macrophage activation syndrome children systemic juvenile ...arlar.org/wp-content/uploads/2014/adel...
TRANSCRIPT


Macrophage Activation Syndrome in
Children with
Systemic Juvenile Rheumatoid Arthritis
Adel wahadneh MD Consultant Pediatric Immunologist and
Rheumatologist QRCH-KHMC-JORDAN
2

A 7 year male patient Diagnosis of systemic onset JIA was made 3 years ago Controlled on: Prednisolne 5 mg/day, Methotrexate 20 mg/week, Etanercept 20 mg/week 12 months ago, admitted with unremitting fever, petechial rash, nasal epistaxis, hepatosplenomegaly Patient’s data as follow
3

34
36
38
40
42
W1
W2
W3
W4
M1
M2
M3
M4
W2
1
W2
2
W2
3
W2
4
FEVER
0
5000
10000
15000
20000
25000
30000
1 2 3 4 5 6 7 8 9 101112
WBC
0
50
100
150
1 2 3 4 5 6 7 8 9 10 11 12
ESR
4

0
1000
2000
3000
4000
5000
1 2 3 4 5 6 7 8 9 10 11 12
CRP
FERRITTEN
0
2
4
6
8
1 2 3 4 5 6 7 8 9 10 11 12
FIBRINOGEN
0
500000
1000000
1500000
1 2 3 4 5 6 7 8 9 10 11 12
PLATLETS
5

0
100
200
300
400
500
1 2 3 4 5 6 7 8 9 101112
AST
ALT
TG
Extensive work up for infection was inconclusive
6

Diagnosis : Macrophage Activation Syndrome
Clinical and laboratory improvement were observed during with corticosteroid and cyclosporine therapy
7

8

9

10
Occult macrophage activation syndrome in patients
with systemic juvenile idiopathic arthritis (Behrens EM
et al. J Rheumatol 2007;34:1133-8)
Retrospective review of 15 patients with syst JIA who
underwent BM aspiration within initial diagnostic workup
Eight of 15 (53%) patients had BM aspirate suggestive of
MAS
Two patients were diagnosed clinically with MAS
Three patients had frank hemophagocytosis, only 1 of
whom was diagnosed with MAS clinically
Suggestion: MAS may be an integral part of the spectrum
of syst JIA, ranging from its most severe, life-threatening
form to its mild, occult form manifest only by biochemical
abnormalities and BM hemophagocytosis
11

Preliminary diagnostic guidelines for
MAS complicating systemic JIA
Laboratory criteria
• Decreased PLT (≤ 262 x 109)
• Elevated GOT/AST (> 59 mU/L)
• Hypofibrinogenemia (≤ 2.5 g/L)
• Decreased WBC (≤ 4.0 x 109/L)
Histopathologic criterion
Hemophagocytosis in the bone marrow
Clinical criteria
• Hemorrhages (purpura, easy bruising, mucosal bleeding)
• CNS dysfunction (irritability, disorientation, lethargy, headache, seizures, coma)
• Hepatomegaly (≥ 3 cm below the costal arch)
Diagnostic rule: The diagnosis of macrophage activation syndrome requires the presence of any 2 or more the following laboratory criteria or 2 or more of the following clinical criteria: A BM aspirate for the demonstration of macrophage hemophagocytosis may be required only in doubtful cases
Ravelli A et al. J Pediatr 2005;146:598-604 12
clinical discriminators DOR
Hemorrhages 67
central nervous system dysfunction 63
laboratory discriminators DOR
Decreased platelet count 1092
increased aspartate aminotransferase 247
leukopenia 70
hypofibrinogenemia 165
The best separation between patients and control subjects
occurred when any 2 or more laboratory criteria were
simultaneously present
1309
The second best performance was provided by the presence of
any 2, 3, or more clinical and/or laboratory criteria.
765 and
743
respectively

application of the HLH-2004 protocol to MAS/HLH
secondary to sJIA may be imperfect.
13

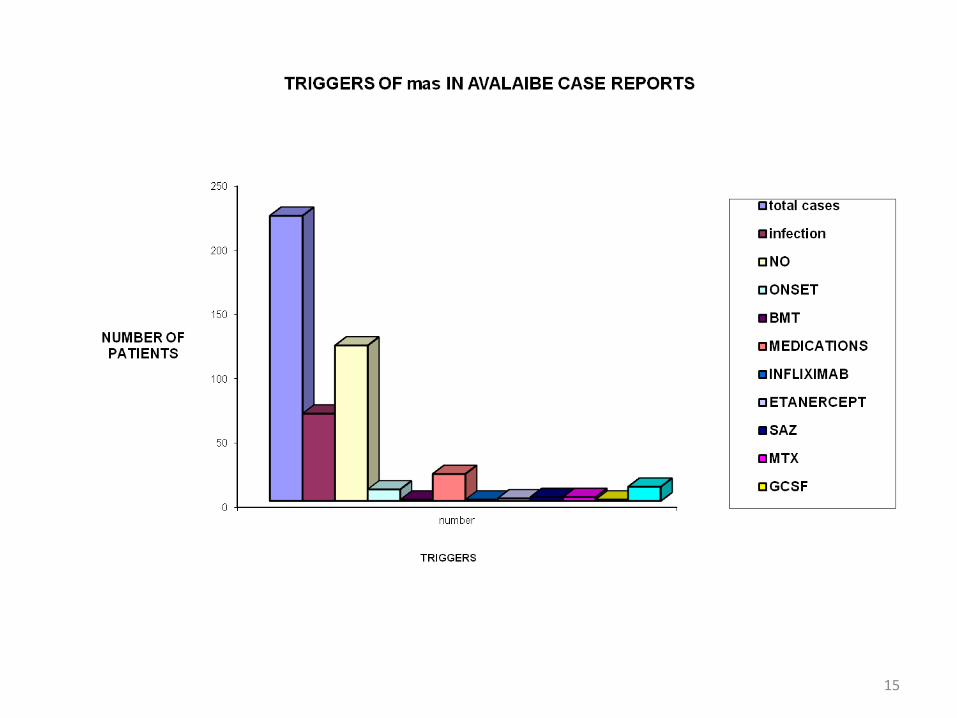
0
50
100
150
200
250
NO. OF MAS CASES IN DIFFERENT RHEUMATIC DISEASES
No,cases
1. Incidence and prevalence unknown, Probably more common than
previously though(7 of 103 diagnosed with soJRA developed MAS at some point
in their illness.)
2. Approximately 100 cases reported in the literature
3. Most commonly an early complication of active disease 14
15

26) STERBA G, STERBA Y, STEMPEL C, BLANK J, AZOR E, GOMEZ L. Macrophage activation syndrome induced by etanercept in a patient with systemic sclerosis. Isr Med Assoc J 2010; 12: 443-445. 29) CUSINI A, GUNTHARD HF, STUSSI G, SCHWARZ U, FEHR T, GRUETER E, MEERBACH A, BOSSART W, SCHAER DJ, RUDIGER A. Hemophagocytic syndrome caused by primary herpes simplex virus 1 infection: report of a first case. Infection 2010; 38: 423-426. 61) PEREZ-DE PEDRO I, MIRANDA-CANDON I, CAMPS-GARCIA MT, GOMEZ-HUELGAS R. [Hemophagocytic syndrome in adult Still disease after initiation of sulfasalazine]. Rev Clin Esp 2010; 210: 251-252. 66) ARLET JB, LE TH, MARINHO A, AMOURA Z, WECHSLER B, PAPO T, PIETTE JC. Reactive haemophagocytic syndrome in adult-onset Still's disease: a report of six patients and a review of the literature. Ann Rheum Dis 2006; 65: 1596-1601. 68) GIANELLA S, SCHAER DJ, SCHWARZ U, KURRER M, HEPPNER FL, FEHR J, SEEBACH JD. Retinal microangiopathy and rapidly fatal cerebral edema in a patient with adult-onset Still's disease and concurrent macrophage activation syndrome. Am J Hematol 2008; 83: 424-427. 69) STERN A, RILEY R, BUCKLEY L. Worsening of macrophage activation syndrome in a patient with adult onset Still's disease after initiation of Etanercept therapy. J Clin Rheumatol 2001; 7: 252-256. 73) AGARWAL S, MOODLEY J, AJANI GOEL G, THEIL KS,MAHMOOD SS, LANG RS. A rare trigger for macrophage activation syndrome. Rheumatol Int 2011; 31: 405-407. 74) ODA Y, URUSHIDANI Y, OOI S, ENDOH A, NAKAMURA R,ADACHI K, FUKUSHIMA H. Hemophagocytic lymphohistiocytosis in a rheumatoid arthritis patient treated with infliximab. Intern Med 2012; 51: 655-657. 75) AOUBA A, DE BANDT M, ASLANGUL E, ATKHEN N, PATRIB. Haemophagocytic syndrome in a rheumatoid
arthritis patient treated with infliximab. Rheumatology (Oxford) 2003; 42: 800-802. 76) SANDHU C, CHESNEY A, PILIOTIS E, BUCKSTEIN R, KOREN S. Macrophage activation syndrome after Etanercept treatment. J Rheumatol 2007; 34: 241-242. 77) TSUBOI H, IWATA H, NAMPEI A, MATSUSHITA M, SHI K. Hemophagocytic syndrome in a patient with rheumatoid arthritis. Mod Rheumatol 2011; 21: 532-535. 83) ARAKI D, FUJII H, MATSUMURA M, YAMAGISHI M, YACHIE A, KAWANO M. Etanercept-induced lupus accompanied by hemophagocytic syndrome. Intern Med 2011; 50: 1843-1848. 89) SAWAR H, ESPINOZA LR, GEDALIA A. Macrophage activation syndrome and etanercept in children with systemic juvenile rheumatoid arthritis. J Rheumatol 2004; 31: 623; author reply 623-624. 98) NADIA EA, CARVALHO JF, BONFA E, LOTITO AP, SILVA CA. Macrophage activation syndrome associated with etanercept in a child with systemic onset juvenile idiopathic arthritis. Isr Med Assoc J 2009;11: 635-636. 99) RAMANAN AV, SCHNEIDER R. Macrophage activation syndrome following initiation of etanercept in a child with systemic onset juvenile rheumatoid arthritis. J Rheumatol 2003; 30: 401-403. 128) TRONCOSO MARINO A, CAMPELO SANCHEZ E, MARTINEZ LOPEZ DE CASTRO N, INARAJA BOBO MT. Haemophagocytic syndrome and paradoxical reaction to tuberculostatics after treatment with infliximab. Pharm World Sci 2010; 32: 117-119.
In 20 cases HLH might have been triggered by immunosuppressive treatment of the rheumatic condition, including adalimumab/, infliximab,etanercept, leflunomide, sulfasalazine, azathioprine, methotrexate
It is possible that immunosuppression
induced by anti-TNF-á treatment may favor
the occurrence of serious infections leading,
in turn, to HLH.
16

Pathogenesis
• Central question: is there an underlying abnormality of the immune
response that contributes to lack of control of an exaggerated
immune response?
• Starting point: strong clinical similarities with hemophagocytic
lymphohistiocytosis (HLH)
• Familial HLH: decreased NK and cytotoxic cell function often
secondary to mutations in the gene encoding perforin (PRF1), a protein that
mediates cytotoxic activity of NK and T cells. The number of NK
cells is usually normal
• Virus-associated HLH: very low or absent cytolitic NK cell activity
related to profoundly decreased number of NK cells rather than impaired
perforin expression. NK function may completely recover after
resolution of acute phase 17

18
19

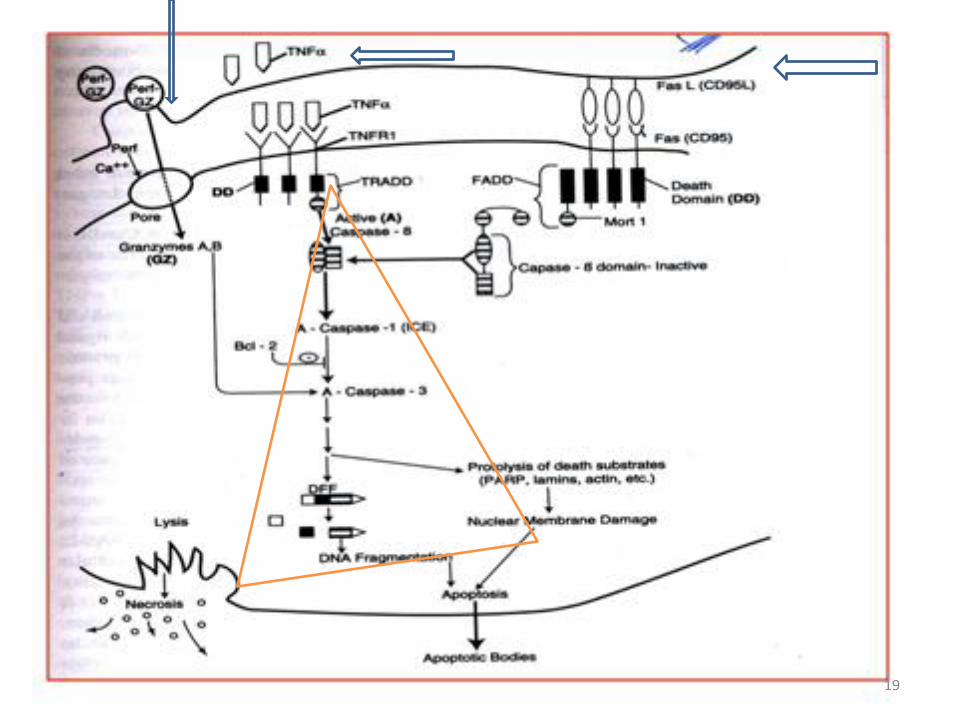
Role of Perforin in the Cytotoxic Response
The Mechanism of Action of Perforin - N Engl J Med 335 (22): 1651, 1996
20

21

Pathogenesis of Hemophagocytic Syndromes
Decreased
Perforin Expression
+ / -
Trigger
(Drug or infection)
Excessive
Macrophage Activation
Hypercytokinemia
End organ damage
22

23

24

25
26
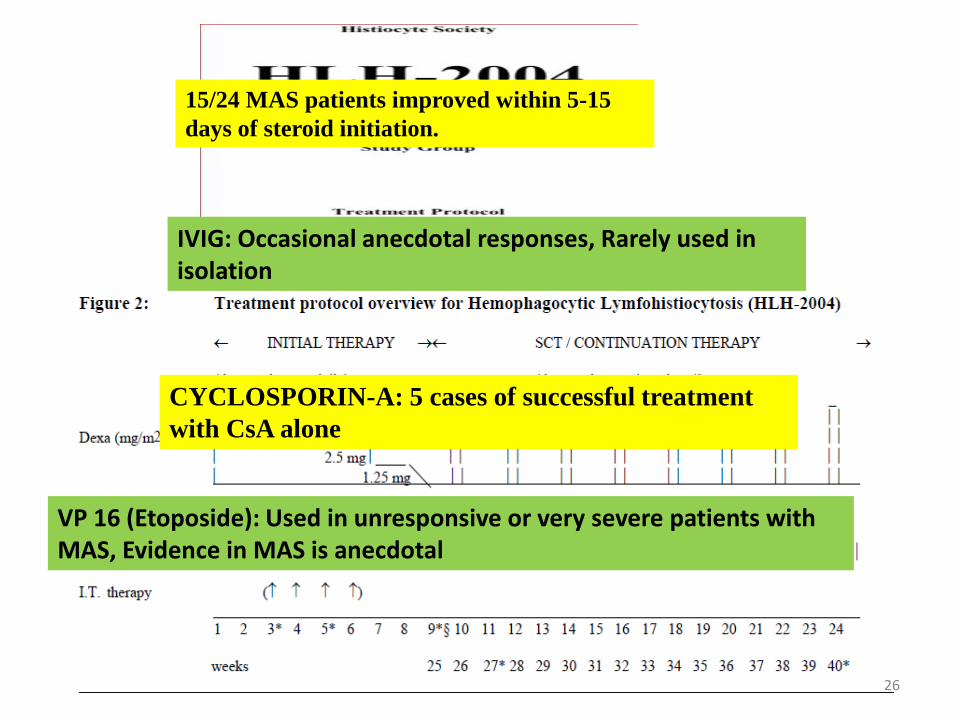
15/24 MAS patients improved within 5-15
days of steroid initiation.
IVIG: Occasional anecdotal responses, Rarely used in isolation
CYCLOSPORIN-A: 5 cases of successful treatment
with CsA alone
VP 16 (Etoposide): Used in unresponsive or very severe patients with MAS, Evidence in MAS is anecdotal

Med Sci Monit. 2008 Mar;14(3):RA27-36. Macrophage activation syndrome: a
frequent but under-diagnosed complication associated with rheumatic
diseases. Tristano AG
Treatment of MAS in patients with rheumatic diseases has not been standardized yet, but it commonly includes a variety of agents such as high-dose corticosteroids, cyclosporine, cyclophosphamide, etoposide, and intravenous immunoglobulin (IVIG).
Pediatr Blood Cancer. 2007 Feb;48(2):124-31. HLH-2004: Diagnostic and
therapeutic guidelines for hemophagocytic lymphohistiocytosis. Henter
JI,et al.
HLH-2004 chemo-immunotherapy includes etoposide, dexamethasone, cyclosporine A upfront and, in selected patients, intrathecal therapy with methotrexate and corticosteroids. Subsequent hematopoietic stem cell transplantation (HSCT) is recommended for patients with familial disease or molecular diagnosis, and patients with severe and persistent, or reactivated, disease.
27

Rheumatology (Oxford). 2001 Nov;40(11):1285-92. Reactive haemophagocytic
syndrome in children with inflammatory disorders. A retrospective study of
24 patients. Stéphan JL
immediate withdrawal of potentially triggering medications, anti-infective therapy when relevant, and urgent immunosuppressive treatment, measures that are very often effective. Cyclosporin A may be the drug of choice.
J Pediatr. 1996 Nov;129(5):750-4. Efficacy of cyclosporine A in the
treatment of macrophage activation syndrome in juvenile arthritis:
report of five cases. Mouy R,
These observations underline the usefulness of cyclosporine A in this complication. The use of this drug may circumvent the need for increased doses of corticosteroids in some patients. The mechanism of action of cyclosporine A remains speculative, but these results indicate indirectly that T-helper lymphocytes may play a role in the pathogenesis of MAS.
28

J Pediatr. 1996 Feb;128(2):275-8. Macrophage activation syndrome in
systemic juvenile rheumatoid arthritis successfully treated with
cyclosporine. Ravelli A,
A macrophage activation syndrome, possibly related to methotrexate toxicity, developed in a boy with systemic juvenile rheumatoid arthritis. Corticosteroid administration was ineffective, whereas a prompt response to cyclosporine was observed. Two months later, Pneumocystis carinii pneumonia developed.
29

51) KIKUCHI H, YAMAMOTO T, ASAKO K, TAKAYAMA M, SHIRASAKI R, ONO Y. Etanercept for the treatment of intractable hemophagocytic syndrome with systemic lupus erythematosus. Mod Rheumatol 2011; 22: 308-311. 52) TAKAHASHI N, NANIWA T, BANNO S. Successful use of etanercept in the treatment of acute lupus hemophagocytic syndrome. Mod Rheumatol 2008; 18:72-75. 53) IDEGUCHI H, OHNO S, TAKASE K, HATTORI H, KIRINO Y,TAKENO M, ISHIGATSUBO Y. Successful treatment of refractory lupus-associated haemophagocytic lymphohistiocytosis with infliximab. Rheumatology (Oxford) 2007; 46: 1621-1622. 54) HENZAN T, NAGAFUJI K, TSUKAMOTO H, MIYAMOTO T, GONDO H, IMASHUKU S, HARADA M. Success with infliximab in treating refractory hemophagocytic lymphohistiocytosis. Am J Hematol 2006; 81: 59-61. 70) MAESHIMA K, ISHII K, IWAKURA M, AKAMINE M, HAMASAKI H, ABE I, HARANAKA M, TATSUKAWA H, YOSHIMATSU H. Adult-onset Still's disease with macrophage activation syndrome successfully treated with a combination of methotrexate and etanercept. Mod Rheumatol 2012; 22: 137-141. 93) CORTIS E, INSALACO A. Macrophage activation syndrome in juvenile idiopathic arthritis. Acta Paediatr Suppl 2006; 95: 38-41. 100) PRAHALAD S, BOVE KE, DICKENS D, LOVELL DJ, GROM AA. Etanercept in the treatment of macrophage
activation syndrome. J Rheumatol 2001; 28:2120-2124. 101) BRUCK N, SUTTORP M, KABUS M, HEUBNER G, GAHR M, PESSLER F. Rapid and sustained remission of systemic juvenile idiopathic arthritis-associated macrophage activation syndrome through treatment with anakinra and corticosteroids. J Clin Rheumatol 2011; 17: 23-27. 102) KELLY A, RAMANAN AV. A case of macrophage activation syndrome successfully treated with
anakinra. Nat Clin Pract Rheumatol 2008; 4:615-620.
In 18 cases biologicals were used for HLH treatment including infliximab in three cases etanercept in 13 cases, and Anakinra in two cases
30

Anakinra & MAS
– Lurati A et al. MAS during anakinra therapy in a child with systemic JIA. Pediatr Rheumatol Oline J 2005
– Commentary: The paradox of macrophage activation syndrome triggered by biologic medications. Pediatr Rheumatol
Oline J 2005
– On day 13 of treatment 2 patients presented laboratory features consistent with MAS
– Both patients discontinued anakinra and were treated with oral corticosteroids and Cyclosporin A, with rapid control of MAS
– Six months later, one patient was re-treated with anakinra for a relapse of his underlying disease and no signs of MAS were observed after 6 mo of follow-up
31

32

0
50
100
150
200
250
1
NUMBER OF PATIENTS
OUTCOME
EVOLUTION OF MAS IN REPORTED CASES
TOTAL
FAVOURABLE
DEATH
NR
33
MAS mortality estimated 8-22%

Hematopoietic stem cell transplantation as a curative treatment for primary Hemophagocytic Lymphohistiocytosis in children: Immunology group at Queen Rania Children’s Hospital Experience:
Primary diagnosis Fulfill criteria of
HLH
Initial treatment Engraftment and
chimerism
Immunreconstitution
Chediak
Higashi
Syndrome
COMPLETE HLH-2004 100% DONOR CURED/FULL
Chediak
Higashi
Syndrome
COMPLETE HLH-2004 100% DONOR CURED/FULL
Chediak
Higashi
Syndrome
COMPLETE HLH-2004 100% DONOR CURED/FULL
Griscelli
Syndrome type
II
COMPLETE HLH-2004 100% DONOR CURED/FULL
Griscelli
Syndrome type
II
COMPLETE HLH-2004 100% DONOR CURED/FULL
34

Key messages
1. MAS is a rare complication of childhood rheumatic disease 2. It is a potentially fulminant disorder, which may occur as part of the initial presentation of the rheumatic disease 3. An infective trigger may herald the onset of this complication in predisposed patients 4. Differentiation from a disease flare may be difficult, but is critical to ensure optimal outcome 5. An early and dramatic fall in platelet count is characteristic, with changes in WBC and haemoglobin being more variable early and common 6. Elevation in transaminases and coagulation abnormalities may not be present at onset of MAS 7. Bone marrow examination is supportive, but false negative reports occur as a result of sampling errors or the subtle nature of the disease 8. Multisystem involvement is a poor prognostic sign
35

36