marius m hoeper the use of era after seraphin, compass-2 and ambition
TRANSCRIPT
Marius M Hoeper
The use of ERA after SERAPHIN, COMPASS-2 and AMBITION


Galie N et al. J Am Coll Cardiol 2013;62:D60-72
Grade I recommendation and high level of
evidence only for initial mono-therapy

The future of combination therapy
1. Is monotherapy still adequate?2. Sequential or up-front?3. Are all drugs the same?

Is monotherapy still adequate?


Macitentan reduced morbidity/mortality events in treatment-naive patients
Macitentan 10 mg: 55%
00
20
40
80
100
60
12 18 24 30 366
Pat
ien
ts w
ith
ou
t th
e ev
ent
(%)
Macitentan 10 mg
Macitentan 3 mg
Placebo
Treatment difference 3 mg 10 mg
Hazard ratio (HR) 0.53 0.45
Log-rank p-value 0.007 <0.001
Risk reduction of primaryendpoint event vs placebo
Macitentan 3 mg: 47%
Patients at risk
88 74 68 64 58 38 17 Macitentan 10 mg86 74 63 59 56 29 13 Macitentan 3 mg96 66 54 45 42 24 13 Placebo
Time from treatment start (months)
Pulido T, et al. N Engl J Med 2013; 369: 809-18.
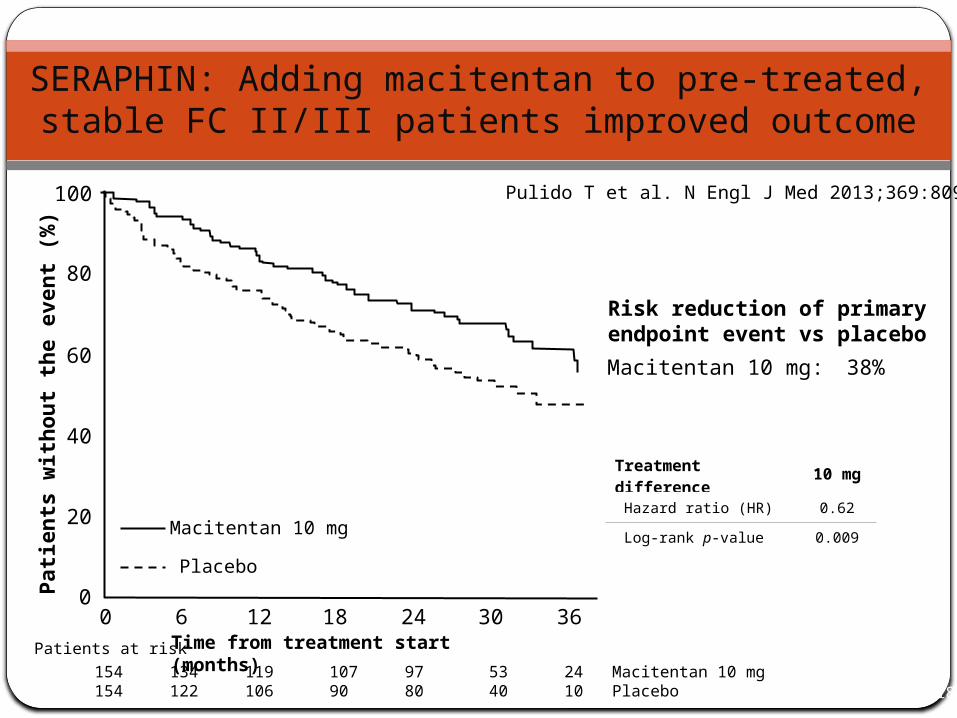
SERAPHIN: Adding macitentan to pre-treated, stable FC II/III patients improved outcome
Pulido T, et al. N Engl J Med 2013; 369: 809-18.
Macitentan 10 mg: 38%
Pat
ien
ts w
ith
ou
t th
e ev
ent
(%)
0 12 18 24 30 360
20
40
80
100
60
6
Macitentan 10 mg
Placebo
Treatment difference 10 mg
Hazard ratio (HR) 0.62
Log-rank p-value 0.009
Risk reduction of primaryendpoint event vs placebo
Patients at risk
154 134 119 107 97 53 24 Macitentan 10 mg154 122 106 90 80 40 10 Placebo
Time from treatment start (months)
Pulido T et al. N Engl J Med 2013;369:809-18

SERAPHIN – Patient characteristics
All patientsn = 742
Placebon = 250
Macitentan 3 mg n = 250
Macitentan 10 mg n = 242
Female sex, % 77 74 75 80
Age, years, mean ± SD 45.6 ± 16.1 46.7 ± 17.0 44.5 ± 16.3 45.5 ± 15.0
6-MWD, m, mean ± SD 360 ± 100 352 ± 111 364 ± 96 363 ± 93
PVR, dyn.sec/cm5 1026 ± 696.7 996 ± 784.3 1044 ± 624.2 1040 ± 672.5
WHO FC, %
I/II
III/IV
53
47
52
48
56
44
50
50
Background PAH therapy, %
PDE-5 inhibitors
Oral/inhaled prostanoids
64
61
5
62
60
3
66
62
7
64
62
6
Pulido T et al. N Engl J Med 2013;369:809-18

SERAPHIN – primary endpoint
Pulido T et al. N Engl J Med 2013;369:809-18
Time to 1st morbidity
or mortality
event
Death
Atrial septostomy
Lung transplantation
Initiation of i.v. or s.c. prostanoids
OR
OR
OR
OROther worsening
of PAH
All events adjudicated by a blinded
clinical events
committee
A decrease in 6-MWD of at least 15%, confirmed by 2 tests on different days
Worsening of PAH symptoms, which must include either:• An increase in FC, or • Appearance or worsening of
symptoms of RHF
Need for new PAH treatment(s):• Oral or inhaled prostanoids• Oral PDE-5 inhibitors• ERA after study
discontinuation• Intravenous diuretics
AND
AND
Other worsening of PAH
OR

Conclusions from SERAPHIN
Patients with PAH presenting in FC II/III benefit from macitentan, regardless of them being treatment-naïve or pre-treated with a PDE5i
Monotherapy with PDE5i may no longer be appropriate for patients with PAH

Up-front or sequential?

AMBITION – Objective
“The primary objective of this study is to compare thedifference between two treatment strategies;
first-line combination therapy (with ambrisentan 10mg od and tadalafil 40mg od) vs. monotherapy (with ambrisentan 10 mg od or tadalafil 40 mg od) in subjects with PAH.
This will be assessed by time to first clinical failure(TtCF) event.”

AMBITION – Study design
Combination arm: AMB + TAD
Monotherapy arm: AMB + PBO Group
Randomized 2:1:1 to Combination arm or Monotherapy arm
Monotherapy arm: TAD + PBO Group
105 events in PAS:
primary endpoint
PAH Patients
N = 610
(n=500 PAS)
OR
AMB: ambrisentan
TAD: tadalafil
PBO: placebo

AMBITION – Primary endpoint („time to clinical failure“) Adapted to reflect current clinical practice
Time to clinical failure is defined as the time from randomization to the first occurrence of: Death (all-cause) Hospitalization for worsening PAH (adjudicated)
Non-elective hospitalization for worsening PAH Lung or heart/lung transplant Atrial septostomy Initiation of parenteral prostanoid therapy
Disease progression (adjudicated) >15% decrease from baseline in 6MWD combined with WHO class III or IV
symptoms (at two consecutive post-baseline clinic visits separated by ≥14 days) Unsatisfactory long-term clinical response (adjudicated, all criteria required)
Receiving randomized treatment for at least 6 months A decrease from baseline in 6MWD at two consecutive post-baseline clinic visits
separated by ≥14 days Sustained WHO class III or IV symptoms for ≥6 months
These events trigger combination therapy according to the goal-oriented approach recommended in
current guidelines
The monotherapy arms in AMBITION represent standard of care, i.e. sequential
combination therapy if treatment goals are not met

GSK Press release 08.09.2014

AMBITION – adverse events
Combination therapy
Ambrisentan monotherapy
Tadalafil monotherapy
Peripheral edema 46% 33% 28%
Headache 42% 33% 35%
Nasal congestion 21% 15% 12%
Anemia 15% 6% 12%
GSK, press release 29.08.2014

The implications of SERAPHIN and AMBITION
Combination therapy with an ERA and a PDE-5i is probably going to become standard of care for patients with newly diagnosed PAH presenting in functional class II or III
Evidence to support this concept has been generated by both the SERAPHIN and AMBITION study
Both trials suggest that the concept of goal-oriented therapy may no longer valid for the initial PAH therapy (but continues to be relevant for further treatment decisions)

Are all drugs the same?
ERA

Macitentan reduced the number of morbidity/mortality events
Pulido T et al. N Engl J Med 2013;369:809-18
Months
HR 0.7, p=0.01HR 0.55, p<0.001
6MWD 10 mg vs placebo +22 m (p=0.008)

GSK Press release 08.09.2014
Ambrisentan + Tadalafil provides better long-term results than Tadalafil monotherapy

COMPASS-II: Adding bosentan to sildenafil did not improve outcome
www.clinicaltrials.gov

Sildenafil plasma concentrations are reduced by bosentan therapy
Paul GA et al. Br J Pharmacol 2005;60:107-12
X
Sildenafil 100 mg alone
4 weeks bosentan 62.5 mg bid
4 weeks bosentan 125 mg bid
Sildenafil AUC dropped by 69% when bosentanwas co-administered at 125 mg bid for 4 weeks

Which ERAs will be used in the future?
Long-term efficacy has been demonstrated for ambrisentan (in combination with tadalafil) and macitentan, but not for bosentan
Where available and reimbursed, ambrisentan or macitentan are expected to become the preferred ERAs for treatment-naïve patients
Based on previous studies (BREATHE-I, EARLY), bosentan is still a valuable option when other ERAs are not available/not reimbursed, as well as in bosentan pre-treated patients with a satisfying clinical response

Functional class IV

Sitbon O, et al. Eur Respir J. 2014;43:1691-7
Upfront triple combo therapy: i.v. epoprostenol + bosentan + sildenafil
19 incident (i.e. newly diagnosed) patients with Idiopathic (n=9) or heritable (n=10) PAH
Mean age 39 ± 14 years (18 – 63)
NYHA FC III (n=8) or IV (n=11)
Severe haemodynamics: CI < 2.0 L/min/m2 or PVR > 1000 d.s.cm-5

Upfront triple combination therapy: Effect on haemodynamics
Prospective, observational analysis of idiopathic or heritable PAH patients (n = 19) treated with upfront combination therapy (epoprostenol, bosentan and sildenafil)
Baseline 4-monthLast visit
(32 ± 19 months)
RAP (mmHg) 11.9 ± 5.2 4.9 ± 4.9* 5.2 ± 3.5*
mPAP (mmHg) 65.8 ± 13.7 45.7 ± 14.0* 44.4 ± 13.4*
PCWP (mmHg) 8.4 ± 3.5 6.7 ± 3.2 7.9 ± 2.8
CI (l/min/m2) 1.66 ± 0.35 3.49 ± 0.69* 3.64 ± 0.65*
PVR (d.s.cm-5) 1718 ± 627 564 ± 260* 492 ± 209*
Heart rate (bpm) 92.3 ± 10.7 83.9 ± 9.8* 79.9 ± 13.4*
Mean BP (mmHg) 92.1 ± 12.5 80.1 ± 11.7* 84.9 ± 19.4
SvO2 (%) 51.0 ± 8.5 69.7 ± 5.2* 72.2 ± 4.0*
*p < 0.01 versus baseline n = 18
Sitbon O, et al. Eur Respir J. 2014; Epub ahead of print.

Sitbon O, et al. Eur Respir J. 2014;43:1691-7
Baseline 4 months* Last visit*02468
101214161820
8
1
10
17 18
FC I/II FC III FC IV
Pa
tie
nts
(n
)

Despite lack of robust evidence, up-front triple combination therapy (ERA + PDEi or sGC + IV PCA) may be the best approach to FC IV patients (and FC III patients with severe haemodynamic impairment)
Initial therapy for WHO-FC IV

Conclusions
Up-front or early combination therapy is expected to become standard of care for patients with PAHERA + PDE5i for patients in FC II/IIIERA + PDE5i + IV/SC PCA in FC IV (or severe FC III)
The future role of new drugs such as Riociguat or Selexipag in PAH still needs to be defined
Thank you!