lh hormone in assited reproduction
TRANSCRIPT

LH IN ASSISTED REPRODUCTION
Dr G A RAMA RAJU.
KRISHNAIVF
VISAKHAPATNAM.

Dr.Subhas mukherjee
http://drsubhasmukhopadhyay.blogspot.com/
I dedicate this lecture

LH IS BAD Controlled Important Harmful
Replacement useful in some
only
LH

4
• Is there a need for recombinant luteinizing hormone?
• Has the appropriate patient population been defined?
• Has a safe and effective dose been identified?
75 IU/day
• Is the composite primary endpoint of follicular development an appropriate endpoint to assess efficacy in this patient population?

Luveris® (lutropin alfa for injection)
Luteinizing hormone produced
by recombinant DNA technology
Common names
• Recombinant human luteinizing hormone
• r-hLH
Lyophilized powder in 75 IU vials
Self-administered by subcutaneous
injection

Agenda
Therapeutic window
Potential indication
Current scientific evidence
Clinical Perspective and
Risk/Benefit Assessment
Summary and Conclusions

7
LH and FSH Action on the Follicle
Theca externa cells
Theca interna cells
Capillary network Basement membrane
CumulusOophoruscells
OocyteZona pellucida
Granulosacells Follicular
antrum
LH receptorson theca cells
FSH receptors on granulosa cells
E2
FSH
LHA

8
The LH Therapeutic Window Concept
• Follicular growth impaired
• Inadequate androgen (and estrogen) synthesis
• No full oocyte maturation
LH threshold
Normal follicular growth and development
Normal androgen and estrogen biosynthesis
Normal oocyte maturation
Balasch J, Fábreques F. Curr Opin Obstet Gynecol 2002, 14:265-274
• Suppression of granulosa cell proliferation
• Follicular atresia (nondominant follicles)
• Premature luteinization (preovulatory follicle)
• Oocyte development compromisedLH ceiling

9
CNS Influence
Steroidal and
Nonsteroidal
Feedback
GnRH
LH FSH
HH Can Be Caused by Hypothalamic Disorders, Pituitary Disease or Both
Hypothalamus
Pituitary
Ovary

10
HH Treated with r-hFSH Alone
Shoham Z et al. Fertil Steril 1993; 59:738
0
5
10
15
0 5 10 15 20Days
Serum FSH
50
100
Follicle
Estradiol
r-hFSH
Estradiol(pg/ml)
Follicle Size(mm)
and FSH(IU/L)
0
9EndometrialThickness
(mm)
11
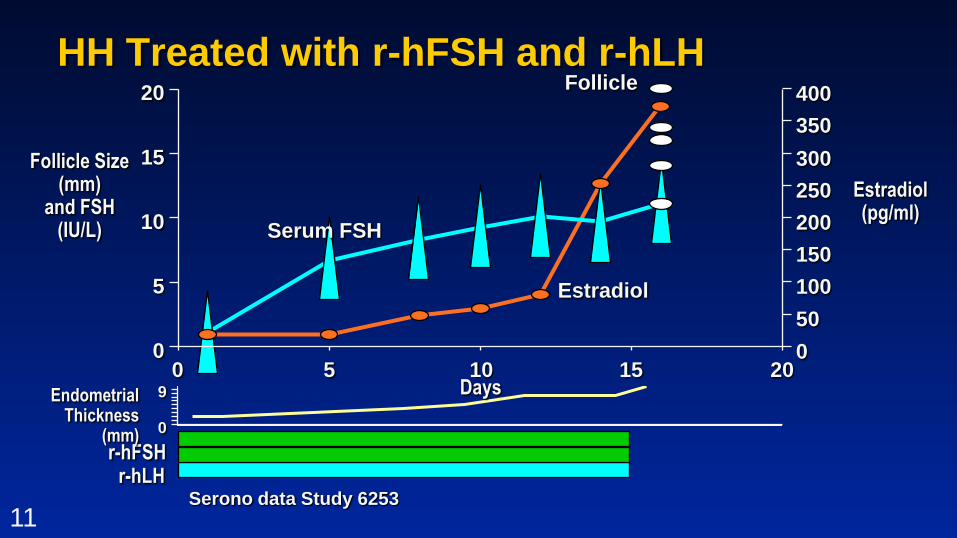
HH Treated with r-hFSH and r-hLH
Estradiol(pg/ml)
Serono data Study 6253
Follicle Size(mm)
and FSH(IU/L)
r-hFSHr-hLH
0
5
10
15
0 5 10 15 20Days
50
100
20
Serum FSH
Follicle
Estradiol
150
200
250
300
350
400
0
0
9EndometrialThickness
(mm)

12
Follicular Development in HH
•Give back what’s missing
LH
HMG
GNRH

Beneficial effect of LH supplementation in ART
> 5
< .5

14
Precise
Purity
Consistency
Half life 24 hrs
Modest accumulation 1.2 miudl
Higher binding HCG
>30 hrs hal life
Accumulation after 7 day 10.7 miu/dl
LH

Beneficial effect of LH supplementation in ART
Age• Marrs et
al;Humaidanet al 2004
Initial poor responder
Follicular stagnation
• Ferrarettti et al; 2004
Low poor responders• Ruvolo et al. 2007
LH POLYMORPHISIM

Women > 35 years:
16
The number of functional LH receptors decreases with age
•
Vihko et al,1996
Endogenous LH may become less potent or biologically active
•Mitchell et al, 1995
The only group to benefit from LH supplementation with an increase in thenumber of mature eggs collected, improved implantation and pregnancy rates
• Marrs et al, 2003; Humaidan et al, 2004

Poor responders:10-15% of IVF patients have an inadequate response to FSH stimulation by day 8
De Placido et al, 2001, 2004
Women showing a hypo-responsive response in IVF down regulated cycles had asignificant increase in pregnancy and implantation rates with the addition ofrecombinant LH (40.7% vs. 22%)
Ferraretti et al, 2004Prospective randomised controlled
trial

Beneficial effect of LH supplementation in ART
• >3000 units Fsh
• Less than 4 oocyte
• >800 pg /ml
poor responder in previous
cycle
• No follicle > 10 mm by day 6
• , 200 pg /ML ON DAY 6
• Poor progression or slow follicular growth
• < 2mm in 3 days
Suboptimal responder in the current cycle

19
How did an optimal dose found.
Dose Finding Studies LH
Controlled ovarian stimulation and HH

20
Percentage of Patients with Follicular Development
63.6%
70.0%
25.0%
11.1%
0 IU LH 25 IU LH 75 IU LH 225 IU LH
1/9 2/8 7/11 7/10
p = 0.467 p = 0.020 p = 0.012p-values vs 0 IU LH
Trend Test*
p = 0.004
* Statistically significant and robust

21
Risks• Known complications of gonadotropins in infertility treatment–Ovarian Hyperstimulation Syndrome (OHSS)–Multiple births
• Other minimal/transient treatment-related adverse events (minor)
• Risks mitigated with proper diagnosis, dosing and observation

22
Risks vs. Benefits
Optimal folliculogenesisand endocrine
profile based on individualized
treatment
Convenience (subcutaneous, self-administered)
Safety profile comparable to
currently marketed
gonadotropins
High pregnancy rate in this profoundly
LH-deficient patient
population

ASIA PACIFIC LH ADBOARD.

ASIA PACIFIC LH ADBOARD.

Indian study :krishnaivf LH study submitted for publicationGrhn triptolein
protocol adding lh lesser dosage
Slight improvement in pregnancy rate
Significant on going
pregnancy rate
More frozen embryo

Adding Lh
26
More frozen embryo
Significant on going pregnancy
rate
Slight improvement in pregnancy rate
Grhn triptoleinprotocol adding lh
decreased total fshdosage

Thank u
27