long-term outcome after cataract surgery – a longitudinal...
TRANSCRIPT

UMEÅ UNIVERSITY MEDICAL DISSERTATIONS
New series No 1319 •ISSN 0346-7532 • ISBN 978-91-7264-911-8
____________________________________
Long-term outcome after cataract
surgery – a longitudinal study.
Britta Lundqvist
Umeå 2010
From the Department of Clinical Sciences, Ophthalmology
Umeå University, Umeå, Sweden
2
Department of Clinical Sciences Ophthalmology Umeå University SE-901 85 Umeå Sweden
Copyright © Britta Lundqvist New Series No 1319 ISSN: 0345-7532 ISBN: 978-91-7264-911-8 Printed in Sweden by Arkitektkopia, Umeå, 2009

3
To Oskar, Amanda, and Julia!

4
ABSTRACT
Background
Cataract surgery is the most common surgical procedure carried out
in the developed world and surgery volumes have increased
considerably during the last decades. Various aspects of the surgical
procedure, including surgical incision size and intraocular lens
materials, have changed substantially, improving the safety and the
quality of the outcome. Previous research has primarily focused on
the visual function results with a short follow-up time. Long-term
population-based studies, exceeding a few years, presenting visual
functional results postoperatively, have not been published.
Aims
To determine the effects of cataract surgery on subjectively
experienced visual function and visual acuity in a defined population,
and compare the results between sub-groups, on a long-term basis.
Methods
In this prospective, population-based investigation, all patients with
presenile and senile cataract (n=810), operated on during a one-year
period (1997-98), at Umeå University Hospital were included. The
frequency of cataract surgery at that time, was 5.2 per 1000
population studied. Visual acuity was tested and an eye examination
was performed before surgery, 4-8 weeks postoperatively, and five
and ten years after surgery. Subjective visual function was assessed
using self-administered questionnaires (VF-14) at all occasions.
Statistical evaluations comprised analyses of variance, Mann-Whitney
5
U-test, chi-square test, multiple linear regression, a life-table
calculation, and Cox’s proportional hazard model.
Results
Five years after cataract surgery, subjective and objective visual
function remained stable in most patients. The most frequent cause of
deterioration of visual acuity and decrease in VF-14 scores was age-
related macular degeneration (ARMD).
Two thirds of the patients in the cohort were women. They were
significantly older than the men and more often operated on both
eyes. After adjustment for age and visual acuity, women cataract
surgery patients assessed their visual function worse than men both
before surgery and 4 months postoperatively. Five years after surgery
these differences were no longer significant.
At baseline, 13% of the patients were diabetics. At the five-year follow-
up, subjective and objective visual function remained stable in most
surviving diabetics, and the longitudinal visual function was not
significantly worse compared with the non-diabetics.
Ten years after surgery, 28% had received treatment for posterior
capsular opacification (PCO). A significantly larger proportion of
patients less than 65 years at surgery (37%) compared with those 65
years or older (20%) had been treated.
Conclusions
Most patients sustain their level of visual acuity and visual function
also five and ten years after cataract surgery. Ocular co-morbidity,
such as ARMD, is the major cause of longitudinally reduced visual
6
function. Patients suffering from diabetes did not have a significantly
worse visual function after five years. A surprisingly large proportion
of patients had received treatment for PCO after ten years.
Key words
Cataract, cataract surgery outcome, longitudinal study, subjective
visual acuity.
7
SVENSK SAMMANFATTNING
Bakgrund
Kataraktkirurgi (gråstarroperation) är den vanligaste operationen i
västvärlden och operationsvolymerna har ökat markant under de
senaste decennierna. Olika aspekter av kirurgin, som t.ex. storleken
på operationssnittet och materialet i de nya linserna, har förändrats
väsentligt. Det har medfört ökad kvalité och bättre resultat. Tidigare
forskning har framförallt bekrivit operationsresultaten med kort
uppföljningstid. Långtidsstudier beträffande synfunktionen som
sträcker sig längre än några år efter operationen har inte tidigare
publicerats.
Syfte
Att fastställa hur kataraktkirurgi påverkar subjektiv synfunktion och
synskärpa i en befolkning under ett längre tidsperspektiv. Att jämföra
resultaten mellan olika grupper.
Metod
I denna prospektiva, populationsbaserade undersökning
inkluderades alla patienter med senil och presenil katarakt (n=810),
som opererades under ett års tid (1997-98) vid ögonkliniken, Umeå
Universitetssjukhus. Vid tiden för studien var frekvensen
kataraktoperationer 5.2 per 1000 invånare. Synskärpan
kontrollerades och en ögonundersökning genomfördes före
operationen, 4-8 veckor efter operationen, samt 5 och 10 år senare.
Den subjektiva synfunktionen kontrollerades med hjälp av en enkät,
den s.k. VF-14. Olika metoder som, variansanalys, Mann-Whitney U-

8
test, chi-square test, multipel linjär regression, samt Cox-analys
tillämpades för de statistiska beräkningarna.
Resultat
Både subjektiv (resultat från enkät) och objektiv (synskärpa)
synfunktion var stabil bland de flesta patienter. Den vanligaste
orsaken till försämring av synfunktionen var åldersförändringar i gula
fläcken (makuladegeneration).
Två tredjedelar av studiens deltagare var kvinnor. De var signifikant
äldre än männen och oftare opererade på båda ögonen. Efter
justering för ålder och synskärpa, skattade kvinnorna sin synfunktion
sämre än männen både före operationen och efter 4 månader. Fem år
senare var skillnaderna inte längre signifikanta.
Vid studiens början var 13% av deltagarna diabetiker. Vid 5-
årskontrollen var både den subjektiva och de objektiva synfunktionen
stabil hos de flesta diabetiker som fortfarande var i livet.
Förändringen i synskärpa från postoperativt till fem år efter
operationen var inte signifikant sämre än den som noterades hos
icke-diabetiker.
Tio år efter operationen hade 28% behandlats med laser pga
efterstarr. En signifikant större andel patienter som var yngre än 65
år vid tiden för operation (37%) jämfört med de som var 65 år eller
äldre vid operationstillfället (20%) hade behandlats.
9
Konklusion
Hos de flesta patienter bibehålls både synskärpan och den subjektiva
synfunktion 5 och 10 år efter kataraktoperationen. Den vanligaste
orsaken till försämrad synskärpa/synfunktion var andra
ögonsjukdomar som t.ex ålderförändringar i gula fläcken. Diabetiker
hade inte sämre synfunktion efter 5 år jämfört med icke-diabetiker.
Tio år efter kataraktoperationen hade en förvånansvärt stor andel
patienter behandlats med YAG-laser pga efterstarr.
Nyckelord
Gråstarr, resultat efter gråstarrkirurgi, långtidsstudier, subjektiv
synfunktion.
10
ABBREVIATIONS ARMD Age-related macular degeneration
BCVA Best corrected visual acuity
DR Diabetic retinopathy
ECCE Extra capsular cataract extraction
ETDRS Early Treatment Diabetic Retinopathy Study
ICCE Intra-capsular cataract extraction
IOL Intraocular lens
logMAR Logarithm of the minimum angle of resolution
Nd:YAG Neodymium, yttrium, aluminium, and garnet
PCO Posterior capsular opacification
PMMA Poly (methyl metacrylate)
PVA Presenting visual acuity
SD Standard deviation
VA Visual acuity
VF-14 Visual Function Questionnaire (with 14 questions)
WHO World Health Organization
QOL Quality of Life
11
TABLE OF CONTENTS ABSTRACT .................................................................. 4
SVENSK SAMMANFATTNING .................................... 7
ABBREVIATIONS ..................................................... 10
ORIGINAL PAPERS ................................................... 13
INTRODUCTION
Cataract, definition and anatomy .............................................. 14
History of cataract surgery ......................................................... 17
Surgical techniques and indications .......................................... 20
Epidemiology and public demands ............................................ 24
Outcome studies ......................................................................... 27
Gender in medicine .................................................................... 29
Diabetes retinopathy, diabetes and cataract ............................. 32
Posterior capsular opacification ................................................ 34
AIMS OF THE STUDY ........................................................... 39
ETHICS ..................................................................... 39
PATIENTS AND METHODS
Study design and study population……………………………………..40
Inclusion and exclusion criteria .................................................40
Examinations……………………………………………………………………41
Data collected before and shortly after surgery…………………….41
Questionnaire…………………………………………………………………..43
Data collected 5 and 10 years after surgery…………………………..45
Subgroups ................................................................................... 50
Statistical methods ..................................................................... 51

12
RESULTS
Cataract surgery demographics ................................................. 54
Subjective visual ability .............................................................. 58
Visual acuity results ................................................................... 59
Women and men ........................................................................60
Diabetics ..................................................................................... 62
Younger cataract patients .......................................................... 63
DISCUSSION
Study design, validity and reliability ......................................... 66
Visual outcome analysis ............................................................. 70
Gender-related differences in cataract surgery outcome .......... 72
Visual function and progression of retinopathy in diabetics .... 74
Cataract surgery outcome in younger patients .......................... 77
CONCLUSION ........................................................... 79
FUTURE PERSPECTIVES .......................................... 80
ACKNOWLEDGEMENTS ........................................... 82
REFERENCES ........................................................... 84
APPENDIX ............................................................... 103
PAPERS I-IV
13
ORIGINAL PAPERS This thesis is based on the following original papers, which will be
referred to in the text by their Roman numerals.
I Lundqvist B., Mönestam E. Longitudinal changes in
subjective and objective visual function 5 years after
cataract surgery, a population based study. J Cataract
Refract Surg 2006;32:1944-50.
II Lundqvist B., Mönestam E. Gender-related differences
in cataract surgery outcome: a 5-year follow-up. Acta
Ophthalmol 2008;86(5):543-48.
III Lundqvist B., Mönestam E. Longitudinal changes in
subjective and objective visual function in diabetics 5
years after cataract surgery. Submitted.
IV Lundqvist B., Mönestam E. Ten-Year Longitudinal
Visual Function and YAG Laser capsulotomy Rates in
Patients Less Than 65 Years at Cataract Surgery. In
press for publication in Am J Ophthalmol. Published on
line (www.ajo.com) November 18, 2009.
Reprints were made with permission from the publishers.
14
INTRODUCTION
Cataract, definition and anatomy
Cataract is defined as an opacification of the crystalline lens leading to
visual impairment, usually manifested in ageing people. There is no
known protective agent that can delay the onset or progression of
cataract. The disorder cannot be cured by laser or drugs, and in the
past it led to blindness. Today, only one treatment is known, to
surgically remove the lens and replace it by an intraocular plastic
lens.1
The crystalline lens is one of the few structures of the body with
continuous growth during lifetime.2 The structure is transparent,
biconvex, and avascular, and situated in the anterior part of the eye,
behind the iris.
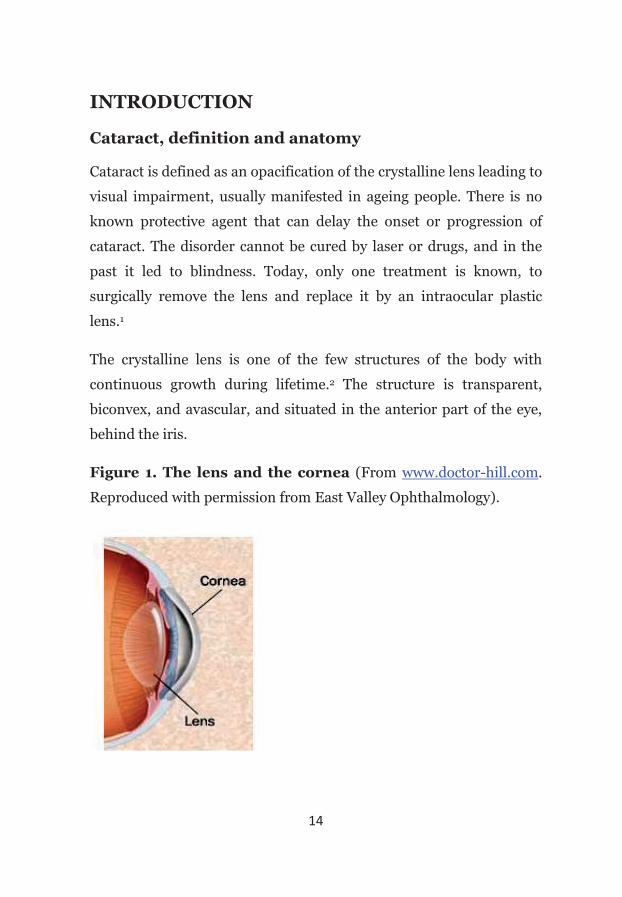
Figure 1. The lens and the cornea (From www.doctor-hill.com.
Reproduced with permission from East Valley Ophthalmology).
15
The lens plays a major role in the optical system of the eye and is
responsible for 1/3 of the refractive power, while the remaining 2/3
are provided by the cornea. At birth, the diameter of the lens
measures about 6.5 mm at the equator, and increases in size to
approximately 9 mm in the adult eye. The lens is derived from
ectodermal tissue and contains epithelial cells that produce lens fibres
throughout life-time. With increasing age, these lenticular fibres
become more compact and thicker, and gradually there is an
accumulation of yellow-brown pigment in the fibres. These changes
reduce light transmission, and when there is a loss of optical clarity,
the lens is cataractous3. Since cataract most commonly appear in
elderly people, it is called “senile cataract”. However, if cataract
develops before the age of 60, it can be defined as a presenile cataract.
The lens fibres are surrounded by a capsule, and zonular fibres
attached to the ciliary body support the lens.
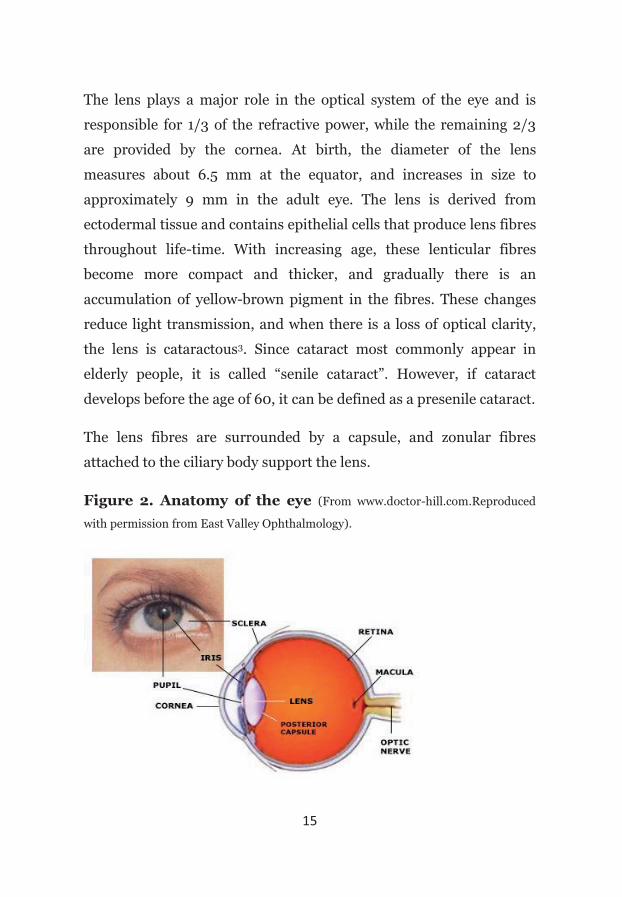
Figure 2. Anatomy of the eye (From www.doctor-hill.com.Reproduced
with permission from East Valley Ophthalmology).
16
Cataract is not always due to ageing. Other causes include congenital
disorders, metabolic conditions, and various forms of trauma, e.g.
direct penetration and contusion.2 Furthermore, cataract
development is enhanced by environmental factors such as smoking,4
and ultraviolet radiation.5 Systemic and inhaled corticosteroids have
been associated with posterior subcapsular cataract, and higher doses
and longer duration increase the risk for cataract.6 In several
epidemiological studies, diabetes has also been considered a risk
factor for cataract.7-9 In experimental studies, cataract develops more
frequently in mice lacking the enzyme superoxide dismutase.10,11 This
enzyme protects against oxidative stress, which plays an important
role in the development of cataract as well as macular degeneration.
There are three main types of age-related cataracts: nuclear, cortical,
and posterior subcapsular.12
Nuclear cataracts tend to progress slowly, and they are
usually bilateral. This type of cataract forms in the nucleus, in
the center of the lens. Typically they cause greater impairment
of distance vision because increased density of the lens
nucleus causes a “myopic shift”, which also may enable
presbyopic individuals to read without glasses.
Opacification of the lens cortex can lead to cortical cataract,
where the main symptoms can be glare, and monocular
diplopia. The opacities are located in the cortical layer and
initially develop in the lower portion of the lens. In early
stages of cortical cataracts, water clefts and vacuoles can be

17
seen. In more advanced stages, wedge-shaped opacities
progress circumferentially.
Posterior subcapsular cataract is located in the posterior
cortical layers of the lens. At slit-lamp examination, granular,
sometimes glistening opacities are present in the posterior
pole. This type of cataract is especially associated with the use
of steroids, myopia, and diabetes. Patients with posterior
subcapsular cataract often complain of glare and poor vision
under bright lightning conditions. Near vision acuity tends to
be more reduced than distance visual acuity.
Figure 3. Nuclear, cortical, and subcapsular cataract
(Photograph of cortical cataract from www.dr-hill.com. Reproduced with permission
from East Valley Ophthalmology).
All these three types of cataract lead to blurred vision at far and near,
reduced contrast acuity and color perception. Cataract surgery is the
only available treatment.
History of cataract surgery
The word cataract, “chatharacta”, derives from the Greek word
meaning waterfall. Until the mid 1770s, it was thought that cataract

18
was formed by opaque material, flowing like a waterfall, in the eye.
Sankskrit manuscripts from the 5th century B.C. describe a type of
cataract surgery known as “couching” or “reclination”. In this
technique, a needle was inserted into the eye, and the cataractous lens
was displaced away from the pupil and pushed into the vitreous
cavity13. This displacement enabled the patient to see better.
Figure 4. Couching (From www.mrcophth.com).
The complication rate with this kind of surgery was extremely high,
and the visual results were, at that time, very limited without
spectacles. This method would, however, allow patients with mature
cataracts to regain a limited degree of vision which was better than
cataract blindness.14
A new method for removing the cataract was introduced by Jaques
Daviel in Paris in 1748.15 By using pressure of his thumb, he removed
the entire lens intact through an incision.

19
Figure 5. Daviel’s method of cataract extraction.
(From www.mrcophth.com.)
It was not until the 1840s that general anesthesia was introduced for
surgical procedures, and in 1884 cocaine drops were developed for
topical anesthesia.13
In 1949, after studying shrapnel wounds in the eyes of soldiers during
World War II, the British ophthalmologist Harold Ridley was the first
surgeon to introduce the intraocular lens (IOL), a permanent plastic
lens implanted inside the eye to replace the crystalline lens.16 Over the
next years many doctors disagreed with replacing the natural lens
with a foreign, artificial lens. It was not until the end of the 1970s,
20
that replacement of the opaque lens by a plastic intraocular lens
became the technique of choice when performing cataract surgery.
In 1957, the Spanish ophthalmologist, Barraquer, used alpha-
chymotrypsin to dissolve the zonular threads to simplify removal of
the lens.17 Cryosurgery was introduced in 1961 by the Polish surgeon
Krwawicz.18 The lens was removed by using a tiny probe that could
attach by freezing a small area on the surface of the cataract.
In the late 1960s, Charles Kelman from New York developed a
technique of emulsifying the lens contents within the capsular bag,
using ultrasonic vibrations and aspiration of the emulsified cataract.19
The ultrasonic technique is still the treatment of choice for most
cataract surgery in the western world.
Surgical techniques and indications
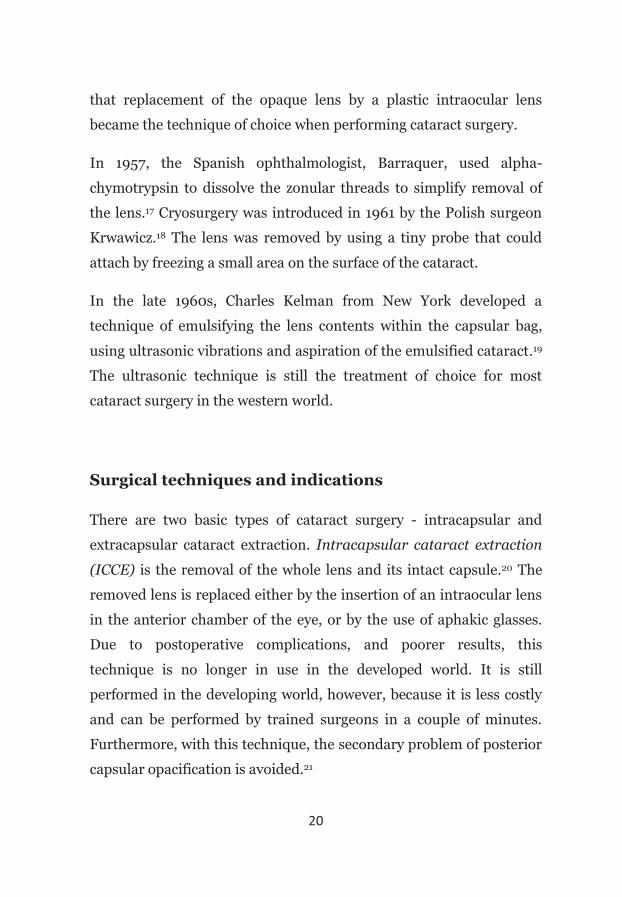
There are two basic types of cataract surgery - intracapsular and
extracapsular cataract extraction. Intracapsular cataract extraction
(ICCE) is the removal of the whole lens and its intact capsule.20 The
removed lens is replaced either by the insertion of an intraocular lens
in the anterior chamber of the eye, or by the use of aphakic glasses.
Due to postoperative complications, and poorer results, this
technique is no longer in use in the developed world. It is still
performed in the developing world, however, because it is less costly
and can be performed by trained surgeons in a couple of minutes.
Furthermore, with this technique, the secondary problem of posterior
capsular opacification is avoided.21
21
Extracapsular cataract extraction (ECCE) was introduced in the
early 1980s. The posterior lens capsule is retained in the eye, and the
lens contents are removed through a relatively large incision (9mm).
A posterior chamber lens can then be placed in the capsular bag.22,23
The modern extracapsular cataract extraction technique, use
phacoemulsification, in which ultrasonic energy breaks the nucleus
down into small pieces that can be aspirated. This can be done
through a small incision of about 2mm. The advantages with these
small incisions are faster visual rehabilitation and low induced
astigmatism. On the other hand, it requires an expensive
phacoemulsification machine, and trained surgeons.24
In Sweden, during the 1990s, an increasing proportion of cataract
surgery was performed using phacoemulsification. When the study
this thesis is based on started in 1997, 89% of all cataract surgery was
performed by phacoemulsification.25
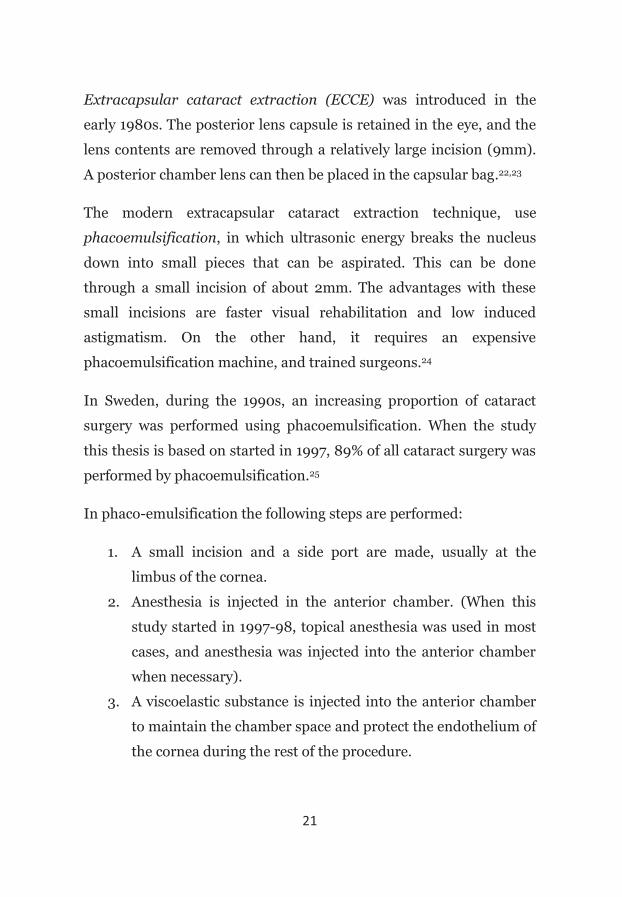
In phaco-emulsification the following steps are performed:
1. A small incision and a side port are made, usually at the
limbus of the cornea.
2. Anesthesia is injected in the anterior chamber. (When this
study started in 1997-98, topical anesthesia was used in most
cases, and anesthesia was injected into the anterior chamber
when necessary).
3. A viscoelastic substance is injected into the anterior chamber
to maintain the chamber space and protect the endothelium of
the cornea during the rest of the procedure.
22
4. A round shaped tear is made in the central part of the anterior
capsule of the lens. This allows access to the contents of the
lens.
5. Hydrodissection of the lens by fluid in order to separate the
lens from the lens capsule, and the lens nucleus from the
cortical layer.
6. The lens is removed by the phacoemulsification handpiece.
7. Once the capsule bag is empty, further viscoelastic substance
is injected, to maintain the space while the foldable
replacement lens implant is positioned into the capsular bag
(in-the-bag IOL implantation).
8. Injection of an antibiotic substance into the anterior chamber
to reduce the risk of endophthalmitis.
Figure 6. Phacoemulsification.
(Reproduced with permission from Alcon).
23
Indications for cataract surgery
In the past, when cataract surgery was performed by removing the
entire lens and leaving the patient aphakic (ICCE), it was necessary
that the cataract was dense enough to be able to remove it in a single
entire piece. As the surgical techniques have become safer and the
visual results have improved,26 “matureness” of the cataract is no
longer a consideration, and surgery is performed at a much earlier
stage when phacoemulsification is used. It is beneficial, in terms of
surgical complications, to remove the cataract before it becomes too
advanced.27
It is widely accepted, that visual acuity alone is an inadequate
measure of the need for cataract surgery.28 Visual acuity measures
only the smallest detail we can see, but in general, it does not
represent the quality of vision. Instead, any problem with self
assessed visual function is regarded as the single most important
variable when cataract surgery is recommended.29
There is no distinct rule regarding when to perform cataract
extraction. The indication varies, depending on the patients’ age and
visual functional demands.21 At present, the basic indication for
cataract surgery is a significant cataract, which reduces visual
function, making activities of daily living more difficult. Surgery
should be considered when the benefits from removal of symptoms
outweigh the small risks caused by modern surgery.2

24
Epidemiology and public demands
Cataract remains the leading cause of blindness globally, except in the
most developed countries.30 The World Health Organization (WHO),
estimated that in 2002, about 45 million people worldwide were
blind, half of them because of cataract.1,31 Due to the changing
demographic structure of several populations, with increasing
proportion of elderly in society,32-34 and longer life expectancy also in
the developing world, the number of people blind from cataract is
expected to rise. WHO projections indicate that, in 2020, as many as
40 million people will be blind because of cataract.35,36
The prevalence of cataract has been investigated in several
epidemiological studies. One of the most cited is the Framingham eye
study, in which 2675 of the inhabitants in the town Framingham,
Massachusetts, USA, were investigated for glaucoma, diabetic
retinopathy, age-related macular degeneration, and cataract. Lens
opacities were found in 80% of those over the age of 75, and in 46%,
there was a decrease in vision to 20/30 or worse as well.37
In the Beaver Dam Study from 1988-90, Klein et al. examined 4926
participants with slit lamp and retro-illumination lens photographs to
estimate the presence of cataract.38 The prevalence of cataract
formation in combination with a decrease in vision to 20/30 or worse
was found in 25% of women and in 13% of men older than 75 years.
In a Swedish cross-sectional population-based study from 2001, 5000
inhabitants between 70-84 years of age were examined. When using a
definition of cataract based on morphologic changes only, regardless
of the visual acuity level, the prevalence of cataract was 24% for
25
women and 14% for men in the entire cohort.39 If any previous
cataract surgery was included, the total prevalence increased to 42%
for women, and 27% for men. The difference between men and
women was significant in all age groups, except for the youngest (70-
74). Also, the VA level was lower in women than in men.
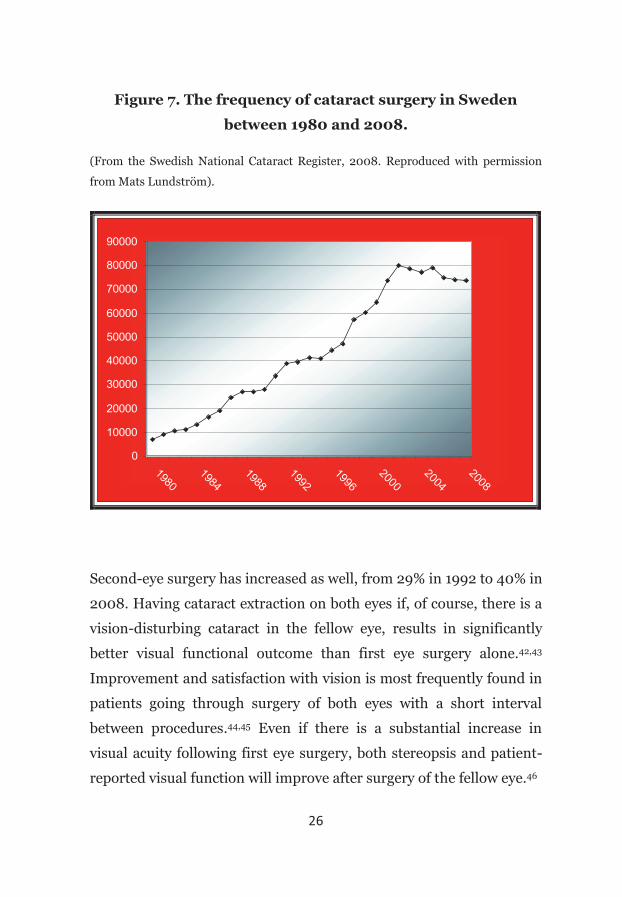
The modern life-style with pronounced need for excellent vision, has
increased the demand for cataract surgery.40 In combination with the
improved postoperative surgical results, as well as the increased life
expectancy, the number of cataract extractions performed has risen
dramatically over the last thirty years. In 1980, about 7000 cataract
extractions were performed in Sweden. In 2003, this figure had
increased to just above 80000, making up to more than a 10-fold
increase. In the last few years, the rate of surgery has decreased, but
still there were almost 74000 eyes operated on in 2008.41 In the
admitting area of the present study, this corresponds to a surgical rate
of 7.8 per 1000 inhabitants, compared with 5.2 per 1000 inhabitants
when this study started in 1997. The increase in frequency of cataract
surgery is equal for both sexes and all age groups.
26
Figure 7. The frequency of cataract surgery in Sweden
between 1980 and 2008.
(From the Swedish National Cataract Register, 2008. Reproduced with permission
from Mats Lundström).
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
19801984
19881992
19962000
20042008
Second-eye surgery has increased as well, from 29% in 1992 to 40% in
2008. Having cataract extraction on both eyes if, of course, there is a
vision-disturbing cataract in the fellow eye, results in significantly
better visual functional outcome than first eye surgery alone.42,43
Improvement and satisfaction with vision is most frequently found in
patients going through surgery of both eyes with a short interval
between procedures.44,45 Even if there is a substantial increase in
visual acuity following first eye surgery, both stereopsis and patient-
reported visual function will improve after surgery of the fellow eye.46

27
It has previously been well documented that the cataract surgery rate
in Sweden is significantly higher in women than in men,47 except for
the younger age groups (<65), and for the very old (>90).48 In 2008,
61% of all the patients having cataract surgery were women. This is in
part explained by women living longer than men and being more
numerous in the older ages. Age-related lens opacities are also more
common in women than in men, regardless of age.49
Outcome studies
With increasing cataract surgery volumes in most parts of the world,
the importance of well conducted follow-ups have been emphasized.50
There are several studies on cataract surgery outcome, presenting
complications and the benefits concerning final VA.51,52
However, traditional clinical measures of vision, such as Snellen
visual acuity and decimal acuity, are imperfect when calculating the
need for or outcome of cataract surgery. 53-55 The most important
outcome measure is the patients’ self assessed visual function.56
Different generic and disease-specific health status instruments have
been developed to evaluate patients’ outcomes. A generic health
status questionnaire intends to describe the quality of life, defined by
WHO as “an individuals’ perception of their position in life in the
context of the culture and value systems in which they live, and in
relation to their goals, expectations, standards and concerns”.57 Some
of the more frequently used generic measures in medical outcome
studies are the MOSSF-36 (Medical Outcome Study Short Form-

28
36),58 the SIP (sickness impact profile),59 and the HRQoL (Health
Related Quality of Life).60
When presenting the outcome after cataract surgery, disease-specific
measures are more adequate in describing visual functional change.61
When this study started, in 1997, the VF-14 questionnaire had been
introduced a few years earlier.62 It was found to be a reliable and valid
measure of functional impairment caused by cataract. Also, it
provided more information than visual acuity or general health status
measures could reveal.62,63 After the VF-14 questionnaire was
introduced in 1994, several other well-validated instruments, such as
the Catquest, developed for use in the Swedish National Cataract
Register, have been presented.64 Other disease-specific instruments
that measure cataract related quality of vision are the ADVS
(Activities of Daily Vision Scale),65 and the 12-item Cataract TyPE
Spec.66 Today, there are also several quality of life questionnaires
measuring the contentment of patients suffering from other ocular
diseases such as glaucoma,67-68 and optic neuritis.69
In terms of health economics, cataract surgery is described as a
relatively cost-effective intervention.70-72 A cost-benefit analysis
compares the costs of a specific surgery, against the money saved, e.g.
what does it cost if someone can not work because of vision-impaired
cataract or what is the cost for society if an elderly person needs home
assistance because of hip arthritis.73 However, in these analyses
quality of life issues are ignored.
The cost-effectiveness analysis describes the quality of life issues as
well.73 DALY (disability-adjusted life years), or vision-years in
ophthalmology, intends to specify the life-years gained or saved by a

29
specific intervention. A cost-utility analysis takes all these matters
into account, and therefore enables a comparison between different
medical interventions that include surgery, i.e. epileptic surgery, hip
arthroplasty, knee arthroplasty, carpal tunnel surgery, and
defibrillator implantation.74The cost-utility of cataract surgery can
vary significantly depending on the duration of benefit, the life
expectancy of the patient, and the impairment of visual acuity at the
time of surgery. In a meta-analysis, including 12000 cataract surgery
eyes from different countries, cataract surgery proved to be
comparable in terms of cost-effectiveness to hip arthroplasty, and in
general more cost-effective that both knee arthroplasty, and
defibrillator implantation.74 One of the aims of the present study was
to evaluate and describe the duration of the improvement of visual
function after a cataract extraction.
Gender in medicine
During the past decades, there have been several reports of gender
biases in clinical research, and to prevent this, a gender perspective
has been requested.75 Gender is a wider concept than sex, and
includes the social, cultural, and symbolic conception of men and
women in society. There are two main types of models described in
the scientific literature, explaining differences in health between men
and women; the biological/generic models, which emphasize sex
differences in biological makeup in terms of genes, hormones and
physiology, and the socio-cultural models, which focus on gender
30
differences in health-related behavior and on life circumstances such
as work and family.76
Previous studies in ophthalmological research have reported sex-
related differences in incidence and prevalence of several disorders,
such as age-related macular degeneration,77 keratoconus,78 and dry
eyes.79 It is also well known that cataract extractions are performed
more frequently in women compared to men, and women is the
predominant group among patients undergoing cataract surgery by a
2:1 ratio.80 This difference remains when adjusting for the fact that
women live longer. The predominance of women seems to be more
pronounced in the higher age groups.81
Several explanations have been suggested. One reason could be a
higher prevalence of cataract in women.82 Another reason could be
that men tend to accept a larger visual loss before they request
surgery. Diverging results have been reported concerning gender-
related differences in visual acuity before cataract surgery. Ninn-
Pedersen et al 82 as well as Morgan et al 83 reported that men tend to
accept a larger visual loss than women before they request surgery.
This is in conflict with the results of Carlsson & Sjöstrand47 who
reported no difference between sexes in pre-operative visual acuity in
the better-seeing eye. They explained the higher utilization of cataract
surgery in women simply with a higher prevalence of cataract.
Another study presenting data on differences in pre-operative visual
acuity reported women with a moderately impaired visual acuity in
the best eye to have cataract surgery to a much higher degree than
men with the same pre-operative visual acuity loss.48 The question
was raised whether women and men request cataract surgery at

31
different stages of visual impairment. Regarding the subjective visual
function, Mönestam et al reported in 1998, that women experience
more functional impairment than men at the same visual acuity
level.84
Lundström et al,48 discussed three possible hypotheses responsible
for the higher utilization of cataract surgery in women:
1. The prevalence of cataract is higher in women compared to
men in certain age groups.
2. Women request cataract surgery more often than men because
their everyday life is more disturbed by a cataract.
3. The need for cataract surgery is equal in women and men but
women are favored by the health care system.
A plausible explanation to the third hypothesis could be that women,
compared with men, because of a higher frequency of other medical
problems, more often have contact with the health care system. They
have more opportunities to mention visual problems, and ask for a
referral to an ophthalmologist. Another explanation could be that
maybe men are less verbal than women and less prone to express
visual functional problems.48
The role of hormones such as estrogen in cataract formation is
contradictory.85,86 Whether the excess risk of women developing
cataract is related to different hormonal effects or differences in
metabolic or noxious effects due to life style is not known. In their
report from the Beaver Dam Eye Study, Klein et al. presented results
showing that current use of postmenopausal estrogens was associated
32
with a reduced risk for nuclear sclerosis.87 Older age at menopause
was associated with a decreased risk for cortical cataracts. This
suggests that estrogen exposure has a modest protective effect on the
lens. Similarly, in the Framingham Eye Study, a longer duration of
postmenopausal estrogen therapy was inversely associated with
nuclear cataract, but no association was found for cortical cataract.88
On the other hand, the Blue Mountain Eye study from Australia
reported no association with age at menopause, number of children,
or use of the oral contraceptive pill.89 However, low age at menarche
was associated with increased prevalence of all types of cataract.
In a recently published Swedish cohort study investigating risk factors
for cataract in women, the results indicate an increased risk for the
development of lens opacities in postmenopausal women using
hormone replacement therapy for long period of time.90
Awareness of the differences between men and women in prevalence
of cataract is important in the management of patients seeking
medical care for vision-related problems.
Diabetic retinopathy, diabetes and cataract
Diabetes affects more than 6% of the overall population in developed
countries,91 and the prevalence is rising throughout the world.92
According to WHO projections, the number of people suffering from
the disease will be close to 370 million by 2030.92 With increasing
rates of diabetes over the past decades,93 complications like diabetic
retinopathy (DR) will probably become more common.
33
Diabetes is characterized by a persistently high blood glucose level,
either from low insulin production in the pancreas or from a
resistance to insulin in the body tissues. Eye complications from
diabetes include, for example, DR and cataract.94 Diabetic patients
develop cataracts more frequently than non-diabetic patients and at a
younger age.95
One of the most common risk factors for cataract in the developed
world is diabetes. There is a three- to fourfold increased prevalence of
cataract in diabetic patients under the age of 65 years, and a twofold
increased prevalence in diabetics over 65.96
Cataract in diabetics is significant for a number of reasons. It impairs
the recognition of sight-threatening DR and there is a risk that any
present DR can deteriorate. Particularly diabetic maculopathy can be
exacerbated by cataract surgery.97-100
Previous quidelines did not recommend cataract surgery in diabetic
patients until vision was severely deteriorated, due to the increased
risk for postoperative complications, e.g. inflammatory reactive
uveitis and progression of retinopathy. However, this belief is
outdated as modern cataract surgery using small incision
phacoemulsification is less disruptive than intracapsular and
extracapsular cataract extraction.101,102 Several studies have reported
fewer postoperative complications and generally more encouraging
result.103-105
The best time to perform cataract surgery in diabetics is simply when
the patient is symptomatic and before the view of the retinal fundus
becomes significantly impaired. Preferably this would be when there

34
is no DR present, as it has been shown that the severity of retinopathy
at the time of the cataract extraction is the most important predictor
of poor visual acuity.106 If any retinopathy is present it should be
optimally treated prior to surgery.107
There are several previous studies describing diabetic retinopathy
progression after cataract surgery. However, few reports concern
visual function, and in these studies only short-term data are
presented.97,99
Posterior capsular opacification (PCO)
Posterior capsular opacification (PCO) can be suspected if the visual
acuity declines and visual disturbances such as halos, impaired
contrast sensitivity, and monocular diplopia occur after cataract
surgery.108,109 Even if there is polishing of the anterior and posterior
capsule at the time of cataract surgery, some lens fibres are retained
in the lens capsule periphery.110 Slowly, over time, residual lens
epithelial cells can proliferate and migrate into the visual axis.111 The
capsule can become so hazy and cloudy it may seem as if the cataract
has returned (after-cataract). However, the cataract can never
reoccur, but a secondary membrane with light scattering migrating
cells may appear.
In clinical practice, PCO is evaluated through slit-lamp examination.
Different scientific methods have been developed for evaluating the
amount of PCO. The EPCO (Evaluation of Posterior Capsule
Opacification) image analysis system uses retro-illumination color

35
photographs to score PCO. The individual PCO score is calculated by
multiplying the density of the opacification, graded from 0 to 4
(0=none, 1=minimal 2=mild, 3=moderate, 4=severe), by the area of
the posterior optic involved.112,113 Another method for measurement of
PCO is the Anterior Eye Segment Analysis System (EAS-1000; Nidek,
Japan) using the Scheimpflug photography system. The central 3-mm
portion of the posterior capsule is quantitated by means of area
densitometry. Scheimpflug slit images are taken at 4 different
meridians after dilatation of the pupil and analysed with a computer
program.114,115
When the PCO becomes clinically significant, in terms of reduced
vision, the patient may demand a Nd:YAG laser capsulotomy. The
initials are an acronym for neodymium, yttrium, aluminum, and
garnet, which are the materials components utilized to allow the laser
to function properly, as a knife, and open the membrane. The laser
procedure is fairly easy but can be associated with complications such
as cystoid macular edema,116,117 retinal attachment,118-120 intraocular
pressure elevation,117 and damage to the intraocular lens.121-124
The incidence of PCO can be influenced by:
patient-related factors (age, systemic or ocular diseases)
surgery-related factors (capsulorhexis size, cortical clean-up,
in-the-bag IOL fixation, anterior capsule over-lap)
IOL design related factors125-131
In pediatric cataract surgery, posterior capsular opacification
formation is a well-known complication, occuring in 40-100% of cases
36
if the posterior capsule is left intact.132-134To preserve a clear visual
axis, a primary posterior capsulorhexis can be performed.135 After the
cataractous lens is removed, viscoelastic is placed in the capsular bag
to stabilize it. With the capsulorhexis forceps, a round opening of the
posterior capsule can then be completed.136
To prevent PCO formation also in adults, some surgeons perform a
posterior optic buttonholing (POBH) through a primary posterior
capsulohexis.137 In this procedure, a standard anterior capsulorhexis
and phacoemulsification is completed. A posterior capsulorhexis is
then performed and the lens is implanted with the haptics in the
capsular bag and the optic behind the posterior capsule. This method
is sometimes called the “sandwich method”, since the posterior
capsule blocks optic contact and thus fibrosis of the anterior capsule.
Posterior optic buttonholing prevents after-cataract independent of
optic edge design. Favorable results have been published,137 however,
the surgical technique is demanding. Longer follow-up to determine
whether this method is an alternative to standard in-the-bag IOL
implantation is not yet available.
Remnants of the lens epithelium increase the risk for PCO. Therefore,
it is of importance to perform a thorough cortical clean-up at surgery.
Furthermore, the size of the capsulorhexis should be slightly smaller
than the optic to enable the anterior capsule rim to cover the IOL.
PCO is one of the major problems following cataract extraction, and
some studies indicate a higher rate after cataract surgery in
diabetics.138,139 Other studies, on the contrary, have failed to show any
differences in the PCO rates between diabetics and non-
diabetics.112,140 It has been proposed that inflammatory mediators
37
resulting from the breakdown of blood-aqueous barrier after surgery
may contribute to the development of PCO.141 In all patients, it is
important to maintain visual acuity after cataract surgery. In
diabetics, it is also valuable to keep the posterior capsule clear to
make retinopathy screening, retinal photocoagulation, and any future
retinal surgery possible.
Following cataract extraction, implantation of an IOL decreases the
incidence of PCO.142 In order to reduce the risk for PCO as well as
retinal detachment, IOL implantation in highly myopic patients
should be performed after cataract extraction, even though it might
not be necessary for refractive reasons.143
In the 1980s, when IOLs were first implanted, the material of choice
was PMMA (poly methyl metacrylate). The frequency of posterior
capsulotomies after implanting these lenses was as high as 50% in
several studies.144-147 More modern IOL materials, such as the silicone
lenses, and the hydrophobic acrylate IOLs, have been reported to
induce a lower rate of PCO.148-151
In recent years, IOL-design has undergone significant changes and
there has been a general shift toward acrylic IOL materials, as well as
sharp posterior edges for IOL optics.64,152 The square edge aims to
inhibit the lens epithelial cell ingrowth between the capsule and the
IOL surface.153 Comparative studies have established that the
hydrophobic Acrysof® IOL (Alcon Inc) have lower rates of PCO and
Nd:YAG treatment compared with silicone and PMMA lenses.154-157
When these comparative studies started the only square-edged lens
on the market was the Acrysof® IOL.158 This lens remained the only
square-edged IOL until 2001, when the CeeOn Edge®911A
38
(Pharmacia and Upjohn) and the Sensar®AR40(AMO) were
introduced.
However, in a recent retrospective study by Vock et al.,152 the
protective effect of the square edge lenses has been questioned. In
their study, 143 eyes implanted with either MA60BM Acrysof® or a
silicone lens (SI-30NB or SI-40, both Allergan) were examined for
presence of PCO using digital images. The silicone IOLs had less after
cataract ten years after surgery, 42% of the patients with Acrysof
acrylic lenses and 18% of patients with silicone lenses implanted had
been treated with Nd:YAG laser capsulotomy.
Even though recent improvements in intraocular lens technologies
have reduced vision disturbing PCO, it is still a common complication
after cataract extractions.137 Furthermore, increasing patient
expectation for perfect quality of vision following cataract surgery has
led to an increased demand for posterior capsulotomies even for
minor PCO.158
39
AIMS OF THE STUDY
The overall purpose of this thesis was to longitudinally study different
aspects of cataract surgery on a long-term basis.
The specific aims were:
To analyze the subjective and objective visual functional
results at the time of surgery, and compare with the long-term
outcomes.
To determine if there are any gender-related differences in
long-term cataract surgery outcome.
To analyze the long-term visual functional results after
cataract surgery in patients with diabetes, and compare the
results with the outcomes of non-diabetics.
To investigate the long-term results in younger cataract
surgery patients, and to analyze the incidence of posterior
capsular opacification and treatment with Nd:YAG laser.
ETHICS
The study was approved by the local Ethics Committee at Umeå
University. Informed consent was obtained from all patients at
surgery and at each follow-up.

40
PATIENTS AND METHODS
Study design and study population
The papers in this thesis are based on prospective data from a
population-based cohort of all adult patients having surgery for senile
and presenile cataract at one clinic during a one-year period. Between
June 1st, 1997 and May 31st, 1998, all patients who underwent
cataract surgery with IOL implantation at Norrlands University
Hospital in Umeå, Sweden, were prospectively registered. The
admitting area is situated in the northern part of Sweden and has a
population of about 182 000 people with about 4 inhabitants per
square kilometer. Our population represents 2% of the inhabitants in
Sweden.
At baseline, all cataract surgery in the region was performed at the
University Clinic. As a result of the Swedish Health Care Policy at that
time, there were no private surgery alternatives, and patients very
seldom crossed county borders to obtain treatment during the study
period.
Inclusion and exclusion criteria
During the one-year period, 928 cataract surgeries were performed.
Excluded from the study were 38 patients who had cataract
extractions for reasons other than restoring vision or combined with
other types of surgery, for example posterior segment procedures,
glaucoma filtering surgery, or corneal transplants. Also excluded was
41
one patient who was scheduled for cataract surgery without IOL
implantation. Patients with dementia or whose mental status was too
poor to enable them to participate with the questionnaire, were also
excluded (n=17). At the postoperative follow-up, 4-8 weeks after
surgery, 13 patients did not show up, and 17 were deceased. Five
patients denied to participate already at the time of surgery. Thus, the
base cohort included 837 senile and presenile cataract cases. Twenty-
seven patients (3%) had surgery on both eyes during the time-period
studied, resulting in 810 cataract surgery patients finally included in
the study.
Examinations
The patients were examined at the following occasions:
A few weeks before cataract surgery.
Between 4-8 weeks after surgery.
Five years after surgery.
Ten years after surgery.
Data collected before and shortly after surgery
All patients were examined a few weeks before surgery. Included in
the examination were presenting visual acuity (PVA), best corrected

42
visual acuity (BCVA), tonometry, keratometric readings, and a slit
lamp examination of both eyes.
PVA at distance, i.e. the visual acuity with the habitual correction
glasses worn by the patient, or if the patient did not use glasses,
without spectacles, was tested using a Monoyer-Granström letter
chart. In the same way the BCVA, i.e. the visual acuity with the
additional correction needed to obtain the best possible visual acuity,
was recorded. It has been pointed out earlier that the patients’
subjective visual function is more dependent on the visual acuity in
the better eye.62 Since the better eye is seldom the operated eye, both
variables were included. Furthermore, this also explains why some of
the patients had a Snellen VA of 20/20 (=1.o decimal VA or logMAR
0.0) or better on their better seeing eye before surgery.
Data concerning age, sex, presence of pseudo-exfoliations, surgery on
right or left eye, and of first and second eye surgery was recorded for
each patient.
Presence of amblyopia, or any history of past ocular diseases such as,
retinal detachment or central vein occlusion was recorded. Present
ocular co-morbidity, like glaucoma, diabetic retinopathy, or age-
related macular degeneration was noted.
Between four and eight weeks after the surgery the first follow-up
examination was performed. The same eye examination as before
surgery was conducted. Also, data on the surgery, the type of IOL, any
complications such as zonular rupture and/or vitreous loss was
added.
43
The questionnaire
The questionnaire used was a Swedish translation of the Visual
Function-14 (VF-14) questionnaire. This is a well-validated
instrument to assess visual function in cataract patients. It was
developed in the United States by Steinberg et al.,62 and has been
accepted for use in various translated versions in Europe.159 Changes
in visual function can be assessed by analyzing questionnaire
responses before surgery and compare with after surgery. The
following set of functional activities was included in the questions
from which the VF-14 is derived:
1. Reading small print, such as labels on medicine bottles, a telephone book, or food labels;
2. Reading a newspaper or book;
3. Reading a large-print book or newspaper or the numbers on a telephone;
4. Recognizing people when they are close to you;
5. Seeing steps, stairs, or curbs;
6. Reading traffic, street, or store signs;
7. Doing fine handwork such as sewing, knitting, crocheting, or carpentry;
8. Writing checks or filling out forms;
9. Playing games such as bingo, dominos, card games, or mahjong;
10. Taking part in sports such as bowling, handball, tennis, or golf;
11. Cooking;
44
12. Watching television;
13. Daytime driving;
14. Nighttime driving;
For each of the 14 items, patients are asked whether, even with
glasses, they have any difficulty in doing the activity. Allowed
responses are yes, no, or do not do the activity for reasons unrelated
to vision. If respondents answer positively, that they have problems,
they are asked to rate whether the amount of difficulty they currently
have with the activity is “a little”, “a moderate amount”, or “a great
deal” or whether they are “unable to do” the activity because of their
vision. The exact wording of each of the 14 items and the associated
response options are provided in the appendix.
According to the instructions outlined by Steinberg et al.,62 each
activity is scored from 0 to 4 corresponding to whether the
respondent is “unable” to do the activity, or “can with great difficulty”,
“can with moderate difficulty”, “can with little difficulty”, or “can with
no difficulty” do the activity. All scored items are averaged and
multiplied by 25. The final VF-14 score can range from 0 (unable to
do all applicable activities because of vision) to 100 (able to do all
applicable activities without difficulty). An item is not included in
scoring if patients do not do the activity for a reason other than their
vision (e.g., individuals who had never cooked for themselves or had
never taken part in sports), and no minimum number of applicable
items is therefore required.
A few days before surgery, the questionnaire was sent by mail to all
patients and brought to the clinic at the day of surgery. The nurses

45
involved were trained to check that the questions had been
understood and completely answered. About one month after the
patients had received their prescription glasses, they were by mail
again asked to answer the same questionnaire. The mean time from
date of surgery to return of the second questionnaire was 3.7 (± 1.4)
months (SD).
Five and ten years after surgery, a similar questionnaire was mailed to
all surviving patients who were able to participate. Those who also
had the eye examination delivered the questionnaire to the clinic, and
those who were not examined mailed the questionnaire to the
research team.
Data collected 5 and 10 years after surgery
Five and ten years after surgery, the patients still alive were offered an
eye examination and once more asked to answer the questionnaire.
After the studied started in 1997-98, the patients’ hospital records
have been computerized, which makes it fairly easy to locate patients.
Phone-calls were made to all patients alive, scheduling them for the
examination. Some patients with obvious dementia were at that time
excluded from the study. Since our region is sparsely populated, with
long-distances to travel, some of the patients were offered the
examination at their nearest health care center. In this way, the
participation rate at five years was as high as 90% of the survivors for
the questionnaire and 79% for the examination. At the ten-year
follow-up, 85% answered the questionnaire, and 73% were examined.

46
The major reason for not participating with the eye examination was
either illness/old age, or reluctance to travelling.
At the examination before surgery and 4-8 weeks postoperatively,
visual acuity was measured with the Monoyer-Granström letter chart,
which expresses acuity measures in decimals.
Visual acuity measures the ability to detect small details at a
distance.The results from visual acuity testing indicate the foveal
function, the most sensitive part of the retina. The size of the retinal
image depends upon the size of the object and its distance from the
eye. The further away an object is located, the smaller the retinal
image. The angle that the image subtends at the nodal point of the eye
is the visual angle. By combining the two factors of size and distance,
it is possible to determine the minimum visual angle, that is, the
smallest retinal image that can be discriminated. The so-called
normal eye can identify an entire letter subtending an angle of 5
minutes of arc and any component of a letter subtending 1 minut of
arc. Many persons, however, can resolve letters subtending a smaller
visual angle.
In many English speaking countries, visual acuity is expressed in
Snellen fractions. The fractions, 20/20, 20/30 etc., are measures of
visual acuity at a specified distance. The first number represents the
test distance, 20 feet. The second number represents the distance that
the average eye can see the letters on a certain line of the eye chart. A
visual acuity of 20/20 is considered a normal acuity in healthy adults.
The quidelines for publications in ophthalmological journals often
recommend Snellen acuity charts. This is why some of the tables in
47
the papers included in this thesis, present visual acuity as Snellen
acuity.
At the five and ten year follow-ups, the same examination was
conducted but the early treatment diabetic retinopathy (ETDRS)
chart was used for testing VA.160 The ETDRS acuity test was
developed to improve the evaluation of the changes in vision
following panretinal photocoagulation in patients with diabetic
retinopathy. The advantage with this method is that it describes
changes in visual acuity more accurate.
When using a Snellen or a decimal chart, there are different numbers
of letters on each line, and also the individual lines are not equally
spaced. The inadequacies in the decimal acuity tests, such as the
Monoyer Granström letter chart and the Snellen acuity chart, makes
it impossible to properly evaluate the acuity data and to compare data
from study to study.
The EDTRS test has a specific design including:
The same number of letters per row (5 letters)
Equal spacing of the rows on a log scale (the rows are
separated by 0.1 log unit).
Equal spacing of the letters on a log scale.
Individual rows balanced for letter difficulty.
When the ETDRS charts were presented by Bailey & Lovie in 1976,161
and introduced in the Early Treatment Diabetic Retinopathy Study by
Ferris et al. in 1982,162 it was a time-consuming test not always well
48
accepted by the patients. Therefore, Camparini et al presented, in
2001, the ETDRS-Fast, which is the method we used five and ten
years after surgery.160 In the statistical methods section, the
scientifically accepted method of conversion from the decimal visual
acuity results to the logarithmic ETDRS results is described. The
ETDRS acuity testing is expressed as logMAR acuity (the logarithm of
the minimal angle of resolution). A conversion table, presenting VA
with the Monoyer Granström letter chart, the Snellen acuity chart,
and the EDTRS chart, is presented in the appendix (p. 104).
Figure 8.
The Monoyer-Granström letter-chart and the ETDRS chart.
Five and ten years after surgery, the participants had the same eye
examination as before, and shortly after surgery. At the follow-up
examinations there was also a subjective assessment of any present
PCO, and a testing of low-contrast VA. Monocular low-contrast VA
was tested using Sloan letter logarithmic translucent contrast charts

49
(10% and 2.5%) (Precision Vision®) at a distance of 4 m. Participants
who failed to read the largest letters at 4 m were tested at 1 m.
Contrast sensitivity measures the ability to see details at low contrast
levels, e.g. grey of various shades on a white background. Visual
information at low contrast levels is important in several situations,
e.g. recognizing people and relate to facial expressions, in orientation
and mobility where we need to see curbs, stairs and shadows, and in
near vision tasks like writing. In traffic, the demanding situations are
at low contrast levels, for example, seeing in dusk, rain, fog, snow fall,
and at night. Measurement of contrast sensitivity can help us to better
understand the complaints of a person whose visual acuity at high
contrast (black letters on white) has not changed but whose vision has
decreased at low contrast levels. Cataract, age-related macular
degeneration, and PCO - among other ocular diseases - cause reduced
contrast acuity.
50
Subgroups
Males/Females (Paper II).
In the baseline cohort, 283 (35%) of the total 810 patients were men,
and 527 (65%) were women. Among these 810 patients, 237 (68 men
and 169 women) had undergone cataract surgery on their first eye
before the study started.
Diabetics (Paper III).
When the study started in 1997-98, 106 of the 810 patients were
diabetics treated with insulin or oral anti-hyperglucaemic agents.
Patients with dietary treatment only, were not included in the diabetic
group.
The Modified Airlie House Classification was used when determining
the level of retinopathy (Diabetic Retinopathy Study 1981163; Early
Treatment Diabetic Retinopathy Study Group (ETDRS), Report no.
12:1991).164 The four levels of DR were as follows, I:no DR, II:mild
non-proliferative DR (NPDR), III:moderate-severe NPDR, and
IV:proliferative DR (PDR). The degree of retinopathy was established
at the slip-lamp examination.
Younger cataract surgery patients (Paper IV).
At the beginning of the study, 116 of the 810 patients in the cohort
were between 30 and 64 years of age. At the ten-year follow-up, all
the surviving participants were examined with slit-lamp examination
for detection of any PCO.
51
Statistical methods
To be able to compare the visual acuity results using the Monoyer-
Granström letter-chart with the results from the ETDRS-charts, and
to evaluate changes of VA in an appropriate manner, the values were
converted into a log scale using the method outlined by Holladay &
Prager.165 In this method, the proper manner for computing the
average visual acuity from any notation is to convert the value to the
logMAR equivalent and then take the average of the logMAR values.
The easiest way to compute the logMAR value is to convert to decimal
notation and then take the negative of the logarithm, e.g., 20/20=1
and the log of 1 is 0, and 20/200=0.10 and the negative of the log
is+1.0. The formulas for going from decimal to logMAR and back are:
LogMAR=-Log (Decimal Acuity)
Decimal acuity=antilog (-LogMAR)=10-LogMAR
When using the ETDRS-chart, VA was scored as the total number of
letters read correctly, and expressed as logarithm of the minimum
angle of resolution (logMAR) units. Patients with failure to read any
letters were tested using counting fingers (CF), hand movements
(HM), and light perception (LP). For VA less than CF 0.5 m the
following arbitrary logMAR values were used; CF in front of the
eye=logMAR 2.2, HM=logMAR 2.5, and no LP=logMAR 3, in a
similar manner as previously described.62,166
To define changes of VA, the logMAR acuity after surgery was
subtracted from the logMAR acuity before surgery. For example, VA
before surgery =logMAR0.7 (decimal acuity 0.2) and after surgery
52
=logMAR0.1 (decimal acuity 0.8) indicates an improvement in VA of
0.6 logMAR units (0.7 – 0.1). Consequently, a negative value denotes
worse VA after surgery. A decline in VA was defined as an increase in
logMAR of 0.1 or more, compared with the VA recorded after surgery,
for each eye, respectively.
Age-differences between groups were calculated by independent
sample t-tests. Multiple linear regression analyses were used to
determine the associations before surgery, postoperatively, and 5
years after surgery, between VF-total score and gender, controlling for
age and BCVA of the better eye. Age and BCVA were modelled as
continuous variables.
Since the VF-14 scores, and the VA-data were highly skewed, non-
parametric Mann-Whitney U tests, and Kruskal-Wallis tests were
used when analyzing the variables. Yates’ corrected chi-square tests
were used to analyse the cathegoric variables in two-by-two tables,
when appropriate.
The change in VA and VF-14 total score from postoperatively to 10
years after surgery, was calculated by paired Wilcoxon signed ranks
test. Changes in trend were analyzed by chi-square tests for trend,
and by linear by linear association.
Univariate ANOVA controlling for age was used to associate change in
VF-total score and change in BCVA of the better eye.
A life-table analysis using Cox proportional hazard model was used to
determine the risk for having treatment with Nd:YAG laser during the
ten-year follow-up. The cumulative incidence described in this model

53
takes into account both length of survival and length of follow-up, and
therefore more accurately describes the over-all risk.
The SPSS statistical software ver. 16.0 (Statistical Package for the
Social Sciences for MS Windows, SPSS Inc., Chicago, IL), and
Microsoft Office Excel software were used for statistical calculations.
All statistical tests were two-sided and P<0.05 was considered
statistically significant.
54
RESULTS
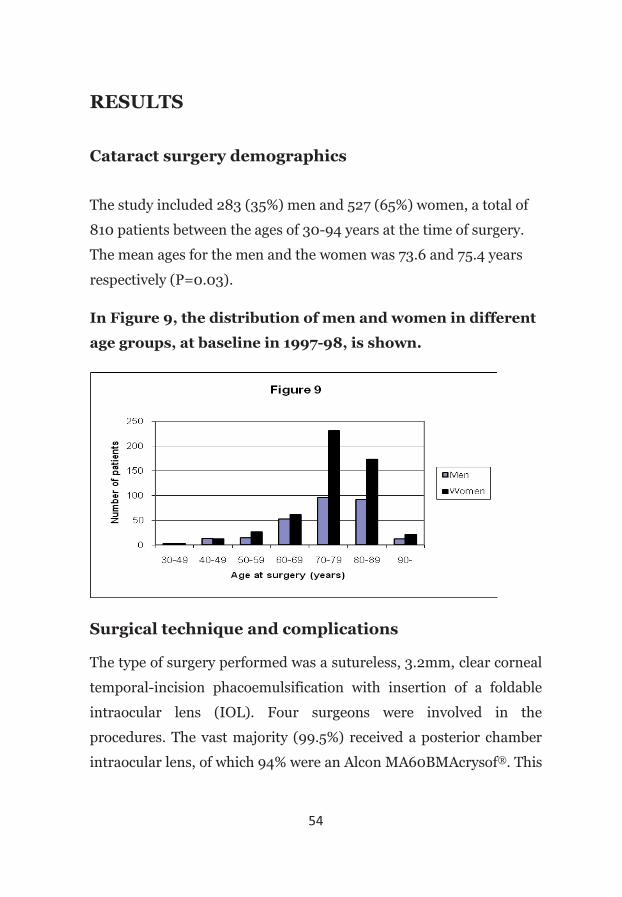
Cataract surgery demographics
The study included 283 (35%) men and 527 (65%) women, a total of
810 patients between the ages of 30-94 years at the time of surgery.
The mean ages for the men and the women was 73.6 and 75.4 years
respectively (P=0.03).
In Figure 9, the distribution of men and women in different
age groups, at baseline in 1997-98, is shown.
Surgical technique and complications
The type of surgery performed was a sutureless, 3.2mm, clear corneal
temporal-incision phacoemulsification with insertion of a foldable
intraocular lens (IOL). Four surgeons were involved in the
procedures. The vast majority (99.5%) received a posterior chamber
intraocular lens, of which 94% were an Alcon MA60BMAcrysof®. This
55
lens is a 3-piece IOL, with a 6 mm diameter acrylic optic, and PMMA
haptics, with a total length of 13.0 mm.
The complication rates of posterior capsule and/or zonular rupture
and vitreous loss were, in all 810 cases 5.7% and 2.7%, respectively.
Demographics 5 and 10 years after surgery
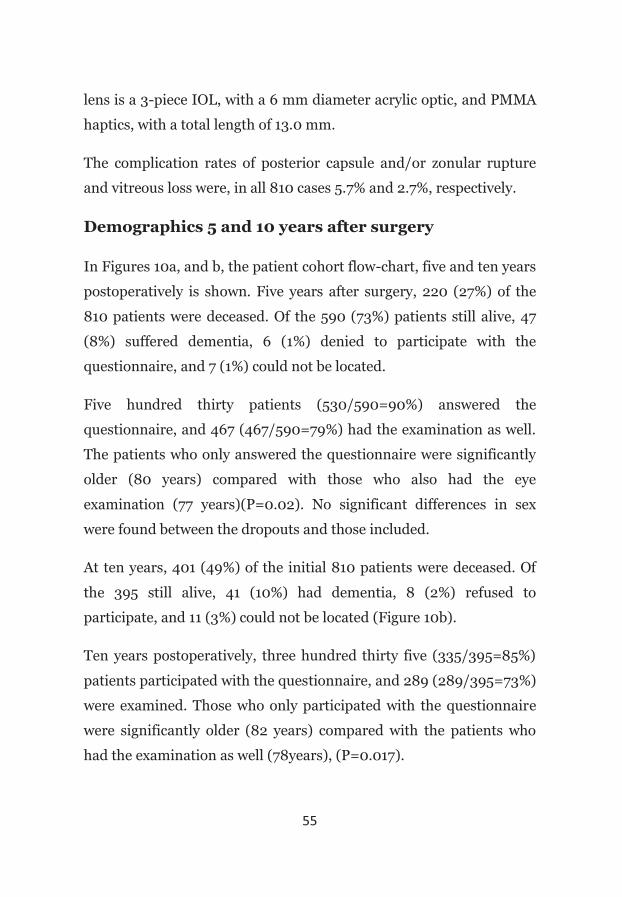
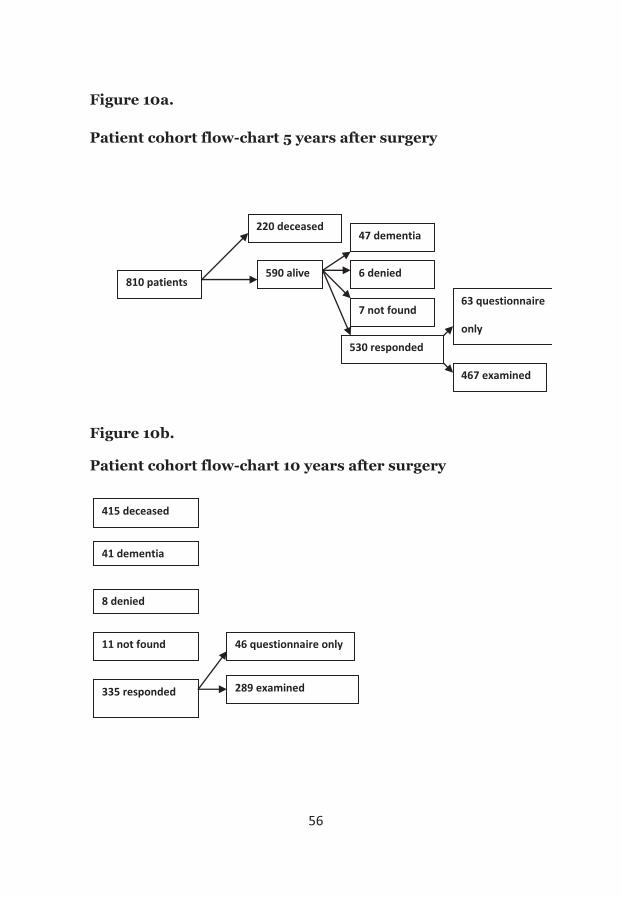
In Figures 10a, and b, the patient cohort flow-chart, five and ten years
postoperatively is shown. Five years after surgery, 220 (27%) of the
810 patients were deceased. Of the 590 (73%) patients still alive, 47
(8%) suffered dementia, 6 (1%) denied to participate with the
questionnaire, and 7 (1%) could not be located.
Five hundred thirty patients (530/590=90%) answered the
questionnaire, and 467 (467/590=79%) had the examination as well.
The patients who only answered the questionnaire were significantly
older (80 years) compared with those who also had the eye
examination (77 years)(P=0.02). No significant differences in sex
were found between the dropouts and those included.
At ten years, 401 (49%) of the initial 810 patients were deceased. Of
the 395 still alive, 41 (10%) had dementia, 8 (2%) refused to
participate, and 11 (3%) could not be located (Figure 10b).
Ten years postoperatively, three hundred thirty five (335/395=85%)
patients participated with the questionnaire, and 289 (289/395=73%)
were examined. Those who only participated with the questionnaire
were significantly older (82 years) compared with the patients who
had the examination as well (78years), (P=0.017).
56
Figure 10a.
Patient cohort flow-chart 5 years after surgery
Figure 10b.
Patient cohort flow-chart 10 years after surgery
810 patients
220 deceased
590 alive
47 dementia
6 denied
7 not found
530 responded
63 questionnaire
only
467 examined
8 denied
41 dementia
11 not found
335 responded
415 deceased
46 questionnaire only
289 examined
57
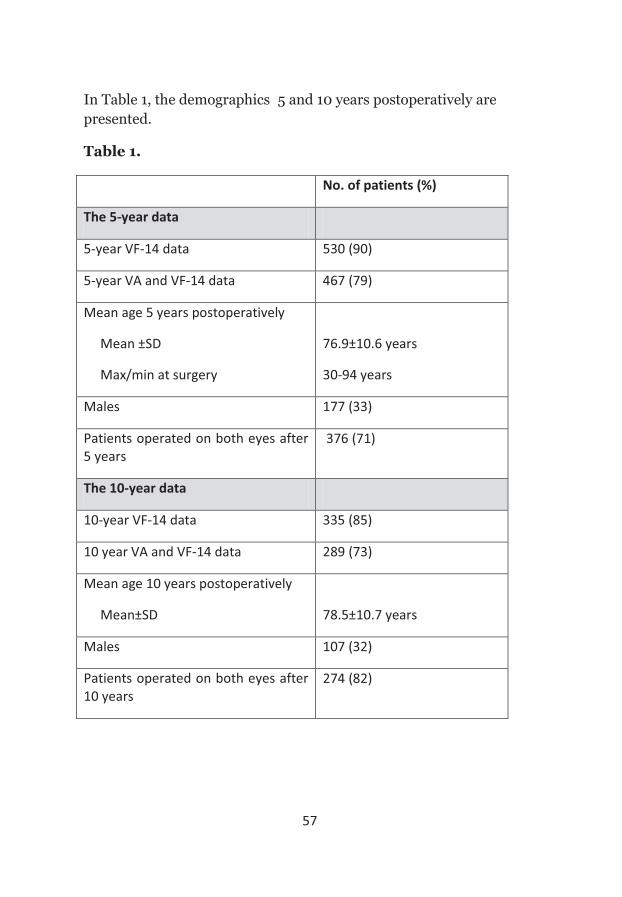
In Table 1, the demographics 5 and 10 years postoperatively are presented.
Table 1.
No. of patients (%)
The 5-year data
5-year VF-14 data 530 (90)
5-year VA and VF-14 data 467 (79)
Mean age 5 years postoperatively
Mean ±SD
Max/min at surgery
76.9±10.6 years
30-94 years
Males 177 (33)
Patients operated on both eyes after 5 years
376 (71)
The 10-year data
10-year VF-14 data 335 (85)
10 year VA and VF-14 data 289 (73)
Mean age 10 years postoperatively
Mean±SD
78.5±10.7 years
Males 107 (32)
Patients operated on both eyes after 10 years
274 (82)
58
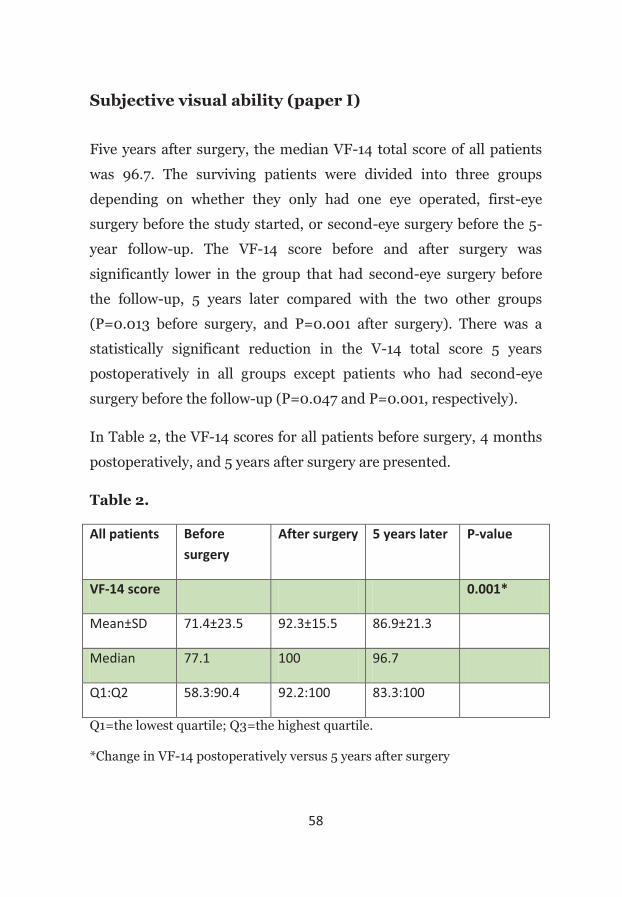
Subjective visual ability (paper I)
Five years after surgery, the median VF-14 total score of all patients
was 96.7. The surviving patients were divided into three groups
depending on whether they only had one eye operated, first-eye
surgery before the study started, or second-eye surgery before the 5-
year follow-up. The VF-14 score before and after surgery was
significantly lower in the group that had second-eye surgery before
the follow-up, 5 years later compared with the two other groups
(P=0.013 before surgery, and P=0.001 after surgery). There was a
statistically significant reduction in the V-14 total score 5 years
postoperatively in all groups except patients who had second-eye
surgery before the follow-up (P=0.047 and P=0.001, respectively).
In Table 2, the VF-14 scores for all patients before surgery, 4 months
postoperatively, and 5 years after surgery are presented.
Table 2.
All patients Before surgery
After surgery 5 years later P-value
VF-14 score 0.001*
Mean±SD 71.4±23.5 92.3±15.5 86.9±21.3
Median 77.1 100 96.7
Q1:Q2 58.3:90.4 92.2:100 83.3:100
Q1=the lowest quartile; Q3=the highest quartile.
*Change in VF-14 postoperatively versus 5 years after surgery
59
Visual acuity results (paper I)
A the five-year follow-up, there were no significant differences in
presenting visual acuity (PVA) and BCVA in the operated eye between
the 3 patient groups. However, there was a significant difference in
presenting visual acuity and BCVA in the fellow eye and between
BCVA in the better seeing eye (P=0.000, P=0.000, and P=o.007,
respectively). Patients who had first-eye surgery between June 1st,
1997, and May 31st, 1998, and second-eye surgery before the follow-up
5 years later had significantly better visual acuity in the better-seeing
eye compared with those who had first-eye surgery before June 1st,
1997, and those who had only one eye operated on. A significantly
larger proportion of patients had co-morbidity in the group that had
first-eye surgery before the study started. (P=0.000).
Changes in VF-14 total score and visual acuity (paper I)
When comparing the subjective (VF-14 total score) and objective (VA
results) visual function results five years after surgery with the
postoperative (a couple of months after surgery) results, we found
that 22% of the patients had a reduction of more than 10 points in
their VF-14 score, and that 37% had lost more than 0.1 logMAR of
visual acuity in the operated eye. Age-related macular degeneration
and glaucoma were the most common diagnoses explaining the
reduction in subjective and objective visual function.
A regression analysis was conducted showing significant associations
60
between the changes in the VF-14 total score and BCVA in the better
eye postoperatively compared with 5 years after surgery, after
controlling for age (P=0.0001). All the independent variables (age,
VF-14 score after surgery, co-morbidity) were highly significant in
explaining the VF-14 score 5 years after surgery. The adjusted r2 value
for the model was 0.53.
Women and men (paper II).
At the 5-year follow-up, 353 women and 177 men participated with
the questionnaire, and 311 women as well as 156 men were examined.
After 5 years, 75% of the women had undergone cataract surgery on
both eyes, compared with 63% of the men, which is a significant
difference (P=0.005).
The women were significantly older than the men at all occasions. The
mean age 5 years after surgery was 78 years (±10), compared with 75
years(±11.6) for the men (P=0.009).
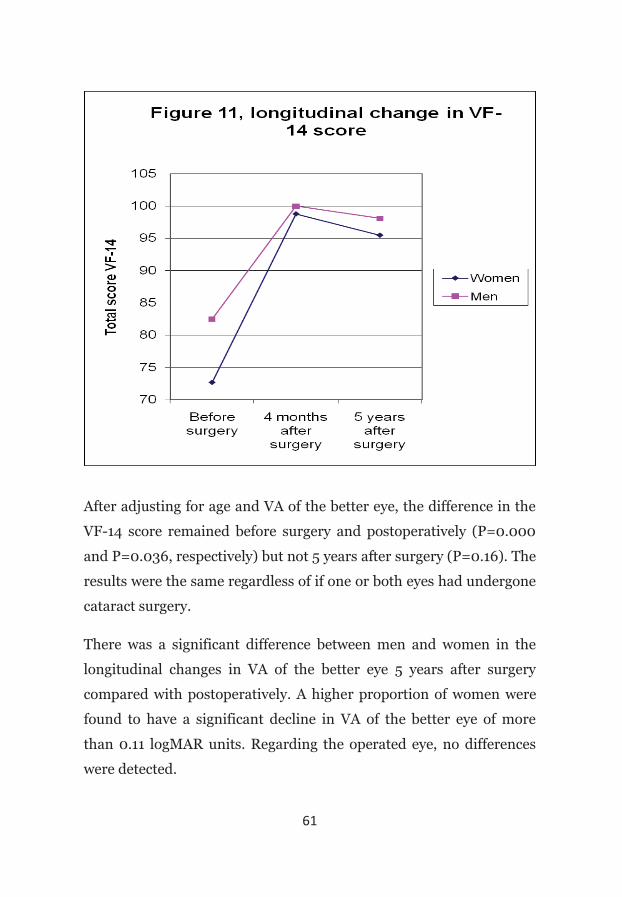
In figure 11, the subjective visual function (VF-14 total score) before
surgery, postoperatively, and 5 years after surgery is presented. Both
before surgery, and at the follow-ups, the median VF-14 scores were
significantly lower for the women.
61
After adjusting for age and VA of the better eye, the difference in the
VF-14 score remained before surgery and postoperatively (P=0.000
and P=0.036, respectively) but not 5 years after surgery (P=0.16). The
results were the same regardless of if one or both eyes had undergone
cataract surgery.
There was a significant difference between men and women in the
longitudinal changes in VA of the better eye 5 years after surgery
compared with postoperatively. A higher proportion of women were
found to have a significant decline in VA of the better eye of more
than 0.11 logMAR units. Regarding the operated eye, no differences
were detected.

62
When investigating the individual responses in the questionnaire, the
women had significantly worse self-assessed visual ability for several
questions, for instance reading, doing handwork and driving. If the
patient did not participate in a specific activity, i.e. driving, the item
was not included in the scoring. A major part of the women did not
take part in activities like sports and driving, but on the other hand
they participated more often than men in areas like cooking.
Diabetics (paper III)
Five years after surgery, 42% of the diabetics compared with 25% of
the non-diabetics were deceased (P=0.001). Fifty-seven of the 63
diabetics, still alive five years after surgery, participated with the
questionnaire, and 47 of them were examined. VA data and degree of
DR of the 10 diabetic patients who were not examined at 5 years was
collected from their records. This was possible as the routine diabetic
care in Sweden includes retinal imaging with a fundus camera every
to every other year, and at the time of the study, VA examinations as
well.
At the time of surgery, 60% (34/57) of the diabetics were treated with
oral anti-hyperglucaemic agents, and 40% (23/57) received insulin.
After 5 years, another two patients were treated with insulin.
Regarding the level of diabetic retinopathy, 65% (37/57) were
unchanged, and 33% (19/57) had progressed. One patient (2%) had
improved, since the removal of the cataract had made treatment of
PDR, including macular oedema, with photocoagulation possible.
63
No significant differences between the 45 diabetics who had died
before the 5-year follow-up, and the 57 surviving diabetics, regarding
VF-14 score, BCVA of the operated eye 4 months postoperatively, and
degree of DR could be detected.
At the 5-year follow-up, the diabetics had somewhat lower VF-14 and
VA results, compared with the non-diabetics. However, these
differences were not significant.
When investigating the longitudinal changes in the VF-14 and VA
results, there was a decrease among both the diabetics and the non-
diabetics. Again, the differences between these two groups were not
significant (P=o.87 and 0.76, respectively).
Younger cataract patients (paper IV)
Ten years after surgery, 12% (14/116) of the younger cataract surgery
patients (30-64 years) were deceased in comparison to 58%
(401/694) of those 65 years or older at surgery.
A total of 95 (93%) patients under the age of 65 years at surgery, and
240 (82%) over 65, answered the questionnaire. The examination
was conducted on 86 (84%) of the 102 younger patients, and on 203
(69%) of the older patients still alive. A larger proportion of the older
patients were women, 72% compared with 57% of those under the age
of 65.
When evaluating the visual functional longitudinal changes, there
were no significant differences between the younger and the older

64
cataract surgery patients before surgery and 4 months after surgery.
However, after ten years, the patients less than 65 years at surgery
had a significantly better VF-14 score (median 98.5 compared with
95.0 for those over 65, (P=0.000)).
Regarding the change in BCVA of the operated eye, 68% of the
patients under 65 years of age at surgery, had better or unchanged
visual acuity results at the 5-year follow-up compared with a couple of
months after surgery. This is a significant larger proportion compared
with the older patients where 42% had better or unchanged BCVA of
the operated eye (P<0.0002).
Ten years after surgery, 28% of all the patients that participated with
the questionnaire had been treated with Nd:YAG capsulotomy
because of posterior capsular opacification. A significantly higher
proportion of those under the age of 65 at surgery were represented in
this group, 37% compared with 20% of the older patients (P=0.003).
When looking specifically at the Nd:YAG laser treatments of the
younger patients, we found that this was especially frequent among
the youngest, 44% of those aged 30-54 compared to 32% of the
patients aged 55-65 years at surgery.
There were significant differences between the younger and the older
patients in the low-contrast VA results, both when testing with the
10% and the 2.5% charts (P=0.000). However, no differences in the
low-contrast VA results between the younger patients that had been
treated with Nd:YAG laser, and those that were not treated, could be
detected.
A life-table analysis was performed to enable an evaluation on the risk

65
of needing treatment with Nd:YAG laser over the ten-year period
studied (Figure 12). Ten years after surgery, the cumulative
proportion of “no capsulotomy” was 72% for patients less than 65 at
surgery and 85% for the patients 65 years or older. At 2.5 and 6 years
postoperatively, there was a steepening of the curve, indicating an
increased risk for YAG laser treatment for the patients less than 65
years of age at surgery.
Figure 12. A survival curve showing the cumulative
proportion of “no capsulotomy” (no treatment with
Nd:YAG) in patients less than 65 years and those 65 years or
older at surgery, from time of surgery to 10 years.
66
DISCUSSION
The study design, validity and reliability
In this prospective population-based cohort study 90% of the patients
still alive five years after surgery, and 85% still alive at ten years,
participated with the questionnaire. Five and ten years
postoperatively, 80% and 73%, respectively, were also examined. In a
cohort study, the major potential selection bias is loss to follow-up.
Bias is a systematic error in a study that might influence the results.
This kind of systematic error might lead to a distortion of study
results that makes the association stronger or weaker than it really is.
The most common classification divides biases into three categories:
selection bias, information bias or confounding.167
In order to reduce selection bias, and apply the results on the
population as a whole, great efforts were made to minimize data
losses. At the five and ten year follow-ups, phone-calls were made to
all the patients still alive, in order to offer them a scheduled
appointment for the follow-up examination. Instead of mailing an
invitation letter, this manner probably increased the participation
rate at the follow-ups, minimizing the possibility that findings based
on the cohort were biased by loss to follow-up.
Information bias can occur when there is a systematic inaccuracy in
measurements. To reduce information bias, the same research nurse
tested the visual acuity of all participating patients at the five-and ten
year follow-ups. At the eye-examination five years postoperatively,
two ophthalmologists conducted the slit-lamp examinations. Ten

67
years postoperatively, all examinations were performed by one
ophthalmologist.
Confounding comes from the Latin word, confundere, which means
“to mix together”. It refers to the mixing of the effect of a variable
which may influence the comparability between individuals. In order
to control for confounding in the analyses, adjustments were made for
age, first or second eye surgery, BCVA of the better eye, and co-
morbidity.
The concept of validity concerns the degree to which a measurement
or study reaches a correct conclusion. If, in a study population, the
results are not valid, there is little reason to suspect that those results
will apply to other populations. Internal validity is the extent to
which the results of an investigation accurately reflect the true
situation of the study population. It is important for a study to have
internal validity, the ability to measure what it sets out to measure.168
In this study, at all follow-ups, the VF-14 questionnaire was used to
determine the subjective visual function. This questionnaire is a well-
validated instrument to assess visual function, presented by Steinberg
et al. in 1994.62 It has thoroughly been described in the “material and
methods “section.
Patient-reported questionnaires in the assessment of cataract surgery
is now widely appreciated.169,170 There are several questionnaires
developed for this matter, such as the VF-14,62 the Visual Disability
Assessment (VDA),171 and the Catquest.172 Some of the limitations
with these questionnaires are the validity of the scoring method and
the validity of the items included.173 Therefore, to evaluate if an
outcome method is still valid, Rasch-analysis can be performed. In
68
brief, Rasch analysis is a mathematical model developed by the
Danish mathematician George Rasch, which attempts to estimate the
values of a latent variable on an interval scale from items that form an
ordinal scale. Disability can be considered to lie on a ruler, and the
range of disability is expressed in log-odd units. The Rasch-model has
been used in the validation of several vision-specific questionnaires,
for example the Activities of Daily Vision Scale,174 the NEI,175 and the
Catques-9SF.172 In a study by Lee et al from 2006, a Rasch
methodology analysis proved the VF-14 to be an appropriate measure
of visual functioning in cataract surgery patients.176 However, when
investigating the separate questions, the item “taking part in sports”
showed low applicability, probably due to the old age of the
participants.
External validity or generalizability is the extent to which the results
of a study are applicable to other populations. This is of particular
interest in clinical research in determining if a finding can be
applicable in a clinical practice. The cohort described in this thesis,
well represents the Swedish cataract population with 65% women,
and a mean age at surgery of 73.6 and 75.4 years, for the men and the
women, respectively. The rate of cataract surgery was 5.2 per 1000
population, which is well comparable with that of the country as a
whole at the time. Given the internal and external validity discussed
above without strong bias or confounding factors, the results in the
papers could therefore be generalized to a Swedish population.
This thesis describes a cohort including all patients having cataract
surgery in a defined area during a one-year period. Population-based
studies, as the present one, remain the most valid to determine the

69
prevalence and incidence of a disease and to better treat these
diseases.177 The Swedish health care system is especially suitable for
these evaluations since it is comparatively easy to locate patients even
five and ten years after surgery, which reduces the drop-out rate.
Furthermore, at the time of the study, the likelihood of cataract
patients having surgery outside county borders was negligible which
also increases the validity. Repeated surveys over time may also
demonstrate the impact of preventive strategies. Long-term follow-up
studies of existing population-based cohorts, provide important
insights in risk factors and disease pathogenesis and allow
documentation of the incidence of diseases, and changing levels of
risk factors over time. In the last 30 years, the role of some of the
most important risk factors for eye diseases have been detected using
prospective follow-up of population-based cohorts, eg. the role of
hyperglycemia as a risk factor for diabetic retinopathy in WESDR,178
the role of hypertension in risk of AMD in the Beaver Dam Eye
Study.179
Moreover, some associations are seen only with longer-term follow-
up, for example the role of dietary factors in AMD progression,
presented in the Blue Mountain Eye Study, was seen in the 10-year
but not in the five-year follow-up study.
The integration of current best evidence with clinical practice is
referred to as evidence-based medicine. Medical practice must be
evidence-based as a result of tight budgets, waiting lists, and the need
to target resources. From the individuals’ point-of –view it is also
valuable to receive information on the long-term results after surgery.

70
Visual outcome analysis
Five years after surgery, more than half of the patients had unchanged
or better VF-14 score compared with a couple of months
postoperatively, which must be considered as a favorable outcome.
More than three-quarters had a decline of less than 10 points. Almost
two thirds, or 296 (63%) of the 467 patients examined, had preserved
VA (less than 0.1 logMAR deterioration) in the operated eye 5 years
after surgery.
In studies assessing cataract surgery outcome one must be aware of
the fact that the patients before surgery, in most instances, have two
eyes with varying degree of cataract, or that the fellow eye might
already have had surgery. At the five-year follow-up, the patients were
divided into three groups based on whether they had cataract surgery
on one or two eyes. The first group had first eye surgery, the second
group had their first eye operated on before the study started, and the
third group had second eye surgery sometimes between baseline and
the five-year follow-up.
At baseline, the VA was measured on a decimal chart, and at the five-
and ten year follow-ups, the EDTRS chart was used. It would have
been preferable to utilize the same VA test charts at all occasions, but
when this study commenced the EDTRS charts were not an option. At
each examination, the visual acuity was measured on both the
operated eye, and the fellow eye. The better-seeing eye is the eye with
the best VA, most commonly, but not always, equivalent to the eye not
having surgery. In outcome studies the VA-result is often associated
with the subjective visual function assessed by a questionnaire. In
these cases it is essential to assess the VA of the patients’ better-

71
seeing eye, as the subjective visual function has been shown to depend
more on the vision of the better eye than the worse eye.62,180
At the five-year follow-up, 29% of the patients had only one eye
operated. This patient group sustain their subjective and objective
visual function well, probably because they do not have a significant
vision disturbing cataract in the fellow eye.
The patients in the group that had first eye surgery before the study
started, in 1997, had a significant decrease in their VF-14 total score
five years after surgery compared with postoperatively. Only 26% had
a BCVA better than 20/25 of the fellow eye. Five years after surgery,
these patients presented a larger proportion of ocular co-morbidity,
which might have been true also when they entered the study. The
importance of co-morbidity in explaining deterioration of visual
function has previously been discussed by Lundström et al. in 2005.181
The surgical methods used before 1995 at our clinic, ie. extracapsular
cataract extraction with an incision length of more than 6mm, may
not have been as effective as phacoemulsification in restoring VA and
visual function. The frequency of posterior capsular opacification
might also have been higher with older lens materials. There was no
significant difference in age between the groups. Hence, the patients
in the group that had first eye surgery before the enrolment in 1997
were younger when they first requested surgery.
The patients who had their first eye operated on in 1997-98 and had
second eye surgery before the follow-up 5 years later had a
significantly lower VF-14 score before surgery and at the first
postoperative follow-up (about 4 months after surgery) compared
with the other two groups. The reason for this is probably that they
72
had cataract on both eyes when they were enrolled. When
investigating the change in VF-14 score five years after surgery
compared with postoperatively, there was no significant decrease in
this patient group. This is expected, as in this group, the fellow eye
surgery had improved the VA, and VF-14 total score.
The findings of this study are in accordance with previous research,
and show that the most important reason for the worsening of both
the subjective visual function (VF-14 total score), and the VA (BCVA
operated eye), was age-related macular degeneration (60% and 47%
respectively). The issue whether or not ARM is augmented by cataract
surgery has intensely been discussed in several papers.182 There are
studies showing both the benefits,183,184 and risks,185 with cataract
surgery on ARM-patients. The present study was however not
designed to analyze the potential risks with cataract surgery, nor
answer the question if cataract surgery might exaggerate the
development of ARM.
Gender-related differences
In this population-based study, men came earlier to surgery as they
had significantly better BCVA of their better-seeing eye before
surgery. These findings deviate from several previous studies who
before surgery found no significant difference in VA of the better eye
between men and women.47,82,84 These results might be explained by a
larger proportion of men being active car-drivers in the older age
groups, and therefore require better vision. In a previous study on
visual function in car drivers from 2006, 66% of the active drivers
73
before surgery were men.186 Car-driving especially in darkness and
dusk is challenging for people with cataracts. The impact of lower VA,
glare sensitivity and reduced contrast sensitivity might explain why,
in the present study, it was found that men came earlier to surgery.
Before surgery and a few months postoperatively, the women
experienced significantly more subjective visual functional
impairment compared with the men, even after adjustment for age
and BCVA of the better eye. This is consistent with previous research
that the pre-operative VF-14 score was slightly better for men.62,84 In
this study the difference 5 years after surgery was less obvious. The
women still had a lower VF-14 score but after adjusting for age and
BCVA of the better eye, the difference was not significant. The
findings agree with previous research that women score worse than
men in self-reported visual function.49
Gender-related differences have been observed in objective and self-
reported perceived health also in general health care. Women are
believed to be more prone to a poor self-rated health status and they
report more physical symptoms than men.187 Previous health
researchers conclude than men and women differ in how symptoms
are perceived, evaluated and acted upon.188 Some of them support the
hypothesis that women have a higher selective attention to their
bodies.76,187 Traditional ideals not to succumb to weaknesses among
men might to some part explain these gender-related differences.
When evaluating the responses to specific questions, significant
gender-related differences were found regarding most items. Women
were more likely than men to report that their vision limited their
ability to read road signs, to recognize people across the street, and to

74
drive at night. Most elderly women did not take part in sport-
activities and were not active car-drivers, which caused a low
response-rate for these questions. This is also true for men regarding
cooking. The VF-14 questionnaire has been revalidated with Rasch
analysis.176 However, it has not been validated to determine if it is
appropriate for use in both women and men. Further studies are
required to establish the validity of questionnaire instruments and
one way might be to validate questionnaires separately for men and
women.
The results of this study illustrate that gender differences in
subjective and objective visual function exist among cataract patients
before and after surgery, as well as on a long-term basis. These
gender-related differences in the perception of visual function should
be considered when analyzing questionnaire results regarding visual
function.
Visual function and progression of retinopathy in
diabetics
When this population-based study was initiated, in 1997, 108 (13%) of
the 810 participants were diabetics treated with either insulin or anti-
hyperglucaemic agents. Since the phacoemulsification surgery
technique became widely accepted in the 1990s, fewer postoperative
complications in diabetics, like cystoid macular oedema and
progression of DR, have been reported.102,189 In the present study,
progression of DR was seen in 37% of the diabetic patients 5 years
after surgery, compared with postoperatively. This is a larger

75
proportion compared with the study by Mittra et al. from 200097
(follow-up time 6-10 months after phacoemulsification), but it is
consistent with the results by Antcliff et al. from 1997103 (follow-up
time two years), Pollack et al. 1991190(6 months) ,and Henricsson et al
1996191 (2 years). However, the considerably longer follow-up time
most probably explain the higher percentage of progression in this
study.
The question is whether this is a natural history of the disease or not.
Paired-eye comparisons (one eye having cataract surgery, the other
not operated on) have been conducted by Krepler et al in 2002,192 and
Squirrel et al in 2002.104 None of these studies could detect any
significant differences in DR progression rates between operated and
non-operated eyes, although the reported progression rates were
consistently and slightly higher in operated compared with non-
operated eyes.104,,192
There were no significant differences in VF-14 score or in VA-results
between the diabetics and the non-diabetics. As expected, the
diabetics with PDR had the lowest BCVA of the operated eye at all
examinations. However, they did not have a significantly greater
longitudinal loss in median BCVA compared with patients with less
DR. The majority of these diabetic patients had a considerably better
VA of the operated eye at the 5-year follow-up compared with
preoperatively. This indicates that cataract surgery is beneficial also
for diabetics with PDR.
A larger percentage of the diabetics (42%) compared with the non-
diabetics (25%) were deceased 5 years after surgery. This is probably
due to other medical problems, like cardiovascular disease, being

76
more common among diabetics.193 The diabetics that had died before
the 5-year follow-up did not have a significantly worse DR level at
surgery compared with the diabetics who were still alive at the 5-year
follow-up. However, previous studies on diabetes and complications
have presented significant associations between levels of retinopathy
and mortality.194
Some limitations of the study should be noted. First, the number of
surviving diabetics five years after cataract surgery is rather small
compared with the non-diabetics. This is inevitable, since most
patients operated for cataract are old and many of them die within
five years after surgery. Diabetics have a shorter life-span than non-
diabetics.193 However, a recently published paper found improved
survival in diabetics.195 Age-adjusted survival rates increased from
approximately 70% in 1985 to more than 80% in 2005, probably due
to significant changes in cardiovascular prevention therapy.
The small insignificant differences in VA and VF-14 between diabetics
and non-diabetics made power calculations necessary. At least 8000
patients would be needed in each group to reach significance – an
impossible number of patients for any study with a 5-year follow-up.
A second limitation is that the preoperative level of DR was assessed
by studying the patients’ records. At the follow-up five years after
surgery any DR was determined at the slit-lamp examination. It
would have preferable to compare retinal fundus photographies from
all occasions. However, this was not possible since the cataract, in
many cases, made it difficult to obtain a photograph sharp enough to
evaluate. Furthermore, if the cataract was completely mature, the
grading of any DR was impossible. If no information about DR was
77
recorded preoperatively, the level of DR at the postoperative follow-
up, 4-8 weeks after surgery, was denoted as the preoperative DR.
Cataract surgery outcomes in younger patients
PCO is by far the most common complication after cataract surgery,
and is considered a normal wound healing process.196 Almost 40% of
the patients in the study less than 65 at surgery, had received Nd:YAG
laser treatment 10 years after surgery compared with 20% of the
patients 65 years or older. This is consistent with earlier observations,
reporting a higher incidence of PCO in younger patients.197 The
figures exceed previously published 2-year results on Nd:YAG
capsulotomy rates after phacoemulsification and implantation of
Alcon AcrySof® MA60BM IOLs, of 2.7%.198 A similar high rate of
Nd:YAG capsulotomy, as found in this study, was presented in a
recently published article by Vock et al.199 In their retrospective study,
42% of 99 eyes (mean age 66.4 years) with acrylic hydrophobic lenses
(MA60BMAcrysof® IOL, Alcon Inc) had received Nd:YAG laser
capsulotomy after 10 years. However, the results from the study
presented in this thesis do not indicate that the sharp-edged
hydrophobic lenses lose their protectiveness against PCO after 10
years, as postulated by Vock et al. A considerable rise in the PCO rates
was present as early as after 2.5 years with a deceleration six years
after surgery (Figure 12).
In this study, the vast majority (90%) of patients less than 65 years of
age, had a decline in VF-14 score of fewer than 10 points, ten years
after surgery, and more than 60% had unchanged or better VF-14
78
total score. Eighty percent had preserved VA (less than 0.1 logMAR
deterioration) in the operated eye 10 years after surgery. These long-
term results must be considered a favorable outcome.
The lack of difference in low contrast VA, between the patients less
than 65 at surgery that were treated or not treated with Nd:YAG laser,
indicates that most of the patients in need for posterior capsulotomy
already had received this at the 10-year follow-up. Because of the
Swedish Social Security system it is considerably easy to receive an
appointment with an ophthalmologist, and the cost for the patient is
fairly modest. In view of the longer life-expectancy among younger
cataract patients, stable visual functional results are important also
decades after surgery.
79
CONCLUSION
Paper 1. Five years after cataract surgery, approximately 50% of
the patients in the population-based cohort had
unchanged or better subjective and objective visual
function compared with the postoperative results. The
main reason for the decline in VF-14 total score and the
visual acuity results was age-related macular
degeneration.
Paper 2. Women undergoing cataract surgery assess their visual
function worse than men after adjustment for age and
VA preoperatively and a few months postoperatively.
These differences were not significant five years after
surgery although the men had better BCVA of their
better seeing eye. It is important to be aware of gender-
related differences in perception when performing
questionnaire-based outcome studies.
Paper 3. Five years after surgery, diabetics sustain their
subjective and objective visual function at
approximately the same level as non-diabetics. No
significant differences between diabetics and non-
diabetics regarding VF-14 total score, visual acuity or
the longitudinal changes in visual function could be
detected. Five years after surgery, only 33 % of the
diabetics had a progression in their DR. The data
suggest that phacoemulsification is beneficial also five
years after surgery in terms of visual and functional

80
improvement in diabetics with significant cataract.
Paper 4. Ten years after surgery, subjective and objective visual
function remained stable in most patients younger than
65 years at surgery. Approximately 80% had unchanged
or better VA of the operated eye, and 90% had less than
10 points decline in their VF-14 score. More than one-
third had been treated with Nd:YAG because of vision-
disturbing PCO. The cumulative proportion of “no
capsulotomy” 10-years after surgery was 72% for those
less than 65 at surgery, and 85% for the patients 65
years or older.
FUTURE PERSPECTIVES
In 2012, 15 years will have passed since the first patients included in
this cohort had cataract surgery. The intention is to continue to follow
the surviving patients 15 and 20 years postoperatively. The
participation rate at the follow-ups completed so far has been high.
However, in a cohort with mostly elderly people, as the one described
in this thesis, it is inevitable that some will die. For the patients as
well as for the health care providers it is important that long-time
results are analyzed and published.
At the five-year follow-up, 530 cataract surgery patients participated
with the questionnaire. After ten years there were still 335 people
included in the study. Long-term, prospective, population-based
studies after cataract surgery including data ten years postoperatively
81
are scarce. The Swedish health care system, in 1997, was especially
suitable for these studies, because the risk for cataract patients to be
operated outside county borders was small, and it is fairly easy to
locate patients also after several years. The northern part of the
country, in particular, is appropriate for these studies since private
options for cataract surgery are insignificant.
Changes in the Swedish Health Care Policy, with a more favorable
attitude towards private health care, and an increased freedom of
choice, have resulted in a greater likelihood for patients to have
cataract surgery outside the area of their registered residence.
Furthermore, pre- and post-operative examinations in cataract
surgery have been heavily rationalized, resulting in fewer follow-up
occasions than previously. Today, a similar study like the one
described in this thesis would be much more difficult to accomplish.

82
ACKNOWLEDGEMENTS
I wish to express my warmest gratitude to:
Associate Professor, Eva Mönestam, my supervisor, for your
never-ending enthusiasm, valuable advice, and clear answers
to all my questions. I am deeply impressed by your incredible
speed, and statistical knowledge!
My co-supervisor, Professor Emerita Lillemor
Wachtmeister, for your vast knowledge, encouraging
interest for the project, helpful comments and support.
Fatima Pedrosa-Domellöf, Professor of the Department of
Ophthalmology, for creating a stimulating research
atmosphere.
Associate Professor, as well as the head of the Division of
Ophthalmology, Christina Lindén, for your energy, good
moods, and beautiful clothing.
The Eye Clinic at Lycksele Hospital for providing me with
the data necessary to accomplish this study.
Hans Stenlund, PhD, Department of Epidemiology and
Statistics, Umeå University, for your support and aid with the
statistical analyses.
Mikael Hansson, research nurse, for invaluable work during
the collection of data, and for safe driving on the way to
Vilhelmina and Storuman……..
83
The administrator at the Division of Ophthalmology, Birgit
Johansson, for skilful assistance with all administration.
My collagues at the eye clinic, NUS, Umeå, for doing all the
clinical work while I was working on this thesis.
Ann Germann at Arkitektkopia, for computer support
before the thesis was printed.
Birgitta Glaas, Gittan, my best friend, for devoted help with
difficult English grammar. Thank you for your patience with
my complaints!
My husband, Per, for all the gourmet cooking and music
entertainment!
Last, but not least, all the cataract surgery patients who
participated in this study.
This study was supported by grants from the Västerbotten County
Councils, Crown Princess Margareta’s Committee for the Blind, the
Swedish Medical Society, and Karin Sandqvists Stiftelse.

84
REFERENCES
1. Asbell PA, Dualan I, Mindel J, et al. Age-related cataract. Lancet 2005;365:599-609.
2. Allen D, Vasavada A. Cataract and surgery for cataract. BMJ 2006;333:128-132.
3. Johns KJ, Feder RS, Hammill BM, et al. Lens and Cataract: section 11, basic and clinical science course. San Francisco 2003: American Academy of Ophthalmology.
4. Klein BE, Klein R, Moss SE. Incident cataract surgery: the Beaver Dam eye study. Ophthalmology 1997;104(4):573-580.
5. McCarty CA, Taylor HR. A review of the epidemiologic evidence linking ultraviolet radiation and cataract. Dev Ophthalmol 2002;35:21-31.
6. Jobling AI, Augusteyn RN. What causes steroid cataracts? A review of steroid-induced posterior subcapsular cataracts. Clinical and Experimental Optometry 2002;85(2):61-75.
7. Leske MC, Wu SY, Hennis A et al. Diabetes, hypertension, and central obesity as cataract risk factors in a black population. The Barbados Eye Study. Ophthalmology 1999;106(1):35-41.
8. Jacques PF, Moeller SM, Hankinson SE, et al. Weight status, abdominal adiposity, diabetes, and early age-related lens opacities. Am J Clin Nutr 2003;78(3):400-405.
9. Mukesh BN, Le A, Dimitrov PN et al. Development of cataract and associated risk factors: the Visual Impairment Project. Arch Ophthalmol 2006;124(1):79-85.
10. Spector A. Oxidative stress-induced cataract: mechanism of action. FASEB J. 1995;9:1173-1182.
11. Olofsson E, Marklund S, Behndig A. Enhanced age-related cataract in copper-zinc superoxide dismutase null mice (manuscript). Paper IV from the thesis “Superoxide dismutase 1 and Cataract” 2009, ISBN 978-91-7264-749-7. “
85
12. Kuszak JR, Deutsch TA, Brown HG. Anatomy of aged and senile cataractous lenses. In: Albert DM, Jakobiec FA, eds. Principles and Practice of Ophthalmology. Philadelphia: Saunders;1994;564-575.
13. Sayeh RR, Floyd RP, Ghanem RC. History of cataract surgery. In: Albert D M MJW, ed. Albert & Jakobiec´s Principles and Practice of Ophthalmology. Philadelphia: Saunders;2008;1,3.
14. Datilies M. Clinical Evaluation of Catarcts. Duanes’ Clinical Ophthalmology 1996:1-25.
15. Daviel J. Sur une nouvelle méthode de guérir la cataracte par l´extraction du crystallin. Mém Acad Roy Chir 1753;2:337-354.
16. Ridley H. Further observations on intraocular acrylic lenses in cataract surgery. J Int Coll Surg 1952;18:825-833.
17. Barraquer J. [Total extraction of the lens after disintegration of the zonula by alphachymotrypsin=enzyme zonulysis]. Klin Monatsblatter Augenheilkd Augenarzil Fortbild 1958;133:609-615.
18. Krwawicz T. Further Experience With Intracapsular Cataract Extraction By Application Of Low Temperature. Br J Ophthalmol 1963;47:36-38.
19. Kelman CD. Phaco-emulsification and aspiration. A new technique of cataract removal. A preliminary report. Am J Ophthalmol 1967;64:23-35.
20. Elder 1969. Duke-Elder S. Systems of Ophthalmology. XI Diseases of the lens. Vol 11. Henry Kimpton, 1969.
21. Riaz Y, Mehta JS, Wormald R, et al. Surgical intervention for age-related cataract. The Cochrane Library 2009, Issue 4.
22. Duane T. Textbook of Ophthalmology. Lippincott-Raven, 1986:25.
23. Apple DH, Mamalis N, Olson, et al. Intraocular lenses: Evolution, Designs, Complications, and Pathology. William & Wilkins, 1989:225-361.
86
24. Ruit S, Paudyal G, Gurung R, et al. An innovation in developing world cataract surgery: sutureless extracapsular cataract extraction with intraocular lens implantation. Clinical and Experimental Ophthalmology 2000;28:274-279.
25. Lundström Mats, Stenevi U, Thorburn W. Svensk Kataraktkirurgi, årsrapport 2001. www.cataractreg.com.
26. Snellingen T, Evans JR, Ravilla T, et al. Surgical interventions for age related cataract. Cochrane Database Syst Rev 2002;(2):CD001323.
27. Osborne SA, Adams WE, Bunce CV, et al. Validation of two scoring systems for the prediction of posterior capsule rupture during phacoemulsification surgery. Br J Ophthalmol 2006;90:333-6.
28. Obstbaum SA. Indications and timing of cataract surgery. J Cataract Refract Surg 1995;21(5):483.
29. Romanchuk KG, Sanmugasunderam S, Hadorn DC. Developing cataract surgery priority criteria: results from the Western Canada Waiting List Project. Can J Ophthalmol 2002;37:145-54.
30. Kupfer C. The International Agency for the Prevention of Blindness. Am J Ophthalmol 1994;117(2):253-257.
31. Foster A, Resnikoff S. The impact of Vision 2020 on global blindness. Eye 2005;19:1133-1135.
32. Minassian DC, Mehra V. 3.8 million blinded by cataract each year: projections from the first epidemiological study of the incidence of cataract blindness in India. Br J Ophthalmol 1990;74(6):341-3.
33. Limburg H, Kumar R, Bachani D. Monotoring and evaluating cataract intervention in India. Br J Ophthalmol 1996;80(11):951-955.
34. Thylefors B. A global initiative for the elimination of avoidable blindness. Am J Ophthalmol 1998;125(1):90-93.
35. Resnikoff S, Passolini D, Eryalale D, et al. Global data on
87
visual impairment in the year 2002. Bulletin of The World Health Organisation 2004;82:844-851.
36. Passolini D, Mariotti SP, Pokharel GP, et al. Global update of available data on visual impairment: a compilation of population-based prevalence studies. Ophthalmic Epidemiology 2004:11:67-115.
37. Kahn HA, Leibowitz HM, Ganley JP, et al. The Framingham Eye Study. Outline and major prevalence findings. Am J Epidemiol 1977;106:17-32.
38. Klein BEK, Klein R, Linton KLP. Prevalence of age-related lens opacities in a population. The Beaver Dam Eye Study. Ophthalmology 1992;99:546-552.
39. Östberg A, Löth A, Gustafson D, et al. Prevalence of Lens Opacities in a Swedish Community. Ophthalmology 2006;113:970-5.
40. Gray CS. Waiting in the dark: cataract surgery in older people. BMJ 1999;318:1367-1368.
41. Lundström M, Stenevi U, Montan P, et al. Svensk Kataraktkirurgi, Årsrapport 2008 baserad på data från Nationella Kataraktregistret, www.cataractreg.com.
42. Javitt JC, Brenner MH, Curbow B, Legro MW, Street DA. Outcomes of cataract surgery: Improvement in visual acuity and subjective visual function after surgery in the first, second , and both eyes. Arch Ophthalmol 1993;111:686-91.
43. Lundström M, Stenevi U, Thorburn W. Quality of life after first- and second-eye cataract surgery. Five-year data collected by the Swedish National Cataract Register. J Cataract Refract Surg 2001;27:1553-1559.
44. Laidlaw A, Harrad R. Can second eye cataract extraction be justified? Eye 1993;77:680-686.
45. Elliott DB, Patla AE, Furniss M, et al. Improvements in clinical and functional vision and quality of life after second eye cataract surgery. Optom Vis Sci 2000;77:13-24.
88
46. Castells X, Comas M, Alonso J, et al. In a randomized controlled trial, cataract surgery in both eyes increased benefits compared to surgery in one eye only. J Clin Epidemiol 2006;59:201-207.
47. Carlsson B, Sjöstrand J. Increased incidence of cataract extractions in women above 70 years of age. A population-based study, Acta Ophthalmol Scand 1996;74:64-68.
48. Lundström M, Stenevi U, Thorburn W. Gender and cataract surgery in Sweden 1992-1997, a retrospective observational study based on the Swedish National Cataract Register. Acta Ophthalmol Scand 1999;77:204-208.
49. Klein BE. Lens opacities in women in Beaver Dam, Wisconsin: is there evidence of an effect of sex hormones? Trans Am Ophthalmol 1993;91:517-44.
50. Lundstsröm M. Measuring surgical outcomes. J Cataract Refract Surg 2004;10:2025-2026.
51. Holland GN, Earl DT, Wheeler NC, et al. Results of inpatient and outpatient cataract surgery. Ophthalmology 1992;99:845-52.
52. Powe NR, Schein OD, Giese SC, et al. Synthesis of the literature on visual acuity and complications following cataract extraction with intraocular lens implantation. Arch Ophthalmol 1994;112:239-252.
53. Hess R, Woo G. Vision through cataracts. Vision Res. 1978;17:428-435.
54. Elliott DB, Hurst MA, Weatherill J. Comparing clinical tests of visual function in cataract with the patient’s perceived visual disability. Eye 1990;4:712-717.
55. Bernth-Petersen P. Visual functioning in cataract patients: methods of measuring and results. Acta Ophthalmol (Copenh). 1981;59:198-205.
56. Cataract Management Guideline Panel. Cataract in adults: management of functional impairment. Rockville, MD: US Department of Health and Human Services, Public Health
89
Service, Agency for Health Care Policy and Research, 1993 (AHCPT Publication No 93-0542;Clinical Practice guideline NO 4).
57. Parrish RK. Visual impairment, visual functioning, and quality of life assessments in patients with glaucoma. Trans Am Ophthalmol Soc 1996;19:919-1028.
58. Garratt AM, Ruta DA, Abdalla MI, et al. The SF36 health survey questionnaire: an outcome measure suitable for routine use within the NHS? BMJ 1993;306:1440-44.
59. Bergner M, Bobbitt RA, Carter WB, et al. The Sickness Impact Profile:development and final revision of a health status measure. Med Care 1981;19(8):787-805.
60. Wilson I, Cleary P. Linking Clinical Variables With Health-Related Quality of Life – a conceptual model of patient outcome. JAMA 1995;273(1):59-65.
61. Damiano AM, Steinberg EP, Cassard SD, et al. Comparison of generic versus disease-specific measures of functional impairment in patients with cataract. Med Care 1995;33:AS120-AS130.
62. Steinberg E, Tielsch J, Schein O, et al. The VF-14, an index of functional impairment in patients with cataract. Arch Ophthalmol 1994;112:630-638.
63. Cassard SD, Patrick DL, Damiano AM, et al. Reproducibility and responsiveness of the VF-14. An index of functional impairment in patients with cataracts. Arch Ophthalmol 1995;113:1508-1513.
64. Lundström M, Stenevi U, Thorburn W. The Swedish National Catatact Register: a 9-year review. Acta Ophthalmol Scand 2002;80:248-257.
65. Mangione C, Phillips R, Seddon J, et al. Development of the Activities of Daily Vision Scale. Medical Care 1992;30(12):1111-1126.
66. Javitt JC, Jacobson G, Schiffman RM. Validity and reliability of the Cataract TyPE Spec: an instrument for measuring

90
outcomes of cataract extraction. Am J Ophthalmol 2003;136:285-290.
67. Gutierrez P, Wilson R, Johnston C, et al. Influence of glaucomatous visual field loss on health-related quality of life. Arch Ophthalmol 1997;115:777-784.
68. Ross J E, Bron AJ, Clarke DD. Contrast sensitivity and visual disability in chronic simple glaucoma. Br J Ophthalmol 1984;68:821-827.
69. Cleary PA, Beck RW, Bourque LB, et al. Visual symptoms after optic neuritis:results from the optic neuritis treatment trial. J Neuro-Ophthalmol 1997;17:18-28.
70. World Development Report 1993. Investing in Health. New York: Oxford University Press; 1993:23. Available at:http://www.dcp2.Org/file/62/world%20Development%20Report%201993.pdf. Accessed December 1, 2006.
71. Kobelt G, Lundström M, Stenevi U. Cost-effectiveness of cataract surgery. A method to assess cost-effectiveness using registry data. J Cataract Refract Surg 2002;28(10):1742-1749.
72. Busbee B, Brown M, Brown G, et al. Incremental cost-effectiveness of initial cataract surgery. Ophthalmology 2002;109(3):606-612.
73. Brown MM, Brown GC. How to interpret a healthcare economic analysis. Curr Opin Ophthalmol 2005;16:191-194.
74. Lansingh C, Carter M, Martens M. Global cost-effectiveness of Cataract Surgery. Ophthalmology 2007;114:1670-1678.
75. Risberg G, Johansson E, Westman G, et al. Gender in medicine – an issue for women only? A survey of physician teachers’ gender attitudes. International Journal for Equity in Health 2003;2:10-19.
76. Hammarström A, Härenstam A, Östlin P. Gender and health: Concepts and explanatory models. In: Östlin. Gender inequalities in health: a Swedish perspective. Cambridge; MA: Harvard Center for Population and Development Studies, Harvard University. 2000. Press 1-22.
91
77. Fink B, Wagner H, Steger-May K, et al. Differences in Keratoconus as a Function of Gender. Am J Ophthalmol 2005;140:459-468.
78. McCarty CA, Ng I, Waldron B, et al. Relation of hormonal and menopausal status to outcomes following excimer laser photorefractive keratectomy in women. Aust N Z J Ophthalmol 1996;124:215-222.
79. Schaumberg DA, Sullivan DA, Dana MR. Epidemiology of dry eye syndrome. Adv Exp Med Biol 2002;506:989-998.
80. Bishara SA, Goya V & Rand WJ. Cataract and ocular parameters: Sexual comparison. Ann Ophthalmol 20:73-74.
81. Olofsson P, Lundström M, Stenevi U. Gender in referral to cataract surgery in Sweden. Acta Ophthalmol Scand 2001;79:350-353.
82. Ninn-Pedersen K, Stenevi U, Ehinger B. Cataract patients in a defined Swedish population 1886-1990. Acta Ophthalmol (Copenh)1994;72:1-9.
83. Morgan LW, Schwab IR. Epidemiologic Aspects of Senile Cataract Extraction Stratified by Visual Acuity, Age and Sex. Am J Ophthalmol 1985;100:520-522.
84. Mönestam E, Wachtmeister L. Cataract surgery from a gender perspective – a population-based study in Sweden. Acta Ophthalmol Scand 1998;76(6):711-716.
85. Freeman EE, Munoz B, Schein OD, et al. Hormone replacement therapy and lens opacities: the Salisbury Eye Evaluation Project. Arch Ophthalmol 2001;119:1687-1692.
86. Younan C, Mitchell P, Cumming RG, et al. Hormone replacement therapy, reproductive factors and the incidence of cataract and cataract surgery: the Blue Mountains Eye Study. Am J Epidemiol 2002;155:997-1006.
87. Klein B, Klein R, Lee K. Reproductive exposures, incident age-related cataracts, and age-related maculopathy in women: the Beaver Dam Eye Study. Am J Ophhalmol 2000;130:322-326.
92
88. Worzala K, Hiller R, Sperduto RD, et al. Postmenopausal hormone use, type of menopause, and lens opacities: the Framingham studies. Arch Intern Med 2001;161(11):1448-1454.
89. Cumming RG, Mitchell P. Hormone replacement therapy, reproductive factors, and cataract. The Blue Mountains Eye Study. Am J Epidemiol 1997;145:242-249.
90. Ejdervik Lindblad B, Håkansson N, Philipson B, et al. Hormone replacement therapy in relation to risk of cataract extractions. A prospective cohort study of women (manuscript). From the thesis “Risk Factors for Age-related Cataract-a prospective cohort study”. 2008, ISBN 978-91-7409-199-1.
91. King H. Epidemiology of glucose intolerance and gestational diabetes in women of childbearing age. Diabetes Care 1998, 21 Supplement. 2:B9-13.
92. Wild S, Roglic G, Green A, et al. Global Prevalence of Diabetes, Diabetes Care 2004;27:1047-1053.
93. Lee PP, Feldman ZW, Ostermann J, et al. Longitudinal prevalence of major eye diseases. Arch Ophthalmol 2003;121:1303-1310.
94. Klein BE, Klein R, Lee K. Diabetes, Cardiovascular Disease Risk Factors, and the 5-year Incidence of Age-Related Cataract and Progression of Lens Opacities: The Beaver Dam Eye Study. Am J Ophthalmol 1998;126:782-790.
95. Klein BE, Klein R, Moss SE. Incidence of cataract surgery in the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Am J Ophthalmol 1995;119:295-300.
96. Steele C, Steel D, Waine C. Diabetes and the eye. 2008, page 170. ISBN 978-0-08-045307-1.
97. Mittra R, Borrillo J, Mieler W, et al. Retinopathy Progression and Visual Outcomes After Phacoemulsification in Patients With Diabetes Mellitus. Arch Ophthalmol 2000;118:912-917.
98. Liu Y, Luo L, He M, et al. Disorders of the blood-aqueous

93
barrier after phacoemulsification in diabetic patients. Eye 2004;18:900-904.
99. Mozzafarieh M, Heinzl H, Sacu S, et al. Clinical outcomes of phacoemulsificatin cataract surgery in diabetes patients visual function (VF-14), visual acuity and patient satisfaction. Acta Ophthalmol Scand 2005;83:176-183.
100.Hong T, AppSci B, Mitchell P, et al. Development and Progression of Diabetic Retinopathy 12 Months after Phacoemulsification Cataract Surgery. Ophthalmology 2009;116:1510-1514.
101. Dowler JC, Hykin PG, Hamilton AM. Phacoemulsification versus extracapsular cataract extraction in patients with diabetes, Ophthalmology 2000;107:457-462.
102. Minassian DC, Rosen P, Dart JK, et al. Extracapsular cataract extraction compared with small incision surgery by phacoemulsification: a randomized trial. Br J Ophthalmol 2001;85:822-829.
103. Antcliff J, Espallargues M, Andersen TF, et al. Phacoemulsification in diabetics. Eye 1997;10:737-741.
104. Squirrel D, Bhola R, Bush J. A prospective, case controlled study of the natural history of diabetic retinopathy and maculopathy after uncomplicated phacoemuslification cataract surgery in patients with type 2 diabetes. Br J Ophthalmol 2002;86:565-571.
105. Romero-Aroca P, Fernández-Ballart J, Almena-Garcia M, et al. Non-proliferative diabetic retinopathy and macular oedema progression after phacoemulsification: Prospective study. J Cataract Refract Surg 2006;32:1438-1444.
106. Liao SB, Ku WC. Progression of diabetic retinopathy after phacoemulsification in diabetic patients: a three-year analysis. Chang Gund Med J 2003;26:829-834.
107. Hauser D, Katz H, Pokroy R, et al. Occurence and progression of diabetic retinopathy after phacoemulsifcation cataract surgery. J Cat Refr Surg 2004;30:428-432.
94
108. Sunderraj P, Villadda JR, Joyce PW, et al. Glare testing in pseudophakes with posterior capsule opacification. Eye 1992;6:411-413.
109. Claesson M, Klarén L, Bechman C, et al. Glare and contrast sensitivity before and after Nd:YAG laser capsulotomy. Acta Ophthalmol Scand 1994;72:27-32.
110. Apple DJ, Solomon KD, Tetz MR, et al. Posterior capsule opacification. Surv Ophthalmol 1992;37:73-116.
111. Apple DJ, Rabb MF. Lens and pathology of intraocular lenses. In: Apple DJ & Rabb MF (eds) Ocular Pathology 1998 Mosby, ST. Louis, Missouri, p.175.
112. Tetz MR, Ries MW, Lucas C. Inhibition of posterior capsule opacificatin by an intraocular-lens-bound sustained drug delivery system: An experimental animal study and literature review. J Cat Refract Surg 1996;22:1070-1078.
113. Tetz MR, Auffart GU, Sperker M, et al. Photographic image analysis system of posterior capsule opacification. J Cataract Refract Surg 1997;23:1515-1520.
114. Hayashi K, Hayashi H, Makao F, et al. In vivo quantitative measurement of posterior capsule opacification after extracapsular cataract surgery. Am J Ophthalmol 1998;125:837-843.
115. Hayashi H, Hayashi K, Nakao F, et al. Anterior capsule contraction and intraocular lens dislocation after implant surgery in eyes with retinitis pigmentosa. Ophthalmology 1998;105:1239-1243.
116. Bath PE, Fankhkauser F. Long-term results of Nd:YAG laser posterios capsulotomy with the Swiss laser. J Cataract Refract Surg 1986;12:150-153.
117. Steinart RF, Puliafito CA, Kumar SR, et al. Cystoid macular edema, retinal detachment, and glaucoma after Nd:YAG laser posterior capsulotomy. Am J Ophthalmol 1991;112:373-380.
118. Koch DD, Liu JF, Gill P, et al. Axial myopia increases the risk of retinal complications after neodymium:YAG laser posterior

95
capsulotomy. Arch Ophthalmol 1989;107:986-990.
119. Rickman-Barger L, Florine CW, Larson RS, et al. Retinal detachment after neodymium:YAG laser posterior capsulotomy. Am J Ophthalmol 1989;107:531-536.
120. Javitt JC, Tielsch JM, Canner JK, et al. National outcomes of cataract extraction. Increased risk of retinal complications associated with Nd:YAG laser capsulotomy. Ophthalmology 1992;99:1487-1498.
121. LiesegangTJ, Bourne WM, Ilstrup DM. Secondary surgical and neodymium:YAG laser discussions. Am J Ophthalmol 1985;100:510-519.
122. Stark WJ, Worthen D, Holladay JT. Neodymium:YAG lasers. An FDA report. Ophthalmology 1985;92:209-212.
123. Joo CK, Kim JH. Effect of neodymium:YAG laser photo disruption on intraocular lenses in vitro. J Cataract Refract Surg 1992;18:562-566.
124. Newland TJ, Auffarth GU, Wesendahl TA, et al. Neodymium:YAG laser damage on silicone intraocular lenses. A comparison of lesions on explanted lenses and experimentally produced lesions. J Cataract Refract Surg 1994;20:527-533.
125. Apple DJ, Peng Q, Visessook N, et al. Surgical prevention of posterior capsule opacification. Part 1: progress in eliminating this complication of cataract surgery. J Cataract Refract Surg 2000;26:180-187.
126. Peng Q, Apple DJ, Visessook N, et al. Surgical prevention of posterior capsule opacification. Part 2: enhancement of cortical cleanup by focusing on hydrodissection. J Cataract Refract Surg 2000;26:188-197.
127. Hollick EJ, Spalton DJ, Meacock W. The effect of capsulorhexis size on posterior capsular opacification: one-year results of a randomized prospective trial. Am J Ophthalmol 1999;128:271-279.
128. Ram J, Apple DJ, Peng Q, et al. Update on fixation of rigid and
96
foldable posterior chamber intraocular lenses. Part II. Choosing the correct haptic fixation and intraocular lens design to help eradicate posterior capsule opacification.
129. Smith SR, Daynes T, Hinckley M, et al. The effect of lens edge design versus anterior capsule overlap on posterior capsule opacification. Am J Ophthalmol 2004;138:521-526.
130. Ayaki M, Ishida Y, Nishimure E, et al. Lens epithelial cell migration between posterior capsule and intraocular lens with variously finished posterior optic edge and two haptic angulations. Ophthalmic Res 2003;35:261-267.
131. Vasavada AR, Dholakia SA, Raj SM, et al. Effect of cortical cleaving hydrodissection on posterior capsule opacification in age-related nuclear cataract. J Cataract Refract Surg 2006;32:1196-1200.
132. Gimble HV, Ferensowicz M, Raanan M, et al. Implantation in children. J Pediatr Ophthalmol Strabismus 1993;30:69-79.
133. BenEzra D, Cohen E. Posterior capsulectomy in pediatric cataract surgery; the necessity of a choice. Ophthalmolgy 1997;104:2168-2174.
134. Plager DA, Lipsky SN, Snyder SK, et al. Capsular management and refractive error in pediatric intraocular lenses. Ophthalmology 1997;104:600-607; discussion by AW Biglan, 607.
135. Vasavada A, Desai J. Primary posterior capsulorhexis with and without anterior vitrectomy in congenital cataracts. J Cataract Refract Surg 1997;23:645-651.
136. Gimble H, Sun R, Ferensowicz M, et al. Intraoperative management of posterior capsule tears in phacoemulsification and intraocular lens implantation. Ophthalmology 2001;108:2186-2189.
137. Menapace R. Routine posterior optic buttonholing for eradication of posterior capsule opacification in adults. J Cataract Refract Surg 2006;32:929-943.
138. Hayashi K, Hayashi K, Nakao F. Posterior capsule
97
opacification after cataract surgery in patients with diabetes mellitus. Am J Ophthalmol 2002;134:10-16.
139. Ebihara Y, Kato S, Oshhika T, et al. Posterior capsule opacification after cataract surgery in patients with diabetes mellitus. J Cataract Refract Surg 2006;32:1184-1187.
140. Zaczek A, Zetterström C. Posterior capsule opacification after phaco-emulsification in patients with diabetes mellitus. J Cataract Refract Surg 1999;25:233-237.
141. Cortina P, Gomez-Lechon M, Navea A, et al. Diclofenac sodium and cyclosporine A inhibit human lens epithelial cells proliferation in culture. Arch Clin Exp Ophthalmol 1997;235:180-185.
142. Nishi O. Incidence of posterior capsule opacification in eyes with and without posterior intraocular lenses. J Cataract Refract Surg 1986;12:519-522.
143. Badr IA, Hussain HM, Jabak M, et al. Extracapsular cataract extraction with or without posterior chamber intraocular lenses in eyes with cataract and high myopia. Ophthalmology 1995;102:1139-1343.
144. Condon PI, Brancato R, Hayes P, et al. Heparin-surface-modified IOLs compared with regular PMMA IOLs in patients with diabetes and/or glaucoma – 1 year results of a double-blind randomized multi-independent trial. Eur J Implant Ref Surg 1995;7:194-201.
145. Winther-Nielsen A, Johansen J, Pedersen GK, et al. Posterior capsule opacification and neodymium:YAG capsulotomy with heparin-surface-modified intraocular lenses. J Cataract Refract Surg 1998:24:949-944.
146. Khan AJ, Percival PB. 12 years results of a prospective trial comparing poly (methyl methacrylate) and poly (hydroxyethyl methacrylate) intraocular lenses. J Cataract Refract Surg 1999;25:1404-1407.
147. Hollick EJ, Spalton DJ, Ursell PG. Surface cytologic features on intraocular lenses. Can increased biocompatibility have disadvantages? Arch Ophthalmol 1999;117:872-878.
98
148. Cumming JS. Postoperative complications and uncorrected acuities after implantation of plate haptic silicone and three-piece silicone intraocular lenses. J Cataract Refract Surg 1993;19:263-273.
149. Mamalis N, Phillips B, Kopp CH, et al. Neodymium:YAG capsulotomy rates after phacoemulsification with silicone posterior chamber intraocular lenses. J Cataract Refract Surg 1996;22(2):1296-1302.
150. Oshika T, Suzuki Y, Kizaki H, et al. Two year clinical study of a soft acrylic intraocular lens. J Cataract Refract Surg 1996;22:104-109.
151. Akahoshi T. 10000 AcrySof Implantations. Proc. ASCRS Symposium on Cataract, IOL and Refractive Surgery, Seattle, USA 1999:Abstr. P 176.
152. Vock L, Menapace R, Stifter E, et al. Posterior capsule opacification and neodymium:YAG laser capsulotomy rates with a round-edged silicone and a sharp-edged hydrophobic acrylic intraocular lens 10 years after surgery. J Cataract Refract Surg 2009;35(3):459-465.
153. Linnola RJ, Holst A. Evaluation of a 3-piece silicone intraocular lens with poly (methyl methacrylate) haptics. J Cataract Refract Surg 1998;24:1509-1514.
154. Apple DJ, Peng Q, Visessook N, et al. Eradication of posterior capsule opacification; documentation of a marked decrease in Nd:YAG laser posterior capsulotomy rates noted in an analysis of 5416 pseudophakic human eyes obtained postmortem. Ophthalmology 2001;108:506-518.
155. Ernest PH. Posterior capsule opacification and neodymium:YAG rates with AcrySof acrylic and PhacoFlex II silicone intraocular lenses. J Cataract Refract Surg 2003;29:1546-1550.
156. Wejde G, Kugelberg M, Zetterström C. Posterior capsule opacification: comparison of 3 intraocular lenses of different materials and design. J Cataract Refract Surg 2003;29:1556-1559.
99
157. Auffarth GU, Brezin A, Caporossi A, et al. Comparison of Nd:YAG capsulotomy rates following phacoemulsification with implantation of PMMA, silicone, or acrylic intra-ocular lenses in four European countries; European OCO Study Group. Ophthalmology 2004;11:319-329.
158. Cleary G, Spalton D, Koch D. Effect of square-edged intraocular lenses on neodymium:YAG laser capsulotomy rates in the United States. J Cataract Refract Surg 2007;33:1899-1906.
159. Alonso J, Espallargues M, Andersen TF, et al. International applicability of the VF-14; an index of visual function in patients with cataracts. Ophthalmology 1997;104:799-807.
160. Camparini C, Cassinari P, Ferrigno L, et al. ETDRS-Fast:implementing psychophysical adaptive methods to standardized visual acuity measurement with ETDRS charts. Invest Ophthalmol Vis Sci 2001;42:1226-1231.
161. Bailey I, Lovie J. New design principles for visual acuity letter charts. Am J Optom Physiol Opt 1976;53:740-745.
162. Ferris F, Sperduto R. Standardized illumination for visual acuity testing in clinical research. Am J Ophthalmol 1982;94:97-98.
163. Diabetic Retinopathy Study. Design, methods and baseline results. Report No.6. A modification of the Airlie House classification of diabetic retinopathy. Prepared by the Diabetic Retinopathy Study. Invest Ophthalmol Vis Sci 1981;21:1-226.
164. Early Treatment Diabetic Retinopathy Study Research Group: Grading diabetic retinopathy from stereoscopic colour fundus photographs: an extension of the modified Airlie House classification. ETDRS Report No. 10. Ophthalmology 1991;98:786-806.
165. Holladay JT, Prager TC. Visual acuity measurements. J Cataract Refract Surg 2004;30(2):287-290.
166. Mönestam E, Wachtmeister. Dissatisfaction with cataract surgery in relation to visual results – a population-based study in Sweden. J Cataract Surg 1999;25:1127-1134.
100
167. Greenberg R, Daniels S, Flanders W, et al. Medical Epidemiology, Fourth Edition. 2005, p. 169-173.
168. Grimes DA, Schulz KF. Bias and causal associations in observational research. Lancet 2002;359(9306):614-618.
169. Brenner MH, Curbow B, Javitt JC, et al. Vision change and quality of life in the elderly; response to cataract surgery and treatment of other chronic ocular conditions. Arch Ophthalmol 1993;11:680-685.
170. Desai P, Reidy A, Minassian DC, et al. Gains from cataract surgery; visual function and quality of life. Br J Ophthalmol 1996;80:868-873.
171. Pesudovs K, Coster DJ. An instrument for assessment of subjective visual disability in cataract patients. Br J Ophthalmol 1998;82:617-624.
172. Lundström M, Roos P, Jensen S, et al. Catquest questionnaire for use in cataract surgery care: Description, validity and reliability. J Cataract Refract Surg 1997;23:1226-1236.
173. Gothwal V, Wright T, Lamoureux E, et al. Using Rasch analysis to revisit the validity of the Cataract TyPE Spec instrument for measuring cataract surgery outcomes. J Cataract Refract Surg 2009;35:1509-1517.
174. Pesudovs K, Garamendi E, Keeves JP, et al. The Activities of Daily Vision Scale for cataract surgery outcomes: re-evaluating validity with Rasch analysis. Invest Ophthalmol Vis Sci 2003;44:2892-2899.
175. Massof RW, Fletcher DC. Evaluation of the NEI visual function questionnaire as an interval measure of visual ability in low vision. Vision Res 2001;41:397-413.
176. Lee JE, Sung JH. Rasch Analysis of the Korean Version of the VF-14:calibration and unidimensionality. International Journal of Methods in Psychiatric Research 2006;10(4):196-203.
177. Wong T, Hyman L. Population-based Studies in Ophthalmology. Am J Ophthalmol 2008;146:656-663.

101
178. Klein R, Klein BE, Moss SE. Glycosylated hemoglobin predicts the incidence and progression of diabetic retinopathy. JAMA 1988;260:2864-2871.
179. Klein R, Klein BE, Tomany SC, et al. The incidence of age-related maculopathy: the Beaver Dam Eye Study. Ophthalmology 2003;110:1273-1280.
180. Mönestam E, Wachtmeister L. Impact of catatact surgery on the visual ability of the very old. Am J Ophthalmol 2004;137(1):145-155.
181. Lundström M, Wendel E. Duration of self-assessed benefit of cataract extraction – a long-term study. Br J Ophthalmol 2005;89:1017-1020.
182. Pollack A, Bukelman A, Zalish M, et al. The course of age-related macular degeneration following bilateral cataract surgery. Ophthalmic Surg Lasers 1998;29:286-294.
183. Armbrecht AM, Findlay C, Kaushal S, et al. Is cataract surgery justified in patients with age related macular degeneration? A visual function and quality of life assessment. Br J Ophthalmol 2000;84:1343-1348.
184. van der Schaft TL, Mooy CM, de Bruijn WC, et al. Increased prevalence of disciform macular degeneration after cataract extraction with implantation of an intraocular lens. Br J Ophthalmol 1994;78:441-445.
185. Klein R, Klein BEK, Wong T, et al. The association of cataract and cataract surgery with the long-term incidence of age-related maculopathy; the Beaver Dam Study. Arch Ophthalmol 2002;120:1551-1558.
186. Mönestam E,Lundqvist B. Long-term results and associations between subjective visual difficulties with car driving and objective visual function 5 years after cataract surgery. J Cataract Refract Surg 2006;32(1):50-55.
187. Gijsbers van Wijk C, Kolk A. Sex differences in physical symptoms; the contribution of symptom perception theory. Soc Sci Med 1997;45:231-246.
102
188. Hibbard JH, Pope CR. Gender roles, illness orientation and use of medical services. Soc Sci Med 1983;17(3):129-137.
189. Menchini U, Cappelli S, Virgili G. Cataract surgery and diabetic retinopathy. Semin Ophthalmol 2003;18:103-108.
190. Pollack A, Dotan S, Oliver M. Progression of diabetic retinopathy after cataract extraction. Br J Ophthalmol 1991;75:547-551.
191. Henricsson M, Heilj A, Janzon L. Diabetic retinopathy before and after cataract surgery. Br J Ophthalmol 1996;80:789-93.
192. Krepler K, Biowski R, Schrey S, et al. Cataract surgery in patients with diabetic retinopathy; visual outcome, progression of diabetic retinopathy: and incidence of diabetic macular oedema. Graefes Arch Clin Exp Ophthalmol 2002;240:735-738.
193. Morgan C, Currie C, Peters J. Relationship between diabetes and mortality. Diabetes Care 2000;23(8):1103-1107.
194. Cusick M, Meleth A, Agrón E, et al. Early Treatment Diabetic Retinopathy Study Research Group. Associations of Mortality and Diabetes Complication in Patients With Type 1 and Type 2 Diabetes. Diabetes Care 2005;28:617-625.
195. Eliasson M, Talbäck M, Rosén M. Improved survival in both men and women with diabetes between 1980 and 2004 – a cohort study in Sweden. Cardiovascular Diabetology 2008;7:32.
196. Fagerholm P, Fitzsimmons T, Harfstrand A, et al. Reactive formation of hyaluronic acid after small and large lens injury. Acta Ophthalmol Scand 1992;70:58-64.
197. Hosai BM, Biglan AW. Risk factors for secondary membrane formation after removal of paediatric cataract. J Cataract Refract Surg 2002;28(2):302-309.
198. Hayashi H, Hayashi K, Nakao F, et al. Quantitative comparison of posterior capsule opacification after polymethylmethacrylate, silicone, and soft acrylic intraocular lens implantation. Arch Ophthalmol 1998;116(12):1579-1582.
103
199. Vock L, Crnej A, Findl O, et al. Posterior Capsule Opacification in Silicone and Hydrophobic Acrylic Intraocular Lenses with Sharp-edge Optics Six Years After Surgery. Am J Ophthalmol 2009;147(4):683-690.
104
APPENDIX
The original questions included in the VF-14 were as follows:
1. Do you have any difficulty, even with glasses, reading small
print, such as tables on medicine bottles, a telephone book,
food tables?
2. Do you have any difficulty, even with glasses, reading a
newspaper or a book?
3. Do you have any difficulty, even with glasses, reading a large
print book or large-print newspaper or numbers on a
telephone?
4. Do you have any difficulty, even with glasses, recognizing
people when they are close to you?
5. Do you have any difficulty, even with glasses, seeing steps,
stairs, or curbs?
6. Do you have any difficulty, even with glasses, reading traffic
signs, street signs, or store signs?
7. Do you have any difficulty, even with glasses, doing fine
handwork like sewing, knitting, crocheting, carpentry?
8. Do you have any difficulty, even with glasses, writing checks or
filling out forms?
9. Do you have any difficulty, even with glasses, playing games
such as bingo, dominos, card games, mah-jong?

105
10. Do you have any difficulty, even with glasses, taking part in
sports like bowling, handball, tennis, golf?
11. Do you have any difficulty, even with glasses, cooking?
12. Do you have any difficulty, even with glasses, watching
television?
Do you currently drive a car? __Yes __No
If the answer is Yes, please answer questions 13 and 14.
13. How much difficulty do you have driving during the day
because of your vision?
14. How much difficulty do you have driving at night because of
your vision?
To questions 1-12, the possible answers are:
__Yes __No __Not applicable
If yes, how much difficulty do you currently have?
A little
A moderate amount
A great deal
Are you unable to do the activity?
To questions 13 and 14, the possible answers are:
No difficulty

106
A little difficulty
A moderate amount of difficulty
A great deal of difficulty
The first page of each questionnaire contained instructions regarding
how to fill out the questionnaires (not shown). The wording of the
questions and answering options of the questionnaires listed above
have been translated into Swedish. The lay-out of the questionnaires
and the print size has been considerably condensed to save space.
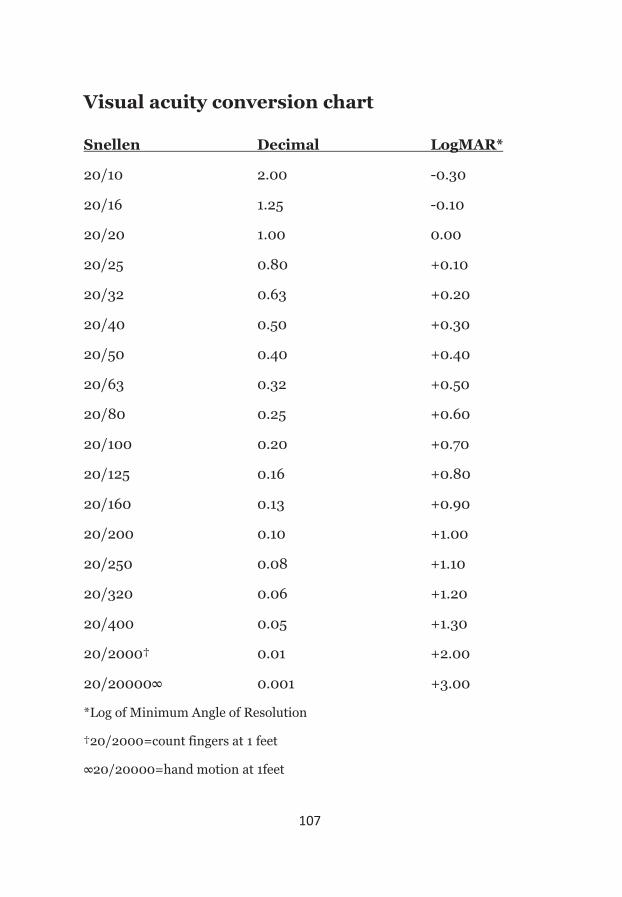
107
Visual acuity conversion chart
Snellen Decimal LogMAR*
20/10 2.00 -0.30
20/16 1.25 -0.10
20/20 1.00 0.00
20/25 0.80 +0.10
20/32 0.63 +0.20
20/40 0.50 +0.30
20/50 0.40 +0.40
20/63 0.32 +0.50
20/80 0.25 +0.60
20/100 0.20 +0.70
20/125 0.16 +0.80
20/160 0.13 +0.90
20/200 0.10 +1.00
20/250 0.08 +1.10
20/320 0.06 +1.20
20/400 0.05 +1.30
20/2000† 0.01 +2.00
20/20000∞ 0.001 +3.00
*Log of Minimum Angle of Resolution
†20/2000=count fingers at 1 feet
∞20/20000=hand motion at 1feet