mantle cell lymphoma: a clinicopathologic study of 80 cases
TRANSCRIPT

Mantle Cell Lymphoma: A Clinicopathologic Study of 80 Cases
By Larry H. Argatoff, Joseph M. Connors, Richard J. Klasa, Douglas E. Horsman, and Randy D. Gascoyne
Mantle cell lymphoma (MCL) is a relatively uncommon yet zone (6%); the OS among these groups was identical. In-creased mitotic activity (Û20 mitotic figures per 10 highdistinct type of malignant lymphoma whose clinical and
pathological characterization has been limited by the small power fields), blastic transformation, and peripheral bloodinvolvement at diagnosis also predicted for a worse out-numbers of cases published to date. We studied 80 cases of
MCL seen at a single institution over 7 years to determine come, but bone marrow involvement did not. The presenceor absence of a translocation t(11;14) by cytogenetic analysisboth clinical and pathological prognostic factors. The pa-
tients in this study were predominantly male (70%) and older or a bcl-1 rearrangement by Southern analysis did not sig-nificantly predict outcome. In summary, this study of 80(mean age, 63 years) and presented with advanced-stage
disease (88%). Extranodal involvement was common. Me- cases of MCL highlights its distinctive clinicopathologic fea-tures and shows that increased mitotic activity, blastic mor-dian overall survival (OS) was 43 months. Except for perfor-
mance status, prognosis was not significantly influenced by phology, and peripheral blood involvement at diagnosis areprognostically important factors.clinical prognostic factors. Histologically, MCL architecture
was classified as diffuse (78%), nodular (16%), or mantle q 1997 by The American Society of Hematology.
ogy,4-6,13,14 peripheral blood (PB) involvement,8,14,15,17,18 andM increased mitotic activity8,11,14 connote a poor prognosis, al-ANTLE CELL LYMPHOMA (MCL) is a relativelyuncommon type of malignant lymphoma (ML) ac-
though the numbers of cases in each study were small. Thecounting for approximately 5% of ML in North America andobjective of this study was to examine these and other rele-Europe. MCL possesses unique morphological, immunophe-vant clinicopathologic variables in a population-based cohortnotypic, cytogenetic, and molecular genetic features, someof patients with MCL, diagnosed and treated at the Britishof which have been elucidated only recently. Based on im-Columbia Cancer Agency (BCCA). Its aim was not to un-munophenotypic and histochemical data, MCL is a neoplasmcover novel diagnostic features of MCL, but to illustrate thecomposed of cells resembling those residing in follicularclinical and pathological findings of MCL in British Colum-mantle zones. In the past, MCL has been referred to bybia and to provide further insight into the factors that mayvarious names including intermediately differentiatedhave prognostic significance in this disease.lymphocytic lymphoma, centrocytic lymphoma, and mantle
zone lymphoma (MZL). Cytogenetic and molecular evidenceMATERIALS AND METHODSthat emerged in the past decade has made it apparent that
intermediately differentiated lymphocytic lymphoma, cen- Patientstrocytic lymphoma, and MZL denote a common entity, now Eighty cases diagnosed as MCL between 1988 and 1995 werereferred to as MCL.1,2
obtained from the pathology files of the BCCA, the main cancerMorphologically, MCL can be recognized as a distinct referral center for the province of British Columbia, which has a
type of ML by its monotonous, diffuse, and/or nodular prolif- population of approximately 3.6 million people. All cases were re-viewed by two pathologists to ensure that each case had an adequateeration of small- to medium-sized cells with slightly irregulartissue biopsy specimen procured before the initiation of treatmentnuclei, inconspicuous nucleoli, and absence of both largeand that the biopsy material met the accepted morphological criteriatransformed (noncleaved) cells and proliferation centers. Im-for MCL.1,2,19 Examination of the biopsy material was undertakenmunophenotypically, MCL coexpresses pan-B–cell antigenswithout knowledge of any individual patient’s outcome. Cases inand CD5, a pan-T–cell antigen. A recurring cytogeneticwhich treatment was initiated based solely on bone marrow (BM)
abnormality, t(11;14), occurs in MCL, resulting in rearrange- and/or PB findings were excluded (n Å 29) . Detailed clinical infor-ment of the bcl-1 gene locus and overexpression of the cyclin mation including stage, treatment, and follow-up was available forD1 (CCND1/PRAD1) gene.3 This genetic event is thought to each of these 80 cases.have an important role in the pathogenesis of MCL, becauseoverexpression of cyclin D1 protein is thought to lead to Morphologyderegulation of the normal cell cycle, particularly at the G1- Tissue biopsy specimens were fixed in buffered formalin or B5S-phase transition. Despite refinements in the diagnostic cri- fixative, routinely processed, sectioned at 3 mm, and stained withteria, clinical classification of MCL into existing schemeshas been problematic. In the past, most cases of MCL wereclassified in the Working Formulation as diffuse small From the Departments of Pathology and Medical Oncology, Brit-cleaved-cell lymphoma, with a minority classified as small ish Columbia Cancer Agency, University of British Columbia, Van-lymphocytic, follicular small cleaved-cell, or lymphoblastic couver, British Columbia, Canada.
Submitted July 10, 1996; accepted October 28, 1996.lymphoma. These difficulties in classification, as well as theAddress reprint requests to Randy D. Gascoyne, MD, Departmentlack of large numbers of cases of MCL for study, have
of Pathology, British Columbia Cancer Agency, 600 W 10th Ave,hindered the understanding of its clinical behavior.Vancouver, British Columbia, V5Z 4E6, Canada.Clinically, MCL is considered by most investigators as an
The publication costs of this article were defrayed in part by pageML of intermediate grade, with a median overall survival
charge payment. This article must therefore be hereby marked(OS) of 2 to 5 years.4-12 Some studies suggest that specific ‘‘advertisement’’ in accordance with 18 U.S.C. section 1734 solely tomorphological subsets of MCL, particularly those with a indicate this fact.mantle zone (MZ) pattern, behave in a more indolent man- q 1997 by The American Society of Hematology.
0006-4971/97/8906-0008$3.00/0ner.13-16 Others have suggested that blastic cell morphol-
2067Blood, Vol 89, No 6 (March 15), 1997: pp 2067-2078
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

ARGATOFF ET AL2068
Table 1. Clinical Characteristics of 80 Patients With MCLhematoxylin and eosin. BM biopsy specimens were fixed in B5,decalcified with 10% nitric acid, processed, and sectioned in the
Characteristic No. of Patients (%)usual manner. BM and PB smears were stained with a Wright-
Age at presentationGiemsa stain. Immunoperoxidase staining was performed according°60 yr 29 (36)to well-established protocols.ú60 yr 51 (64)
SexImmunophenotypingMale 56 (70)
For immunophenotyping, cell suspensions of tissue and mononu- Female 24 (30)clear cell suspensions of PB and BM specimens were prepared ac- Primary site of involvement at presentationcording to well-established methods. A direct antibody-labeling tech- Lymph node 60 (75)nique was employed using mouse monoclonal antibodies CD2, CD3, Extranodal 20 (25)CD4, CD5, CD7, CD8, CD10, CD11c, CD14, CD19, CD20, CD23, Waldeyer’s ring 5 (6)and CD45 (Becton Dickinson, San Jose, CA); goat polyclonal anti- Intestine 4 (5)k and anti-l (Tago Inc, Burlingame, CA); and FMC-7 (Silenus Labo- Orbit 2 (3)ratories) labeled with either phycoerythrin or fluorescein isothiocya- Salivary gland 2 (3)nate. Specimens were analyzed on the Coulter Epics Profile II flow Stomach 2 (3)cytometer (Coulter, Hialeah, FL). Breast 1 (1)
Epidural 1 (1)Liver 1 (1)Genetic AnalysisPleura 1 (1)Cytogenetic analyses were performed according to establishedSpleen 1 (1)protocols. Southern analysis (SA) to detect bcl-1 gene rearrange-
Ann Arbor stagements was performed in a manner similar to previously describedI 5 (6)methods.20 In summary, high molecular weight DNA was extractedII 6 (6)from fresh or frozen material, digested with EcoRI, BamHI, andIII 11 (14)HindIII restriction endonucleases, electrophoresed on 0.7% agaroseIV 57 (71)gels, and transferred onto nylon filters. A 2.1-kb Sst I fragmentNot staged* 1 (1)representing the major translocation cluster on chromosome 11q13
B symptomswas used as the probe (courtesy of Dr A. Bakhshi, Bethesda, MD).Present 19 (24)Absent 61 (76)
Statistics Serum LDH levelNormal 34 (43)OS time was defined as the time from diagnosis to the time of
death from any cause. Patients still alive were censored at the last Elevated 22 (27)Unknown 24 (30)known date of contact. Actuarial survival times were estimated by
the Kaplan-Meier method.21 Differences in survival between patient PS (ECOG)0, 1 45 (56)groups were analyzed univariately by the log-rank test.22
2-4 12 (15)Unknown 23 (29)RESULTS
No. of extranodal sites at presentationClinical Features None 18 (23)
1 25 (31)MCL comprised approximately 4% of ML cases observedú1 37 (46)at the BCCA during the 7-year study period. The clinical
characteristics of the 80 patients are summarized in Table Abbreviations: LDH, lactate dehydrogenase; ECOG, Eastern Cooper-ative Oncology Group.1. The median age at presentation was 65 years, with a mean
* Patient not staged because of severe coincident multiple sclerosis.age of 63 years (range, 39 to 86 years). The majority ofpatients were male, with a male-to-female ratio of 2.3:1.Most patients (88%) presented with advanced-stage disease(IIB bulky, III, or IV). Bulk disease was defined as lymph ceived irradiation with or without adjuvant chemotherapy.
Patients with advanced-stage disease received chemotherapynode masses greater than 10 cm. Extranodal involvement atpresentation occurred in 76% of cases; the most common based on the clinical behavior of the disease. Those with
indolent progression received single-agent chemotherapy,sites were BM (63%), PB (34%), gastrointestinal tract (10%),Waldeyer’s ring (10%), and liver (8%). In 25% of cases, and those with more aggressive disease were treated with
multiagent protocols including cyclophosphamide, doxoru-extranodal localization of disease was the primary presenta-tion. Multiple lymphomatous polyposis, defined as two or bicin, and additional agents. A cohort of 16 patients under the
age of 60 was treated aggressively with the chemotherapeuticmore sites of gastrointestinal mucosal involvement, wasfound in 5 patients either at presentation or during the course regimen BP-VACOP (bleomycin, cisplatin, etoposide, doxo-
rubicin, cyclophosphamide, vincristine, prednisone) in com-of their disease. Coincident breast cancer was present in 2patients. The median follow-up period for the entire group bination with involved-region radiotherapy (IRRT).23
OS for the whole group of 80 patients is graphically shownwas 39 months (range, 1 to 101 months).Treatment was heterogeneous because of variation in age, in Fig 1, with a median OS of 43 months. Comparisons of OS
between clinically relevant patient subsets were performed.stage, symptomatic state, and era of treatment. In general,patients with limited stage disease (IA, IIA nonbulky) re- Survival was significantly influenced by performance status
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

MANTLE CELL LYMPHOMA 2069
toses and lymphoblast-like cells. Perivascular hyaline sclero-sis was also a feature common to the majority of involvedlymph nodes.
Cytologically, MCL nuclei were round to ovoid, slightlyirregular with inconspicuous nucleoli and slightly clumpedchromatin (Fig 3A). Cytoplasm was scant. Larger cells withmedium-sized nuclei, fine chromatin, inconspicuousnucleoli, and scant cytoplasm were present in most cases tovarying degrees. These cells resembled lymphoblasts ratherthan large noncleaved cells, prolymphocytes, or paraimmu-noblasts. In some cases, lymphoblast-like cells were presentin significantly increased numbers (Figs 3B and C), implyingcytologic transformation (discussed below). Mitoses wereeasily found in the majority of cases, the prognostic signifi-cance of which is discussed below.Fig 1. OS of all 80 patients with MCL. (MED SURV, median OS in
Patterns of pretreatment biopsy architecture, mitotic activ-months).ity, and features of cytologic transformation were analyzedto determine their prognostic significance in terms of overallpatient survival. The criteria used for defining these histolog-
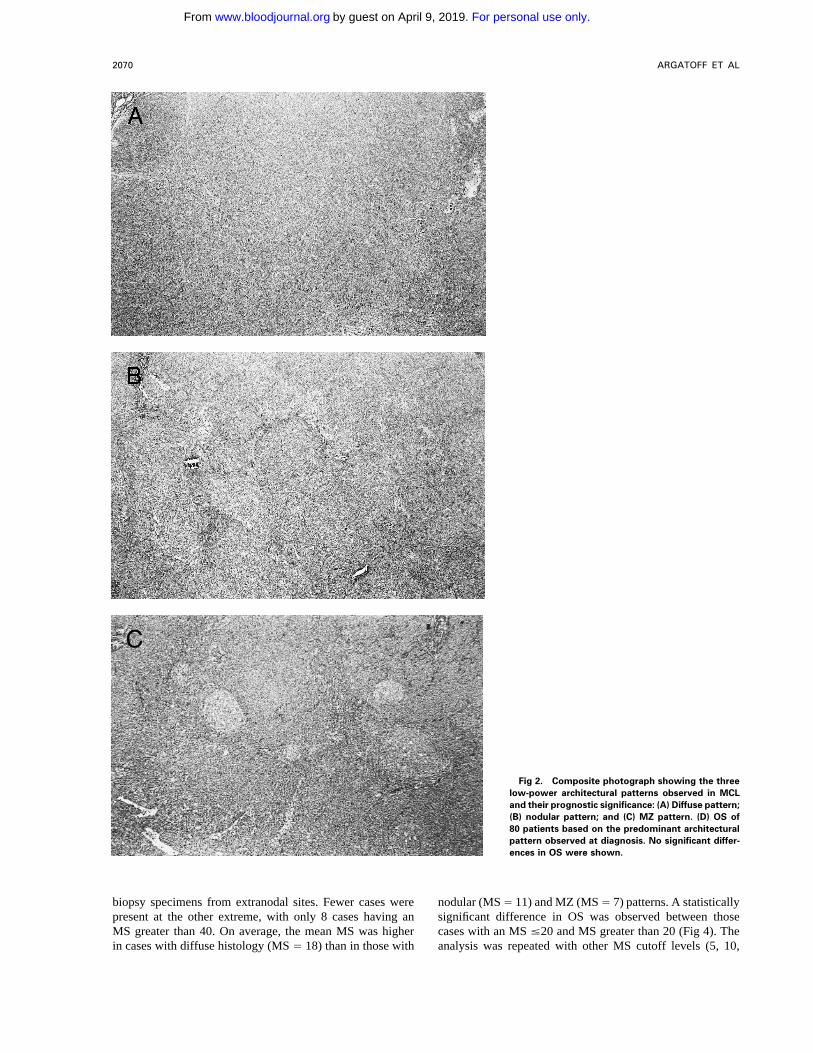
(PS), in that those patients with PS of greater than 1 (n Å ical parameters are discussed below, and the results of sur-12) had a significantly shorter OS than did those with PS of vival analysis are shown in Figs 2D, 3D, and 4 and are°1 (n Å 45; OS, 14 v 45 months; P õ .01). Age (°60 v summarized in Table 2.ú60 years), stage (limited versus advanced), serum lactate Architecture. The architecture of both nodal and extra-dehydrogenase (LDH; normal versus elevated), and number nodal tissue was classified as diffuse, nodular, or MZ ac-of extranodal sites of involvement (°1 v ú1 site) did not cording to the predominant pattern observed with the lowsignificantly predict for patient outcome, but each of these power (21) objective and shown in Fig 2. Cases with clear,clinical variables did show a trend toward shorter survival well-defined nodularity and lacking a significant MZ patternin the presence of the respective adverse factor. A calculated (n Å 13) were classified as ‘‘nodular,’’ similar to those ofInternational Prognostic Index (IPI) score,24 available for 44 other investigators.6 Cases with diffuse architecture lackedpatients, did not significantly predict for patient outcome. any nodularity, although scattered, compressed germinalSurvival differences between clinically relevant treatment centers were occasionally observed. When a mixture of pat-groups was limited by small numbers; however, in the group terns was encountered, architecture was arbitrarily assignedof patients under the age of 60, the BP-VACOP/IRRT group based on which pattern occupied greater than 50% of the(n Å 16) did not have significantly different survival from cross-sectional area of all sections available for review. Inthat of the remainder (n Å 13). 5 cases, architecture was difficult to assign for two main
reasons, biopsy size and extranodal origin. The 5 biopsyHistological Findings specimens, obtained from colonic, conjunctival, gastric, he-
patic, or pleural sites, morphologically fit the criteria of MCLLymph node biopsy specimens were obtained from 60and had ancillary studies providing confirmation. Becausepatients at presentation, whereas biopsy specimens were ob-none of these 5 biopsy specimens showed any evidence oftained from extranodal sites in the remaining 20. All biopsynodularity, all were arbitrarily assigned to the diffuse cate-material fulfilled the diagnostic criteria for MCL.1,19 At lowgory.power, lymph nodes were completely effaced by small- to
Between these architectural subtypes, no statistically sig-medium-sized lymphocytes in a diffuse and/or nodular pat-nificant differences in OS were observed (Fig 2D), nor weretern. Extranodal tissue, depending on the site, showed eitherany significant differences in OS observed after exclusionsheets or nodules of small/medium-sized lymphocytes re-of the 20 extranodal cases. Also, no survival differencesplacing normal structures or invading stromal tissue. No pro-were observed when the nodular and MZ cases were com-liferation centers were observed in any case. Occasionalbined and compared with the cases with a diffuse architec-compressed germinal centers lacking a normal MZ (nakedture.germinal centers) were observed in a minority of cases with
Mitotic activity. A mitotic score (MS) was calculated fordiffuse architecture and were not taken as evidence of a trueeach case by counting mitotic figures in 10 hpf (401 objec-MZ pattern. At low power, a characteristic mottled patterntive, 101 ocular) selected at random within a representativewas observed, imparted by scattered, large epithelioid histio-tissue section. In virtually all 80 cases, it was found thatcytes with pale eosinophilic cytoplasm and no tingible bodiesmitoses were uniformly distributed. This was confirmed by(Fig 2A). In 1 case, the histiocytic component was florid,counting mitoses in an additional 10 or 20 hpf in approxi-forming nodules and small sheets. Tingible body macro-mately 30% of cases, with special attention to those withphages were observed in only a minority of cases; in the 6low mitotic activity (MS ° 5). Overall, the mean MS wascases in which they were numerous (at least one in every16, with a median of 10 and a range of 0 to 87. In 22 caseshigh power field [hpf]), there was evidence of increased
cellular proliferation, in particular, increased numbers of mi- the MS was low (°5), and, of note, 14 of these represented
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom
ARGATOFF ET AL2070
Fig 2. Composite photograph showing the threelow-power architectural patterns observed in MCLand their prognostic significance: (A) Diffuse pattern;(B) nodular pattern; and (C) MZ pattern. (D) OS of80 patients based on the predominant architecturalpattern observed at diagnosis. No significant differ-ences in OS were shown.
biopsy specimens from extranodal sites. Fewer cases were nodular (MSÅ 11) and MZ (MSÅ 7) patterns. A statisticallysignificant difference in OS was observed between thosepresent at the other extreme, with only 8 cases having an
MS greater than 40. On average, the mean MS was higher cases with an MS °20 and MS greater than 20 (Fig 4). Theanalysis was repeated with other MS cutoff levels (5, 10,in cases with diffuse histology (MS Å 18) than in those with
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

MANTLE CELL LYMPHOMA 2071
smear at the time of staging and was confirmed by flowcytometry in all cases in which the number of circulatingMCL cells was low.
OS was compared between those patients that presentedwith PB involvement and the remainder of the patients inwhich PB involvement was either not present or unknown.Survival was significantly shorter in those who were leuke-mic at presentation (Fig 5B).
BM Biopsy Findings
Staging BM trephine biopsies were performed in 75 pa-tients. In 47, there was clear histological evidence of involve-ment by MCL, the patterns of which are summarized inTable 4. In 3 cases, the core biopsy specimen was histologi-cally nondiagnostic; however, in each of these 3, flow cyto-Fig 2 (cont’d).metric immunophenotyping showed a clonal B-cell popula-tion with CD5 coexpression. In 2 cases, the core biopsyspecimen was suspicious but not diagnostic for involvementand 15), but 20 was found to be the most discriminant (databy MCL, and, in 23, no evidence of MCL was observed.not shown). When the 20 extranodal cases were excludedBiopsies were not performed in 5 cases for various reasonsfrom the analysis, the results were the same.including advanced comorbid neurological disease (n Å 2),Blastic features. Virtually all 80 cases had at least a fewthe presence of circulating lymphoma cells (n Å 1), andcells with larger nuclei, finer chromatin, and inconspicuousundefined (n Å 2).nucleoli; however, in the majority of cases, these cells were
In all histologically positive BM biopsy specimens, thepresent in small numbers. When present in increased num-lymphomatous infiltration was found predominantly in anbers, these lymphoblast-like cells were almost always ac-interstitial or intertrabecular location, arranged in either nod-companied by an increase in mitotic activity and, occasion-ular aggregates or diffuse infiltrates, or a combination ofally, the presence of tingible body macrophages (Fig 3B).both. A few cases showed a prominent paratrabecular patternThese cases were designated as having prominent featuresreminiscent of small cleaved-cell lymphoma. In all cases,of cytologic transformation. In a minority (n Å 5), the blasticthe cellular morphology was virtually identical to that ofcells were so numerous that the histology was nearly indistin-MCL observed in lymph nodes, lacking large transformedguishable from that of lymphoblastic lymphoma; these casescells and proliferation centers. In 1 case, the cytomorphologywere designated blastic MCL (Fig 3C). The mean MS in thewas indistinguishable from acute lymphoblastic leukemia.blastic MCL cases was 57.Prognostic significance was determined by comparing thoseThe OS was significantly shorter for those cases withcases (n Å 50) that were positive for involvement with theblastic morphology (Fig 3D). No statistically significant dif-remainder of cases (n Å 30), in which BM involvement wasferences in survival were observed between the 16 cases thatnot evident (n Å 25) or was unknown (n Å 5). No significantwere transformed to some degree but not truly blastic anddifference in survival was found (data not shown). Outcomethe remaining 59 cases that showed no evidence of transfor-was also assessed based on the degree of staging BMmation.involvement, estimated on the core biopsy specimen as lessthan or greater than 50% (Table 4). Those with heavyPB Findingsinvolvement by MCL (n Å 12) tended to have a shorter OS
PB films were available for review in 69 cases. The results than did those with partial involvement (n Å 35), althoughare summarized in Table 3. The typical PB appearance of the results were of borderline significance (median OS, 26circulating MCL was a polymorphous mixture of small, me- v 45 months; P Å .06; data not shown).dium, and large lymphocytes, a pattern also described byothers.17 The predominant cell type in most cases had a
Sequential Biopsies: Histological Patterns of Diseaseslightly irregular nucleus with fine chromatin, a small nucle-Progressionolus, and a thin rim of gray-blue cytoplasm. Cells with a
small cleaved or chronic lymphocytic leukemia (CLL)-like Thirty-seven patients underwent additional biopsies dur-ing the course of their illness. The material examined in-morphology were often present, as were immature cells with
L1 and L2 lymphoblast-like morphology (Fig 5A). In 1 case, cluded BM (n Å 9), extranodal tissue (n Å 9), lymph node(n Å 5), spleen (n Å 4), fine-needle aspirate of an involvedthe blastic population predominated, creating the initial im-
pression of acute lymphoblastic leukemia. Although absolute site (n Å 7), and PB (n Å 3). A median period of 22 months(range, 1 to 70 months) separated the procurement of theselymphocyte counts were not recorded, a significant propor-
tion of cases with PB involvement did not have an elevated specimens from the time of the diagnostic biopsy. In 29 ofthese cases (78%), the cytology and/or architecture werelymphocyte count by peripheral smear assessment. Leuke-
mic involvement at diagnosis was defined as the presence unchanged from the time of diagnosis (median interval fromoriginal biopsy, 15 months; range, 1 to 67 months). In theof any detectable circulating MCL cells observed on the PB
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

ARGATOFF ET AL2072
Fig 3. Composite photograph showing the cyto-logic features of MCL. (A) Typical cytology of MCLcharacterized by cells with small, slightly irregularnuclei, inconspicuous nucleoli, and minimal cyto-plasm. Note the frequent epithelioid histiocytes(arrows). (B) MCL with prominent features of trans-formation, but not clearly blastic. Increased numbersof larger cells with fine chromatin and inconspicuousnucleoli are shown (arrows). (C) Blastic MCL. Notethe cytologic resemblance to lymphoblasticlymphoma. (D) OS of 80 patients with MCL based onthe presence of blastic features. The 5 cases desig-nated as blastic MCL were associated with a signifi-cantly shorter survival when compared with that ofall others (n ! 75) including those with features oftransformation as shown in (B).
AID Blood 0040 / 5H30$$0040 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

MANTLE CELL LYMPHOMA 2073
Table 2. Prognostic Significance of Architecture, Mitotic Activity,and Cellular Morphology of 80 Cases of MCL
No. of Cases Median OSHistologic Feature (%) (mo)
ArchitectureDiffuse 62 (78) 39Nodular 13 (16) 47MZ 5 (6) —
P Å NSMitotic activity (mitotic figures/10 hpf)°20 62 (78) 52ú20 18 (22) 15
Cytologic transformationNot prominent 59 (74)
45Prominent but not blastic 16 (20)Prominent blastic 5 (6) 15
(P õ .001)Fig. 3 (cont’d).
remaining 8 (22%), increased numbers of larger,lymphoblast-like cells were observed, indicating cytologic and 4 from extranodal or unspecified sites). In 5 cases, the
results were not diagnostic of lymphoma. Results of thetransformation (median interval from original biopsy, 34months; range, 14 to 70 months). Of these 8, the 5 open 44 positive cases are shown in Table 5. The characteristic
immunophenotype of the MCL cases analyzed was CD19/,lymph node biopsy specimens showed more mitotic activityand blastic cells than were observed in the original biopsy CD20/, CD5/, and FMC-7/ and CD100 and CD230, with
a slight preponderance of l surface Ig (SIg) positivity. SIgspecimens, but none were frankly blastic. In another 2 cases,increased numbers of blastic cells were present in the PB. brightness was documented in only one quarter of the cases,
and, in all of these, SIg was moderate to bright. Three casesIn the eighth case, transformation was diagnosed on a lymphnode fine-needle aspirate. Large noncleaved cells were not showed an aberrant immunophenotype. One coexpressed
both CD5 and CD10, and another lacked CD5 expression,observed in any of this material. Nodal architecture remaineddiffuse in 4 cases, nodular in 1 case, and changed from while the third weakly coexpressed CD23. All 3 had other
data to substantiate the diagnosis of MCL. CD11c expres-nodular to diffuse in 1 case. All 8 patients in which cytologicchange was found died within 12 months (median, 9 sion, although not shown in Table 5, was consistently nega-
tive in all cases analyzed.months), whereas only 16 of 29 patients without cytologicchange have died (median follow-up period for all 29 pa-
Cytogenetic Findingstients, 8 months; range, 0 to 67 months). No significantdifference in OS between the two groups was found. Cytogenetic analysis was performed in 31 cases. Results
are summarized in Table 6. The translocation t(11;14)Immunophenotypic Findings (q13;q32), characteristic of MCL, was the most frequently
occurring abnormality in this group. The next most commonImmunophenotyping by flow cytometry was performed in49 cases (19 from lymph node tissue, 26 from BM or PB, groups of abnormalities involved chromosomes 9 and 17.
Monosomy 9 was observed in 2 cases; whereas, in 3 cases,structural abnormalities of 9q were found, ie, an inversion,a deletion, and a balanced translocation with 14q32. In 2cases, 17p11 was disrupted because of balanced transloca-tions with chromosomes 3 and 15, respectively; whereas, inanother 2 cases, monosomy 17 was found. The cases withabnormal clones not obviously including t(11;14) may have
Table 3. PB Involvement in 80 Cases of MCL
PB Involvement No. of Patients (%)
Positive 39 (49)At presentation 27 (34)Later in course
(negative or unknown at presentation) 12 (15)Negative 39 (37)
Fig 4. OS of 80 patients with MCL bases on MS (mitoses/10 ran- Unknown* 11 (14)dom hpf). An MS of greater than 20 was associated with a signifi-cantly shorter survival. * PB films unavailable for review.
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

ARGATOFF ET AL2074
Fig 5. (A) PB involvement in MCL is characterizedby a polymorphous cell population including largercells with immature nuclei and prominent nucleoli.(B) OS of 80 cases of MCL based on PB involvementat diagnosis. Those cases positive for PB involve-ment (n ! 27) were associated with a significantlyshorter survival when compared with those in whichPB was not involved or not assessed (n ! 53).
Molecular Genetic Findings
SA for bcl-1 gene rearrangement was performed in 20cases. Table 7 summarizes these results and compares themwith the cytogenetic results. No significant differences insurvival could be shown between the 11 cases with and 9cases without SA evidence of bcl-1 rearrangement.
DISCUSSION
The pathology of MCL is well defined, but the criteria forand clinical relevance of histological subclassification remaincontroversial. Some regard MCL with an MZ architecture as‘‘low grade,’’ whereas others find that survival in these casesis similar to that of cases with a diffuse growth pattern.2 Inaddition, some studies have suggested that factors such as mi-totic activity and increased numbers of blast-like cells signal aworse outcome. Resolution of these issues has been slow be-had complex or cryptic alterations involving the bcl-1 andcause of the small numbers of cases available for study andIg heavy-chain loci. No significant differences were foundthe lack of consensus diagnostic criteria. This analysis of 80between the 14 cases with t(11;14) and the 4 cases in whichcases of MCL, the largest series to date, was undertaken withanalysis was successful but failed to show a t(11;14). Simi-the intent to help resolve some of these questions.larly, no differences in survival could be shown between the
Attempts at determining which pathological and clinicalgroups of patients with chromosome 9 and 17 abnormalitiesfactors are of prognostic value in patients with MCL haveand the remainder of MCL cases. However, the number ofproduced variable results. In particular, several studies sug-cases was too small to make a meaningful statistical compari-gest that the MZ variant behaves in a more indolent mannerson.
Table 5. Results of Immunophenotyping in 44 Cases of MCLTable 4. BM Examination: Patterns of Involvement Seen in Staging
No. of CasesBM Biopsy Specimens of 47 Cases Positive for MCL
Result No. of Patients (%) Antigen Positive Negative Not Analyzed
Degree of BM involvement CD5 42 1 1Heavy (ú50% of biopsy) 12 (26) CD10 1 41 1Partial (°50% of biopsy) 35 (74) CD19/20 44 0 0
Pattern CD23 1 (dim) 14 29Interstitial/intertrabecular 34 (72) FMC-7 11 0 33
Diffuse 13 (28) k* 18 — 0Nodular 17 (36) l* 26 — 0Mixed nodular/diffuse 4 (9)
* Surface IG brightness was moderate to strong in those cases (11)Mixed paratrabecular/interstitial 13 (28)
in which it was documented.
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

MANTLE CELL LYMPHOMA 2075
Table 6. Results of Cytogenetic Analysis in 31 Cases of MCL BP-VACOP/IRRT regimen did not produce a survival ad-vantage despite being administered only to patients underNo. of
Result Cases the age of 60.All 80 cases met the accepted histological criteria fort(11;14)(q13;q32) present* 14
MCL.1 Particularly useful features distinguishing MCL fromt(11;14)(q13;q32) absent, but karyotype abnormal 4Case no. 1: 43-44,X,0Y,der(3)t(3;?)(p11;?),t(8;9)(q24;q13), other diffuse small-cell ML include the monotonous
der(9)t(9;14)(q13;q32),011,015,del(14)(q23), lymphoid infiltrate, absence of growth centers, scattered epi-der(17)t(3;17)(q13;p11),021,/mar[cp16] thelioid histiocytes, perivascular hyaline sclerosis, and vir-
Case no. 2: 47,X,0Y,/3,add(14)(q32),/mar1,/mar2[7] tual absence of large transformed cells. Although mitoticCase no. 3 and 4: complex abnormal cell lines† figures were conspicuous in most cases, it is important to
Analysis unsuccessful‡ 13note that, in 22 cases, the MS was low (°5). Also, it is
* Includes 1 case with complex disruption of both 11q13 and 14q32 apparent from examination of sequential biopsy specimensbut no clearly identifiable translocation. that the pattern of transformation of MCL can be best de-
† Patients with concurrent breast cancer in lymph node specimens.scribed as a progressive increase in cells with slightly larger
Abnormal karyotype is likely that of carcinoma.nuclei and finer chromatin, but a lack of nucleoli in tissue‡ Specimens that failed to yield analyzable metaphases or yieldedsections. This cytologic transformation is often accompaniedonly normal metaphases from suboptimal tissue sites (eg, BM or PB).by an increase in mitotic rate.
The prognostic significance of three histological features,architecture, mitotic activity, and relative number of
than the diffuse type,5,25 with a quoted OS of 88 months,14
lymphoblast-like cells is summarized above; however, sev-whereas others have shown no differences in survival.6 Oth-eral points need to be addressed. First, this study failed toers have shown decreased survival in cases with increasedshow any significant differences in OS between the MZ,mitotic activity,8,11,14 prominent blastic morphology,4,5,6,14,26
nodular, and diffuse subtypes. These results are similar toor PB involvement.6,8,15,17 Other factors examined includethe findings of Norton et al6 but contrast those of Duggan etage, sex, B symptoms, splenomegaly, remission status, he-al,14 who found MCL with an MZ architecture to be indolent.moglobin level, platelet count, lymphocyte count, serum al-Although the appearance of an MZ pattern is well describedbumin, serum sodium, CD10 positivity, Ki67 positivity,in the literature, the criteria for a true MZ pattern are unde-cyclin D1 expression, and p53 gene anomalies with varyingfined and are subject to interobserver variability. When com-results.6,10,11,14,25-27
pared with other MCL series, the proportion of MZ casesIn this study, all 80 cases had clinical features and survivalobserved here (6%) is similar to that observed by Norton etcharacteristics fully compatible with those described foral6 (6%) and Pittaluga et al15 (11%) but is significantly lowerMCL, as summarized in Table 1 and shown in Fig 1. Of thethan that reported by Lardelli et al5 (55%) and WeisenburgerIPI clinical prognostic variables,24 prognosis was signifi-et al25 (30%), two studies in which there were demonstrablecantly influenced by PS but was not significantly influenceddifferences in survival between MZ and other architecturalby age, stage, LDH level, and extranodal involvement, al-subtypes. The reasons for this are unclear but are likely tothough a trend toward a worse outcome was observed forbe caused by differences in criteria for defining an MZ pat-the latter four factors. The IPI score also did not significantlytern, rather than true geographic differences in frequency.predict for patient outcome. Although the numbers of pa-Because the criteria for defining an MZ pattern in this studytients, particularly those with limited-stage disease, may notmay have been more strict than those in other series, wehave been large enough to permit detection of a survivalalso pooled the nodular and MZ cases together and compareddifference using the IPI prognostic variables, it is more likelythem with the diffuse cases. However, once again, no differ-that simply having the diagnosis of MCL, with its inherentlyence in OS was found.poor outcome, supersedes any prediction of behavior based
A diagnosis of blastic MCL, defined in this study andon clinical factors. Definitive statements of effectiveness ofby others5 as MCL with the appearance of lymphoblasticcertain treatment protocols were not possible in this study
because no treatment group did well. Even the more intense lymphoma, assigns the patient a very unfavorable prognosis.
Table 7. Summary of bcl-1 Rearrangement Results and Comparison With Cytogenetics for 80 Cases of MCL
Southern Analysis Result
Cytogenetic Result bcl-1 Rearranged bcl-1 Germline Not Analyzed Total Cases
Abnormal karyotypet(11;14) present 5 5 4 14t(11;14) absent* 0 1 3 4
Normal karyotype or unsuccessful analysis 5 2 6 13Not analyzed 1 1 47 49
Total cases 11 9 60 80
* See Table 6, case no. 1 was in germline configuration for bcl-1, and cases no. 2, 3, and 4 were not tested.
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

ARGATOFF ET AL2076
This histological pattern should be relatively reproducible; increased biological aggressiveness rather than only overalltumor burden.however, it is unclear what number of blastic cells is needed
to make the diagnosis. The fact that others refer to similar Immunophenotypically, the 44 cases with diagnostic anal-yses had, with 3 exceptions, the typical immunoprofile ofcases as ‘‘blastoid,’’6 ‘‘large-cell,’’26 or ‘‘anaplastic’’27 vari-
ants attests to the current lack of standardized diagnostic MCL. Antibody FMC-7, described by others in the differen-tiation of subgroups of B-cell lymphoproliferative disor-criteria. Attempts have been made by others to count large
cells manually14,28 or by image analysis26; however, the cyto- ders,30 when used in combination with CD23, was very use-ful in distinguishing MCL from CLL/small lymphocyticmorphology of MCL cell is a spectrum, making it a difficult
task when applied in a routine clinical setting, excepting lymphoma (SLL) in our series, because the majority of casesof MCL were FMC-7/ and CD230, whereas the oppositethose cases with florid blastic change as described herein.
More objective methods of assessing the proliferation rate, pattern occurs in the majority of CLL/SLL cases.17,31
No morphologic or clinical differences could be attributedincluding mitotic counts and Ki67 nuclear antigenic expres-sion, have also been applied to MCL and appear to be closely to the presence or absence of the t(11;14)(q13;q32) or bcl-1
gene rearrangement. Addtionally, no outcome or histologicallinked with blastic morphology, as would be expected. Ithas been shown by the results of this study and by those of differences were observed for those cases with chromosome
9 or 17 abnormalities, but the number of affected cases wasothers, that increased mitotic activity predicts for a worsetoo small to allow for a meaningful statistical comparison.outcome, although the exact number of mitoses at whichMost reports have identified t(11;14) and bcl-1 gene rear-prognosis was found to be different varies from study torangements as highly specific for MCL32-34; however, thesestudy (10 of 10 hpf,14 20 of 30 hpf,8 and 20 of 10 hpf11).abnormalities have also been rarely described in SLL andAlthough not evident from examination of the results ofplasma cell dyscrasias. In a recent report in which the pres-these studies, this variability may be the result of differencesence of a t(11;14) or bcl-1 rearrangement was associatedin patient populations, but is more likely to be caused by thewith ML with morphologic findings atypical for MCL, theinherent interobserver variability of counting mitotic figures.clinical course of these patients was similar to that of MCL.35Regardless, the data indicate that prognosis is closely linkedSimilarly, we have recently observed a case of ML with ato the mitotic count in MCL, which is similar to that observedt(11;14) and a bcl-1 rearrangement that had classical prolif-in other lymphomas of aggressive histology,29 and mitoticeration centers in which the clinical course was more akinactivity and blastic morphology are unlikely to be indepen-to MCL than to SLL. We were unable to show a survivaldent variables, although this postulate can only be testeddifference in this study for cases with or without a t(11;14)with multivariate analysis.or a bcl-1 rearrangement. It is unlikely that the presence ofCytologic evidence of blastic change in sequential biopsythese cytogenetic and/or molecular genetic findings will bespecimens was found in 8 patients (11% of the total nonblas-prognostically important, because the recent development oftic cases), all 8 of whom died within 12 months. However,sophisticated fluorescence in situ hybridization techniquesthe OS of these patients was no different from those withouthas shown that virtually all cases of MCL possess thesetransformation and may reflect a lead-time bias: the patientsabnormalities.36,37 We did not stain these cases for cyclinwith transformation were serially biopsied later in theirD1 protein, but virtually all cases of MCL overexpress thiscourse (median, 34 months from original biopsy) than wereprotein,3,38-42 making it a useful diagnostic reagent but anthose without transformation (median, 15 months). Unfortu-unlikely prognostic marker. Perhaps, the interaction of cyclinnately, the exact incidence of blastic change in this patientD1 with other cellular proteins (retinoblastoma gene, p16,population is not known because autopsy follow-up resultsp21, ubiquitin, and so on) contributes to lymphoma develop-were unavailable, but the results of Norton et al6 suggestment, and measurement of one or more of these proteinsthat it occurs at a higher frequency (28%) than is currentlymay prove to be independent prognostic factors in MCL.recognized.
In summary, this study confirms the aggressive nature ofThe high incidence of PB and BM involvement by MCLMCL and provides evidence that MS, blastic morphology,at diagnosis observed in 34% and 63% of cases, respectively,and leukemic involvement at diagnosis predict for poor out-is in keeping with that found by others.6,11,15 PB involvementcome. Standard clinical indicators of prognosis such as age,at diagnosis predicted for a shortened survival in our study;stage, number of extranodal sites, or presence of B symptomshowever, interestingly, the presence or absence of BMhad little discernable impact because the overall prognosisinvolvement did not. Although heavy BM infiltration waswas so poor. Such factors are unlikely to be predictive untilassociated with a trend toward shorter survival, no correla-more effective treatments become available. We have alsotion of this feature with PB involvement could be shown.shown that, although architecture does not have prognosticThe predictive power of PB involvement may be the resultimportance, there is a need to develop standardized histologi-of a bias toward increased numbers of cases with MS ofcal criteria for both ‘‘MZ’’ and ‘‘blastic’’ morphologies.
greater than 20 in the leukemic group versus that in theResolution of these problems together with large collabora-
nonleukemic group (41% v 17%; P Å .03); in contrast, casestive studies are crucial to provide further insight into the
with MS of greater than 20 were evenly distributed through-effective treatment and possible cure of this disease.
out both positive and negative BM cases (data not shown).ACKNOWLEDGMENTMultivariate analysis would be necessary to confirm PB
involvement as an independent variable; however, these data The authors thank Drs S. O’Reilly, P. Hoskins, and T. Shenkierfor their help in providing clinical data for this study; Drs C. Coppinimply that, in some cases, leukemic involvement may reflect
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

MANTLE CELL LYMPHOMA 2077
and A. Coldman for their assistance with statistical analysis; and trephine and peripheral blood smears in 55 patients with mantle celllymphoma. Leuk Lymphoma 21:115, 1996Ms C. Wong for her help with data collection.
16. Weisenburger DD, Kim H, Rappaport H: Mantle-zoneREFERENCES lymphoma. A follicular variant of intermediate lymphocytic
lymphoma. Cancer 49:1429, 19821. Banks PM, Chan J, Cleary ML, Delsol G, De Wolf-Peeters C,17. Pombo De Oliveira MS, Jaffe ES, Catovsky D: LeukaemicGatter K, Grogan TM, Harris NL, Isaacson PG, Jaffe ES, Mason D,
phase of mantle zone (intermediate) lymphoma: Its characterisationPileri S, Ralfkiaer E, Stein H, Warnke RA: Mantle cell lymphoma.in 11 cases. J Clin Pathol 42:962, 1989A proposal for unification of morphologic, immunologic, and molec-
18. Vadlamudi G, Lionetti KA, Greenberg S, Mehta K: Leukemicular data. Am J Surg Pathol 16:637, 1992phase of mantle cell lymphoma. Two case reports and review of the2. Weisenburger DD, Armitage JO: Mantle cell lymphoma—Anliterature. Arch Pathol Lab Med 120:35, 1996entity comes of age. Blood 87:4483, 1996
19. Zucca E, Stein H, Coiffier B: European Lymphoma Task3. Rimokh R, Berger F, Delsol G, Charrin C, Bertheas MF,Force (ELTF): Report of the workshop on mantle cell lymphomaFrench M, Garoscio M, Felman P, Coiffier B, Bryon PA, Rochet(MCL). Ann Oncol 5:507, 1994M, Gentilhomme O, Germain D, Magaud JP: Rearrangement and
20. Taylor SA, Tsang AOW, Fu KH, Kalousek DK, Horsmanoverexpression of the BCL-1/PRAD-1 gene in intermediate lympho-DE: Comparative study of automated versus manual extraction ofcytic lymphomas and in t(11q13)-bearing leukemias. Blood 81:3063,DNA from clinical specimens. Am J Clin Pathol 93:749, 19901993
21. Kaplan EL, Meier P: Nonparametric estimation from incom-4. Fisher RI, Dahlberg S, Nathwani BN, Banks PM, Miller TP,plete observations. J Am Stat Assoc 53:457, 1958Grogan TM: A clinical analysis of two indolent lymphoma entities:
22. Peto R, Peto J: Asymptomatically efficient rank invariantmantle cell lymphoma and marginal zone lymphoma (including the(logrank) procedures. J Roy Stat Soc 135:185, 1972mucosa-associated lymphoid tissue and monocytoid B-cell subcate-
23. Klasa RJ, Hoskins PJ, O’Reilly SE, Fairey R, Voss N, Gas-gories): A Southwest Oncology Group study. Blood 85:1075, 1995coyne R, Connors JM: BP-VACOP and extensive lymph node irradi-5. Lardelli P, Bookman MA, Sundeen J, Longo DL, Jaffe ES:ation (RT) for advanced stage low grade lymphoma (abstract). ProcLymphocytic lymphoma of intermediate differentiation. Morpho-Am Soc Clin Oncol 11:328, 1992logic and immunophenotypic spectrum and clinical correlations. Am
24. The International Non-Hodgkin’s Lymphoma Prognostic Fac-J Surg Pathol 14:752, 1990tors Project: A predictive model for aggressive non-Hodgkin’s6. Norton AJ, Matthews J, Pappa V, Shamash J, Rohatiner AZS,lymphoma. N Engl J Med 329:987, 1993Lister TA: Mantle cell lymphoma: natural history defined in a seri-
25. Weisenburger DD, Duggan MJ, Perry DA, Sanger WG, Armi-ally biopsied population over a 20-year period. Ann Oncol 6:249,tage JO: Non-Hodgkin’s lymphomas of mantle zone origin. Pathol1995Annu 26:139, 19917. Pittaluga S, Wlodarska I, Stul MS, Thomas J, Verhoef G,
26. Zoldan MC, Inghirami G, Masuda Y, Vandekerckhove F,Cassiman JJ, Van Den Berghe H, De Wolf-Peeters C: Mantle cellRaphael B, Amorosi E, Hymes K, Frizzera G: Large-cell variantslymphoma: A clinicopathological study of 55 cases. Histopathologyof mantle cell lymphoma: Cytologic characteristics and p53 anoma-26:17, 1995lies may predict poor outcome. Br J Haematol 93:475, 19968. Swerdlow SH, Habeshaw JA, Murray LJ, Dhaliwal HS, Lister
27. Ott MM, Ott G, Kuse R, Porowski P, Gunzer U, Feller AC,TA, Stansfeld AG: Centrocytic lymphoma: a distinct clinicopatho-Muller-Hermelink HK: The anaplastic variant of centrocyticlogic and immunologic entity. A multiparameter study of 18 caseslymphoma is marked by frequent rearrangements of the bcl-1 geneat diagnosis and relapse. Am J Pathol 113:181, 1983and high proliferation indices. Histopathology 24:329, 19949. Teodorovic I, Pittaluga S, Kluin-Nelemans JC, Meerwaldt JH,
28. Perry DA, Bast MA, Armitage JO, Weisenburger DD: DiffuseHagenbeek A, van Glabbeke M, Somers R, Bijnens L, Noordijkintermediate lymphocytic lymphoma. A clinicopathologic study andEM, De Wolf Peeters C for the European Organization for the Re-comparison with small lymphocytic lymphoma and diffuse smallsearch and Treatment of Cancer Lymphoma Cooperative Group:cleaved cell lymphoma. Cancer 66:1995, 1990Efficacy of four different regimens in 64 mantle cell lymphoma
29. Akerman M, Brandt L, Johnson A, Olsson H: Mitotic activitycases: Clinicopathologic comparison with 498 other non-Hodgkin’sin non-Hodgkin’s lymphoma. Relation to the Kiel classification andlymphoma subtypes. J Clin Oncol 13:2819, 1995to prognosis. Br J Cancer 55:219, 198710. Velders GA, Kluin-Nelemans JC, De Boer CJ, Hermans J,
30. Huh YO, Pugh WC, Kantarjian HM, Stass SA, Cork A, Tru-Noordijk EM, Schuuring E, Kramer MHH, Van Deijk WA, Rahderjillo JM, Keating MJ: Detection of subgroups of chronic B-cellJB, Kluin PM, Van Krieken JHJM: Mantle-cell lymphoma: a popula-leukemias by FMC7 monoclonal antibody. Am J Clin Patholtion-based clinical study. J Clin Oncol 14:1269, 1996101:283, 199411. Weisenburger DD, Nathwani BN, Diamond LW, Winberg
31. Kilo MN, Dorfman DM: The utility of flow cytometric immu-CD, Rappaport H: Malignant lymphoma, intermediate lymphocyticnophenotypic analysis in the distinction of small lymphocytictype: A clinicopathologic study of 42 cases. Cancer 48:1415, 1981lymphoma/chronic lymphocytic leukemia from mantle cell12. Zucca E, Fontana S, Roggero E, Pedrinis E, Pampallona S,lymphoma. Am J Clin Pathol 105:451, 1996Cavalli F: Treatment and prognosis of centrocytic (mantle cell)
32. Raffeld M, Jaffe ES: bcl-1, t(11;14), and mantle cell-derivedlymphoma: A retrospective analysis of twenty-six patients treatedlymphomas. Blood 78:259, 1991in one institution. Leuk Lymphoma 13:105, 1994
33. Brito-Babapulle V, Ellis J, Matutes E, Oscier D, Khokhar13. Bookman MA, Lardelli P, Jaffe ES, Duffey PL, Longo DL:T, MacLennan K, Catovsky D: Translocation t(11;14)(q13;q32) inLymphocytic lymphoma of intermediate differentiation: morpho-chronic lymphoid disorders. Genes Chromosomes Cancer 5:158,logic, immunophenotypic, and prognostic factors. J Natl Cancer Inst199282:742, 1990
34. Jadayel D, Matutes E, Dyer MJS, Brito-Babapulle V, Khokhar14. Duggan MJ, Weisenburger DD, Ye YL, Bast MA, Pierson JL,MT, Oscier D, Catovsky D: Splenic lymphoma with villous lympho-Linder J, Armitage JO: Mantle zone lymphoma. A clinicopathologiccytes: analysis of bcl-1 rearrangements and expression of the cyclinstudy of 22 cases. Cancer 66:522, 1990D1 gene. Blood 83:3664, 199415. Pittaluga S, Verhoef G, Criel A, Maes A, Nuyts J, Boogaerts
M, De Wolf Peeters C: Prognostic significance of bone marrow 35. Swerdlow SH, Zukerberg LR, Yang W-I, Harris NL, Williams
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom

ARGATOFF ET AL2078
ME: The morphologic spectrum of non-Hodgkin’s lymphomas with 39. Rimokh R, Berger F, Bastard C, Klein B, French M, Archi-mbaud E, Rouault JP, Santa Lucia B, Duret L, Vuillaume M, Coiffierbcl-1/cyclin D1 gene rearrangements. Am J Surg Pathol 20:627,
1996 B, Bryon PA, Magaud JP: Rearrangement of CCND1(BCL1/PRAD1)3* untranslated region in mantle-cell lymphomas and t(11q13)-asso-36. Coignet L, Schuuring E, Kibbelaar R, Raap T, Kleiverda K,
Bertheas M-F, Wiegant J, Beverstock G, Kluin P: Detection of 11q13 ciated leukemias. Blood 83:3689, 199440. Zukerberg LR, Yang W-I, Arnold A, Harris NL: Cyclin D1rearrangements in hematologic neoplasms by double-color fluores-
cence in situ hybridization. Blood 87:1512, 1996 expression in non-Hodgkin’s lymphomas. Detection by immunohis-tochemistry. Am J Clin Pathol 103:756, 199537. Vaandrager J-W, Schuuring E, Zwikstra E, de Boer C, Klei-
verda K, van Krieken J, Kluin-Nelemans H, van Ommen G-J, Raap 41. de Boer C, Schuuring E, Dreef E, Peters G, Bartek J, KluinP, van Krieken J: Cyclin D1 protein analysis in the diagnosis ofA, Kluin P: Direct visualization of dispersed 11q13 chromosomal
translocations in mantle cell lymphoma by multicolor DNA fiber mantle cell lymphoma. Blood 86:2715, 199542. Yatabe Y, Nakamura S, Seto M, Kuroda H, Kagami Y, Suzukifluorescence in situ hybridization. Blood 88:1177, 1996
38. Swerdlow SH, Yang W-I, Zukerberg LR, Harris NL, Arnold R, Ogura M, Kojima M, Koshikawa T, Ueda R, Suchi T: Clinico-pathologic study of PRAD1/ cyclin D1 overexpressing lymphomaA, Williams ME: Expression of cyclin D1 protein in centrocytic/
mantle cell lymphomas with and without rearrangement of the with special reference to mantle cell lymphoma. Am J Surg Pathol20:1110, 1996BCL1/cyclin D1 gene. Hum Pathol 26:999, 1995
AID Blood 0040 / 5H30$$$781 02-12-97 08:55:04 blda WBS: Blood
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom
1997 89: 2067-2078
Larry H. Argatoff, Joseph M. Connors, Richard J. Klasa, Douglas E. Horsman and Randy D. Gascoyne Mantle Cell Lymphoma: A Clinicopathologic Study of 80 Cases
http://www.bloodjournal.org/content/89/6/2067.full.htmlUpdated information and services can be found at:
(4182 articles)Neoplasia Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
For personal use only.on April 9, 2019. by guest www.bloodjournal.orgFrom