loss of correction in spinal cord injury-related scoliosis after pedicle screw fixation
TRANSCRIPT

ORIGINAL PAPER
Loss of correction in spinal cord injury-related scoliosisafter pedicle screw fixation
Mina G. Safain & Steven Hwang & Joseph King &
Patrick Cahill & Amer Samdani
Received: 20 August 2013 /Accepted: 29 October 2013# Springer-Verlag Berlin Heidelberg 2013
AbstractPurpose Spinal cord injury (SCI) in the pediatric populationis an infrequent but clinically important disease to scoliosissurgeons. Spinal deformity after SCI is extremely commonand almost uniformly develops in patients being injured be-fore the growth spurt. Most treatment paradigms extrapolatemanagement from both the adult literature as well as adoles-cent idiopathic scoliosis data. Since these patient populationsare different in many respects, we sought out to investigate therates of loss of correction over time as well as the factorsassociated with loss of correction in pediatric patients under-going pedicle screw fixation for treatment of SCI-relatedscoliosis.Methods All consecutive pediatric patients with spinal cordinjury and paralytic scoliosis managed with pedicle screwconstructs were identified at a single institution. Clinical andradiographic parameters were reviewed and analyzed withspecific focus on parameters associated with loss of correctionat an average follow-up of 2 years.Results Approximately 15 % of patients had a loss of correc-tion of greater than 10° of Cobb angle. Postoperative sagittalimbalance was found to be significantly greater in patientswho lost greater than 10° of correction compared to patientswho did not lose correction (53.6±39.9 vs 4.3±41.3 mm, p =0.02).Conclusions Correction of patients with paralytic associatedscoliosis should aim for a neutral sagittal balance in order to
prevent postoperative loss of correction. Further study isneeded on this subgroup of patients with scoliosis given thedifferences in strategies needed to correct and maintain theirdeformity correction.
Keywords Spinal cord injury . Scoliosis . Pedicle screw .
Paralytic scoliosis . Loss of correction
Introduction
Spinal cord injury (SCI) in children is a rare but clinicallyimportant injury accounting for approximately 2,000 casesannually in the USA [5]. Two distinct mechanisms of injurypredominate in the pediatric population: motor vehicle acci-dents affecting younger children and sports activities in ado-lescents [4]. Roughly 33 % of children with cervical spineinjuries have clinical signs of SCI [4, 10] and can suffer fromdevastating outcomes due to neurologic deficit. The majorityof these children suffer from an incomplete neurologic injuryand their prognosis is typically better than adults [7]. There-fore, appropriate management is imperative to provide themmaximal function in their adult lives [23].
A relatively unique management issue in this population isthe development of spinal deformity after SCI. Multiple stud-ies have determined that scoliosis after SCI in children isextremely common [6, 13, 15, 18], especially if the neurolog-ical insult occurs at a younger age. Several studies have shownthat scoliosis develops more frequently in children less than12 than in adults [2] and that children being injured before thegrowth spurt almost uniformly develop scoliosis compared topatients who have an injury after their growth spurt [6]. In thispatient population, brace management should be initiated assoon as a spinal deformity is identified and even initiatingbracing on curves less than 10° may prevent future spinalfusion [16].
M. G. Safain : S. Hwang (*)Department of Neurosurgery, Tufts Medical Center and FloatingHospital for Children, 800 Washington St, Box #178, Boston,MA 02111, USAe-mail: [email protected]
J. King : P. Cahill :A. SamdaniDepartment of Orthopedic Surgery, Spine Service, Shriner’s Hospitalfor Children, Philadelphia, PA, USA
Childs Nerv SystDOI 10.1007/s00381-013-2316-0

However, even with bracing, many children progress andrequire deformity correction. The benefit of instrumentedfusion as well as the instrumentation type remains controver-sial [17]. With the increased popularity of thoracic pediclescrews for adolescent idiopathic scoliosis (AIS), similar con-structs are being used to correct neuromuscular scoliosis.However, deformity correction in AIS, even using pediclescrews, has been associated with a loss of correction over time[9]. It remains unclear if neuromuscular patients are also atrisk of loss of correction and what impact this may have onthem.
Most series of neuromuscular scoliosis tend to combineSCI-associated scoliosis with other syndromic causes includ-ing cerebral palsy-associated scoliosis and therefore may nottruly reflect outcomes from paralytic scoliosis. Patients withSCI-related scoliosis may have greater cognitive as well asphysical function and may represent a distinct subgroup ofpatients. Given that these patient populations are different inmany respects, we sought out to investigate the rates of loss ofcorrection over time as well as factors associated with loss ofcorrection in pediatric patients undergoing pedicle screw fix-ation for correction of SCI-related scoliosis.
Methods
Local IRB approval was obtained from our institution. Med-ical records and radiographs were retrospectively reviewedfrom a single institution, Shriner's Hospital for Children Phil-adelphia, from November 2004 to February 2011. All consec-utive pediatric patients (<18 years of age) with spinal cordinjury and paralytic scoliosis were identified. Only patientshaving had a deformity correction surgery at our institutionusing pedicle screw constructs (>80% screws) were included.All patients were then stratified into two groups defined byeither (1) loss of correction in cobb angle of greater than 10° atlast patient follow-up (group A) or (2) less than 10° in loss ofcorrection at last patient follow-up (group B) (Fig. 1).
Clinical and radiographic measurements were recorded.Data fields collected included age, gender, weight, neurolog-ical level of injury, functional parameters, age at injury, etiol-ogy of injury, curve pattern, years between injury and surgery,and radiographic parameters. Thoracic kyphosis was mea-sured from T2 to T12 unless the kyphosis extended beyondT12 with loss of lumbar lordosis; the kyphosis was thenmeasured from the appropriate lumbar level to obtainmaximalvalues of kyphosis. Thoraco-lumbar kyphosis was measuredfrom T10 to L2 and lumbar lordosis was obtained from L1 toS1. Sagittal balance wasmeasured as a distance (in millimeter)between a vertical line dissecting the posterior edge of thesacrum and a plumb line from the centroid of C7 (Fig. 2). Thecoronal balance was inferred from the distance (in millimeter)between the central sacral vertical line and a line from the
centroid of C7 (Fig. 2). Pelvic obliquity was calculated bymeasuring the angle subtended between the line tangential toboth iliac crests and the horizontal. Shoulder balance wasinferred by measuring the clavicle angle as reported by Kukloet al. [12]. Radiographs were obtained standing if the patientwas ambulatory, but otherwise were sitting.
Statistical analysis was performed using SPSS 12.0.2®software using Student's t tests, Chi square tests, and Fisher'sexact tests when appropriate. All results were reported asmeans and standard deviation. A p value of 0.05 was consid-ered statistically significant.
Results
A total of 37 pediatric patients with spinal cord injury andparalytic scoliosis underwent surgical management of theirscoliosis using pedicle screw constructs (>80 % screws) dur-ing the study period time. Three of these patients did not havefollow-up radiographic data and therefore loss of correctiondata was unavailable. Our results show data for the totalcohort (37) patients when possible and on the remaining 34patients when data for the three patients lost to follow-up areunavailable. These patients were then stratified into twogroups defined by either (1) loss of correction in cobb angleof greater than 10° at last patient follow-up (group A) or (2)less than 10° in loss of correction at last patient follow-up(group B). Overall, five patients had a loss of correctiongreater than 10° equating to 14.7 % (5/34 patients) of the caseseries.
There were no differences between groups A or B in regardto demographic parameters (Table 1). The average age atinjury of the full cohort was 6.5±4.9 years and the averageage at surgery was 14.9±3.3 years. There were slightly moremales (21) in the full cohort but this did not reach statisticalsignificance. Most injuries occurred in the cervical and tho-racic levels (41.2 and 55.9 % of the total cohort, respectively).The cause of injury in this cohort was mostly traumatic butother causes of injury including iatrogenic injury, infectious,or inflammatory conditions were included in this cohort. Pre-injury scoliosis status was unknown in the majority of cases.The average follow-up time for the full cohort was 23.5±19.4 months with a range of 1–79 months.
Preoperative radiographic measurements were obtained asdetailed in the methods section (Table 2). There were nodifferences between groups A or B in regard to preoperativeradiographic measurements. The average preoperative Cobbangle of the full cohort was 65.5±25.7°. The average preop-erative thoracic kyphosis of the full cohort was 39.4±19.2°.The average preoperative sagittal balance of the full cohortwas 13.2±61.7 mm. The average preoperative coronal bal-ance of the full cohort was 3.5±33.4 mm. In addition, therewere no statistically significant differences between the full
Childs Nerv Syst
cohort, group A, or group B in terms of lumbar lordosis,thoraco-lumbar kyphosis, or pelvic obliquity (Table 2).
Intraoperative parameters are provided of the full cohort,and groups A or B (Table 3). Most rostral instrumentationextended to the T2 level. The most distal instrumented levelwas to the pelvis. There was no difference between the groupsin the number of levels instrumented or the number ofosteotomies performed. Allograft, autograft, and bone mor-phogenic protein (BMP) were used to accomplish fusion at thesurgeon's preference. The type of graft used did not differbetween the groups.
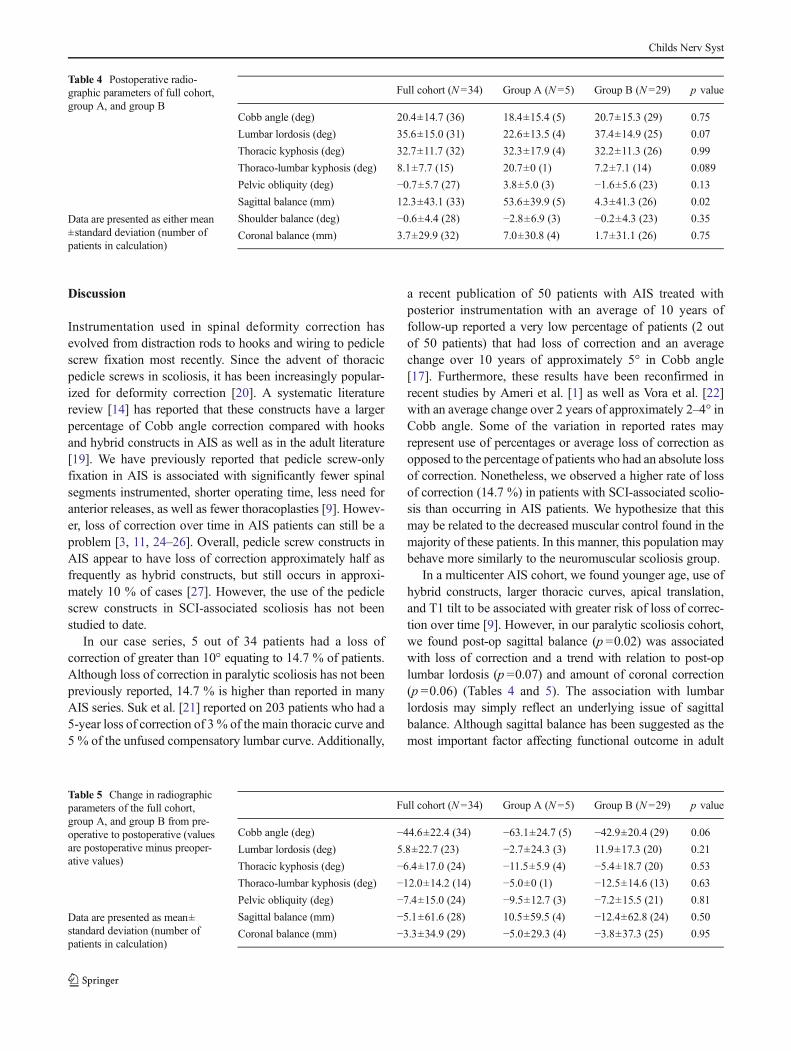
Postoperative radiographic measurements were simi-larly obtained as detailed in the methods section(Table 4). Postoperative sagittal balance was found tobe significantly different between groups A and B.Group A had a significantly higher sagittal balance thangroup B (53.6 ±39.9 vs 4.3 ± 41.3 mm, p =0.02).
Postoperative lumbar lordosis approached significancewith group A trending to have a lower lumbar lordosisthan group B (22.6±13.5° vs 37.4±14.9°, p =0.07). Allother postoperative radiographic measurements showedno significant difference including Cobb angle, thoracickyphosis, thoraco-lumbar kyphosis, pelvic obliquity,shoulder balance, and coronal balance.
The change in radiographic parameters of the full co-hort, group A, and group B are shown (Table 5). Allvalues were calculated with preoperative values beingsubtracted from postoperative values. Change in Cobbangle trended toward significance between groups A andB (−63.1±24.7° vs −42.9±20.4°, p =0.06). All otherchanges between postoperative and preoperative measure-ments showed no significant difference including lumbarlordosis, thoracic kyphosis, thoraco-lumbar kyphosis, pel-vic obliquity, sagittal balance, or coronal balance.
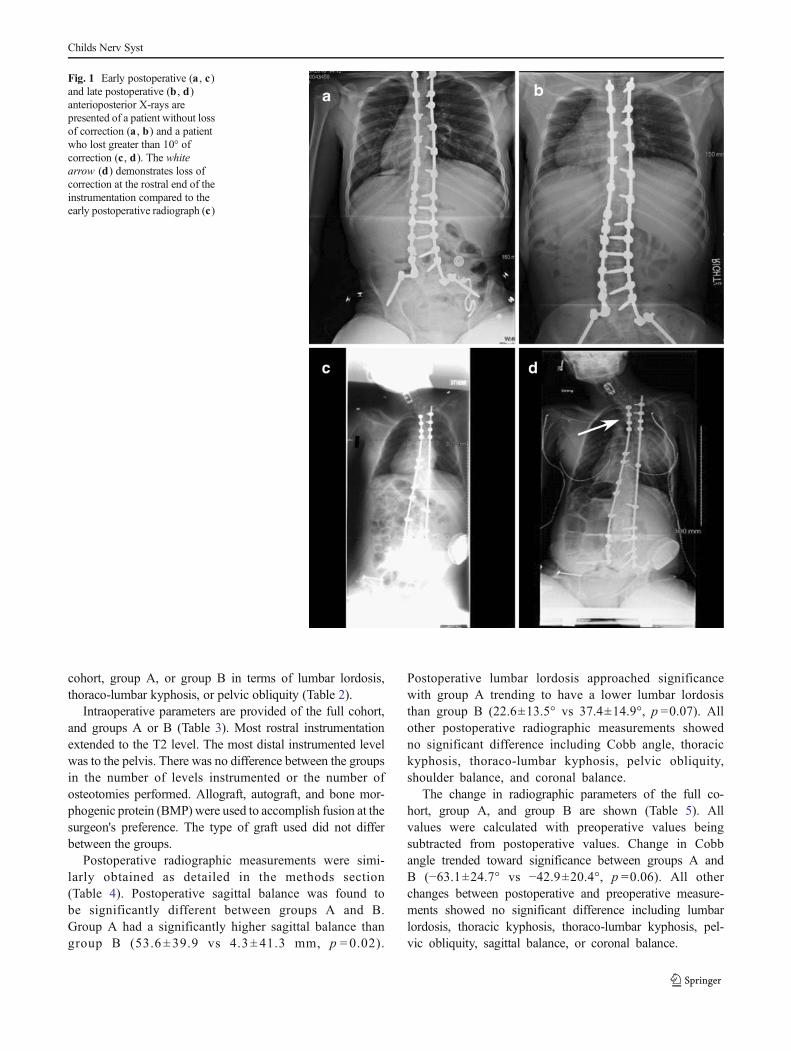
Fig. 1 Early postoperative (a , c)and late postoperative (b , d)anterioposterior X-rays arepresented of a patient without lossof correction (a , b) and a patientwho lost greater than 10° ofcorrection (c , d). The whitearrow (d) demonstrates loss ofcorrection at the rostral end of theinstrumentation compared to theearly postoperative radiograph (c)
Childs Nerv Syst
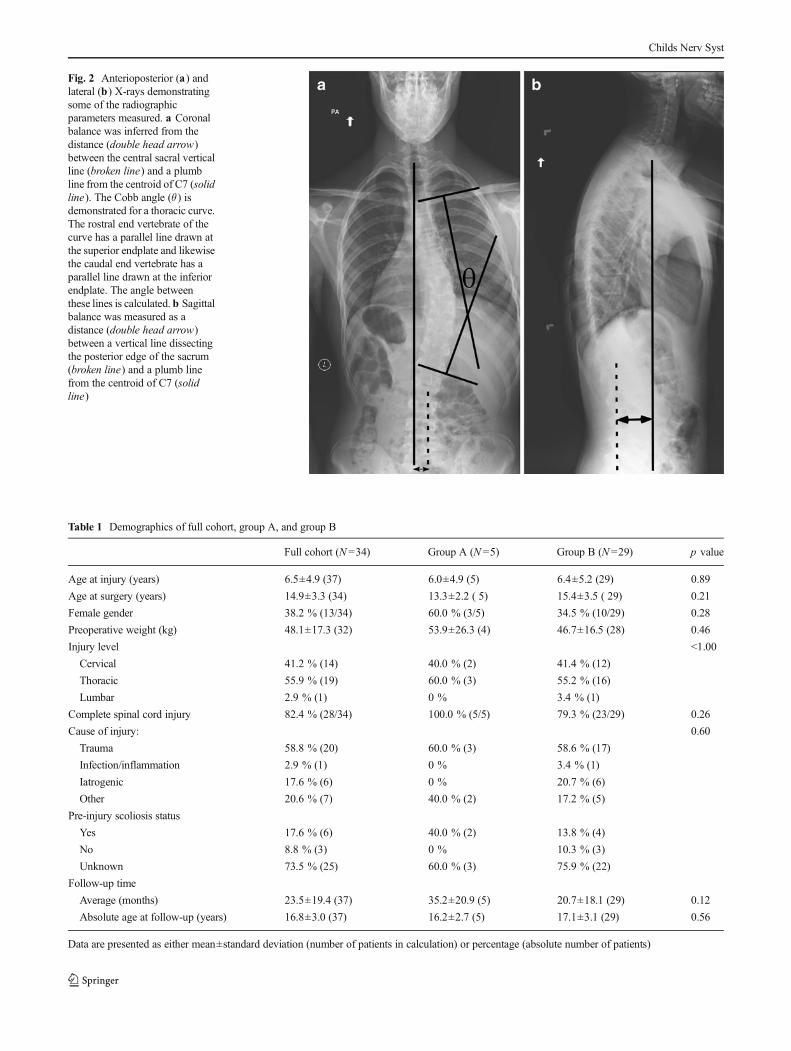
Fig. 2 Anterioposterior (a) andlateral (b) X-rays demonstratingsome of the radiographicparameters measured. a Coronalbalance was inferred from thedistance (double head arrow)between the central sacral verticalline (broken line) and a plumbline from the centroid of C7 (solidline). The Cobb angle (θ) isdemonstrated for a thoracic curve.The rostral end vertebrate of thecurve has a parallel line drawn atthe superior endplate and likewisethe caudal end vertebrate has aparallel line drawn at the inferiorendplate. The angle betweenthese lines is calculated. b Sagittalbalance was measured as adistance (double head arrow)between a vertical line dissectingthe posterior edge of the sacrum(broken line) and a plumb linefrom the centroid of C7 (solidline)
Table 1 Demographics of full cohort, group A, and group B
Full cohort (N=34) Group A (N =5) Group B (N =29) p value
Age at injury (years) 6.5±4.9 (37) 6.0±4.9 (5) 6.4±5.2 (29) 0.89
Age at surgery (years) 14.9±3.3 (34) 13.3±2.2 ( 5) 15.4±3.5 ( 29) 0.21
Female gender 38.2 % (13/34) 60.0 % (3/5) 34.5 % (10/29) 0.28
Preoperative weight (kg) 48.1±17.3 (32) 53.9±26.3 (4) 46.7±16.5 (28) 0.46
Injury level <1.00
Cervical 41.2 % (14) 40.0 % (2) 41.4 % (12)
Thoracic 55.9 % (19) 60.0 % (3) 55.2 % (16)
Lumbar 2.9 % (1) 0 % 3.4 % (1)
Complete spinal cord injury 82.4 % (28/34) 100.0 % (5/5) 79.3 % (23/29) 0.26
Cause of injury: 0.60
Trauma 58.8 % (20) 60.0 % (3) 58.6 % (17)
Infection/inflammation 2.9 % (1) 0 % 3.4 % (1)
Iatrogenic 17.6 % (6) 0 % 20.7 % (6)
Other 20.6 % (7) 40.0 % (2) 17.2 % (5)
Pre-injury scoliosis status
Yes 17.6 % (6) 40.0 % (2) 13.8 % (4)
No 8.8 % (3) 0 % 10.3 % (3)
Unknown 73.5 % (25) 60.0 % (3) 75.9 % (22)
Follow-up time
Average (months) 23.5±19.4 (37) 35.2±20.9 (5) 20.7±18.1 (29) 0.12
Absolute age at follow-up (years) 16.8±3.0 (37) 16.2±2.7 (5) 17.1±3.1 (29) 0.56
Data are presented as either mean±standard deviation (number of patients in calculation) or percentage (absolute number of patients)
Childs Nerv Syst
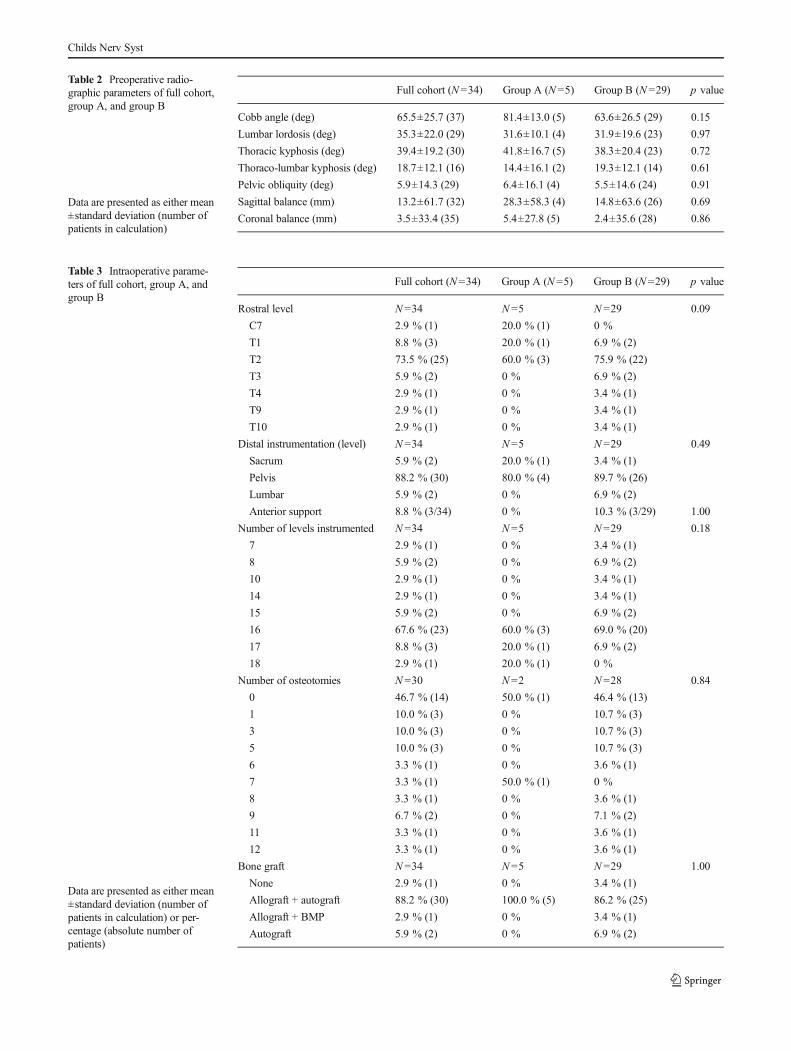
Table 2 Preoperative radio-graphic parameters of full cohort,group A, and group B
Data are presented as either mean±standard deviation (number ofpatients in calculation)
Full cohort (N =34) Group A (N =5) Group B (N=29) p value
Cobb angle (deg) 65.5±25.7 (37) 81.4±13.0 (5) 63.6±26.5 (29) 0.15
Lumbar lordosis (deg) 35.3±22.0 (29) 31.6±10.1 (4) 31.9±19.6 (23) 0.97
Thoracic kyphosis (deg) 39.4±19.2 (30) 41.8±16.7 (5) 38.3±20.4 (23) 0.72
Thoraco-lumbar kyphosis (deg) 18.7±12.1 (16) 14.4±16.1 (2) 19.3±12.1 (14) 0.61
Pelvic obliquity (deg) 5.9±14.3 (29) 6.4±16.1 (4) 5.5±14.6 (24) 0.91
Sagittal balance (mm) 13.2±61.7 (32) 28.3±58.3 (4) 14.8±63.6 (26) 0.69
Coronal balance (mm) 3.5±33.4 (35) 5.4±27.8 (5) 2.4±35.6 (28) 0.86
Table 3 Intraoperative parame-ters of full cohort, group A, andgroup B
Data are presented as either mean±standard deviation (number ofpatients in calculation) or per-centage (absolute number ofpatients)
Full cohort (N=34) Group A (N =5) Group B (N =29) p value
Rostral level N =34 N=5 N =29 0.09
C7 2.9 % (1) 20.0 % (1) 0 %
T1 8.8 % (3) 20.0 % (1) 6.9 % (2)
T2 73.5 % (25) 60.0 % (3) 75.9 % (22)
T3 5.9 % (2) 0 % 6.9 % (2)
T4 2.9 % (1) 0 % 3.4 % (1)
T9 2.9 % (1) 0 % 3.4 % (1)
T10 2.9 % (1) 0 % 3.4 % (1)
Distal instrumentation (level) N =34 N=5 N =29 0.49
Sacrum 5.9 % (2) 20.0 % (1) 3.4 % (1)
Pelvis 88.2 % (30) 80.0 % (4) 89.7 % (26)
Lumbar 5.9 % (2) 0 % 6.9 % (2)
Anterior support 8.8 % (3/34) 0 % 10.3 % (3/29) 1.00
Number of levels instrumented N =34 N=5 N =29 0.18
7 2.9 % (1) 0 % 3.4 % (1)
8 5.9 % (2) 0 % 6.9 % (2)
10 2.9 % (1) 0 % 3.4 % (1)
14 2.9 % (1) 0 % 3.4 % (1)
15 5.9 % (2) 0 % 6.9 % (2)
16 67.6 % (23) 60.0 % (3) 69.0 % (20)
17 8.8 % (3) 20.0 % (1) 6.9 % (2)
18 2.9 % (1) 20.0 % (1) 0 %
Number of osteotomies N =30 N=2 N =28 0.84
0 46.7 % (14) 50.0 % (1) 46.4 % (13)
1 10.0 % (3) 0 % 10.7 % (3)
3 10.0 % (3) 0 % 10.7 % (3)
5 10.0 % (3) 0 % 10.7 % (3)
6 3.3 % (1) 0 % 3.6 % (1)
7 3.3 % (1) 50.0 % (1) 0 %
8 3.3 % (1) 0 % 3.6 % (1)
9 6.7 % (2) 0 % 7.1 % (2)
11 3.3 % (1) 0 % 3.6 % (1)
12 3.3 % (1) 0 % 3.6 % (1)
Bone graft N =34 N=5 N =29 1.00
None 2.9 % (1) 0 % 3.4 % (1)
Allograft + autograft 88.2 % (30) 100.0 % (5) 86.2 % (25)
Allograft + BMP 2.9 % (1) 0 % 3.4 % (1)
Autograft 5.9 % (2) 0 % 6.9 % (2)
Childs Nerv Syst
Discussion
Instrumentation used in spinal deformity correction hasevolved from distraction rods to hooks and wiring to pediclescrew fixation most recently. Since the advent of thoracicpedicle screws in scoliosis, it has been increasingly popular-ized for deformity correction [20]. A systematic literaturereview [14] has reported that these constructs have a largerpercentage of Cobb angle correction compared with hooksand hybrid constructs in AIS as well as in the adult literature[19]. We have previously reported that pedicle screw-onlyfixation in AIS is associated with significantly fewer spinalsegments instrumented, shorter operating time, less need foranterior releases, as well as fewer thoracoplasties [9]. Howev-er, loss of correction over time in AIS patients can still be aproblem [3, 11, 24–26]. Overall, pedicle screw constructs inAIS appear to have loss of correction approximately half asfrequently as hybrid constructs, but still occurs in approxi-mately 10 % of cases [27]. However, the use of the pediclescrew constructs in SCI-associated scoliosis has not beenstudied to date.
In our case series, 5 out of 34 patients had a loss ofcorrection of greater than 10° equating to 14.7 % of patients.Although loss of correction in paralytic scoliosis has not beenpreviously reported, 14.7 % is higher than reported in manyAIS series. Suk et al. [21] reported on 203 patients who had a5-year loss of correction of 3 % of the main thoracic curve and5 % of the unfused compensatory lumbar curve. Additionally,
a recent publication of 50 patients with AIS treated withposterior instrumentation with an average of 10 years offollow-up reported a very low percentage of patients (2 outof 50 patients) that had loss of correction and an averagechange over 10 years of approximately 5° in Cobb angle[17]. Furthermore, these results have been reconfirmed inrecent studies by Ameri et al. [1] as well as Vora et al. [22]with an average change over 2 years of approximately 2–4° inCobb angle. Some of the variation in reported rates mayrepresent use of percentages or average loss of correction asopposed to the percentage of patients who had an absolute lossof correction. Nonetheless, we observed a higher rate of lossof correction (14.7 %) in patients with SCI-associated scolio-sis than occurring in AIS patients. We hypothesize that thismay be related to the decreased muscular control found in themajority of these patients. In this manner, this population maybehave more similarly to the neuromuscular scoliosis group.
In a multicenter AIS cohort, we found younger age, use ofhybrid constructs, larger thoracic curves, apical translation,and T1 tilt to be associated with greater risk of loss of correc-tion over time [9]. However, in our paralytic scoliosis cohort,we found post-op sagittal balance (p =0.02) was associatedwith loss of correction and a trend with relation to post-oplumbar lordosis (p =0.07) and amount of coronal correction(p =0.06) (Tables 4 and 5). The association with lumbarlordosis may simply reflect an underlying issue of sagittalbalance. Although sagittal balance has been suggested as themost important factor affecting functional outcome in adult
Table 4 Postoperative radio-graphic parameters of full cohort,group A, and group B
Data are presented as either mean±standard deviation (number ofpatients in calculation)
Full cohort (N =34) Group A (N =5) Group B (N=29) p value
Cobb angle (deg) 20.4±14.7 (36) 18.4±15.4 (5) 20.7±15.3 (29) 0.75
Lumbar lordosis (deg) 35.6±15.0 (31) 22.6±13.5 (4) 37.4±14.9 (25) 0.07
Thoracic kyphosis (deg) 32.7±11.7 (32) 32.3±17.9 (4) 32.2±11.3 (26) 0.99
Thoraco-lumbar kyphosis (deg) 8.1±7.7 (15) 20.7±0 (1) 7.2±7.1 (14) 0.089
Pelvic obliquity (deg) −0.7±5.7 (27) 3.8±5.0 (3) −1.6±5.6 (23) 0.13
Sagittal balance (mm) 12.3±43.1 (33) 53.6±39.9 (5) 4.3±41.3 (26) 0.02
Shoulder balance (deg) −0.6±4.4 (28) −2.8±6.9 (3) −0.2±4.3 (23) 0.35
Coronal balance (mm) 3.7±29.9 (32) 7.0±30.8 (4) 1.7±31.1 (26) 0.75
Table 5 Change in radiographicparameters of the full cohort,group A, and group B from pre-operative to postoperative (valuesare postoperative minus preoper-ative values)
Data are presented as mean±standard deviation (number ofpatients in calculation)
Full cohort (N =34) Group A (N =5) Group B (N=29) p value
Cobb angle (deg) −44.6±22.4 (34) −63.1±24.7 (5) −42.9±20.4 (29) 0.06
Lumbar lordosis (deg) 5.8±22.7 (23) −2.7±24.3 (3) 11.9±17.3 (20) 0.21
Thoracic kyphosis (deg) −6.4±17.0 (24) −11.5±5.9 (4) −5.4±18.7 (20) 0.53
Thoraco-lumbar kyphosis (deg) −12.0±14.2 (14) −5.0±0 (1) −12.5±14.6 (13) 0.63
Pelvic obliquity (deg) −7.4±15.0 (24) −9.5±12.7 (3) −7.2±15.5 (21) 0.81
Sagittal balance (mm) −5.1±61.6 (28) 10.5±59.5 (4) −12.4±62.8 (24) 0.50
Coronal balance (mm) −3.3±34.9 (29) −5.0±29.3 (4) −3.8±37.3 (25) 0.95
Childs Nerv Syst

deformity [8], its impact in paralytic scoliosis has not beenwell described. It is possible that a significant sagittal imbal-ance may cause continued strain on the instrumentation orlead to occult pseudarthrosis that could account for loss ofcorrection over time. Our mean sagittal imbalance of 53.6±39.9mm does exceed the 50mm correlated by Glassman et al.[8] with pain and poor functional status in adult deformity. It isunlikely that sagittal imbalance would have as much of aclinical impact in our cohort as many patients are non-ambulatory, but sagittal imbalance may contribute to unduestress on the construct leading to loss of correction as seen inour cohort.
We also noted that a greater correction of the coronalcurvature had a trend towards increased risk of loss of correc-tion (Table 5). Use of pedicle screws in AIS has been associ-ated with greater correction of the coronal curvature [14];however, coronal balance is likely more important than per-cent correction in our cohort. Although not statistically signif-icant, our group A had slightly greater coronal imbalance (7.0±30.8 mm) than group B (1.7±31.1 mm). Our small numberswith wide standard deviations may prevent us from identify-ing significant variables in this series, but correction of coro-nal curvature may be an indirect marker of this parameter.
Our series is clearly limited by its retrospective nature andrelatively small sample size. However, some of this arisessecondary to the infrequent nature of pediatric SCI-relatedscoliosis. The wide range within standard deviations also isa reflection of the small sample size and variability within thecohort.
Overall, we found that patients who had a loss of correctionof scoliosis were more likely to have greater post-op sagittalimbalance. This would suggest that surgeons dealing with thispatient population should be mindful of the sagittal balance.Ideally, correction should aim for a neutral sagittal balance inorder to prevent post-op loss of correction in paralyticscoliosis.
Conclusion
We present a case series of patients with paralytic scoliosis andsuggest that postoperative loss of correction occurs approxi-mately in 15 % of children and is associated with a largersagittal postoperative imbalance. Further study is needed onthis subgroup of scoliosis given the differences in strategiesneeded to correct and maintain their deformity correction.
Conflict of interest The authors report no conflict of interestconcerning the materials or methods used in this study or the findingsspecified in this paper. This manuscript has not been previously publishedin whole or in part or submitted elsewhere for review.
References
1. Ameri E, Behtash H, Mobini B, Omidi-Kashani F, Momeni B (2008)Radiographic outcome of surgical treatment of adolescent idiopathicscoliosis in males versus females. Scoliosis 3:12. doi:10.1186/1748-7161-3-12
2. Apple DF Jr, Anson CA, Hunter JD, Bell RB (1995) Spinal cordinjury in youth. Clinical pediatrics 34(2):90–95
3. Ayvaz M, Olgun ZD, Demirkiran HG, Alanay A, Yazici M (2012)Posterior all-pedicle screw instrumentation combined with multiplechevron and concave rib osteotomies in the treatment of adolescentcongenital kyphoscoliosis. The spine journal. doi:10.1016/j.spinee.2012.10.016
4. Brown RL, Brunn MA, Garcia VF (2001) Cervical spine injuries inchildren: a review of 103 patients treated consecutively at a level 1pediatric trauma center. Journal of pediatric surgery 36(8):1107–1114. doi:10.1053/jpsu.2001.25665
5. Collopy KT, Kivlehan SM, Snyder SR (2012) Pediatric spinal cordinjuries: anatomical differences bring different challenges with kids.EMS world 41(8):52–57
6. Dearolf WW 3rd, Betz RR, Vogel LC, Levin J, Clancy M, Steel HH(1990) Scoliosis in pediatric spinal cord-injured patients. J PediatrOrthop 10(2):214–218
7. Dickman CA, Zabramski JM, Hadley MN, Rekate HL, Sonntag VK(1991) Pediatric spinal cord injury without radiographic abnormali-ties: report of 26 cases and review of the literature. J Spinal Disord4(3):296–305
8. Glassman SD, Bridwell K, Dimar JR, HortonW, Berven S, Schwab F(2005) The impact of positive sagittal balance in adult spinal defor-mity. Spine 30(18):2024–2029
9. Hwang SW, Samdani AF, Wormser B, Amin H, Kimball JS, AmesRJ, Rothkrug AS, Cahill PJ (2012) Comparison of 5-year outcomesbetween pedicle screw and hybrid constructs in adolescent idiopathicscoliosis. J Neurosurg Spine 17(3):212–219. doi:10.3171/2012.6.SPINE1215
10. Kewalramani LS, Kraus JF, Sterling HM (1980) Acute spinal-cordlesions in a pediatric population: epidemiological and clinical fea-tures. Paraplegia 18(3):206–219. doi:10.1038/sc.1980.36
11. Kim YJ, Lenke LG, Kim J, Bridwell KH, Cho SK, Cheh G,Sides B (2006) Comparative analysis of pedicle screw versushybrid instrumentation in posterior spinal fusion of adolescentidiopathic scoliosis. Spine 31(3):291–298. doi:10.1097/01.brs.0000197865.20803.d4
12. Kuklo TR, Lenke LG, Graham EJ, Won DS, Sweet FA, Blanke KM,Bridwell KH (2002) Correlation of radiographic, clinical, and patientassessment of shoulder balance following fusion versus nonfusion ofthe proximal thoracic curve in adolescent idiopathic scoliosis. Spine27(18):2013–2020
13. Lancourt JE, Dickson JH, Carter RE (1981) Paralytic spinal defor-mity following traumatic spinal-cord injury in children and adoles-cents. J Bone Joint Surg (Am Vol) 63(1):47–53
14. Ledonio CG, Polly DW Jr, Vitale MG, Wang Q, Richards BS (2011)Pediatric pedicle screws: comparative effectiveness and safety: asystematic literature review from the Scoliosis Research Societyand the Pediatric Orthopaedic Society of North America task force.J Bone Joint Surg (Am Vol) 93(13):1227–1234. doi:10.2106/JBJS.J.00678
15. Mayfield JK, Erkkila JC, Winter RB (1981) Spine deformity subse-quent to acquired childhood spinal cord injury. J Bone Joint Surg(Am Vol) 63(9):1401–1411
16. Mehta S, Betz RR,MulcaheyMJ,McDonald C, Vogel LC, AndersonC (2004) Effect of bracing on paralytic scoliosis secondary to spinalcord injury. J Spinal Cord Med 27(Suppl 1):S88–S92
17. Mueller FJ, Gluch H (2009) Adolescent idiopathic scoliosis (AIS)treated with arthrodesis and posterior titanium instrumentation: 8 to
Childs Nerv Syst

12 years follow upwithout late infection. Scoliosis 4:16. doi:10.1186/1748-7161-4-16
18. Parisini P, Di Silvestre M, Greggi T (2002) Treatment of spinalfractures in children and adolescents: long-term results in 44 patients.Spine 27(18):1989–1994
19. Rose PS, Lenke LG, Bridwell KH, Mulconrey DS, Cronen GA,Buchowski JM, Schwend RM, Sides BA (2009) Pedicle screwinstrumentation for adult idiopathic scoliosis: an improvement overhook/hybrid fixation. Spine 34(8):852–857. doi:10.1097/BRS.0b013e31818e5962, discussion 858
20. Suk SI, Lee CK, Kim WJ, Chung YJ, Park YB (1995) Segmentalpedicle screw fixation in the treatment of thoracic idiopathic scoliosis.Spine 20(12):1399–1405
21. Suk SI, Lee SM, Chung ER, Kim JH, Kim SS (2005) Selectivethoracic fusion with segmental pedicle screw fixation in the treatmentof thoracic idiopathic scoliosis: more than 5-year follow-up. Spine30(14):1602–1609
22. Vora V, Crawford A, Babekhir N, Boachie-Adjei O, Lenke L, PeskinM, Charles G, Kim Y (2007) A pedicle screw construct gives anenhanced posterior correction of adolescent idiopathic scoliosis whencompared with other constructs: myth or reality. Spine 32(17):1869–1874. doi:10.1097/BRS.0b013e318108b912
23. Wang MY, Hoh DJ, Leary SP, Griffith P, McComb JG (2004)High rates of neurological improvement following severe trau-matic pediatric spinal cord injury. Spine 29(13):1493–1497,discussion E1266
24. Yang C,Wei X, Zhang J,Wu D, Zhao Y,Wang C, Zhu X, He S, Li M(2012) All-pedicle-screw versus hybrid hook-screw instrumentationfor posterior spinal correction surgery in adolescent idiopathic scoli-osis: a curve flexibility matched-pair study. Arch Orthop TraumaSurg 132(5):633–639. doi:10.1007/s00402-011-1454-7
25. Yilmaz G, Borkhuu B, Dhawale AA, Oto M, Littleton AG, MasonDE, Gabos PG, Shah SA (2012) Comparative analysis of hook,hybrid, and pedicle screw instrumentation in the posterior treatmentof adolescent idiopathic scoliosis. J Pediatr Orthop 32(5):490–499.doi:10.1097/BPO.0b013e318250c629
26. Yu CH, Chen PQ, Ma SC, Pan CH (2012) Segmental correction ofadolescent idiopathic scoliosis by all-screw fixation method in ado-lescents and young adults. Minimum 5 years follow-up with SF-36questionnaire. Scoliosis 7:5
27. Hwang SW, Samdani AF, Stanton P, Marks MC, Bastrom T, NewtonPO, Betz RR, Cahill PJ (2013) Impact of pedicle screw fixation onloss of deformity correction in patients with adolescent idiopathicscoliosis. J Pediatr Orthop 33:377–382
Childs Nerv Syst