main contents -...
TRANSCRIPT
1
Intestinal Communicable Diseases
Jiang Yong
Department of Pathology
West China Hospital
Sichuan University
Main contents
Intestinal Infections: Typhoid Fever;
Bacillary dysentery
Systemic Fungal Infections
Parasitosis: Amoebiasis;
Schistosomiasis
Basic properties of
communicable diseases
Inflammation
consistent with the basic laws of
inflammation:alteration,exudation
and proliferation
Epidemiology of communicable
diseases in China
Extinct:
Smallpox、Leprosy、Poliomyelitis
Controllable with increasing incidence:
Tuberculosis ; Syphilis
New-borne communicable diseases:
SARS; H7N9……
2
WHO:优先关注的传染病
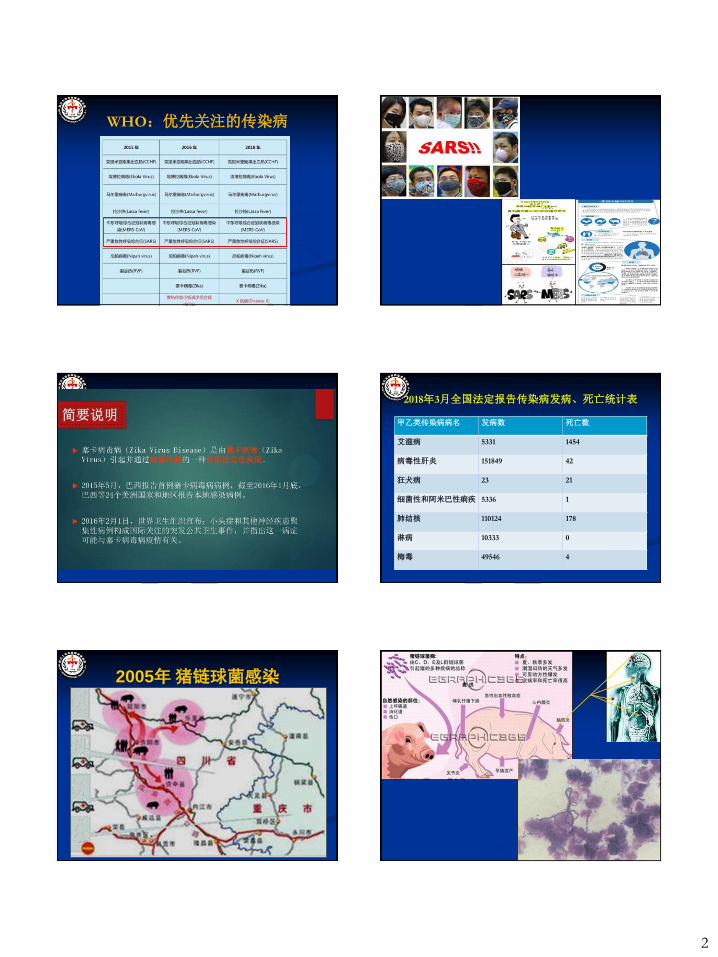
2018年3月全国法定报告传染病发病、死亡统计表
甲乙类传染病病名 发病数 死亡数
艾滋病 5331 1454
病毒性肝炎 151849 42
狂犬病 23 21
细菌性和阿米巴性痢疾 5336 1
肺结核 110124 178
淋病 10333 0
梅毒 49546 4
2005年 猪链球菌感染
3
Typhoid Fever
Acute communicable disease caused by bacillus
typhi
Acute proliferative inflammatory reaction
characterized by increase in macrophages in
Mononuclear Phagocyte System and by lesions of
lymphoid tissues at terminal ileum.
Clinical manifestations: Persistent fever,
bradycardia, hepatosplenomegaly, skin rash (rose
spots), and leukopenia.
Bacillus typhi (G-)
endotoxin
Flagella “H” antigen
Thallus “O” antigen
Widal reaction
Infection sources:
patients and bacteria-carrier
Routes of transmission :
fecal—oral route
Population
All are susceptible
and immunized from disease
Typhoid fever Pathogensis
Adsorption to intestinal mucosa after being swallowed , drained
by thoracic lymph duct to blood stream after invading into
lymphatic tissue of bowel. (bacteremia) multiply in
macrophages in different organs . (incubative stage)
second bacteremia (septicemia), generalized lesions
(medullary swelling stage) necrosis caused by bacteria
getting into intestine again from cholecyst bowel ulcer
cellular immunity upgraded and healed gradually
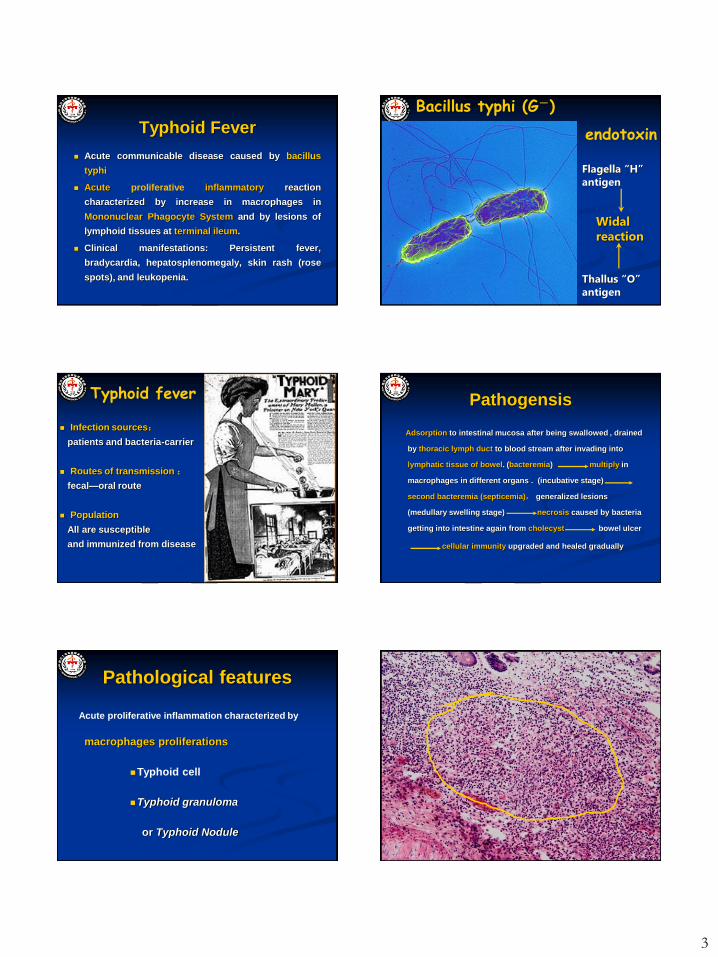
Pathological features
Acute proliferative inflammation characterized by
macrophages proliferations
Typhoid cell
Typhoid granuloma
or Typhoid Nodule
4
Typhoid granuloma
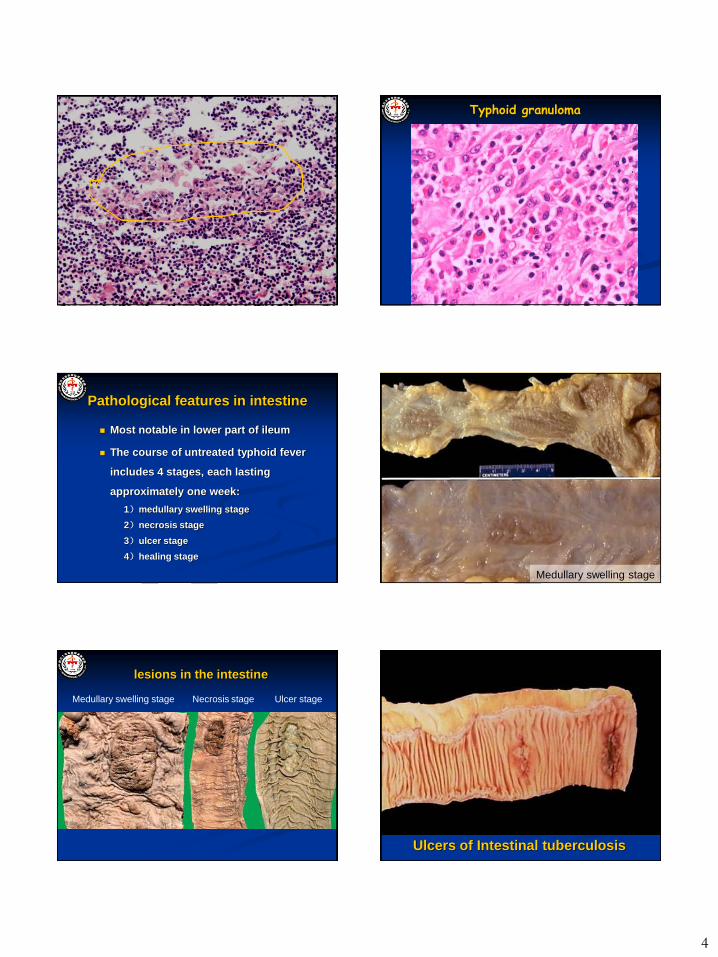
Pathological features in intestine
Most notable in lower part of ileum
The course of untreated typhoid fever
includes 4 stages, each lasting
approximately one week:
1)medullary swelling stage
2)necrosis stage
3)ulcer stage
4)healing stage
Medullary swelling stage
Medullary swelling stage Necrosis stage Ulcer stage
lesions in the intestine
Ulcers of Intestinal tuberculosis
5
How to detect pathogens in different stages?
Other lesions in Mononuclear Phagocyte System
Enlargement of lymph nodes ,liver ,spleen and bone marrow
Other lesions in other organs
heart—toxic myocarditis
skin—rose spot
cholecyst—to carry bacteria for a long term, important source of
infection
kidney—immune complexing nephritis
muscle—coagulative necrosis(cerosis)
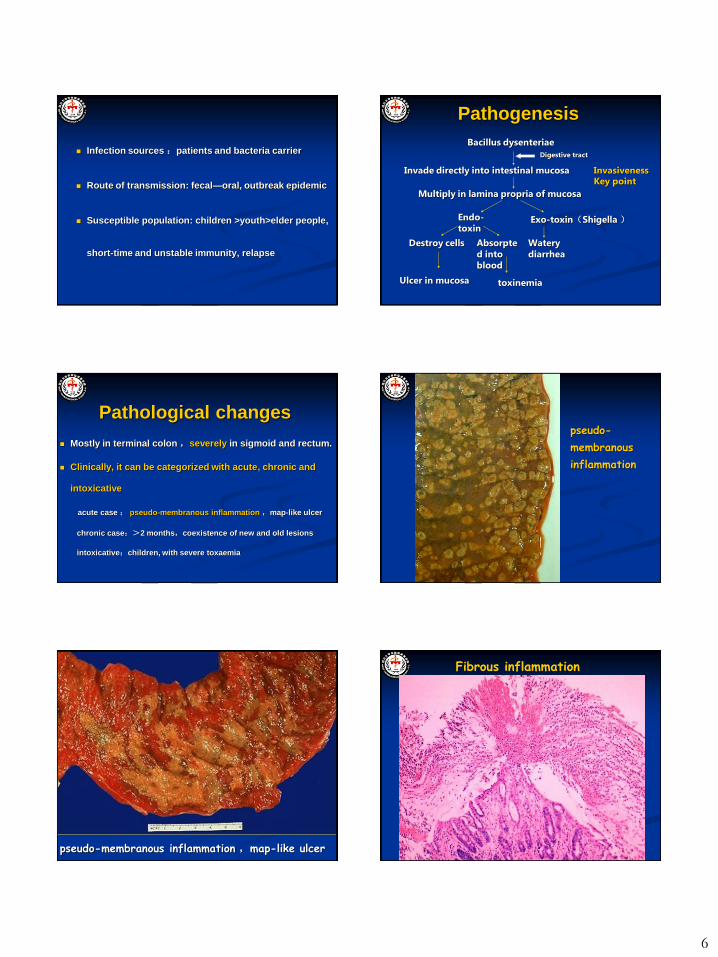
Typhoid rose spot Outcome and complications
Most can heal with strong immunity
Complications
Entero-hemorrhage
Enteric perforation
Lobular pneumonia
Bacillary Dysentery
A common enteric communicable disease caused by
bacillus dysenteriae
Pathological changes are mostly limited to distal colon
Characterized by pseudo-membranous inflammation
caused by fibrous exudations .
Clinical manifestations: fever,abdominal pain,diarrhea,
Stool with blood stained mucus and pus,and tenesmus
6
Infection sources :patients and bacteria carrier
Route of transmission: fecal—oral, outbreak epidemic
Susceptible population: children >youth>elder people,
short-time and unstable immunity, relapse
Pathogenesis
Bacillus dysenteriae
Invade directly into intestinal mucosa
Multiply in lamina propria of mucosa
Endo-toxin
Exo-toxin(Shigella )
Destroy cells Absorpted into blood
toxinemia
Watery diarrhea
Ulcer in mucosa
Digestive tract
Invasiveness Key point
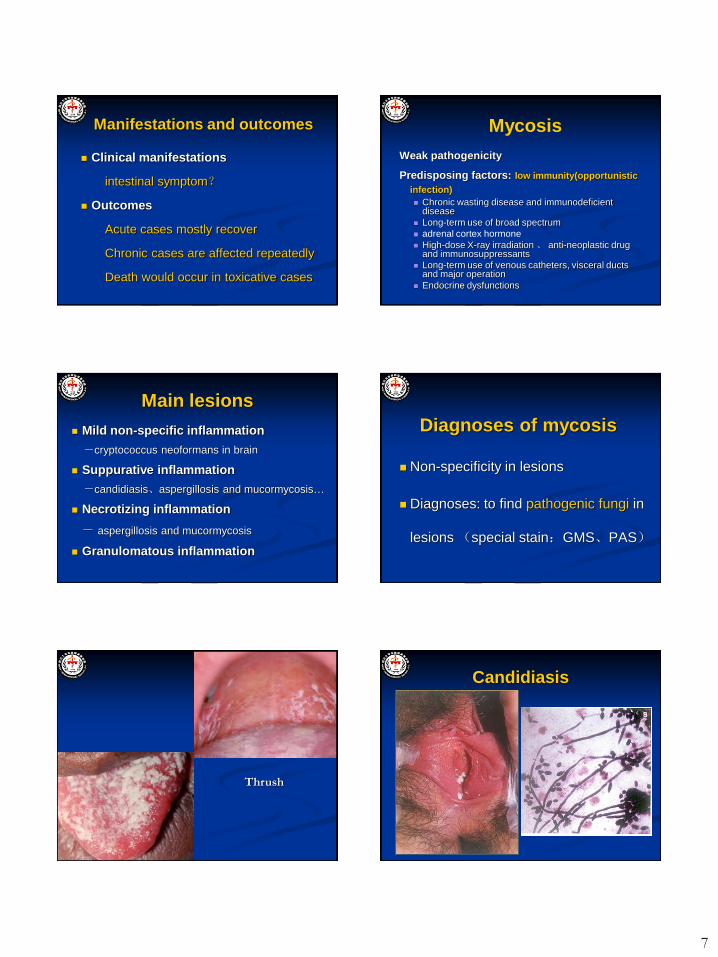
Pathological changes
Mostly in terminal colon ,severely in sigmoid and rectum.
Clinically, it can be categorized with acute, chronic and
intoxicative
acute case : pseudo-membranous inflammation ,map-like ulcer
chronic case:>2 months,coexistence of new and old lesions
intoxicative:children, with severe toxaemia
pseudo-
membranous
inflammation
pseudo-membranous inflammation ,map-like ulcer
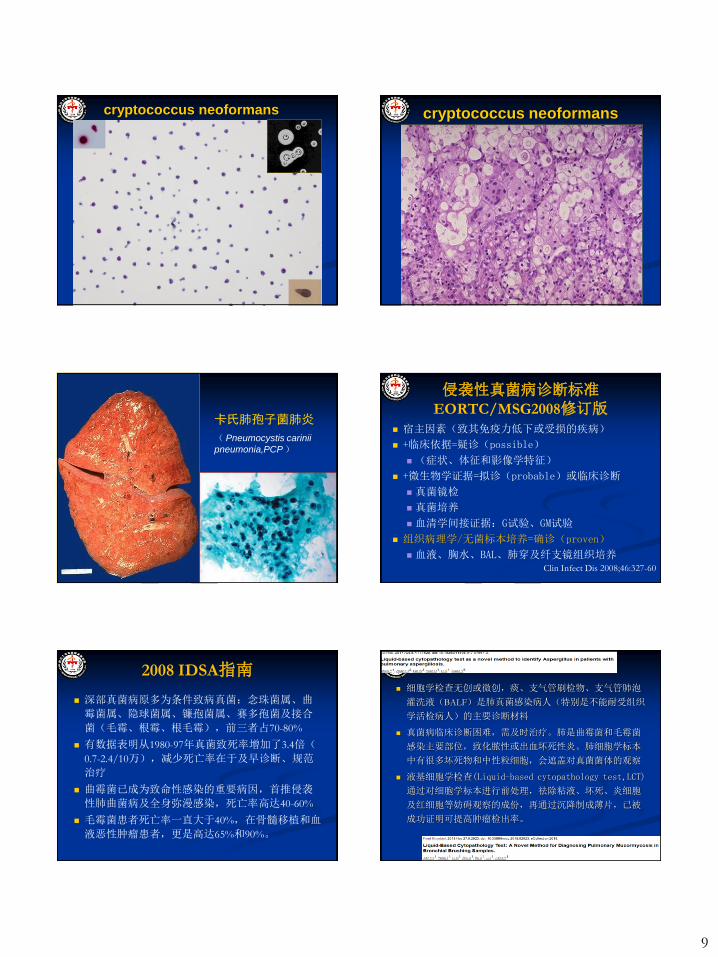
Fibrous inflammation
7
Manifestations and outcomes
Clinical manifestations
intestinal symptom?
Outcomes
Acute cases mostly recover
Chronic cases are affected repeatedly
Death would occur in toxicative cases
Mycosis
Weak pathogenicity
Predisposing factors: low immunity(opportunistic
infection)
Chronic wasting disease and immunodeficient disease
Long-term use of broad spectrum
adrenal cortex hormone
High-dose X-ray irradiation 、 anti-neoplastic drug and immunosuppressants
Long-term use of venous catheters, visceral ducts and major operation
Endocrine dysfunctions
Main lesions
Mild non-specific inflammation
-cryptococcus neoformans in brain
Suppurative inflammation
-candidiasis、aspergillosis and mucormycosis…
Necrotizing inflammation
- aspergillosis and mucormycosis
Granulomatous inflammation
Diagnoses of mycosis
Non-specificity in lesions
Diagnoses: to find pathogenic fungi in
lesions (special stain:GMS、PAS)
Thrush
Candidiasis

8
Aspergillosis Aspergillosis
GMS
mucormycosis
PAS
GMS
鉴别点 曲菌 毛霉菌
背景 脓肿、坏死及肉芽肿 同前,但炎细胞少,
有时在血管壁上
菌丝
粗细均匀,可有膨大,放射状或平行排列,偶见分生孢子头及孢子
粗细不均,壁厚,有时形成皱褶,常片段
状不规则分布,
分支 分支多,常45度锐角 分支少而不规则,常
成直角
宽度 直径约2-7μm 多数10-15μm(5-60)
分隔 有,密 无或偶分隔
特染 PAS佳,银染色深 PAS不佳,银染色淡
9
cryptococcus neoformans cryptococcus neoformans
卡氏肺孢子菌肺炎
( Pneumocystis carinii
pneumonia,PCP )
侵袭性真菌病诊断标准
EORTC/MSG2008修订版
宿主因素(致其免疫力低下或受损的疾病)
+临床依据=疑诊(possible)
(症状、体征和影像学特征)
+微生物学证据=拟诊(probable)或临床诊断
真菌镜检
真菌培养
血清学间接证据:G试验、GM试验
组织病理学/无菌标本培养=确诊(proven)
血液、胸水、BAL、肺穿及纤支镜组织培养 Clin Infect Dis 2008;46:327-60
2008 IDSA指南
深部真菌病原多为条件致病真菌:念珠菌属、曲
霉菌属、隐球菌属、镰孢菌属、赛多孢菌及接合
菌(毛霉、根霉、根毛霉),前三者占70-80%
有数据表明从1980-97年真菌致死率增加了3.4倍(
0.7-2.4/10万),减少死亡率在于及早诊断、规范
治疗
曲霉菌已成为致命性感染的重要病因,首推侵袭
性肺曲菌病及全身弥漫感染,死亡率高达40-60%
毛霉菌患者死亡率一直大于40%,在骨髓移植和血
液恶性肿瘤患者,更是高达65%和90%。
细胞学检查无创或微创,痰、支气管刷检物、支气管肺泡
灌洗液(BALF)是肺真菌感染病人(特别是不能耐受组织
学活检病人)的主要诊断材料
真菌病临床诊断困难,需及时治疗。肺是曲霉菌和毛霉菌
感染主要部位,致化脓性或出血坏死性炎。肺细胞学标本
中有很多坏死物和中性粒细胞,会遮盖对真菌菌体的观察
液基细胞学检查(Liquid-based cytopathology test,LCT)
通过对细胞学标本进行前处理,祛除粘液、坏死、炎细胞
及红细胞等妨碍观察的成份,再通过沉降制成薄片,已被
成功证明可提高肿瘤检出率。
10
Parasitosis
Characteristics of parasitosis
Chronic inflammation
Characteristics of communicable diseases and epidemics
Need to detect parasites and their eggs in diagnosis.
Eosinophilic abcess and granuloma are significant.
Amoebiasis
pathogen:pathogenic entamoeba histolytica
Locations :systemic diseases
mainly intestine、liver、lung and brain
lesions: liquefactive necrosis→ulcer or abscess
cyst
Small trophozoit
Large trophozoit
Intestinal amoebiasis
Location :cecum and ascending colon ,then
sigmoid and rectum
Basic lesions :degenerated inflammation mainly
with tissue liquefactive necrosis
acute stage :flask-shaped ulcers
chronic stage:Coexistence of new and old
lesions —necrosis ,ulcer, scar formation and
hyperplasia of granulation tissues
11
flask-shaped ulcers
Amoebiasis Dysentery
Pathogens Entamoeba histolytica Shigella dysenteriae
Locations Cecum and ascending colon Sigmoid colon and rectum
Pathologic
nature
Focal necrotic
inflammations
Disseminated pseudomembranous
inflammations
Depth of ulcers Deep, flask-shaped Shallow, irregular
Border of ulcers Undermining Non-undermining
Mucosa
between ulcers
Normal Inflammatory pseudomembranes
Generalized
manifestations
Mild, fever is infrequent Severe, fever is frequent
Intestinal
conditions
Tenderness in right lower
quadrant, diarrhea. No
tenesmus.
Tenderness in left lower quadrant,
diarrhea, and tenesmus.
Stool
examinations
Foul-odor; bloody;
erythrocytes and trophizoits
are present under
microscope
Stool with mucus and pus; bloody;
pus cells are present under
microscope
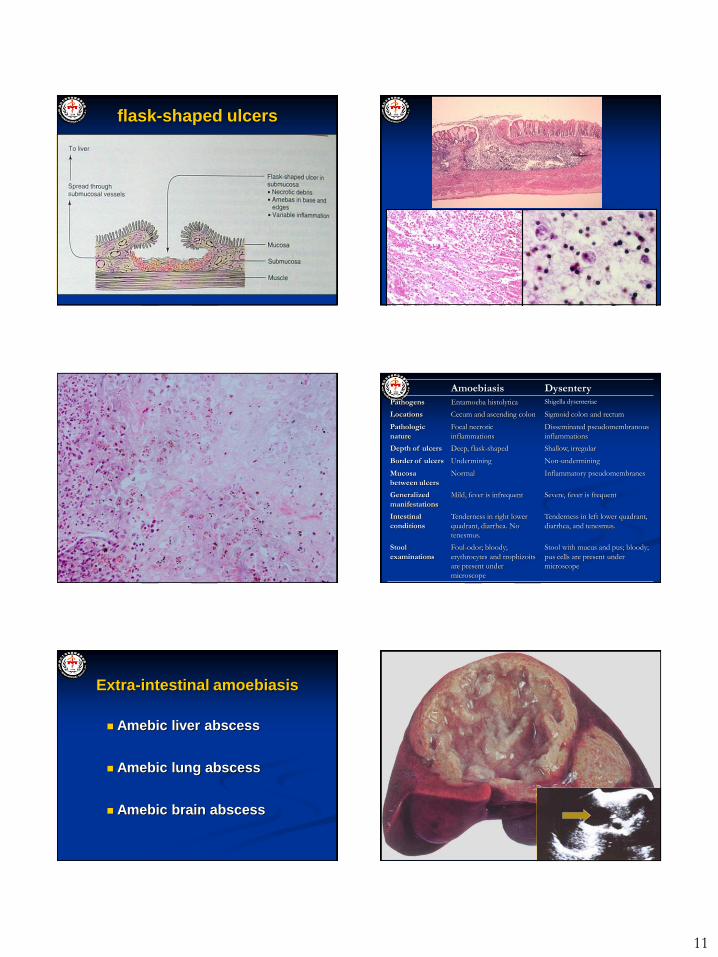
Extra-intestinal amoebiasis
Amebic liver abscess
Amebic lung abscess
Amebic brain abscess
12
Schistosomiasis
Pathogen :schistosoma(japonicum)
Irntemediate host :oncomelania
Pathogenesis:mechanical injury, allergy
Especially lesions induced by eggs
Characteristic pathological changes:
necrosis (acute egg nodule formation)
proliferation (chronic egg granuloma formation)
Life cycle
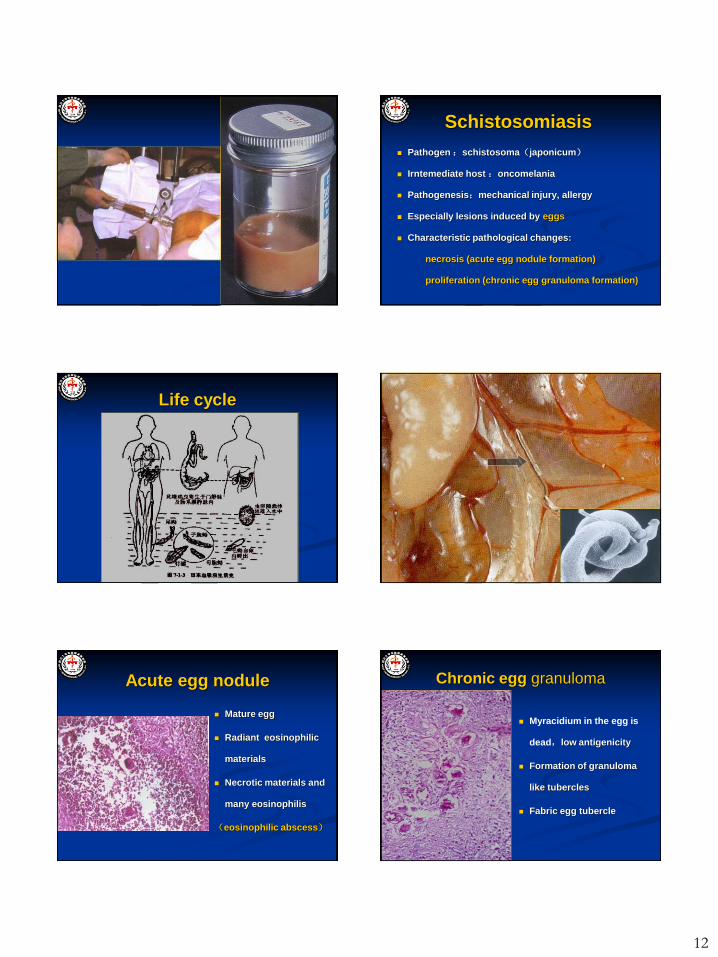
Acute egg nodule
Mature egg
Radiant eosinophilic
materials
Necrotic materials and
many eosinophilis
(eosinophilic abscess)
Chronic egg granuloma
Myracidium in the egg is
dead,low antigenicity
Formation of granuloma
like tubercles
Fabric egg tubercle

13
Main affective organ
colon
liver
spleen
lung
brain
Intestinal schistosomiasis
Involve in the whole colon, sigmoid colon
and rectum are the most notable
Early stage:acute egg nodule ,superficial ulcers
Advanced stage:Coexistance of new and old lesions;
fibrosis of intestinal wall and egg nodules, which can
cause stenosis of intestinal lumen and bowel obstruction
Can induce concurrent cancers
Hepatic schistosomiasis
Early stage: eggs deposites at portal area
Advanced stage: chronic egg nodules and fibrosis
schistosomal hepatic cirrhosis
-there are no pseudolobules
-portal hypertension appears early and severe
eosinophilic abscess
14
Bilharzial hepatic cirrhosis Bilharzial hepatic cirrhosis
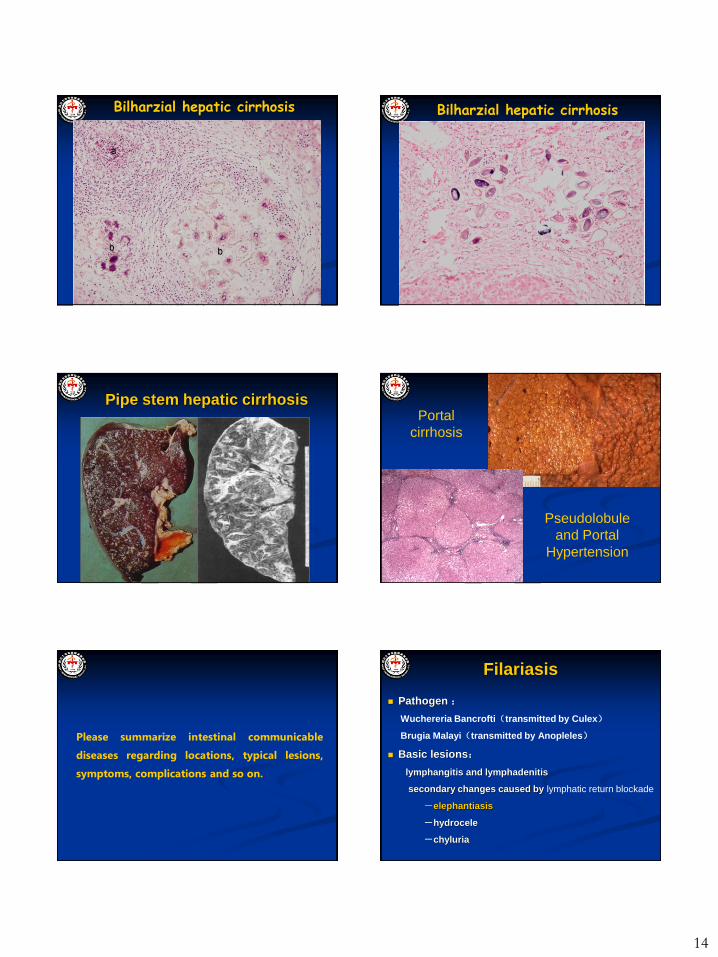
Pipe stem hepatic cirrhosis Portal
cirrhosis
Pseudolobule
and Portal
Hypertension
Please summarize intestinal communicable
diseases regarding locations, typical lesions,
symptoms, complications and so on.
Filariasis
Pathogen :
Wuchereria Bancrofti(transmitted by Culex)
Brugia Malayi(transmitted by Anopleles)
Basic lesions:
lymphangitis and lymphadenitis
secondary changes caused by lymphatic return blockade
-elephantiasis
-hydrocele
-chyluria
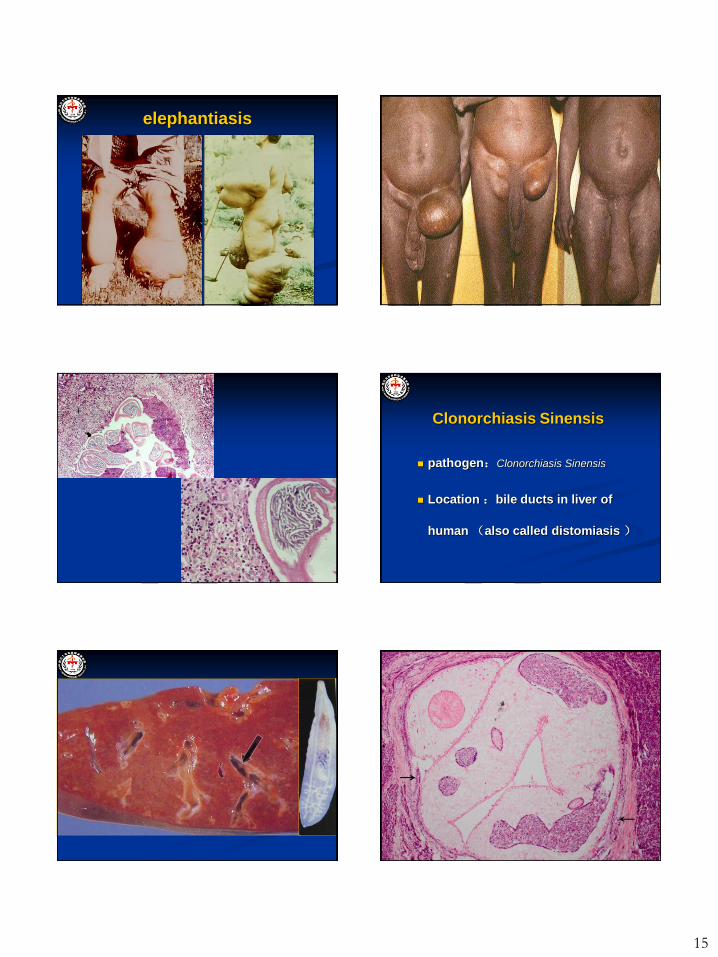
15
elephantiasis
Clonorchiasis Sinensis
pathogen:Clonorchiasis Sinensis
Location :bile ducts in liver of
human (also called distomiasis )
16
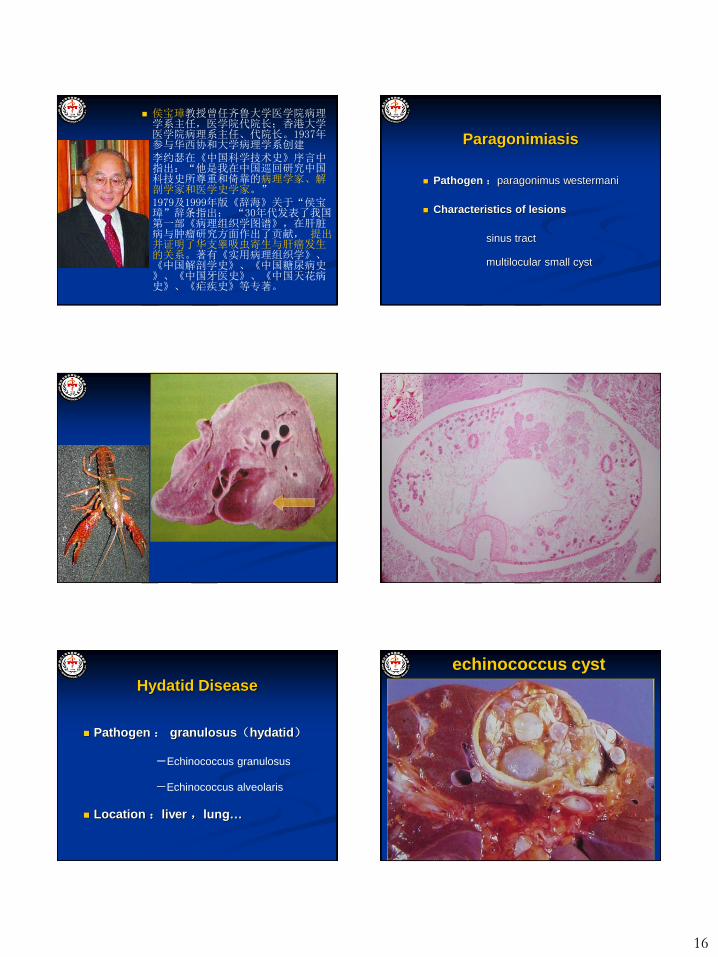
侯宝璋教授曾任齐鲁大学医学院病理学系主任,医学院代院长;香港大学医学院病理系主任、代院长。1937年参与华西协和大学病理学系创建
李约瑟在《中国科学技术史》序言中指出:“他是我在中国巡回研究中国科技史所尊重和倚靠的病理学家、解剖学家和医学史学家。”
1979及1999年版《辞海》关于“侯宝璋”辞条指出: “30年代发表了我国第一部《病理组织学图谱》,在肝脏病与肿瘤研究方面作出了贡献, 提出并证明了华支睾吸虫寄生与肝癌发生的关系。著有《实用病理组织学》、《中国解剖学史》、《中国糖尿病史》、《中国牙医史》、《中国天花病史》、《疟疾史》等专著。
Paragonimiasis
Pathogen :paragonimus westermani
Characteristics of lesions
sinus tract
multilocular small cyst
Hydatid Disease
Pathogen : granulosus(hydatid)
-Echinococcus granulosus
-Echinococcus alveolaris
Location :liver ,lung…
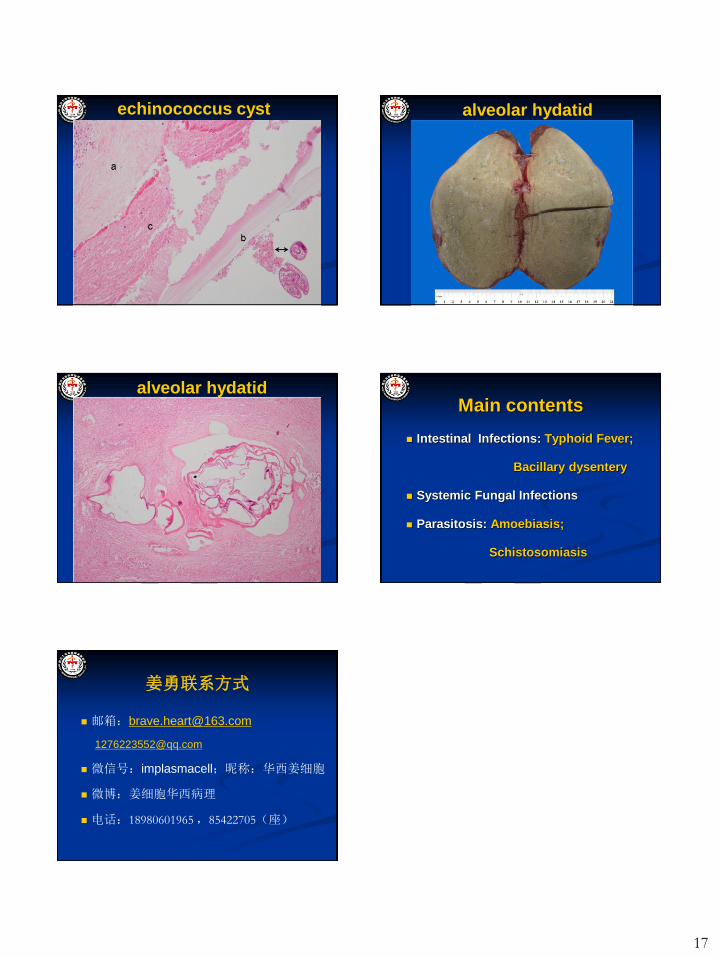
echinococcus cyst
17
echinococcus cyst alveolar hydatid
alveolar hydatid Main contents
Intestinal Infections: Typhoid Fever;
Bacillary dysentery
Systemic Fungal Infections
Parasitosis: Amoebiasis;
Schistosomiasis
姜勇联系方式
微信号:implasmacell;昵称:华西姜细胞
微博:姜细胞华西病理
电话:18980601965 ,85422705(座)