lower back pain: management and prevention jon rowe, bkin, cep
TRANSCRIPT
Lower Back Pain: Management and Prevention
Jon Rowe, Bkin, CEP
Objectives
• Review specific anatomy in relation to the lower back (lumbar spine)
• Touch on a few spinal injuries and mechanisms of injury
• How to determine some causes of lower back pain (LBP)
• Action after identifying cause of LBP• Management and Prevention

Sources
• McGill, Stuart; Lower Back Disorders, 2nd edition
• McGill, Stuart; Ultimate Back Fitness and Performance, 4th edition

Anatomy of the Lumbar SpineHighly vascular, with the exception of the disk – only they remain avascular
Circular vertebral body,
filled with cancellous bone
Pedicle attaches body
to posterior elements
“Neural Arch” is composed of
laminae and pedicles;
transverse processes
and spinous process
attach to neural arch
Neural arch is relatively flexible
while body is more rigid
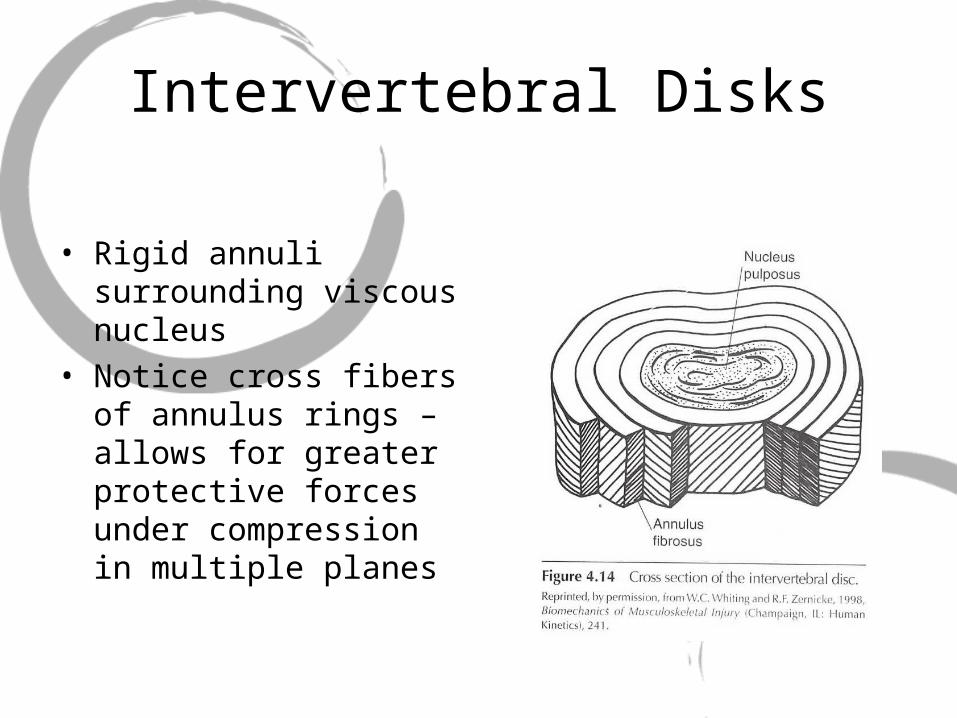
Intervertebral Disks
• Rigid annuli surrounding viscous nucleus
• Notice cross fibers of annulus rings – allows for greater protective forces under compression in multiple planes
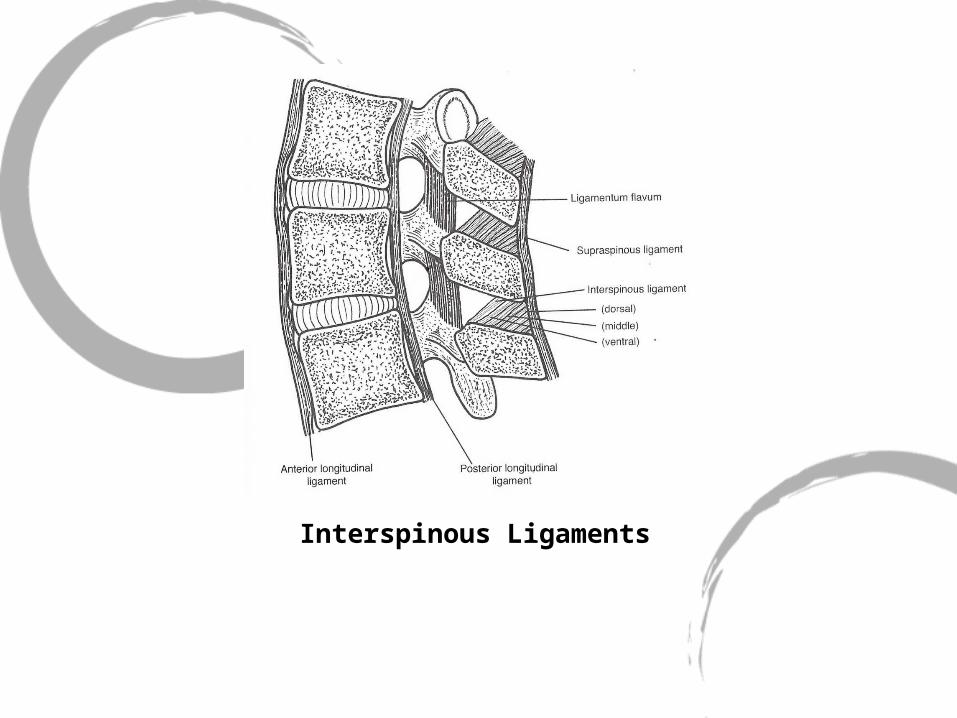
Interspinous Ligaments

Some Key Musculature
• Iliocostalis and longissimus both act as thoracolumbar extensors; also posterior shear force protectors, moreso in the lumbar region
• Thus, they are essential for maintaining a neutral spine
• Multifidus also act as extensors, but more local to lumbar spine
• Function can change through thoracic flexion, hip flexion, and lumbar flexion – erectors to shear force protectors

Latissimus Dorsi
• Involved in lumbar extensor moment generation; often acts as a major stabilizer
• Originates at each lumbar spinous process and inserts on humerus – giving it a very large extensor moment arm
• Active during pulling and lifting, which has implications for training proper functional motion patterns
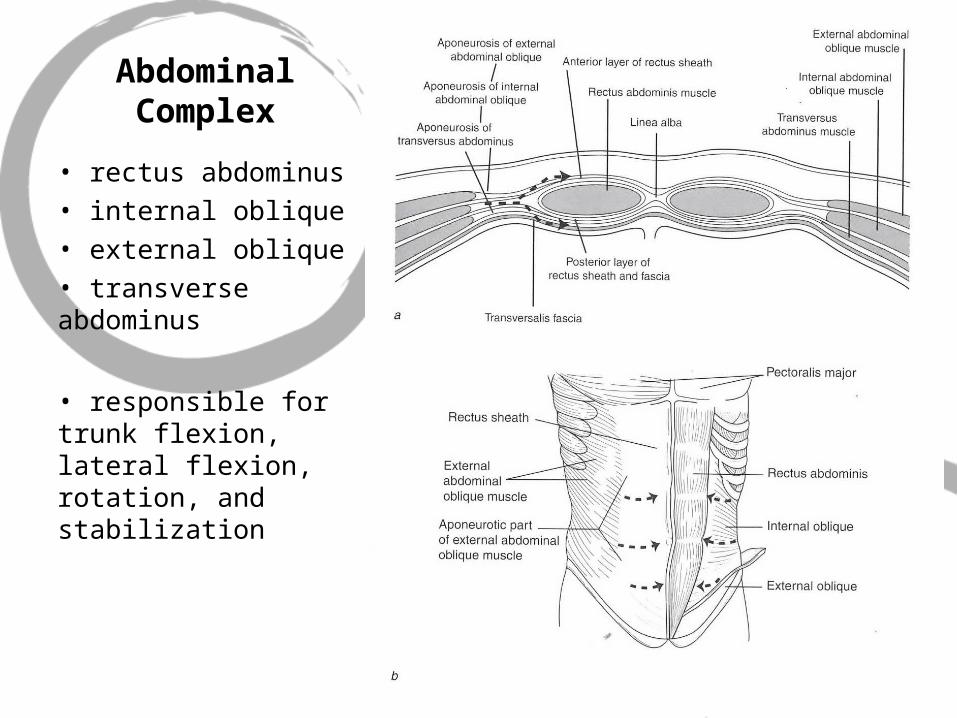
Abdominal Complex
• rectus abdominus• internal oblique• external oblique• transverse abdominus
• responsible for trunk flexion, lateral flexion, rotation, and stabilization

“Hoop” Stresses

Psoas
• acts mostly as a hip flexor• when the hip is flexed, psoas can also act as a lumbar stabilizer

Quadratus Lumborum
• lumbar stabilizer
How does a normal spine function?
• “[compression]…tolerance of the lumbar spine in an average healthy young man probably approaches 12 to 15kN (2688-3360 lb)”, LBD, p. 82
• Competitive weight lifters have safely exceeded 20kN (4480 lb)
• The lumbar spine can withstand up to 2000-2800 N of shear force
When does injury occur?

Tolerance Until Failure
• “Injury, or failure of a tissue, occurs when the applied load exceeds the failure tolerance (or strength of the tissue)”, LBD, p11.

When the tissue fails…

Optimal Loading
• “…very few back injuries…result from a single event”, LBD, p11
• Just as most systems of the body, the spine needs appropriate loads to improve capabilities
What are some causes of tissue overload?
• “…jobs characterized by manual handling of materials, sitting in vibrating vehicles, and remaining sedentary are all linked with lower back disorder”, LBD, p 29.
• Though these risk factors do not necessarily determine LBP/LBD, they are part of a list of surrogate factors: “static work posture; seated work postures; frequent bending and twisting; lifting; pulling and pushing; and vibration (especially seated)”, LBD, p 29.

The Spine Itself
• A purely ligamentous spine buckles under 90 N of compression, about 20 lbs (LBD, p. 114)
• Since we know the spine can withstand much more compression, this shows how the musculature greatly increases compressive load potential by acting as “guy wires”

What are some specific injuries?
• Bulge/Herniation• Compression +
flexion, especially full flexion = herniation
• Add rotation and the disk tends to bulge away from the axis of rotation
• Spondylolisthesis• Full cycling of flexion
and extension can fatigue the neural arch (laminae and pedicles)
• Excessive shear force can cause damage to posterior elements

Lower Back Pain vs. Injury
• Assuming spinal injury is not present, ie: fracture, bulge, spondy, avulsion, neural, etc.
• Assess each client to see what movement causes the pain or where deficiencies lie
After Injury
• It is necessary to identify the mechanism of injury, ascertain potentially injured tissues (bone, ligament, muscle, etc); and develop the next plan of action
• There is strong evidence to support that after a lower back injury, muscle activation patters are altered
• “…stability comes from stiffness, passive stiffness is lost with tissue damage and active stiffness throughout the range of motion is lost with perturbed motor patterns following injury”, LBD, p. 119

McGill’s 5 Steps
1. Groove motion patterns, motor patterns, and corrective exercise
2. Build whole-body and joint stability
3. Increase Endurance
4. Build Strength
5. Develop speed, power, agility

1. Grooving Patterns
• It is important to begin corrections pain free
• Neutral spine is desired and should never be compromised in this phase
• Proper motor control is correct muscles engaged for corresponding movement
• Eg: gluteal amnesia following injury
• Eliminate the faults in testing movements

2. Spinal Stability
• “Big Three”1. Curl-Up
2. Side Bridge
3. Birddog
• Abdominal bracing vs. hollowing or protruding
• Fascial raking

Why the “Big Three”?
• Curl up imposes minimal compressive loads to the lumbar spine and allows neutral lordodic curve
• Side Bridge activates entire abdominal complex, plus lower back stabilizers like QL and lats, while maintaining neutral spine
• Birddog activates entire set of spinal extensors, though not to MVC, while keeping the spine in neutral
• Compressive forces reach ~3000N
• Traditional sit up imposes ~3300N (~730lbs) of compression on lumbar spine; plus add full flexion!
• “Superman” extension exercise can impose up to 6000N (over 1300lbs) of compression on spine; Roman Chair extension can impose over 4000N (~890lbs), LBD, p. 91

3. Building Endurance
• Do not take muscles to fatigue failure
• Complete repetitions while muscles are still strong: McGill advocates reverse pyramid reps/sets• Side plank, birddog, chin ups, squats

4. Building Strength
• This is where you get creative
• Know what will be required of your client and train them accordingly
• Be sure to maintain proper progression
• Never let a regression of technique occur: DO NOT compromise neutral spine!
• Can introduce labile surfaces: SB, wobble boards, Airex pads, etc.

5. Develop Speed, Power, Agility
• Once sufficient endurance and strength are achieved, performance skills should be integrated into training regime• Olympic Lifting, MB work, sport specific
exercises

“The motor control system is able to control stability of the joints through coordinated muscle coactivation and to a lesser degree by placing joints in positions that modulate passive stiffness contribution. However, a faulty motor control system can lead to inappropriate magnitudes of muscle force and stiffness, allowing … for a joint to buckle or undergo shear translation”, LBD, p. 119.

Be wise…
…and be careful