ltc lunch & learn: barking, havering & redbridge - complex care model: health 1000
TRANSCRIPT

WELCOME
Tuesday 9 June 2015 WebinarBarking Havering & Redbridge Complex
Care Model: Health 1000

Barking Havering & Redbridge Complex Care Model: Health 1000
Tuesday 9 June 201512.00pm – 1.00pm
Rob MeakerBarking Havering & Redbridge
&Beverley Matthews
LTC Programme Lead, NHS Improving Quality
#LTCImp

Beverley Matthews
LTC Programme Lead
NHS Improving Quality
#LTCImp
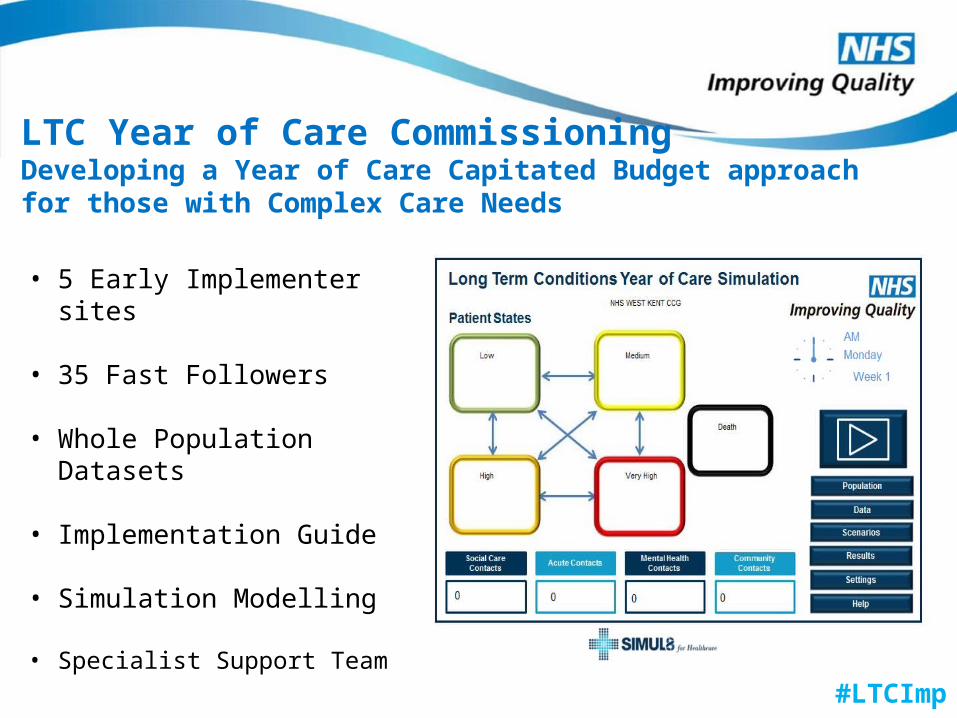
LTC Year of Care Commissioning Developing a Year of Care Capitated Budget approach for those with Complex Care Needs
• 5 Early Implementer sites
• 35 Fast Followers
• Whole Population Datasets
• Implementation Guide
• Simulation Modelling
• Specialist Support Team
#LTCImp
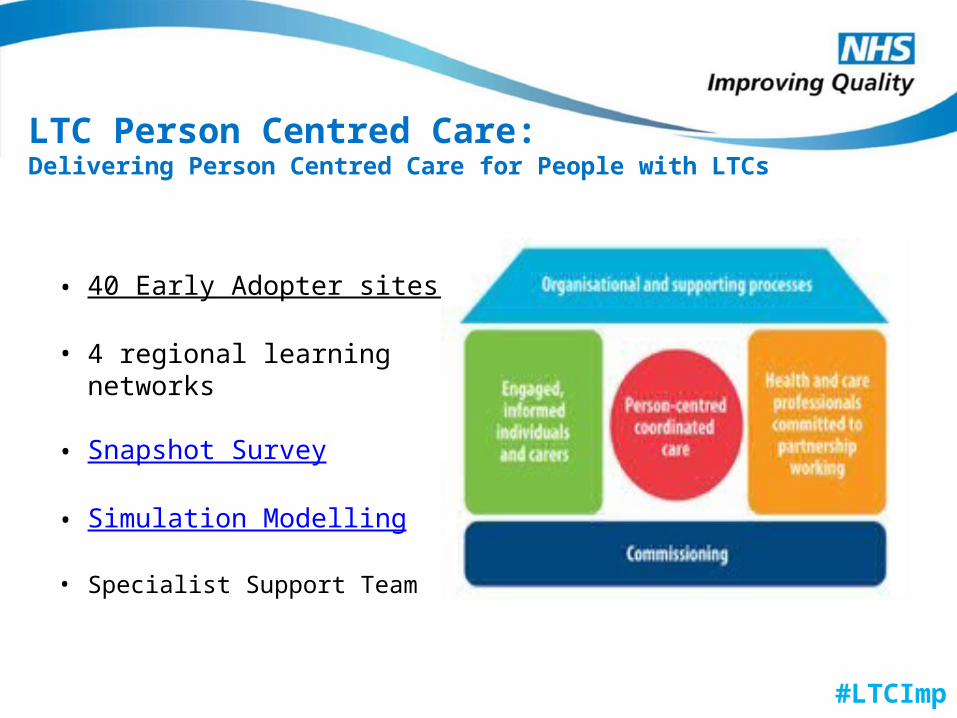
LTC Person Centred Care:Delivering Person Centred Care for People with LTCs
• 40 Early Adopter sites
• 4 regional learning networks
• Snapshot Survey
• Simulation Modelling
• Specialist Support Team
#LTCImp

LTC Learning CommunityEstablishing a Virtual Community for All to Share and Learn
• LTC Dashboard
• Case Studies
• Lunch and Learn Series
• The Bulletin
• Specialist Support Team
@NHSIQ @bev_j_matthews #LTCImp #LTCyearofcare
#LTCImp
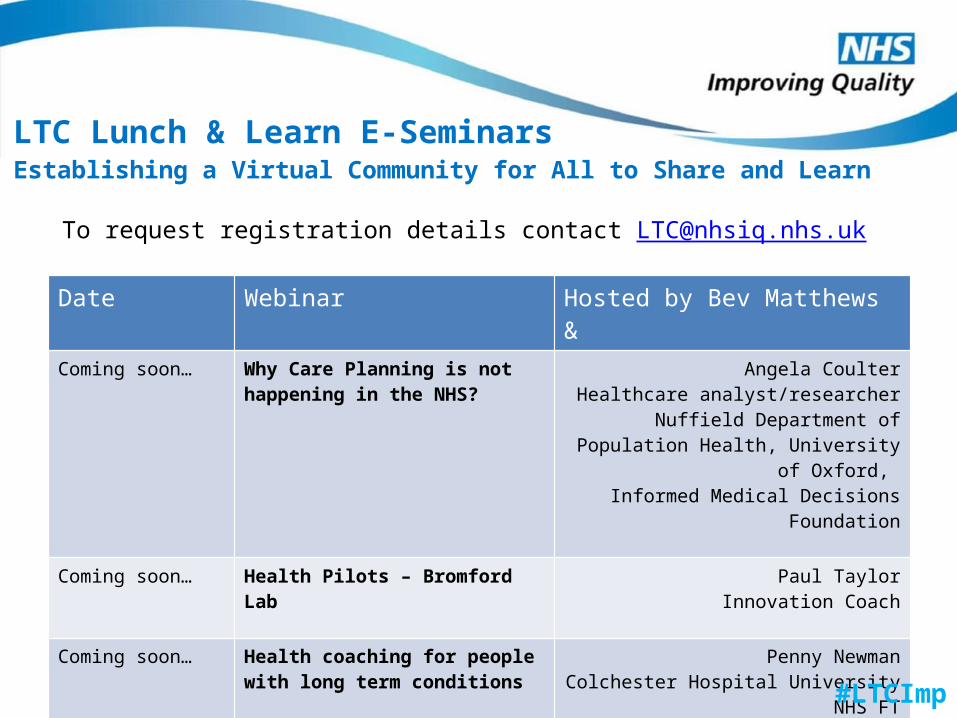
To request registration details contact [email protected]
Date Webinar Hosted by Bev Matthews &Coming soon… Why Care Planning is not
happening in the NHS?Angela Coulter
Healthcare analyst/researcherNuffield Department of Population
Health, University of Oxford, Informed Medical Decisions Foundation
Coming soon… Health Pilots – Bromford Lab Paul TaylorInnovation Coach
Coming soon… Health coaching for people with long term conditions
Penny NewmanColchester Hospital University NHS FT
LTC Lunch & Learn E-SeminarsEstablishing a Virtual Community for All to Share and Learn
#LTCImp
My services selected by Me
• Introduction
• Technology developed to facilitate “YoC research and Health 1000 provision”
• YoC Research & Cohorts
• Implementation of a Person Centred Provider organisation
• Current Situation – Health 1000 Limited.
Establishing a Complex Care Organisation in East London
Presenter : Rob MeakerDate : 9th June 2015

Background on the pilot site area in East London
Introduction

East Of England
LAS Station
Central London
Cluster 1
Cluster 2
Cluster 3
Cluster 4
Cluster5
Cluster4
Cluster6
Clus
ter3
Cluster2
Cluster 1
Cluster 1
Cluster 2
Cluster 3
Cluster 4
Cluster 6
Walk In Centre
Cluster 5
Hospital
Geography of the boroughs and key health infrastructure
Borough Population 770,000
Emerging GP federations
Redbridge federation
Havering federation
Barking & Dagenham federation
Introduction

Alignment between YoC and the vision for health and social care in BHR
Introduction

2008 – Polysystems & Person Centred Care
2009 – Risk Stratification
2010 – Integrated data
2011 – LTC management, & The Year of Care
2012 – Integrated Case Management
2013 – Rapid Response & Community Treatment Teams
2014– Complex Primary Care Practice establishment
2015– becomes operational.
Timeline for person centred care & complex care organsiation
Introduction

Operational January 2015, Core Staff Recruited, Patients No increasing
Ben and Eileen have been married for 59 years. They have four children, nine grandchildren and eighteen great-grandchildren and they also spent fifteen years fostering teenagers. Now, their focus is on enjoying life and their family.Eileen was diagnosed with osteoporosis in 1986, and has had resulting problems with her knees and joints. She overcame breast cancer and she also had a heart attack in 2012. Her husband, Ben, was diagnosed with prostate cancer last year and has a collapsed vertebrae in his back. They had been registered at their previous GP practice for 40 years when they received the call from Health 1000. Staff at the new practice explained that there would be specialists on hand, that they would be able to get an appointment whenever was convenient for them and that they could be looked after in their own home if need be. At first, they weren’t sure if they were doing the right thing by moving practice, but the support they’ve received since joining Health 1000 has left them confident that they’ve made the right decision. For Eileen, the biggest difference is that someone is always on the other end of the phone to help. When calling the practice, she can get straight through to their key worker who is already aware of all their problems and the medication they take. She said: “They’re always informative and eager to help. It feels like they know you personally and they’re interested in your welfare. It makes you feel more confident. We haven’t been with Health 1000 very long, but we’ve seen a big improvement.” The emotional support that they receive from Health 1000 is as important as the physical care. A while ago, Eileen was worried about her husband’s health. She called the practice and spoke to their doctor, who offered to come out to their home and give him a check-up that same day. She said: “Just offering to get someone to come and see you makes you feel so much better. You might not need it, but you know it’s there. They can make you feel better in yourself just by being there, and you know that they’re taking a real interest. That’s the most important thing.”
Patient case study - Health 1000
Ben and Eileen Eaton
Introduction
Before joining Health 1000, Maurice had been registered with the same GP practice in Barking his entire life. Maurice keeps busy and doesn’t like to take up too much of his doctor’s time, but he has a number of health problems and his GP suggested that he join Health 1000, as doctors there would be able to treat him in a way that would work better for him. Asked for his views on how he’s been treated since joining Health 1000, Maurice said: “I find I’m getting more attention here than at my old practice. Before I was just a number, but here I feel like they really listen to me. It gives me confidence.”Maurice finds it easier to get an appointment to see his doctor: “At my old practice, I might have had to wait two weeks to see my doctor. But pain doesn’t wait a fortnight! You want to get treatment for it there and then. Now I know I can call up in the morning, come down to Health 1000 and see someone.”He also knows that if the doctor has any concerns or if he needs an X-ray, they can send him on to the relevant department straight away, and it’s quicker and easier for him to collect his prescriptions.For Maurice, one of the best things about Health 1000 is the people that work there: “So far I’m impressed. They listen. Without a doubt I would recommend the practice to other people.”
Patient case study - Health 1000
Maurice Wilson
Introduction

The graphic below captures the experience of two patients using Health 1000
Play Video 540
Patient Story Part 1
https://youtu.be/x5ThfJ3dvxU

The Year of Care Pilot
Data Analysis and Cohort selection
Data Analysis and cohort selection
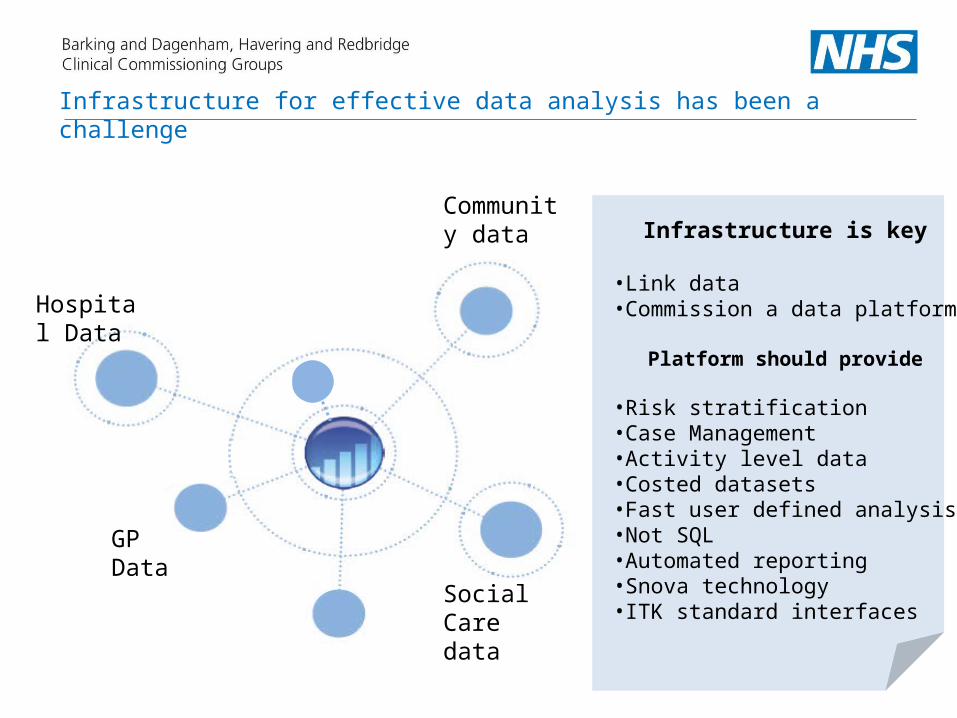
Infrastructure for effective data analysis has been a challenge
Hospital Data
GPData
Infrastructure is key
•Link data•Commission a data platform
Platform should provide
•Risk stratification•Case Management•Activity level data•Costed datasets•Fast user defined analysis•Not SQL•Automated reporting•Snova technology•ITK standard interfaces
Community data
Social Care data

Cohort selection
Data Analysis
Case Management
3949 individuals
Care ManagementSupported self care
40,248 individuals
Self CarePrevention and wellbeing promotion
162,163 individuals
RELATIVE RISK 2-20%Emergency admits = 7129 A&E visits = 26,756Total Cost= £47 million
RELATIVE RISK 0-1%Emergency admits = 3931A&E visits = 7158Total Cost = £16 million
RELATIVE RISK 21-100%Emergency admits = 1512 A&E visits = 23,586Total Cost= £22 million
Case ManagementImproving outcomes for patients with complex health and social care needs
Care ManagementIncreasing the ‘value of care’ provided to patients with long term conditions
Self CareEmpowering patients, carers & families to make informed decisions about their care treatment & providing choice in primary care to meet these needs

BHR
Kirklee
s
Lambeth
Leeds
North St
affs
South Es
sex0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Average cost of care for complex pa-tients 1 % risk
Average cost per patientAverage
BHR
Kirklee
s
Lambeth
Leeds
North St
affs
South Es
sex
West
Hamps
02,0004,0006,0008,000
10,00012,00014,00016,00018,000
Average cost of care for patients 10 %
Average cost per patientAverage
BHR Total
Kirklee
s Total
Lambeth
Total
Leeds T
otal
North St
affs T
otal
South Es
sex To
tal
West
Hamps
0
5000
10000
15000
20000
25000
30000
Combined average for patient care
Average cost per patientAverage
Data Analysis
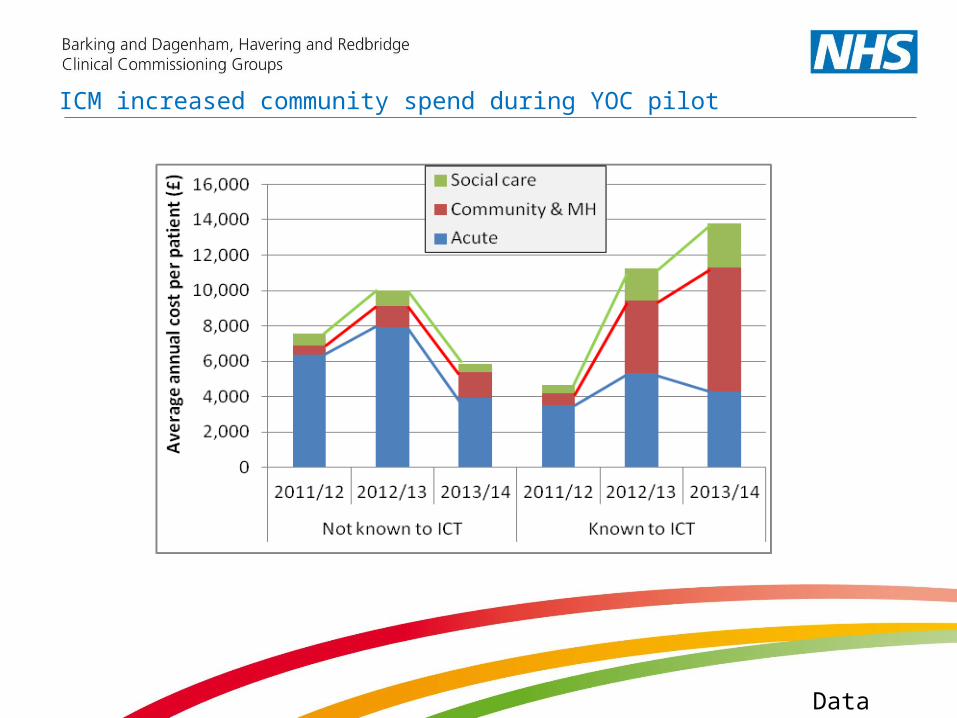
ICM increased community spend during YOC pilot
Data Analysis

Moved towards – comorbidities based on Scottish multimorbidity report 2008
Data Analysis

Diabetes
DementiaStroke
COPD
HypertensionCVD
Heart Failure Depression
Patient cohort for the service 5 or more long term conditions.2000 patients eligible across BHRCCGs and aim to recruit 1000
Patient cohortRow Labels Cohort Hypertension CHD Diabetes Stroke Depression COPD Heart Failure DementiaLTC 5+ 100 99 96 80 70 80 69 75 36Scottish modified LTC 4+ 1924 1816 1559 1421 863 793 783 679 303Grand Total 2024 1915 1655 1501 933 873 852 754 339
The selected cohort criteria, excludes CHC patients

The number of patients in the complex care cohort by the annual number of primary care contacts - 2013/14 data only, Barking & Dagenham CCG cohort only
This illustrates a relatively normal distribution of patients receiving primary care contacts around the mean of 51 contacts per year , but still there was one patient with 186 contacts in 2013/14 . The relatively normal distribution of numbers around the mean is represented by a skewness value of close to 1

Activity Cost (£thousand)
2012/13 2013/14 2014/15 2012/13 2013/14 2014/15
Primary Care Contact85,311 91,416 91,288 3,839 4,114 4,108
Pharmacy272,793 271,471 274,340 4,804 4,781 4,831
Acute care A&E2,341 2,342 1,936 277 291 244
Outpatient11,523 11,077 11,320 1,219 1,502 1,546
Daycase1,130 925 572 858 740 439
Elective162 131 128 579 392 353
NEL short-stay443 435 336 497 461 336
NEL long-stay959 985 768 3,174 3,178 2,538
Community care Face-to-Face12,052 20,654 24,936 2,210 3,814 4,396
Telephone1,032 1,859 2,244 55 96 109
Total17,511 19,368 18,899
Total annual number of events and total annual cost for all patients in the complex care cohort - all CCGs
Activity and cost for the cohort

Variation in activity between patients
The averages in the previous slide hide a great deal of variation. Thus if we take one example, patient's in the complex care cohorts on average visit A&E once a year but over 50% of patients did not visit A&E at all during 2013/14, and one patient visited 41 times .
Perhaps the most striking feature of the data is that large percentages of patient in the complex care cohorts didn't require acute inpatient care at all in 2013/14.

The trend in adjusted cost for all patient in the complex care cohort by service type
• Costs have more than doubled in 7 years
• 0ver 50% of costs are primary care
• Acute care accounts for 29% of cost and reducing
• £10k average cost per patient but escalates dramatically in last year of life
The costs have increased for these patients over the 7 years, presumably as more of the patients in the cohorts need services and/or patients in the cohorts need greater volumes of services
The greatest cost increases over the period for patients in the cohorts were primary care and community care. In percentage terms, the cost of acute care has decreased over the period.

The Implementation of a Complex Care organisation
Implementation
Legal & governance issues , Clinical design, Financial model, location and Patient recruitment

• Establishing the financial arrangements for the service as set up, then BAU and capitated budget moving forward
• CQC registration• Insurances wider provision of services• GPs and the Provider list and having a non GP as the clinical lead• CCG membership • Receiving records from practices- system challenges• Legal requirements for the Limited Company,• The APMS contract• Recruiting clinical teams for a time limited project and people leaving• GPs and the Provider list and having a non GP as the clinical lead
Challenges setting up the organisation

• Early Implementer site for YOC
• Advanced data sets from primary care, acute community and social care
• PMCF Bid to include testing of capitated budget being developed to one provider in early 2014
• PMCF Bid to include testing of capitated budget being developed to one provider in early 2014
• PMCF bid approved may 2014
May 2014
• Started work on project
May 2014
June-September 2014
• academic development of the service model and staffing requirements with UCLP
• Set up of the legal entity to operate the service
• Source premises• Source clinical leadership
October-January 2014
• Commence recruitment of staff
• Training • Premises set up• Legal entity formed• APMS discussions started• Engagement with practices • January 16th APMS
contract signed• January 19th first patient
registered
Complex Care organisation timeline

Governance
Community Trust
Private Provider
Voluntary Sector
GP Federation
Acute Trust

ROLE WTE at start up
Start up Cover provided WTE by month 3
MD and Geriatrician (50:50 role)
1.0 20 hours direct patient care plus 17.5 hours management plus on call support as required
1.0
HCS Key workers 5.0 73.5 hours per week 8am to 18.30pm Monday to Sunday. This is a dual function role covering reception and health care support and requires two members of staff to be on duty during 08.00 to 18.30pm Monday to Friday
6.0
GPs 3.0 52 hours per week 08am to 18.30pm Monday to Friday plusOn call for 5 hours per week Monday to Friday 6.30 to 8pm and 24 hours on Saturday and Sunday from 8am to 8pmA total of 81 hours per week
3.0
Practice Manager 1.0 37.5 hours per week as required to cover 7 days per week on rota
0.5
Nurse 1.0 37.5 hours per week during 8am to 6.30pm 0OT 0.5 18.5 hours per week during 8am to 6.30pm 3.0Physiotherapist 0.5 18.5 hours per week during 8am to 6.30pm 2.0Pharmacist 0.5 18 hours per week Monday to Friday as required 1
Community Nurse 0.0 Not applicable 4.0
Mental health Nurse 0 Not applicable 0.5
Social Worker 1.0 Seconded from Local Authority
Complex Care organisation staffing model

Operation process for the clinical model
Key Features of the clinical model
• GP lead model of chronic disease management with proactive case management of medical and social care
• Tele-monitoring• Patient and carer education and enhanced self-management• Promotion of independence and personal responsibility• Shared care record with agreed care plan• Quality improvement embedded in culture• Key worker skills and competencies developed

Age UK care navigator pilot
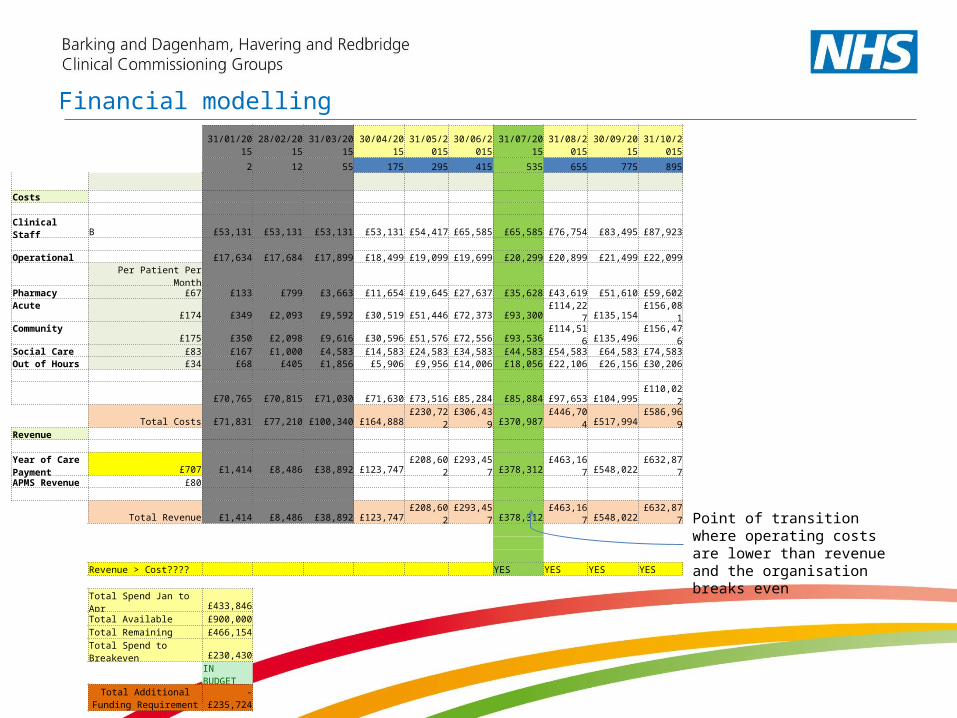
Financial modelling
31/01/2015 28/02/2015 31/03/2015 30/04/201531/05/201
530/06/201
5 31/07/201531/08/201
5 30/09/201531/10/201
5
2 12 55 175 295 415 535 655 775 895
Costs Clinical Staff B £53,131 £53,131 £53,131 £53,131 £54,417 £65,585 £65,585 £76,754 £83,495 £87,923 Operational £17,634 £17,684 £17,899 £18,499 £19,099 £19,699 £20,299 £20,899 £21,499 £22,099 Per Patient Per Month Pharmacy £67 £133 £799 £3,663 £11,654 £19,645 £27,637 £35,628 £43,619 £51,610 £59,602Acute £174 £349 £2,093 £9,592 £30,519 £51,446 £72,373 £93,300 £114,227 £135,154 £156,081Community £175 £350 £2,098 £9,616 £30,596 £51,576 £72,556 £93,536 £114,516 £135,496 £156,476Social Care £83 £167 £1,000 £4,583 £14,583 £24,583 £34,583 £44,583 £54,583 £64,583 £74,583Out of Hours £34 £68 £405 £1,856 £5,906 £9,956 £14,006 £18,056 £22,106 £26,156 £30,206 £70,765 £70,815 £71,030 £71,630 £73,516 £85,284 £85,884 £97,653 £104,995 £110,022
Total Costs £71,831 £77,210 £100,340 £164,888 £230,722 £306,439 £370,987 £446,704 £517,994 £586,969Revenue Year of Care Payment £707 £1,414 £8,486 £38,892 £123,747 £208,602 £293,457 £378,312 £463,167 £548,022 £632,877APMS Revenue £80
Total Revenue £1,414 £8,486 £38,892 £123,747 £208,602 £293,457 £378,312 £463,167 £548,022 £632,877
Revenue > Cost???? YES YES YES YES
Total Spend Jan to Apr £433,846Total Available £900,000Total Remaining £466,154Total Spend to Breakeven £230,430
IN BUDGET
Total Additional Funding Requirement -£235,724
Point of transition where operating costs are lower than revenue and the organisation breaks even
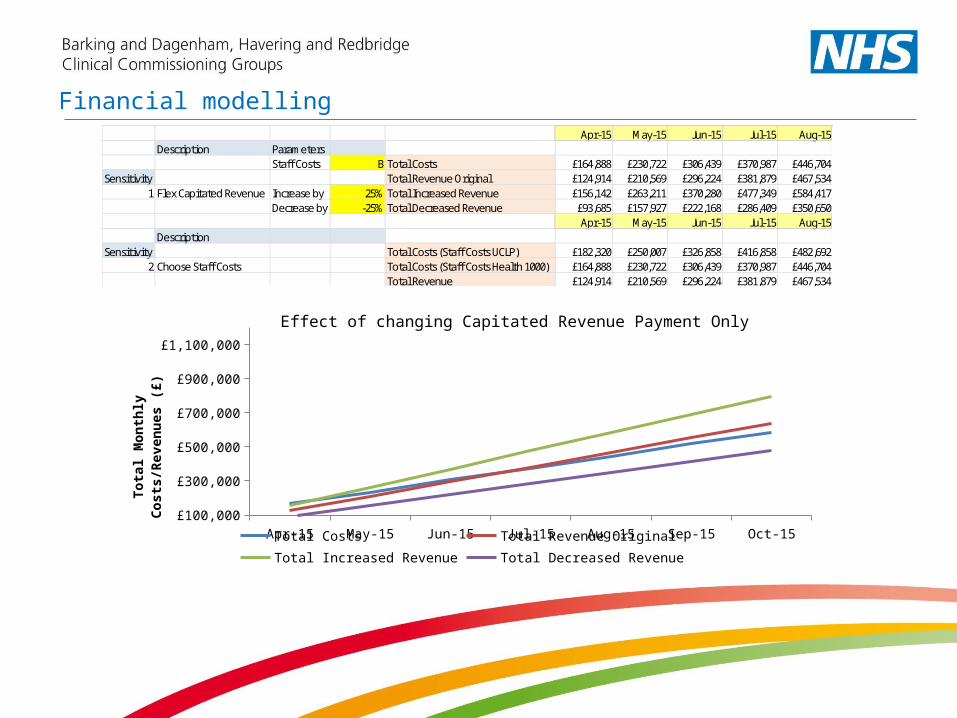
Financial modellingApr-15 May-15 Jun-15 Jul-15 Aug-15
Description ParametersStaff Costs B Total Costs £164,888 £230,722 £306,439 £370,987 £446,704
Sensitivity Total Revenue Original £124,914 £210,569 £296,224 £381,879 £467,5341 Flex Capitated Revenue Increase by 25% Total Increased Revenue £156,142 £263,211 £370,280 £477,349 £584,417
Decrease by -25% Total Decreased Revenue £93,685 £157,927 £222,168 £286,409 £350,650Apr-15 May-15 Jun-15 Jul-15 Aug-15
DescriptionSensitivity Total Costs (Staff Costs UCLP) £182,320 £250,007 £326,858 £416,858 £482,692
2 Choose Staff Costs Total Costs (Staff Costs Health 1000) £164,888 £230,722 £306,439 £370,987 £446,704Total Revenue £124,914 £210,569 £296,224 £381,879 £467,534
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15£100,000
£300,000
£500,000
£700,000
£900,000
£1,100,000
Total Costs Total Revenue Original Total Increased Revenue Total Decreased Revenue
Tota
l Mon
thly
Cos
ts/R
even
ues (
£)
Effect of changing Capitated Revenue Payment Only
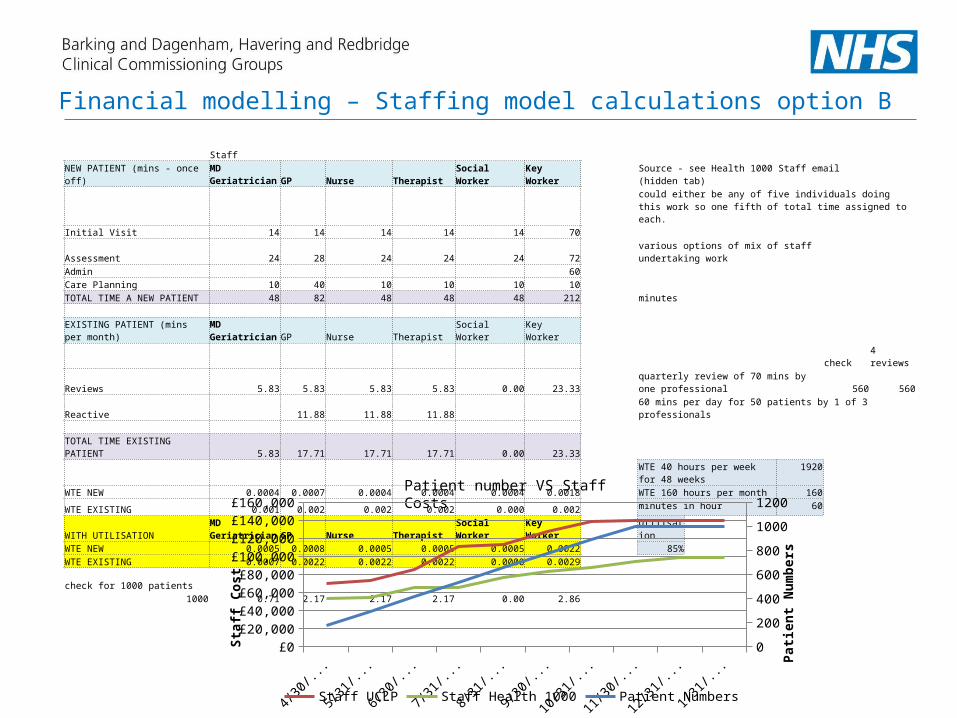
StaffNEW PATIENT (mins - once off) MD Geriatrician GP Nurse Therapist Social Worker Key Worker Source - see Health 1000 Staff email (hidden tab)
could either be any of five individuals doing this work so one fifth of total time assigned to each.
Initial Visit 14 14 14 14 14 70Assessment 24 28 24 24 24 72 various options of mix of staff undertaking workAdmin 60Care Planning 10 40 10 10 10 10TOTAL TIME A NEW PATIENT 48 82 48 48 48 212 minutes EXISTING PATIENT (mins per month) MD Geriatrician GP Nurse Therapist Social Worker Key Worker check 4 reviewsReviews 5.83 5.83 5.83 5.83 0.00 23.33 quarterly review of 70 mins by one professional 560 560Reactive 11.88 11.88 11.88 60 mins per day for 50 patients by 1 of 3 professionals TOTAL TIME EXISTING PATIENT 5.83 17.71 17.71 17.71 0.00 23.33
WTE 40 hours per week for 48 weeks
1920
WTE NEW 0.0004 0.0007 0.0004 0.0004 0.0004 0.0018 WTE 160 hours per month 160
WTE EXISTING 0.001 0.002 0.002 0.002 0.000 0.002minutes in hour 60
WITH UTILISATION MD Geriatrician GP Nurse Therapist Social Worker Key Worker UtilisationWTE NEW 0.0005 0.0008 0.0005 0.0005 0.0005 0.0022 85%WTE EXISTING 0.0007 0.0022 0.0022 0.0022 0.0000 0.0029
check for 1000 patients1000 0.71 2.17 2.17 2.17 0.00 2.86
Financial modelling – Staffing model calculations option B
Patient number VS Staff Costs
4/1/2
015
5/1/2
015
6/1/2
015
7/1/2
015
8/1/2
015
9/1/2
015
10/1/2
015
11/1/2
015
12/1/2
015
1/1/2
016£0
£20,000£40,000£60,000£80,000
£100,000£120,000£140,000£160,000
0
200
400
600
800
1000
1200
Staff UCLP Staff Health 1000 Patient Numbers
Staff
Cos
t
Patie
nt N
umbe
rs

1-Jan-15 1-Feb-15 1-Mar-15 1-Apr-15 1-May-15 1-Jun-15 1-Jul-15 1-Aug-15 1-Sep-15 1-Oct-15 1-Nov-15 1-Dec-15
Actual cumulative
2 14 61 74 87 0 0 0 0 0 0 0
Planned
4 35 55 115 205 325 445 565 685 805 925 1045
100
300
500
700
900
1100
Nu
mb
er
of
regis
tere
d p
ati
en
ts
Patient recruitment
Play Video 540
Patient Story Part 2

Outcomes per £ Spent
CO
MS
PR
EM
S
PROMS
Evaluation – Independent evaluation by the Nuffield Trust

#LTCImp
To request registration details contact [email protected]
Date Webinar Hosted by Bev Matthews &Coming soon… Why Care Planning is not
happening in the NHS?Angela Coulter
Healthcare analyst/researcherNuffield Department of Population
Health, University of Oxford, Informed Medical Decisions Foundation
Coming soon… Health Pilots – Bromford Lab Paul TaylorInnovation Coach
Coming soon… Health coaching for people with long term conditions
Penny NewmanColchester Hospital University NHS FT
LTC Lunch & Learn E-SeminarsEstablishing a Virtual Community for All to Share and Learn
#LTCImp