lidocaine unmasks l-type ca2+ spikes in the thalamus
TRANSCRIPT
Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.XXX 2016 • Volume XXX • Number XXX www.anesthesia-analgesia.org 1
Copyright © 2016 International Anesthesia Research SocietyDOI: 10.1213/ANE.0000000000001158
Lidocaine, when present in the systemic circulation, produces well-known concentration-dependent cen-tral nervous system (CNS) toxicity whose manifesta-
tion initially reflects inhibitory symptoms such as sedation, drowsiness, and alterations in sensorium, before progress-ing to excitatory phenomena including generalized sei-zures, and, in the most severe cases, coma and death.1,2 That lidocaine affects the CNS is not surprising, because it read-ily passes the blood–brain barrier.3 However, in contrast to lidocaine’s peripheral local anesthetic (LA) effects, the
mechanisms and sites of its central actions have received comparatively little study because previous work has emphasized the spinal cord, leaving supraspinal actions relatively unexplored.4 Accordingly, there are no specific mechanism-based therapies for LA CNS toxicity.
Exploring the thalamus as a central site implicated in sys-temic LA actions, we previously found in rat thalamocortical (TC) neurons that lidocaine at clinically neurotoxic concen-trations increases excitability mediated by Na+-independent, high-threshold (HT) action potential spikes.5 Although the
BACKGROUND: High systemic lidocaine concentrations exert well-known toxic effects on the central nervous system (CNS), including seizures, coma, and death. The underlying mechanisms are still largely obscure, and the actions of lidocaine on supraspinal neurons have received com-paratively little study. We recently found that lidocaine at clinically neurotoxic concentrations increases excitability mediated by Na+-independent, high-threshold (HT) action potential spikes in rat thalamocortical neurons. Our goal in this study was to characterize these spikes and test the hypothesis that they are generated by HT Ca2+ currents, previously implicated in neurotoxic-ity. We also sought to identify and isolate the specific underlying subtype of Ca2+ current.METHODS: We investigated the actions of lidocaine in the CNS-toxic concentration range (100 μM–1 mM) on ventrobasal thalamocortical neurons in rat brain slices in vitro, using whole-cell patch-clamp recordings aided by differential interference contrast infrared videomicroscopy. Drugs were bath applied; action potentials were generated using current clamp protocols, and underly-ing currents were identified and isolated with ion channel blockers and electrolyte substitution.RESULTS: Lidocaine (100 μM–1 mM) abolished Na+-dependent tonic firing in all neurons tested (n = 46). However, in 39 of 46 (85%) neurons, lidocaine unmasked evoked HT action potentials with lower amplitudes and rates of de-/repolarization compared with control. These HT action potentials remained during the application of tetrodotoxin (600 nM), were blocked by Cd2+ (50 μM), and disap-peared after superfusion with an extracellular solution deprived of Ca2+. These features implied that the unmasked potentials were generated by high-voltage–activated Ca2+ channels and not by Na+ channels. Application of the L-type Ca2+ channel blocker, nifedipine (5 μM), completely blocked the HT potentials, whereas the N-type Ca2+ channel blocker, ω-conotoxin GVIA (1 μM), had little effect.CONCLUSIONS: At clinically CNS-toxic concentrations, lidocaine unmasked in thalamocortical neu-rons evoked HT action potentials mediated by the L-type Ca2+ current while substantially suppress-ing Na+-dependent excitability. On the basis of the known role of an increase in intracellular Ca2+ in the pathogenesis of local anesthetic neurotoxicity, this novel action represents a plausible contrib-uting candidate mechanism for lidocaine’s CNS toxicity in vivo. (Anesth Analg 2015;XXX:00–00)
Central Nervous System–Toxic Lidocaine Concentrations Unmask L-Type Ca2+ Current–Mediated Action Potentials in Rat Thalamocortical Neurons: An In Vitro Mechanism of Action StudyIgor Putrenko, PhD,* Amer A. Ghavanini, MD, PhD, FRCPC,* Katrin S. Meyer Schöniger, MD,*† and Stephan K. W. Schwarz, MD, PhD, FRCPC*†
From the *Department of Anesthesiology, Pharmacology & Therapeutics, The University of British Columbia, Vancouver, British Columbia, Canada; and †Department of Anesthesia, St. Paul’s Hospital, Vancouver, British Columbia, Canada.
Amer A. Ghavanini, MD, PhD, FRCPC, is currently affiliated with the Division of Neurology, University of Toronto, Ontario, Canada; and Trillium Health Partners, Mississauga, Ontario, Canada.
Katrin S. Meyer Schöniger, MD, is currently affiliated with the Klinik für Anästhesie, Chirurgische Intensivmedizin, Rettungsmedizin und Schmerztherapie [KLIFAIRS], Luzerner Kantonsspital, Luzern, Switzerland.
Accepted for publication December 3, 2015.
Funding: Supported in part by the Canadian Anesthesia Research Foundation through a Canadian Anesthesiologists’ Society Research Award and a
Canadian Anesthesiologists’ Society/Abbott Laboratories Ltd. Career Scientist Award in Anesthesia (Toronto, Ontario, Canada); the Canada Foundation for Innovation (Ottawa, Ontario, Canada); the British Columbia Knowledge Development Fund (Victoria, British Columbia, Canada); a Pfizer Neuropathic Pain Research Award (independently peer-reviewed public oper-ating grant competition sponsored by Pfizer Canada Inc.; Kirkland, Quebec, Canada); and the St. Paul’s Hospital Department of Anesthesia (Vancouver, British Columbia, Canada). Dr. Schwarz holds the Dr. Jean Templeton Hugill Chair in Anesthesia, supported by the Dr. Jean Templeton Hugill Endowment for Anesthesia Memorial Fund.
The authors declare no conflicts of interest.
Reprints will not be available from the authors.
Address correspondence to Stephan K. W. Schwarz, MD, PhD, FRCPC, Department of Anesthesiology, Pharmacology & Therapeutics, The University of British Columbia, 2176 Health Sciences Mall, Vancouver, BC, Canada V6T 1Z3. Address e-mail to [email protected].

Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
Lidocaine Unmasks L-Type Ca2+ Spikes in the Thalamus
2 www.anesthesia-analgesia.org aNesthesia & aNalgesia
ionic basis of these action potentials is unknown, TC neu-rons–central to the generation of conscious states, absence epilepsy, as well as drug-induced sedation, anesthesia, and analgesia6–9–express high-voltage–activated (HVA) Ca2+ cur-rents that generate HT potentials, similar to those in our investigations.10–12 Hence, we conducted an in vitro mecha-nism of action study with the goal to characterize these HT potentials and determine their specific underlying ionic con-ductances, testing the hypothesis that they are generated by HT Ca2+ currents, previously implicated in neurotoxicity.13,14 We also sought to identify and isolate the specific underlying subtype of HT Ca2+ current and investigate the mechanisms that mediate the observed increase in excitability.
METHODSPreparation of Brain SlicesAll animal experiments were approved by the Committee on Animal Care of the University of British Columbia. Our experimental procedures were similar to those described previously.5 Sprague-Dawley rats, aged P13 to P16, were decapitated under deep isoflurane (Abbott Laboratories, Montreal, Canada) anesthesia. The cerebrum was rapidly removed and placed in oxygenated (5% CO2/95% O2), cold (1°C–4°C), artificial cerebrospinal fluid (ACSF) of the fol-lowing composition (mM): 124 NaCl, 2.5 KCl, 1.25 NaH2PO4, 2 CaCl2, 2 MgCl2, 26 NaHCO3, 10 dextrose (pH, 7.3–7.4; 290 mOsm). The brain was dissected into 1 block and mounted on a tissue slicer with cyanoacrylate adhesive. Coronal slices (thickness, 250–300 μm) containing the ventrobasal tha-lamic nuclei were cut on a Leica VT1200S vibratome (Leica Biosystems, Nussloch, Germany), and the block was sub-merged in oxygenated cold ACSF. After cutting, the slices were incubated for >1 hour at room temperature (22°C to 24°C) in oxygenated ACSF.
Electrophysiologic RecordingsWhole-cell patch-clamp recordings were performed in the current-clamp mode with a MultiClamp 700B ampli-fier (Molecular Devices, LLC, Sunnyvale, CA). The patch pipettes for recording were prepared with a Narishige PP-83 2-stage electrode puller (Narishige Scientific Instrument Lab, Tokyo, Japan) using thin-walled boro-silicate glass (World Precision Instruments, Inc., Sarasota, FL) and filled with a solution containing the following (in mM): 139 K-gluconate, 10 ethylene glycol-bis(β-aminoethyl ether)-N,N,N′,N′-tetraacetic acid, 6 KCl, 4 NaCl, 3 MgCl2, 10 HEPES, 0.5 CaCl2, 3 adenosine 5′-triphosphate (disodium salt, Na2ATP), 0.3 guanosine-5′-triphosphate (sodium salt, NaGTP), titrated to pH 7.3 to 7.4 with 10% gluconate. The range of the measured electrode resistances was 5 to 6 MΩ, and access resistance ranged from 10 to 25 MΩ.
For recording, the slices were transferred into a Perspex submersion chamber (volume, 1.5 mL), where they were immobilized with nylon mesh and continuously perfused by gravity with oxygenated ACSF at a flow rate of 2.5 mL/min controlled by a FR-50 flow valve (Harvard Apparatus, Holliston, MA). Individual neurons were visualized with the aid of differential interference contrast infrared videomi-croscopy. For this purpose, an Axio Examiner.D1 fixed-stage microscope (Carl Zeiss Microimaging GmbH, Göttingen,
Germany) was equipped with an apochromatically corrected water immersion objective (W Plan-APOCHROMAT 40×/1.0 DIC M27; working distance, 2.5 mm), differential interference as well as Dodt contrast optics, and a 0.9 condenser. Infrared light was obtained by placing a 770-nm polarizer in the light path. The images were recorded with an IR-1000 infrared CCD video camera system (DAGE-MTI, Michigan City, IN) and displayed on a Triview TBM-1503 black and white moni-tor (Tatung Company of America, Inc., Long Beach, CA).
The patch pipettes were mounted on the headstage of the amplifier and advanced with an MP-285 motorized precision micromanipulation system (Sutter Instrument, Novato, CA). Signals were low-pass filtered at a frequency of 3 kHz and digitized at 10 kHz with a Digidata 1440A 16-bit data acqui-sition system (Molecular Devices, LLC) controlled using pCLAMP software version 10 (Molecular Devices, LLC). Membrane potentials were corrected offline for a liquid junc-tion potential of −8 mV.15 No leak subtraction was performed.
DrugsLidocaine HCl, Cd2+, and nifedipine were obtained from Sigma-Aldrich Canada Ltd. (Mississauga, ON, Canada); ω-conotoxin GVIA and tetrodotoxin (TTX) were obtained from Alomone Labs, Ltd. (Jerusalem, Israel). To prepare con-centrated drug stock solutions, lidocaine and Cd2+ were dis-solved in ACSF; TTX and ω-conotoxin GVIA were dissolved in distilled water; and nifedipine was dissolved in dimethyl sulfoxide. Before application, required aliquots of the stock solutions (stored at 4°C [lidocaine, nifedipine] and −20°C [Cd2+, TTX, ω-conotoxin GVIA, respectively]) were dissolved in fresh ACSF to obtain the respective concentrations. All drugs were applied to the bath by switching from the con-trol perfusate to ACSF containing a desired drug concentra-tion with the aid of a VC-6 perfusion valve control system (Warner Instruments, LLC, Hamden, CT). Recordings were conducted after 6 minutes of perfusion of the slices with a test solution. All results reported reflect steady-state responses.
Data AnalysisData are presented as mean ± SD unless mentioned oth-erwise. Multigroup dose-response comparisons were con-ducted with the use of 1-way analysis of variance with the Bonferroni post test as appropriate. Testing for differences of normalized data from baseline (i.e., a hypothetical mean of 1.0) was performed with a 1-sample t test. Comparisons between 2 groups were conducted with the use of a paired Student t test. We quantified the degree to which 2 variables are related by computing the Pearson correlation coefficient. Statistical tests were 2 tailed. Sample sizes were based on pre-vious experiments,5,16 and, to be conservative, results of sta-tistical comparisons were considered significant at α = 0.01. Configuration variables (amplitudes and dV/dtmax) of indi-vidual spikes in action potential trains are given descriptively and expressed as ranges. Data were analyzed with the use of ORIGIN (OriginLab Corporation, Northampton, MA) and Prism (GraphPad, La Jolla, CA) software.
RESULTSAll neurons used in this study exhibited the characteristic electrophysiologic properties of TC relay neurons, firing

Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2016 • Volume XXX • Number XXX www.anesthesia-analgesia.org 3
repetitive tonic spikes when depolarized by direct current injection from membrane potentials near rest, and a low-threshold Ca2+ potential triggering a spike burst on depolar-ization from hyperpolarized potentials or on rebound from hyperpolarizing pulses.5,10,16 They were characterized by an average resting membrane potential of −64.6 ± 4.8 mV, input resistance of 315 ± 131 MΩ, and membrane capacitance of 188 ± 62 pF (n = 46).
Lidocaine Unmasks High-Threshold Action Potentials
Consistent with its well-known LA properties, bath applica-tion of lidocaine at 100 μM to 1 mM abolished Na+-dependent tonic firing evoked by injection of depolarizing current pulses
into cells current-clamped at approximately −58 mV in all neurons (Fig. 1A, left and center panels). However, in 39 of 46 (85%) neurons, lidocaine unmasked a distinct repetitive fir-ing pattern evoked by injection of current pulses of increased amplitude and characterized by a higher activation threshold and a different spike configuration (Fig. 1A, right panel). The average activation threshold for these HT potentials, defined as the lowest membrane voltage at which these potentials were activated after depolarizing injection of increasing step current pulses from a holding potential of approximately −58 to −60 mV, was −21 ± 8 mV (n = 12), compared with −44 ± 3 mV for control action potentials (P < 0.001). The average low-est current pulse evoking HT potentials (“current threshold”) exceeded that for control action potentials approximately
Figure 1. Lidocaine unmasked high-threshold (HT) action potential spikes in ventrobasal thalamocortical neurons. A, Typical fast tonic repeti-tive action potential firing is evoked in a current-clamped neuron superfused with normal artificial cerebrospinal fluid under baseline condi-tions (control) by injection of a 1-second depolarizing current pulse (left). Application of 100 μM lidocaine completely blocked the tonic firing (middle), but on injection with a current pulse of increased amplitude, lidocaine unmasked a distinct pattern of repetitive HT action potential firing (right). Note that the first 1 to 3 spikes in a train of HT action potentials unmasked by lidocaine of similar morphology to those in control. Lidocaine’s effects were reversible after washout (data not shown). B, Illustrated are magnifications of the fifth spike in a train from (A) at baseline (control) and after application of lidocaine. Lidocaine unmasked spikes of a different configuration, with markedly higher activation thresholds, decreased amplitudes, slower depolarization/repolarization phases, and larger afterhyperpolarizations (AHP; arrow). C, Application to a different neuron of the tonic Na+ channel blocker, tetrodotoxin (TTX; 600 nM), also completely blocked fast tonic “control” firing (left and middle) and unmasked HT potentials when injected with a current pulse of increased amplitude (right). In contrast to lidocaine, neurons treated with TTX fired no action potentials at the beginning of the HT spike trains of similar morphology as those in control.
Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
Lidocaine Unmasks L-Type Ca2+ Spikes in the Thalamus
4 www.anesthesia-analgesia.org aNesthesia & aNalgesia
4-fold (251 ± 158 vs 60 ± 42 pA; n = 12; P < 0.001). The indi-vidual HT action potentials themselves had lower amplitudes (range, 25−37 vs 60−75 mV in control) but were followed by fast afterhyperpolarizations (AHPs) characterized by higher amplitudes (range, 8−16 vs 3−11 mV in control). The HT potentials also exhibited markedly slower depolarization and repolarization phases (maximum rates of increase and decrease, dV/dtmax), which ranged between 0.23 to 0.55 and 2.5 to 4.4 mV/ms, respectively, compared with 13 to 48 and 7 to 23 mV/ms for control action potentials at baseline (Fig. 1B). Of note, the first 1 to 3 spikes in a train of HT action potentials unmasked by lidocaine were fast and had similar morphology to those in control (Fig. 1A, right panel). TTX application to neurons (600 nM) also suppressed baseline tonic firing and unmasked the tonic firing of HT potentials (Fig. 1C). As opposed to lidocaine, TTX completely inhib-ited all fast action potentials preceding the HT potentials. Compared with the 39 neurons in which lidocaine unmasked HT potentials, the 7 neurons that did not exhibit lidocaine-induced HT potentials had similar resting membrane poten-tials and input resistances (P = 0.88 and 0.43, respectively); the average membrane capacitance in the latter was 136 ± 51 vs 197 ± 60 pF in the former (P = 0.015; 95% confidence interval of difference between means, 12−109).
Ionic Basis of High-Threshold Action Potentials Unmasked by Lidocaine
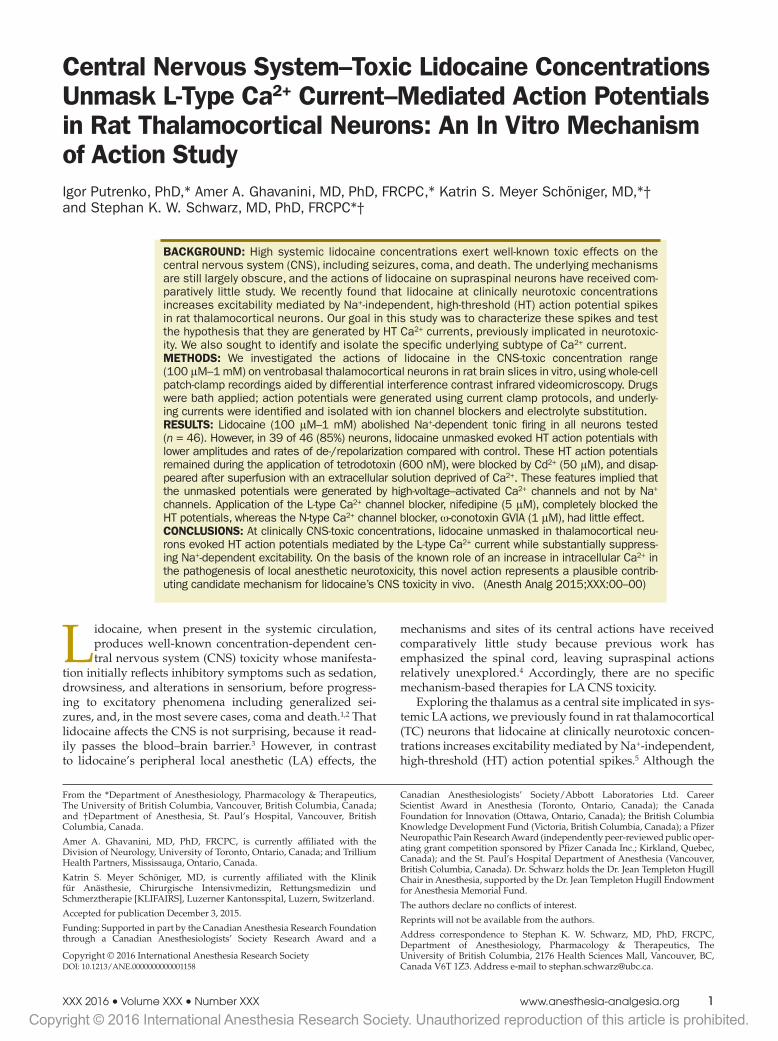
Coapplication of TTX (600 nM) with lidocaine did not block the unmasked HT potentials, supporting the hypothe-sis that the underlying current was not primarily carried by Na+ ions but mediated by Ca2+. When neurons in which HT potentials were evoked in the presence of lidocaine and TTX were perfused with an extracellular solution deprived of Ca2+, the potentials disappeared completely in all neurons
tested (n = 4, Fig. 2A). This effect was fully reversible, with the HT potentials reappearing instantly when the super-fusing medium was changed back to the Ca2+-containing control solution. Application of the nonselective HVA Ca2+ channel blocker, Cd2+ (50 μM),12 completely blocked these HT potentials in a reversible manner in all neurons tested (n = 4; Fig. 2B). Collectively, these results indicated that the HT action potentials unmasked by lidocaine in TC neurons are driven by a HVA Ca2+ current.
The L-Type Ca2+ Current Mediates High-Threshold Action Potentials Unmasked by Lidocaine
Ventrobasal TC neurons express a variety of HVA Ca2+ currents that potentially could underlie the HT poten-tials, including L, N, P/Q, and R types.17 Of these, N-type, L-type, and residual “R”-type currents have been shown to mediate HT potentials in TC neurons in a composite man-ner, with the latter R-type current previously reported to represent the major component.12,18 In the present experi-ments, the observed sustained nature of the HT tonic firing and depolarized holding potential implied that inactivation properties (voltage dependence and rate of inactivation) of Ca2+ currents are critical for determining their suitability for mediating this firing. Characterized by the slowest inactiva-tion rate and most depolarized voltage dependence of inac-tivation among HVA Ca2+ currents is the “long-lasting” L type.19,20 To test the hypothesis that this current mediates the HT tonic firing unmasked by lidocaine, we used the selec-tive L-type Ca2+ channel blocker, nifedipine. In all neurons tested, application of 1 μM nifedipine decreased the ampli-tude of HT potentials (paired t test, P = 0.0001, n = 4) from 34 ± 4 to 25 ± 4 mV (mean ± SD of pairwise difference, −8 ± 1 mV) and increased (depolarized) their activation threshold (paired t test, P = 0.009, n = 4) from −24 ± 9 to −17 ± 10 mV
Figure 2. The high-threshold (HT) action potentials unmasked by lidocaine are mediated by a high-voltage–activated Ca2+ cur-rent. A, The HT action potentials, evoked in the presence of lido-caine (600 μM) and coapplica-tion of tetrodotoxin (TTX; 600 nM; to block Na+ currents and presynaptic transmitter release), reversibly disappeared when the superfusing artificial cerebrospi-nal fluid was deprived of Ca2+. B, The nonselective high-voltage–activated Ca2+ channel blocker, Cd2+ (50 μM), reversibly pro-duced a complete blockade of the HTSs. HTS = high threshold spike (arrows).

Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2016 • Volume XXX • Number XXX www.anesthesia-analgesia.org 5
(mean ± SD of pairwise difference, 7 ± 2 mV. At 5 μM, nife-dipine completely blocked the HT potentials and produced low-amplitude (~2–5 mV) irregular membrane potential oscillations (Fig. 3A). Of note, the fast action potentials at the beginning of the current pulse were not affected by nifedipine. The above effects of nifedipine were reversible. Application of the selective N-type Ca2+ channel blocker, ω-conotoxin GVIA (1 μM), had little effect on the HT fir-ing in 2 of 4 tested neurons (data not shown) and decreased (hyperpolarized) its activation threshold without affecting the amplitude of potentials in the other 2 neurons (ΔV, −7 and −8 mV, respectively; Fig. 3B). Collectively, these results implied that the L-type Ca2+ current, and not N- or R-type currents, mediates the HT action potentials unmasked by lidocaine in TC neurons.
Na+ Channel–Independent Actions of Lidocaine Contribute to the Unmasking of High-Threshold Action Potentials
In addition to voltage-gated Na+ channels, a variety of other ion channels and receptors have been implicated in the actions of lidocaine.5,21–24 To better understand whether such Na+ channel–independent actions contribute to the unmasking of HT spikes in TC neurons, we investigated lidocaine’s actions under conditions of robust Na+ channel blockade in neurons pretreated with TTX (600 nM).
Lidocaine concentration dependently decreased the cur-rent pulse magnitude required to trigger HT potentials in neurons (“current threshold”; Fig. 4A). This effect corre-lated strongly with a concomitant concentration-dependent increase in neuronal input resistance (Fig. 4B).5 At the same time, lidocaine did not affect HT potential spikes per se. The voltage threshold for activation of the HT potential spikes remained unaffected by 600 μM lidocaine in 3 of 5 neu-rons (Fig. 4A); in 2 neurons, the threshold decreased from approximately −19 and −30 to −29 and −37 mV, respectively (data not shown). We observed no significant shift in the voltage threshold of HT potentials with higher (1 mM) and lower (100 and 300 μM) concentrations; as illustrated in Figure 4A, lidocaine also did not significantly affect HT potential amplitudes over the concentration range (each concentration, n = 3−5; data not shown).
At the same time, however, lidocaine blocked the slow AHPs after cessation of depolarizing current pulse injections, known to be attributable to deactivation of the hyperpolar-ization-activated mixed cationic current, Ih
25 (Fig. 5). Under control conditions (TTX), injection in 15-second intervals of step current pulses of a successively increased magnitude (20–40 pA increments) into neurons produced successively larger slow AHPs that gradually hyperpolarized the resting potential at the onset of the next depolarizing pulse (Fig. 5, A and C). This AHP increase was most pronounced (maximum
Figure 3. The L-type Ca2+ current mediates the high-threshold (HT) action potentials unmasked by lidocaine. A, Voltage responses of a current-clamped neuron (upper traces) to 1-second depolarizing suprathreshold step current pulse injections. In the neuron shown, 100 μM lidocaine unmasked tonic HT action potential firing. Coapplication of the L-type Ca2+ current blocker, nifedipine, concentration-dependently (1 μM, partially; 5 μM, completely) and reversibly blocked the HT potential trains under control conditions. B, Shown is the example of another neuron firing HT action potentials unmasked by 600 μM lidocaine. Coapplication of the N-type Ca2+ current blocker, ω-conotoxin GVIA (1 μM), produced no inhibiting effects on the HT potentials. In contrast, in the neuron shown, ω-conotoxin GVIA decreased (hyperpolarized) the HT potential activation threshold, without affecting amplitude, by approximately 7 mV (note also the higher baseline HT potential voltage threshold and current pulse magnitude required to trigger HT potentials [“current threshold”] compared to 100 μM lidocaine; cf., Fig. 4A and body text).

Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
Lidocaine Unmasks L-Type Ca2+ Spikes in the Thalamus
6 www.anesthesia-analgesia.org aNesthesia & aNalgesia
increase, 10 mV) at depolarized voltages after the activation of tonic HT potential firing and associated with a successive decrease in their frequency (Fig. 5, B and D). Application of lidocaine at 100 μM substantially (Fig. 5, A and B) and at 600 μM completely (Fig. 5, C and D) inhibited the AHPs and facilitated the HT firing, such that neurons responded to increased current amplitudes with higher discharge fre-quencies in a quasilinear manner (Fig. 5D).
DISCUSSIONIn the present in vitro mechanism of action study, we found that lidocaine, in the clinically CNS-toxic and con-vulsive concentration range, reversibly unmasked evoked HT action potentials mediated by the L-type Ca2+ current in rat TC neurons, while blocking Na+-dependent excit-ability as expected. The higher thresholds, slower rates of rise and fall, and lower amplitudes of the unmasked Ca2+-dependent action potentials compared with those driven by Na+ are explained by the differences between the activation and inactivation properties of voltage-gated Ca2+ versus Na+ channels.19,26,27
These findings in TC neurons, implicated in the systemic CNS actions of LAs,5,16 are in contrast to previous obser-vations in other tissue preparations that lidocaine blocks various Ca2+ conductances.28–31 Conversely, our results are remarkably consistent with those of Mulle et al.,32 who reported an unmasking of fast prepotentials in TC neurons by intracellular injection of QX-314 (0.1 M in the pipette), a relatively impermeable experimental quaternary lidocaine derivative. The authors concluded that these potentials rep-resent dendritic Ca2+ spikes. Somewhat similarly, Liu et al.33 found in dorsal root ganglion neurons from newborn rats that ropivacaine at 10 and 30 μM markedly increases a HVA Ca2+ current (but decreases it at ≥50 μM).
What possible functional implications do the present results have, and how do they change our views about LA neurotoxicity and its mechanisms? The overall physiologic role of HVA Ca2+ currents in TC neurons, while incom-pletely defined, includes regulation of tonic repetitive firing by triggering Ca2+-induced Ca2+ release from intracellular stores with subsequent activation of Ca2+-dependent K+ cur-rents (IK(Ca))11,17,18,34,35 and generation of high-frequency oscil-latory activity.36 They often complement the firing on top of the low-threshold Ca2+ potentials mediated by T-type Ca2+ currents,37 providing a range of burst firing patterns, and have been implicated in activity-dependent synaptic plas-ticity.38 In addition to these putative physiologic functions, however, HVA Ca2+ channels play an important role in neurotoxicity and cell death in the CNS. The pathogenesis of neurotoxicity involves several mechanisms that collec-tively lead to an increase in intracellular Ca2+ concentra-tions ([Ca2+]i). HVA Ca2+ channels participate in this process both directly and indirectly. They directly facilitate Ca2+ flux intracellularly, which, partially because of their slow inac-tivation, may produce substantial increases in [Ca2+]i.11,34 Alternatively, HVA Ca2+ channels, particularly those of the N type, may increase [Ca2+]i indirectly by mediating excit-atory amino acid release12,39 and subsequent excitatory amino acid–induced excitotoxicity.40 In this regard, the pres-ent observations that lidocaine also unmasked the HT Ca2+ spikes under conditions of presynaptic transmitter release blockade by TTX and N-type Ca2+ channel blockade render direct increases in [Ca2+]i from extracellular sources more likely to be relevant for lidocaine’s neurotoxicity than indi-rect actions such as those mediated by N-type channels.
Although more is known in the literature about the pro-cesses that govern excitotoxicity in general (cf. above) than those involved in systemic LA neurotoxicity specifically, the present findings add to the growing body of evidence indicating that impaired Ca2+ homeostasis similarly con-tributes to the complex and multifaceted mechanisms of the latter. For example, a previous study found that IV lido-caine increases [Ca2+]i in the cortex of anesthetized rats.41 In vitro, an increase in [Ca2+]i in cultured neurons has been reported to play a critical role in the pathogenesis of lido-caine toxicity.23,42 However, it is noteworthy that the effec-tive millimolar concentrations of lidocaine in the latter in vitro studies were higher than the micromolar concentra-tions corresponding to systemic CNS-toxic blood plasma levels in vivo and are, therefore, perhaps more applicable to spinal and regional anesthesia, where such high perineural
Figure 4. Lidocaine decreased the amplitudes of injected current pulses required to trigger high-threshold (HT) action potentials. A, HT potential firing evoked in a neuron under conditions of robust tonic Na+ channel blockade in a neuron pretreated with tetrodo-toxin (TTX; left). Lidocaine had no effects on the voltage thresh-old for activation of HT potentials (arrows) or their amplitudes but decreased the current pulse magnitude required to trigger the HT potentials (current threshold; 600 μM: mean, 76.4% of con-trol [95% confidence interval, 53.1%–99.7%; P = 0.0485; n = 4]). B, Concentration-dependent effects of lidocaine in neurons pre-treated with TTX (600 nM) on the reductions in HT potential current threshold (ΔI) in correlation with concomitant increases in normal-ized neuronal input resistance (ΔRi). The 2 variables exhibited negative correlation based on the 3 concentrations, with a Pearson correlation coefficient of r = −0.9993. Shown are normalized means ± SEM; each concentration, n = 3−5. All effects of lidocaine showed recovery after washout.

Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2016 • Volume XXX • Number XXX www.anesthesia-analgesia.org 7
concentrations of lidocaine are normally encountered.43 These considerations notwithstanding, there has been com-paratively little research on the specific molecular and cellu-lar mechanisms that govern lidocaine-induced increases in [Ca2+]i; both the release of Ca2+ from internal stores and the influx of extracellular Ca2+ have been implicated.23 Hence, the present finding of an unmasking of an L-type channel–mediated HVA Ca2+ current may help bridge the gap in explaining the mechanistic basis of CNS toxicity produced by high lidocaine concentrations in vivo.
Clustered at the somatodendritic junction, L-type Ca2+ channels in TC relay neurons are coupled to intracellular Ca2+ stores through ryanodine receptors and modulate Na+-dependent tonic firing by triggering Ca2+-induced Ca2+ release (cf. above).35,44,45 Therefore, a lidocaine-induced unmasking of L-type Ca2+ current-driven firing can lead to considerable Ca2+ influx and increases in [Ca2+]i in these neurons. The roles of L-type Ca2+ channels in the media-tion of neurodegeneration and cell death, on one hand, and neuroprotective attenuation by pharmacologic L-type Ca2+
channel blockade, on the other hand, are well known from studies in other neuronal tissues.13,14,46,47 For LA neurotox-icity, the observation in the peripheral nervous system by Bainton and Strichartz48 that nifedipine renders frog sciatic nerves more resistant to lidocaine-induced degradation supports this hypothesis. Given the previous findings on the role of [Ca2+]i increases in the pathogenesis of LA neuro-toxicity (mentioned earlier),23,42 the present results are con-sistent with the literature and, hence, represent a plausible contributing mechanism for lidocaine’s supraspinal toxic effects. However, the net level of [Ca2+]i increases in ventro-basal TC relay neurons in humans in vivo is unknown and will also depend on whether lidocaine affects other regula-tory mechanisms of Ca2+ homeostasis, such as Ca2+-induced Ca2+ release, Ca2+-dependent inactivation, and functioning of the Na+–Ca2+ exchanger.35,49–51 For example, Xu et al.22 reported that lidocaine inhibits KCl- and carbachol-evoked intracellular Ca2+ transients in a concentration range similar to that in our study (0.1–2.3 mM), albeit in a neuronal cell culture. Clearly, further research, including studies using
Figure 5. Lidocaine effects on afterhyperpolarizations (AHPs) following step current pulse injection and high-threshold (HT) action potential current–frequency relationships. A and C, Tonic firing of HT action potentials in current-clamped neurons evoked by 1-second depolarizing current step pulses injected in 15-second intervals under conditions of Na+ channel blockade with 600 nM tetrodotoxin (TTX; control) and after coap-plications of 100 and 600 μM lidocaine, respectively. Under control conditions, the incrementally increasing step depolarizations (red traces) were followed by successively larger slow AHPs (left: arrows), leading to gradual hyperpolarization of the baseline resting potential (in the neuron shown, −61 and −59 mV, respectively). Lidocaine at 100 μM partially and at 600 μM completely blocked these AHPs (right: asterisks). Under control conditions, the frequency of HT potential firing evoked by incremental injection of successive step current pulses peaked around 10 Hz; subsequent injection with pulses of higher magnitude decreased firing frequency; red traces on the left side of (A) and (C). B and D, Number of HT spikes triggered in the corresponding neurons (A and B, respectively) plotted against the amplitude of injected current pulses.

Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
Lidocaine Unmasks L-Type Ca2+ Spikes in the Thalamus
8 www.anesthesia-analgesia.org aNesthesia & aNalgesia
Ca2+ imaging, will be helpful and required to elucidate the net effect of lidocaine on Ca2+ homeostasis in the thalamus.
Ventrobasal thalamic neurons functionally express 2 L-type Ca2+ channel isoforms that are distinguished bio-physically and pharmacologically, Cav1.2 and Cav1.3.51–53 Cav1.3 channels, which are less sensitive to dihydropyri-dines, are blocked by 5 to 10 μM nifedipine, whereas Cav1.2 channels are already significantly (>90%) inhibited by nife-dipine concentrations as low as 1 μM.52 Therefore, our obser-vations imply that Cav1.3, rather than Cav1.2, likely drives the observed HT action potentials. Furthermore, the more hyperpolarized (~20–25 mV) activation range of Cav1.3 channels compared with Cav1.2 would render them more suitable for mediating the tonic HT firing. The biophysi-cal properties of a fast rate of inactivation, hyperpolarized inactivation range, and depolarized activation threshold collectively appear to be the key factors preventing other HVA Ca2+ currents expressed in TC neurons from mediat-ing the HT firing. In this regard, our findings also indicate that an R-type Ca2+ current, contrary to what might have been expected based on older studies12,18 (cf. Results, fourth parapgraph) does not significantly contribute to the HT potentials unmasked by lidocaine. This in turn is consistent with reports that the R-type channel, Cav2.3, is not densely expressed in TC neurons.54,55
In this study, TTX also was able to unmask tonic HT firing while completely inhibiting Na+-dependent action potentials. However, the actions of lidocaine, which unlike TTX readily crosses the blood–brain barrier,3 differed from those of TTX in a number of ways because its unmasking effect was more pronounced than TTX. First, the threshold amplitudes of injected current evoking Ca2+-dependent action potentials were lower in lidocaine-treated neurons. It is noteworthy in this context that the HT potentials recorded in the presence of TTX had voltage thresholds consistent with those previously observed in ventrobasal thalamus by Ries and Puil (circa ≥−30 mV)56 but higher than those reported in rat auditory thalamus (ventral partition of the medial geniculate body; approximately ≥−40 mV) by Tennigkeit et al.37 Although these discrepancies remain unclear because neither of these 2 studies isolated the spe-cific underlying HVA Ca2+ currents, it is known that Ca2+ channels, and specifically those of the L type, are subject to differential distribution and expression in different thalamic neurons.45 Second, as opposed to TTX, lidocaine-treated neurons, because of the concentration-dependent inhibi-tion of the slow AHPs, were able to respond to increased current amplitudes by increased HT firing frequency. These effects of lidocaine were likely because of its robust inhibi-tion of Ih in these neurons, which we have previously shown to result in an increase in input resistance and AHP inhibi-tion.5 Third, the activation threshold of the HT potentials, although not in all neurons, was higher in the presence of TTX. A direct action of lidocaine on the L-type Ca2+ current producing a hyperpolarization of the activation threshold may account for this effect. In addition, we have previously demonstrated that inhibition of Ih and a K+ conductance (other than the inward rectifier, IKir) by lidocaine in the high micromolar range produces depolarization of TC neurons operating in the tonic firing mode.5 The latter is consistent
with recent evidence that LAs block various members of the 2-pore domain (“tandem”) K+ channel family that underlies “leak” K+ currents (IKL) in a range of other tissues/prepara-tions.57–59 Combined with a concomitant increase in input resistance, a lidocaine-induced K+ conductance blockade explains the reduction of the amplitudes of injected current required for triggering Ca2+-dependent potentials to the lev-els necessary for evoking Na+-dependent action potentials under control conditions. In this regard, our findings sup-port the 3-decade-old hypothesis of Mulle et al.32 that the occurrence of dendritic HT spikes in TC neurons in the pres-ence of QX-314 (cf. above) results from an increase in input resistance because of inhibition of persistent Na+ and/or K+ conductances. Given the all-or-none nature of Ca2+-driven action potentials, we postulate that the above Na+ channel–independent actions of lidocaine collectively account for the unmasking of HT action potentials driven by the L-type Ca2+ current.
Regarding the clinical relevance of the present lidocaine concentrations, 100 μM lidocaine HCl converts to approxi-mately 27 μg/mL (i.e., a 0.0027% solution). Lidocaine read-ily passes the blood–brain barrier; according to the classic study by Usubiaga et al.,3 CSF concentrations of lidocaine in humans after IV injection correlate to arterial blood lev-els with a factor between 0.73 and 0.83. In rabbits receiv-ing a continuous IV lidocaine infusion, the correlation factor (with a 10-minute latency between arterial and CSF sampling) ranges between ~0.47 and 0.64.60 These data col-lectively imply that a 100 μM CSF concentration would correspond to arterial levels between ~33 and 57 μg/mL in vivo, which unequivocally is in the CNS-toxic range.a
By the nature of the experimental methodology, this study has inherent limitations and shortcomings. First, because the investigations were conducted in juvenile rat brain slices in vitro, the question arises as to what extent the results can be extrapolated to the human patient in vivo. We recognize that such extrapolations require caution. For example, because the experiments were performed at room temperature to facilitate neuronal viability and stable recording conditions, it is reasonable to assume that effec-tive concentrations at 37°C in vivo would likely be lower. Consistent with this, Yokoyama et al.62 found the mean lidocaine plasma concentrations in adult rats at the onset of CNS toxicity (using convulsions as an end point) to be 10.8 μg/mL; similar observations were made by Spiegel et al.63 Although systemic CNS toxicity in humans has been observed at concentrations <5 μg/mL,64 plasma lidocaine levels associated with systemic analgesia in humans are remarkably similar to those effective in rats.65–67 Second, the present studies focused on TC neurons in the ventrobasal thalamus; although these neurons have characteristic elec-trophysiologic properties,5,10,16 it remains to be determined whether other types of neurons would exhibit similar responses to lidocaine. Third, we did not study lidocaine
aIn contrast to the aforementioned studies are the results of 1 investigation that found correlation factors between ~0.06 and 0.08 in humans.61 Although lidocaine’s well-known property to readily penetrate biological membranes at physiologic pH values raises questions about the plausibility of these results, whole brain lidocaine concentrations in the study (1) were signifi-cantly higher than those in the CSF or blood and (2) exceeded cortical con-centrations, indicating that lidocaine accumulates in the cerebral tissue with a preference for subcortical structures, e.g., thalamic nuclei.

Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
XXX 2016 • Volume XXX • Number XXX www.anesthesia-analgesia.org 9
concentrations in excess of 1 mM. However, as discussed earlier, although LA systemic toxicity is not normally associ-ated with millimolar concentrations in the CSF, Mulle et al.32 found that intracellular injection of TC neurons with quater-nary lidocaine at a pipette concentration of 0.1 M unmasked fast dendritic Ca2+ spikes. Fourth, in part because of the well-known difficulties in attaining adequate space clamp of dendritically expressed currents in neurons with a large dendritic tree, we report no data from experiments where HVA Ca2+ currents of TC neurons in the slices were voltage clamped. Finally, it must be emphasized that it was not the goal of this electrophysiologic in vitro study in brain slices to examine histologic or behavioral end points of LA CNS toxicity or investigate lidocaine’s effects on [Ca2+]i; clearly, a body of such future work will be required to elucidate the myriad of concentration-dependent effects that LAs exert on the brain. However, despite unavoidable shortcom-ings, experiments with slices provide a unique opportunity to study neurons in a relatively intact physiologic tissue environment.
In summary, at high-micromolar and clinically CNS-toxic concentrations, lidocaine unmasked in rat TC neurons evoked HT action potentials mediated by the L-type Ca2+ current while substantially suppressing Na+-dependent excitability. The present findings add to our understanding of the complex myriad of LA actions. On the basis of the well-known role of an increase in [Ca2+]i in the pathogenesis of LA neurotoxicity, this novel action in the thalamus, implicated as a central supraspinal site for LAs to produce their systemic CNS effects, represents a plausible contributing candidate mechanism for lidocaine’s CNS toxicity in vivo. E
DISCLOSURESName: Igor Putrenko, PhD.Contribution: This author helped conduct the study, collect the data, analyze the data, and prepare the manuscript.Attestation: Igor Putrenko has reviewed the original study data and data analysis, attests to their integrity, and approved the final manuscript.Name: Amer A. Ghavanini, MD, PhD, FRCPC.Contribution: This author helped conduct the study, collect the data, analyze the data, and prepare the manuscript.Attestation: Amer A. Ghavanini approved the final manuscript.Name: Katrin S. Meyer Schöniger, MD.Contribution: This author helped conduct the study and collect the data.Attestation: Katrin S. Meyer Schöniger approved the final manuscript.Name: Stephan K. W. Schwarz, MD, PhD, FRCPC.Contribution: This author developed the study rationale and design; helped conduct the study, collect the data, analyze the data, and prepare the manuscript; and is the archival author.Attestation: Stephan K. W. Schwarz has reviewed the origi-nal study data and data analysis, attests to their integrity, and approved the final manuscript.This manuscript was handled by: Markus W. Hollmann, MD, PhD, DEAA.
ACKNOWLEDGMENTSThe authors thank Ernest Puil, PhD, for valuable discussions and insightful comments.
REFERENCES 1. Covino BG. Toxicity and systemic effects of local anesthetic
agents. In: Strichartz GR, ed. Handbook of Experimental Pharmacology, Vol 81: Local Anesthetics. Berlin: Springer-Verlag, 1987:187–212
2. Wallace MS, Laitin S, Licht D, Yaksh TL. Concentration-effect relations for intravenous lidocaine infusions in human volun-teers: effects on acute sensory thresholds and capsaicin-evoked hyperpathia. Anesthesiology 1997;86:1262–72
3. Usubiaga JE, Moya F, Wikinski JA, Wikinski R, Usubiaga LE. Relationship between the passage of local anaesthetics across the blood-brain barrier and their effects on the central nervous system. Br J Anaesth 1967;39:943–7
4. Mao J, Chen LL. Systemic lidocaine for neuropathic pain relief. Pain 2000;87:7–17
5. Putrenko I, Schwarz SK. Lidocaine blocks the hyperpolariza-tion-activated mixed cation current, I(h), in rat thalamocortical neurons. Anesthesiology 2011;115:822–35
6. McCormick DA, Bal T. Sleep and arousal: thalamocortical mechanisms. Annu Rev Neurosci 1997;20:185–215
7. Alkire MT, Hudetz AG, Tononi G. Consciousness and anesthe-sia. Science 2008;322:876–80
8. Franks NP. General anaesthesia: from molecular targets to neuronal pathways of sleep and arousal. Nat Rev Neurosci 2008;9:370–86
9. Kuisle M, Wanaverbecq N, Brewster AL, Frère SG, Pinault D, Baram TZ, Lüthi A. Functional stabilization of weakened tha-lamic pacemaker channel regulation in rat absence epilepsy. J Physiol 2006;575:83–100
10. Jahnsen H, Llinás R. Ionic basis for the electro-responsiveness and oscillatory properties of guinea-pig thalamic neurones in vitro. J Physiol 1984;349:227–47
11. Hernández-Cruz A, Pape HC. Identification of two calcium currents in acutely dissociated neurons from the rat lateral geniculate nucleus. J Neurophysiol 1989;61:1270–83
12. Pfrieger FW, Veselovsky NS, Gottmann K, Lux HD. Pharmacological characterization of calcium currents and synaptic transmission between thalamic neurons in vitro. J Neurosci 1992;12:4347–57
13. Mason RP, Leeds PR, Jacob RF, Hough CJ, Zhang KG, Mason PE, Chuang DM. Inhibition of excessive neuronal apoptosis by the calcium antagonist amlodipine and antioxidants in cerebel-lar granule cells. J Neurochem 1999;72:1448–56
14. Cano-Abad MF, Villarroya M, García AG, Gabilan NH, López MG. Calcium entry through L-type calcium channels causes mitochondrial disruption and chromaffin cell death. J Biol Chem 2001;276:39695–704
15. Zhang L, Krnjević K. Whole-cell recording of anoxic effects on hippocampal neurons in slices. J Neurophysiol 1993;69:118–27
16. Schwarz SK, Puil E. Analgesic and sedative concentrations of lignocaine shunt tonic and burst firing in thalamocortical neu-rones. Br J Pharmacol 1998;124:1633–42
17. Kammermeier PJ, Jones SW. High-voltage-activated calcium currents in neurons acutely isolated from the ventrobasal nucleus of the rat thalamus. J Neurophysiol 1997;77:465–75
18. Guyon A, Leresche N. Modulation by different GABAB recep-tor types of voltage-activated calcium currents in rat thalamo-cortical neurones. J Physiol 1995;485(pt 1):29–42
19. Yamakage M, Namiki A. Calcium channels—basic aspects of their structure, function and gene encoding; anesthetic action on the channels–a review. Can J Anaesth 2002;49:151–64
20. Snutch TP, Peloquin J, Mathews E, McRory JE. Molecular properties of voltage-gated calcium channels. In: Zamponi G, ed. Voltage-Gated Calcium Channels. New York: Kluwer Academic/Plenum Publishers, 2005:61–94
21. Sakura S, Bollen AW, Ciriales R, Drasner K. Local anesthetic neurotoxicity does not result from blockade of voltage-gated sodium channels. Anesth Analg 1995;81:338–46
22. Xu F, Garavito-Aguilar Z, Recio-Pinto E, Zhang J, J Blanck TJ. Local anesthetics modulate neuronal calcium signaling through multiple sites of action. Anesthesiology 2003;98:1139–46
23. Gold MS, Reichling DB, Hampl KF, Drasner K, Levine JD. Lidocaine toxicity in primary afferent neurons from the rat. J Pharmacol Exp Ther 1998;285:413–21
Copyright © 2016 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
Lidocaine Unmasks L-Type Ca2+ Spikes in the Thalamus
10 www.anesthesia-analgesia.org aNesthesia & aNalgesia
24. Bischoff U, Bräu ME, Vogel W, Hempelmann G, Olschewski A. Local anaesthetics block hyperpolarization-activated inward current in rat small dorsal root ganglion neurones. Br J Pharmacol 2003;139:1273–80
25. McCormick DA, Pape HC. Properties of a hyperpolarization-activated cation current and its role in rhythmic oscillation in thalamic relay neurones. J Physiol 1990;431:291–318
26. Docherty RJ, Farmer CE. The pharmacology of voltage-gated sodium channels in sensory neurones. Handb Exp Pharmacol 2009:519–61
27. Ohmori H, Sato Y, Namiki A. The anticonvulsant action of pro-pofol on epileptiform activity in rat hippocampal slices. Anesth Analg 2004;99:1095–101
28. Frelin C, Vigne P, Lazdunski M. Biochemical evidence for phar-macological similarities between alpha-adrenoreceptors and voltage-dependent Na+ and Ca++ channels. Biochem Biophys Res Commun 1982;106:967–73
29. Palade PT, Almers W. Slow calcium and potassium currents in frog skeletal muscle: their relationship and pharmacologic properties. Pflugers Arch 1985;405:91–101
30. Oyama Y, Sadoshima J, Tokutomi N, Akaike N. Some prop-erties of inhibitory action of lidocaine on the Ca2+ current of single isolated frog sensory neurons. Brain Res 1988;442:223–8
31. Sugiyama K, Muteki T. Local anesthetics depress the calcium current of rat sensory neurons in culture. Anesthesiology 1994;80:1369–78
32. Mulle C, Steriade M, Deschênes M. The effects of QX314 on tha-lamic neurons. Brain Res 1985;333:350–4
33. Liu BG, Zhuang XL, Li ST, Xu GH, Brull SJ, Zhang JM. Effects of bupivacaine and ropivacaine on high-voltage-activated calcium currents of the dorsal horn neurons in newborn rats. Anesthesiology 2001;95:139–43
34. Zhou Q, Godwin DW, O’Malley DM, Adams PR. Visualization of calcium influx through channels that shape the burst and tonic firing modes of thalamic relay cells. J Neurophysiol 1997;77:2816–25
35. Budde T, Sieg F, Braunewell KH, Gundelfinger ED, Pape HC. Ca2+-induced Ca2+ release supports the relay mode of activity in thalamocortical cells. Neuron 2000;26:483–92
36. Pedroarena C, Llinás R. Dendritic calcium conductances gener-ate high-frequency oscillation in thalamocortical neurons. Proc Natl Acad Sci USA 1997;94:724–8
37. Tennigkeit F, Schwarz DW, Puil E. Modulation of bursts and high-threshold calcium spikes in neurons of rat auditory thala-mus. Neuroscience 1998;83:1063–73
38. Lo FS, Ziburkus J, Guido W. Synaptic mechanisms regulating the activation of a Ca(2+)-mediated plateau potential in devel-oping relay cells of the LGN. J Neurophysiol 2002;87:1175–85
39. Takahashi T, Momiyama A. Different types of calcium channels mediate central synaptic transmission. Nature 1993;366:156–8
40. Choi DW. Excitotoxic cell death. J Neurobiol 1992;23:1261–76 41. Du C, Yu M, Volkow ND, Koretsky AP, Fowler JS, Benveniste
H. Cocaine increases the intracellular calcium concentration in brain independently of its cerebrovascular effects. J Neurosci 2006;26:11522–31
42. Johnson ME, Saenz JA, DaSilva AD, Uhl CB, Gores GJ. Effect of local anesthetic on neuronal cytoplasmic calcium and plasma membrane lysis (necrosis) in a cell culture model. Anesthesiology 2002;97:1466–76
43. Kalichman MW, Moorhouse DF, Powell HC, Myers RR. Relative neural toxicity of local anesthetics. J Neuropathol Exp Neurol 1993;52:234–40
44. Pape HC, Munsch T, Budde T. Novel vistas of calcium-medi-ated signalling in the thalamus. Pflugers Arch 2004;448:131–8
45. Budde T, Munsch T, Pape HC. Distribution of L-type calcium channels in rat thalamic neurones. Eur J Neurosci 1998;10:586–97
46. Porter NM, Thibault O, Thibault V, Chen KC, Landfield PW. Calcium channel density and hippocampal cell death with age in long-term culture. J Neurosci 1997;17:5629–39
47. Thibault O, Landfield PW. Increase in single L-type calcium channels in hippocampal neurons during aging. Science 1996;272:1017–20
48. Bainton CR, Strichartz GR. Concentration dependence of lidocaine-induced irreversible conduction loss in frog nerve. Anesthesiology 1994;81:657–67
49. Rankovic V, Ehling P, Coulon P, Landgraf P, Kreutz MR, Munsch T, Budde T. Intracellular Ca2+ release-dependent inac-tivation of Ca2+ currents in thalamocortical relay neurons. Eur J Neurosci 2010;31:439–49
50. Miller RJ. The control of neuronal Ca2+ homeostasis. Prog Neurobiol 1991;37:255–85
51. Cheong E, Lee S, Choi BJ, Sun M, Lee CJ, Shin HS. Tuning thalamic firing modes via simultaneous modulation of T- and L-type Ca2+ channels controls pain sensory gating in the thala-mus. J Neurosci 2008;28:13331–40
52. Xu W, Lipscombe D. Neuronal Ca(V)1.3alpha(1) L-type chan-nels activate at relatively hyperpolarized membrane potentials and are incompletely inhibited by dihydropyridines. J Neurosci 2001;21:5944–51
53. Lipscombe D, Helton TD, Xu W. L-type calcium channels: the low down. J Neurophysiol 2004;92:2633–41
54. Weiergräber M, Henry M, Ho MS, Struck H, Hescheler J, Schneider T. Altered thalamocortical rhythmicity in Ca(v)2.3-deficient mice. Mol Cell Neurosci 2008;39:605–18
55. Parajuli LK, Nakajima C, Kulik A, Matsui K, Schneider T, Shigemoto R, Fukazawa Y. Quantitative regional and ultra-structural localization of the Ca(v)2.3 subunit of R-type calcium channel in mouse brain. J Neurosci 2012;32:13555–67
56. Ries CR, Puil E. Mechanism of anesthesia revealed by shunting actions of isoflurane on thalamocortical neurons. J Neurophysiol 1999;81:1795–801
57. Kindler CH, Paul M, Zou H, Liu C, Winegar BD, Gray AT, Yost CS. Amide local anesthetics potently inhibit the human tan-dem pore domain background K+ channel TASK-2 (KCNK5). J Pharmacol Exp Ther 2003;306:84–92
58. Kim Y, Bang H, Kim D. TASK-3, a new member of the tandem pore K(+) channel family. J Biol Chem 2000;275:9340–7
59. Kindler CH, Yost CS. Two-pore domain potassium channels: new sites of local anesthetic action and toxicity. Reg Anesth Pain Med 2005;30:260–74
60. Momota Y, Artru AA, Powers KM, Mautz DS, Ueda Y. Concentrations of lidocaine and monoethylglycine xylidide in brain, cerebrospinal fluid, and plasma during lidocaine-induced epileptiform electroencephalogram activity in rabbits: the effects of epinephrine and hypocapnia. Anesth Analg 2000;91:362–8
61. Tsai PS, Buerkle H, Huang LT, Lee TC, Yang LC, Lee JH. Lidocaine concentrations in plasma and cerebrospinal fluid after systemic bolus administration in humans. Anesth Analg 1998;87:601–4
62. Yokoyama M, Benson KT, Arakawa K, Goto H. Effects of flu-mazenil on intravenous lidocaine-induced convulsions and anticonvulsant property of diazepam in rats. Anesth Analg 1992;75:87–90
63. Spiegel DA, Dexter F, Warner DS, Baker MT, Todd MM. Central nervous system toxicity of local anesthetic mixtures in the rat. Anesth Analg 1992;75:922–8
64. Landy C, Schaeffer E, Raynaud L, Favier JC, Plancade D. Convulsions after normal dose of lidocaine: a probable drug interaction. Br J Anaesth 2012;108:701
65. Puig S, Sorkin LS. Formalin-evoked activity in identified pri-mary afferent fibers: systemic lidocaine suppresses phase-2 activity. Pain 1996;64:345–55
66. Abram SE, Yaksh TL. Systemic lidocaine blocks nerve injury-induced hyperalgesia and nociceptor-driven spinal sensitiza-tion in the rat. Anesthesiology 1994;80:383–91
67. Sinnott CJ, Garfield JM, Strichartz GR. Differential efficacy of intravenous lidocaine in alleviating ipsilateral versus contralat-eral neuropathic pain in the rat. Pain 1999;80:521–31