malnutrition jsna
TRANSCRIPT
1
Malnutrition JSNA September 2016
Overview
Malnutrition (or undernutrition) is a serious global public health problem that is significantly under-
recognised and under-treated1 with associated healthcare costs in the UK exceeding £13 billion annually2.
In the UK, one in three patients admitted to acute care and 35% of those admitted to care homes will be
malnourished or at risk, however 93% of those who are malnourished live in the community3.
There is a lack of local data of the prevalence of malnutrition in Kingston. However, based on national
prevalence of malnutrition it can be assumed that approximately 3,053 older people (>65 years) are
malnourished in Kingston.
In addition to the financial burden of malnutrition, there are numerous adverse outcomes on quality of life
for individuals and their carers. Malnutrition can lead to reduced immune function, decreased physiological
functions, delayed wound healing, increased vulnerability to disease, and prolonged recovery from disease
and injury4. As a result, people who are malnourished have an increased dependence on both primary and
secondary care. For example, people who are malnourished make 65% more GP visits, account for 82%
more hospital admissions and stay in hospital 30% longer when compared with people who are well
nourished5. In addition, malnutrition negatively affects quality of life for both individuals and their carers and
so it is important to both prevent malnutrition and treat it in its early stages.
There can be many contributing factors for malnutrition at an individual level and it can be both a cause and
consequence of ill health. Although specific illnesses or disease processes may play a role, for example
through reducing appetite/intakes, increasing requirements or decreasing the body’s ability to absorb
nutrients, there are other factors including social and psychological influences which may cause or
exacerbate malnutrition. Examples of these include dementia, depression, anxiety, poor access to
transport, poor mobility, poor dentition, taking medication, poverty, social isolation, inadequate care and
substance misuse6.
Various groups of the population can be malnourished or ‘at-risk’ of malnutrition. The focus of this chapter
will be on the over 65’s who are particularly vulnerable to malnutrition, with the UK having an estimated
10% over 65s being malnourished or at risk of malnutrition.
References 1 World Health Organisation (European Food and Nutrition Action Plan 2015-2020). 2 Brotherton, A. and Simmonds, N. on behalf of the BAPEN Quality Group. Malnutrition Matters Meeting Quality Standards in Nutritional Care. Redditch, Worcs. British Association for Parenteral and Enteral Nutrition (BAPEN). 2010. 3 NHS England Guidance – Commissioning Excellent Nutrition and Hydration 2015-2018. 4 NICE Nutrition support in adults: oral nutrition support, enteral tube feeding and parenteral nutrition Costing report Implementing NICE guidance in England. NICE Clinical Guideline no. 32: February 2006. 5 British Dietetic Association (BDA) Key Fact sheet. Dietitian Key Facts Malnutrition 2014. 6 The Malnutrition Taskforce. Malnutrition in Later Life: Prevention and Early Intervention Best Practice Principles & Implementation Guide. A Local Community Approach. London. Malnutrition Malnutrition Taskforce (2013) Malnutrition in Later Life: Prevention and Early Intervention Best Practice Principles and Implementation Guide A Local Community Approach.

2
Introduction
Malnutrition is defined as a state in which a deficiency or imbalance of energy, protein,
vitamins or minerals causes measurable adverse effects on body composition, function or
clinical outcome1. The word ‘malnutrition’ applies to both over and undernutrition, however in
the context of this chapter, malnutrition will be used to refer to undernutrition.
Malnutrition negatively impacts a person’s quality of life and life expectancy and is estimated
to cost the NHS £13 billion pounds annually to treat2, with total public health and social care
costs in England of £19.6 billion3. This equates to approximately 15% of the total
expenditure on health and social care, although most is attributable to healthcare.
Approximately three million people in the UK are affected by malnutrition at any given time,
the majority (93%) of whom live in the community (including those who live at home or in
sheltered accommodation). A further 5% are living in care homes and just 2% are in
hospital4. Despite the hospital setting accounting for a small proportion of those who are
malnourished, the volume of patient’s means that hospitals remain a vital point of care at
which malnutrition can be identified and treatment initiated5.
Age
Eating disorders (including anorexia, bulimia nervosa and binge eating disorder) are a range
of conditions that are characterised by an abnormal attitude towards food and cause
someone to change their eating habits and behaviours. Malnutrition may be related to eating
disorders which often involve severe restriction or purging of nutrients. This can result in
poor health and social outcomes, such as reduced fertility and a negative impact on
relationships. The prevalence of eating disorders is difficult to determine due to their
complex nature and inconsistencies in their diagnosis. However it has been estimated that
between 608,000 and 725,000 people in the UK are suffering with an eating disorder6.
The number of hospital admissions across the UK for teenagers with eating disorders has
nearly doubled in the last three years, according to the NHS. They increased from 959 in 13
to 19-year-olds in 2010/11 to 1,815 in 2013/147. Although the numbers are relatively small,
experts say the rate of increase (89%) is mirrored by a larger number of cases that don't go
to hospital7. The Royal College of Psychiatrists attributes much of the increase to social
pressure made worse by online images.
The risk of malnutrition is more commonly associated with those aged 65 or over; one in ten
people over 65 are malnourished or at-risk of malnutrition5.
The causes of malnutrition in the elderly are multifactorial and there are numerous clinical
consequences for this age group. In older adults, changes to digestive capacity, taste, basal
metabolic rate, and feelings of hunger, satiety and thirst can all increase the risk of nutritional
compromise. Age-related chronic neurodegenerative diseases such as dementia,
Parkinson’s disease and strokes can have a particularly significant impact on nutritional
status8.
The Office for National Statistics predicts that the number of adults in the UK aged over 65 is
expected to increase by 50% in the next 20 years to over 16 million9. Therefore more, older

3
people will be affected by malnutrition. The risk of malnutrition increases with age and those
aged over 75 are at highest risk. Furthermore, 14% of older people in sheltered homes are
at high risk of malnutrition10. Other groups at risk include children born prematurely, those
living in deprived circumstances and those suffering from chronic disease with an impact on
nutrition e.g. intestinal disease, cancer and those with eating disorders.
Common risk factors for malnutrition are described in further detail in Table 1. Some of these
are not related to disease and may be preventable.
Risk factors in Table 1 may be more commonly associated with adults however the list also
applies to younger age groups and children who may suffer from specific problems as
outlined above.
Table1: Factors associated with Malnutrition
Medical Factors Lifestyle/Social
Factors
Other Risk
Factors
Risk Factors in
Hospital/Care Homes
Reduced appetite
due to illness/
underlying medical
condition
Dysphagia
(Swallowing
problems due to
poor dentition/loss of
teeth)
Nausea and vomiting
Infections Other
diseases e.g.
Cancer,
Neurological,
Intestinal,
Respiratory or
Endocrine Disease
Ageing process lead to
declining taste
Limited mobility/high
risk of falls due to
reduced bone
synthesis
Poverty
Social isolation
Poor access to shops
Lack of cooking skills
Limited access to
facilities/equipment to
cook
Religious dietary
restriction
Limited mobility or a
lack of knowledge
making it difficult to go
shopping or cook food
at home or go out to
meet other people
further exacerbates
social isolation leading
to malnutrition
Recent discharge from
hospital
Misconception that its
normal to become
thinner as you get older
Lack of
awareness
amongst staff
of identifying
and treating
malnutrition
effectively
Lack of
nutrition
training for
medical staff
so it’s
perceived as
less important
Depression
Recent
bereavement
Dementia
Anxiety
Confusion
Quality assurance of
catering food provision
for patients-how food is
presented, limited food
choices on menu
Missing teeth/poor oral
hygiene
Unable to reach food,
use cutlery, open
packages especially if
they have suffered from
Stroke and are confused
Unpleasant sights, smell
and sounds
Increased nutrient
requirements due to
infection, wound healing
Not taking account of
religious/cultural dietary
needs
Nil by mouth or missing
meals whilst having
tests, altered taste due to
radiotherapy or
chemotherapy
Limited mobility with
hands and feet following
surgery, may require
assistance with feeding
Source: Table modified from: Hickson, M. (2006). Malnutrition and Ageing. Postgraduate Medical Journal. 82,
p.2-8.

4
In addition to these general risk factors for malnutrition, there are some specific conditions
and social factors which carry a significant nutritional burden. Some of these are outlined
below:
Cancer
Patients presenting with cancer can have significant nutritional problems which arise from
not only the disease process but also, the anatomical locality of the cancer and its
treatments. Weight loss is common amongst people with cancer and weight loss or
malnutrition affects up to 85% of cancer patients at some point6,11. Symptoms at
presentation can include weight loss, dysphagia, early satiety, loss of appetite, nausea and
vomiting, all of which can impact negatively on nutritional status. In addition, being
overweight or obese is a risk factor for oesophageal cancer and this may mask the problem
of weight loss in such patients; therefore careful nutritional assessment is important.
Malnutrition is associated with poorer treatment and patient-centred outcomes, however
adequate nutrition can help people with cancer to maintain their weight, maximise outcomes
and improve quality of life7,9,12,13.
Dementia
Patients with dementia are particularly at risk of malnutrition. As dementia progresses,
patients with dementia often experience increased difficulty with eating and drinking, and this
can result in weight loss and poor health outcomes12. The majority of people with dementia
live in the community, with around a third estimated to live in a care home9,13. Studies
reviewed in the report Nutrition and Dementia have shown that up to 45 percent of those
living with dementia experience clinically significant weight loss over one year, and up to half
of people with dementia in care homes have an inadequate food intake10,14. Therefore it is
important to consider nutritional care and support in the community to support the nutritional
status of people with dementia.
Depression
Mental health conditions such as depression and anxiety can contribute to malnutrition11,15.
Depression could act as a powerful risk factor for malnutrition in older people and is the most
common mental health problem in people in Kingston12,16.
Living alone, social isolation and housing
Malnutrition is common in those who may be socially isolated living alone with no support or
limited mobility13,17. Social isolation has been defined as an individual lacking a sense of
belonging, social engagement and quality relationships with others18. Although social
isolation is difficult to measure directly, as the proportion of older people living in the borough
increases, more residents are at risk of becoming socially isolated. Older adults who are
socially isolated also have an increased nutritional risk15,19.
According to POPPI estimates, in 2015 the total population aged over 75 predicted to be
living alone is 5,305. This number is predicted to increase by 53% by 2030 to 2128.
5
Food Poverty
Research evidence shows that malnutrition is common in people from lower socio-economic
groups. Food poverty is associated with a poor diet and is a risk factor for major diseases. It
is estimated that as many as 10 million people in the UK live in poverty, including nearly
three million children16,20. Low income households tend to consume fewer nutrients and
fewer fresh fruit and vegetables than average-income households17,21 and the Fabian
commission on food and poverty suggests that in the UK, household food insecurity arises
from the cost of living rising faster than income 18,22. Due to a lack of official measurement, it
is unclear how many people are affected by household food insecurity in the UK however
there has been an increase in the number of hospital admissions for malnutrition. Data
collected in 2013 show primary and secondary diagnoses of malnutrition (caused by lack of
food or very poor diet) rose from 3,161 in 2008/09 to 5,499 in 2012/1319,23 suggesting
societal factors may be playing a role in increasing malnutrition.
Child poverty is expected to rise to 3.9 million by 2015. A survey carried out by save the
children, ‘Child Poverty in 2012 it shouldn’t happen here’20,24, shows that poverty in the UK
can result in parents cutting back on food so their children don’t go hungry. In 2012, nearly
12% of all dependent children under 20 in Kingston were in relative poverty (living in
households where income is less than 60% of median household income before housing
cost).
Causes and Risk Factors
The causes of malnutrition can be broadly categorised into three groups, however in reality,
the cause is often multi-factorial. Some examples of the causes of malnutrition are outlined
below:
Reduced nutritional intake (e.g. due to low food availability of food, loss of appetite,
problems with eating and drinking, poor access to food (social exclusion, poor
transport, difficulties shopping), poverty, cognitive decline, poor mental wellbeing,
depression, anxiety)
Reduced nutrient absorption (may be caused by disease processes e.g. Crohns,
complications from drug therapy)
Increased requirements (e.g. acute illness/infection, surgery, disease processes e.g.
cancer pr Parkinson’s disease, medical intervention e.g. drains).
In the UK, the most common causes of malnutrition amongst children are medical conditions
such as cystic fibrosis and cerebal palsy that impact nutrient absorption, reduce appetite,
and cause an increase in energy needs21,25. Amongst young children, malnutrition as a result
of inadequate food intake is rare in the UK, although malnutrition may occur if a child is
neglected, living in poverty or being abused. Children might also become malnourished
because they avoid eating due to issues with their body image or have an eating
disorder26,27.

6
For older people or those in care homes or hospitals, who have difficulties with eating and
drinking, inadequate care relating to nutrition and hydration may exacerbate malnutrition.
Common occurrences include8.
A lack of support with feeding
Food left out of reach
Nutritional supplements not given frequently.
There are numerous adverse outcomes of malnutrition on quality of life for both individuals
and their carers. There is a summary of some of the clinical consequences of malnutrition.
Further detail of the clinical effects of malnutrition can be found in Table 2 of Malnutrition
Matters Meeting Quality Standards in Nutritional Care (2010)
The clinical consequences of malnutrition include1,28:
Impaired immune response (and increased vulnerability to disease)
Reduced muscle strength
Impaired wound healing
Prolonged recovery from disease or injury
Loss of temperature regulation
Impaired psychosocial function
Specific nutrient deficiencies
Impaired ability to regulate body electrolytes salt and fluid.
Malnourished individuals, compared to well nourished, individuals have an increased
dependence on both primary and secondary care, including:
Greater healthcare needs in the community (e.g. more care at home, antibiotics)8
More intensive care needs amongst those in nursing home settings
65% more GP visits costing the NHS £1,449 per patient per year29
Increased prescription costs2
Increased (82% more) admissions and re-admissions to hospital8
Increased medical complications (e.g. infections)8
Increased length of stay (30% longer) at hospital8
Increased morbidity30
Increased risk of death30,31
Managing malnutrition
Since malnutrition increases a person’s vulnerability to ill-health, adequate nutrition support
should improve outcomes although in reality the situation is more complex, as are decisions
on the most effective and safe means of providing nutritional support which should
be individually tailored to a person’s needs.
However there is some evidence that improving nutrition, with support from a dietitian, can
help to12:
Prevent health problems
Improve functional status32
Increase quality of life and wellbeing for people living with long-term conditions (such
as such as cancer, chronic obstructive pulmonary disease (COPD) and dementia)
Provide cost savings to the NHS2.
7
Regular screening for nutritional risk with validated screening tools, such as the Malnutrition
Universal Screening Tool (MUST), is recommended by various key groups including the
National Institute for Health and Care Excellence (NICE)1, and the national patient safety
agency; however various care settings are failing to screen patients as recommended5. This
delays the initiation of appropriate care and nutritional support for vulnerable patients and
may lead to further deterioration of those who are already malnourished5.
Malnutrition in those aged 65 and over
Malnutrition is largely a preventable and treatable condition and there is good evidence that
nutritional support in older people can decrease weight loss, improve functional outcomes
(e.g. muscle strength, walking distance, activity levels and mental health) and also improve
clinical outcomes in both community and hospital settings33. In addition, for those people
living in care homes, there is some evidence that appropriate nutritional screening and
support can:
Reduce in hospital admissions
Reduce length of hospital stay (with associated cost savings)12.
Similarly, nutritional support for patients with conditions such as cancer can support
treatment, reduce treatment complications, reduce the length of time in hospital and improve
quality of life.
Managing malnutrition in the community and in care settings could also provide significant
financial benefits. NICE identifies malnutrition as the sixth largest potential source for NHS
savings34 and early identification and treatment of malnutrition in adults could save the NHS
£13 million a year after costs of training and screening1. NICE have also demonstrated that
screening, early intervention and treatment could save £71,800 per 100,000 people35 and
appropriate use of oral nutritional supplements (ONS) has been found to save £849 per
patient based on length of stay in hospital36.
Health and social care organisations in the community are well placed to manage the burden
of cost related to malnutrition37,38. One strategy to achieve this involves enabling older
people to remain in their own home or sheltered accommodation. This includes staff from
health and social care raising self-awareness amongst older people of malnutrition and
hydration.
BAPEN have produced the malnutrition universal screening tool (MUST) to identify and
manage malnutrition in both the acute and community settings. The NICE (2006) CG32
guideline has shown that this will contribute to significant cost savings. The benefits for
investing in prevention and treatment of malnutrition outweigh the cost leading to significant
cost saving opportunities.
The Malnutrition Task force has produced a fact sheet which outlines further costs and
impact of malnutrition.
Evidence highlights the appropriate use of oral nutritional supplements (ONS) is associated
with a reduction of overall hospital readmissions related to malnutrition by 30%.
8
Key Drivers for Improvements to Malnutrition
Malnutrition is recognised as a key public health issue and more work is required to address
it. This includes meeting evidence-based recommendations highlighted in the key policy
guideline documents listed below:
NICE 2006 guidelines. Refreshing the National Public Health outcome framework
2015-2016 domain 4d for improving patient’s experience with hospital food
BAPEN Malnutrition Matters meeting quality care standards in nutritional care
Malnutrition Taskforce to address malnutrition in the community
Managing Adult Malnutrition in the Community pathway
Care Quality Commission (CQC) standards for nutrition
NHS England Commissioning guidance for excellent nutrition and hydration
BAPEN report on cost savings from nutritional interventions
Fabian Policy Report – Hungry for Change
Visit Managing Adult Malnutrition in the Community for more information.
References for Introduction 1 NICE. Nutrition Support for Adults: Oral Nutrition Support, Enteral Tube feeding and Parenteral Nutrition.
Methods, Evidence and Guidance. National Collaborating Centre for Acute Care, London. February 2006 2 Elia, M. The cost of malnutrition in England and potential cost savings from nutritional interventions (full
report). Southampton: Biomedical Research Centre. 2015. 3 BAPEN. Introduction to Malnutrition. 4 Elia M.and Russell C.A. BAPEN. Combating Malnutrition: Recommendations For Action Output of a meeting of
the Advisory Group on Malnutrition 12 June 2008 5 Beating Eating Disorders (BEAT) The Costs of Eating Disorders. Social, Health and Economic Impacts. BEAT
[Internet] 2015 6 Brotherton, A. and Simmonds, N. on behalf of the BAPEN Quality Group. Malnutrition Matters Meeting Quality
Standards in Nutritional Care. Redditch, Worcs. British Association for Parenteral and Enteral Nutrition (BAPEN).
2010. 7 Beating Eating Disorders (BEAT) (2015) Rising Eating Disorder Hospital Admissions – What the Figures Mean. 8 The Malnutrition Taskforce. Malnutrition in Later Life: Prevention and Early Intervention Best Practice Principles
& Implementation Guide. A Local Community Approach. London. Malnutrition Malnutrition Taskforce (2013)
Malnutrition in Later Life: Prevention and Early Intervention Best Practice Principles & Implementation Guide A
Local Community Approach. 9 Age UK. Later Life in the United Kingdom. February 2016. 10 Elia, M. And Russell, C.A. Screening for Malnutrition in Sheltered Housing. (BAPEN). 2009. 11 The British Dietetic Association The Value of Nutritional Care in Helping the NHS to Deliver on the NHS
Outcomes Framework: An assessment of how delivering high quality nutritional care can enhance the quality of
life for people with long-term conditions. 12 Sauer, A.C. and Coble Voss, A. Abbott Nutrition Institute. ‘White Paper: Improving Outcomes with Nutrition in
Patients with Cancer,’ 2012 13 Baldwin, C., Spiro, A., Ahern, R. And Emery, P.W. A Systematic Review and Meta-Analysis Journal of the
National Cancer Institute. Oral Nutritional Interventions in Malnourished Patients with Cancer. 2012
9
14 Alzheimer’s Disease International 2014. Nutrition and Dementia London. Alzheimer’s Disease International. 15 Vfaei, Z., Mokhtari, H., et al. Journal Research Medical Science. Malnutrition is associated with depression in
rural elderly population. 2013. 18; S15-S19. 16 NHS Kingston CCG. Dementia Strategy for Kingston upon Thames 2015-2020. 17 McHugh, J., Lee, O., Aspell, N.L., Brian, A. & Brennan, S. Medline JMIR Research Protocols. A shared
mealtime approach to improving social and nutritional functioning among older adults living alone: study protocol
for a randomized controlled trial. 2015. 4; pg 43. 18 Dury, R. (2014). Social isolation and loneliness in the elderly: An exploration of some of the issues. British
Journal of Community Nursing, 19(3), 125-128. 19 Locher, J. L., Ritchie, C. S., Roth, D. L., Baker, P. S., Bodner, E. V., & Allman, R. M. (2005). Social isolation,
support, and capital and nutritional risk in an older sample: Ethnic and gender differences. Social Science and
Medicine, 60, 747–761. 20 Faculty of Public Health (2015). 21 Public Health England. (2008/2009-2011/12). National Diet and Nutrition Survey: Results from years (-4)
(combined) of the rolling programme (2008/2009-2011/12). Executive Summary. 22 Tait C. On behalf of the FABIAN Society. The final report of the Fabian Commission on Food and Poverty:
Hungry for Change. Online October 2015 23 Parliament website. Publications and Records. 24 Whitman G. On behalf of Save the Children. Child Poverty in 2012: It shouldn’t happen here. Online 2012. 25 NHS Choices Website. Malnutrition Causes. 26 Campbell, K. And Peebles, R. Eating Disorders in Children and Adolescents: State of the Art
Review. American Academy of Paediatrics. 2014. 134; 582. 27 Sahib, A. And Radhi, El. Appropriate care for children with eating disorders and obesity. British Journal of
Nursing. 24; 518-522. 28 Managing Adult Malnutrition in the Community (2012). Including a pathway for the appropriate use of Oral
Nutrition Supplements (2012). Produced by Multi Professional Consensus Panel. 29 The Malnutrition Taskforce. A review and summary of the impact of malnutrition in older people and the
reported costs and benefits of interventions. May 2013. 30 Stratton, R.J., King, C.L., Stroud, M.A et al (2006). Malnutrition Universal Screening Tool predicts mortality and
length of hospital stay in acutely ill elderly. British Journal of Nutrition. 95, pg 325-330. 31 Charlton, K.E., Batterham, M.J., Bowden, S. et al A high prevalence of malnutrition in acute geriatric patients
predicts adverse clinical outcomes and mortality within 12 months. E-Spen Journal. 2013. 8. (3): e120-e125. 32 Cawood, AL. et al Systematic review and Meta-analysis of the effects of high protein and oral nutritional
supplements. Ageing Research Review. 2012; 11 278-296. 33 Gandy, J. (eds). Manual of Dietetic Practice. 5th ed. Oxford. British Dietetic Association 2014. 34 Malnutrition Taskforce. Addressing Malnutrition: Commissioners Mini-Guide. 35 NICE support for commissioners and others using the quality standard on nutrition support in adults November
2012. 36 Elia, M. et al, The cost of disease related malnutrition in the in the UK and economic considerations for the use
of oral nutritional supplements (ONS) in adults, BAPEN, 2005 37 Rebecca, M. (2014). Community Management of Nutrition and Hydration Community Nutrition. Vol 6, p. 11. 38 Carers UK the Voice of UK. Malnutrition and Caring. The hidden cost for families. Nutricia Advanced Medical
Nutrition. 2012.

10
Local Picture
There is a lack of local data of the prevalence of malnutrition in Kingston. However, based
on national prevalence of malnutrition (Table 2), it can be assumed that approximately 3,053
older people (>65 years) are malnourished in Kingston.
The main points are summarised below, for the local data that is available. These are
grouped together into different topics and include accommodation, costs, mental health, life
expectancy, poverty, dementia, cancer and social isolation.
Royal Borough of Kingston (RBK) Sheltered Housing: Malnutrition is common
amongst older tenants in sheltered housing. In Kingston there are 843 sheltered
homes which suggests between 82 and 115 people aged 55+ living in sheltered
homes are at risk of malnutrition (based on national prevalence predicted by
BAPEN). See Table 2
Total Population aged 65 and over requiring Care at Home: Malnutrition is higher
in care settings such as care homes, hospital inpatients and those receiving care at
home. This is influenced by the increased likelihood of patients in these settings
being more accurately monitored and malnutrition recorded more often. The number
of malnourished people in Kingston receiving care at home is 183
Total Population aged 65 and over living in a care home with or without
nursing care: The longer a person is able to remain independent in their own home,
the less likelihood of them becoming malnourished, relying on care homes and
hospitals. The total population aged 65 and over living in a care home, with or without
nursing care is estimated to increase from 776 to 1200 between 2015-2030; an
estimated increase of 54% by 2030 according to POPPI.
Potential Cost for Over 65 year olds admitted to hospital: Following diagnosis of
malnutrition, the incremental six monthly costs to the NHS attributable to malnutrition
was estimated to be £1,003 per patient1. In addition, severely malnourished patients
identified in general practice incur additional health care costs of £1,449 per patient
in the year following diagnosis (mainly incurred through additional GP consultations
and hospital visits37). Put into a local context, with an estimated 3,053 adults over 65
years of age malnourished in Kingston from 2014, this equates to malnutrition-related
healthcare costs of £3,062,159 over six months
Mental health units all admissions: Nationally, it’s estimated there is 19%
prevalence of malnutrition in mental health unit admissions2. In Kingston over 21,000
adults are estimated to have a common mental health disorder (CMD). These figures
could indicate that approximately 20% of this cohort could possibly be at risk of
malnutrition.
Life Expectancy: From 2011-13, life expectancy at 65 years was 19.4 years for
males living in Kingston and 21.7 years for females; above the England averages
11
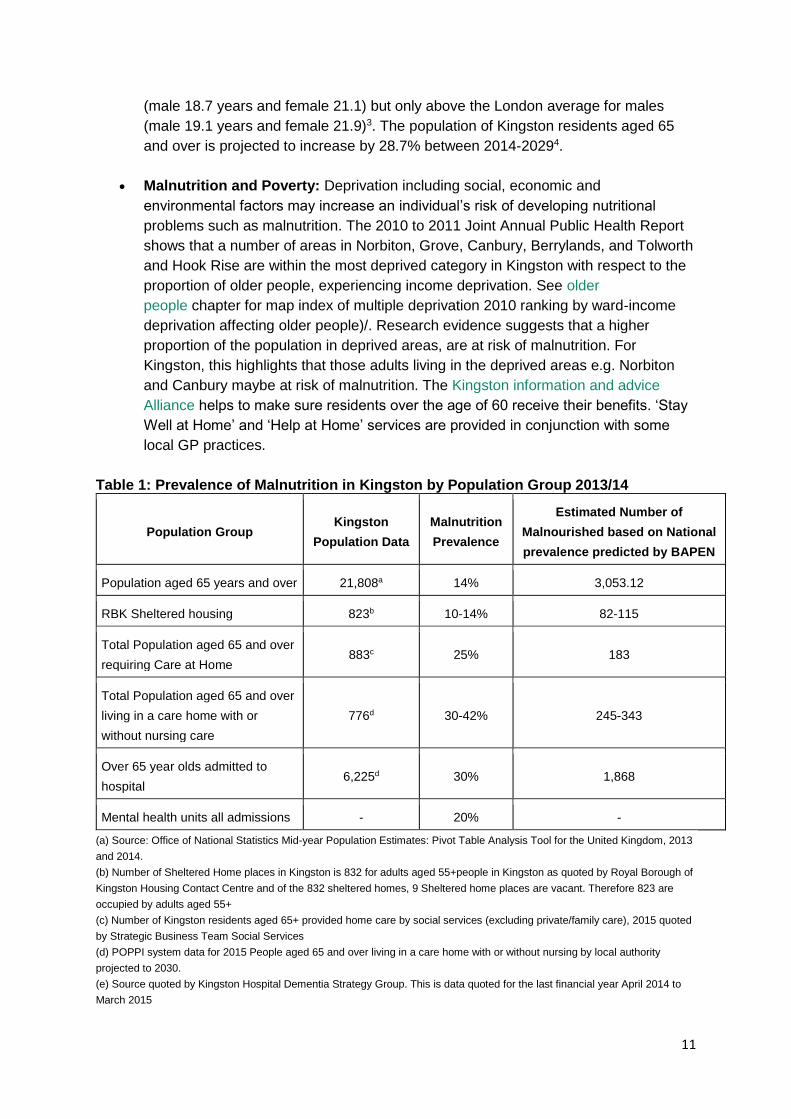
(male 18.7 years and female 21.1) but only above the London average for males
(male 19.1 years and female 21.9)3. The population of Kingston residents aged 65
and over is projected to increase by 28.7% between 2014-20294.
Malnutrition and Poverty: Deprivation including social, economic and
environmental factors may increase an individual’s risk of developing nutritional
problems such as malnutrition. The 2010 to 2011 Joint Annual Public Health Report
shows that a number of areas in Norbiton, Grove, Canbury, Berrylands, and Tolworth
and Hook Rise are within the most deprived category in Kingston with respect to the
proportion of older people, experiencing income deprivation. See older
people chapter for map index of multiple deprivation 2010 ranking by ward-income
deprivation affecting older people)/. Research evidence suggests that a higher
proportion of the population in deprived areas, are at risk of malnutrition. For
Kingston, this highlights that those adults living in the deprived areas e.g. Norbiton
and Canbury maybe at risk of malnutrition. The Kingston information and advice
Alliance helps to make sure residents over the age of 60 receive their benefits. ‘Stay
Well at Home’ and ‘Help at Home’ services are provided in conjunction with some
local GP practices.
Table 1: Prevalence of Malnutrition in Kingston by Population Group 2013/14
Population Group Kingston
Population Data
Malnutrition
Prevalence
Estimated Number of
Malnourished based on National
prevalence predicted by BAPEN
Population aged 65 years and over 21,808a 14% 3,053.12
RBK Sheltered housing 823b 10-14% 82-115
Total Population aged 65 and over
requiring Care at Home 883c 25% 183
Total Population aged 65 and over
living in a care home with or
without nursing care
776d 30-42% 245-343
Over 65 year olds admitted to
hospital 6,225d 30% 1,868
Mental health units all admissions - 20% -
(a) Source: Office of National Statistics Mid-year Population Estimates: Pivot Table Analysis Tool for the United Kingdom, 2013
and 2014.
(b) Number of Sheltered Home places in Kingston is 832 for adults aged 55+people in Kingston as quoted by Royal Borough of
Kingston Housing Contact Centre and of the 832 sheltered homes, 9 Sheltered home places are vacant. Therefore 823 are
occupied by adults aged 55+
(c) Number of Kingston residents aged 65+ provided home care by social services (excluding private/family care), 2015 quoted
by Strategic Business Team Social Services
(d) POPPI system data for 2015 People aged 65 and over living in a care home with or without nursing by local authority
projected to 2030.
(e) Source quoted by Kingston Hospital Dementia Strategy Group. This is data quoted for the last financial year April 2014 to
March 2015

12
Dementia
In Kingston is it estimated that there are between 1,417 residents over the age of 65 who
have dementia, which equates to 7.28% of the local population over 655. This figure is
projected to rise to 1,594 although this will be a decrease in value as the older population
rises (6.78% of population over 65) by 2021.
Currently, there are more people registered with Kingston GPs (under the responsibility of
Kingston Clinical Commissioning Group) than live in the borough, and for this group the
estimated number of people with dementia in 2015 was between 1,5536 and 1,8747. The
number of people with dementia who are looked after by Kingston GPs is higher because
people from outside Kingston borough are registered with Kingston GPs and this number is
also rising. Furthermore, there are currently 1000 people on the dementia register locally.
In Kingston hospital 48% of inpatients above the age of 75 have confirmed or suspected
diagnosis of Dementia, a cohort of which is more likely to be at risk of malnutrition. As
quoted by the Kingston Hospital Dementia Strategy group from April 2014 to March 2015,
14089 admissions to Kingston hospital were with patients aged over 75. Fifty percent of
these patients suffer Dementia (7,405 adults) and 45% (3332 adults aged over 75) will also
be at risk of malnutrition.
Cancer:
The incidence of Cancer in Kingston is similar to the rest of England (381.9 per 100,000
people)8.Patients presenting with cancer can have significant nutritional problems which
arise from not only the disease process but also, the anatomical locality of the cancer and its
treatments. Weight loss is common amongst people with cancer and weight loss or
malnutrition affects up to 85% of cancer patients at some point9. Malnutrition is associated
with poorer treatment and patient-centred outcomes, however adequate nutrition can help
people with cancer to maintain their weight, maximise outcomes and improve quality of life10,
11.
Living alone, social isolation and housing
Almost 36.4% of Kingston residents aged 65 and over are predicted to be living alone in
Kingston (8,425 people), including 22.9% of those aged 75+ (5,305). Over two–thirds
(67.6%) of those living alone are female. This is projected to rise by 44.9% to 12,208 by
2030. Older people living alone at home may require support from social, housing and
voluntary services. There are a range of health risks associated with living alone; a study by
Kharicha et al12 found in their study that those living alone were more likely to report fair or
poor health, and poor diet was one of the key themes of the study.
Living alone can increase social isolation and impact wellbeing for older people, as housing
under occupancy can impact financial standing and mood, which may also have an effect on
food intake and nutrition.
The majority of older people in Kingston live in homes that are owned by them instead of
social housing.
3.3% of those over 65 (776 residents) are estimated to be living in a care home in
Kingston13. Care home residents have a unique, complex mix of health-care needs.
Dementia, stroke, degenerative neurological conditions, advanced cardio-respiratory

13
disease, cancer and painful arthritis are common conditions, and ones that are often
accompanied by loss of appetite or difficulty with eating and drinking14.
References for Local Picture
1 The Malnutrition Taskforce. A review and summary of the impact of malnutrition in older people and the
reported costs and benefits of interventions. May 2013.
2 Bapen. Nutrition Screening Survey in the UK and Republic of Ireland in 2011.
3 Office of National Statistics, 2015.
4 2014 Round of Demographic Projections- trend based population projections, short term migration scenario,
2015. © GLA 2015 Round Demographic Projections
5 Local Dementia UK statistics (England).
6 Calculation based on target number for Kingston CCG from NHS England, and based on CFASII
7 Calculation based on Alzheimer’s Society Research 2007 which estimates 0.0095% of total population has
dementia
8 Cancer Research UK. Local Cancer Statistics.
9 The British Dietetic Association The Value of Nutritional Care in Helping the NHS to Deliver on the NHS
Outcomes Framework: An assessment of how delivering high quality nutritional care can enhance the quality of
life for people with long-term conditions. October 2013
10 Sauer, A.C. and Coble Voss, A. Abbott Nutrition Institute. ‘White Paper: Improving Outcomes with Nutrition in
Patients with Cancer,’ 2012
11 Baldwin, C., Spiro, A., Ahern, R. And Emery, P.W. A Systematic Review and Meta-Analysis Journal of the
National Cancer Institute. Oral Nutritional Interventions in Malnourished Patients with Cancer. 2012
12 Karicha et al (2007). Health risks appraisal in older people 1: are older people living alone san ‘at risk’ group?
British Journal of General Practice. 57 (537), 271-276.
13 Apetito Value of Meals on Wheels Service 2013. Meeting the Wider Funding Challenge The Real Value of
Meals on Wheels.
14 British Geriatrics Society (2011) Quest for quality an inquiry into the quality of healthcare support for older
people in care homes: a call for leadership, partnership and improvement.

14
What Works
There are numerous guidelines around the treatment and prevention of malnutrition such
as NICE CG32 and The Malnutrition Task force.
These suggest that malnutrition in older people can be prevented by:
Maintaining independence
Reducing social isolation
Ensuring access to food and services
Tackling poverty
Improving quality of life
Holistic multi-disciplinary approach
Raising awareness and training frontline staff.
Improved nutritional care has been identified as having a large potential cost saving to the
NHS. NICE has recognised malnutrition as the sixth largest source for potential NHS
savings.
Preventing malnutrition should be an integral part of preventative health care and located
within the public health agenda. The malnutrition task force offers 5 best practice principles
for tackling malnutrition in the community and care settings1, which are in line with NICE
clinical guidelines. Recommendations from both are summarised below.
Raising awareness among front line staff to support prevention and early treatment of
malnutrition through better education for staff and individuals
Organisations should prioritise malnutrition as part of their care plans and should
include staff training of the importance of adequate nutrition and hydration as well as
coordinated care from a multidisciplinary team.
Multidisciplinary team (MDT): e.g. in and across care homes and hospitals
A joined up multi-disciplinary approach (MDT) ensures there is good communication
between patients and professionals
Setting up a steering committee to oversee and manage malnutrition in both acute
and community settings should be represented by an MDT
MDT including commissioners and providers from health and social care with a
universal attitude is required to tackle and prevent malnutrition.
Identifying malnutrition in the individual using validated screening tools such as the
MUST (Malnutrition Universal Screening Tool) and identifying prevalence within
organisations and the community
Early screening is cost effective compared to treating malnutrition once established
at both national and local level
15
Regular screening and monitoring should take place at GP visits, routine health
checks, vaccinations, routine weights, on admission to care homes, and whenever
there is clinical concern.
Developing personalised and dignified plans of care, treatment, support and
monitoring
In the first instance, it is recommended to treat the underlying condition that may cause
malnutrition. Management options include:
Support with feeding
Addressing social issues
Ensuring ability to shop (physical and financial) and prepare food
Texture modification, dietary advice to maximise nutritional intake (also known as
food first).
Oral and Artificial Nutrition Support (following screening, oral nutrition support
measures such as):
First line approach is dietary advice to optimise oral intake
Food fortification
Snacks
Sip feeds
Artificial feeding depends on clinical judgement such as when nutritional
requirements are less likely to be completely met via oral nutrition support.
Evaluating the impact of the care and support on a patient’s weight, improvements
and outcomes.
Monitoring both the individual (their food intake and weight) as well as the processes
in place to address malnutrition.
Social Interventions
Taking a whole person holistic approach (addressing several of the causes of malnutrition) is
important to managing malnutrition. There are several areas that could be addressed at both
an individual and community level. Examples of these include:
Encouraging eating together in care homes/creating positive dining experience

16
Encouraging increased food intake
Tackling lack of access to food
Tackling difficulties in cooking
Reducing isolation
Preventing ill health
Reducing poverty
Reducing depression
Supporting independence.
Supporting older people to maintain independence is one way to prevent malnutrition.
Community projects can offer improved access to food and additional social value. For
example, The Food Train Dumfries programme in Scotland enables older people to access a
healthy acceptable diet and to remain independent at home whilst reducing social isolation,
thereby tackling other risk factors for malnutrition.
Meals on Wheels Services also encourage people to remain independent and stay in their
own home2. They can aid people with eating regularly, encourage personal contact and
being regularly monitored to ensure care needs are met and their nutrition risk does not
increase.
Care Plans
Local and national guidelines including government bodies listed below summarise the
approaches and recommendations that should be implemented to prevent or treat
malnutrition.
1. BAPEN (2010) Malnutrition Matters Quality Care Standards
2. NICE (2006) guidelines (CG32) on Nutrition Support in Adults Oral Nutrition Support
Enteral Tube Feeding & Parenteral Nutrition
3. The Malnutrition Task Force (2013): A review and summary of the impact of malnutrition
in older people and the reported costs and benefits of interventions
4. Managing Adult Malnutrition in the Community (includes a pathway for the appropriate
use of oral nutritional supplements (ONS))
5. The Malnutrition Task Force (2013). Prevention and Early Intervention of Malnutrition in
Later Life consists of the best practice principles and implementation guide to use for a
local community approach
6. NICE Quality Standard 24 (2012). Meeting Quality Standards For Nutrition Support in
Adults
7. Meeting Nutritional Needs-Essential Outcomes Care Quality Commission (2010)
8. Care Quality Commission Report: Time to Listen Dignity & Nutrition in NHS Hospitals
Inspection Programme (2012)
9. Care Quality Commission Report: Time to Listen Dignity
10. NICE guidance (2006) is guidance document for the care of patients with or at risk of
malnutrition.

17
References from What Works
1 The Malnutrition Taskforce. Malnutrition in Later Life: Prevention and Early Intervention Best Practice Principles
& Implementation Guide. A Local Community Approach. London. Malnutrition Malnutrition Taskforce (2013)
Malnutrition in Later Life: Prevention and Early Intervention Best Practice Principles & Implementation Guide A
Local Community Approach.
2 Apetito Value of Meals on Wheels Service 2013. Meeting the Wider Funding Challenge. The Real Value of
Meals on Wheels.

18
Current Services
The Royal Borough of Kingston and local stakeholders have supported the development of a
new Healthy Weight and Physical Activity Needs Assessment and Strategy 2013-2016. The
action plan outlines key recommendations and objectives. This is for partners to meet
current and future needs, providing a framework to deliver key strategic targets:
Reducing the overall prevalence of obesity in children and adults reversing the tide)
Minimising the current increase in obesity prevalence from Reception Year to Year 6
Ensuring all professionals (both health professionals and non-health professionals)
can access relevant training and support the implementation of clear pathways to
follow for adults and children in Kingston
Ensuring robust surveillance data is available to inform service planning and
commissioning.
Older people with poor mobility are likely to find it difficult to access services to help them
with maintaining adequate nutrition and hydration, therefore older people with limited mobility
may be more vulnerable to malnutrition. This is identified in the strategy as a key barrier for
accessing services. Language could also be a barrier but it is thought that many services are
making good progress at incorporating Kingston Interpreting Service support when
necessary. This includes using local community members to translate and incorporate
English lessons within the service content. Further work is required to see if this need is
already met or, if more support is necessary.
Hospital Screening
To tackle malnutrition, all inpatients at Kingston Hospital are assessed for malnutrition using
the MUST tool. Patients identified at high risk are referred to the ward dietitian and assessed
on an individual basis. Appropriate nutritional intervention is then initiated and monitored. At
discharge, a letter outlining nutrition recommendations with details of any nutritional
supplements is sent to the patient’s GP. The GP will assess the patient and prescribe
nutrition support if appropriate; however this post-discharge care is not standardised across
the borough and is likely to vary from GP to GP.
Community Dietetics
There is no commissioned dietetic domiciliary service in the community or nursing homes
unless the patient is enterally fed (when a patient is fed via a tube into the gastro-intestinal
tract). Patients can be seen by the primary care dietitian however this service is limited to
one clinic a month per surgery. In order to access this service, patients need to be mobile
enough to attend the clinic which may leave vulnerable patients without an accessible
service. Patients can either be referred directly by the GP or as a hospital referral to be

19
actioned post discharge. Hospital in-patients are often not mobile enough post discharge to
attend a service, therefore may not be adequately monitored for nutritional outcomes. Local
commissioners should therefore investigate and consider the size of this gap in service.
Stay Well At Home (Kingston service)
The Stay Well at Home Service includes volunteers supporting recently discharged patients
from hospital in their home. Volunteers visit the clients’ home over a number of weeks
making sure the client has shopping. And that fresh food is available at home.
This service looks for different ways the client can get regular and varied food. This includes:
Most days a week, clients using Wiltshire Farm foods
Twice a week, eating at Raleigh House
Once a week, going to a local pub or cafe.
Dining Companion’s Project (Kingston service)
The Dining Companions scheme started in 2012 offering older patients with practical care,
support and companionship at mealtimes. They recruited 387 Dining Companion Volunteers
including public volunteers, non-clinical staff and community groups. This frees up nursing
staff time to focus on patients with more complex feeding requirements.
Dining Companion scheme encourage older patients to eat well and independently at their
highest level of functioning. The scheme has reached 301 volunteers (two volunteers per
mealtime on each ward, seven days a week). More than 50 members of non-clinical
Kingston Hospital Foundation Trust staff since 2012 have been trained as Dining
Companions.
Although these services are specifically focusing on malnutrition, the following services
target families that could potentially be at risk of malnutrition.
Healthy Start Project
Healthy Start is a national programme that targets teenage and low income pregnant
women, and young families. The scheme includes food vouchers and vitamin tablets for
pregnant women. Healthy Start is embedded into midwifery service delivery and is regularly
discussed at strategic meetings that feed into the Health and Wellbeing Board (via the
Residents Health Care Services Committee). This includes the Maternal Obesity Action
Group, the Infant Feeding Partnership, and the Maternity Services Liaison Committee.
Cook and Eat Programmes in Children Centres
Most of the children centres in Kingston upon Thames run Cook and Eat programmes for
families with children aged zero to five to address fussy eating and support families to cook
healthy meals for their children.

20
Eating disorders in Young People
Increasing access to Psychological Therapies (IAPT) welcome referrals for mild to moderate
eating, that does not, require a specialist service. Referrals can be made in a variety of
ways, including self-referral or referral via the GP, community mental health team or other
health professionals. In severe cases, or where more specialist input is required, referrals
must be made to the South West London and St George’s Eating Disorder Service. Kingston
Hospital Dietetics team will routinely review any patients with a diagnosed eating disorder
who is admitted to the hospital. There is currently no specialist eating disorder service at
Kingston Hospital; however patients can be referred for specialist support. On discharge,
patients are referred back into community services where applicable.
Cook and Eat Programmes for adults
Cook and Eat programmes for adults aim to promote a healthy diet and healthy weight by
providing participants with the confidence and skills to cook and consume a healthier diet.
They are provided at a variety of local community settings. Programmes are not targeted at
individuals suffering from malnutrition, but can form part of the prevention agenda,
empowering participants to confidently cook and eat healthily. Examples of cook and eat
programmes relevant to malnutrition include:
Cook and Eat for adults who are homeless, recovering from drug or alcohol addiction
at Joel Night Shelter Accommodation
Cook and Eat for adults delivered in 2013 accessing Food Bank. Food banks are
charities that provide a minimum of three days emergency food and support to
people experiencing crisis in the UK
Cook and Eat for adults recovering from poor mental health.
The five Cook and Eat programmes in Kingston in 2014-15 have reached a total of 94
people. Participants on all of the programmes have reported improvements in a range of
dietary behaviours and knowledge including improved understanding of food labels and
ingredients.
21
Community Voice
The consequences of malnutrition can impact a patient’s ability to access care, for instance
attending a GP appointment. In addition, malnutrition can have significant social
consequences for the affected individual and their family. Carers UK, a national charity,
highlight that1:
60% of carers worry about the nutrition of the person they care for
One in six carers are looking after someone at real risk of malnutrition but do not
have nutritional support of any kind
55% of carers look after older people on nutritional supplements
16% of the adults that carers care for are underweight with a small appetite.
There has been no consultation specifically about malnutrition with older people locally in
Kingston. It’s recommended that this work takes place, to find out about local services,
perceived need and any other relevant contributions. National evidence from the Malnutrition
Taskforce UK where there has been consultation in 2013 with older people has found:
Engagement with older people on the issue of malnutrition requires avoiding the term
‘malnutrition’ as it’s perceived negatively and is viewed as a sign of poverty and
neglect
The word ‘malnutrition’ should be avoided when communicating with public and
instead terms such as undernourished or underweight should be used instead
Language is important to establishing accurate community voice
Older people prefer positive messages about the effects of malnutrition such as
“Eating and drinking enough is important to maintain your health and independence”
For identifying malnutrition they prefer messages such as “They have lost weight,
they look thin or they have a poor appetite”
Older people felt it is really important to dispel the myth that unintentional weight loss
is a normal part of ageing
It will also be vital to establish reasons behind malnutrition.
A survey carried out by ICM on behalf of Age UK; ‘Cut Backs Survey (2009) in Later
Life’2 showed:
22
22% (3 million people) of people aged 60+ in UK (2009) skipped meals to cut back
on food costs
42% (5.8 million people) of people aged 60+ in UK (2009) agreed they struggle to
afford essential items e.g. food, gas, electricity
Findings from the Review of Kingston Sheltered Housing Report highlighted that even those
that have had recent improvements to housing, often fail basic mobility requirements, such
as lifts to upper floors. This may limit older peoples’ ability to go out this has potential to
further increase social isolation and limit access to nutrition as people may find it difficult to
get out into their local community.
References for Community Voice
1 Carers UK (2012). Malnutrition and Caring. The Hidden Cost For Families. Trowbridge. Nutricia.
2 Age UK. Later Life in the United Kingdom. February 2016.
23
Recommendations
Recommendations for local mapping
Improve surveillance to ensure a clearer picture of local need is available.
Surveillance and analysis of malnutrition should identify any gaps in services for
malnutrition which can then be addressed through the action plan. A Malnutrition
needs assessment has been agreed to take place for residents in Kingston upon
Thames
Map the use of the MUST tool for screening or other identification tools used in care
settings in the borough
Review the actions taken as a result of malnutrition screening to establish pathways
of care currently in place and determine if key guidelines and CQC standards are met
Collection of local prevalence data on malnutrition (e.g. BMI and/or MUST score at
various points of care) in community and hospital/care settings
Identify if older people settings have their own local nutrition treatment care plans in
place and if they are adhering to these nutrition care plans
Ensure local strategy for healthy weight includes malnutrition and fits with national
policy
Complete a full Malnutrition needs assessment consulting local stakeholders and
patient including mapping current services available relating to malnutrition across
the life course.
Recommendations for planning of service provision
Review dietetic capacity within GP practices to assess if the current level of one clinic
per month per practice is enough to meet the needs of Kingston patients
Use dietetic expertise to review the use of oral nutritional supplementation (ONS) in
Kingston including tackling gaps between prescriptions and ensuring compliance with
protocols. The financial benefits of having a community dietitian have been explored
by the London Procurement Programme, which reported that appropriate ONS
prescriptions could save 15% on ONS expenditure over 2 years
Explore wider determinants of malnutrition such as housing to identify local need

24
Improve accessibility of services. This may include geographical location of services
but also linking with other services, including adult social care and also influencing
planning processes and transport links
Recommendations for service provision/commissioners
Develop a Community follow up protocol upon discharge of patients identified as
malnourished in hospitals in Kingston
Considering commissioning a community Dietitian for domiciliary dietetic visits for
malnourished patients in the community with the aim of reduce patients coming into
hospital as malnourished. Currently there is a service gap for community/nursing
home patients who are malnourished but unable to attend a dietetic appointment at
the GP surgery
Support the dietetic business case for oncology dietitian to increase capacity for
nutritional support for patients with caner
Encourage routine use of the MUST tool screening of individuals in care settings in
the community to identify malnutrition e.g. upon registration with GP, home visit on
admission to care home or hospital. Other screening opportunities include contact
with community pharmacist or District Nurse. Sheltered homes to identify and
manage malnutrition
Ensure Health and social care includes malnutrition in all care pathways for an older
person’s care. Ensuring good communication so older people receive oral nutritional
supplements appropriately and there are no gaps between prescriptions
Identify nutrition training needs amongst front line staff across health, social and
voluntary sector involved with older peoples care in relation to malnutrition
Support care homes in meeting CQC standards with appropriate training as required
Review the need to provide wider prevention programmes such as targeted Cook
and Eat courses
Review if all providers of meals within lunch clubs and day centres for older people
are now adhering to the nutrition standards set for older people.

25
Glossary:
NICE: National Institute for Health and Care Excellence
BAPEN: British Association for Parenteral Enteral Nutrition
GLA: Greater London Authority; The Greater London Authority (GLA) was established by the
GLA Act 1999. GLA staff is appointed by the Head of Paid Service, the GLA’s most senior
official, and serve both the Mayor and the London Assembly.
HLE: Healthy life expectancy (HLE); also called disability adjusted life expectancy,
represents the average number of years that a person can expect to live in full health. This
measure of full health is based on contemporary mortality rates and the prevalence of self-
reported good health. The prevalence of good health is derived from responses to a survey
question on general health.
Multidisciplinary Team (MDT): is a group of health care workers who are members of
different disciplines (professions e.g. Psychiatrists, Social Workers, etc.), each providing
specific services to the patient
MUST: Malnutrition Universal Screening Tool; The ‘MUST’ is a five-step screening tool to
identify adults, who are malnourished, at risk of malnutrition (undernutrition), or obese. It also
includes management guidelines which can be used to develop a care plan.
ONS: Oral Nutritional Supplements
CQC: Care Quality Commission; The CQC are the independent regulator of health and
social care in England. The CQC monitor, inspect and regulate services to make sure they
meet fundamental standards of quality and safety.
Dementia: Dementia is a syndrome resulting from a change in brain tissue causing a loss of
intellectual function and is characterised by a progressive decline in memory, reasoning,
communication skills and gradual loss of skills required for carrying out everyday activities1
(Thomas, B. Manual of Dietetic Practice. British Dietetic Association. 3rd edn. pg
566.Oxford: Blackwell Science Publishing; 2001). Individuals may also develop behavioural
and psychological symptoms such as depression, psychosis, aggression and wandering.
26
Other Needs Assessments
Healthy Weight and Physical Activity Needs Assessment and Strategy 2013-2016
Useful Links
BAPEN Malnutrition Self-Screening Tool
British Dietetic Association Food Facts
NHS Choices Malnutrition Pages: Treatment
NHS Choices Dehydration
NICE: Diet Nutrition and Obesity
Help and Information
NHS Choices: Malnutrition pages for information on malnutrition; overview, causes
and treatment
Malnutrition Taskforce Website
Malnutrition Taskforce: List of Key references on malnutrition