lib.sumdu.edu.ualib.sumdu.edu.ua/library/docs/rio/2015/m3888.docx · web viewlib.sumdu.edu.ua
TRANSCRIPT

MINISTRY OF EDUCATION AND SCIENCE OF UKRAINE
MINISTRY OF PUBLIC HEALTH OF UKRAINESUMY STATE UNIVERSITY
3888
Methodical instructions for practical lessonsCHILDREN INFECTIOUS DISEASES
for students specialty 7.110101of full-time studying
Poliomyelitis
SumySumy State University
2015

Children infectious diseases. Methodical instructions for practical lessons. “Poliomyelitis” / Compilers: O. I. Smiyan, T. P. Bynda, O. G. Vasilyeva. – Sumy : Pub. SumSU, 2015. – 50 p.
Department of Pediatrics of Postgraduate Education with the courses of Propedeutics Pediatrics and Children Infectious Diseases

ACUTE EPIDEMIC POLIOMYELITIS
Actuality of themePoliomyelitis is a viral disease that predominantly develops in
preschoolers (75–90 %). It is also called infantile paralysis. It is a transmittable viral illness that in its final stage causes paralysis, difficulty in breathing, and can also leads to death. In poliomyelitis, generally 90 % to 95 % of infections cause no symptoms and 5 to 10 % of people have minor symptoms such as: fever, headache, vomiting, diarrhea, neck stiffness and pain in the arms and legs. These people are usually back to normal within one or two weeks. In about 0,5 % of cases there is muscle weakness resulting in inability to move. This can occur over a few days. Many, but not all affected people fully recover. In those with muscle weakness, about 2 % to 5 % of children and 15 % to 30 % of adults die.
Its frequency decreased more than 100 times due to vaccination. Sporadic paralytic forms of poliomyelitis have been registered in many countries in the past few years. Mortality was 9–10 % in those cases.
It is hoped that vaccination efforts and early detection of cases will result in global eradication of the disease by 2018. In 2013; however, there were reports of new cases in Syria and in May 2014, the World Health Organization declared a public health emergency of international concern due to the outbreaks of disease in Asia, Africa and the Middle East.
That's why knowledge about poliomyelitis, diagnostic criteria, treatment and prevention is very critically important.
The overall aim – to be able to put a preliminary diagnosis, to prove the tactics of individual treatment of patients with poliomyelitis and organize anti-epidemic actions in the source of infection.

To be able to: The specific objectives
1. Observe the basic rules of work at the bedside of patients with poliomyelitis.
2. Select the complaints, medical history and physical examination of the patient symptoms that are characteristic of poliomyelitis.
3. Conduct individual diagnostic research and interpret these additional methods of investigation.
The objectives of the initial level1. Give virological characteristics of the causative agent of poliomyelitis (Department of Microbiology and Virology).2. Collect and evaluate complaints, history, including epidemiological, and data of physical examination of the patient (Department of Propaedeutic of Pediatrics).3. To estimate the volume, sequence of inspection and interpret survey data for additional researches: general, biochemical, serological, immunological (Department of Propaedeutic of Pediatrics), virological (Department of Microbiology and Virology).
Recognize and interpret the morphological substrate (Department of Pathological Anatomy).
To estimate the mechanisms of functioning of immune system, namely, to have an understanding of antiviral immunity (Department of Pathophysiology).

4. Establish preliminary clinical diagnosis – poliomyelitis. Identify clinical forms of the disease. To carry out a differential diagnosis.
5. Identify the treatment in patients with poliomyelitis taking into account the etiology, age of the child, premorbid background, and severity of disease.
6. To plan and carry out primary prevention and control measures aimed at preventing the spread of poliomyelitis.
7. Write the clinical case history.
8. Apply the deontological communication skills with patients.
4. Allocate syndromes and symptoms of the disease (Department of Propaedeutic of Pediatrics).
5. Apply the etiologic agents, pathogenetic and symptomatic therapy (Department of Pharmacology).
6. Interpret the meaning reactivity of the organism and its role in the inflammatory process in poliomyelitis (Department of Pathophysiology), the role of viruses and their pathogenic factors in the development of infection (Department of Microbiology and Virology).
7. Complete a case history (Department of Propaedeutic of Pediatrics).
To determine whether the output level of your necessary knowledge and skills is enough, follow these objectives, check the correctness of solving problems, comparing with the standard answers.

Tasks for self-correction output level of skills
Task 1
A boy, 5 years old is ill with acute disease: body temperature rose to 38,9ºC, headache, vomited twice, sneezing, runny nose. After 3 days, the body temperature decreased to 37,1ºC but the pain in the left lower extremity and staggering gait appeared.
Objective: The child’s state was moderate severity. Child was sluggish. Catarrhal phenomenon was marked (hyperemia of the posterior wall of the pharynx). The breathing was exagerrated. Tones of heart were clear and rhythmical. The abdomen was soft and painless. The liver and spleen were not enlarged. Movement of the left foot is restricted and is raising in the supine position is unable to stand alone. Muscle tone decreased. The tendon reflexes (knee and Achilles) on his left leg were reduced. The used serological diagnostic methods helped to reveal the increase of antibody titer in the paired serums to polio by 5 times.
Where are often localized changes at this disease? A In ganglion cells of the posterior horns of the spinal cord. B In ganglion cells of the anterior horns of the spinal cord. C In ganglion cells of the brain. D In large pyramidal cells of the cerebral cortex.E In large pyramidal cells of the pyramidal tract.
Task 2
Disease of the child of 1 year 7 months old, was manifested by increasing of temperature to 39ºC, general weakness, and decreasing of appetite. After 2 days on the background of temperature, there was weakness in the legs, staggering gait, and limitation of movement of the left hand. From the history of life it is known that the child is from the first pregnancy, first birth from twins. Pregnancy and the families of the mother were normal; the

child was on mixed feeding. Vaccinations were by age. The physical and neuro-psychological development are normal for his age. The second child was at that time in the hospital with enterovirus infection – epidemic myalgia. Objective: the state of moderate severity. Child is sluggish, slowed. Catarrhal phenomena is not expressed. The breathing is exagerrated. The tones of heart are clean, rhythmical. The abdomen was soft and painless. The liver and spleen were not enlarged. The movements of the left hand are limited. Muscle tone is sharply reduced. Tendon reflexes are reduced on the left hand, Achilles reflex and knee reflex – on both legs, lower abdominal reflex and cremaster’s reflex. The symptoms of tension are negative. The titer of antibodies to the polio virus in the dynamics is without growth. On the background of prolonged therapy, positive dynamics of symptoms were recorded. On the 15th day of illness child walked without support. The muscles tone of the lower extremities was good, tendon reflexes are present. However, the movements of his left hand remained limited, baby could not hold toys in hand. After 1 month of onset of the disease the baby held toys with left hand and rested her, the range of motion was not. The pain in hand was absent. Tonus and tendon reflexes were reduced. Moderate malnutrition of deltoid muscle and muscles of shoulder was observed. Full recovery occurred within 6 weeks of onset.
What is characterized by peripheral paralysis?
A. Increasing of muscle tonus and tendon reflexes and decreasing or absence of cutaneous reflexes.B. Advent hyperkinesia, decrease of cutaneous reflexes.C. When improving of muscle tonus, decreasing of tendon-periosteal reflexes, muscle atrophy, changes in electroexcitation of nerves and muscles in the unaltered skin reflexes. D. Increasing of muscle tonus, decreasing of tendon-periosteal reflexes, muscle hypertrophy, changes in electroexcitation of nerves and muscles in the unaltered skin reflexes.

E. Reduction or loss of muscle tonus, tendon-periosteal reflexes, muscle atrophy, changes in electroexcitation of nerves and muscles in the unaltered skin reflexes.
Task 3
A boy, 3 years old, acute illness, body temperature rose to 38,6°C, marked by recurrent vomiting, headache, dizziness, muscle weakness. On the 3rd day, parents noticed that the right eyelids could not close, during a conversation – distorted face. Body temperature decreased to 37,1ºC, but pain appeared in the left lower extremity and staggering gait. Objective: the state of child was of moderate severity. Child was sluggish. Catarrhal phenomenon was marked (hyperemia of the posterior wall of the pharynx). The breathing was exaggerated. Tones of heart were clear, rhythmical. The abdomen was soft and painless. The liver and spleen were not enlarged. When face is viewed, right eyelids could not close, during a conversation – distorted face. Movement of the left foot is unable and restricted when raising it in the supine position. Decreasing of muscle tonus is noted. The tendon reflexes (knee and Achilles) on his left leg are reduced. The increase in antibody titer in the paired serums at 5 times was revealed in child using serological diagnostic methods. Preventive vaccination has not been received.
When is vaccination and revaccination against poliomyelitis for children done according to the order?
A. It can be made at 3 months and carried out once. Revaccination is carried out at 3 years, 6 years and 14 years (once at every stated age).B. It can be made at 1 month and is done three times at intervals of 30 days. Revaccination is carried out at 18 months, 3 years, 6 years and 14 years (once).C. It can be done at 3 months and is done three times with intervals of 30 days. Revaccination is carried out at 18 months, 3 years, 6 years and 14 years (once).

D. It starts at 12 months and is done three times at intervals of 30 days. Revaccination is carried out at 3 years, 6 years and 14 years (once). E. It begins at 3 months and is done three times at intervals of 30 days. Revaccination is not performed.
Task 4
A 9-month-old baby has spinal form of poliomyelitis.What group of viruses are the causative agents of this disease?
A. Arboviruses.B. Rotaviruses.C. Reoviruses.D. Picornaviruses.E. Togaviruses.
Task 5
An 18-month-old non-vaccinated baby was hospitalized due to flabby paralysis of the left leg. There is loss of muscle tonus, absence of active movement and tendon reflexes. Cutaneous sensitivity is present.
Where is the CNS lesion localized?A. Anterior horns of the spinal cord.B. Posterior horns of the spinal cord.C. Cerebellum.D. Precentral gyrus of the brain.
Task 6
A child is 2 years old. The disease started sharply with the rise of temperature up to 38,8°C, vomiting, headache, flaccidity, pain in the abdomen and softening of stool. In 3 days weakness in the left

leg, hypotonia, hyporeflexia, hypodynamia at the same place appeared and the skin on the left leg was pale and cold.
What is the main route of transmission of this disease?A. Respiratory.B. Fecal-oral.C. Respiratory and fecal-oral.D. Respiratory and contact.E. Fecal-oral and parenteral.
Answers to tasks:
Task 1: B. Task 2: E. Task 3: C.Task 4: D.Task 5: A. Task 6: B.

References:1. Infectious diseases in children / Yu. P. Kharchenko, A. M.
Mikhailova, S. O. Kramarev, I. V. Yurchenko, G. A. Shapovalova, A. I. Savchuk – Odessa: The Odessa State Medical University, 2008. – 264 p.
2. Selected lectures in children’s infectious diseases for English medical students / Compilers: S. V. Kuznetsov, O. N. Olchovskaya, A. N. Tatarkina. – Kharkov: KSMU, 2006. – 164 p.
3. Dyabina T. Digest on Children Infectious diseases / T. Dyabina, Y. Vyaltseva – Simferopol, 2007. – 127 p.
Additional:1. Ambulatory Pediatric care 2nd / edited by Robert Derchewitz;
Lippingcot-Raven, 1992. – p. 58–59; 315–319.2. Current therapy in pediatric infectious disease/ 2 / edited by
John D. Nelson, M. D. – B. C. Decker inc. Toronto. Philadelphia, 1988. – p. 47–49.
3. Dale D. C. Infectious diseases: the clinician guide to Diagnosis, Treatment and Prevention / Dale D. C. WebMD, Corporation 2004. – 310 p.
4. Krugman's Infectious Diseases of Children, 11th edition, Mosby Publishers, 2004. – 574 p.
5. Principles and Practice of Pediatric Infectious diseases, 2nd edition / Long S. et al., Elsevier Science, 2003. – 1675 p.
6. Mark H. Beers. Merck Manual of Diagnosis and therapy / Mark H. Beers / 18lh edition, Merck research laboratories, Whitehouse Station, NJ 2006. – 2992 p.
7. Murray. Medical Microbiology / Murray. – 4th edition, Mosby Publishers, St Louis, 2002– 687 p.
8. Berman R. Nelson Textbook of Pediatics, / Berman R., Kliegman R., Jenson H. 16th edition W.B. Saunders company, 2004 – 2672 p.
9. Hal B. Jenson. Pediatric infectious diseases: principles and practice (textbook) / Hal B. Jenson – USA, W. B. Saunders Company. 2002. – 697 p.
10. Textbook of Pediatric Nursing. Dorothy R. Marlow; R. N., Ed. D. – London, 1989. – 661 p.
11. Pediatrics ( 2nd edition, editor – Paul H. Dworkin, M. D.) – 1992. – 550 p.
If you are convinced that your output level of knowledge and skills meet the requirements of entry-level goals, go to mastering of the training content.
List of theoretical questions to the topic:
1. The state of morbidity of poliomyelitis among children and adults today.2. The etiology of poliomyelitis.3. Epidemiology of poliomyelitis.4. Pathogenesis of poliomyelitis.5. Classification, clinics of poliomyelitis.6. Give the definition of "suspect" and "probable" cases of poliomyelitis.7. Diagnostics of poliomyelitis.8. Differential diagnosis of poliomyelitis. 9. Complications of poliomyelitis. 10. Peculiarities of poliomyelitis in infants. 11. Tactics of district pediatrician, pediatrician, doctor "emergency" in detecting a child with clinics of acute flaccid paralysis. 12. Treatment (in the period of paralysis and during the period of early and late reconvalescence) and recovery criteria.13. Criteria of writing out for convalescents from hospital.14. Forecast.

15. Prevention of poliomyelitis and antiepidemic measures for the source of infection. What are the complications in the course of postvaccinal period after the introduction of polio vaccine you know?
A summary of the material
Poliomyelitis is an acute infectious disease that is caused by one of three types of poliovirus and is characterized by a large range of clinical forms (from abortive to paralytic one).
Etiology: the etiological agent is the poliovirus from the Picornaviridae family, sort of enterovirus.
Epidemiology:• The source of infection are patients, viral carriers;• The mechanism of transmission is droplet, fecal-oral;• Receptivity is high, especially in children till 3 years.
Pathogenesis:1. Inoculation and reproduction of virus in the intestinal or
upper respiratory tract epithelium.2. Lymphogenic distribution of virus.3. Reproduction in organs and tissues.4. Fixation in nervous tissues, damage of moto neurons.
ClassificationForms of poliomyelitis without CNS damage:
I. Innaparant (virus carrying).II. Abortive (small illness).
Forms of poliomyelitis with CNS damage:I. Nonparalytic or meningeal.II. Paralytic:
1. Spinal (neck, pectoral, lumbar, limited or widespread).

2. Pontinus.3. Bulbar. 4. Pontospinal.5. Bulbospinal.6. Bulbopontospinal.
Diagnostic criteria of several poliomyelitis forms.
Meningeal:• latent period is 5–35 days;• severe toxic syndrome;• meningeal syndrome;• CSF changes, as at serous meningitis (on 4–5 day);• pain in extremities, neck, back;• horizontal nystagmus (in half of patients);•complete recovery in. 3–4 weeks.
Paralytic:Preparalytic period (lasts for 2–3 days):• high fever, intoxication;• insignificant catarrhal phenomena;• dyspepsia syndrome;• pain in neck, back, extremities;• hyperesthesia;• positive tension symptoms;• CSF changes (as at serous meningitis);• typical "tripod" position of a patient.
Paralytic period (1 day – 2 weeks):• development of flaccid (peripheral) paralyses and paresis;• sometimes secondary increase of temperature;• damage of lower limbs (80 %), or upper limbs, trunk or neck muscles;• muscular tonus is decreased;

• tendon reflexes are absent.
Period of rehabilitation (to 1 year):• renewal of the least affected moto neurons function.
Residual period:• increasing muscular atrophy, contractures, osteoporosis, bone deformities.
Laboratory investigation:• Total blood analysis: leucocytosis, neutrophilia with a shift to the left, or without changes.• Analysis of CSF: flows out under raised pressure, turbid, lymphocyte pleocytosis; elevated protein, decreased glucose and chlorides level.
Specific confirmation of diagnosis:• virology research of excrements, pharyngeal mucus, CSF;• serologic research (NR., CBR) of paired sera.
Diagnosis example: poliomyelitis, paralytic pontospinal form, period of rehabilitation.
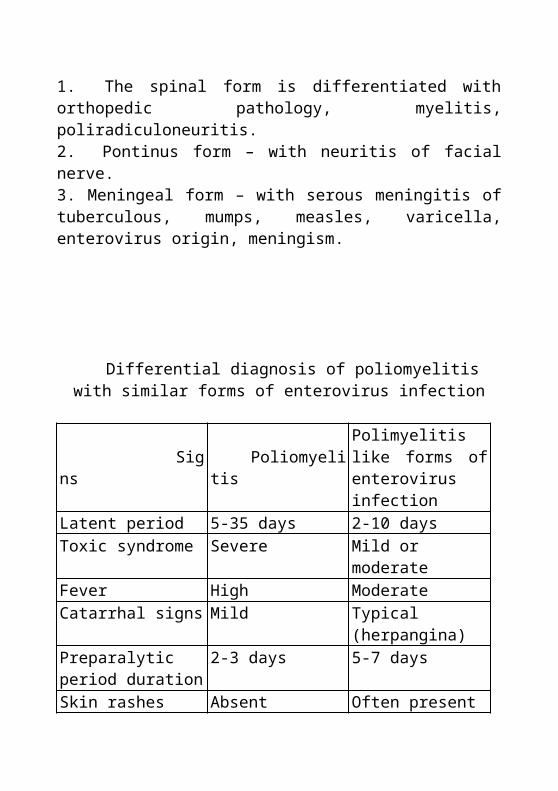
Differential diagnosis1. The spinal form is differentiated with orthopedic pathology, myelitis, poliradiculoneuritis.2. Pontinus form – with neuritis of facial nerve.3. Meningeal form – with serous meningitis of tuberculous, mumps, measles, varicella, enterovirus origin, meningism.

Differential diagnosis of poliomyelitis with similar forms of enterovirus infection
Signs PoliomyelitisPolimyelitis like forms of enterovirus infection
Latent period 5-35 days 2-10 daysToxic syndrome Severe Mild or moderateFever High ModerateCatarrhal signs Mild Typical (herpangina)Preparalytic period duration
2-3 days 5-7 days
Skin rashes Absent Often presentParalysis Peripheral paralysis,
stablePeripheral paresis, usually disappears
The tendon reflexes Absent Decreased or normalMuscular atrophy Typical Rare, some musclesRenewal of function Less damaged moto
neurons in a yearPractically complete in 3–4 weeks.
CSF changes As in serous meningitis
Not typical
Virological studies Poliovirus Coxsackie A, ECHO
Treatment:In acute period• Obligatory hospitalization.• Physical and psychical rest.• Analgetics (analgin 50 % 0,1 ml/year of life, bromides).• Thermal procedures (hot wrappings, ozocerite, paraffin appliques).• Dehydration (lasix 1-3 mg/kg, mannit, mannitol 1-1.5 g/kg).• Glucocorticoids (in severe cases) 1-3 mg/kg (prednisolone).• Human immunoglobulin 0.5 ml/kg 2-3 days.

In the early period of rehabilitation• Proserin 1 mg/year of life, galantamin, dibasol 1-5 mg per day for 20-30 days.• Physical exercises, physiotherapy, ozocerite, paraffin appliques, diathermy, massage.• Vitamins (B6, B|2), ATPh.• Anabolic steroids (2-3 courses per year).An orthopaedic correction in residual period.
Prophylaxis• Isolation for 21 days from the beginning of disease, hospitalization of patient.• Observation of contacts for 3 weeks.• Specific active: vaccination by an inactivated (once) then an oral (twice) polio vaccine (IPV, OPV) from 3 month of age, with a 30 day interval, OPV revaccination at 18 months, 6, 14 years.Vaccine is associated with poliomyelitis (diagnostic criteria).• Beginning of illness not earlier than 4 days and not later than 30 days after the reception of vaccine. For those, who contacted with vaccinated children – up to 60 days.• Development of flaccid paresis or paralyses without violation of sensitiveness with stable (after 2 month) remaining phenomena.• Absence of the disease progress.• Selection of identical virus as the vaccinal virus (by the antigen properties), 4 times growth increasing of specific antibodies.

Several models of solving the problems using diagnostic and therapeutic algorithms
Task 1
A child, 2 years 9 months. He was hospitalized to infectious department on the 5th day of disease with complaints of fever up to 38,1°C, pronounced weakness, redness of the throat, running nose, lack of active movement in the legs, inability to stand, walk, headache, irritability. He was acutely ill, fever – 38,7°C, running nose, redness of the throat, severe weakness, hypersensitivity. On examination: skin was pale, lower limbs were cold, throat congestion, hypersensitivity, positive symptoms of tension, he was sitting in a "tripod" pose. He had passive movements of the feet, all types of sensitivity has been saved. He had vesicular breathing in the lungs. Breathing rate was 26 per min. Heart sounds were weakened, heart rate was 115 per min. The abdomen was soft, there were painful bowel movements. Defecation was once a day and feces were undigested and mushy.
1 What is your preliminary diagnosis?A. Poliomyelitis.B. Myasthenia.C. ARVI, nasopharyngitis.D. Enterovirus infection herpanhina.E. Meningitis.
2 What is the etiological factor of the disease?A. Virus of the herpes family, I type.B. Virus of the herpes family, II type.C. Virus from the family Picornaviridae.

D. Virus from the family Paramyxoviridae.E. Virus from the family Orthomyxoviridae.3 What material should be collected from people suspected with poliomyelitis?A. Liquor.B. Serum.C. Swabs from the nasopharynx.D. Faeces.E. All answers are correct.
4 How long should the patient be isolated?A. On the 5th day after the disease.B. 14 days of the disease.C. 18 days of the disease.D. On the 21 days from the date of disease.E. Isolation of the patient is required.
The correct answers are: 1-A, 2-B, 3-D, 4-D.
Task 2
A boy is 5 years old. He is acutely ill, body temperature rise to 39,6°C, marked by recurrent vomiting, dizziness and muscular weakness. On the 3rd day, parents marked that eyelids could not close, during a conversation – distorted face. He did not receive preventive vaccination.
1 What is the first disease you think of?A. Poliomyelitis, pontinus form.B. Neuritis of the facial nerve.C. Encephalitis.D. Meningitis.E. Surround process in the brain.

2 In the study of cerebrospinal fluid after 14 days of onset of poliomyelitis it was detected:A. Neutrophilic pleocytosis, proteinorahia, cell-protein dissociation.B. Significant lymphocytic pleocytosis, reducing of protein in the cerebrospinal fluid, hyperglucosorahia.C. Mild lymphocytic pleocytosis, proteinorahia, protein-cell dissociation, hyperglucosorahia.D. Neutrophilic pleocytosis, reducing of protein in cerebrospinal fluid, hyperglucosorahia.E. CSF – age norms.
3 Nonparalytic forms of poliomyelitis include:A. Spinal.B. Pontinus.C. Bulbar.D. Meningeal, innaparant, abortive.E. Residual.
4 What term of quarantine should be set for children who have been in contact with a patient with poliomyelitis?A. 5 days.B. 14 days.C. 20 days.D. 35 days.E. 60 days.
The correct answers are: 1-A, 2-B, 3-D and 4-B.
Task 3
A boy, 7 years old, became ill 3 days ago: body temperature was 39,6°C, repeated vomiting, headache, weakness. On the 3rd day he couldn't close right eye, his face has appeared asymmetry during the speech. The boy wasn't vaccinated.

1. What disease is suspected?2. What must his family doctor do?
1. Poliomyelitis, typical pontinus form, paralytic period, severe stage.2. The boy must be hospitalized into infectious hospital, where he must be isolated for 40 days; inform sanitary-epidemiologic structures; observation of contacts.
Task 4
A healthy boy, 5 months old, was brought to ambulatory clinic to perform planned vaccination.
1. What vaccine against poliomyelitis would he receive, when next dose of booster vaccination must be given?2. What specific complication may occur?
1. Oral poliomyelitis vaccine, in 18 months.2. Vaccinal poliomyelitis.
Task 5
A girl of 2 years became ill acutely from raising of temperature to 38.3 °C, catarrhal phenomena. During three days, cough and cold were present. Then a temperature decreased, but a child could not stand on feet. A doctor reveals limitation of movements, lowering of muscular tone in lower extremities. Sensitiveness is normal.
What is the name of preliminary diagnosis?A. Osteomyelitis.B. Enterovirus infection.C. Poliomyelitis.D. Rotavirus infection.

E. Flu.
The correct answer is C. Task 6
A child of 2,5 years, not vaccinated is ill for 4 days. The disease had begun from hyperthermia to 38,5°C, weakness, mild catarrhal phenomena and liquid emptying. On a 5th day a temperature was normal, however much pains appeared in the muscles of feet and acute limitation of movements, lowering of tendon reflexes.
What is the name of preliminary diagnosis?A. Acute intestinal infection.B. Acute encephalitis.C. URT infection.D. Osteomyelitis.E. Poliomyelitis.
The correct answer is E.
Task 7
In a child of 4 years about 3 days there was fever and catarrhal signs. On the 4th day temperature was normal, but the boy began to pull his left leg. A doctor suspected poliomyelitis.
What form of disease is the most probable?A. Bulbar.B. Abortive.C. Pontinus.D. Spinal.E. Meningeal.
The correct answer is D.
Short guidance to work on a practical classes
At the beginning of classes, there shall be a test control to check level of knowledge. Then – the independent work of students with patients. Under the guidance of the teacher, there will be a clinical analysis of the patient's history of polio. At the end of the class there will be final test control or solving of situational problems.
Technological map of classes
The stageTime, minu-tes
Study Materials Place of conductionmeans of
teachingequip-ment
1. Definition of the initial level of knowledge
10 Tests Training room
2. Supervision of patients with poliomyelitis under the control of teacher
20 Patients Ward
3. Clinical analysis of patients with poliomyelitis under the direction of teacher
20 Case history, algorithms
Training room
4. Justification of preliminary
5 Tables, charts,
Training room

diagnosis algorithms5. Justification of treatment tactics
10 Tables, charts, algorithms
Training room
6. The final control
10 Tests situational tasks
Training room
7. Summing up the work
5 Training room
Algorithm of practical students' workComplaints and anamnesis taking in newborns and infants.1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.4. Tactful and calm conversation with the parents of sick child.5. Explanation of future steps concerning the child (hospitalization, some methods of examination, etc.).
Complaints and anamnesis taking in toddlers and preschoolers (children of age from 1 to 6 years)1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.4. By means of game playing, find a contact with a child.5. Tactful and calm conversation with the parents of sick child.6. Explanation of future steps concerning the child (hospitalization, some methods of examination, etc.).
Complaints and anamnesis taking in school age children.1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.

4. Tactful and calm conversation with sick child his/her parents.
5. Explanation of further steps to child and his/her parents (hospitalization, some methods of examination, etc.).1. To collect complaints:• fever, chills, indisposition, anxiety, insomnia, headache;• cramps, nausea, vomiting, that does not bring facilitation;• pain in a neck, back, extremities;• absence of movements in extremities;• twisted face during the speech, unable to close eyelids, tearing, salivation, unable to stand, walk, violation of speech, violation of co-ordination;• atrophy of muscles, lag in growth of the staggered extremity.
2. To collect anamnesis of disease, epidemiological anamnesis:• acute disease, beginning from fever, severe toxic, pain, total brain, moderate catarrhal, dyspepsia syndromes, rashes, respiratory disorders;• disease beginning in 4-30 days from the contact with ill person;• local cerebral symptoms, extremities flaccid paralyses in 2-3 days after the disease beginning;• gradual renewal of the least staggered moto neurons function during 1 year;• increasing muscular contractures, atrophy, osteoporosis, bone deformities.• conversation accomplishment3. To inspect a patient:
Physical methods of examination of newborns and infants1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.

4. Explain to the parents what examination should be performed and obtain their informed consent.5. Prepare for examination (clean and warm hands, warm phonendoscope, etc.).
Physical methods of examination of toddlers and preschoolers1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.4. Explain to the parents what examination should be performed and obtain their informed consent.5. Find a contact with the child; try to gain his/her confidence.6. Prepare for examination (clean and warm hands, warm phonendoscope, etc.).
Physical methods of examination of school age children1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.4. Explain to the parents what examination should be performed and obtain their informed consent.5. Find a contact with the child; try to gain his/her confidence.6. Prepare for examination (clean and warm hands, warm phonendoscope, use the screen if necessary etc.).
A. Examination:• tripods sign;• pale skin;• hyperemia of throat;• limitation of active movements in the staggered extremities, hyperesthesia, twisted face during the speech, unable to close eyelids, tearing, salivation, asymmetry of reflexes.
B. Palpation:• bulging, tension of large fontanel, hyperesthesia, positive Kernig's, Brudzinsky, Lesage symptoms, nuchal rigidity, depression of tendon, skin reflexes, reactive pain phenomena;• lowering of temperature of the staggered extremities, normal sensitiveness, stored passive movements in extremities.C. Auscultation: tachycardia, deafness of the heart tones. Conversation accomplishment.
Informing about the results of examination1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.4. Explain to a child and his/her parents what examinations should be performed and obtain their informed consent.5. Involve adolescent and his/her relatives into the conversation (comparepresent examination results with previous ones, clarify whether your expectations are clear for them or not).6. Conversation accomplishment.
4. To estimate the results of additional researches• Total blood analysis: leucocytosis, neutrophilia with a shift to the left, or without changes.• Analysis of CSF: flows out under raised pressure, turbid, lymphocyte pleocytosis; elevated protein, decreased glucose and chlorides level.
5. To substantiate the diagnosis.
Planning and prediction of conservative treatment results:1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.

4. Explain to child's parents the necessity of further treatment directions correctly and accessibly.5. Discuss with parents and their child the peculiarities of drug intake, duration of usage, side effects and find out whether they understand your explanations.6. Conversation accomplishment.
6. To prescribe the treatment: obligatory hospitalization, physical and psychical rest, diet, NS AIDs, analgetics, antihistamines, detoxication facilities, corticosteroids, diuretics, thermal procedures, in the early rehabilitation period – proserin, neuroplegics, vitamins B group, ATF, anabolics.
Informing about treatment prognosis.1. Friendly facial expression and smile.2. Gentle tone of speech.3. Greeting and introducing.4. Correct and clear explanation of expected results of treatment.5. Discuss with the parents and their child the importance of continuous treatment, following the treatment scheme; make sure that your explanations are properly understood.6. Conversation accomplishment.
Examples of test controlPoliomyelitis, enteroviral infection
1. Give definition of poliomyelitis:A. Acute viral disease which is characterized by the toxic signs and the damage of the nervous system.B. Acute infectious disease which is characterized by the toxic signs and CNS damage in the form of flaccid paralysis.

C. Acute infectious disease which is characterized by the common signs and CNS damage in the form of spastic paralysis.D. Acute viral-bacterial disease which is characterized by the toxic signs and CNS damage.E. Acute infectious disease which is characterized by the heart and CNS damage in the form of languid paralysis.
2. What type of immunity is formed after poliomyelitis?A. Unstable immunity.B. Typospecific immunity.C. Familyspecific immunity.D. Persistent immunity.E. Absent immunity.
3. The causative agent of polyomyelitis is:A. Shigella.B. Poliovirus hominis.C. Y.enterocolitica.D. Reoviruses.
4. The causative agent of polyomyelitis belongs to the group of:A. Rotaviruses.B. Arboviruses.C. Enteroviruses.D. All answers are incorrect.
5. How many types of polyoviruses are known for nowadays?A. 1.B. 2.C. 3.D. 4.
6. The sourses of polyomyelitis infection are (2):

A. Patients with clinically manifest poliomyelitis, healthy carriers.B. Birds.C. Fish.D. Persons suffering from atypical and abortive forms.
7. The carrier state after clinically manifest form of polyomyelitis infection may last as long as:A. 30 to 40 days.B. 15 to 20 days after an attack.C. 7 to 10 days.D. All answers are incorrect.
8. A 9-month-old baby has spinal form of poliomyelitis. What group of viruses does the causative agent of the disease belong to? A. Picornaviruses.B. Paramyxoviruses.C. Togaviruses.D. Adenoviruses.E. Rotaviruses.
9. An 8-month-old non-vaccinated baby fell ill acutely: fever up to 38.5°C, anorexia, weakness, motor anxiety, mild catarrhal signs and diarrhea. Loss of muscle tone, absence of active movement and tendon reflexes occurred on the right leg on the 5th day of illness. Cutaneous sensitivity is present. What is your preliminary diagnosis? A. Polymyelitis.B. Viral encephalitis.C. Acute respiratory viral infection.D. Acute intestinal infection.E. Osteomyelitis.
10. A 2-year-old boy is having low-grade fever, mild catarrhal signs for 3 days. The body temperature decreases on the 4th day of illness

and flabby paralysis on his right leg occurs. What clinical form of poliomyelitis is present? A. Spinal.B. Abortive.C. Meningeal.D. Pontine.E. Bulbar.
11. What is the most frequent and typical form of paralytic poliomyelitis?A. Spinal form.B. Bulbar form.C. Pontine form.D. Encephalitic form.E. Visceral form.
12. An 18-month-old non-vaccinated baby was hospitalized due to flabby paralysis of the left leg. There is a loss muscle tone, absence of active movement and tendon reflexes. Cutaneous sensitivity is present. Where is the CNS lesion localized? A. Truncus cerebri.B. Postenor cornua of the spinal cord.C. Anterior cornua of the spinal cord.D. Cerebellum.E. Pia matter.
13. A child is 2 years old. The disease started sharply with the rise of the temperature up to 38.8°C, vomiting, headache, flaccidity, pains in the abdomen, softening of stool. In 3 days there were weakness in the left leg, hypotonia, hyporeflexia, hypodynamia at the same place, the skin on the left leg was pale and cold. What are the ways of distribution of the causative agent of this disease? A. Respiratory.B. Fecal-oral.

C. Respiratory and fecal-oral.D. Respiratory and inoculable.E. Fecal-oral and parenteral.
14. A child of 8 years old is hospitalized with complaints on sharp onset of the disease, febrile fever, marked headache, repeated vomiting. On the 2nd day of the disease nystagmus, dysphagia and aphasia developed. Respiration is superficial, cough is silent. What form of poliomyelitis should we think of? A. Nonparalytic, a meningeal form.B. Paralytic, a spinal form.C. Paralytic, a bulbar form.D. Nonapparent form.E. Paralytic, an encephalitic form.
15. A child of 4 years old is hospitalized with complaints on sharply developed paralysis of the right leg against a background of temperature elevation up to 39° C. 4 days before there was a subfebrile fever with insignificant catarrhal symptoms, pain in the abdomen, sweating. Poliomyelitis is suspected. What symptoms, except one, will be characteristic of poliomyelitis? A. Atonia (hypotonia).B. Adynamia (hypodynamia).C. Areflexia (hyporeflexia).D. Anesthesia (hyposthesia).E. Atrophy (hypotrophy).
16. The incubation period of poliomyelitis is ranged:A. From 2-4 to 35 days.B. 3-7 days.C. 11-21 days.D. 15-20 days.
17. In a clinical course of the disease are distinguished:
A. 3 stages.B. 4 stages.C. 5 stages.D. all answers are incorrect.
18. Point out variants of clinical symptoms of preparalytic stage:A. Catarrh of the upper respiratory tract.B. Gastrointestinal disturbances.C. Symptoms pointing to irritation of the nerve roots and meninges.D. All answers are correct.19. The preparalytic stage usually lasts from:A. 2-3 hours.B. 2 to 5 days.C. 7-10 days.D. 1-12 days.
20. What is the characteristic pose of children who has poliomyelitis?A. The Lesage symptom.B. Orthopnoe.C. Pose of ballet-dancer.D. Pose of frog.E. A symptom of tripod.
21. Indicate the correct answer:A. Paralysis may develop at the height of the fever, usually suddenly.B. The lower limbs are most often affected (58 to 82 % of cases).C. Spinal paralysis may be combinated with lesions of the cranial nerves nuclei.D. The paresis and paralysis are characterized by signs of damage of the peripheral neuron.E. All answers are correct.
22. The paralytic stage may lasts (the most complete answer):A. Several months.

B. Several days or one or two weeks, but seldom longer.C. 1-10 days.D. All answers are correct.
23. An elevation of protein content and reduction of cell count in cerebrospinal fluid begin in the:A. Initial, or preparalytic stage.B. Paralytic stage.C. Restitution stage.D. Stage of residual phenomena.24. Indicate the type of paresis or paralysis in poliomyelitis.A. Central type.B. Peripheral type.C. Spinal paralysis or paresis (peripheral type) may be combinated with lesions of the cranial nerves.D. All answers are correct.
25. Paralysis in poliomyelitis is usually:A. Symmetrical.B. Predominantly affects the distal parts of the extremities.C. Asymmetrical, and predominantly affects the proximal parts of the extremities.D. All answers are correct.
26. Indicate the symptoms of the restitution stage beginning.A. Restoration of movement in individual groups of muscles.B. The headache and hyperhidrosis abate.C. The pain in the spine and limbs.D. All answers are correct.
27. The stage of restitution may continue for:A. 1-2 months.B. 1-3 years.C. 20-40 days.

D. several days.
28. Describe the clinical features of spinal form in paralytic poliomyelitis.A. Is accompanied with swallowing, speech, and respiratory disturbances.B. Is characterized by flaccid paralysis of the limbs, trunk, neck, and diaphragm.C. Is expressed in implication of the nucleus of the facial nerve with paresis of the facial muscles.D. Is characterized by general cerebral phenomena and symptoms of focal lesions in the brain.
29. Describe the clinical features of bulbar form in paralytic poliomyelitis.A. Is accompanied with swallowing, speech, and respiratory disturbances.B. Is characterized by flaccid paralysis of the limbs, trunk, neck, and diaphragm.C. Is expressed in implication of the nucleus of the facial nerve with paresis of the facial muscles.D. Is characterized by general cerebral phenomena and symptoms of focal lesions in the brain.
30. Describe the clinical features of pontine form in paralytic poliomyelitis.A. Is accompanied with swallowing, speech, and respiratory disturbances.B. Is characterized by flaccid paralysis of the limbs, trunk, neck, and diaphragm.C. Is expressed in implication of the nucleus of the facial nerve with paresis of the facial muscles.D. Is characterized by general cerebral phenomena and symptoms of focal lesions in the brain.

31. Indicate the clinical features of encephalitic form in paralytic poliomyelitis.A. Is accompanied with swallowing, speech, and respiratory disturbances.B. Is characterized by flaccid paralysis of the limbs, trunk, neck, and diaphragm.C. Is expressed in implication of the nucleus of the facial nerve with paresis of the facial muscles.D. Is characterized by general cerebral phenomena and symptoms of focal lesions in the brain.
32. Specify the frequency of visceral (abortive) form of poliomyelitis.A. 25 to 80 % or more of the total number of poliomyelitis cases.B. 2-3-5%.C. 10-20 %.D. All answers are true.
33. Describe the clinical features of visceral form in paralytic poliomyelitis.A. Symptoms of the initial stage of poliomyelitis.B. Headache, adynamia.C. Sleep disturbances.D. Pain in the muscles of the back, paresthesia.E. All answers are correct.
34. Describe the clinical features of meningeal form in paralytic poliomyelitis.A. Symptoms of the initial stage of poliomyelitis.B. Headache, adynamia.C. Sleep disturbances and meningeal symptoms in addition.D. All answers are correct.

35. Indicate the symptomatic treatment in case of respiratory disorders lesions of the brain:A. 1% lobeline solution, 0,1% adrenalin, and oxygen.B. Ascorbic acid, vitamins of group B.C. Neostigmine methylsulfate.D. Dibazol.
36. Indicate the stimulants of interneural and myoneural conduction:A. 1% lobeline solution, 0,1% adrenalin.B. Ascorbic acid, vitamins of group B.C. Neostigmine methylsulfate (0,1 to 1 ml from 0,05 % solution IM), dibazol.D. Glutamic acid.
37. Glutamic acid is prescribed:A. 0,1 to 1 ml from 0,05 % solution IM.B. Orally in a dose of 0,5 to 2 g daily in powder form or in glucose solution for 10-15 days.C. 0,001 to 0,005 g once a day for 20 to 30 days.D. 0,3 to 0,5 g twice a day.
38. Indicate the thermal procedures which are widely employed during the stage of restitution, except:A. Warm and hot baths.B. Hot packs.C. Paraffin and ozokerite therapy.D. Transthermia.E. Stimulants of intraneural and myoneural conduction.
39. Indicate the term of isolation for patient with poliomyelitis:A. Till 7th day from the beginning of the disease.B. For 21 days from the onset of the disease.C. Till 11 days from the beginning of the disease.D. Till 10th day from the beginning of the disease.
40. In children's institutions (creches, nurseries, kindergartens etc.) the group in which a case of poliomyelitis has been discovered is quarantined for:A. 20 days.B. 30 days.C. 11 days.D. 7 days.
41. The main measure to control poliomyelitis is:A. Antibiotic therapy.B. γ-globulin prescribing.C. Prophylactic vaccination.D. All answers are right.
42. Enumerate measures for prophylaxis of poliomyelitis:A. Earliest isolation of poliomyelitis patient and suspected cases.B. Final disinfection is performed in patient’s dwelling.C. Prophylactic vaccination.D. Contacts are observed for 20 days after isolation of the patient, but are not quarantined.E. All answers are right.
43. Antibiotics in case of poliomyelitis are indicated:A. For prophylaxis.B. To combat complications resulting from secondary infection.C. Should be appointed since the beginning of the disease.D. Should be appointed to all patients with bulbar form in paralytic poliomyelitis.
44. Indicate the stimulants of interneural and myoneural conduction:A. 1% lobeline solution, 0,1% adrenalin.B. Ascorbic acid, vitamins of group B.

C. Neostigmine methylsulfate (0,1 to 1 ml from 0,05 % solution IM), dibazol.D. Glutamic acid.
45. Glutamic acid is prescribed:A. 0,1 to 1 ml from 0,05 % solution IM.B. Orally in a dose of 0,5 to 2 g daily in powder form or in glucose solution for 10-15 days.C. 0,001 to 0,005 g once a day for 20 to 30 days.D. 0,3 to 0,5 g twice a day.46. Indicate the thermal procedures which are widely employed during the stage of restitution, except:A. warm and hot baths.B. Hot packs.C. Paraffin and ozokerite therapy.D. Transthermia.E. Stimulants of intrneural and myoneural conduction.
47. Indicate the term of isolation for patient with poliomyelitis:A. Till 7th day from the beginning of the disease.B. For 21 days from the onset of the disease.C. Till 11 days from the beginning of the disease.D. Till 10th day from the beginning of the disease.
48. In children's institutions (crèches, nurseries, kindergartens etc.) the group in which a case of poliomyelitis has been discovered is quarantined for:A. 20 days.B. 30 days.C. 11 days.D. 7 days.
49. The main measure to control poliomyelitis is:A. Antibiotic therapy.

B. γ-globulin prescribing.C. Prophylactic vaccination.D. All answers are right.
50. Enumerate measures for prophylaxis of poliomyelitis:A. Earliest isolation of poliomyelitis patient and suspected cases.B. Final disinfection is performed in patient’s dwelling.C. Prophylactic vaccination.D. Contacts are observed for 20 days after isolation of the patient, but are not quarantined.E. All answers are right.
51. Antibiotics in case of poliomyelitis are indicated:A. For prophylaxis.B. To combat complications resulting from secondary infection.C. Should be appointed since the beginning of the disease.D. Should be appointed to all patients with bulbar form in paralytic poliomyelitis.
52. The children of what age most often have poliomyelitis?A. In the first months of life.B. In the first year of life.C. In school age.D. In 15-17 years.E. Before 7 years.
53. What system is most sensitive to the virus of poliomyelitis?A. Nervous system.B. Cardio-vascular system.C. Lymphatic system.D. Bone-muscular system.E. System of blood.

54. What typical features of muscles and joints damage in case of poliomyelitis?A. Hypotonia, hyporeflexia, atrophy, tetraparesis, osteoporosis.B. Hypertonia, and hyperreflexia, "mosaic" damage, osteoporosis.C. Atony, arefiexia, "mosaic" damage, atrophy, shakiness of joints.D. Hypertonia, and hyperreflexia, joints ankylosis.E. Atony, arefiexia, hemiparesis, deformation of spine.
55. Indicate the clinical diagnostic criteria of poliomyelitis:A. Presence of hemiparesis and hyperpyrexia.B. Appearance of spastic palsies after a catarrhal period.C. Flaccid paralyses of especially lower extremities that had appeared after the period of hyperthermia.D. Spontaneous appearance of flaccid paralyses.E. Appearance of tetraparesis after the protracted fever.
56. What vaccination is used in the prophylaxis of poliomyelitis?A. Specific active prophylaxis by anatoxin.B. Specific active prophylaxis by the living loosened vaccine.C. Unspecific active prophylaxis.D. By specific Ig.E. By gamma globulin.
57. When is vaccination against poliomyelitis given?A. From 3 months triply with an interval of 1 week.B. In 1 year, 3 and 6 years.C. Only by an epidemic confirmation.D. From 3 months triply with an interval of 1 month.E. It is not conducted.
58. Indicate the way of vaccine introduction in poliomyelitis at the third vaccination and next revaccinations.A. Through a mouth.

B. Subcutaneous.C. Intradermal.D. Intramuscular.E. Intranasal.
Enteroviral infections
1. Enteroviral infections are caused by:A. By reovirus.B. By herpes virus.C. By poliovirus.D. By the respiratory syncitial virus.E. By ECHO and Coxsackie virus.
2. Way of the agent transmission in Enteroviral infection is:A. Contact-domestic and water.B. Water, domestic and transmissible.C. Orally-fecal and air-droplet.D. Transmissible and ascending.E. Air-droplet and domestic.
3. What clinical signs from enumerated are the most typical for Enteroviral infection and differentiate it from other diseases?A. Meningeal signs.B. Sings of conjunctivitis and rhinitis.C. Presence of papulous rashes and itch.D. Hectic temperature and signs of intoxication.

E. Hyperemia the face and neck, sometimes with appearance of the maculo-papulous rashes.
4. What is needed for confirmation of enteroviral infection?A. Virology of nasopharyngeal smears, urine, CSF and complement binding reaction with paired sera.B. Virology of nasopharyngeal smears, feces, CSF and indirect hemagglutination reaction.C. Virology of nasopharyngeal smears, feces, CSF and complement binding reaction with paired sera.D. Virology of urine, feces, CSF and bacteriological research of feces.E. Virology of nasopharyngeal smears, feces, urine and reaction of indirect fluorescence.
5. What treatment of enteroviral infection is the most correct?A. Diet. Only pathogenetic and symptomatic treatment.B. Specific treatment is not present. Antibiotics and symptomatic treatment.C. Diet. Purpose of antiviral and pathogenetic therapy.D. The changes on diet are not needed. Gamma-globulin and ribonuclease is specific treatment.E. A diet is not appointed. Antibiotics and dehydration treatment.
6. Point out the specific sign of enteroviral diarrhea:A. Gastrointestinal disorders are combined with catarrhal signs from the first days of the disease.B. Tenesmus is present.C. The disease course is malignant.D. All variants are incorrect.
7. Indicate clinical features which specify enteroviral infection:A. Various clinical manifestations which are connected with toxemia, fever, lesions of nervous system and muscles.

B. Predominantly lesions of nervous system.C. Predominantly lesions of intestinal tract.D. Predominantly lesions of respiratory system.
8. What is the specific prophylaxis of enteroviral infection?A. Vaccination by inactivated vaccine in age of 1 year.B. A specific prophylaxis is not developed.C. Vaccination by inactivated vaccine in age of 3 and 9 years.D. Infection of specific Ig in the age of 3 months.E. Infection of specific Ig in the age of 15 months.
9. Indicate preventive measures in the focus of enteroviral infection:A. Observation of patients and contacts, final disinfection.B. Hospitalization of sick and contacts for 10 days, current disinfection.C. Hospitalization of patients, isolation of contacts for 14 days, current disinfection.D. Observation of patients, isolation of contacts for 7 days, final disinfection.E. Observation of patients and contacts, giving them interferon.
10. What preparations are given to children in the focus of enteroviral infection?A. Gamma-globulin and interferon 14-15 days.B. Anaferon for 10 days.C. Antibiotics for 5 days.D. Specific Ig 3 for days.E. Specific anatoxin is given for the first 2 days.
11. The most frequent area of enteroviral infection is:A. Wound surface.B. Mucus membranes of the pharynx and intestine.C. Mucus membranes of the upper respiratory tracts and stomach.
D. Mucus membranes of the intestine.E. Lymphoid organs and cardio-vasculary system.
12. Encephalomyocarditis enteroviral diarrhea is a typical form in children of:A. 3-7 year olds.B. 1-year-olds.C. Teenagers.D. Newborns.
13. At what age is paralytic poliomyelitis-like disease characteristic while enteroviral infection?A. 3-7 year olds.B. 1-year-olds.C. Teenagers.D. Newborns.E. Children from 1 to 3 years of age.
14. Which viruses cause enteroviral infection diseases?A. Picornaviridae family.B. Rotaviruses.C. Arboviruses.D. Ortomiksovirus.
15. The main route of transmission of enteroviral infections:A. Fecal-oral.B. Air-droplet (in the first days of the disease especially).C. There is a possibility of transplacental virus infection.D. All answers are correct.
16. Indicate the clinical form of enteroviral infection which explains tropism of enteroviruses to muscles:A. Myocarditis.B. Gastroenteritis.

C. Epidemic myalgia.D. Herpangina.
17. Describe the clinical features that distinguish enterovirus infection of bacterial intestinal infections:A. Considerable toxemia is absent.B. Diarrhea appears against a background of catarrhal signs.C. Diarrhea frequently is combined with serous meningitis, epidemic myalgia, herpangina, enteroviral exanthemas, acute myocarditis.D. All variants are correct.
18. Point out the specific sign of enteroviral diarrhea:A. Gastrointestinal disorders are combined with catarrhal signs from the first days of the disease.B. Tenesmus is present.C. The disease course is malignant.D. All variants are incorrect.
19. Indicate clinical features which specify on enteroviral infection:A. Various clinical manifestations which are connected with toxemia, fever, lesions of nervous system and muscles.B. Predominantly lessions of nervous system.C. Predominantly lessions of intestinal tract.D. Predominantly lessions of respiratory system.
20. The source of enteroviral infection is:A. Sick human and virus carrier.B. Rodents.C. Birds.D. Fish.
21. What epidemiologic information confirm the diagnosis of enteroviral infection?
A. Presence of group diseases or flashes: the sick children have herpangina, myalgia, and meningitis.B. Presence of group diseases: the sick children have diarrhea, fever, meningitis.C. Presence of flashes: the sick children have herpangina, carditis, and diarrhea.D. Presence of group diseases or flashes: the sick children have severe toxic syndrome, meningitis.E. Presence of periodic flashes: the sick children have herpangina, arthritis, and diarrhea.
22. Indicate the age category for which enteroviral infection is most common:A. Adults.B. Newborns.C. Children from 3 to 10 years of age (the babies of some months to 4 years of age – intestinal form).D. Teenagers.