maine pandemic influenza mass fatality management planning
TRANSCRIPT
12-1
Maine Pandemic Influenza Mass Fatality Management Planning
Considerations and Guidelines Medical and health authorities have warned the world and placed a call for government and citizens to take action in preparing for the onset of the next severe pandemic influenza virus. While human to human transmission of the bird flu has not progressed beyond some rare isolated cases, and the H1N1 2009 pandemic was similar in nature to a seasonal outbreak, the possibility of a severe pandemic developing with characteristics of high transmissibility and high mortality remains a very real threat. The U.S. Department of Health and Human Services (HHS) has published the “HHS Pandemic Influenza Plan” outlining specific actions that local, tribal, state, and federal agencies should consider in planning for this potentially catastrophic event. In Maine, the State Department of Health and Human Services (DHHS) has published and updated a ME CDC Pandemic Influenza Operational Plan (2011) providing a framework for DHHS pandemic influenza preparedness, response and recovery activities. Maine stakeholders are currently in the process of developing a comprehensive all hazards Mass Fatality Management Plan. A necessary component of both the ME CDC Pandemic Influenza Operational Plan and the Maine Mass Fatality Management Plan is a plan for managing mass fatalities as a result of a severe pandemic; a pandemic generating from a novel virus with characteristics of high transmissibility and high mortality. This document will discuss the unique considerations, challenges and actions required in preparation for, response to and recovery from a severe pandemic resulting in mass fatalities.
Mass Fatality Management Planning Assumptions for a Severe Influenza Pandemic
• Susceptibility to pandemic influenza will be universal.
WHAT IS PANDEMIC? The word "pandemic" is used to describe a disease that affects people on a worldwide scale. Flu pandemics have occurred roughly every 20 to 30 years throughout history, the most serious being the misnamed "Spanish flu" of 1918, the "Asian flu" of 1957, the "Hong Kong flu" of 1968, and the H1N1 “swine flu” of 2009. Three conditions must be met to result in a pandemic: 1. The emergence of a new flu strain 2. The ability of that strain to infect humans and cause serious illness 3. The ability to spread easily among humans
12-2
• There may be a case fatality rate of up to 5% in addition to the average rate of deaths from other causes.
• An estimated 5,000 Maine residents will die from the deadly virus. Usual death rates experienced on a daily basis may be exacerbated due to lack of medical care.
• Loss of 30% - 40% of the critical workforce due to illness, death or absenteeism during peak periods will significantly impede the capability and capacity of the Medical Examiner (ME) and supporting agencies to provide care and management of the deceased.
• Critical infrastructure, necessary to carry out ME duties and responsibilities, may be disrupted affecting job performance.
• Essential supplies needed to perform ME functions may be in short supply or non-existent due to just-in-time inventories and nation/global competition for supplies.
• ME mutual aid resources from state and federal agencies to support local response efforts may not be available during the course of the pandemic. Each region will face the overwhelming burden of taking care of its own fatality management needs.
• It is estimated that 50% to 70% of deaths will occur outside of a hospital or medical treatment facility.
• A severe pandemic in the US will trigger state and federal disaster declarations. Many local, state and federal laws and regulations will be suspended and / or imposed.
• The death care industry could expect to handle about six months of work within a six to eight week period.
• Common societal group activities and gatherings (including funeral services) will be curtailed or halted to inhibit the spread of the circulating virus.
• Disposition of the deceased and funeral arrangements may not be consistent with accepted cultural/religions practices.
• The time to complete fatality management of a PI event may exceed six months to a year.
TANGENTIAL CONSEQUENCES OF WORST-CASE PANDEMIC* Commerce Disruption Public Safety Disruption Transportation Lawlessness Communications Violence Bankruptcy Public Panic Economic Depression Health Care Disruption Political Unrest Hospital Overload Loss of trust in Government Shortage of Staff Wars over Shortages Shortage of Supplies Global Terrorism Food Shortages Social Fabric Disruption Famine Human suffering and loss Disruption of Supplies to Poor Migration Deaths from Shortages
Long-term Effects Demographic Psychological
* From Larry Brilliant, MD, MPH, Meeting on Effective Response and Business Continuity for UN and Humanitarian Agencies, Tufts University, Boston, 1/12/06
12-3
Mass Fatality Mass Fatality is defined as the number of fatalities that exceeds a local jurisdiction’s capacity to cope due to infrastructure / support limitations. Trigger points for initiating the Mass Fatality Plan may include:
1. The number of increased deaths, 2. Limited storage space at local mortuaries and funeral homes, 3. Worker absenteeism, or 4. A combination of these and other related factors.
These MFM Planning Considerations and Guidelines are intended to be used in conjunction with the Maine CDC Pandemic Influenza Operational Plan and the Maine Mass Fatality Management Plan.
Planning Considerations
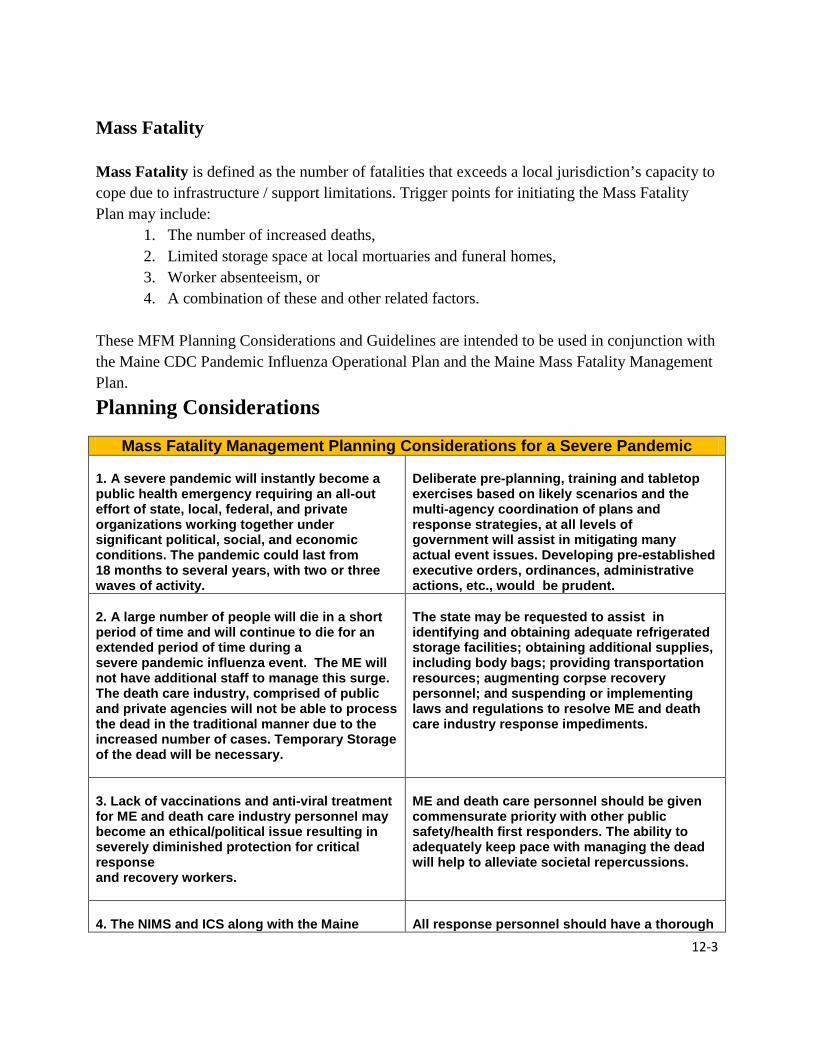
Mass Fatality Management Planning Considerations for a Severe Pandemic 1. A severe pandemic will instantly become a public health emergency requiring an all-out effort of state, local, federal, and private organizations working together under significant political, social, and economic conditions. The pandemic could last from 18 months to several years, with two or three waves of activity.
Deliberate pre-planning, training and tabletop exercises based on likely scenarios and the multi-agency coordination of plans and response strategies, at all levels of government will assist in mitigating many actual event issues. Developing pre-established executive orders, ordinances, administrative actions, etc., would be prudent.
2. A large number of people will die in a short period of time and will continue to die for an extended period of time during a severe pandemic influenza event. The ME will not have additional staff to manage this surge. The death care industry, comprised of public and private agencies will not be able to process the dead in the traditional manner due to the increased number of cases. Temporary Storage of the dead will be necessary.
The state may be requested to assist in identifying and obtaining adequate refrigerated storage facilities; obtaining additional supplies, including body bags; providing transportation resources; augmenting corpse recovery personnel; and suspending or implementing laws and regulations to resolve ME and death care industry response impediments. PLANNING
3. Lack of vaccinations and anti-viral treatment for ME and death care industry personnel may become an ethical/political issue resulting in severely diminished protection for critical response and recovery workers.
ME and death care personnel should be given commensurate priority with other public safety/health first responders. The ability to adequately keep pace with managing the dead will help to alleviate societal repercussions.
4. The NIMS and ICS along with the Maine
All response personnel should have a thorough
12-4
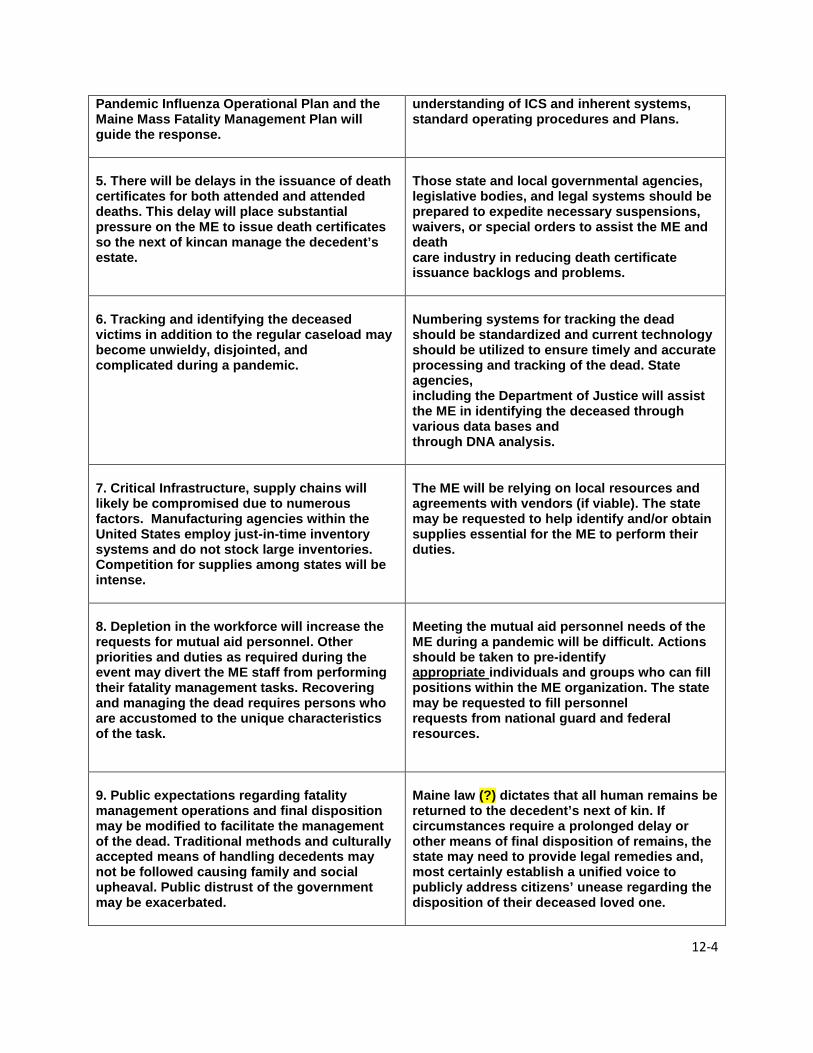
Pandemic Influenza Operational Plan and the Maine Mass Fatality Management Plan will guide the response.
understanding of ICS and inherent systems, standard operating procedures and Plans.
5. There will be delays in the issuance of death certificates for both attended and attended deaths. This delay will place substantial pressure on the ME to issue death certificates so the next of kincan manage the decedent’s estate.
Those state and local governmental agencies, legislative bodies, and legal systems should be prepared to expedite necessary suspensions, waivers, or special orders to assist the ME and death care industry in reducing death certificate issuance backlogs and problems.
6. Tracking and identifying the deceased victims in addition to the regular caseload may become unwieldy, disjointed, and complicated during a pandemic.
Numbering systems for tracking the dead should be standardized and current technology should be utilized to ensure timely and accurate processing and tracking of the dead. State agencies, including the Department of Justice will assist the ME in identifying the deceased through various data bases and through DNA analysis.
7. Critical Infrastructure, supply chains will likely be compromised due to numerous factors. Manufacturing agencies within the United States employ just-in-time inventory systems and do not stock large inventories. Competition for supplies among states will be intense.
The ME will be relying on local resources and agreements with vendors (if viable). The state may be requested to help identify and/or obtain supplies essential for the ME to perform their duties.
8. Depletion in the workforce will increase the requests for mutual aid personnel. Other priorities and duties as required during the event may divert the ME staff from performing their fatality management tasks. Recovering and managing the dead requires persons who are accustomed to the unique characteristics of the task.
Meeting the mutual aid personnel needs of the ME during a pandemic will be difficult. Actions should be taken to pre-identify appropriate individuals and groups who can fill positions within the ME organization. The state may be requested to fill personnel requests from national guard and federal resources.
9. Public expectations regarding fatality management operations and final disposition may be modified to facilitate the management of the dead. Traditional methods and culturally accepted means of handling decedents may not be followed causing family and social upheaval. Public distrust of the government may be exacerbated.
Maine law (?) dictates that all human remains be returned to the decedent’s next of kin. If circumstances require a prolonged delay or other means of final disposition of remains, the state may need to provide legal remedies and, most certainly establish a unified voice to publicly address citizens’ unease regarding the disposition of their deceased loved one.

12-5
10. Cemeteries may only have a limited surge capacity and it is likely that they may not have the space to accommodate thousands of deaths at one time. Funeral homes and crematoriums may have similar problems in providing services in a timely and sufficient manner.
Maine law/regulations (?) governing cemeteries and funeral directors may require emergency actions to ease restrictions in order to facilitate decedent final disposition.
IDERATONS COMMENTS PLANNING CONSIDERATONS COMMENTS
General Guidelines for Mass Fatality Management Planning for a Severe Pandemic
During a pandemic, local authorities will have to be prepared to manage additional deaths due to influenza, over and above the number of fatalities from all causes currently expected during the inter-pandemic period. These guidelines aim to assist local planners and funeral directors in preparing to cope with large-scale fatalities due to an influenza pandemic. A number of issues have been identified, which should be reviewed with coroners/medical examiners, local authorities, funeral directors, and religious groups/ authorities. Personnel All personnel will wear personal protective equipment as directed by the Health Officer.
Protecting employee health and reducing the spread of infection among workers is a priority. All personnel handling dead bodies in mass fatality response will also receive proper
immunizations as appropriate; training in blood borne pathogens, personal protective equipment (PPE), and proper lifting techniques; and PPE as defined by existing regulations, for example:
o Disposable, long-sleeved, cuffed gown (waterproof if possibly exposed to body fluids). o Single-layer non-sterile ambidextrous gloves which cover the cuffs of the long-sleeve
gown. o Surgical mask (a particulate respiratory if handling the body immediately after death). o Surgical cap and face shield if splashing of body fluids is anticipated. o Waterproof shoe covers if required.
Proper hand washing is always recommended when handling remains
Family Emergency Plans
The ME/C, vital records system, and death care industry should encourage employees to develop “family emergency plans” knowing that they may not be able to be with their families for extended periods during waves of severe disease during the pandemic period
Planning for Mass Fatalities In order to identify planning needs for the management of mass fatalities during a severe pandemic, it is important to examine each step in the management of a decedent under normal

12-6
circumstances and then to identify what the limiting factors will be when the number of corpses increase over a short period of time. The following table identifies the usual steps, planning requirements and possible solutions.

12-7
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Emergency Operations Center and Public Health Department Actions for Managing Deceased
Consider ME/C Office and death care industry personnel as first responders.
Classify ME/C Office and death care industry personnel as first responders for priority prophylaxis and antivirals. Ensure the ME/C Office’s and death care industry’s priority access to labor, supplies, personal protective equipment, vaccines, fuel, raw
materials, communication bandwidth, transportation, security, temporary housing as needed, and other resources.
Consider involving Public Health, the ME/C, and police in developing specific investigative checklists, which clarify the concepts of medico-legal determination of cause and manner of death, victim identification procedures, scene documentation, overall investigative requirements, and required PPE and personal decontamination, for all call centers and responders to unattended deaths during a PI event.
Train all first responders in the field about the symptoms of PI deaths and the actions to take when a suspected PI event related death is found vs. when non PI event related deaths are found.
Consider establishing a dispatch/tracking system with a centralized database that is separate from emergency medical services and 911 systems to track patients and deaths. Design it so that it can be managed through family assistance and patient tracking centers. Link all first responders/health care centers/collection points/morgues/family assistance/ME/C Office/law enforcement/etc. to this system. Consider facilitating its use by private citizens.
Consider establishing a county voluntary registry of next of kin so families can register information before a disaster.
Implement reciprocal licensing of mortuary services personnel to overcome variations in state licensing of funeral directors, embalmers, cemetery, and crematory operations, and unionized labor.
12-8
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Educate behavioral health professionals, social service organizations and religious leaders regarding the process for managing human remains to ensure the process is understood and can be properly communicated to the general population in their response activities.
Advise the ME/C Office and death care industry of additional respiratory protection that is needed
During autopsy procedures performed on the lungs or during procedures that generate small-particle aerosols (e.g., use of power saws and washing intestines) in case the decedent was infectious when he/she died.
During embalming procedures prior to burial or cremation.
If families will be transporting loved ones who have died from pandemic influenza, provide education on general precautions for handling dead bodies. Special precautions are not required since the “body” is not contagious after death.
Track federal, state, and local laws applicable to the handling of human remains that impact the ME/C, vital records system, and death care industry. Existing laws, such as time requirements for completing death certificates and disposition permits, may need to be amended/waived. Alert all parties to waivers and modifications that impact services.
Death Reporting/ Missing Persons
Requirement:
If death occurs in the home/business/community then a call in system needs to be established.
Citizens call 911 to request a check on the welfare call for others.
911 or other system needs to be
Provide public education about the call centers, what information to have available when they call, and what to expect from the authorities when a death or missing persons report is made.
Consider planning a Call Center (toll free number) system 24/7 specifically for this task to free up operators for 911 calls on the living.
12-9
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
identified as the lead to perform this task.
Limiting Factors:
Availability of people able to do this task normally 911 operators
Availability of communications equipment to receive and manage large volumes of calls/inquiries
Availability of trained “investigators” to check into the circumstances of each report and to verify death is natural or other
Search for Remains
Requirement:
If death occurs in the home/business then the law enforcement will need to be contacted.
Persons legally authorized to perform
Consider deputization and training (through the investigations unit of law enforcement) of people whose sole responsibility is to search for the dead and report their findings.
Consider having community attorneys involved in the legal issues training for the groups identified.

12-10
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
this task.
Limiting Factors:
Law enforcement availability.
Recovering Remains
Requirement:
Personnel trained in recovery operations and the documentation required to be collected at the “scene”
Personnel protection equipment such as coveralls, gloves, and surgical masks.
Equipment such as stretchers and human remains pouches.
Limiting Factors:
Availability of trained people to perform this task
Availability of transportation assets
Consider training volunteers ahead of time.
Consider refrigerated warehouses, tents or other cold storage as an interim facility until remains can be transferred to the family’s funeral service provider for final disposition.

12-11
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Availability of interim storage facility
Step: Death Pronounced
Requirement:
Person legally authorized to perform this task.
Limiting Factors:
If death occurs at home then one of these people will need to be contacted.
Availability of people able to do this task.
Provide public education on what to do if someone dies, how to access an authorized person to certify death, and where to take the deceased if family or friends must transport them.
Consider planning an on-call system 24/7 specifically for this task that is separate from the 911 System. Keep 911 focused on calls pertaining to life safety missions.
All who interface with decedents should record official personal identification information for patients who enter their systems and maintain this information in the patient’s police report and/or medical record.
If a deceased patient enters the system without an official photo identification, and identity is never established, healthcare facilities should report this person to the patient’s local police department. There is a possibility the deceased has been reported missing by a family member who can visually identify the decedent.
Consult with Native Americans, Jews, Hindus, Muslims and other religious groups that have special requirements for the treatment of bodies and for funerals and involve them in planning for funeral management, bereavement counseling, and communications with their respective communities in the event of a pandemic. During the pandemic, the wishes of the family will provide guidance, however, if no family is available local religious or ethnic communities can be contacted for information.
Step: Death Certified (signing of a death certificate stating the cause of death)

12-12
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Requirement:
Person legally authorized to perform this task.
Limiting Factors:
Legally, may not necessarily be the same person that pronounced the death.
ALL who interface with the deceased should record official personal identification information (first, middle, last name & suffix; race/ethnicity, color of eyes, hair, height, and weight; home address, city, state, zip & telephone number; location of death and place found; place of employment and employer’s address; date of birth, social security number & age; and next of kin—or witness—name, contact number & address).
To ensure proper identification of the deceased, consider implementing standardized methods for collecting samples of deceased such as a right thumbprint, DNA sample (e.g., saliva swab or blood stain card), and a facial photograph. In the case of decomposed bodies, this may also include assistance from the ME/C for identification—anthropological markers, dental impressions, and, if possible, fingerprints, etc.
Although these identification samples may not need to be processed, the samples will ensure that those in authority are able to substantiate the identification of the decedent at a later time should individuals question the ME/C about a decedent’s identity.
Healthcare facilities may want to consider designating a single physician, familiar with patients’ records, as responsible for expeditiously signing death certificates.
Consider pre-identifying “collection points” for the deceased to centralize processing and hold remains at the lowest appropriate local level. Have an authorized person certify deaths en masse and batch process death certificates of identified decedents to improve efficiency.
At the designated collection point, trained personnel should sort bodies by cause and manner of death (identified PI cases vs. ME/C cases) to ease subsequent processing (victim identification and issuing a death certificate).
o Attended deaths will have a known identity and may have a signed death certificate. Unattended deaths may require the ME/C to further process remains to determine

12-13
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
identification, issue the death certificate, track personal effects, and notify next of kin. Establish a uniform method for numbering and tracking decedents, such as the state
abbreviation, zip code, and a case number (with name if identified).
When moving, storing, and/or releasing remains and personal effects, keep detailed records like that of a chain-of–evidence for each individual body and personal effects bag.
Consider broadening the range of professionals who can certify deaths. Explore strategies that facilitate and provide oversight to the process of pronouncing death, determining cause and manner of death, completing death certificates and establishing victim identity. This may include amending/waiving the Health Insurance Portability and Accountability Act of 1996, other regulations, and codes to allow trained and credentialed non-ME/C personnel (such as police, fire and emergency medical services) and retired physicians to assist with these responsibilities during a large-scale emergency.
Establish a call line for ME/C consultations and physician-patient data to assist in determination of death.
Step: Body Wrapped
Requirements:
Person(s) trained to perform this task.
Body bags.
Limiting Factors:
Clearly tag the body and pouch with the individual decedent’s identifiers such as name, date of birth, SSN, location of origination, medical record number, etc. Complete labeling reduces the number of times mortuary staff needs to open pouches to confirm contents.
Consider developing a rotating six months inventory of body bags, given their shelf life.
Consider training or expanding the role of current staff to include this task.

12-14
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Supply of human and physical (body bags) resources.
If death occurs in the home: the availability of these requirements.
Consider providing this service in the home in conjunction with pronouncement and transportation to the morgue.
If personal effects accompany the remains in the human remains pouches, ensure that the funeral director and family are made aware of this so that effects may be safely retrieved before cremation or burial. Funeral directors and others should sign a receipt for items as well as the body.
Step: Transportation (To “Collection Points” and/or the Morgue and To Temporary Storage or Burial Site)
Requirements:
In hospital: trained staff and stretcher.
Outside hospital: informed person(s), stretcher, and vehicle with driver suitable for this purpose.
Limiting Factors:
Availability of human and physical resources.
Consider amending codes as needed regarding the use of volunteers, family members, etc., to transport the deceased.
In hospital:
Consider training additional staff working within facility. Consider keeping old stretchers in storage instead of discarding.
Look for alternate suppliers of equipment that could be used as stretchers in an emergency e.g., trolley manufactures.
Outside hospital:
Provide public education or specific instructions through a toll-free phone service regarding where to take the deceased if the family must transport.
Identify alternate vehicles that could be used for this purpose. (Unmarked vehicles) Consider use of volunteer drivers.

12-15
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Step: Morgue Storage
Requirements:
A suitable facility that can be maintained at 34-37° F, the ideal temperature for storing and preserving human remains. It does not prevent decomposition of the decedent, which continues, albeit at a slow rate for up to six months.
Limiting Factors:
Capacity of such facilities.
Pre-identify and plan for possible temporary morgue storage sites:
Refrigerated trucks with temporary shelves and ramps. Temporary portable facilities. Cold storage lockers. Conex boxes with diesel or electrical power. Hangars. Warehouses. Refrigerated rail cars. Empty public buildings that lend themselves to cooling and proper security.
An organized, segregated storage system will provide the public a higher level of confidence that government agencies are managing the PI event well.
Consider ice skating rinks as a resource when all other resources have been exhausted.
Use processes routinely used in mortuaries to track and locate deceased.
Consider some facilities maintained at -15°/-25° C or 5°/-13° F, used in forensic institutes, especially for bodies which have not yet been identified. The body is completely frozen and decomposition totally halted.
Step: ME/C Office and Autopsy if Required/Requested
Requirement: Ensure that it is public knowledge—that all physicians and families are aware that an autopsy is not required for confirmation of influenza as cause of death.
12-16
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Person qualified to perform autopsy and suitable facility with equipment.
Limiting Factors:
Availability of human and physical resources.
May be required in some circumstances.
However, for the purpose of health surveillance, respiratory tract specimens or lung tissue for culture or direct antigen testing could be collected postmortem to confirm the early cases that start the pandemic.
Examine the capacity, continuity of operations planning, and surge capacity of the ME/C Office in your jurisdiction.
Shift ME/C resources to the most vital public health functions, including body recovery, abbreviated processing, temporary storage, and tracking.
Employ a phased operation to ensure bodies are properly identified and handled with dignity.
Identify ways to augment staff.
Break down functions into tasks so that disaster service workers and volunteers are able to provide more effective assistance.
Consider requesting a volunteer category for death care professionals be added to established organized volunteer Citizen Corps and/or Medical Corps.
Provide just-in-time training for current staff who will be performing new management/oversight roles, for suitable drivers and handlers to support the human remains recovery and for other positions as practicable.
Keep daily death cases separate from PI event cases and number them using different identifiers.
Ensure that critical morgue supplies are stockpiled or develop a rotating six month inventory of essential equipment/supplies.
Consider putting in place contracts and memoranda of agreement to ensure that the ME/C Office
12-17
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
receives priority distribution of water, generators, and gasoline.
If an autopsy is required, usual protocols based on current law will prevail.
Consider advocating for amending regulations regarding reportable deaths. For example, the ME/C assumes jurisdiction over deaths of persons in correctional custody, deaths in mental institutions, and sometimes in nursing care facilities, regardless of the circumstances. Consider requiring ME/C jurisdiction only when the cause of death is of suspicious nature during the pandemic.
Seek direction from Health Officer re: additional respiratory protection needed during autopsy procedures performed on the lungs or during procedures that generate small-particle aerosols (e.g., use of power saws and washing intestines) in case the decedent was infectious when he/she died.
Step: Cremation 1
Requirement:
Suitable vehicle and driver for transportation from morgue to crematorium.
Limiting Factors:
Identify alternate vehicles that could be used for transport.
Examine the capacity, continuity of operations planning, and surge capacity of crematoriums within the jurisdiction.
Arrange for maintenance and inspection of equipment—ahead of periods of peak usage—with backup equipment and replacement parts stockpiled.
1 Cremated bodies are not usually embalmed; families may chose to have a funeral service followed by cremation or to have the body cremated first and a memorial service later.
12-18
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
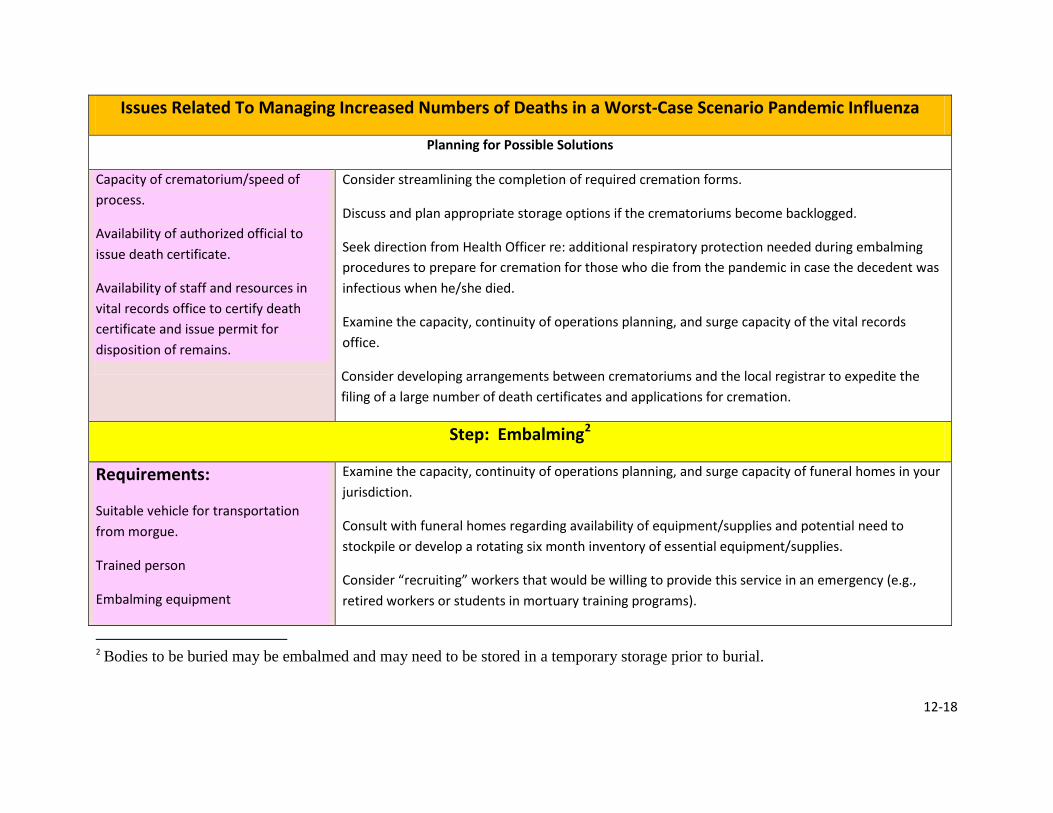
Capacity of crematorium/speed of process.
Availability of authorized official to issue death certificate.
Availability of staff and resources in vital records office to certify death certificate and issue permit for disposition of remains.
Consider streamlining the completion of required cremation forms.
Discuss and plan appropriate storage options if the crematoriums become backlogged.
Seek direction from Health Officer re: additional respiratory protection needed during embalming procedures to prepare for cremation for those who die from the pandemic in case the decedent was infectious when he/she died.
Examine the capacity, continuity of operations planning, and surge capacity of the vital records office.
Consider developing arrangements between crematoriums and the local registrar to expedite the filing of a large number of death certificates and applications for cremation.
Step: Embalming2
Requirements:
Suitable vehicle for transportation from morgue.
Trained person
Embalming equipment
Examine the capacity, continuity of operations planning, and surge capacity of funeral homes in your jurisdiction.
Consult with funeral homes regarding availability of equipment/supplies and potential need to stockpile or develop a rotating six month inventory of essential equipment/supplies.
Consider “recruiting” workers that would be willing to provide this service in an emergency (e.g., retired workers or students in mortuary training programs).
2 Bodies to be buried may be embalmed and may need to be stored in a temporary storage prior to burial.
12-19
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
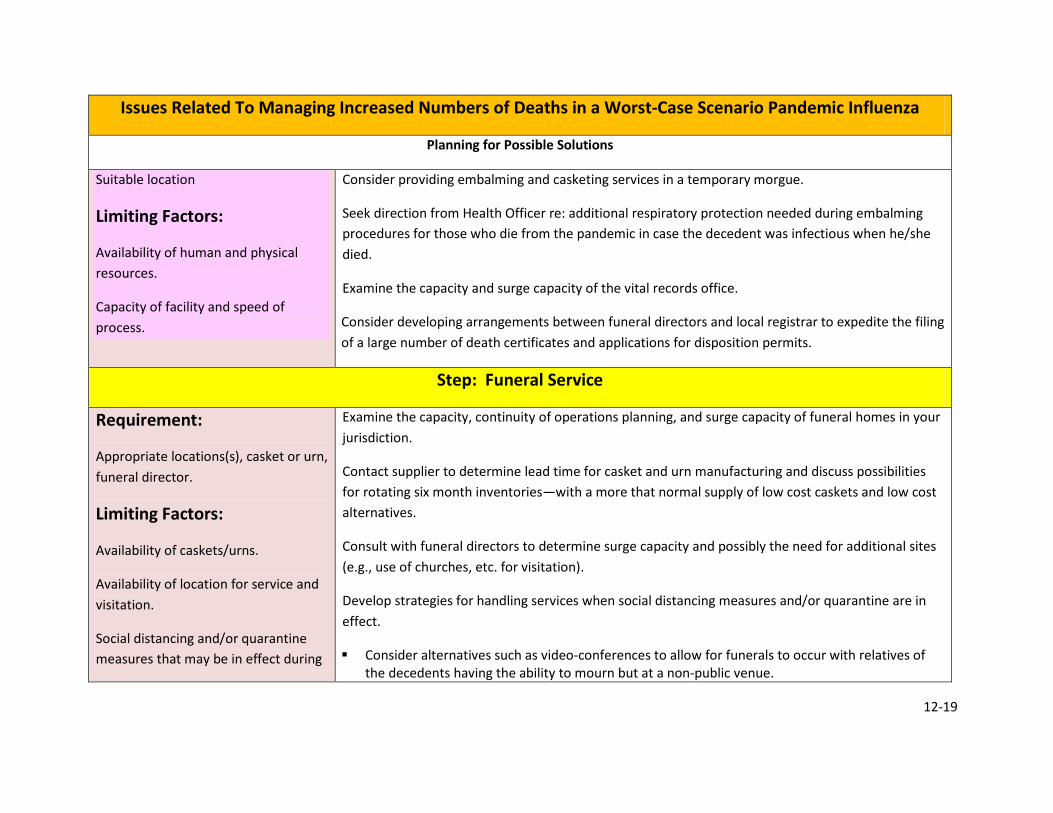
Suitable location
Limiting Factors:
Availability of human and physical resources.
Capacity of facility and speed of process.
Consider providing embalming and casketing services in a temporary morgue.
Seek direction from Health Officer re: additional respiratory protection needed during embalming procedures for those who die from the pandemic in case the decedent was infectious when he/she died.
Examine the capacity and surge capacity of the vital records office.
Consider developing arrangements between funeral directors and local registrar to expedite the filing of a large number of death certificates and applications for disposition permits.
Step: Funeral Service
Requirement:
Appropriate locations(s), casket or urn, funeral director.
Limiting Factors:
Availability of caskets/urns.
Availability of location for service and visitation.
Social distancing and/or quarantine measures that may be in effect during
Examine the capacity, continuity of operations planning, and surge capacity of funeral homes in your jurisdiction.
Contact supplier to determine lead time for casket and urn manufacturing and discuss possibilities for rotating six month inventories—with a more that normal supply of low cost caskets and low cost alternatives.
Consult with funeral directors to determine surge capacity and possibly the need for additional sites (e.g., use of churches, etc. for visitation).
Develop strategies for handling services when social distancing measures and/or quarantine are in effect.
Consider alternatives such as video-conferences to allow for funerals to occur with relatives of the decedents having the ability to mourn but at a non-public venue.
12-20
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
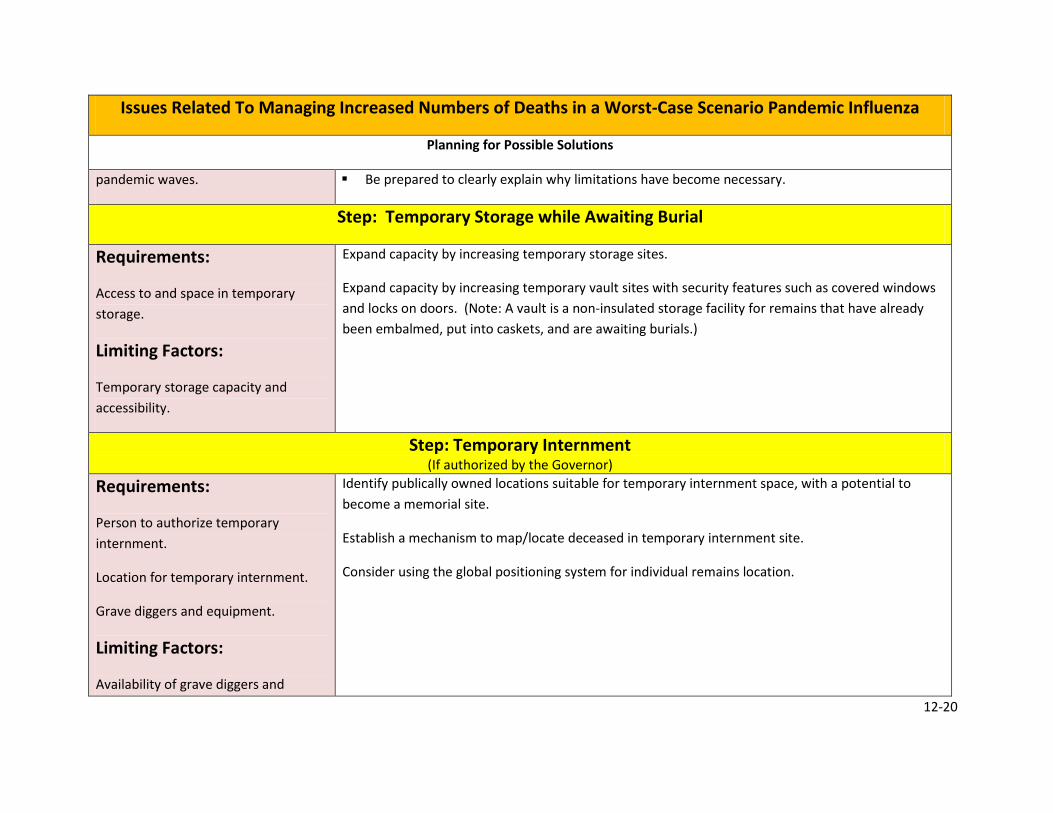
pandemic waves. Be prepared to clearly explain why limitations have become necessary.
Step: Temporary Storage while Awaiting Burial
Requirements:
Access to and space in temporary storage.
Limiting Factors:
Temporary storage capacity and accessibility.
Expand capacity by increasing temporary storage sites.
Expand capacity by increasing temporary vault sites with security features such as covered windows and locks on doors. (Note: A vault is a non-insulated storage facility for remains that have already been embalmed, put into caskets, and are awaiting burials.)
Step: Temporary Internment (If authorized by the Governor)
Requirements:
Person to authorize temporary internment.
Location for temporary internment.
Grave diggers and equipment.
Limiting Factors:
Availability of grave diggers and
Identify publically owned locations suitable for temporary internment space, with a potential to become a memorial site.
Establish a mechanism to map/locate deceased in temporary internment site.
Consider using the global positioning system for individual remains location.
12-21
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
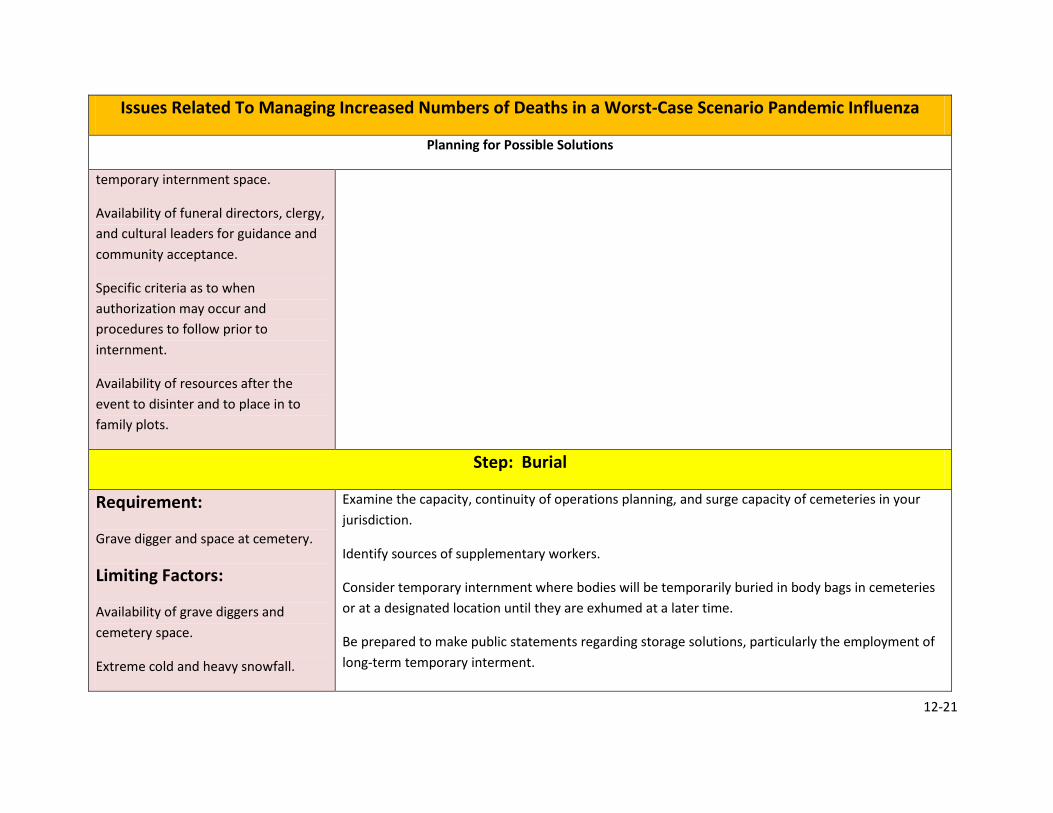
temporary internment space.
Availability of funeral directors, clergy, and cultural leaders for guidance and community acceptance.
Specific criteria as to when authorization may occur and procedures to follow prior to internment.
Availability of resources after the event to disinter and to place in to family plots.
Step: Burial
Requirement:
Grave digger and space at cemetery.
Limiting Factors:
Availability of grave diggers and cemetery space.
Extreme cold and heavy snowfall.
Examine the capacity, continuity of operations planning, and surge capacity of cemeteries in your jurisdiction.
Identify sources of supplementary workers.
Consider temporary internment where bodies will be temporarily buried in body bags in cemeteries or at a designated location until they are exhumed at a later time.
Be prepared to make public statements regarding storage solutions, particularly the employment of long-term temporary interment.

12-22
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Step: Family Assistance
Requirement:
The ME/C Office is responsible for providing family assistance in the event of a mass fatality.
Limiting Factors:
The catastrophic scope of the disaster and mandated social distancing will prohibit a traditional family assistance center and dictate limitations to the provision of direct services.
Identify a local agency/organization to manage family assistance during a pandemic.
Implement a virtual family assistance center model that includes:
Broadcasting information ‘pushed’ to families through mass media channels. Content may include: coping with death and dying at home, coping with illness and death at work, financial support, health issues, emotional and behavioral health concerns, Social Security questions, and legal issues.
“Warm Lines” established and staffed to provide a more direct line of communication with families and track/manage death and missing persons calls. Issues may include: death care guidance, body removal, burial sites, death certificate information, and psychological support. “Warm Lines” may include toll-free telephone lines staffed by behavioral health providers working from their homes and Internet “Counseling Rooms” established for computer-based interactions between behavioral health providers and community members needing assistance.
o May want to consider a separate fatality/missing person information telephone number to report fatalities that can incorporate this information into a national patient tracking system. Consider the National Find Family Hotline as a model.
Face-to-Face Crisis Interventions provided by trained behavioral health services professionals with appropriate PPE for those individuals with acute psychiatric reactions.
Identify interventions and strategies for assisting at-risk and/or special populations, such as those with mental and behavioral illness or disabilities and/or with general pharmaceutical needs or medication withdrawal issues, homeless, senior citizens, immigrants, and undocumented residents.
Step: Behavioral Health Support
12-23
Issues Related To Managing Increased Numbers of Deaths in a Worst-Case Scenario Pandemic Influenza
Planning for Possible Solutions
Requirement:
Prepare public and responders for mass fatality possibilities prior to pandemic.
Assist responders and other PI workers during pandemic and in post pandemic periods.
Limiting Factors:
The pandemic will virtually affect the entire nation. A shortage of MH personnel will complicate the ability to assist people.
Many people will be doing PI tasks that they are mentally unprepared for and will require assistance.
Strategies for providing psychological first aid and educational / informational materials for all response personnel.
Train first responders and some Citizen Corps people in crisis intervention techniques to assist PI teams during the pandemic.
Set up clinics to assist the public separate from the PI workers and first responders.

12-24
Other Important Planning Considerations In order to develop guidelines or adjust existing plans to suit the pandemic situation, local pandemic planners should ensure that the following organizations are involved in mass fatality planning:
• The Coroner/Medical Examiner • The Local Health Officer(s) • The Emergency Response Disciplines • Representatives of the Funeral Directors Association • Representatives from local health care facilities, and • Representatives of local religious and ethnic groups.
Existing disaster plans may include provisions for mass fatalities but should be reviewed and tested regularly, to determine if these plans are appropriate for the relatively long period of increased demand which may occur in a pandemic, as compared to the shorter response period required for most disaster plans. There are currently no plans to recommend mass burials or mass cremations. This should only be considered in the most extreme circumstances. Since it is expected that most fatal influenza cases will seek medical services prior to death, hospitals, nursing homes, and other institutions (including nontraditional sites) must plan for more rapid processing of decedents. These institutions should work with the pandemic planners, Funeral Directors, and the Coroner/M.E. office to ensure that they have access to the additional supplies (e.g., body bags) and can expedite the steps, including the completion of required documents, necessary for efficient fatality management during a pandemic. In order to deal with the increase in fatalities, some municipalities will find it necessary to establish temporary morgues. Plans should be based on the capacity of existing facilities compared to the projected demand, for each municipality. Access to these resources should be discussed with the owner/operators as part of the planning process during the interpandemic period. In the event that local funeral directors are unable to handle the increased number of fatalities and funerals, it will be the responsibility of local governments to make appropriate arrangements. Individual municipalities should work with local funeral directors to plan for alternate arrangements. Planning should also include a review of death documentation requirements and regulatory requires that may affect the timely management of fatalities. Role of the Funeral Directors Association It is recommended that all funeral directors contact their respective Coroner/M.E. and Public Health Officer to become involved in their disaster and pandemic planning activities with respect to the management of mass fatalities at a local level. It is recommended that funeral directors

12-25
consider it a part of their professional standards to make contingency plans for what would happen if they were incapacitated or overwhelmed. Autopsies Many deaths in a pandemic would not require autopsies since autopsies are not indicated for the confirmation of influenza as a cause of death. However, for the purpose of public health surveillance (e.g., confirmation of the first cases at the start of the pandemic), respiratory tract specimens or lung tissue for culture or direct antigen testing could be collected post-mortem. Any changes to regular practices pertaining to the management of fatalities and autopsy requirements during pandemic situations would require the authorization of the Coroner/Medical Examiner. If a physician requires that an autopsy be performed, normal protocols will be followed, including permission from the next of kin. In cases where the death is reportable to a Medical Examiner or Coroner, the usual protocols prevail based on current law. Preparation for Cemeteries and Crematoria In a pandemic, each individual funeral home could expect to handle about six months work within a 6 to 8 week period. That may not be the problem in some communities, but funeral homes in larger cities may not be able to cope with the increased demand. Individual cemeteries should be encouraged to make specific plans regarding the need for additional human resources during a pandemic situation. For example, volunteers from local service clubs or churches may be able to take on tasks such as digging graves, under the direction of current staff. Crematoriums will also need to look at the surge capacity within their facilities. Most crematoriums can handle about one body every four hours and could probably run 24 hours to cope with the increased demand. Cremations have fewer resource requirements than burials and, where acceptable, this may be an expedient and efficient way of managing large numbers of decedents during a pandemic. Planning for Temporary Morgues Additional temporary cold storage facilities may be required during a pandemic, for the storage of decedents prior to their transfer to funeral homes. A temporary morgue must be maintained at 4 – 8 degrees Celsius. However, decedents will begin to decompose in a few days when stored at this temperature. If the body is not going to be cremated, plans may have to be made to expedite the embalming process should be developed since in the case of a pandemic, bodies may have to be stored for an extended period of time.

12-26
Each county should make pre-arrangements for temporary morgues based on local availability and requirements. The resource needs (e.g. body bags) and supply management for temporary morgues should also be addressed. The types of temporary cold storage to be considered may include refrigerated trucks, cold storage lockers and portable facilities. Refrigerated trucks can generally hold 25-30 bodies without additional shelving. To increase storage capacity, temporary wooden shelves can be constructed of sufficient strength to hold the bodies. Shelves should be constructed in such a way that allows for safe movement and removal of bodies (i.e., storage of bodies above the waist height is not recommended). To reduce any liability for business losses, jurisdictions should avoid using trucks with markings of a supermarket chain or other companies, as the use of such trucks for storage of fatalities may result in negative implications for business. Using local businesses for the storage of human remains is not recommended and should only be considered as a last resort. The post-pandemic implications of storing human remains at these sites can be serious, and may result in negative impacts on business with ensuing liabilities. Death Registration Death registration is a municipal responsibility. There is a distinction between the practices of pronouncing and certifying a death. In the pandemic situation, with the increased number of deaths, each jurisdiction must have a fatality collection plan in place to ensure that there is no unnecessary delay in moving a body to the (temporary) morgue. If the person’s death does not meet any of the criteria for needing to be reported to a coroner, then the person could be moved to a holding area soon after being pronounced dead. Then, presumably on a daily basis, a physician could be designated to complete the death certificate. Funeral directors generally have standing administrative policies that prohibit them from collecting a body from the community or an institution until there is a completed death certificate. In the event of a pandemic with many bodies, it seems likely that funeral directors could work out a more flexible practice if directed to do so by some central authority. These special arrangements must be planned in advance of the pandemic and should include consideration of the regional differences in resources, geography, and population. Infection Control Special infection control measures are not required to the handling of persons who died from influenza, as the body is not “contagious” after death. Funeral homes should take special precautions with deaths from influenza.

12-27
Families requesting cremation of their deceased relative are much less likely to request a visitation, thus reducing the risk of spreading influenza through public gatherings. See Addendum A for information pertaining to infectious risk of corpses. Transportation No special vehicle or driver license is needed for transportation of a dead body. Therefore, there are no restrictions on families transporting bodies of family members if they have a death certificate. Transportation of bodies from their place of death to their place of burial in rural communities may become an issue, especially if this requires air transport. Local pandemic planners should consider extreme distances in transporting dead bodies to their burial site. Supply Management Funeral directors may consider not ordering excessive amounts of supplies such as embalming fluids, body bags, etc.; they may have enough on hand in a rotating inventory to handle the first wave of the pandemic (that is enough for six months of normal operation). Fluids can be stored for years, but body bags and other supplies have a limited shelf life. Cremations generally require fewer supplies since embalming is not required. Families having multiple deaths are unlikely to be able to afford higher-cost products or arrangements. Funeral homes could quickly run out of lower-cost items (e.g., inexpensive caskets such as cloth and some wooden caskets) and should be prepared to provide alternatives. Special Populations A number of religious and ethnic groups have specific directives about how bodies are managed after death, and as such must be considered as part of the pandemic planning. Native Americans, Jews, Hindus, Muslims, all have specific directives for the treatment of bodies and for funerals. The wishes of the family will provide guidance; however, if no family is available, local religious or ethnic communities can be contacted for information. As a result of these special requirements, some religious groups maintain facilities such as small morgues, crematoria, and other facilities, which are generally operated by volunteers. Religious groups should be contacted to ensure these facilities and volunteers are prepared to deal with pandemic issues. Religious leaders should be involved in planning for funeral management, bereavement counseling, and communications, particularly in ethnic communities with large numbers of people who do not speak the official languages. * Guideline information adapted from Canadian Pandemic Influenza Plan, February 2004.
12-28
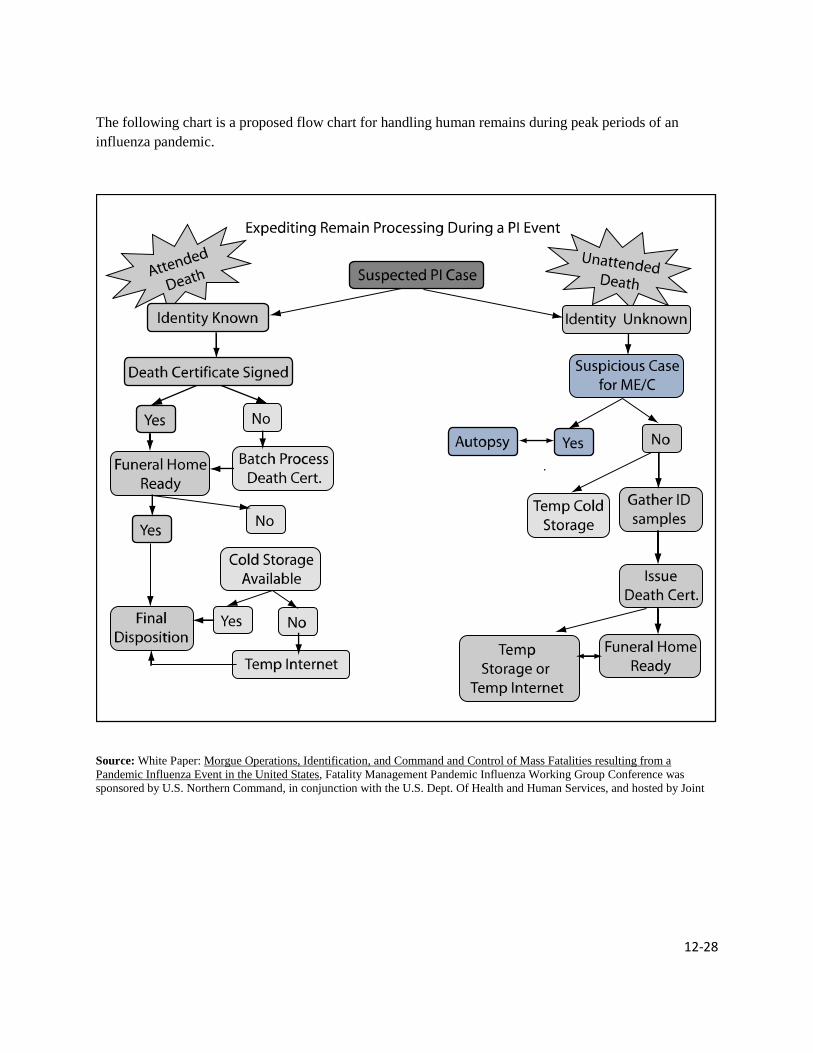
The following chart is a proposed flow chart for handling human remains during peak periods of an influenza pandemic.
Source: White Paper: Morgue Operations, Identification, and Command and Control of Mass Fatalities resulting from a Pandemic Influenza Event in the United States, Fatality Management Pandemic Influenza Working Group Conference was sponsored by U.S. Northern Command, in conjunction with the U.S. Dept. Of Health and Human Services, and hosted by Joint
12-29
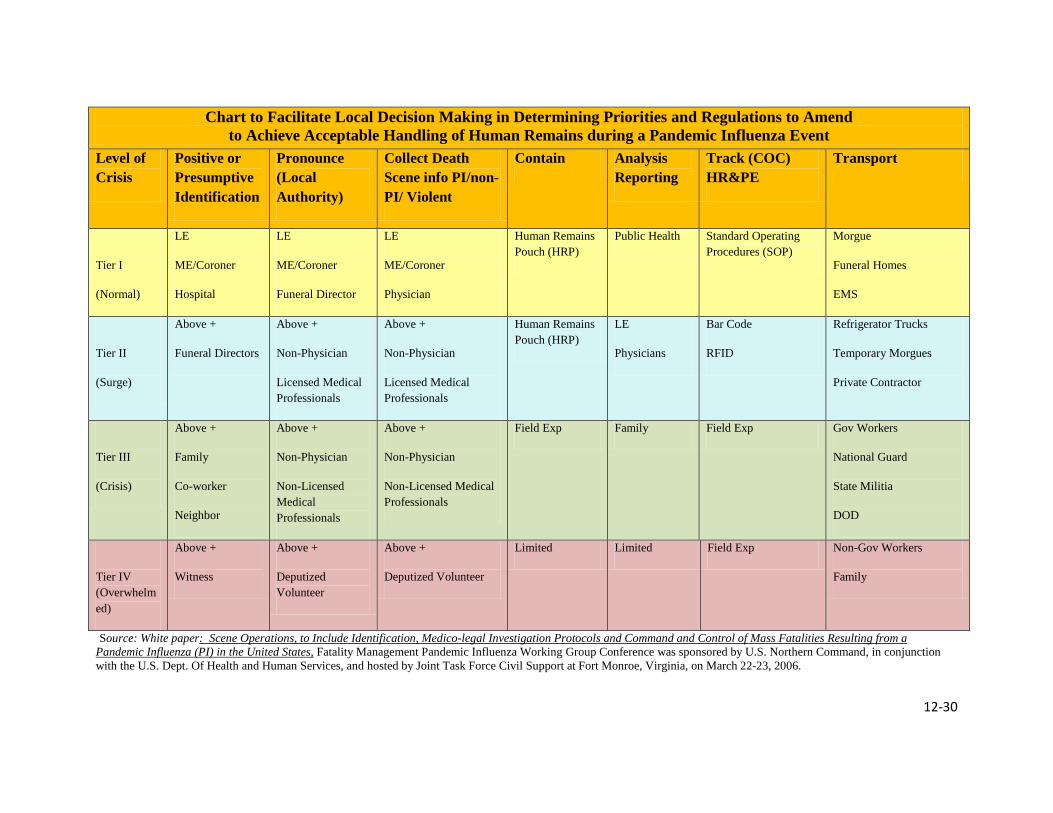
Chart to Facilitate Local Decision Making in Determining Priorities and Regulations to Amend to Achieve Acceptable Handling of Human Remains during a Pandemic Influenza Event
The following chart was developed to assist jurisdictions in making decisions about how they may want to adapt their own regulations and priorities to achieve acceptable handling of deaths in a PI event. It begins from the moment a death is discovered/reported until the body has been transported to whatever is functioning as a morgue. The columns represent the tasks that should be completed to ensure medico-legal concerns are met regarding documentation of the death scene and transport of the body to the morgue. The rows represent a qualitative division of who may have to perform said tasks as the situation deteriorate and resources are depleted.
The chart is presented as a starting point for discussion so that each jurisdiction can use it to arrive at whatever compromise best suits their own situation and priorities. At the time of a PI event, it will then be up to local officials to make the decision about when which functions have reached which Tier. (see below)
12-30
Source: White paper: Scene Operations, to Include Identification, Medico-legal Investigation Protocols and Command and Control of Mass Fatalities Resulting from a Pandemic Influenza (PI) in the United States, Fatality Management Pandemic Influenza Working Group Conference was sponsored by U.S. Northern Command, in conjunction with the U.S. Dept. Of Health and Human Services, and hosted by Joint Task Force Civil Support at Fort Monroe, Virginia, on March 22-23, 2006.
Chart to Facilitate Local Decision Making in Determining Priorities and Regulations to Amend to Achieve Acceptable Handling of Human Remains during a Pandemic Influenza Event
Level of Crisis
Positive or Presumptive Identification
Pronounce (Local Authority)
Collect Death Scene info PI/non-PI/ Violent
Contain Analysis Reporting
Track (COC) HR&PE
Transport
Tier I
(Normal)
LE
ME/Coroner
Hospital
LE
ME/Coroner
Funeral Director
LE
ME/Coroner
Physician
Human Remains Pouch (HRP)
Public Health Standard Operating Procedures (SOP)
Morgue
Funeral Homes
EMS
Tier II
(Surge)
Above +
Funeral Directors
Above +
Non-Physician
Licensed Medical Professionals
Above +
Non-Physician
Licensed Medical Professionals
Human Remains Pouch (HRP)
LE
Physicians
Bar Code
RFID
Refrigerator Trucks
Temporary Morgues
Private Contractor
Tier III
(Crisis)
Above +
Family
Co-worker
Neighbor
Above +
Non-Physician
Non-Licensed Medical Professionals
Above +
Non-Physician
Non-Licensed Medical Professionals
Field Exp Family Field Exp Gov Workers
National Guard
State Militia
DOD
Tier IV (Overwhelmed)
Above +
Witness
Above +
Deputized Volunteer
Above +
Deputized Volunteer
Limited Limited Field Exp Non-Gov Workers
Family
12-31
Addendum A
Infectious Risk of Human Corpses “Epidemic caused by dead bodies: a disaster myth that does not want to die.” Claude de Ville de Goyet In preparing for a catastrophic mass fatality it is important for the responders and the public to understand the myths and realities surrounding the presence of large numbers of dead bodies. There is a widespread false belief that dead bodies are a source of disease and therefore a threat to public health. This misconception by some uninformed community leaders and citizens may place undue pressure on the Coroner/M.E. and state authorities to cause the rapid unplanned disposal of the dead, sometimes before proper identification of the victims can be made. Concerns about disease may also lead to unnecessary “precautions” such as burying the deceased in common graves. The state should coordinate with the local Coroner/M.E. in educating and informing the public regarding the facts and falsehoods of managing the dead after a disaster. The World Health Organization, Regional Office for the Western Pacific has produced a fact sheet that provides more definitive information on the risks in handling dead bodies. See below:

12-32
FACT SHEET World Health Organization Regional Office for the Western Pacific
Care of the Dead in Disasters 07 December 2006
Background Every year, more than 100 000 people are killed during natural disasters and millions are injured and disabled. Governments are frequently overwhelmed by such large numbers of dead and may order mass burials in the interests of protecting public health. Initial media focus is often on the dead and graphic images of dead bodies among the debris creates pressure on governments to “do something”. There is a widespread and erroneous belief, even among some health professionals, that dead bodies are a source of disease and therefore a threat to public health. This is untrue. There has never been a documented case of an epidemic occurring after a natural disaster that could be traced to exposure to dead bodies. In fact, epidemics of any kind are very unusual after natural disasters. In the past five years, there have been many major disasters with tens to hundreds of thousands of dead lying uncollected for days or even weeks. In none of these disasters did epidemics of any kind occur. Those killed by natural disasters are generally healthy at the time of their death, and therefore very unlikely be a source of infection to others. The microorganisms responsible for the decomposition of bodies are not capable of causing disease in living people. Most infectious agents of public health concern that may be present at the time of death will themselves die within hours of the person dying. Generally, for an epidemic to occur, certain necessary conditions related to infectious agents, susceptible hosts and a favorable environment have to be met. If any of these conditions are not present an epidemic cannot occur. Experience has shown that a disaster event of itself does not automatically create these conditions. However, epidemics certainly can occur in the period after a disaster. The peak danger period is between 10 days and one month after the event. Unsafe food and a lack of access to safe water, lack of facilities for personal hygiene and safe sanitation arrangements all create a real risk for outbreaks of infectious disease at any time, but after a disaster these conditions, added to large numbers of people in overcrowded temporary shelters, makes an epidemic certainly possible. It is how the survivors are managed, rather than how the dead are managed, that determines if and when an epidemic may occur. Despite this potential, there have been no recorded serious epidemics in recent times after a disaster, which is evidence of the great progress made in disaster planning, response and recovery. Certain diseases, such as HIV and hepatitis, pose a potential risk for individuals who come into close contact with dead bodies, but not for the general public. Those assigned any roles associated with handling dead bodies and body parts should be properly trained and always use protective equipment. Overall, care of the dead is not a primary health sector responsibility. There is no public health threat from dead bodies and this misapprehension causes unnecessary diversion of staff and resources at a critical time. Pressure from misinformed journalists and media organizations can

12-33
cause governments to behave inappropriately, for example spraying the area around dead bodies with disinfectant or covering dead bodies with lime. These operations are costly, time consuming, require complicated logistics and coordination, take staff away from caring for survivors and are totally unnecessary. Recommendations for the care of the dead Care of the dead and missing is an important area of work after a disaster and is clearly a major social responsibility of government. It is very important for the psychological recovery of survivors to have their dead relatives returned to them for culturally appropriate rites and disposal. A well organized system for the retrieval, storage, identification and disposal of the dead is an essential part of a national disaster management structure, but like other parts of that structure, it must be properly planned and resourced. WHO recommends the following: 1. Governments must define in law and national policy the arrangements required for dealing with the dead after a disaster and mandate a specific agency to take responsibility for this task. 2. The mandated agency must have the resources needed to fulfill its responsibility and its staff must have the required knowledge and skills to fulfill their role. 3. Local government must have plans in place for dealing with large numbers of dead bodies, based on the protocols, procedures and guidelines issued by the mandated agency. References A list of references and downloadable material can be found at: http://www.who.int/hac/techguidance/ems/myths/en/index

12-34
References
Managing Mass Fatalities: A Toolkit for Planning, Santa Clara County Public Health Department Advanced Practice Center (APC), May, 2008 is available at: http://www.sccgov.org/portal/site/phd/agencychp?path=%2Fv7%2FPublic%20Health%20Department%20(DEP)%2FAPC%2FManaging%20Mass%20Fatalities
Morgue Operations, Identification, and Command and Control of Mass Fatalities Resulting from a Pandemic Influenza Event in the United States, Fatality Management Pandemic Influenza Working Group Conference White Paper, March 2006 is available at: http://www.icfa.org/pdf/white_paperMFM.pdf
Scene Operations, to Include Identification, Medico-legal Investigation Protocols and Command and Control of Mass Fatalities resulting from a Pandemic Influenza Event in the United States, Fatality Management Pandemic Influenza Working Group Conference White Paper, March 2006 is available at: http://www.pandemicpractices.org/practices/resource.do?resource-id=176&standards-id=4.
The California Mass Fatality Management Guide: A Supplement to the State of California Coroner’s Mutual Aid Plan, Governor’s Office of Emergency Services, September, 2007.
The Canadian Pandemic Influenza Plan for the Health Sector, Annex I Guidelines for the Management of Mass Fatalities During an Influenza Pandemic, Public Health Agency of Canada, February 2004 is available at: http://www.phac-aspc.gc.ca/cpip-pclcpi/ann-i-eng.php