• Consistent approach – in it for the long term, using
agreed ways of working
• Increased patient to clinician value-added contact time
• Patients benefit from greater safety, less delay in
seeing clinicians for care and more timely results and
treatments
• Virginia Mason saved $11 million in planned capital
investment by using space more efficiently and freed
an estimated 25,000 square feet of space using better
designs
• They reduced supply costs by $2 million through
inventory reduction and the 5S process.

Virginia Mason Hospital 15 Year Journey
• A not-for-profit medical group in Seattle, Washington providing primary and hospital care
• 336 bed hospital, 445 doctors, multiple primary and secondary care clinics
• A leader in setting patient care quality standards in the US
• From unsafe (Institute of Medicine, 2001) to very safe (the USA’s “Hospital of the Decade”)

• One of 5 Trusts in England to successfully apply to the TDA
for this partnership programme – previous successful individual NHS partnerships in North-East
England and Shropshire and Staffordshire Mental Health Trust
• 5 year partnership including: – training, mentorship and on-going support from a dedicated member
of the Virginia Mason Institute team
• Learn key principles and systems to help us to continue to
improve patient safety and experience in our Trust
The story so far: Cultural Transformation

The story so far: Cultural Transformation
54
• Successful Bid to NHSI/NHSE
• Formation of KPO team
• Launch of Organisational Strategy
• Underpinned by SaTH Values
• Launch of Transforming Care Institute
• Launch of Leadership Academy
• Values in Practice Agreements (Compact work) including Leaders/Medical/STP

TCI Self Sustaining

Guiding Team
56
Profile of Trust Guiding Team
Edwin Borman Medical Director/Executive Sponsor for Value Stream
#2 (Sepsis)
Julia Clarke Corporate Management Director
Deborah
Dollard
VMI Executive Sensei
Tony Fox Deputy Medical Director/Executive Sponsor for Value
Stream #4 (Outpatient Clinics)
Sara Biffen Interim Chief Operating Officer/Executive Sponsor for
Value Stream #1 (Respiratory Discharge)
Victoria Maher Workforce Director/Executive Sponsor for Value
Stream #3 (Recruitment)
Brian Newman Non-Executive Director
Neil Nisbet Finance Director
Deidre Fowler Director of Nursing & Quality/Executive Sponsor for
Value Stream #5 (Patient Safety)
Cathy Smith KPO Lead
Fran Steele NHSI Representative
Simon Wright Chief Executive

The story so far: embedding a Production System
57
• Leaders Standard Work • Huddles • Stand Ups • Genba Walks • Report Outs • 5 Whys
• Standard Work • 5S • Value Streams • Kaizen Events • Every Day Kaizen
• Alignment • One improvement method

Engagement and Pace
58
Target: Educate 3000 : Year 3 Target: Engage 750: Year 3
558 Engaged using VMI
Methodology
Guiding Team
Members
Value Stream Sponsor Teams
RPIW’s
5S
Roll out
Genba Rounding/
Walks
Lean for Leaders
Transforming Care
Methodology Report
Out
2327

Developing Lean Leaders
• Over 80 Lean for Leader set to
graduate from 2016/17 cohorts
• Over 45 Lean for Leaders set to
commence their L4L training in
2018
• Waiting list for 2019 L4L training
59

5S Kaizen Events
60

Value Streams
Value Stream #1: Respiratory Discharge
Value Stream #2: Sepsis Pathway
Value Stream #3: Recruitment
Value Stream #4: Outpatient Clinics (Ophthalmology)
Value Stream #5: Patient Safety
Value Stream #6: Emergency Department, PRH
(Launching March 2018)
Value Stream #6: Radiology (Launching April 2018)
61

Respiratory Value Stream
62
Improvements
• Lead time target has been met
with a reduction of over 40 hours
• Additional patient spells have
been accommodated
• Standard work has been
implemented including 4pm
huddles, board round and ward
round
• Visual controls to aid timely
provision of medication,
discharge summary and
handovers are supporting the
process

Sepsis Value Stream
63
Improvements
• 12 quality improvements made within the
sepsis pathway including use of screening tools,
Sepsis trolley, reduction in late observations and
blood culture processing
• 11 ½ hours of non value adding time
removed from screening for sepsis , diagnosis
of sepsis and delivery of sepsis bundle pathway
(single patient pathways)
• 968 steps no longer required to collect
equipment and collect/deliver blood culture
samples (single patient episodes)
• Sepsis Trolley rolling out to AMU,
Emergency Departments at RSH and PRH
• Sepsis Box rolling out to AMU at PRH
Recruitment Value Stream
64
Improvements • Lead time (from vacancy identified to staff
member’s first day) reduced by 10 weeks from 135 days to 63 days
• Delay in receiving candidate references reduced
from 21 days to 1 day • Reduction in length of time from approval to post
being advertised reduced to 1 day (in test
genba and having sustained at 90-days now
suitable for roll-out)
• Potential new staff aware of interview date at
advert stage – 19 day improvement
• Lead time from close of advert to interview
reduced by 15 days

Outpatient Clinic - Ophthalmology Value
Stream
65
Improvements
• 52 day reduction in the time from receipt of
referral until first contact is made with patient
• 47% reduction in the number of times letters are
delayed due to requesting a letter after the deadline for
electronic transfer to next process
• 100% reduction in the number of Booking staff
unaware of overall process for sending patient letters
(Process = from referral arriving at SATH, to patient
arriving in clinic)
• 5S applied to Ophthalmology clinic letters resulting in
reduction from 17 letters to 1 letter
• 32% reduction in lead time to prepare patient
notes for clinic
• 93% reduction in lead time with the introduction
of electronic grading
Patient Safety Value Stream
66
Improvements
• 80% reduction in time (229 mins to 90
mins) following an incident to reporting an
incident
• Safety huddle implemented with 100%
compliance to standard work at 30-day
remeasures
• Production board implemented to
support requirement for daily safety huddle

The Story so far….
• Over 57,000 patient journeys are safer and kinder
• Over 3,370 miles less walking for staff
• Over 9,500 patient experiences have been improved since the commencement of VS#4 (OPD – Ophthalmology)
• Over 2300 staff educated in Transforming Care Production System
• Over 550 staff using the Transforming Care Production System tools
• Over 80 Lean for Leaders deploying the Transforming Care Production System to improve patient safety and transform our organisational culture
• 6 staff successfully completed their ALT and progressing to TL role
Next Steps
• ALT certified staff undertaking improvement
workshops
• Share and Spread of the improvement work
• Expansion of the KPO Team
• 5S training for all staff
• All Leaders completing Lean for Leaders training
• Promoting Innovation Training
• Mistake Proofing Training
Any Questions ?
Thank You

www.improvement.nhs.uk/resources/
lean-programme
71