male hypogonadism and testosterone therapy · men with clinical symptoms and testosterone
TRANSCRIPT

Male Hypogonadism and Male Hypogonadism and
Testosterone therapyTestosterone therapy
Ketan DhatariyaKetan Dhatariya

Overview: Male HypogonadismOverview: Male Hypogonadism
Physiology of testosterone secretionPhysiology of testosterone secretion
Aetiology and clinical features Aetiology and clinical features
EpidemiologyEpidemiology
DiagnosisDiagnosis
Indications for treatmentIndications for treatment
Treatment optionsTreatment options
Monitoring Monitoring
ConclusionConclusion

Physiology of testosterone Physiology of testosterone
secretionsecretion

Testis structureTestis structure

TestosteroneSMOOTH
ENDOPLASMICRETICULUM
Cholesterol
Pregnenolone
Testosterone
Progesterone
17αααα-OH-Progesterone
Androstenedione
Testosterone
cAMP ATP
Cholesteryl
esters
LH
Cholesterol
P450scc
Pregnenolone
MITOCHONDRIA
Testosterone synthesis in the Leydig cell
17αααα-OH-Pregnenolone
DHEA
Androstenediol
3β-HSD
3β-HSD
3β-HSD
3β-HSD
17α-OH-lase17α-OH-lase
17,20 lyase17,20 lyase
17β-HSD17β-HSD

TestosteroneTestosterone
O
OH
Testosterone is the most important hormone Testosterone is the most important hormone
produced by the testisproduced by the testis
Between 5 and 7mg of testosterone are Between 5 and 7mg of testosterone are
produced by the Leydig cells daily in adult menproduced by the Leydig cells daily in adult men
Nieschlag E and Behre HM. Testosterone: action, deficiency, substitution (3rd Edition). Cambridge University Press, 2004

Hypothalamus
(Activin)
Regulation of Testicular FunctionRegulation of Testicular Function
GnRH
FSH
Oestradiol
Testosterone Inhibin B
LH
Leydig cells Sertoli cells
Interstitial cells
ENDOCRINE
Seminiferous tubules
EXOCRINE

Binding of TestosteroneBinding of Testosterone
T firmly bound T firmly bound
to SHBGto SHBG
60%60%
BIOAVAILABLE TESTOSTERONE BIOAVAILABLE TESTOSTERONE
= Albumin= Albumin--bound T + Free Tbound T + Free T
Free TFree TT loosely bound T loosely bound
to albuminto albumin
2%2%38%38%

Testosterone and its MetabolitesTestosterone and its Metabolites
Sexual differentiationMusculature
Bone massErythropoiesisPsychotropic actionPotency/libidoLipid metabolism
Bone massEpiphyseal closurePsychotropic actionLipid metabolismFeedback action
Prostate
Sexual differentiationSecondary hairSebum production
Prostate
Testosterone
Dihydrotestosterone Oestradiol
Aromatase
Aromatase
55ΩΩ-- Reduct
ase
Reductase

Hypogonadism: Aetiology and Hypogonadism: Aetiology and
Clinical FeaturesClinical Features

HypogonadismHypogonadism Hypogonadism is inadequate function of the Hypogonadism is inadequate function of the
testestestes
Prevalence: 5 men in 1000 in the UKPrevalence: 5 men in 1000 in the UK
22--4 million men in the US, estimated only 5% treated4 million men in the US, estimated only 5% treated
Diagnosis: clinical symptoms and biochemical Diagnosis: clinical symptoms and biochemical
teststests
PresentationPresentation
PrePre--pubertal: lack of secondary sexual development pubertal: lack of secondary sexual development
in teensin teens
PostPost--pubertal: insidious onset, features overlapping pubertal: insidious onset, features overlapping
with many systemic conditions, infertilitywith many systemic conditions, infertilityPetak SM et al. Endocrine Pract 2002;8:439-456. Nieschlag E et al. Eur Urol 2005;48:1-4. Handelsman DJ.
Androgens. In: Male reproductive endocrinology; Ed. Mclachlan RI. Endotext.com; 2002 Rhoden EL & Morgentaler A. NEJM 2004;350:482-92.

Clinical Picture of Testosterone Clinical Picture of Testosterone
DeficiencyDeficiency
•• Decreased muscle Decreased muscle
bulk/powerbulk/power
•• Abdominal obesityAbdominal obesity
•• Loss of libidoLoss of libido
•• Hot flushes/palpitationsHot flushes/palpitations
•• Decreased body hairDecreased body hair
•• AnaemiaAnaemia
•• SubfertilitySubfertility
•• Subnormal genital sizeSubnormal genital size
•• Loss of pubic hairLoss of pubic hair
•• Erectile dysfunctionErectile dysfunction
•• Sexual dysfunctionSexual dysfunction
•• DepressionDepression
•• Reduced wellReduced well--beingbeing
•• Low self esteemLow self esteem
•• Poor concentration/drivePoor concentration/drive
General body effectsGeneral body effects
Reproductive systemReproductive system
EmotionalEmotional ComplicationsComplications•• OsteoporosisOsteoporosis
•• Raised lipidsRaised lipids
•• Insulin resistanceInsulin resistance
•• SarcopaeniaSarcopaenia
Nieschlag E and Behre HM. Testosterone: action, deficiency, substitution (3rd Edition). Cambridge University Press; 2004.
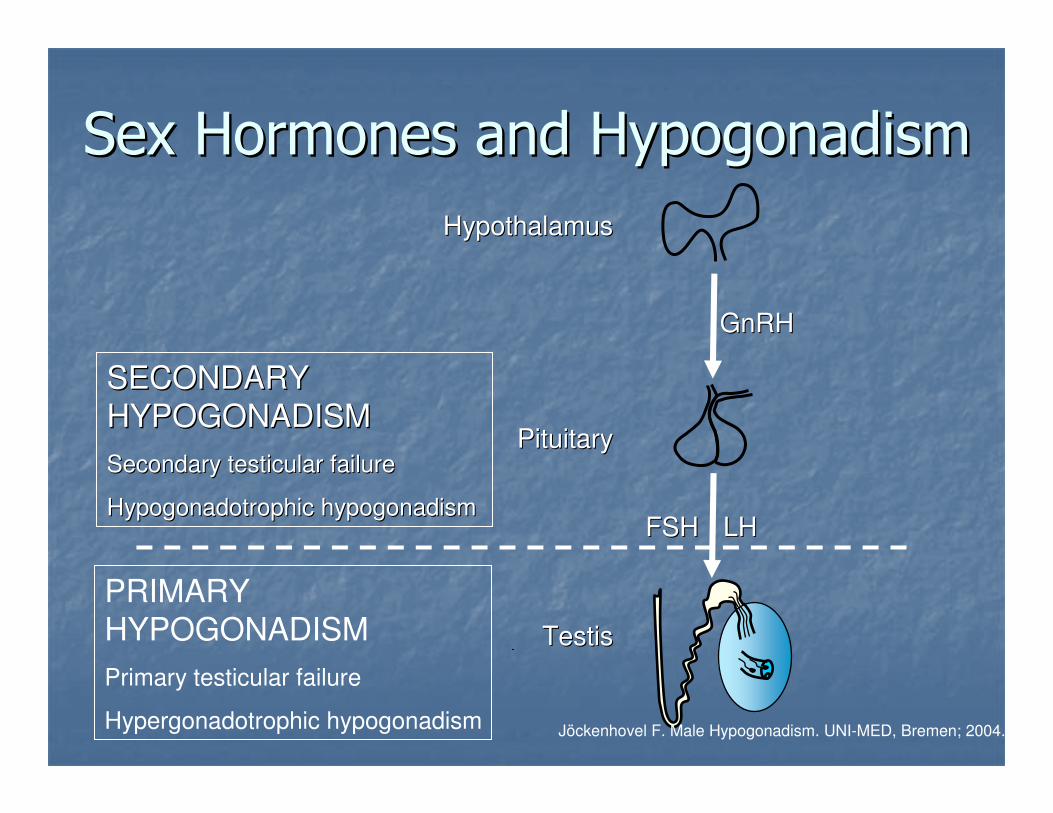
Sex Hormones and HypogonadismSex Hormones and Hypogonadism
Jöckenhovel F. Male Hypogonadism. UNI-MED, Bremen; 2004.
LHLHFSHFSH
GnRHGnRH
HypothalamusHypothalamus
PituitaryPituitary
TestisTestis
SECONDARY SECONDARY
HYPOGONADISMHYPOGONADISM
Secondary testicular failure Secondary testicular failure
HypogonadotrophicHypogonadotrophic hypogonadismhypogonadism
PRIMARY HYPOGONADISM
Primary testicular failure
Hypergonadotrophic hypogonadism

Causes of Primary HypogonadismCauses of Primary Hypogonadism
CongenitalCongenital
Chromosomal defects e.g. Klinefelter's syndromeChromosomal defects e.g. Klinefelter's syndrome
Congenital Congenital anorchiaanorchia
Androgen receptor/enzyme defectsAndrogen receptor/enzyme defects
AcquiredAcquired
Testicular trauma/torsionTesticular trauma/torsion
Surgical removalSurgical removal
Chemotherapy/irradiationChemotherapy/irradiation
Complications of illnessComplications of illness
e.g. diabetes, renal failure, alcoholic liver disease, e.g. diabetes, renal failure, alcoholic liver disease,
cirrhosiscirrhosis Nieschlag E et al. Human Reprod Update 2004;10(5):409-419.
Causes of Secondary HypogonadismCauses of Secondary Hypogonadism CongenitalCongenital
KallmannKallmann’’ss syndromesyndrome
Idiopathic Idiopathic hypogonadotrophichypogonadotrophic hypogonadism (IHH)hypogonadism (IHH)
PraderPrader--Willi syndromeWilli syndrome
AcquiredAcquired
ProlactinomaProlactinoma
Pituitary adenomaPituitary adenoma
Hypothalamic tumourHypothalamic tumour
Anabolic steroid abuseAnabolic steroid abuse
Complications of illnessComplications of illness
e.g. AIDS, e.g. AIDS, haemochromatosishaemochromatosisNieschlag E & Behre HM. Andrology, Male reproductive health and dysfunction (2nd Edition). Springer, Heidelberg; 2002.
Nieschlag E et al. Human Reproduct Update 2004;10(5):409-419.

LateLate--onset Hypogonadismonset Hypogonadism
A clinical and biochemical syndrome associated A clinical and biochemical syndrome associated
with advancing age and characterised by with advancing age and characterised by
typical symptoms and a deficiency in serum typical symptoms and a deficiency in serum
testosterone levelstestosterone levels
Nieschlag E et al. Eur Urology 2005;48:1-4.
Vermeulen A et al. J Clin Endocrinol Metab 1996;81:1821-1826.
SHBG Free T (x100) TestosteroneSHBG Free T (x100) Testosterone
0
25
50
75
25-34
(n=45)
35-44
(n=22)
45-54
(n=23)
55-64
(n=43)
65-74
(n=47)
75-84
(n=48)
75=100
(n=21)
Ho
rmo
ne level (n
mo
l/L
)
Age

EpidemiologyEpidemiology

Hypogonadism Incidence and Hypogonadism Incidence and
Age (US data)Age (US data)
0
5
10
15
20
25
Overall 48-59 60-69 70-79
Incid
ence
per
1,0
00 p
ers
on-y
ears
Age (years)
Expected 481,000 new cases p.a. in US men Expected 481,000 new cases p.a. in US men
4040--69 yrs69 yrs Araujo A et al. J Clin Endocrinol Metab 2004;89(12):5920-5926.

Low Testosterone and MortalityLow Testosterone and Mortality
0
10
20
30
40
50A
ll-C
ause M
ort
alit
y (
%)
Shores M et al. Arch Intern Med 2006;166:1660-166588% (88% (PP<0.001)<0.001)38% (38% (P P = 0.06)= 0.06)--
Increased Increased
mortality mortality
riskrisk
1.88 (1.341.88 (1.34--2.63)2.63)1.38 (0.991.38 (0.99--1.92)1.92)1.001.00Hazard Hazard
Ratio Ratio
(adjusted)(adjusted)
Low TLow T
(n=166)(n=166)
‘‘EquivocalEquivocal’’ T T
(n=240)(n=240)Normal T levels Normal T levels
(n=452)(n=452)
Mean fo
llow
-up
perio
d 4
.3 y
rs

Hypogonadism and CV risk Hypogonadism and CV risk
factorsfactors
Low testosterone levels in men frequently Low testosterone levels in men frequently
coco--exist withexist with
Type 2 diabetes mellitusType 2 diabetes mellitus
Erectile dysfunctionErectile dysfunction
Abdominal obesityAbdominal obesity
Other CV risk factorsOther CV risk factors
Component of the metabolic syndrome?Component of the metabolic syndrome?
CV, cardiovascular
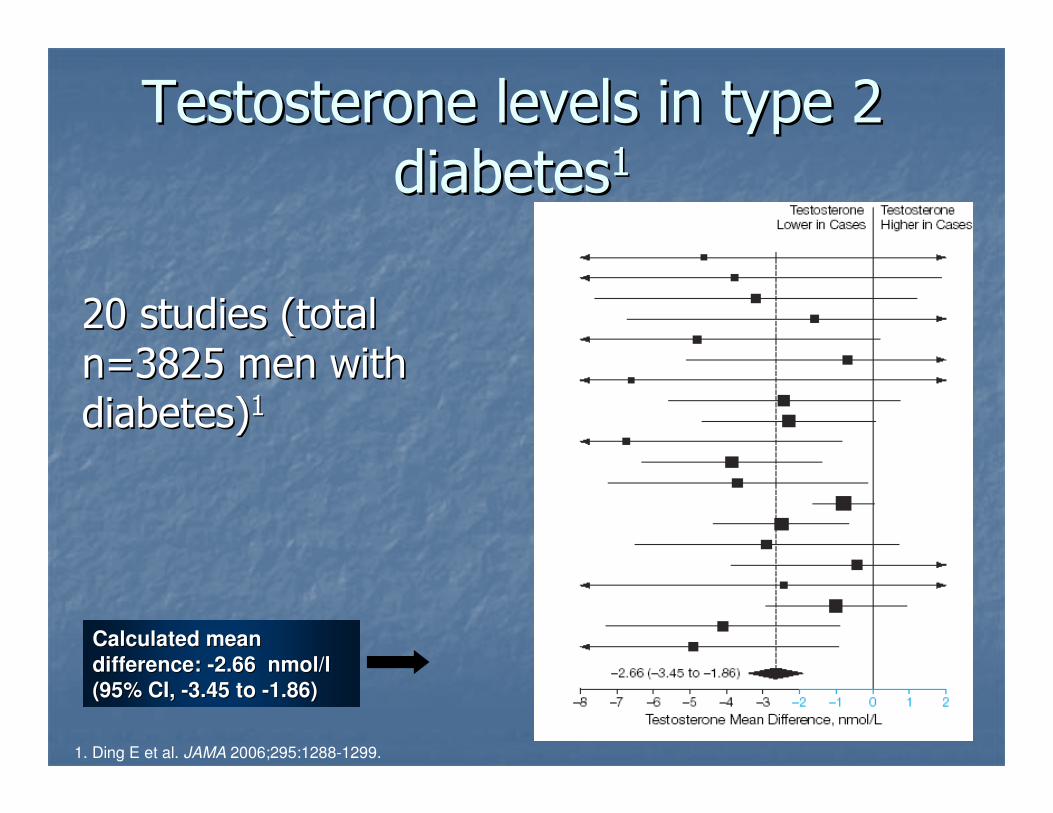
Testosterone levels in type 2 Testosterone levels in type 2
diabetesdiabetes11
20 20 studiesstudies (total (total
n=3825 n=3825 menmen with with
diabetes)diabetes)11
1. Ding E et al. JAMA 2006;295:1288-1299.
Calculated mean Calculated mean
difference: difference: --2.66 nmol/l 2.66 nmol/l
(95% CI, (95% CI, --3.45 to 3.45 to --1.86) 1.86)

Testosterone levels in type 2 Testosterone levels in type 2
diabetesdiabetes11
16%
34%50%
T<7.5nmol/l
T 7.5-12nmol/l
T>12nmol/l
1. Kapoor D et al. Endocrine Soc Abstract Book 2004: 448.
300 UK men (mean age, 58 yrs) with 300 UK men (mean age, 58 yrs) with
type 2 diabetes type 2 diabetes
Testosterone
≤12 nmol/l

Prevalence of hypogonadism Prevalence of hypogonadism
in diabetesin diabetes
0
10
20
30
40
50
Free T Total T Bioavailable T
Perc
enta
ge o
f patients
1. Dhindsa S et al. J Clin Endocrinol Metab 2004; 89(11): 5462-5468.
n=103 men with type 2 diabetesn=103 men with type 2 diabetes

Prevalence of hypogonadism in Prevalence of hypogonadism in
EDED
n=2823 n=242
n=521 n=990
n=165
0
10
20
30
40
50
Bodie,
2003
Low,
2001
Guay,
2001
Guay,
1999
Martinez,
2006*
Perc
enta
ge o
f patients
with
hypog
ona
dis
m
Study:
1. Bodie J et al. J Urol 2003; 169:2262-2264.
2. Low WY et al. J Sex Med 2004;1, Suppl. 1:111.3. Guay AT et al. J Androl 2001;22(5):793-797.
4. Guay AT et al. Endocr Pract 1999;5(6): 314-321.
5. Martinez-Jabaloyas JM et al. BJU Int 2006;97:1278-1283. *Diagnosed from free testosterone level

Hypogonadism in diabetic vs Hypogonadism in diabetic vs
nondiabeticnondiabetic men with EDmen with ED11
22.3
34.0
All ages
ED no diabetes Diabetes
0
10
20
30
40
50
30-39 40-49 50-59 60-69 >70
Age (Years)
% H
yp
og
on
ad
ism
(T
<1
2n
mo
l/L
) p <0.0001
p <0.0001
1. Corona G et al. Eur Urol 2004; 46(2): 222-228.
n=1027 men with ED with and without type 2 diabetes mellitus
+ ED

0
4
8
12
16
20
24
<94cm 94 - 101.9cm 102cm≥
Waist circumference and Waist circumference and
testosterone leveltestosterone level11T
ota
l te
sto
ste
rone (
nm
ol/l)
1. Svartberg J et al. Europ J Epidemiol 2004;19:657-663.
Waist circumference (age-adjusted)
p =0.012
vs <94cm
The The TromsTromsøø Study: n=1548 Study: n=1548 communitycommunity--
dwellingdwelling menmen (age 25 (age 25 –– 84)84)11
--
(<37 inches) (37-40.1 inches) (≥40.2 inches)
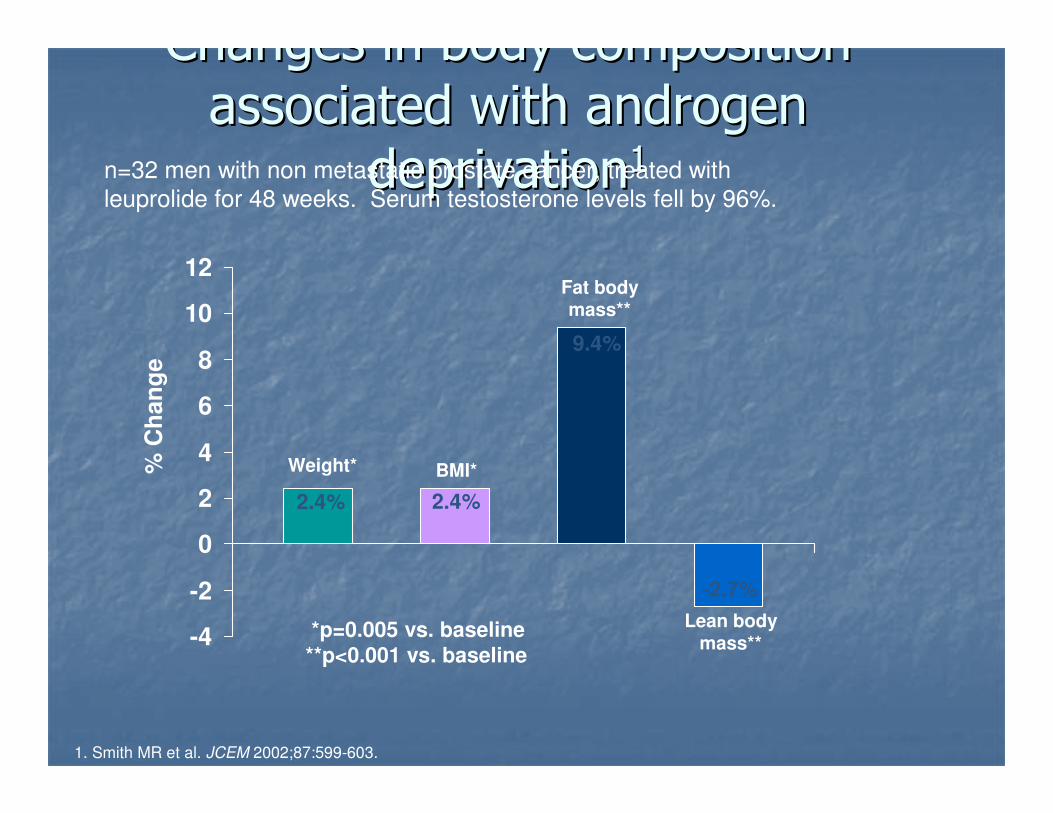
Changes in body composition Changes in body composition
associated with androgen associated with androgen
deprivationdeprivation11
1. Smith MR et al. JCEM 2002;87:599-603.
n=32 men with non metastatic prostate cancer, treated with
leuprolide for 48 weeks. Serum testosterone levels fell by 96%.
-4
-2
0
2
4
6
8
10
12
% C
han
ge
2.4% 2.4%
9.4%
-2.7%
Weight* BMI*
Fat body mass**
Lean body mass**
*p=0.005 vs. baseline
**p<0.001 vs. baseline

1. Hypogonadism and Age1 2. Hypogonadism and Diabetes2
3. Hypogonadism and ED3-7 4. Low T and WaistCircumference8
Hypogonadism and CV risk Hypogonadism and CV risk
factorsfactors
1. Araujo A et al. J Clin Endocrinol Metab 2004;89(12):5920-5926. 2. Dhindsa S et al. J Clin Endocrinol Metab 2004; 89(11): 5462-5468. 3. Bodie J et al. J Urol 2003; 169:2262-2264. 4. Low WY et al. J Sex Med 2004;1, Suppl. 1:111. 5. Guay AT et al. J Androl 2001;22(5):793-797. 6. Guay AT et al. Endocr Pract 1999;5(6): 314-321. 7. Martinez-Jabaloyas JM et al. BJU Int 2006;97:1278-1283. 8. Svartberg J et al. Europ J Epidemiol 2004;19:657-663.
n=1087 n=103
n=1548

Diagnosing hypogonadismDiagnosing hypogonadism

Diagnosis of hypogonadismDiagnosis of hypogonadism11
Appropriate assessment of symptoms as Appropriate assessment of symptoms as
suggested by patientsuggested by patient’’s history and s history and
physical examinationphysical examination
Biochemical tests:Biochemical tests:
Total testosterone assayTotal testosterone assay
Gonadotrophins: LH/FSHGonadotrophins: LH/FSH
ProlactinProlactin
SHBG (can be used to calculate free SHBG (can be used to calculate free
testosterone)testosterone)1. Nieschlag E & Behre HM. Andrology, Male reproductive health and dysfunction (2nd Edition). Springer,
Heidelberg; 2002.
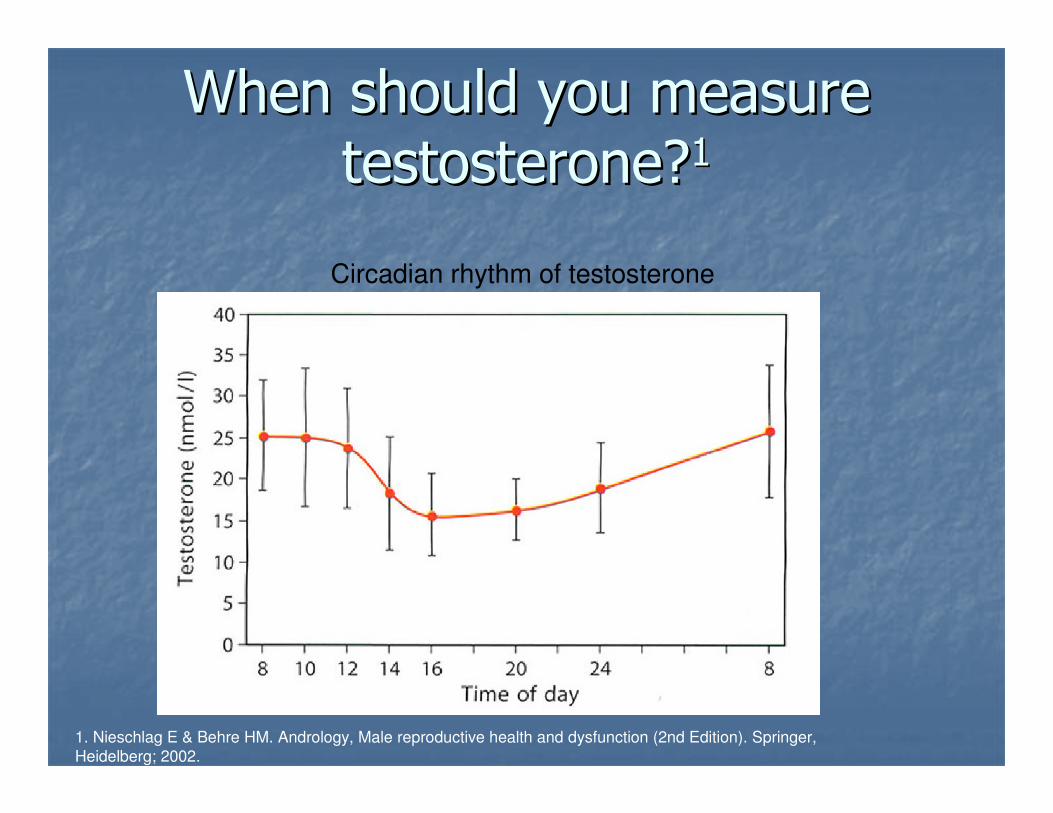
When should you measure When should you measure
testosterone?testosterone?11
Circadian rhythm of testosterone
1. Nieschlag E & Behre HM. Andrology, Male reproductive health and dysfunction (2nd Edition). Springer,
Heidelberg; 2002.

Patient history and physical examinationPatient history and physical examination
Measure serum testosterone levels between 7Measure serum testosterone levels between 7--11am11am
Patient presents with symptomsPatient presents with symptoms
T >12nmol/lT >12nmol/l
Consider alternative Consider alternative
diagnosesdiagnoses
T T ≤≤12nmol/l12nmol/l
Repeat T levelRepeat T level
Measure LH, FSH, Measure LH, FSH,
ProlactinProlactin
Repeat tests Repeat tests HYPOGONADISMHYPOGONADISM
T >12nmol/L, T >12nmol/L,
normal normal
Prolactin and Prolactin and
FSH/LHFSH/LH
T 8T 8--12nmol/L 12nmol/L
normal normal
Prolactin and Prolactin and
FSH/LHFSH/LH
T 8T 8--12nmol/L, 12nmol/L,
and and Prolactin Prolactin
or abnormal or abnormal
FSH/LHFSH/LH
T <8nmol/LT <8nmol/L

Patients with borderline Patients with borderline
testosterone levels (8testosterone levels (8--12 12
nmol/l)nmol/l)1,21,2
Consider additional biochemical testsConsider additional biochemical tests
Gonadotrophins, SHBG, prolactinGonadotrophins, SHBG, prolactin
Careful consideration of comorbiditiesCareful consideration of comorbidities
Calculate free testosterone Calculate free testosterone (see online (see online
calculator at calculator at
www.issam.ch/freetesto.htmwww.issam.ch/freetesto.htm))
Counsel patient regarding treatment Counsel patient regarding treatment
optionsoptions
1. Nieschlag E et al. Eur Urol 2005;48:1-4.
2. Bhasin S et al. J Clin Endocrinol Metab 2006;91(6):1995-2010.

Who should receive Who should receive
testosterone treatment? testosterone treatment? Men with clinical symptoms and Men with clinical symptoms and
testosterone <8 nmol/ltestosterone <8 nmol/l11
Men with clinical symptoms and Men with clinical symptoms and
testosterone 8testosterone 8--12 nmol/l where 12 nmol/l where
additional investigations indicate additional investigations indicate
presence of hypogonadismpresence of hypogonadism11
Older men with significant symptomsOlder men with significant symptoms
LongLong--term risks /benefits have yet to be term risks /benefits have yet to be
clearly demonstratedclearly demonstrated

Who should receive Who should receive
testosterone treatment? testosterone treatment? Contraindications to testosterone treatment
• Untreated or suspected carcinoma of prostate
• Moderate to severe symptoms of BPH
• Breast cancer
• Liver tumour
• Significant polycythaemia
• Severe cardiac failure
• Untreated sleep apnoea

15
12
10
8
0
Loss of libido p<0.001
Loss of vigour p<0.001
Obesity p<0.001
Feeling depressed p=0.001
Disturbed sleep p=0.004
Lack concentration p=0.002
Type 2 diabetes p<0.001
Hot flushes p<0.001
Erectile dysfunction p=0.003
N
84
65
67
75
Increasing prevalence of symptoms with
decreasing androgen concentrations
Zitzmann M et al. JCEM 2006;91:4335-4343
Total testosterone nmol/L

Treating hypogonadismTreating hypogonadism

Goals of testosterone Goals of testosterone
replacement therapyreplacement therapy1,21,2
Restore physiological testosterone levels Restore physiological testosterone levels
Alleviate symptoms of androgen Alleviate symptoms of androgen
deficiencydeficiency
Induce or restore physiological functionsInduce or restore physiological functions
Prevent longPrevent long--term health risks of term health risks of
androgen deficiencyandrogen deficiency
1. Nieschlag E et al. Eur Urol 2005;48:1-4.
2. Bhasin S et al. J Clin Endocrinol Metab 2006;91(6):1995-2010.

20
25
30
35
40
S 0 3 6 9 12 15 18 21 24 27 30
Testosterone therapy increases Testosterone therapy increases
testosterone levels and testosterone levels and
decreases SHBGdecreases SHBG11
Serum
testosterone (nmol/l)
(trough levels)
SHBG levels
(nmol/l)
Time (weeks)
Hypogonadal men Hypogonadal men
on IM on IM
testosterone testosterone
undecanoate undecanoate
(n=20) or IM (n=20) or IM
testosterone testosterone
enanthate (n=20) enanthate (n=20)
for 30 weeksfor 30 weeks
1. Huebler D et al. Int J Impot Res 2002;12 (Suppl.):33 (Abstract).
0
10
20
30
Normal physiological range
Testosterone undecanoate
Testosterone enanthate
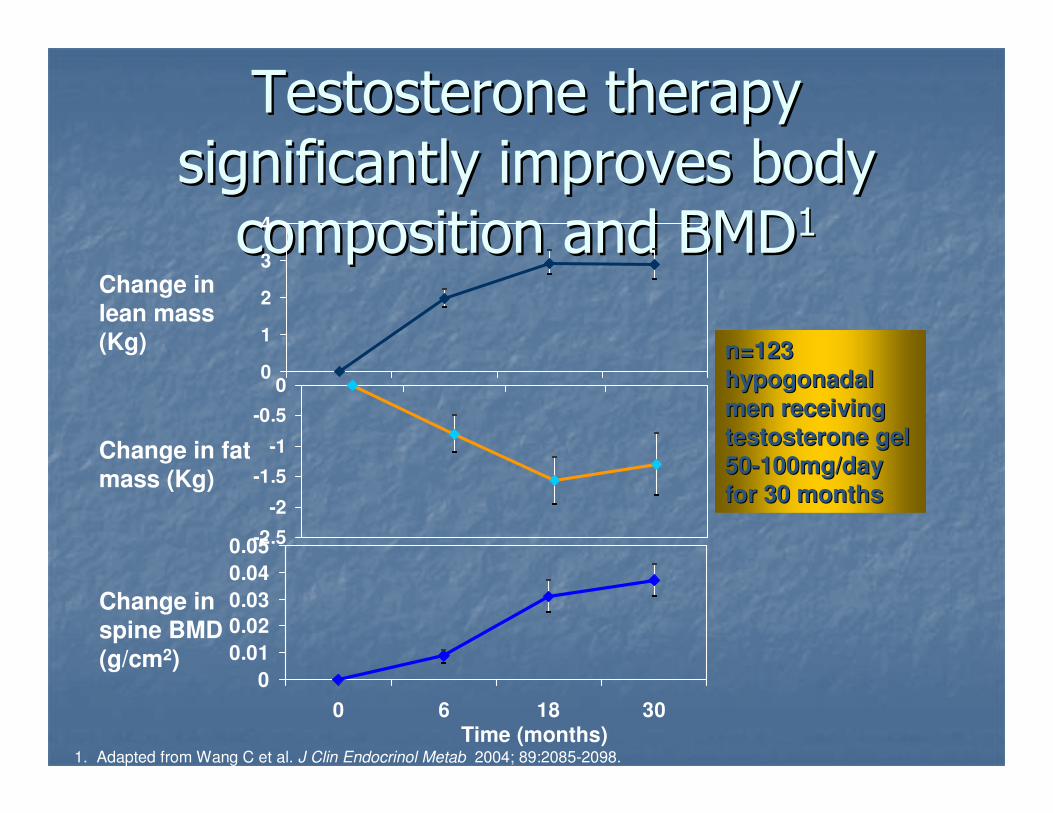
Testosterone therapy Testosterone therapy
significantly improves body significantly improves body
composition and BMDcomposition and BMD11
0
1
2
3
4
-2.5
-2
-1.5
-1
-0.5
0
0
0.01
0.02
0.03
0.04
0.05
0 6 18 30
Change in lean mass (Kg)
Change in fat mass (Kg)
Change in spine BMD
(g/cm2)
Time (months)
n=123 n=123
hypogonadal hypogonadal
men receiving men receiving
testosterone gel testosterone gel
5050--100mg/day 100mg/day
for 30 monthsfor 30 months
1. Adapted from Wang C et al. J Clin Endocrinol Metab 2004; 89:2085-2098.

Testosterone therapy improves Testosterone therapy improves
mood and sexual functionmood and sexual function11
0
1
2
3
4
No
spontaneous morning erections
No
ejaculations
Subjective change in
fatigue
Time (weeks)
Hypogonadal Hypogonadal
men on IM men on IM
testosterone testosterone
undecanoate undecanoate
(n=20) for 30 (n=20) for 30
weeksweeks
1. Rouskova D. Schering Data on file, 6 May 2002..
0
1
2
3
4
0
20
40
60
0 3 6 9 12 15 18 21 24 27 30

Testosterone therapy reduces Testosterone therapy reduces
insulin resistance in insulin resistance in
hypogonadal diabetic menhypogonadal diabetic men11
1. Kapoor D et al. Eur J Endocrinol 2006;154:899-906.
HO
MA
in
de
x
*P=0.02, **P=0.003.
B) Mean (±SEM) change in HbA1c
0
1
2
3
4
5
6
Placebo Testosterone
*
0
1
2
3
4
5
6
Placebo Testosterone
*
Hb
A1
c (
%)
Baseline
3 Months
n=24
A) Mean (±SEM) change in HOMA index

Testosterone therapy improves Testosterone therapy improves
erectile function in hypogonadal erectile function in hypogonadal
men with EDmen with ED11
0
10
20
30
Erectile Function Sexual Desire
Baseline (n=122) Week 12 (n=71)
IIE
F S
core
1. Yassin A et al. World J Urol 2006; 24:639-644.

Effects of testosterone therapyEffects of testosterone therapy
EndocrineEndocrine
Increases testosterone Increases testosterone
Decreases SHBGDecreases SHBG
PhysicalPhysical
Body mass/muscle strength/BMDBody mass/muscle strength/BMD
Sexual functionSexual function
Morning erections, libido, sexual functionMorning erections, libido, sexual function
MoodMood
Improved mood and cognitive functionImproved mood and cognitive function

Treatment optionsTreatment options

Testosterone gelTestosterone gel200200
Testosterone patchTestosterone patch199199
88
Testosterone patchTestosterone patch199199
55
Testosterone patchTestosterone patch199199
22
Oral testosteroneOral testosterone197197
77
ShortShort--acting acting
injectable injectable
testosteronetestosterone
195195
44
Testosterone implantTestosterone implant194194
00

Oral testosterone Oral testosterone
(Restandol(Restandol®®;;AndriolAndriol®®/Testocaps/TestocapsTMTM))1,21,2
Tablets containing 40mg testosterone Tablets containing 40mg testosterone
undecanoate as a maintenance dose taken undecanoate as a maintenance dose taken
22--3 times a day3 times a day
Route of absorption is via lymphatic Route of absorption is via lymphatic
systemsystem
Therefore needs to taken with a meal Therefore needs to taken with a meal
containing dietary fatcontaining dietary fat
Without dietary fat absorption is minimal, and Without dietary fat absorption is minimal, and
pharmacokinetics unreliablepharmacokinetics unreliable1. Nieschlag E et al. Human Reproduct Update 2004; 10 (5):409-419.2. Organon Laboratories Limited. Restandol® SPC; May 1998.

Buccal testosteroneBuccal testosterone1,21,2
(Striant(Striant®®))
30mg testosterone tablet placed above 30mg testosterone tablet placed above
incisor tooth twice dailyincisor tooth twice daily
Avoids hepatic inactivationAvoids hepatic inactivation
Absorbed across oral mucosaAbsorbed across oral mucosa
Good pharmacokinetics, achieving normal Good pharmacokinetics, achieving normal
testosterone levelstestosterone levels
May be application difficultiesMay be application difficulties
Risk of site reactionsRisk of site reactions1. Nieschlag E et al. Human Reproduct Update 2004; 10(5):409-419.
2. Ardana Bioscience. Striant® SPC; March 2005.
SubdermalSubdermal
(Testosterone implants)(Testosterone implants)
Testosterone pellets (100Testosterone pellets (100--600mg) 600mg)
implanted subdermallyimplanted subdermally22
Three to six pellets (600mg to 1.2g) usually Three to six pellets (600mg to 1.2g) usually
maintain plasma testosterone concentrations maintain plasma testosterone concentrations
for 4for 4--6 months6 months11
Risk of supraphysiological testosterone Risk of supraphysiological testosterone
levelslevels
Minor surgical procedureMinor surgical procedure
Can be painful/infection risk/scarringCan be painful/infection risk/scarring
8.5% extrusion of pellets8.5% extrusion of pellets33
1. Nieschlag E et al. Human Reproduct Update 2004; 10(5):409-419.
2. Organon Laboratories Limited. Testosterone Implant 200mg SPC; May 1999.3. Handelsman DJ et al. Clin Endocrinol 1997;47:311-316.

Transdermal patchesTransdermal patches1,21,2
(e.g. Andropatch(e.g. Andropatch®®))
2.52.5--7.5mg testosterone delivered, 7.5mg testosterone delivered,
starting dose starting dose
Daily circadian profile of testosterone Daily circadian profile of testosterone
deliverydelivery3,43,4
Alcohol base to enhance permeation Alcohol base to enhance permeation
Skin reactions common (>50% Skin reactions common (>50%
patients)patients)3,43,4
Size of patch can be obtrusiveSize of patch can be obtrusive
May make crinkling noiseMay make crinkling noise
1. Nieschlag E et al. Human Reproduct Update 2004; 10(5):409-419.
2. GlaxoSmithKline UK. Andropatch® 5mg SPC; August 2002.
3. Wang C et al. J Clin Endocrinol Metab 2000; 85(8):2839-2653.
4. Gooren LJG et al. Drugs 2004.64(17):1861-1891.

Transdermal gelsTransdermal gels1,2,31,2,3
(Testogel(Testogel®®; Testim; Testim®®))
5050--100 mg testosterone gel applied each 100 mg testosterone gel applied each
morning to shoulders, back, or abdomenmorning to shoulders, back, or abdomen
Daily circadian profile of testosterone Daily circadian profile of testosterone
deliverydelivery2,42,4
Skin reactions in 4Skin reactions in 4--10% patients10% patients2,32,3
Avoid washing for 6 hoursAvoid washing for 6 hours
Risk of transfer to another person via skin Risk of transfer to another person via skin
contactcontact
Daily patient compliance requiredDaily patient compliance required
1. Nieschlag E et al. Human Reproduct Update 2004; 10(5):409-419.
2. Schering Health Care Limited. Testogel ® 50mg SPC; February 2004.
3. Ipsen Ltd. Testim ® 50mg SPC; August 2004.4. Wang C et al. J Clin Endocrinol Metab 2000; 85(8):2839-2653.

Intramuscular injections Intramuscular injections -- short short
actingacting1,21,2
(Sustanon(Sustanon®® 100; Sustanon100; Sustanon®®
250; 250; TestovironTestoviron®®)) Currently the most widely used form of Currently the most widely used form of
testosteronetestosterone
Two shortTwo short--acting preparations widely available acting preparations widely available
in UKin UK
Sustanon 100 (testosterone: Sustanon 100 (testosterone:
propionate/propionate/phenylpropionatephenylpropionate/ isocaproate in / isocaproate in arachisarachis
oil)oil)
Sustanon 250 (testosterone: Sustanon 250 (testosterone:
propionate/propionate/phenylpropionatephenylpropionate/ isocaproate/decanoate / isocaproate/decanoate
in in arachisarachis oil)oil)
Injection every 2 weeks (Sustanon 100) or 3 Injection every 2 weeks (Sustanon 100) or 3
weeks (Sustanon 250)weeks (Sustanon 250)2,32,3
Peak and trough testosterone levelsPeak and trough testosterone levels
1 Nieschlag E et al. Human Reproduct Update 2004; 10(5):409-419.
2. Organon Laboratories Limited. Sustanon® 100 SPC; February 2004
3. Organon Laboratories Limited. Sustanon® 250 SPC; January 2006.

Intramuscular injections Intramuscular injections -- long long
actingacting11
(Nebido(Nebido®®)) 1000 mg testosterone undecanoate in 4 1000 mg testosterone undecanoate in 4
ml castor oil ml castor oil
Loading dose at 6 weeks, and then every Loading dose at 6 weeks, and then every
10 to 14 weeks10 to 14 weeks11
Testosterone levels maintained within the Testosterone levels maintained within the
physiological rangephysiological range22
Avoids frequent peaks and troughs in Avoids frequent peaks and troughs in
testosterone levels that may be seen with testosterone levels that may be seen with
shortshort--acting injectionsacting injections33
Increased patient convenience (quarterly Increased patient convenience (quarterly
1. Schering Health Care Limited. Nebido ® SPC; October 2004.
2.Von Eckardstein S et al. J Androl 2002;23(3):419-425.3.Schubert M et al. J Clin Endocrinol Metab 2004;89:5429-5434.

Testosterone therapyTestosterone therapy
Number of testosterone preparations Number of testosterone preparations
availableavailable
Differ by route of applicationDiffer by route of application
Patient choice and satisfaction importantPatient choice and satisfaction important
Patients should be provided with sufficient Patients should be provided with sufficient
information to enable them to make an information to enable them to make an
informed decision regarding suitable informed decision regarding suitable
therapytherapy

Pharmacokinetics of different Pharmacokinetics of different
testosterone preparationstestosterone preparations

Pharmacokinetics: daily Pharmacokinetics: daily
testosterone preparationstestosterone preparations11
1. Gooren LJG et al. Drugs 2004.64(17):1861-1891.
50
40
30
20
10
Note the different timescales on these graphs

Pharmacokinetics of UK available Pharmacokinetics of UK available
injectable testosterone injectable testosterone
preparations: Sustanon 250preparations: Sustanon 25011
1. Lane HA et al. Endocrine Abstracts 2006;11:P677.
0
10
20
30
40
1 2 3 4
Sustanon 250
Weeks

0
10
20
30
40
0 1 2 3 4 5 6 7 8 9 10 11 12Weeks
Se
rum
te
sto
ste
ron
e (
nm
ol/L
)
T undecanoate (1st injection)
T undecanoate (13th injection)
Pharmacokinetics of UK available Pharmacokinetics of UK available
injectable testosterone injectable testosterone
preparations: Nebidopreparations: Nebido11--33
1. Von Eckardstein S et al. J Androl 2002; 23(3):419-425.
2. Behre HM et al. Eur J Endocrinol 1999;140:414-419.
Data are from 2 separate
studies, i.e. not a
comparative trial
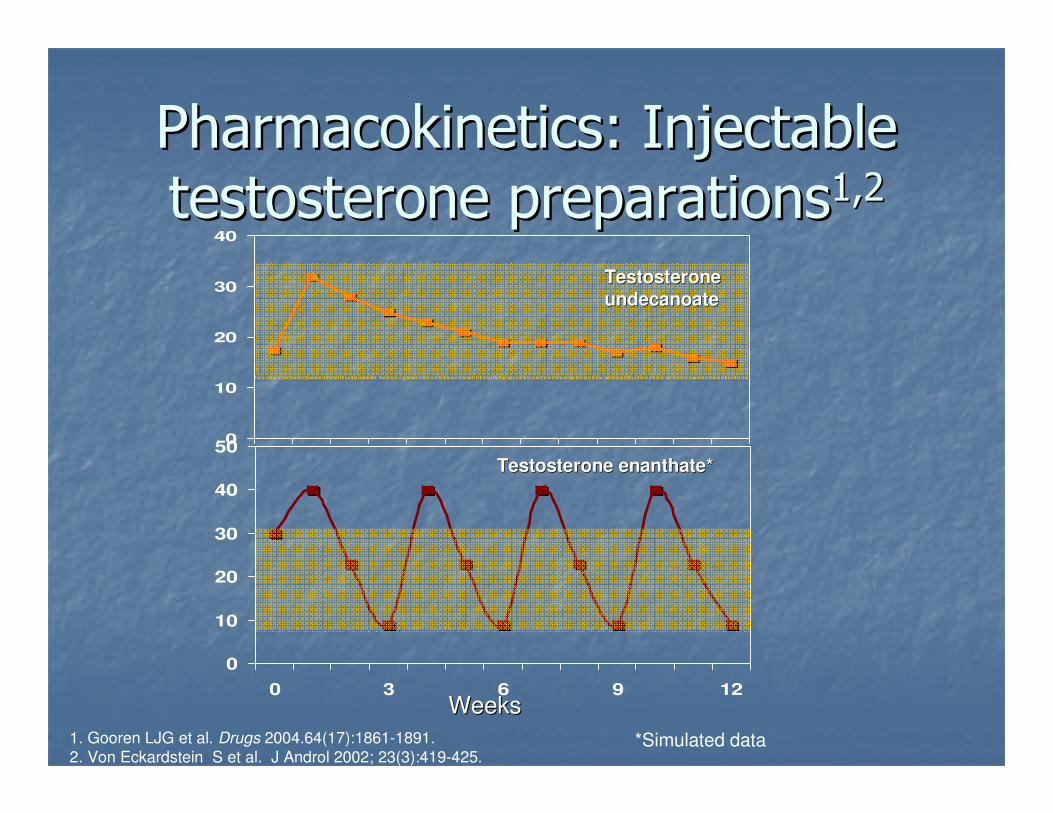
Pharmacokinetics: Injectable Pharmacokinetics: Injectable
testosterone preparationstestosterone preparations1,21,2
1. Gooren LJG et al. Drugs 2004.64(17):1861-1891.
2. Von Eckardstein S et al. J Androl 2002; 23(3):419-425.
0
10
20
30
40
50
0 3 6 9 12
0
10
20
30
40
WeeksWeeks
Testosterone Testosterone
undecanoateundecanoate
Testosterone enanthate*Testosterone enanthate*
*Simulated data

Pharmacokinetics: testosterone Pharmacokinetics: testosterone
implantsimplants
1. Jockenhovel F et al. Clin Endo 1996;45:61-71.

Monitoring patients on Monitoring patients on
testosterone therapytestosterone therapy
Areas of potential concernAreas of potential concern1,21,2
ProstateProstate
CardiovascularCardiovascular
Behavioural changesBehavioural changes
Personality changesPersonality changes
1. Nieschlag E et al. Eur Urol 2005;48:1-4.
2. Bhasin S et al. J Clin Endocrinol Metab 2006;91(6):1995-2010.

Parameters to monitor or to be Parameters to monitor or to be
aware of during therapyaware of during therapy1,21,2
ProstateProstate
Haematocrit and haemoglobinHaematocrit and haemoglobin
Increased levels particularly associated with Increased levels particularly associated with
supraphysiological levels of testosteronesupraphysiological levels of testosterone
Blood lipidsBlood lipids
Liver functionLiver function
Miscellaneous adverse effects of Miscellaneous adverse effects of
testosterone testosterone
E.g. gynaecomastia, acne, oily skin, priapism, E.g. gynaecomastia, acne, oily skin, priapism,
sleep apnoeasleep apnoea
1. Bhasin S et al. J Clin Endocrinol Metab 2006;91(6):1995-2010. 2. Nieschlag E et al. Human Reproduct Update 2004; 10(5):409-419.

Endocrine Society: Endocrine Society:
recommendationsrecommendations11
YY
--
YY
YY
YY
BaselineBaseline
--
YY
YY
YY
YY
3 month3 month
YYBMDBMD
YYTestosteronTestosteron
ee
YYHaematocritHaematocrit
YYDREDRE
YYPSAPSA
AnnualAnnualParametParamet
erer
1. Bhasin S et al. J Clin Endocrinol Metab 2006;91(6):1995-2010.

PSA levelsPSA levels
PSA = screening test for prostate cancerPSA = screening test for prostate cancer
PSA increases with agePSA increases with age
Increase in accepted PSA cutIncrease in accepted PSA cut--off with ageoff with age
4040--49 years 49 years 2.5 2.5 ngng/ml /ml
5050--59 years 59 years 3.5 3.5 ngng/ml /ml
6060--69 years 69 years 4.5 4.5 ngng/ml /ml
Over 70 years Over 70 years 6.5 6.5 ngng/ml /ml

Endocrine Society: Prostate Endocrine Society: Prostate
monitoringmonitoring11
Urological consultation should be sought if Urological consultation should be sought if
there is:there is:
Verified PSA >4.0 Verified PSA >4.0 ngng/ml/ml
Increase in PSA concentration >1.4ng/ml Increase in PSA concentration >1.4ng/ml
within any 12within any 12--month period of testosterone month period of testosterone
treatmenttreatment
PSA velocity >0.4ng/ml/year PSA velocity >0.4ng/ml/year
Detection of a prostatic abnormality on DREDetection of a prostatic abnormality on DRE
1. Bhasin S et al. J Clin Endocrinol Metab 2006;91(6):1995-2010.

0
5
10
15
20
25
0 12 30 0 12 30
Weeks
Prostate Volume (ml)
18.2417.16
14.29 14.51
19.8420.75
1. Huebler D et al. Endo 2000 Abstract Book: 567.
PSA and prostate volume during PSA and prostate volume during
testosterone treatmenttestosterone treatment
Weeks
PSA (µg/l)
0
0.25
0.5
0.75
1
-3 0 3 6 9 12 15 18 21 24 27 30
T enanthate T undecanoate
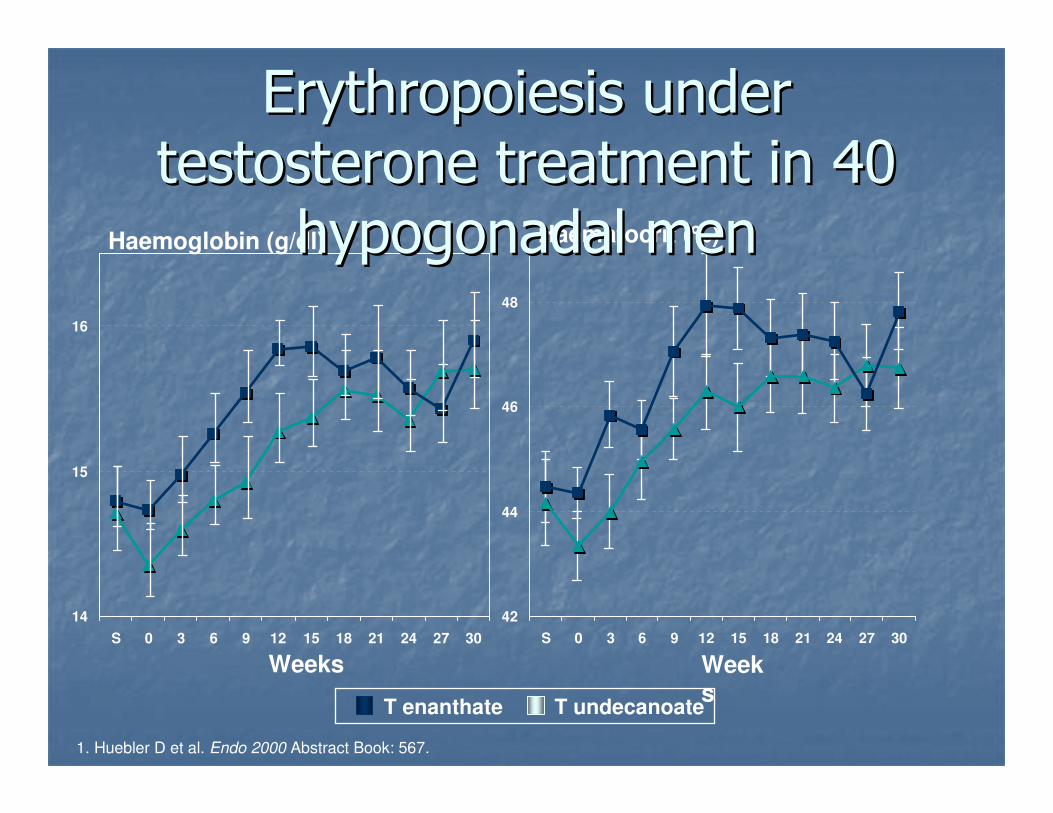
14
15
16
S 0 3 6 9 12 15 18 21 24 27 30
Haemoglobin (g/dl)
Weeks
Haematocrit (%)
Weeks
42
44
46
48
S 0 3 6 9 12 15 18 21 24 27 30
1. Huebler D et al. Endo 2000 Abstract Book: 567.
ErythropoiesisErythropoiesis under under
testosterone treatment in 40 testosterone treatment in 40
hypogonadal menhypogonadal men
T enanthate T undecanoate

Conclusion (1)Conclusion (1)
Testosterone influences sexual, Testosterone influences sexual,
metabolic and psychological functionsmetabolic and psychological functions
Male hypogonadism is inadequate Male hypogonadism is inadequate
functioning of the testes, characterised functioning of the testes, characterised
by abnormally low testosterone levelsby abnormally low testosterone levels
Male hypogonadism is associated with Male hypogonadism is associated with
increasing age, ED, type 2 diabetes and increasing age, ED, type 2 diabetes and
abdominal obesityabdominal obesity
Diagnosis of hypogonadism is based on Diagnosis of hypogonadism is based on
clinical features with biochemical clinical features with biochemical
confirmationconfirmation

Conclusion (2)Conclusion (2)
Testosterone therapy increases circulating Testosterone therapy increases circulating
testosterone levels with significant testosterone levels with significant
symptom improvementsymptom improvement
Treatment decision based on compliance, Treatment decision based on compliance,
convenience, choiceconvenience, choice
Monitor: prostate/haematocrit/clinical Monitor: prostate/haematocrit/clinical
responseresponse
Testosterone therapy provides significant Testosterone therapy provides significant
improvement in quality of life for patients improvement in quality of life for patients
with male hypogonadismwith male hypogonadism

NEBIDO PRESCRIBING INFORMATION 1Nebido (testosterone undecanoate)Presentation: Ampoule with 4ml solution for injection containing 1000mg testosterone undecanoate. Uses: Testosterone replacement therapy for male hypogonadism when testosterone deficiency confirmed by clinical features and biochemical tests.Dosage: One ampoule (1000mg) injected intramuscularly every 10 to 14 weeks. Starting treatment: Measure serum testosterone levels before start and during initiation of treatment. If appropriate, first injection interval may be reduced to a minimum of 6 weeks. Maintenance: Injection interval within 10 to 14 week range. Monitor serum testosterone regularly; adjust injection interval as appropriate.Children: Not for use in children. Not evaluated clinically in males under 18.Contra-indications: Androgen-dependent prostate cancer or breast cancer. Past or present liver tumours. Hypersensitivity to testosterone or any of the excipients.Warnings and precautions: Limited experience in patients over 65. Before therapy exclude prostate cancer. Examine prostate and breast at least annually, or twice yearly in elderly or at risk patients (clinical or familial factors). Periodically check testosterone concentrations, haemoglobin, haematocrit, liver function. Androgens may accelerate the progression of sub-clinical prostate cancer and benign prostatic hyperplasia. Monitor serum calcium concentrations in cancer patients at risk of hypercalcaemia (and hypercalcinuria). Rarely, liver tumours have been reported.Nebido may cause oedema with or without congestive cardiac failure in patients with severe cardiac, hepatic or renal insufficiency or ischaemic heart disease. In this case, stop treatment immediately. Use with caution in patients with renal or hepatic impairment, epilepsy, migraine or blood clotting irregularities. Improved insulin sensitivity may occur.Irritability, nervousness, weight gain, prolonged or frequent erections may indicate excessive androgen exposure requiring dose adjustment. Withdraw treatment if these symptoms persist or reappear. Pre-existing sleep apnoea may be potentiated.Testosterone may produce a positive reaction in anti-doping tests. Not for use in women. Not suitable for developing muscles or increasing fitness in healthy individuals. Inject Nebido extremely slowly to avoid the coughing or respiratory distress reactions that occur rarely with injection of oily solutions.Interactions reported with oral anticoagulants (requires dose monitoring), ACTH or corticosteroids, and thyroxin binding globulin in laboratory tests.

NEBIDO PRESCRIBING INFORMATION 2
Side-effects: Most common reactions are injection site pain (10%). Also reported are: diarrhoea; leg, breast or testicular pain; arthralgia; dizziness; increased sweating; headache; respiratory, skin or prostate disorders; acne; gynaecomastia; pruritus; subcutaneous haematoma at injection site. Other known reactions to testosterone containing preparations are: polycythaemia (erythrocytosis); weight
gain; electrolyte changes; muscle cramps; nervousness, hostility, depression; sleep apnoea; very rarely jaundice and liver function test abnormalities; skin reactions; libido changes; increased frequency of erections; interruption or reduction in spermatogenesis; priapism; prostate abnormalities; prostate cancer (inconclusive data); urinary obstruction; water retention; oedema; hypersensitivity. Basic NHS Price: £76.70 per 1 x 4mlLegal Classification: POMProduct Licence Number: 0053/0350Product Licence Holder: Schering Health Care Ltd.,
The Brow,Burgess Hill,West Sussex RH15 9NE
Nebido is a registered trademark of Bayer Schering Pharma AG (formerly Schering AG)PI revised: 28 June 2007
Information about adverse reaction reporting in the UK can be found at www.yellowcard.gov.uk. Alternatively, adverse reactions can be reported to Bayer plc by email: [email protected]

TESTOGEL PRESCRIBING INFORMATION 1
Testogel (testosterone)Presentation: Sachet containing 50mg testosterone in 5g colourless gel.Uses: Testosterone replacement therapy for male hypogonadism when testosterone deficiency confirmed by clinical features and biochemical tests.Dosage: One 5g gel sachet daily. Can be adjusted in 2.5g gel steps, to a maximum of 10g gel daily. Once sachet opened, apply immediately onto clean, dry healthy skin over both shoulders, or both arms or abdomen. Do not apply to genital areas.Children: Not for use in children. Not evaluated clinically in males under 18.Contra-indications: Known or suspected prostate or breast cancer. Hypersensitivity to testosterone or any constituents of the gel.Warnings and precautions: Before therapy exclude prostate cancer. Examine prostate and breast at least annually, or twice yearly in elderly or at risk patients (clinical or familial factors). Monitor serum calcium concentrations in cancer patients at risk of hypercalcaemia (and hypercalcinuria).Testogel may cause oedema with or without congestive cardiac failure in patients with severe cardiac, hepatic or renal insufficiency. In this case, stop treatment immediately. Use with caution in patients with ischaemic heart disease, hypertension, epilepsy and migraine. Periodically check testosterone concentrations, haemoglobin, haematocrit, liver function (tests), lipid profile.Possible increased risk of sleep apnoea especially if obesity or chronic respiratory disease present. Improved insulin sensitivity may occur.Irritability, nervousness, weight gain, prolonged or frequent erections may indicate excessive androgen exposure requiring dose adjustment.If severe application site reactions occur, discontinue if necessary. Testosterone may produce a positive reaction in anti-doping tests. Not for use in women.Testosterone gel can be transferred to others by close skin to skin contact and can lead to adverse effects (inadvertent androgenisation) if repeated contact. Inform patient of transfer risk that is prevented by clothing or washing of application site. Testogel should not be prescribed for patients who may not comply with safety instructions (e.g. alcoholics, drug abusers, psychiatric patients). Pregnant women must avoid any contact with the application sites. Interactions reported with oral anticoagulants, ACTH or corticosteroids, and thyroxin binding globulin in laboratory tests.

TESTOGEL PRESCRIBING INFORMATION 2Side-effects: Most common (10%) were: skin reactions. Also reported were: changes in
laboratory tests (polycythaemia, lipids), headache, prostatic disorders, gynaecomastia, mastodynia, dizziness, paraesthesia, amnesia, hyperaesthesia, mood disorders, hypertension, diarrhoea, alopecia, urticaria. Other known reactions to testosterone treatments are: muscle cramps; nervousness; depression; hostility; sleep apnoea; skin reactions; libido changes; more frequent erections; hypersensitivity reactions; rarely: jaundice, liver function tests, priapism, prostate
abnormalities, prostate cancer (inconclusive), urinary obstruction. During high dose and/or prolonged treatment: weight gain, electrolyte changes, reversible interruption or reduction of spermatogenesis, water retention, oedema, rarely hepatic neoplasms. Frequent applications may cause irritation and dry skin.
Basic NHS Price: £33.00 per pack of 30 x 5g sachetsLegal Classification: POMProduct Licence Number: 16468/0005Product Licence Holder: Laboratoires BESINS INTERNATIONAL5, rue du Bourg L’Abbé75003 ParisFranceDistributed by: Schering Health Care Ltd.,
The Brow,Burgess Hill,
West Sussex RH15 9NETestogel is a registered trademark of Laboratoires BESINS INTERNATIONALPI revised: 4 July 2007
Information about adverse reaction reporting in the UK Information about adverse reaction reporting in the UK
can be found at can be found at www.yellowcard.gov.ukwww.yellowcard.gov.uk. Alternatively, . Alternatively,
adverse reactions can be reported to Bayer plcadverse reactions can be reported to Bayer plc by by
email:email: [email protected]@bayer.co.uk