lung course 2015 module 4 final - amazon s3 · pfs subgroup analysis prepared by pfizer for an...
TRANSCRIPT
A Multi-Disciplinary
Targeted Therapies in the Management of Non-Small Cell Lung Cancer
Course Faculty
Medical Oncologists:
Dr. Barb Melosky – British Columbia Cancer Agency, Vancouver, BC
Dr. Jeff Rothenstein – Lakeridge Health Oshawa, Oshawa, ON
Dr. Sunil Verma – Odette Cancer Center, Toronto, ON
Radiation Oncologist:
Dr. Patrick Cheung – Odette Cancer Center, Toronto, ON
Pathologists:
Dr. Ming Tsao – Princess Margaret Hospital, Toronto, ON

Disclosures
• Dr. Barb Meloskyo Advisory Board – Astra Zeneca, Roche, Boehringer Ingelheim, Pfizer, Lilly
• Dr. Jeff Rothensteino Advisory Board – Lilly, BMS; Grants/honorarium – Novartis; Clinical trials –
Roche, BMS, AstraZeneca, Boehringer Ingelheim, Novartis
• Dr. Sunil Vermao Advisory Board – AstraZeneca, Roche, Boehringer Ingelheim, Novartis, Lilly
• Dr. Patrick Cheungo None to declare
• Dr. Ming Tsaoo Grants/honorarium – Pfizer, Merck, Roche, AstraZeneca, Boehringer
Ingelheim
Course Objectives
1. To review the evidence for use of biomarkers to help make treatment decisions for patients with advanced non small cell lung cancer
2. To discuss the current opportunities and challenges in integrating biomarkers in clinical care of lung cancer patients
3. To review the latest evidence on targeted therapies incorporating biomarkers
4. To discuss the emerging roles of radiotherapy in the management of metastatic NSCLC.

Course Outline
• Module 1: Case Study & NSCLC Treatment Overview
• Module 2: Molecular Testing in NSCLC
• Module 3: EGFR/TKI: Evidence
• Module 4: ALK Inhibitors: Evidence
Module 4: ALK Inhibitors: Evidence
Targeted Therapies in the Management of Non-Small Cell Lung Cancer: A Multi-
Disciplinary Approach
Dr. Sunil VermaMedical Oncologist, Odette Cancer Center, Toronto, ON
Dr. Barbara MeloskyMedical Oncologist, British Columbia Cancer Agency,
Vancouver, BC
Module 4 Learning Objectives
• Review the clinical data regarding the use of ALK targeted agents in a first line setting in NSCLC patients.
• Describe the common adverse events and quality of life issues associated with ALK targeted therapy.
• Discuss resistance to ALK targeted agents in NSCLC patients.
BiomarkerALK Testing
When do you generally consider ALK Testing?
1. Prior to initiating first line systemic treatment
2. During first line systemic treatment
3. Upon discontinuation/progression on first line systemic treatment
4. Upon discontinuation/progression after all lines of available chemotherapy and EGFR targeted agents
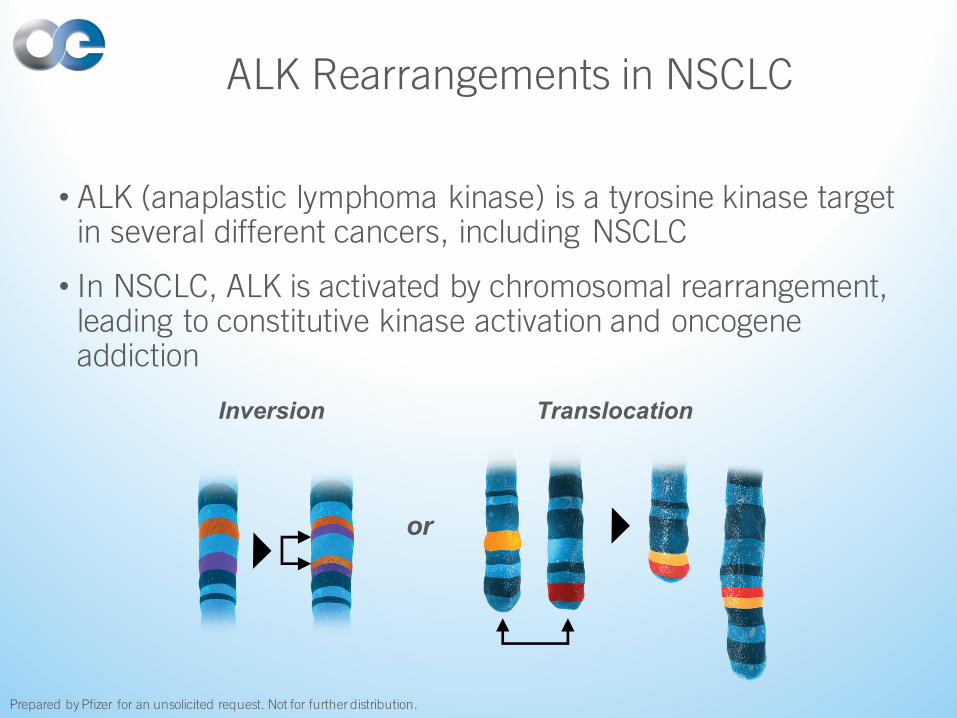
ALK Rearrangements in NSCLC
• ALK (anaplastic lymphoma kinase) is a tyrosine kinase target in several different cancers, including NSCLC
• In NSCLC, ALK is activated by chromosomal rearrangement, leading to constitutive kinase activation and oncogene addiction
or
Inversion Translocation
Prepared by Pfizer for an unsolicited request. Not for further distribution.
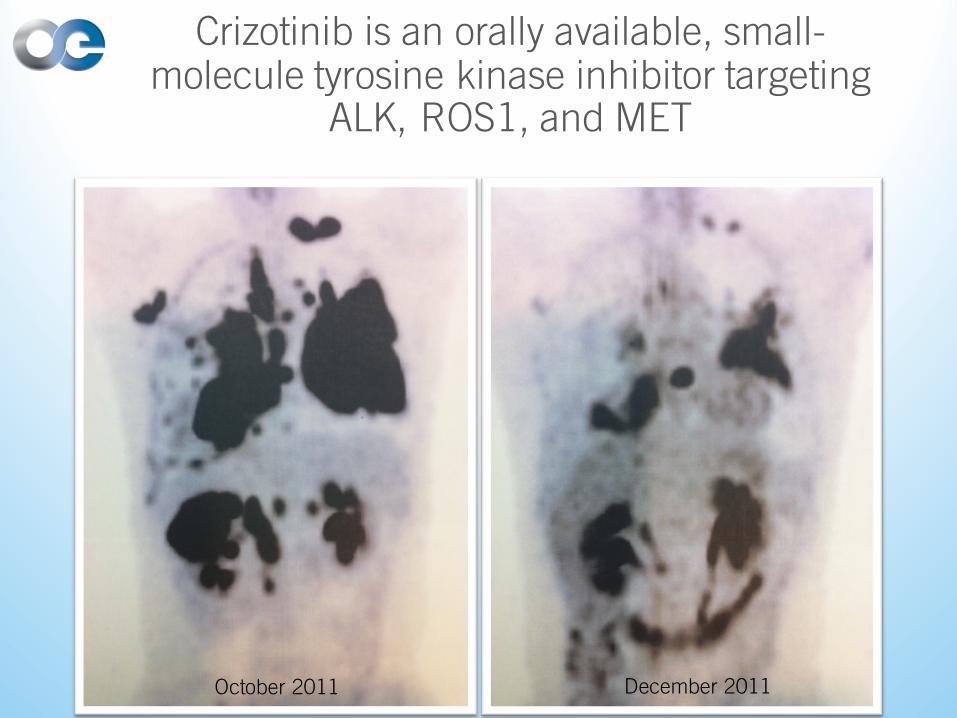
Crizotinib is an orally available, small-molecule tyrosine kinase inhibitor targeting
ALK, ROS1, and MET
October 2011 December 2011
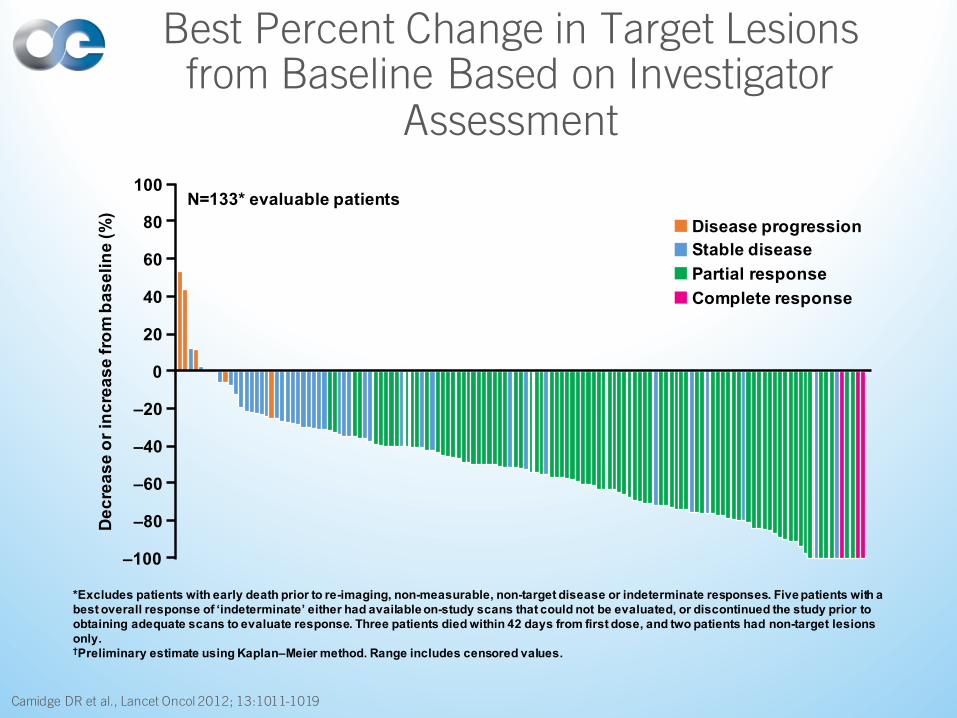
Best Percent Change in Target Lesions from Baseline Based on Investigator
Assessment
Camidge DR et al., Lancet Oncol 2012; 13:1011-1019
*Excludes patients with early death prior to re-imaging, non-measurable, non-target disease or indeterminate responses. Five patients with a best overall response of ‘indeterminate’ either had available on-study scans that could not be evaluated, or discontinued the study prior to obtaining adequate scans to evaluate response. Three patients died within 42 days from first dose, and two patients had non-target lesions only.†Preliminary estimate using Kaplan–Meier method. Range includes censored values.
100
80
–100
–80
–60
–40
–20
0
60
40
20
Decr
ease
or i
ncre
ase
from
bas
elin
e (%
)
Disease progressionStable diseasePartial responseComplete response
N=133* evaluable patients
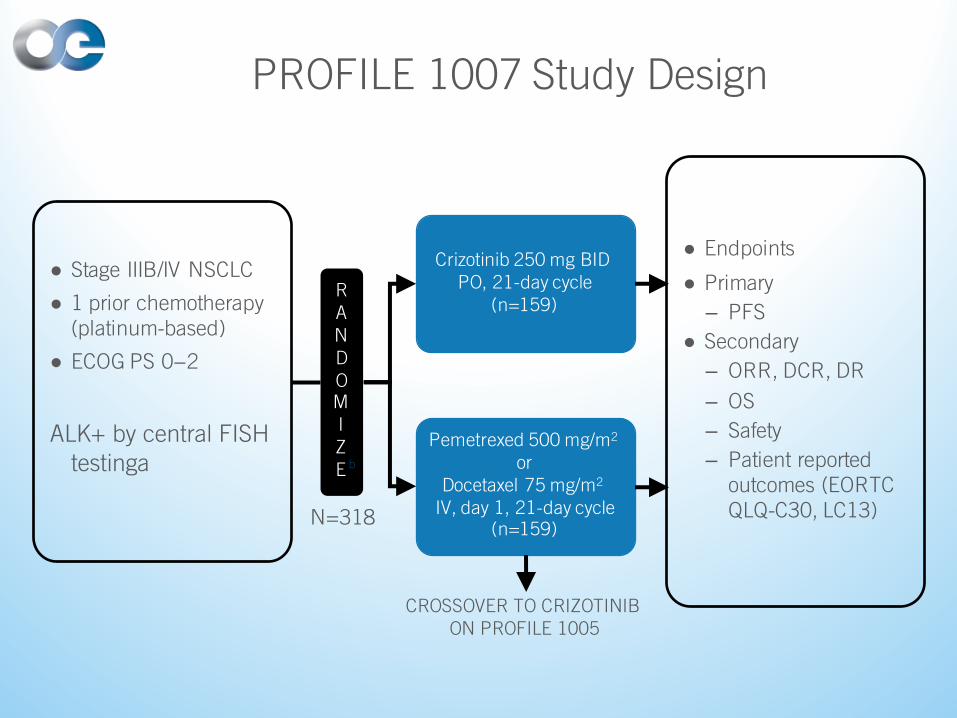
PROFILE 1007 Study Design
● Stage IIIB/IV NSCLC
● 1 prior chemotherapy (platinum-based)
● ECOG PS 0−2
ALK+ by central FISH testinga
N=318
Crizotinib 250 mg BID PO, 21-day cycle
(n=159)
Pemetrexed 500 mg/m2
orDocetaxel 75 mg/m2
IV, day 1, 21-day cycle(n=159)
● Endpoints
● Primary
– PFS
● Secondary
– ORR, DCR, DR
– OS
– Safety
– Patient reported outcomes (EORTC QLQ-C30, LC13)
RANDOMIZE
CROSSOVER TO CRIZOTINIB ON PROFILE 1005
b
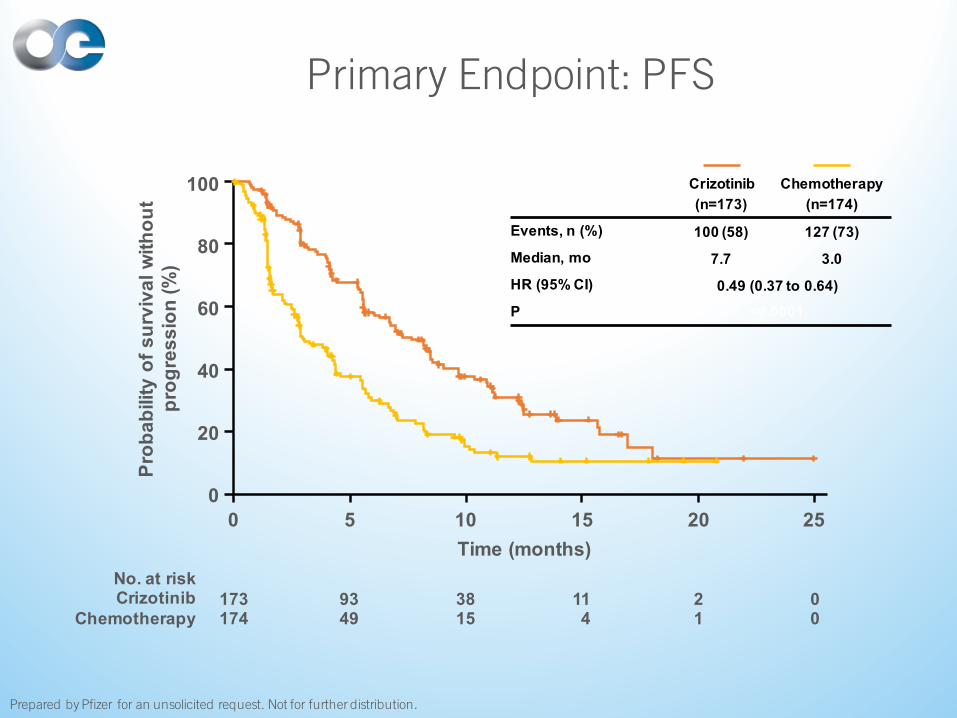
Primary Endpoint: PFS
Prepared by Pfizer for an unsolicited request. Not for further distribution.
Crizotinib(n=173)
Chemotherapy(n=174)
Events, n (%) 100 (58) 127 (73)Median, mo 7.7 3.0HR (95% CI) 0.49 (0.37 to 0.64)P <0.0001
Prob
abili
ty o
f sur
viva
l with
out
prog
ress
ion
(%)
100
80
60
40
20
00 5 10 15 20 25
Time (months)
173 93 38 11 2 0174 49 15 4 1 0
No. at riskCrizotinib
Chemotherapy

PFS Subgroup Analysis
Prepared by Pfizer for an unsolicited request. Not for further distribution.
Subgroup na HR (95% CI)
All patients 347 0.49 (0.37–0.64)
Age ≥65 years 50 0.54 (0.27–1.08)
Age <65 years 297 0.49 (0.37–0.65)
Male 153 0.52 (0.34–0.77)
Female 194 0.48 (0.34–0.68)
Non-Asian 190 0.45 (0.30–0.66)
Asian 157 0.53 (0.36–0.76)
Non-smoker 219 0.45 (0.32–0.63)
Smoker or ex-smoker 127 0.53 (0.34–0.83)
Adenocarcinoma 328 0.50 (0.38–0.66)
Non-adenocarcinoma 12 0.12 (0.01–1.02)
ECOG PS 0/1 313 0.48 (0.36–0.63)
ECOG PS 2 34 0.31 (0.12–0.86)
Brain metastases present 120 0.67 (0.44–1.03)
Brain metastases absent 227 0.43 (0.30–0.60)
Prior EGFR TKI 41 0.48 (0.22–1.03)
No prior EGFR TKI 306 0.49 (0.37–0.66)
0 1 2
HR
Favors chemotherapyFavors crizotinib
aData missing for smoking status (n=1) and tumor histology (n=7)

ORR by RECIST
65.3
19.5OR
R (%
)
ORR ratio: 3.4 (95% CI: 2.5 to 4.7); P<0.0001
Crizotinib (n=173b)
Chemotherapy (n=174b)
80
60
40
20
0Treatment
65.7
29.3
6.9
Crizotinib (n=172c)
Pemetrexed (n=99c)
Docetaxel (n=72c)
Treatment
80
60
40
20
0
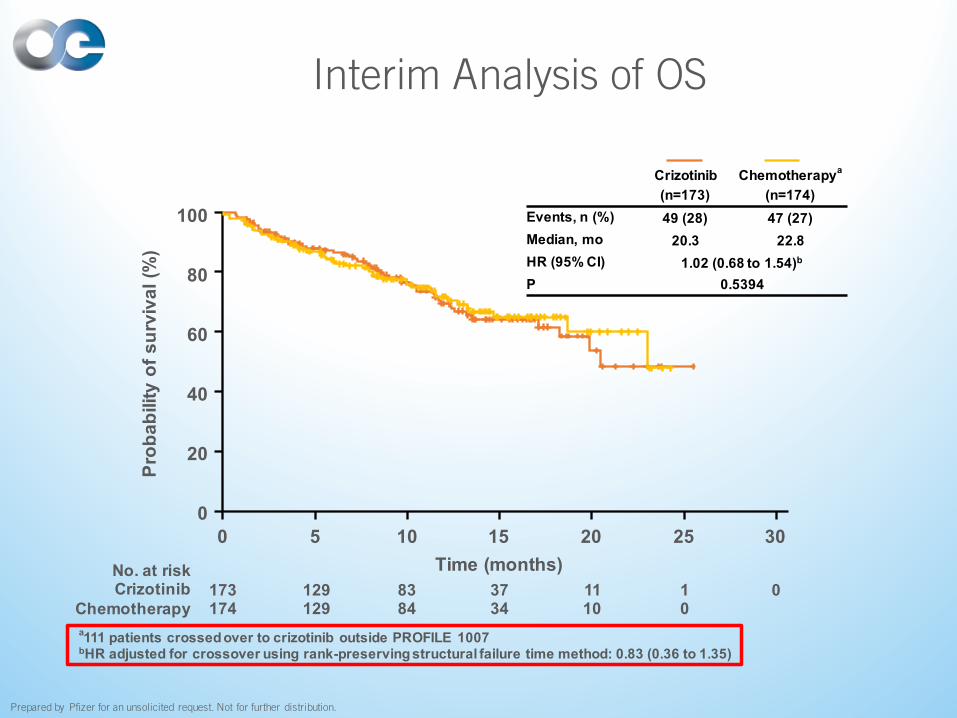
Interim Analysis of OS
a111 patients crossed over to crizotinib outside PROFILE 1007bHR adjusted for crossover using rank-preserving structural failure time method: 0.83 (0.36 to 1.35)
Crizotinib(n=173)
Chemotherapya
(n=174)Events, n (%) 49 (28) 47 (27)Median, mo 20.3 22.8 HR (95% CI) 1.02 (0.68 to 1.54)b
P 0.5394
173 129 83 37 11 1 0174 129 84 34 10 0
No. at riskCrizotinib
Chemotherapy
Prob
abili
ty o
f sur
viva
l (%
)
100
80
60
40
20
00 5 10 15 20 25 30
Time (months)
Prepared by Pfizer for an unsolicited request. Not for further distribution.
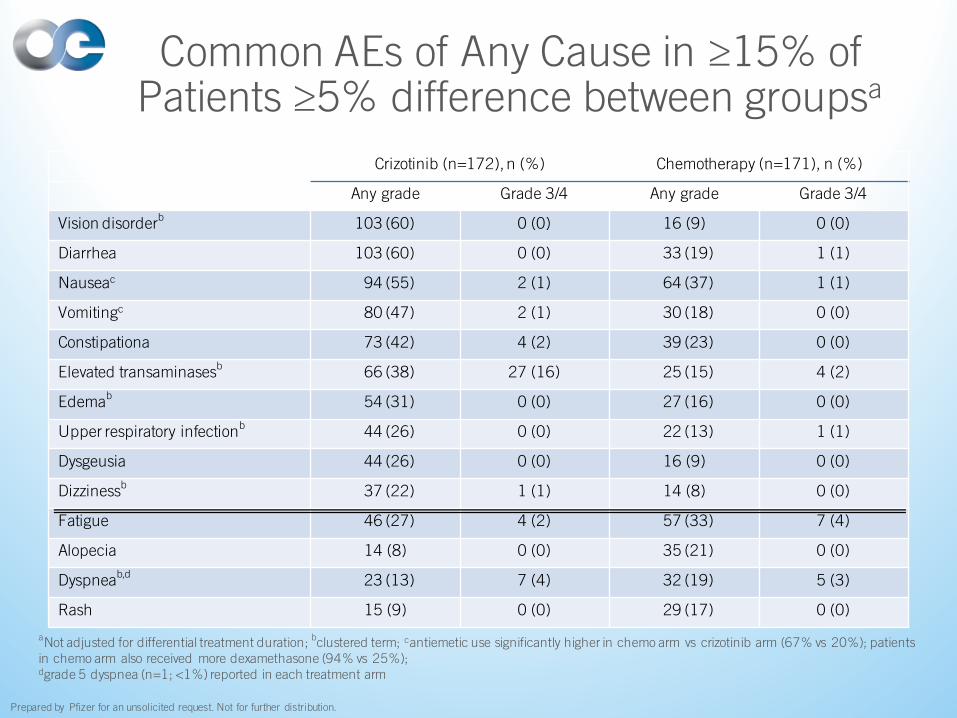
Common AEs of Any Cause in ≥15% of Patients ≥5% difference between groupsa
Crizotinib (n=172), n (%) Chemotherapy (n=171), n (%)
Any grade Grade 3/4 Any grade Grade 3/4
Vision disorderb 103 (60) 0 (0) 16 (9) 0 (0)
Diarrhea 103 (60) 0 (0) 33 (19) 1 (1)
Nauseac 94 (55) 2 (1) 64 (37) 1 (1)
Vomitingc 80 (47) 2 (1) 30 (18) 0 (0)
Constipationa 73 (42) 4 (2) 39 (23) 0 (0)
Elevated transaminasesb 66 (38) 27 (16) 25 (15) 4 (2)
Edemab 54 (31) 0 (0) 27 (16) 0 (0)
Upper respiratory infectionb 44 (26) 0 (0) 22 (13) 1 (1)
Dysgeusia 44 (26) 0 (0) 16 (9) 0 (0)
Dizzinessb 37 (22) 1 (1) 14 (8) 0 (0)
Fatigue 46 (27) 4 (2) 57 (33) 7 (4)
Alopecia 14 (8) 0 (0) 35 (21) 0 (0)
Dyspneab,d
23 (13) 7 (4) 32 (19) 5 (3)
Rash 15 (9) 0 (0) 29 (17) 0 (0)
aNot adjusted for differential treatment duration; bclustered term; cantiemetic use significantly higher in chemo arm vs crizotinib arm (67% vs 20%); patients in chemo arm also received more dexamethasone (94% vs 25%);dgrade 5 dyspnea (n=1; <1%) reported in each treatment arm
Prepared by Pfizer for an unsolicited request. Not for further distribution.
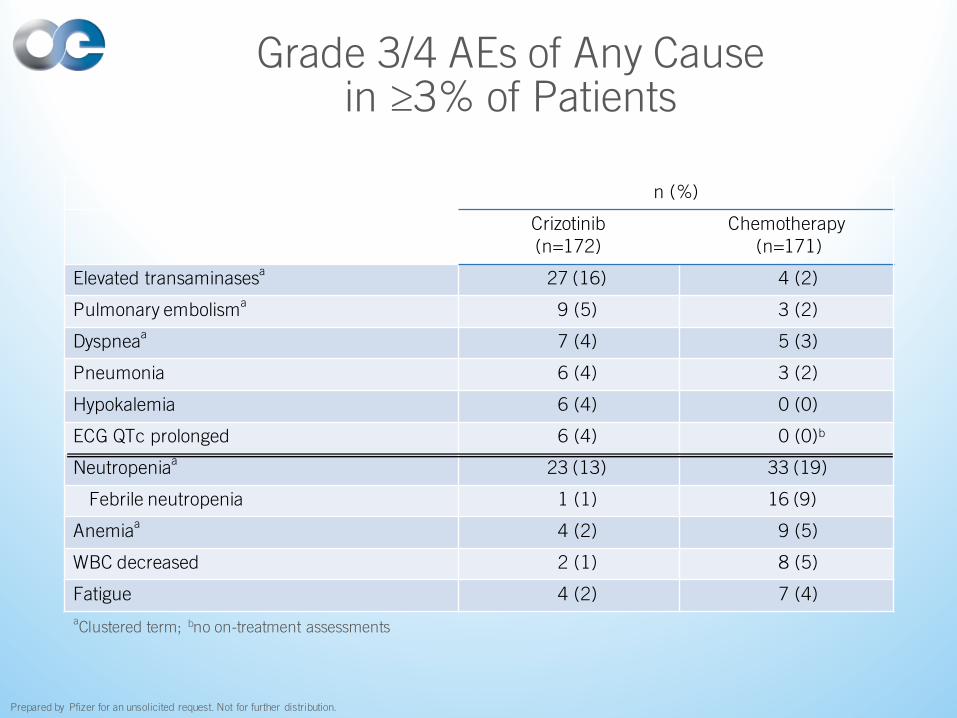
n (%)
Crizotinib(n=172)
Chemotherapy(n=171)
Elevated transaminasesa 27 (16) 4 (2)
Pulmonary embolisma 9 (5) 3 (2)
Dyspneaa 7 (4) 5 (3)
Pneumonia 6 (4) 3 (2)
Hypokalemia 6 (4) 0 (0)
ECG QTc prolonged 6 (4) 0 (0)b
Neutropeniaa 23 (13) 33 (19)
Febrile neutropenia 1 (1) 16 (9)
Anemiaa 4 (2) 9 (5)
WBC decreased 2 (1) 8 (5)
Fatigue 4 (2) 7 (4)
Grade 3/4 AEs of Any Cause in ≥3% of Patients
aClustered term; bno on-treatment assessments
Prepared by Pfizer for an unsolicited request. Not for further distribution.
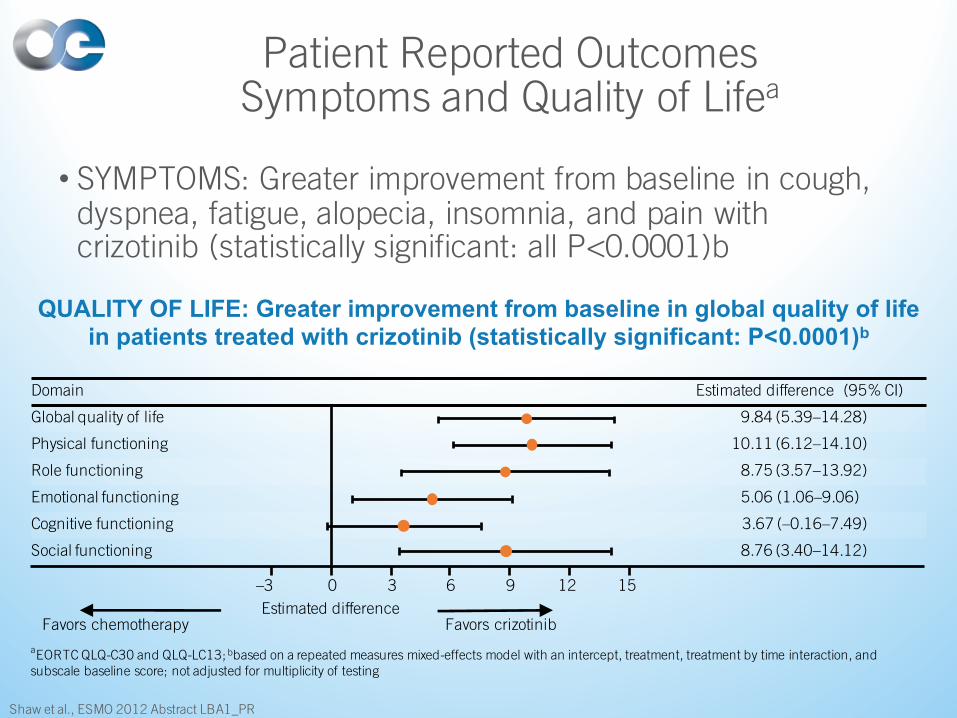
Patient Reported OutcomesSymptoms and Quality of Lifea
• SYMPTOMS: Greater improvement from baseline in cough, dyspnea, fatigue, alopecia, insomnia, and pain with crizotinib (statistically significant: all P<0.0001)b
Shaw et al., ESMO 2012 Abstract LBA1_PR
Domain Estimated difference (95% CI)
Global quality of life 9.84 (5.39–14.28)
Physical functioning 10.11 (6.12–14.10)
Role functioning 8.75 (3.57–13.92)
Emotional functioning 5.06 (1.06–9.06)
Cognitive functioning 3.67 (–0.16–7.49)
Social functioning 8.76 (3.40–14.12)
Favors chemotherapy Favors crizotinibEstimated difference
–3 0 3 6 9 12 15
aEORTC QLQ-C30 and QLQ-LC13; bbased on a repeated measures mixed-effects model with an intercept, treatment, treatment by time interaction, and subscale baseline score; not adjusted for multiplicity of testing
QUALITY OF LIFE: Greater improvement from baseline in global quality of life in patients treated with crizotinib (statistically significant: P<0.0001)b
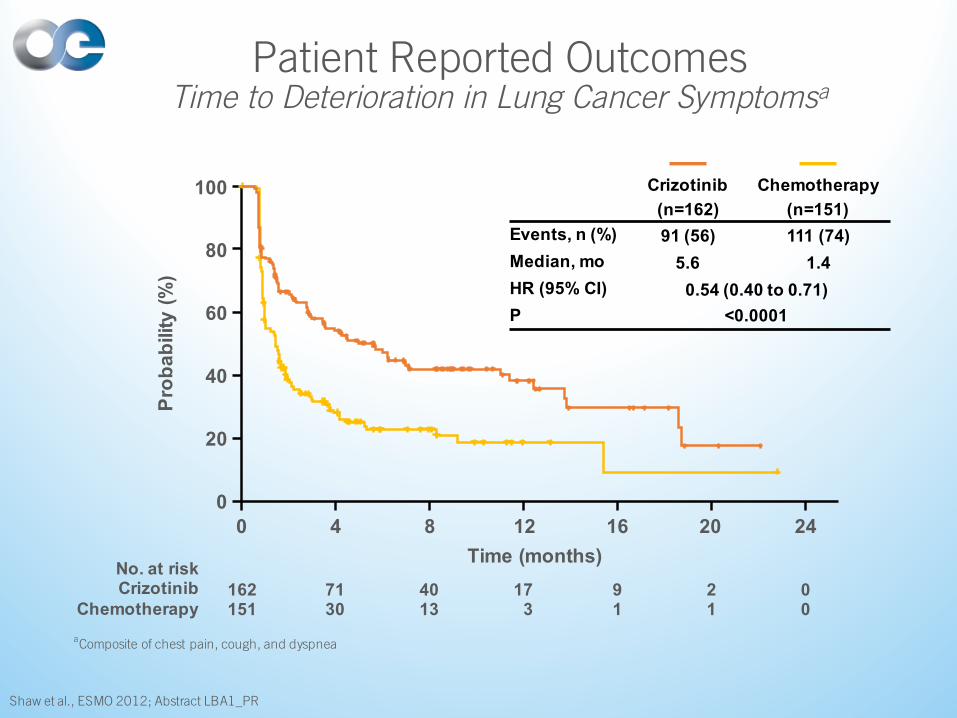
Patient Reported OutcomesTime to Deterioration in Lung Cancer Symptomsa
Shaw et al., ESMO 2012; Abstract LBA1_PR
aComposite of chest pain, cough, and dyspnea
Crizotinib(n=162)
Chemotherapy (n=151)
Events, n (%) 91 (56) 111 (74)Median, mo 5.6 1.4 HR (95% CI) 0.54 (0.40 to 0.71)P <0.0001
Pro
babi
lity
(%)
100
80
60
40
20
00 4 8 12 16 20 24
Time (months)
162 71 40 17 9 2 0151 30 13 3 1 1 0
No. at riskCrizotinib
Chemotherapy
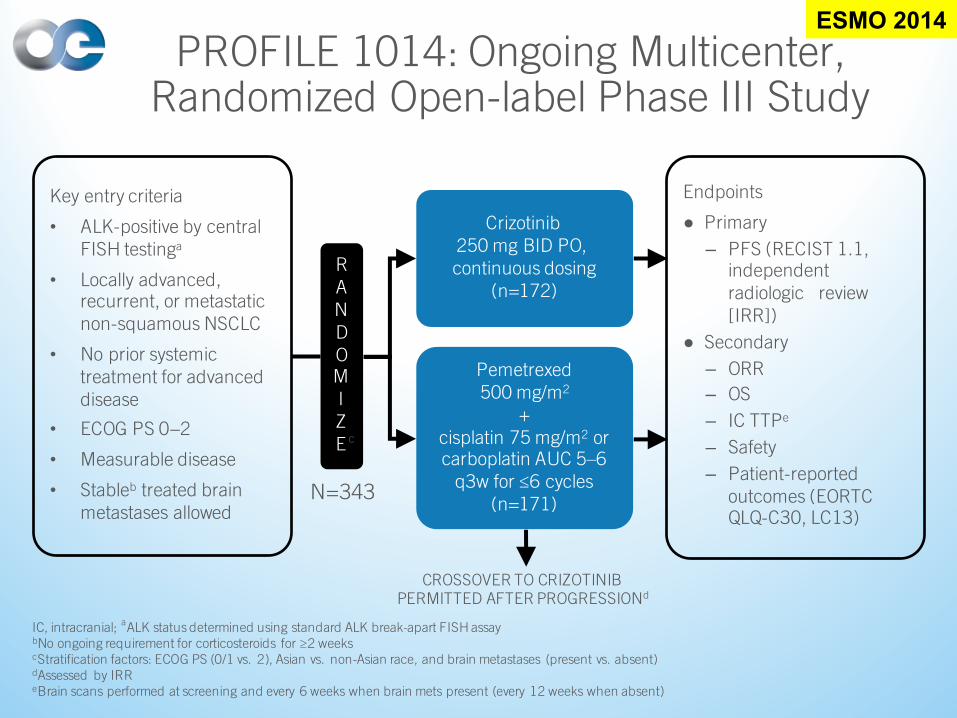
PROFILE 1014: Ongoing Multicenter, Randomized Open-label Phase III Study
IC, intracranial; aALK status determined using standard ALK break-apart FISH assaybNo ongoing requirement for corticosteroids for ≥2 weekscStratification factors: ECOG PS (0/1 vs. 2), Asian vs. non-Asian race, and brain metastases (present vs. absent)dAssessed by IRReBrain scans performed at screening and every 6 weeks when brain mets present (every 12 weeks when absent)
Key entry criteria
• ALK-positive by central FISH testinga
• Locally advanced, recurrent, or metastatic non-squamous NSCLC
• No prior systemic treatment for advanced disease
• ECOG PS 0−2
• Measurable disease
• Stableb treated brain metastases allowed
N=343
Crizotinib 250 mg BID PO, continuous dosing
(n=172)
Pemetrexed 500 mg/m2
+ cisplatin 75 mg/m2 or carboplatin AUC 5–6
q3w for ≤6 cycles(n=171)
Endpoints
● Primary
– PFS (RECIST 1.1, independent radiologic review [IRR])
● Secondary
– ORR
– OS
– IC TTPe
– Safety
– Patient-reported outcomes (EORTC QLQ-C30, LC13)
RANDOMIZE
CROSSOVER TO CRIZOTINIB PERMITTED AFTER PROGRESSIONd
c
ESMO 2014
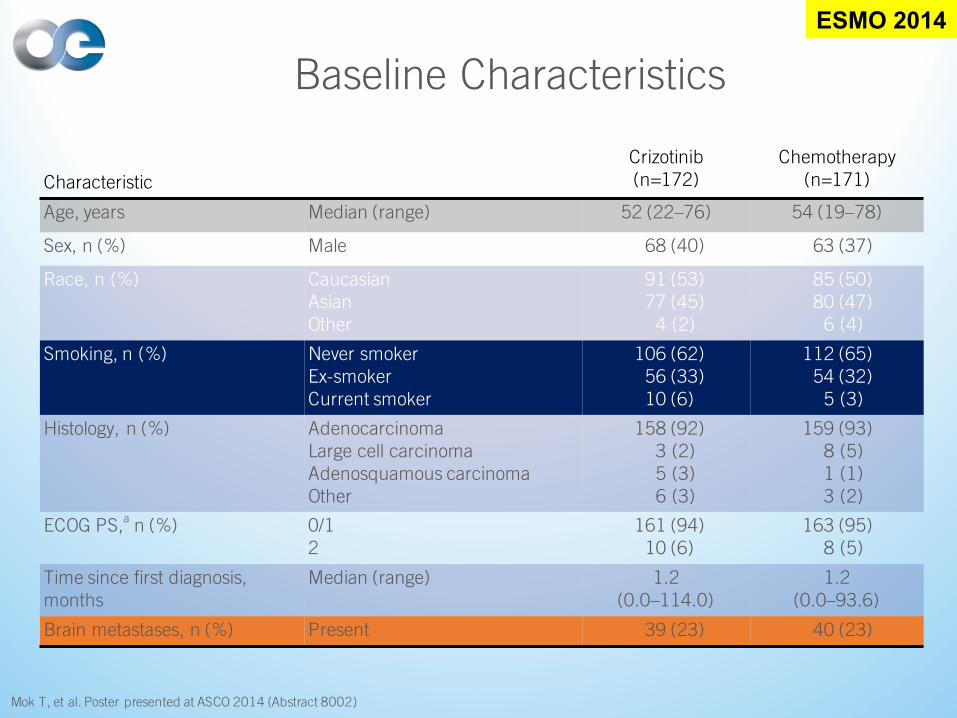
Baseline Characteristics
Characteristic
Crizotinib (n=172)
Chemotherapy (n=171)
Age, years Median (range) 52 (22–76) 54 (19–78)
Sex, n (%) Male 68 (40) 63 (37)
Race, n (%) CaucasianAsianOther
91 (53)77 (45)
4 (2)
85 (50)80 (47)
6 (4)
Smoking, n (%) Never smokerEx-smokerCurrent smoker
106 (62)56 (33)10 (6)
112 (65)54 (32)
5 (3)
Histology, n (%) AdenocarcinomaLarge cell carcinomaAdenosquamous carcinomaOther
158 (92)3 (2)5 (3)6 (3)
159 (93)8 (5)1 (1)3 (2)
ECOG PS,a n (%) 0/12
161 (94)10 (6)
163 (95)8 (5)
Time since first diagnosis, months
Median (range) 1.2(0.0–114.0)
1.2(0.0–93.6)
Brain metastases, n (%) Present 39 (23) 40 (23)
Mok T, et al. Poster presented at ASCO 2014 (Abstract 8002)
ESMO 2014
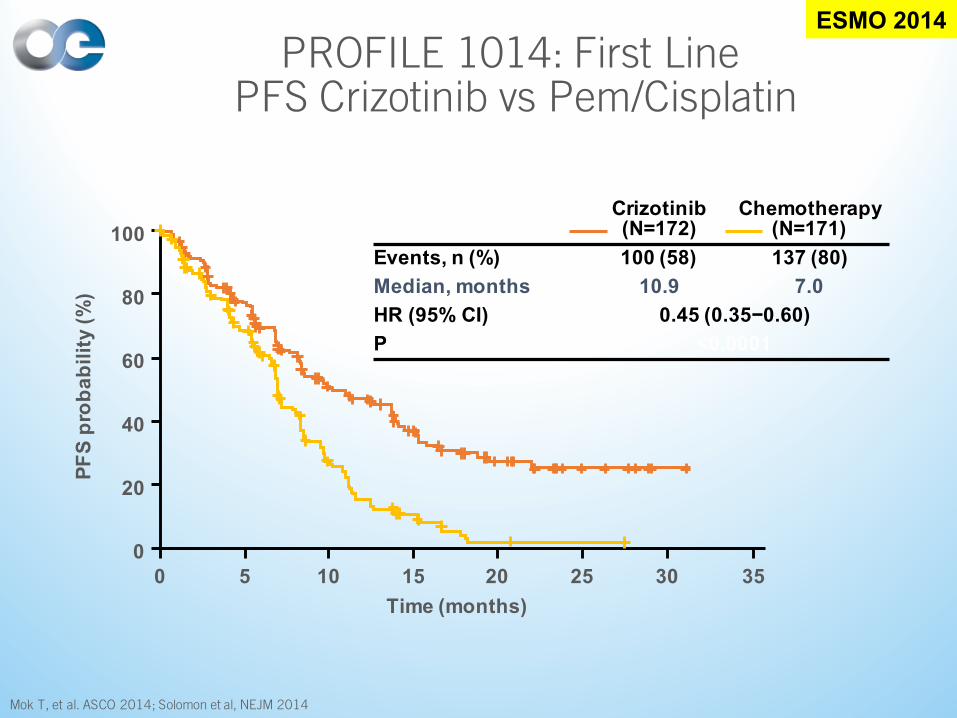
PROFILE 1014: First LinePFS Crizotinib vs Pem/Cisplatin
Mok T, et al. ASCO 2014; Solomon et al, NEJM 2014
ESMO 2014
Crizotinib(N=172)
Chemotherapy(N=171)
Events, n (%) 100 (58) 137 (80)
Median, months 10.9 7.0
HR (95% CI) 0.45 (0.35−0.60)
P <0.0001
PF
S p
rob
ab
ilit
y (
%)
100
80
60
40
20
0
0 5 10 15 20 25 30 35
Time (months)
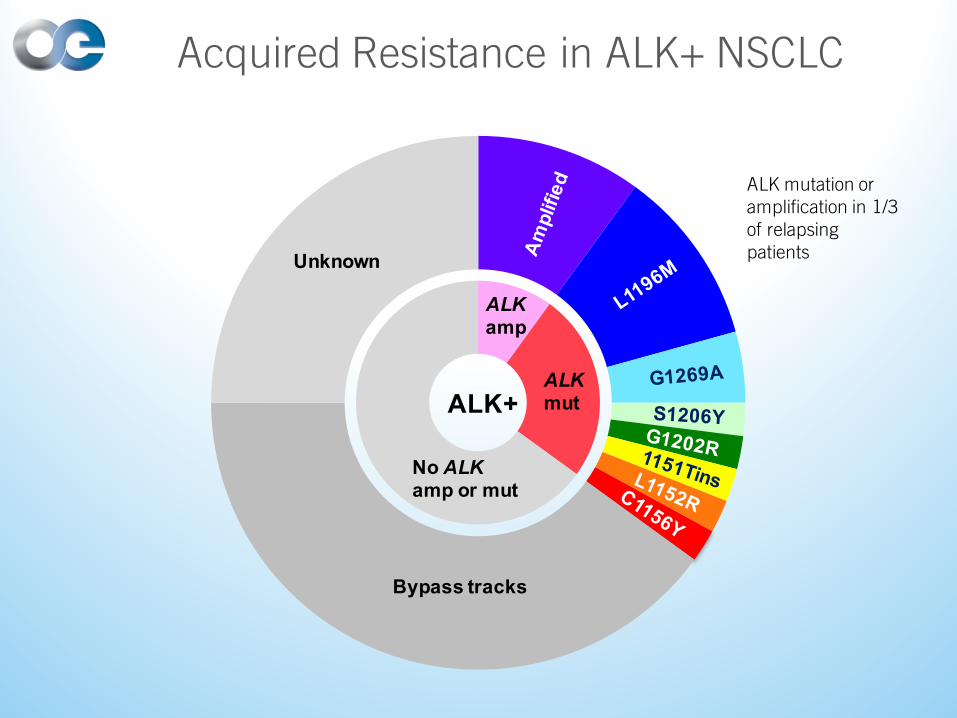
Acquired Resistance in ALK+ NSCLC
ALK mutation or amplification in 1/3 of relapsing patients
Bypass tracks
Unknown
ALKmut
ALKamp
No ALKamp or mut
ALK+
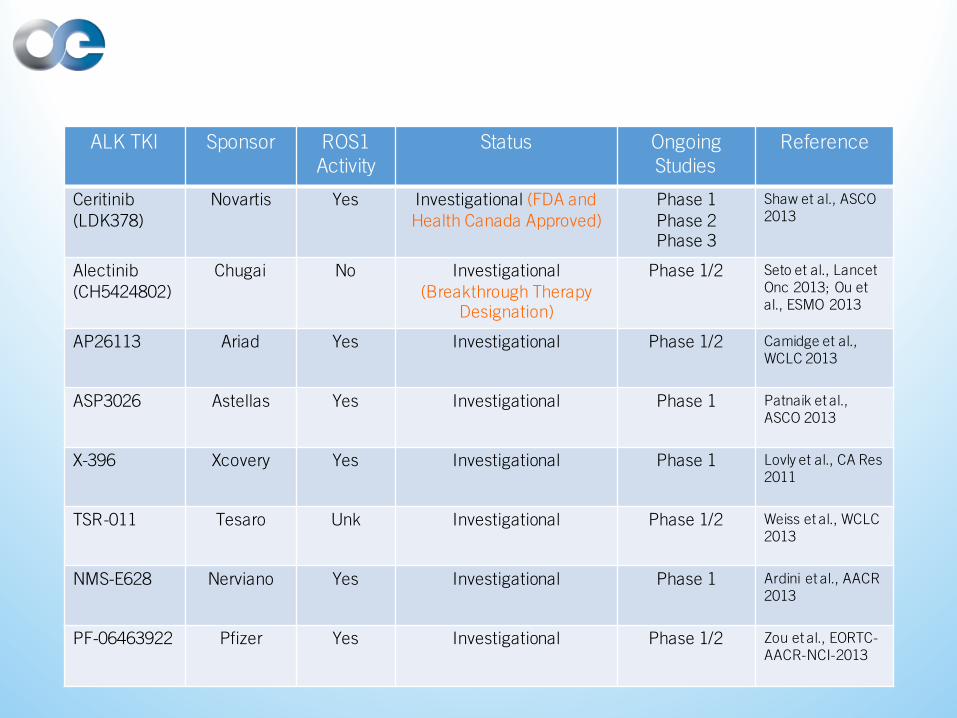
ALK TKI Sponsor ROS1 Activity
Status OngoingStudies
Reference
Ceritinib(LDK378)
Novartis Yes Investigational (FDA and Health Canada Approved)
Phase 1Phase 2Phase 3
Shaw et al., ASCO 2013
Alectinib(CH5424802)
Chugai No Investigational(Breakthrough Therapy
Designation)
Phase 1/2 Seto et al., Lancet Onc 2013; Ou et al., ESMO 2013
AP26113 Ariad Yes Investigational Phase 1/2 Camidge et al., WCLC 2013
ASP3026 Astellas Yes Investigational Phase 1 Patnaik et al., ASCO 2013
X-396 Xcovery Yes Investigational Phase 1 Lovly et al., CA Res 2011
TSR-011 Tesaro Unk Investigational Phase 1/2 Weiss et al., WCLC 2013
NMS-E628 Nerviano Yes Investigational Phase 1 Ardini et al., AACR 2013
PF-06463922 Pfizer Yes Investigational Phase 1/2 Zou et al., EORTC-AACR-NCI-2013
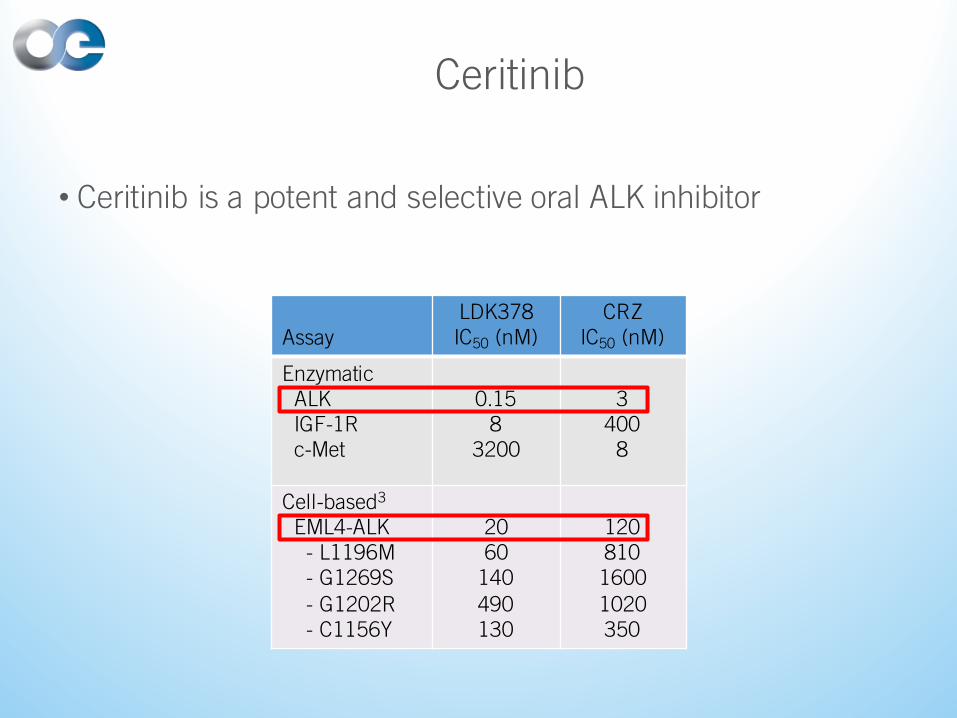
Ceritinib
• Ceritinib is a potent and selective oral ALK inhibitor
AssayLDK378IC50 (nM)
CRZIC50 (nM)
Enzymatic ALK IGF-1Rc-Met
0.158
3200
3400
8
Cell-based3
EML4-ALK - L1196M- G1269S- G1202R- C1156Y
2060
140490130
12081016001020350
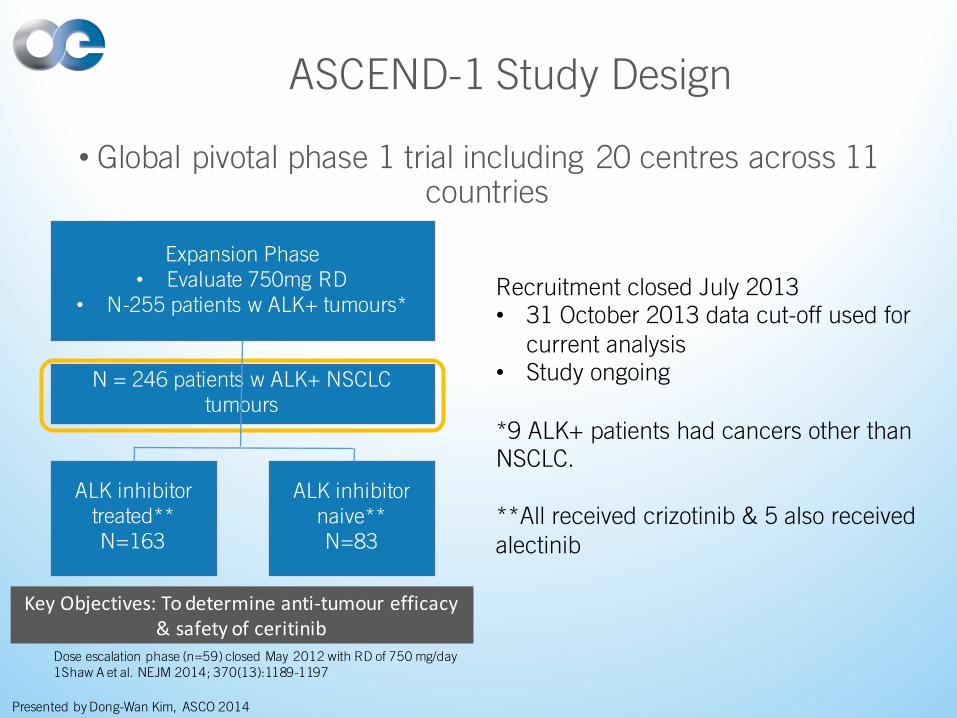
ASCEND-1 Study Design
• Global pivotal phase 1 trial including 20 centres across 11 countries
Expansion Phase• Evaluate 750mg RD
• N-255 patients w ALK+ tumours*
N = 246 patients w ALK+ NSCLC tumours
ALK inhibitor treated**N=163
ALK inhibitor naive**N=83
KeyObjectives:Todetermineanti-tumour efficacy&safetyofceritinib
Recruitment closed July 2013• 31 October 2013 data cut-off used for
current analysis• Study ongoing
*9 ALK+ patients had cancers other than NSCLC.
**All received crizotinib & 5 also received alectinib
Dose escalation phase (n=59) closed May 2012 with RD of 750 mg/day1Shaw A et al. NEJM 2014; 370(13):1189-1197
Presented by Dong-Wan Kim, ASCO 2014
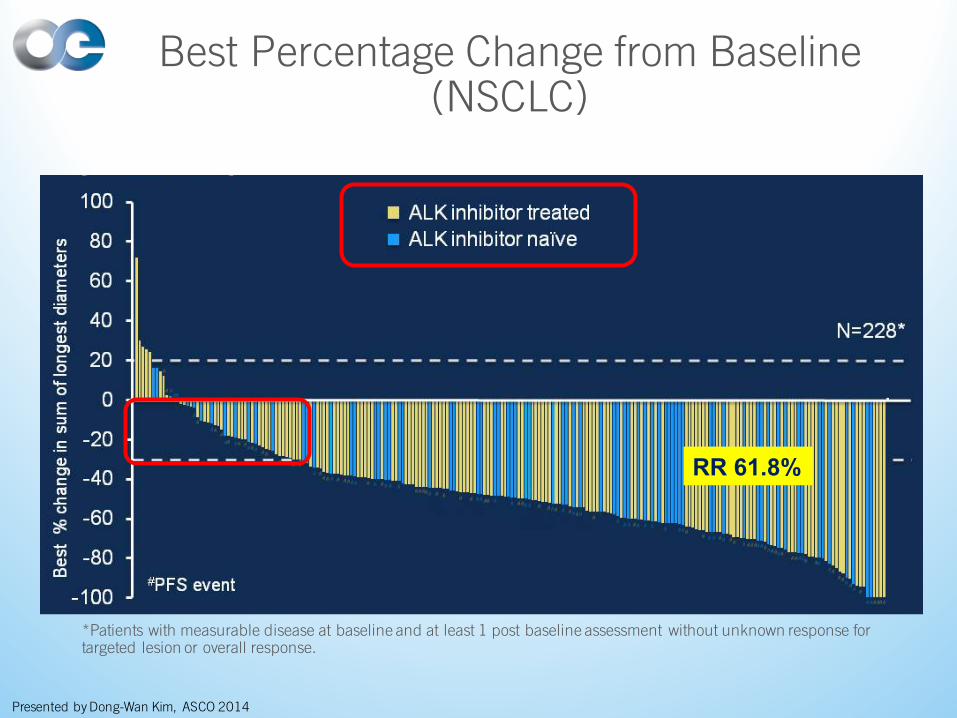
Best Percentage Change from Baseline (NSCLC)
*Patients with measurable disease at baseline and at least 1 post baseline assessment without unknown response for targeted lesion or overall response.
RR 61.8%
Presented by Dong-Wan Kim, ASCO 2014
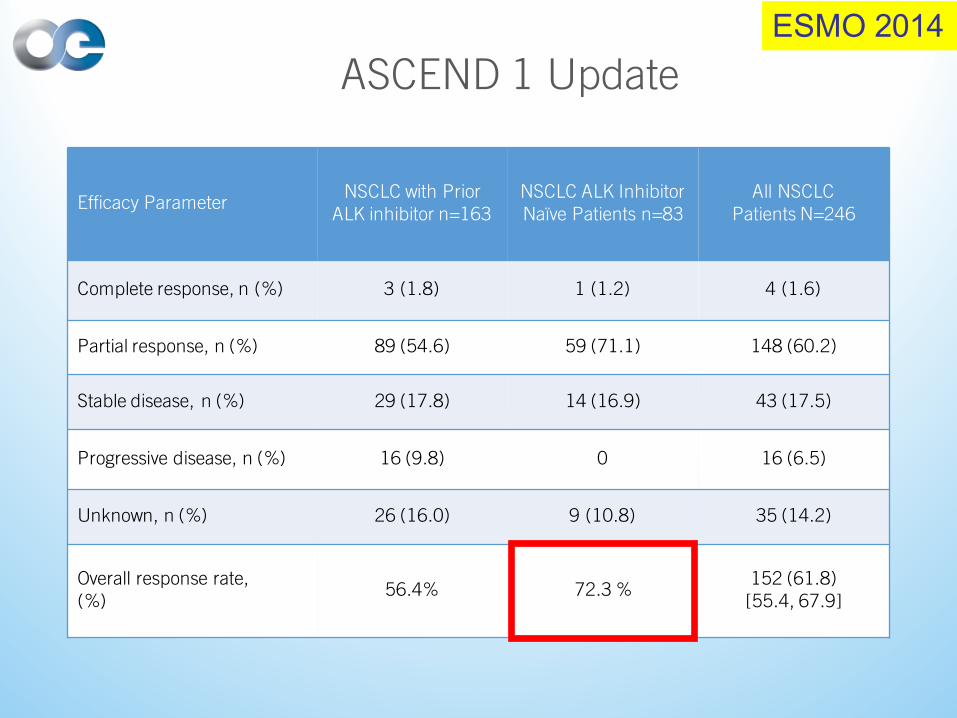
ASCEND 1 Update
Efficacy ParameterNSCLC with Prior
ALK inhibitor n=163NSCLC ALK Inhibitor Naïve Patients n=83
All NSCLCPatients N=246
Complete response, n (%) 3 (1.8) 1 (1.2) 4 (1.6)
Partial response, n (%) 89 (54.6) 59 (71.1) 148 (60.2)
Stable disease, n (%) 29 (17.8) 14 (16.9) 43 (17.5)
Progressive disease, n (%) 16 (9.8) 0 16 (6.5)
Unknown, n (%) 26 (16.0) 9 (10.8) 35 (14.2)
Overall response rate, (%)
56.4% 72.3 %152 (61.8)
[55.4, 67.9]
ESMO 2014
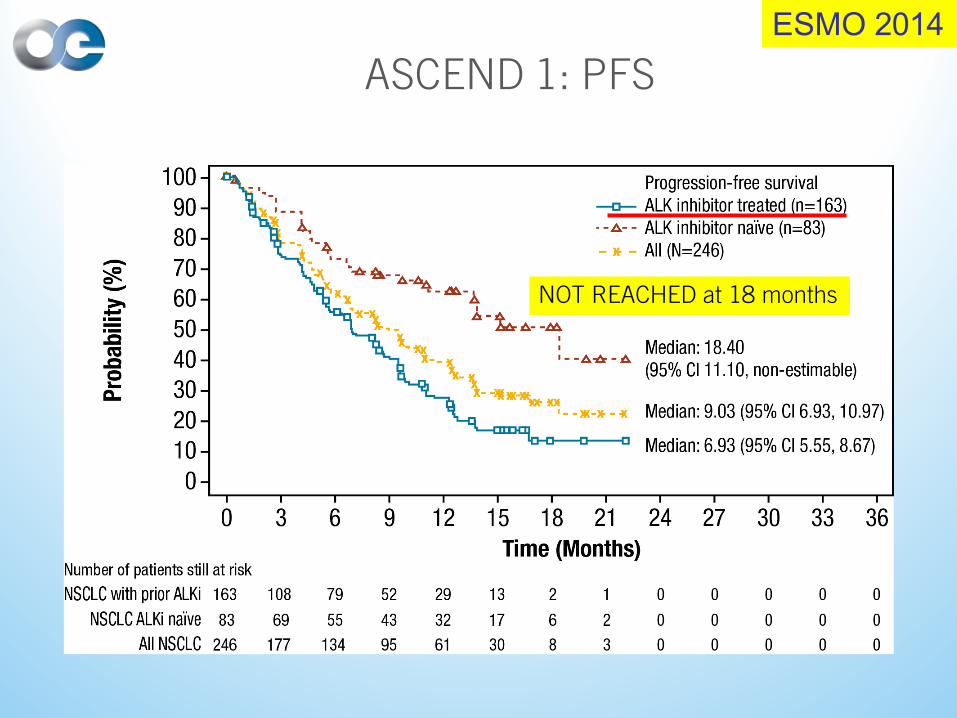
ASCEND 1: PFS
NOT REACHED at 18 months
ESMO 2014
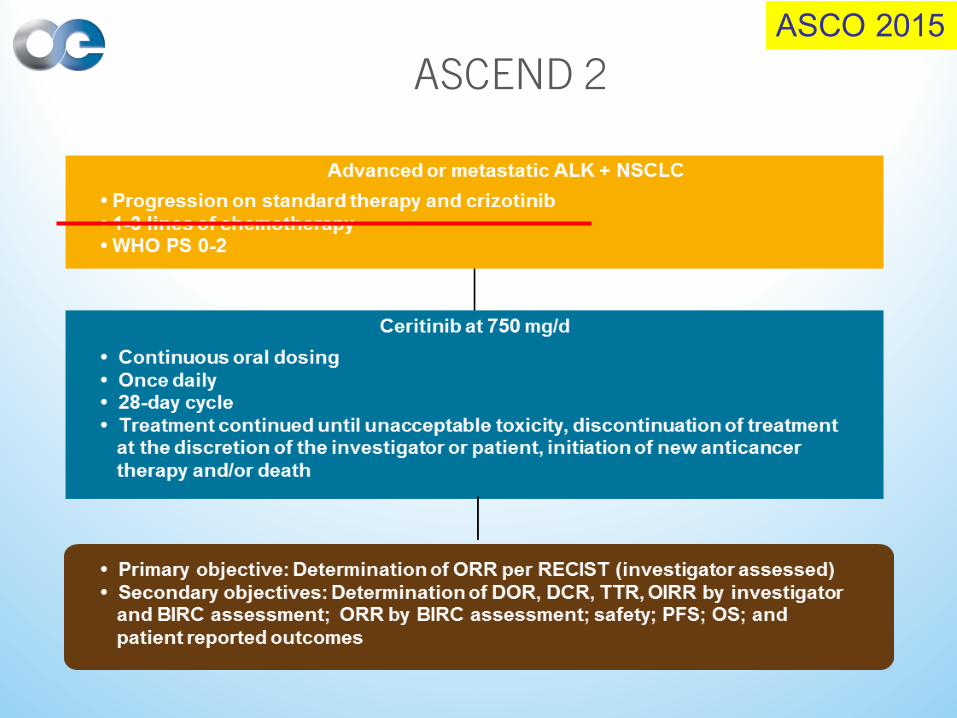
ASCEND 2ASCO 2015
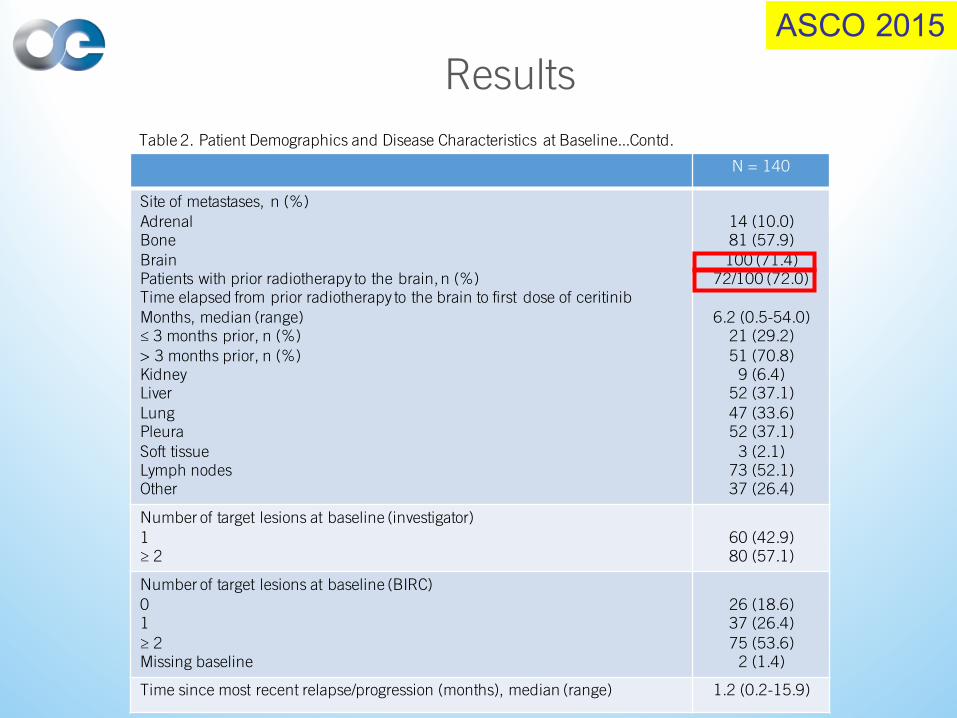
Results
Table 2. Patient Demographics and Disease Characteristics at Baseline...Contd.
N = 140
Site of metastases, n (%)AdrenalBoneBrainPatients with prior radiotherapy to the brain, n (%)Time elapsed from prior radiotherapy to the brain to first dose of ceritinibMonths, median (range)≤ 3 months prior, n (%)> 3 months prior, n (%)KidneyLiverLungPleuraSoft tissueLymph nodesOther
14 (10.0)81 (57.9)100 (71.4)
72/100 (72.0)
6.2 (0.5-54.0)21 (29.2)51 (70.8)
9 (6.4)52 (37.1)47 (33.6)52 (37.1)
3 (2.1)73 (52.1)37 (26.4)
Number of target lesions at baseline (investigator)1≥ 2
60 (42.9)80 (57.1)
Number of target lesions at baseline (BIRC)01≥ 2Missing baseline
26 (18.6)37 (26.4)75 (53.6)
2 (1.4)
Time since most recent relapse/progression (months), median (range) 1.2 (0.2-15.9)
ASCO 2015
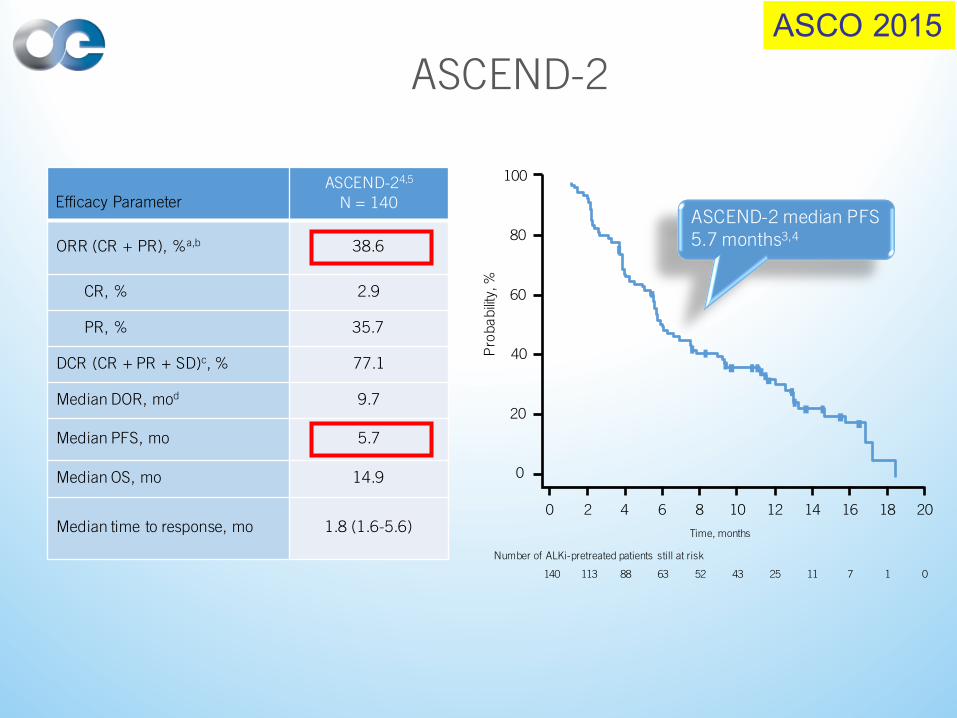
Efficacy ParameterASCEND-24,5
N = 140
ORR (CR + PR), %a,b 38.6
CR, % 2.9
PR, % 35.7
DCR (CR + PR + SD)c, % 77.1
Median DOR, mod 9.7
Median PFS, mo 5.7
Median OS, mo 14.9
Median time to response, mo 1.8 (1.6-5.6)
100
80
60
40
20
0P
robability
, %
Time, months
Number of ALKi-pretreated patients still at risk
140
0 2 4 6 8 10 12 14 16 18 20
113 88 63 52 43 25 11 7 1 0
ASCEND-2 median PFS 5.7 months3,4
ASCEND-2ASCO 2015
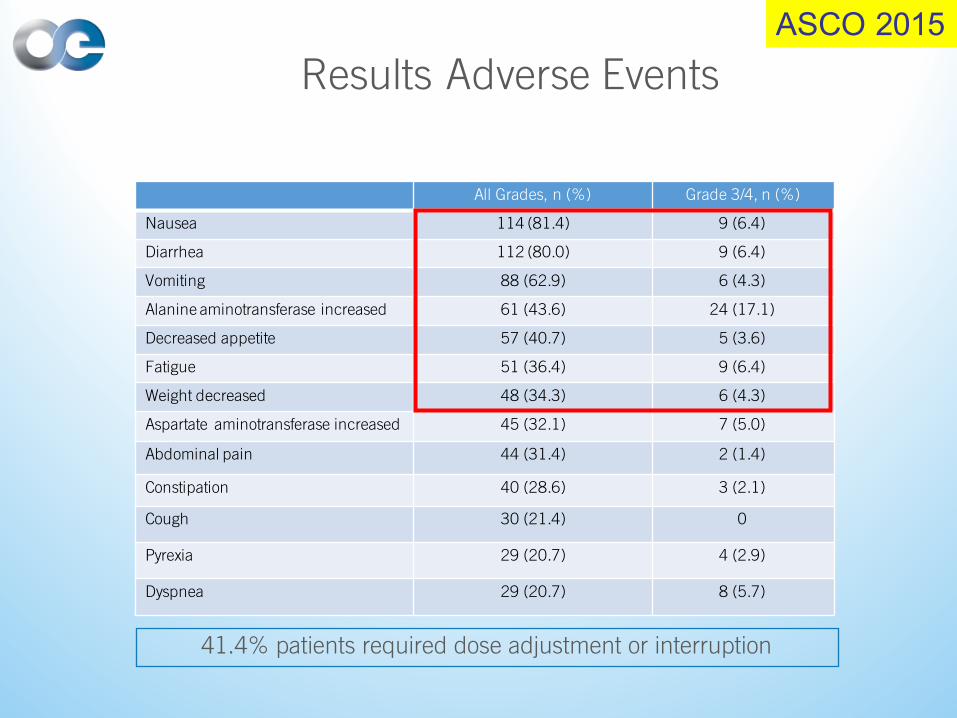
Results Adverse Events
All Grades, n (%) Grade 3/4, n (%)
Nausea 114 (81.4) 9 (6.4)
Diarrhea 112 (80.0) 9 (6.4)
Vomiting 88 (62.9) 6 (4.3)
Alanine aminotransferase increased 61 (43.6) 24 (17.1)
Decreased appetite 57 (40.7) 5 (3.6)
Fatigue 51 (36.4) 9 (6.4)
Weight decreased 48 (34.3) 6 (4.3)
Aspartate aminotransferase increased 45 (32.1) 7 (5.0)
Abdominal pain 44 (31.4) 2 (1.4)
Constipation 40 (28.6) 3 (2.1)
Cough 30 (21.4) 0
Pyrexia 29 (20.7) 4 (2.9)
Dyspnea 29 (20.7) 8 (5.7)
41.4% patients required dose adjustment or interruption
ASCO 2015
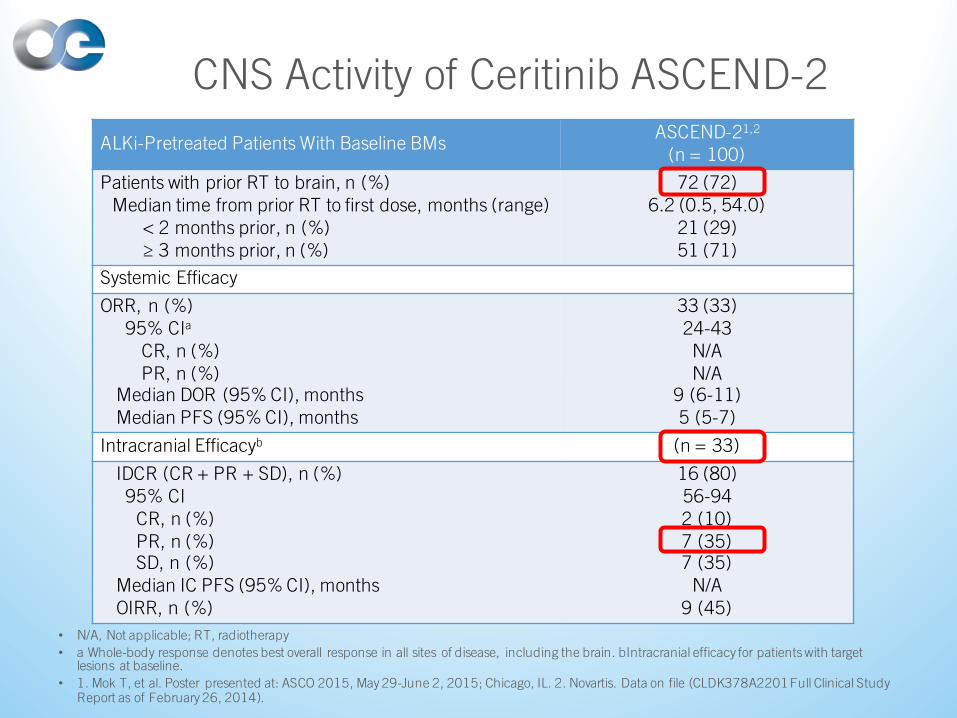
CNS Activity of Ceritinib ASCEND-2
• N/A, Not applicable; RT, radiotherapy
• a Whole-body response denotes best overall response in all sites of disease, including the brain. bIntracranial efficacy for patients with target lesions at baseline.
• 1. Mok T, et al. Poster presented at: ASCO 2015, May 29-June 2, 2015; Chicago, IL. 2. Novartis. Data on file (CLDK378A2201 Full Clinical Study Report as of February 26, 2014).
ALKi-Pretreated Patients With Baseline BMsASCEND-21,2
(n = 100)
Patients with prior RT to brain, n (%)Median time from prior RT to first dose, months (range)
< 2 months prior, n (%)≥ 3 months prior, n (%)
72 (72)6.2 (0.5, 54.0)
21 (29)51 (71)
Systemic Efficacy
ORR, n (%) 95% CIa
CR, n (%)PR, n (%)
Median DOR (95% CI), months Median PFS (95% CI), months
33 (33)24-43N/AN/A
9 (6-11)5 (5-7)
Intracranial Efficacyb (n = 33)
IDCR (CR + PR + SD), n (%) 95% CI
CR, n (%) PR, n (%)SD, n (%)
Median IC PFS (95% CI), monthsOIRR, n (%)
16 (80)56-942 (10)7 (35)7 (35)
N/A9 (45)
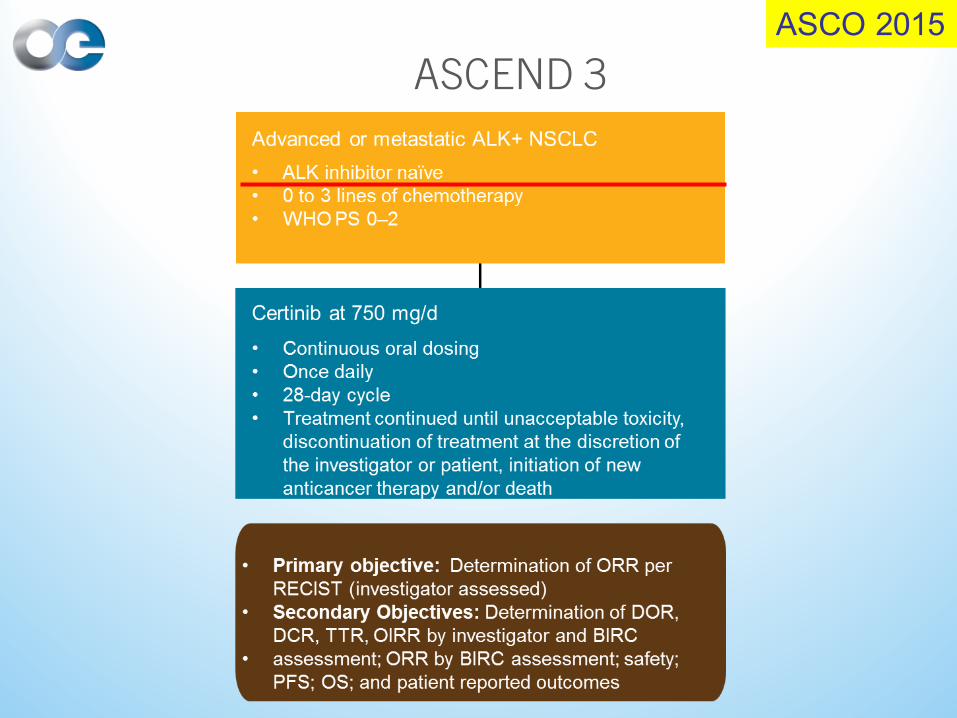
ASCEND 3
ASCO 2015
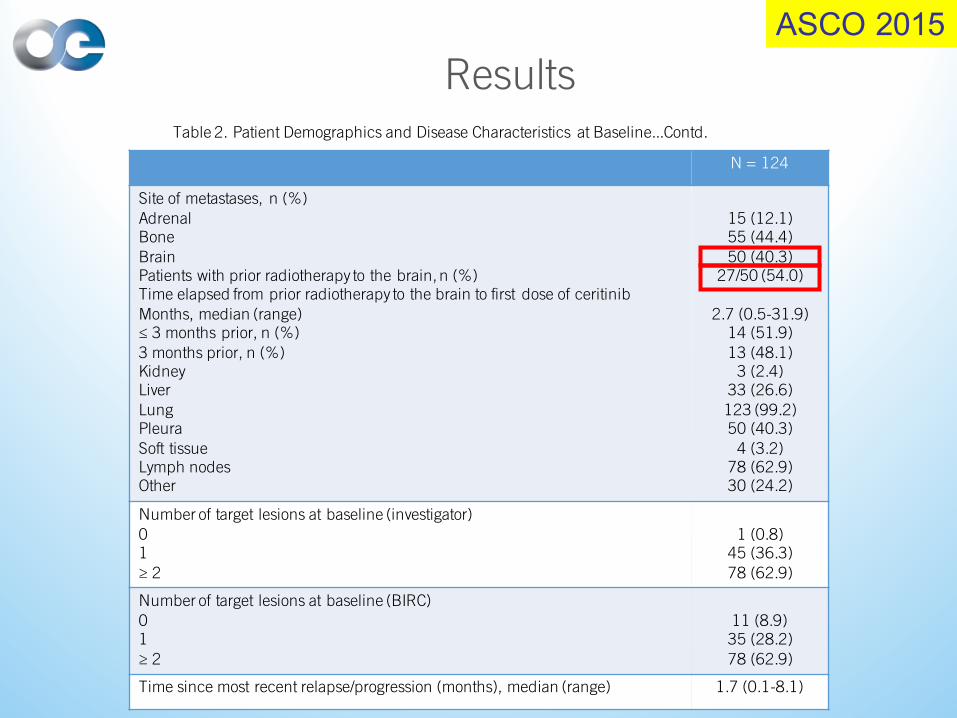
ResultsTable 2. Patient Demographics and Disease Characteristics at Baseline...Contd.
N = 124
Site of metastases, n (%)AdrenalBoneBrainPatients with prior radiotherapy to the brain, n (%)Time elapsed from prior radiotherapy to the brain to first dose of ceritinibMonths, median (range)≤ 3 months prior, n (%)3 months prior, n (%)KidneyLiverLungPleuraSoft tissueLymph nodesOther
15 (12.1)55 (44.4)50 (40.3)
27/50 (54.0)
2.7 (0.5-31.9)14 (51.9)13 (48.1)
3 (2.4)33 (26.6)123 (99.2)50 (40.3)
4 (3.2)78 (62.9)30 (24.2)
Number of target lesions at baseline (investigator)01≥ 2
1 (0.8)45 (36.3)78 (62.9)
Number of target lesions at baseline (BIRC)01≥ 2
11 (8.9)35 (28.2)78 (62.9)
Time since most recent relapse/progression (months), median (range) 1.7 (0.1-8.1)
ASCO 2015
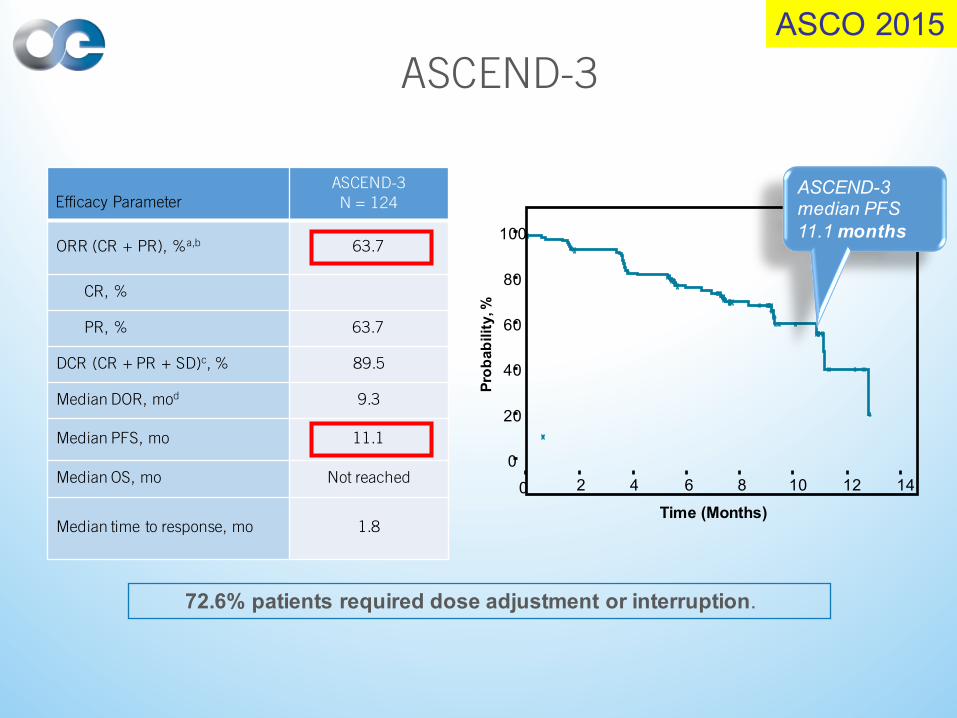
Efficacy ParameterASCEND-3N = 124
ORR (CR + PR), %a,b 63.7
CR, %
PR, % 63.7
DCR (CR + PR + SD)c, % 89.5
Median DOR, mod 9.3
Median PFS, mo 11.1
Median OS, mo Not reached
Median time to response, mo 1.8
Prob
abili
ty, %
ASCEND-3ASCO 2015
100
80
60
40
20
0
Time (Months)
0 2 4 6 8 10 1412
72.6% patients required dose adjustment or interruption.
ASCEND-3 median PFS 11.1months
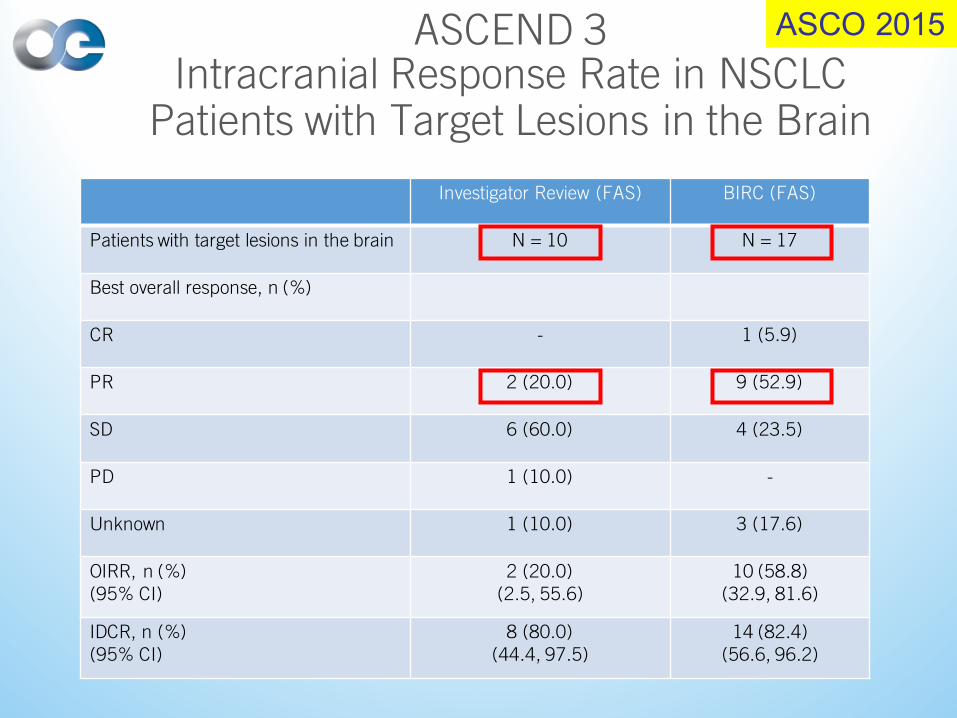
ASCEND 3Intracranial Response Rate in NSCLC
Patients with Target Lesions in the Brain
Investigator Review (FAS) BIRC (FAS)
Patients with target lesions in the brain N = 10 N = 17
Best overall response, n (%)
CR - 1 (5.9)
PR 2 (20.0) 9 (52.9)
SD 6 (60.0) 4 (23.5)
PD 1 (10.0) -
Unknown 1 (10.0) 3 (17.6)
OIRR, n (%)(95% CI)
2 (20.0)(2.5, 55.6)
10 (58.8)(32.9, 81.6)
IDCR, n (%)(95% CI)
8 (80.0)(44.4, 97.5)
14 (82.4)(56.6, 96.2)
ASCO 2015
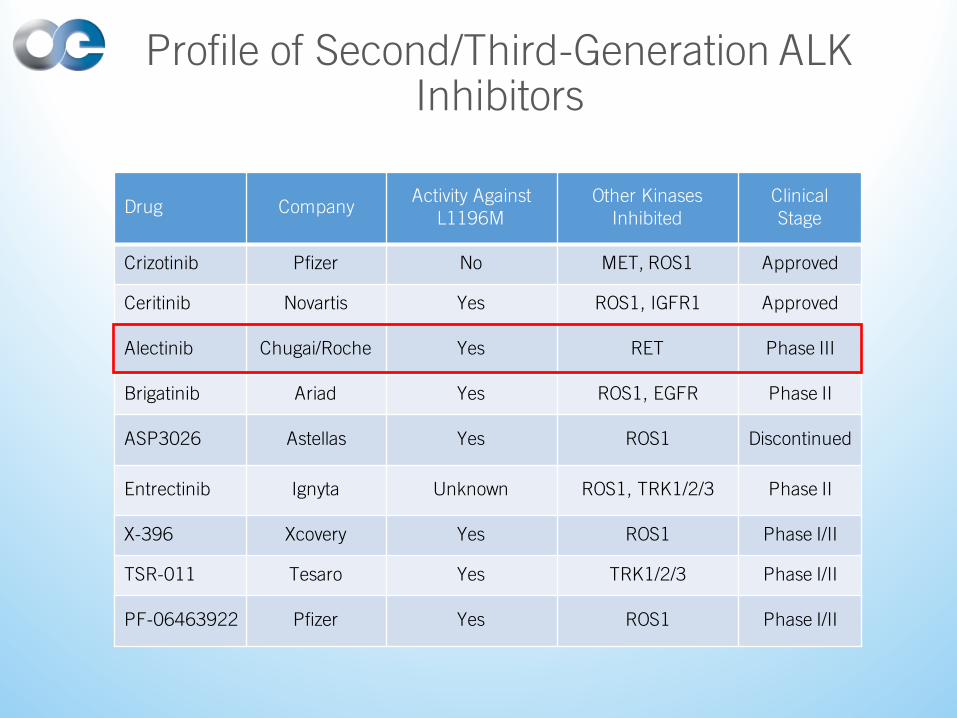
Drug CompanyActivity Against
L1196MOther Kinases
InhibitedClinicalStage
Crizotinib Pfizer No MET, ROS1 Approved
Ceritinib Novartis Yes ROS1, IGFR1 Approved
Alectinib Chugai/Roche Yes RET Phase III
Brigatinib Ariad Yes ROS1, EGFR Phase II
ASP3026 Astellas Yes ROS1 Discontinued
Entrectinib Ignyta Unknown ROS1, TRK1/2/3 Phase II
X-396 Xcovery Yes ROS1 Phase I/II
TSR-011 Tesaro Yes TRK1/2/3 Phase I/II
PF-06463922 Pfizer Yes ROS1 Phase I/II
Profile of Second/Third-Generation ALK Inhibitors
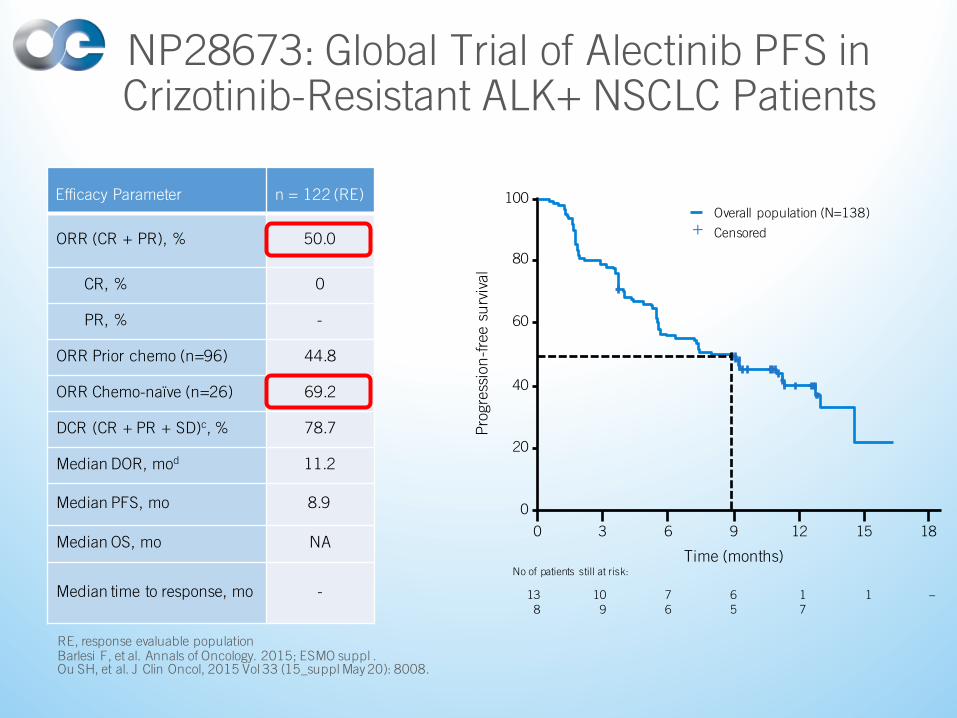
NP28673: Global Trial of Alectinib PFS in Crizotinib-Resistant ALK+ NSCLC Patients
RE, response evaluable populationBarlesi F, et al. Annals of Oncology. 2015; ESMO suppl .Ou SH, et al. J Clin Oncol, 2015 Vol 33 (15_suppl May 20): 8008.
Time (months)
76
–109
138
65
No of patients still at risk:
17
1
Pro
gres
sion
-fre
e su
rviv
al
100
6 1830
80
60
40
20
0
9
Overall population (N=138)
Censored+
12 15
Efficacy Parameter n = 122 (RE)
ORR (CR + PR), % 50.0
CR, % 0
PR, % -
ORR Prior chemo (n=96) 44.8
ORR Chemo-naïve (n=26) 69.2
DCR (CR + PR + SD)c, % 78.7
Median DOR, mod 11.2
Median PFS, mo 8.9
Median OS, mo NA
Median time to response, mo -
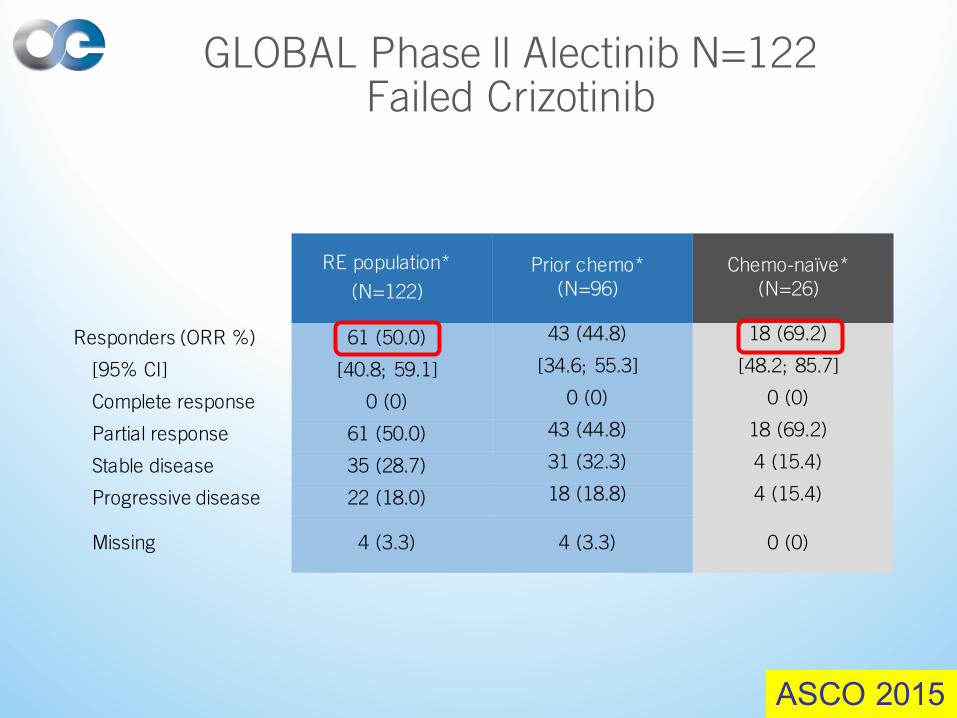
GLOBAL Phase ll Alectinib N=122Failed Crizotinib
RE population*
(N=122)
Prior chemo*(N=96)
Chemo-naïve*(N=26)
Responders (ORR %) 61 (50.0) 43 (44.8) 18 (69.2)
[95% CI] [40.8; 59.1] [34.6; 55.3] [48.2; 85.7]
Complete response 0 (0) 0 (0) 0 (0)
Partial response 61 (50.0) 43 (44.8) 18 (69.2)
Stable disease 35 (28.7) 31 (32.3) 4 (15.4)
Progressive disease 22 (18.0) 18 (18.8) 4 (15.4)
Missing 4 (3.3) 4 (3.3) 0 (0)
ASCO 2015

Long Median PFS in Crizotinib-Resistant ALK+ NSCLC Patients
ASCO 2015
Pro
gres
sion
-fre
e su
rviv
al
100
Time (months)
6 1830
80
60
40
20
0
9
76 –109138 65Overall population
No. at risk:
Overall population (N=138)Censored+
12
17
15
1
Median PFS 8.9 months (95% CI 5.6–11.3)
58% of patients with event
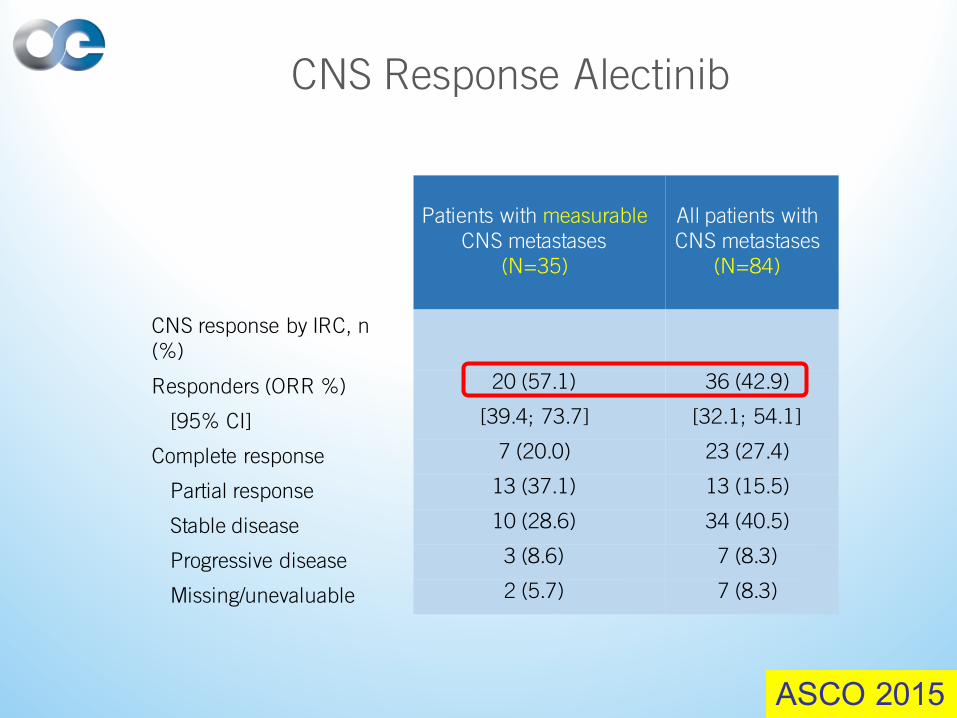
CNS Response Alectinib
Patients with measurableCNS metastases
(N=35)
All patients with CNS metastases
(N=84)
CNS response by IRC, n (%)
Responders (ORR %) 20 (57.1) 36 (42.9)
[95% CI] [39.4; 73.7] [32.1; 54.1]
Complete response 7 (20.0) 23 (27.4)
Partial response 13 (37.1) 13 (15.5)
Stable disease 10 (28.6) 34 (40.5)
Progressive disease 3 (8.6) 7 (8.3)
Missing/unevaluable 2 (5.7) 7 (8.3)
ASCO 2015
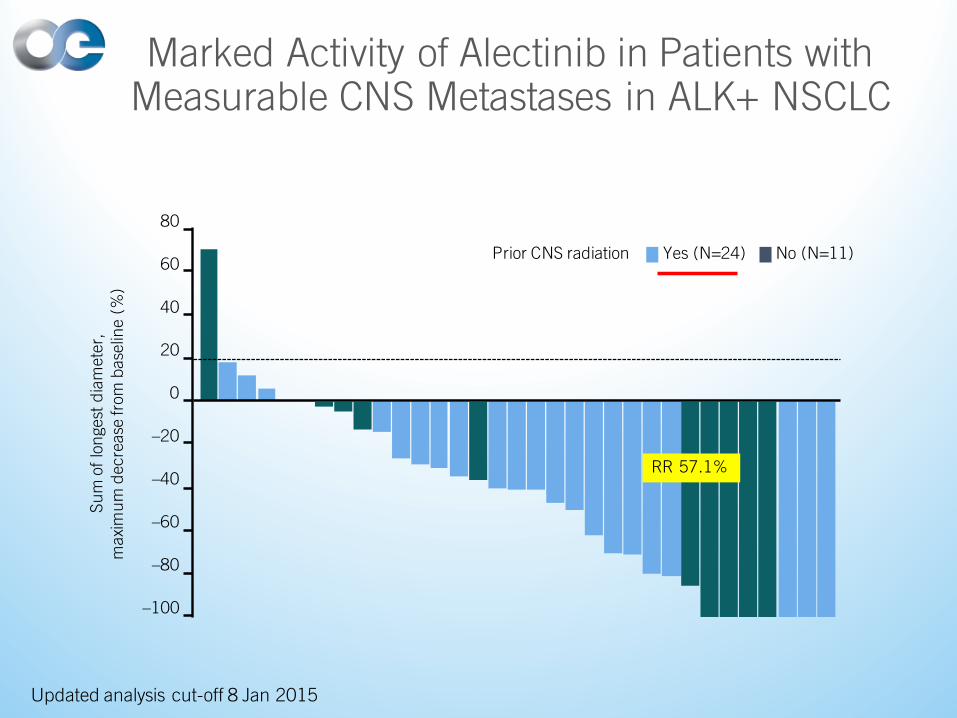
Marked Activity of Alectinib in Patients with Measurable CNS Metastases in ALK+ NSCLC
Updated analysis cut-off 8 Jan 2015
Sum
of l
onge
st d
iam
eter
, m
axim
um d
ecre
ase
from
bas
elin
e (%
)
60
–20
–40
–100
Prior CNS radiation Yes (N=24) No (N=11)
40
20
0
–60
–80
80
RR 57.1%
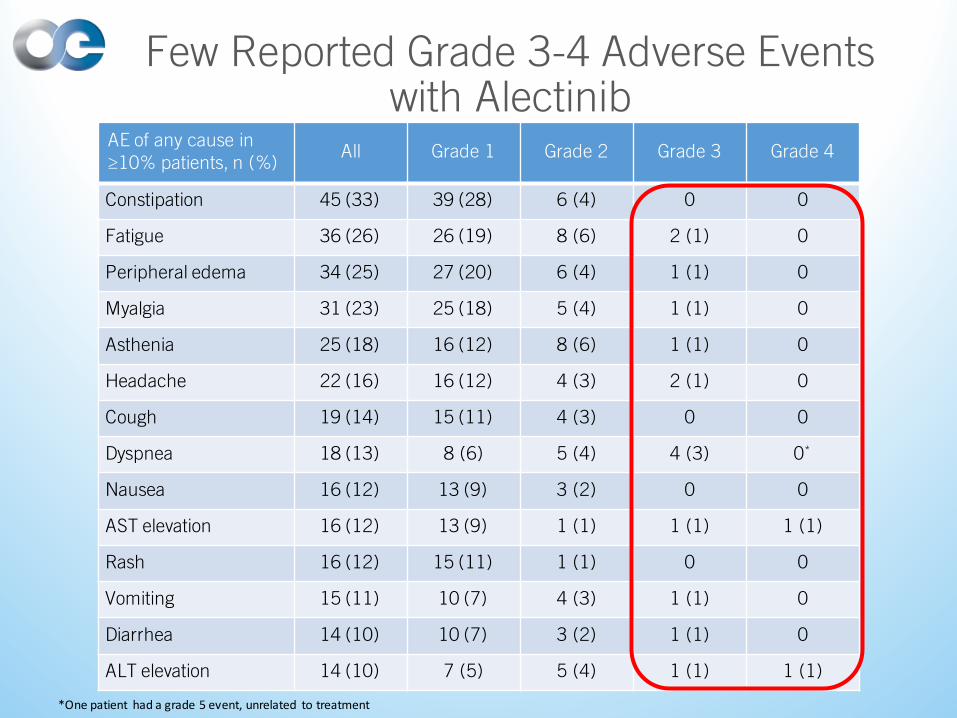
AE of any cause in ≥10% patients, n (%)
All Grade 1 Grade 2 Grade 3 Grade 4
Constipation 45 (33) 39 (28) 6 (4) 0 0
Fatigue 36 (26) 26 (19) 8 (6) 2 (1) 0
Peripheral edema 34 (25) 27 (20) 6 (4) 1 (1) 0
Myalgia 31 (23) 25 (18) 5 (4) 1 (1) 0
Asthenia 25 (18) 16 (12) 8 (6) 1 (1) 0
Headache 22 (16) 16 (12) 4 (3) 2 (1) 0
Cough 19 (14) 15 (11) 4 (3) 0 0
Dyspnea 18 (13) 8 (6) 5 (4) 4 (3) 0*
Nausea 16 (12) 13 (9) 3 (2) 0 0
AST elevation 16 (12) 13 (9) 1 (1) 1 (1) 1 (1)
Rash 16 (12) 15 (11) 1 (1) 0 0
Vomiting 15 (11) 10 (7) 4 (3) 1 (1) 0
Diarrhea 14 (10) 10 (7) 3 (2) 1 (1) 0
ALT elevation 14 (10) 7 (5) 5 (4) 1 (1) 1 (1)
Few Reported Grade 3-4 Adverse Events with Alectinib
*Onepatient hadagrade5event,unrelated totreatment
Discussion Link
• ALK positive cases – how do you approach, timing of testing, first and second line therapies discussion questions to be monitored by faculty
Back to Case
• Pt has received palliative XRT to symptomatic spine met.
• Pt is ALK +ve. Given concerns regarding multiple brain mets, patient undergoes whole brain radiotherapy.
• Crizotinib is then started.
• Patient gets clear radiographic response and remains stable until 8 months later, when the primary lung tumor starts to grow. The lung tumor initially decreased in size to 1cm, and then has grown now to 3 cm over 2 consecutive CT scans, with no other disease progressing anywhere else.
Back to Case
What to do now?
1. Continue with crizotinib despite progression
2. Stop crizotinib and switch to another systemic therapy
3. Treat/eradicate the solitary progressing tumor with local ablative therapy and then stay on crizotinib
Treating “Oligo-Progression”
• When one or “a few” tumors are progressing while all other metastases are controlled with a systemic therapy strategy, one option is to locally treat the rogue progressing tumors and then stay on the same systemic therapy.
• Goal is to remain on the same systemic therapy for as long as possible, especially when the majority of the tumors are responding or under control.
• No high level evidence yet to support such an approach.
Treating “Oligo-Progression”
• One retrospective study in ALK+ve NSCLC patients on crizotinib whose oligo-progressive tumors were treated with stereotactic body radiotherapy (SBRT) suggests that some patients may derive significant added progression free survival while staying on crizotinib, thus delaying the need to switch systemic therapy.
SUMMARY:
o Median PFS in those who received SBRT for oligo-progressive tumors was 14 mos, compared to 7.2 mos in those not eligible for SBRT because of more diffuse progression
o Median overall time remaining on crizotinib for those receiving SBRT for oligo-progression was 28 mos
o Patients remaining on crizotinib > 12 mos had significantly higher overall survival than those on crizotinib < 12 mos.
Conclusions
• Presently only EGFR and ALK testing have utility in treatment decision making in NSCLC patients
• These tests should be performed mainly on tumors with non-squamous histology
• Individual centre should develop a multidisciplinary approach to implement molecular testing algorithms
• Multiplex testing by next generation sequencing can resolve much of complexity of molecular testing
Conclusions
• Treatment of brain metastases in mutation +ve patients should include a multi-disciplinary assessment and may include systemic targeted agent alone in select patients
• Treatment of “oligo-progression” while on systemic therapy may include the use of local ablative therapy (like SBRT) to eradicate the “rogue” metastases and then continuing same systemic therapy