master plan document for the elmira city school … · the elmira city school district health and...
TRANSCRIPT

Master Plan Document for
THE ELMIRA CITY SCHOOL DISTRICT HEALTH AND DENTAL PLAN
(A self-funded group health benefits plan for employees, retirees, and their dependents)
Restatement Effective April 28, 2005

IMPORTANT REMINDERS Enrollment
Failure to report enrollment changes could result in overpayment or denial of benefits. You will be required to reimburse the full amount of any benefit overpayment. Please refer to Section II - Eligibility and Enrollment for details.
You must keep your enrollment information updated. It is important that you immediately notify the Elmira City School District Business Office of the following:
• Change in marital status • Birth of a child or addition of a child • Address change • Student status of child age 19 or older • Enrolled disabled child approaching age 19 • Marriage of your dependent child • Any family member’s death • Other group health plan information, including effective dates of coverage and name and address
of the other group plan(s) • If you or your dependent become eligible for Medicare due to disability, age, or end stage renal
disease. COBRA Continuation of Coverage Written notice of qualifying events must be sent to the Elmira City School District Business Office within 60 days following the event. If written notice is not given within 60 days, COBRA continuation will not be available. Refer to Section II - Eligibility and Enrollment under Continuing Coverage under COBRA for details.

Table of Contents INTRODUCTION ........................................................................................................................................ 1
Plan Identification..................................................................................................................................... 1 Health Claims Administrator .................................................................................................................... 2 Benefit Management Program Administrator........................................................................................... 2
SECTION I – SUMMARY OF BENEFITS ................................................................................................. 3
Summaries of Medical Expense Benefits ................................................................................................. 3 Indemnity.................................................................................................................................................. 3 Network and Out of Network Expenses ................................................................................................... 3 Allowable Fees ......................................................................................................................................... 4
Out of Network Providers .................................................................................................................... 4 Network Providers................................................................................................................................ 4
Network Providers Directory.................................................................................................................... 4 Free Choice of Providers .......................................................................................................................... 4 Maternity Care.......................................................................................................................................... 4 Federal Newborn/Maternity Provision ..................................................................................................... 5 Federal Mastectomy Provision ................................................................................................................. 5
Potential Causes for Benefit Reduction ........................................................................................................ 5 Medicare ................................................................................................................................................... 5
Medicare Effect on Plan Benefits......................................................................................................... 5 Medicare Premiums.............................................................................................................................. 5
Coordination of Benefits Effect on Plan Benefits .................................................................................... 5 Right of Subrogation/Reimbursement ...................................................................................................... 5 Pre-existing Conditions ............................................................................................................................ 6 Schedules of Medical Expense Benefits................................................................................................... 7
SECTION II - ELIGIBILITY AND ENROLLMENT................................................................................ 27 Eligibility for Plan Enrollment.................................................................................................................... 27
Active Employees................................................................................................................................... 27 Retirees ................................................................................................................................................... 28 Active Employees not Eligible ............................................................................................................... 28 Dependents. ............................................................................................................................................ 28
Legal Spouse ...................................................................................................................................... 28 Unmarried Children of Active Employees ......................................................................................... 29
Child Definition ............................................................................................................................. 29 Age Requirements.......................................................................................................................... 29
Persons Not Considered Eligible Dependents for Plan Enrollment ....................................................... 30 Qualified Medical Child Support Orders................................................................................................ 31 Leave of Absence ................................................................................................................................... 31 Survivor Dependents .............................................................................................................................. 31
Enrollment................................................................................................................................................... 32 Individual Coverage ............................................................................................................................... 32 Family Coverage..................................................................................................................................... 32 Enrollment Changes ............................................................................................................................... 33
Effective Dates of Benefits ......................................................................................................................... 33 Employment Waiting Periods................................................................................................................. 33 Employees/Retirees ................................................................................................................................ 33 Dependent General Rules ....................................................................................................................... 34

Special Enrollment Effective Dates........................................................................................................ 34 Adding New Dependents ................................................................................................................... 34 Cancellation of Another Health Plan.................................................................................................. 34
Monthly Participation Contributions .......................................................................................................... 35 End of Coverage ......................................................................................................................................... 35 Extension of Coverage................................................................................................................................ 36
Limited Total Disability Extension ........................................................................................................ 36 Total Disability Extension ...................................................................................................................... 36
Continuing Coverage Under USERRA....................................................................................................... 37 Continuing Coverage Under COBRA......................................................................................................... 37
Qualifying Events ................................................................................................................................... 37 Notification of Qualifying Events .......................................................................................................... 37 COBRA Continuation Periods................................................................................................................ 37 COBRA Election .................................................................................................................................... 44 COBRA Participation Payments............................................................................................................. 44 When Continued Coverage Ends............................................................................................................ 44 COBRA Coverage and Pre-existing Conditions..................................................................................... 44
SECTION III - BENEFIT MANAGEMENT PROGRAM......................................................................... 45 Preadmission Review.................................................................................................................................. 45
Participant Telephone Requirement for Elective/Scheduled Admissions .............................................. 46 Non-compliance Benefit Reduction ....................................................................................................... 46
Concurrent Review ..................................................................................................................................... 46 Medical Case Management ......................................................................................................................... 46 SECTION IV - COVERED SERVICES..................................................................................................... 47 Pre-existing Condition Limitations............................................................................................................. 47
Plan Pre-existing Exclusion.................................................................................................................... 47 Conditions not Considered Pre-existing ................................................................................................. 47 Reduction by Prior Creditable Coverage................................................................................................ 47
Participating Provider Network Program.................................................................................................... 48 Maternity Care ............................................................................................................................................ 48 Federal Mastectomy Provision.................................................................................................................... 49 Alternative Treatment Provision................................................................................................................. 49 Preventive Care (Well or Routine Care) ..................................................................................................... 49
Well Child Care ...................................................................................................................................... 49 Newborn Nursery Care....................................................................................................................... 49 Routine Well Child Care/Immunizations ........................................................................................... 49
Routine Mammography Screening ......................................................................................................... 50 Routine Adult Physicals ......................................................................................................................... 50 Routine Gynecological Examination...................................................................................................... 50
Hospital and Other Facilities....................................................................................................................... 50 Acute Care General Hospital (Hospital)................................................................................................. 50
Inpatient Hospital Expenses ............................................................................................................... 50 Room and Board ............................................................................................................................ 50 Hospital Miscellaneous or Ancillary ............................................................................................. 50 Medical/Surgical Conditions ......................................................................................................... 51 Maternity/Nursery Care ................................................................................................................. 51 Mental Illness or Psychiatric Care ................................................................................................. 51 Substance Abuse Detoxification .................................................................................................... 51

Outpatient Hospital Expenses ............................................................................................................ 52 Preadmission Testing ..................................................................................................................... 52 Emergency Medical Care............................................................................................................... 52 Surgery........................................................................................................................................... 52 Rehabilitative Therapy................................................................................................................... 52 Other Outpatient Hospital Services and Supplies .......................................................................... 53
Birth Center Facility ............................................................................................................................... 53 Ambulatory Surgical Facility ................................................................................................................. 53 Emergency Center or Urgent Care Facility ............................................................................................ 53 Skilled Nursing Facility /Convalescent Facility/Rehabilitation Facility (SNF) ..................................... 53
Inpatient SNF Services....................................................................................................................... 53 Outpatient SNF Services .................................................................................................................... 54
Alcohol/Substance Abuse Facility.......................................................................................................... 54 Inpatient Care ..................................................................................................................................... 54 Outpatient Care .................................................................................................................................. 55
Home Health Care Agency..................................................................................................................... 55 Hospice Care Agency ............................................................................................................................. 55
Other Medical/Surgical Services and Supplies ........................................................................................... 55 Surgeon Expenses................................................................................................................................... 56 Maternity Expenses ................................................................................................................................ 56 Assistant Surgeon ................................................................................................................................... 56 Anesthesia............................................................................................................................................... 56 Inpatient Physician Services. .................................................................................................................. 57 Consultations .......................................................................................................................................... 57 Office, Outpatient, and Home Visits ...................................................................................................... 57 Foot Care and Podiatry Services ............................................................................................................ 57 Outpatient Mental Health Care............................................................................................................... 57 Diagnostic Tests ..................................................................................................................................... 58 Radiation Therapy .................................................................................................................................. 58 Private Duty Nursing/Visiting Nurse ..................................................................................................... 58 Rehabilitation Therapy ........................................................................................................................... 58
Physical Therapy................................................................................................................................ 58 Speech Therapy .................................................................................................................................. 59 Inhalation Therapy ............................................................................................................................. 59
Chemotherapy......................................................................................................................................... 59 Kidney Dialysis ...................................................................................................................................... 59 Ambulance.............................................................................................................................................. 60 Durable Medical Equipment (DME) ...................................................................................................... 60 Prosthetics/Orthotics/Braces................................................................................................................... 60 Medical Supplies (Home Use)................................................................................................................ 61 Blood Services........................................................................................................................................ 61 Contact Lens or Eyeglasses Following Intraocular Surgery................................................................... 61 Oxygen and its Administration............................................................................................................... 61 Diabetic Supplies, Equipment and Education ........................................................................................ 61
Miscellaneous Covered Expense Provisions............................................................................................... 62 Voluntary or Elective Sterilization ......................................................................................................... 62 Transplants/Organ/Autologous Bone Marrow/Stem Cell....................................................................... 62 Dental Care ............................................................................................................................................. 63 Infertility Treatment ............................................................................................................................... 63 Chiropractic Services.............................................................................................................................. 63

Vision Care ............................................................................................................................................. 63 Wigs........................................................................................................................................................ 64 Prescription Drug Expenses.................................................................................................................... 64
Prescription Drug Expense Benefits ........................................................................................................... 64 Covered Prescription Drug Expenses ..................................................................................................... 64 Prior Authorization ................................................................................................................................. 64 Generic Drug Substitution Program ....................................................................................................... 64 Network Pharmacy ................................................................................................................................. 65
Copayments........................................................................................................................................ 65 Plan Identification Card ..................................................................................................................... 65 Obtaining Network Pharmacy Drugs ................................................................................................. 65
Out-of-Network Pharmacy ..................................................................................................................... 65 Mail Service for Maintenance Drugs...................................................................................................... 65
Mail Service Copayment .................................................................................................................... 65 How to Use the Mail Service Pharmacy Program.............................................................................. 65
Prescription Drug Expense Exclusions................................................................................................... 66 Dental Expense Benefits ............................................................................................................................. 67
Option A Schedule of Dental Allowances.............................................................................................. 67 Option B Schedule of Dental Allowances .............................................................................................. 76 Benefits After Termination..................................................................................................................... 76 Dental Exclusions ................................................................................................................................... 76
SECTION V- PLAN EXCLUSIONS ......................................................................................................... 77 SECTION VI - MEDICARE INTEGRATION WITH PLAN BENEFITS ................................................ 83 Medicare Secondary Payer (MSP) Current Rules....................................................................................... 83
Persons Eligible for Medicare due to Age (65 and over) ....................................................................... 83 Persons Eligible for Medicare due to Disability..................................................................................... 84 Persons Eligible for Medicare due to End Stage Renal Disease (ESRD)............................................... 84
Effects of Medicare on Plan Benefits ......................................................................................................... 85 Medicare Payment Integration................................................................................................................ 85 Not enrolled in Medicare........................................................................................................................ 85 Medicare Private Contract Options ........................................................................................................ 85
Allowable Fees............................................................................................................................................ 85 Medicare Premiums............................................................................................................................ 86
SECTION VII - COORDINATION OF BENEFITS (COB)...................................................................... 86 COB Terms and Definitions ....................................................................................................................... 86 Order of Benefit Determination .................................................................................................................. 88
Non-Dependent or Dependent ................................................................................................................ 88 Child Covered under More than One Plan ............................................................................................. 88 Active/Inactive Employee ...................................................................................................................... 88 Continuation Coverage ........................................................................................................................... 89
Medicare Effect on the Order of Benefit Determination............................................................................. 89 COB Effect on Plan Benefits ...................................................................................................................... 89 Right to Receive and Release Needed Information .................................................................................... 91 Facility of Payment ..................................................................................................................................... 91 Right of Recovery ....................................................................................................................................... 91 Examples of COB Order of Benefits .......................................................................................................... 91

SECTION VIII - CLAIM SUBMISSION AND REVIEW PROCEDURES.............................................. 93 How to Submit a Claim............................................................................................................................... 93
Network Claims (Participating Providers).............................................................................................. 93 Hospital Inpatient or Outpatient Claims ................................................................................................. 93 Other Claim Submissions ....................................................................................................................... 93
Time Limit on Claim Submission ............................................................................................................... 94 Payment of Benefits/Authorization to Pay Provider................................................................................... 94 Your Right to Benefits ................................................................................................................................ 94 Health Claim Inquiries ................................................................................................................................ 95 Claim Appeals Procedure............................................................................................................................ 95 Legal Proceedings....................................................................................................................................... 95 SECTION IX - OTHER PROCEDURES AND PROVISIONS................................................................. 96 Not a Contract ............................................................................................................................................. 96 Verification of Claim Information .............................................................................................................. 96 Workers’ Compensation ............................................................................................................................. 96 Indemnity Benefits...................................................................................................................................... 96 Misrepresentation/Fraud ............................................................................................................................. 96 Refund Due to Overpayment of Benefits.................................................................................................... 96 Right of Subrogation/Reimbursement ........................................................................................................ 97
Conditional Benefit Payment.................................................................................................................. 97 Subrogation Agreement .......................................................................................................................... 97
Amendments or Termination of the Plan .................................................................................................... 98 Named Fiduciary and Plan Administrator .................................................................................................. 98 Severability ................................................................................................................................................. 98 Waiver and Estoppel ................................................................................................................................... 98 Headings ..................................................................................................................................................... 99 Federal and State Laws ............................................................................................................................... 99 SECTION X - DEFINITIONS.................................................................................................................... 99 APPENDIX A - Elmira Area Zip Code List ............................................................................................. 111 APPENDIX B - Elmira Area Benefit Clarifications................................................................................. 112 APPENDIX C – Privacy Addendum ........................................................................................................ 115

Elmira CSD – rev. 04/28/05 1
INTRODUCTION
This is the Master Plan Document (MPD) for the Elmira City School District’s Self-Insured Health and Dental Plan (“Plan”). You should carefully read this document to acquaint yourself with its provisions for eligibility, benefit coverage, filing a claim and other important information.
Plan Identification
Plan Name: Elmira City School District Health and Dental Plan Plan Administrator: Elmira City School District, 951 Hoffman St., Elmira, NY 14905 Tel 607-735-3000 Plan Sponsor: Elmira City School District, 951 Hoffman St., Elmira, NY 14905 Tel 607-735-3000 Plan Effective Date: July 1, 2001 Plan Restatement Date: April 28, 2005 Plan Year: Twelve consecutive months beginning July 1 and ending June 30 Type of Plan: This is a self-funded health plan providing benefits for certain medical,
dental, and vision expenses. Plan funding is provided by the Elmira City School District and participation Contributions by Enrollees.
Claims Administrator: POMCO, 2425 James Street, P.O. Box 6329, Syracuse, New York 13217-6329; Tel.: toll-free 1-866-317-7386
Please Note
The pronoun you or your means an eligible and enrolled Employee or Retiree of the Elmira City School District. It also means a COBRA participant whose Social Security number is used for Plan enrollment. Terms throughout this MPD have been capitalized and are defined in Section X - Definitions to help you understand your Plan coverage and benefits. This MPD updates and replaces previous publications showing coverage for the self-funded Plan formerly known as the Elmira City School District Employee Health Benefit Plan. It is a restatement of Plan benefits showing provisions and benefits in effect as of April 28, 2005. Please note that the Indemnity Plan Option and Option A are closed to new enrollees; Plan Option B is accepting new enrollees. Option A may be open to individuals prior to January 2, 2003; consult your collective bargaining agreement. The Elmira City School District (“District”) has designed a plan that provides benefits for a broad range of healthcare services. A number of features have been included in the Plan to manage costs for both you and your employer and to ensure that the health care you receive is within Plan guidelines. This MPD is written in the English language to show your rights and coverage under the Plan. If you do not understand any part of this MPD, the Business Office will provide you with further information and discuss any questions you may have. Only the Plan Administrator is authorized to explain your rights and obligations under the Plan. In no event should you rely on any statements concerning your rights and obligations under the Plan from anyone other than the Plan Administrator. You may also contact the Claim Administrator (POMCO) for assistance on benefits. The Master Plan Document (MPD) of the Elmira City School District Health and Dental Plan consists of the Summary, the terms of the Plan, and any Amendments to the Plan and is maintained and on file with the Plan Administrator. The provisions of this Plan may only be determined accurately by reading the Master Plan Document. To the extent the Summary or other plan information is inconsistent with the provisions of the Master Plan Document, the terms of the Master Plan Document will govern. The Master Plan Document is available for your inspection during regular working hours at the Elmira City School District Business Office. You may

Elmira CSD – rev. 04/28/05 2
also request the Plan Administrator to give you an additional copy of the Master Plan Document for a minimal charge. This MPD and the benefits shown are subject to change in accordance with the collective bargaining process. It is understood that the provision of all professional services are the sole responsibility of the specific health care provider and that the District and the Claims Administrator have no responsibility or liability whatsoever to persons who are Enrollees or participants in this Plan with respect to the provision of any professional services.
A. Health Claims Administrator POMCO administers your medical, dental, and vision expense benefits. Claims should be sent directly to POMCO for benefit determination. If you have any questions or concerns about your coverage, you can phone POMCO or the District Business Office. Claim forms can be obtained from the POMCO website (www.benefitsoft.com), the District’s Business Office or from the School Main Offices. Refer to Section VIII - Claim Submission and Review Procedures for details on submitting your claims.
POMCO P.O. Box 6329
Syracuse, NY 13217 Toll-free 1-866-317-7386
B. Benefit Management Program Administrator
POMCO administers the Benefit Management Program. Please refer to Section III - Benefit Management Program for full details of this program’s requirements. It is recommended to phone the POMCO Benefit Management Unit before certain medical procedures are rendered for you or your Dependents. A phone call is required before scheduled inpatient admissions to a Hospital or other inpatient facility, or within 72 hours after an emergency or urgent admission; when maternity stays exceed 72 hours after normal delivery or 96 hours after caesarean section; when Newborn care exceeds 96 hours after birth.
POMCO Benefit Management Unit Phone Toll-free 1-866-317-7386
This is a 24-hour service. If you wish to talk to the POMCO nurses, you must call between 8:00 a.m. and 4:30 p.m. during normal business days. Otherwise, please provide complete information as requested by the voice mail recording.

Elmira CSD – rev. 04/28/05 3
SECTION I – SUMMARY OF BENEFITS
The information in this section shows the benefits for medical, dental, and vision expenses Covered by the Plan. However, Plan payment is based on all the terms and limitations of the Plan. Please read this entire MPD to find out the full details for Plan coverage, limitations and exclusions. Please refer to page 27 Section II - Eligibility and Enrollment for details on Plan enrollment, eligibility and Effective Dates for Plan coverage. (Please note that the Indemnity Plan Option is not accepting new enrollees.) For detailed Covered service descriptions, please refer to page 47 Section IV - Covered Services, page 77 Section V - Plan Exclusions, and page 98 Section X - Definitions.
Please Note All claims are subject to review to determine whether services are Covered according to Plan limitations. You must comply with requests for additional medical documentation as reasonably necessary to evaluate a claim for benefits. Failure to submit requested documentation or information could result in denial of benefits. The Claims Administrator maintains all medical documents. Treatment decisions are independent from payment decisions. The patient's Physician is responsible for determining whether treatment should be given no matter whether the charges are totally or partially included in, or excluded from, coverage under this Plan. Benefits are determined based on the date the expenses were incurred, not the date the claims were submitted. Incurred means the date services were rendered, not the date of the bill. Payment for services rendered by an Immediate Relative are excluded from coverage.
A. Summaries of Medical Expense Benefits 1. Indemnity. You or your dependents may choose to receive medical care from any licensed health care
provider. 2. Network and Out of Network Expenses for Option A and Option B. The health plan benefits to
which you are entitled are based upon whether the service provider you use is considered to be “In” or “Out” of Network. This is determined as follows:
Option A
Determining whether a licensed health care provider is an “In” Network Provider is based upon where your legal residence is located and where provider services are received.
1. If your legal residence is within a twenty-eight (28) mile radius of the Elmira City School District
Board of Education offices, a licensed health care provider is considered “In” Network if the services provided are within this twenty-eight (28) mile radius. A licensed health care provider outside this twenty-eight (28) mile radius will only be considered an “In” Network Provider if you have been referred to the provider by a licensed health care provider who is “In” Network (the benefit for the referral is paid at 100% of reasonable and customary charges).
2. If your legal residence is not within a twenty-eight (28) mile radius of the Elmira City School District
Board of Education offices, any licensed health care provider is considered “In” Network.
Option B
Determining whether a licensed health care provider is an “In” Network Provider is based upon where your legal residence is located and if the licensed health care provider who provides the services is designated by the Elmira City School District Self Insured Health Plan as a “Preferred Provider”.

Elmira CSD – rev. 04/28/05 4
1. If your legal residence is within a twenty-eight (28) mile radius of the Elmira City School District
Board of Education offices, a licensed health care provider is considered “In” Network if the services provided are provided by a “Preferred Provider”. A licensed health care provider outside this twenty-eight (28) mile radius will only be considered “In” Network if the service can not be provided by Preferred Provider within the twenty-eight (28) mile radius of the Elmira City School District Board of Education offices.
2. If your legal residence is not within a twenty-eight (28) mile radius of the Elmira City School
District Board of Education offices, any licensed health care provider not within the twenty-eight (28) mile radius of the Elmira City School District Board of Education offices is “In” Network (the benefit is paid at 100% of reasonable and customary charges). Inside the twenty-eight (28) mile radius, only licensed health care providers designated as “Preferred Providers” are consider “In” Network.
Option A and Option B Out-of-Area Exception
While traveling away from the Plan’s service area, benefits will be paid at 100% of reasonable and customary. This exception does not apply to pre-arranged procedures outside the twenty-eight (28) mile radius of the Elmira City School District Board of Education offices.
3. Allowable Fees.
a. Out of Network Providers. Allowable Fees mean the usual, customary and reasonable (UCR) charges for covered medical services or supplies rendered and billed by a covered nonparticipating (Out of Network) provider. If you or your dependents use Out of Network Providers, you will be responsible for the payment of charges that are more than the UCR allowance, if any, plus percentage copayment balance amounts.
b. Network Providers. Allowable Fees mean the negotiated or scheduled network allowance for
covered medical services or supplies rendered and billed by Network Providers. The Network Provider has an agreement with the Claims Administrator to bill for covered services and supplies according to the Network schedule of allowances. The Plan will pay the available Network benefits directly to the Network Provider. If you or your eligible dependents use a Network Provider for covered services or supplies, you will be responsible for the Network percentage copayment balance. As the Network allowance is generally lower than the UCR allowance, choosing a Network Provider for medical care can result in cost savings for you and the Plan.
4. Network Providers Directory. Copies of the directory of local Network Providers may be obtained
from the District’s Business Office or you may call POMCO for information on providers near you. You may also find network directories on the District’s website.
5. Free Choice of Providers. You or your dependents may seek medical care from any Healthcare
provider. Covered expenses will be dependent on the coverage you have with the Plan options. Unless specifically shown otherwise, this Plan covers medical expenses and hospital admissions in the
same manner for both Network and Out of Network providers, whether or not the medical condition is an emergency. This Plan does not require that you use a member hospital for your care.
6. Maternity Care. Maternity or pregnancy care is covered the same as any other illness for employees and
dependent spouses including, but not limited to, childbirth and other termination of pregnancy. The Plan excludes elective abortions. Maternity coverage is not available for dependent children. The Plan excludes services and supplies related to surrogate pregnancies.

Elmira CSD – rev. 04/28/05 5
7. Federal Newborn/Maternity Provision. According to the Newborns' & Mothers' Health Protection Act,
a federal law, a health plan, or its managed care program, that offers coverage for Hospital stays in connection with childbirth cannot limit that coverage to less than a 48-hour Hospital stay following an uncomplicated normal delivery; or less than a 96-hour Hospital stay following a Caesarean section delivery. In addition, the health plan cannot restrict benefits for any portion of the required minimum stays in a way that is less favorable than the benefits provided for any preceding portion of the stay. Under Section III - Benefit Management Program, this Plan requires notification of a Hospital length of stay that follows the first 72 hours after a normal delivery or 96 hours after a cesarean section.
8. Federal Mastectomy Provision. On October 21, 1998, the Women’s Health and Cancer Rights Act
requires group health plans providing medical and surgical benefits with respect to a mastectomy to provide the following coverage to a plan participant who elects breast reconstruction in connection with the mastectomy: a. Reconstruction of the breast on which the covered mastectomy has been performed. b. Surgery or reconstruction of the other breast to produce symmetrical appearance; and c. Coverage for prostheses and physical complications of all stages of a covered mastectomy, including
lymphedemas; d. Coverage to be provided in a manner determined in consultation with the attending Physician and the
patient. 9. Potential Causes for Benefit Reduction. a. Medicare. 1) Medicare Effect on Plan Benefits. Your Plan benefits could be reduced by Medicare payments,
if Medicare is considered primary coverage according to Medicare secondary payer rules. This reduction will apply whether or not the person eligible for Medicare is actually enrolled in Medicare. Refer to Section VI - Medicare Integration with Plan Benefits. You or your Dependent should enroll for Medicare upon eligibility or when Medicare is considered the primary coverage. Failure to enroll in Medicare when Medicare is primary could result in significant reduction or denial of your health benefits. You could be responsible for the payment of all or most of your health expenses.
For this Plan to be the secondary payor of benefits, retirees of ISEA must enroll for Medicare. 2) Medicare Premiums. If this Plan is the secondary payor, the Participant is entitled to
reimbursement of Medicare Part B premiums, in accordance with the applicable collective bargaining agreement, as modified. You must present your Medicare card to the District Business Office in order to verify Part B enrollment. Part B premium reimbursement only begins after you notify the Business Office and provide Part B enrollment verification; reimbursement is not retroactive.
b. Coordination of Benefits Effect on Plan Benefits. Your benefits under this Plan could be reduced if
you or your Dependents are Covered by more than one healthcare plan. Refer to Section VII - Coordination of Benefits.
c. Right of Subrogation/Reimbursement. This Plan specifically does not give benefits with respect to
any Injury or Illness for which a third party may be liable or legally responsible. If you or your Dependents receive payment or are entitled to payment from a third party insurance, surety or other type plan resulting from such Injury or Illness, you should not submit a claim under this Plan. The Plan will be entitled to full reimbursement of any Plan payments for medical expenses that are or should have been paid by the third party coverage. For full details, refer to Section IX - Other Procedures and Provisions under Right of Subrogation/Reimbursement.

Elmira CSD – rev. 04/28/05 6
d. Pre-existing Conditions. The Plan pre-existing condition rules apply to newly enrolled persons.
However, the duration that pre-existing conditions could affect Plan benefits will be based on previous health coverages. Please refer to Section IV - Covered Services under Pre-existing Conditions for details.
Elmira CSD – rev. 04/28/05 7
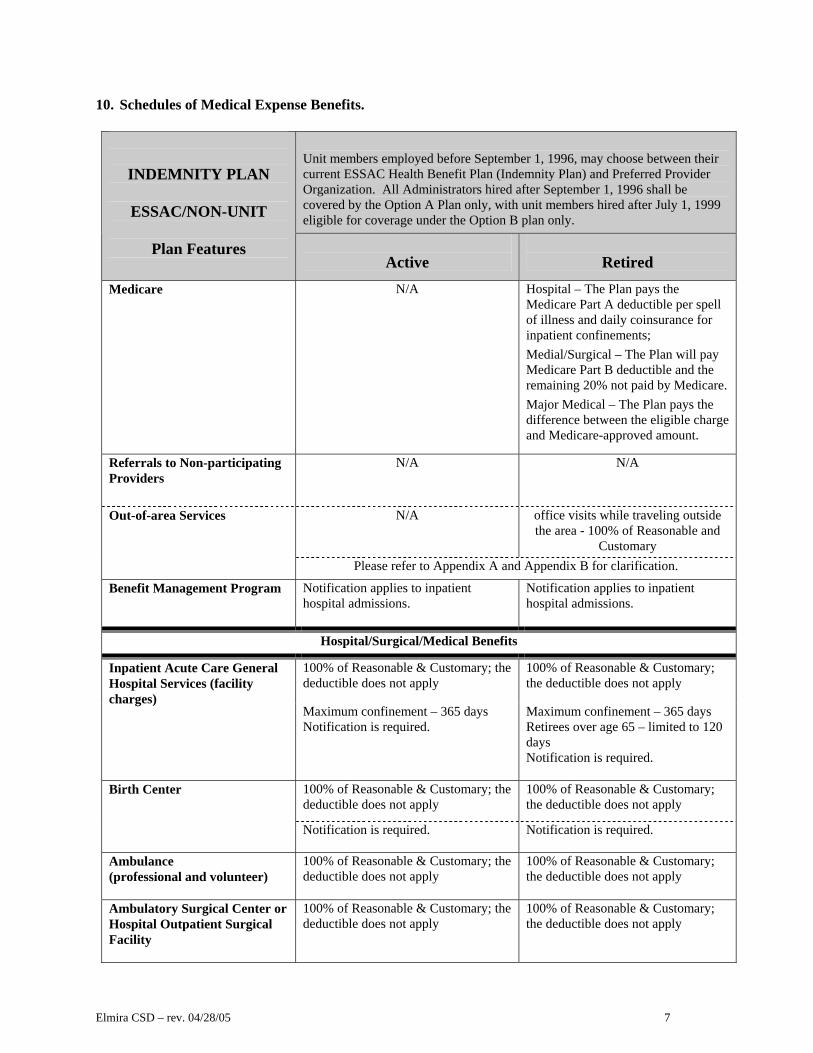
10. Schedules of Medical Expense Benefits.
Unit members employed before September 1, 1996, may choose between their current ESSAC Health Benefit Plan (Indemnity Plan) and Preferred Provider Organization. All Administrators hired after September 1, 1996 shall be covered by the Option A Plan only, with unit members hired after July 1, 1999 eligible for coverage under the Option B plan only.
INDEMNITY PLAN
ESSAC/NON-UNIT
Plan Features
Active
Retired
Medicare
N/A Hospital – The Plan pays the Medicare Part A deductible per spell of illness and daily coinsurance for inpatient confinements; Medial/Surgical – The Plan will pay Medicare Part B deductible and the remaining 20% not paid by Medicare. Major Medical – The Plan pays the difference between the eligible charge and Medicare-approved amount.
Referrals to Non-participating Providers
N/A N/A
N/A office visits while traveling outside the area - 100% of Reasonable and
Customary
Out-of-area Services
Please refer to Appendix A and Appendix B for clarification.
Benefit Management Program
Notification applies to inpatient hospital admissions.
Notification applies to inpatient hospital admissions.
Hospital/Surgical/Medical Benefits
100% of Reasonable & Customary; the deductible does not apply
100% of Reasonable & Customary; the deductible does not apply
Inpatient Acute Care General Hospital Services (facility charges)
Maximum confinement – 365 days Notification is required.
Maximum confinement – 365 days Retirees over age 65 – limited to 120 days Notification is required.
100% of Reasonable & Customary; the deductible does not apply
100% of Reasonable & Customary; the deductible does not apply
Birth Center
Notification is required. Notification is required.
Ambulance (professional and volunteer)
100% of Reasonable & Customary; the deductible does not apply
100% of Reasonable & Customary; the deductible does not apply
Ambulatory Surgical Center or Hospital Outpatient Surgical Facility
100% of Reasonable & Customary; the deductible does not apply
100% of Reasonable & Customary; the deductible does not apply

Elmira CSD – rev. 04/28/05 8
Unit members employed before September 1, 1996, may choose between their current ESSAC Health Benefit Plan (Indemnity Plan) and Preferred Provider Organization. All Administrators hired after September 1, 1996 shall be covered by the Option A Plan only, with unit members hired after July 1, 1999 eligible for coverage under the Option B plan only.
INDEMNITY PLAN
ESSAC/NON-UNIT
Plan Features
Active
Retired
100% of Reasonable & Customary; the deductible does not apply
100% of Reasonable & Customary; the deductible does not apply
Inpatient Mental Health (Hospital or private proprietary psychiatric facility charge)
Maximum confinement – 365 days Notification is required.
Maximum confinement – 365 days Retirees over age 65 – limited to 120 days Notification is required.
Inpatient Alcohol/Substance Abuse (certified facility charge)
100% of Reasonable & Customary; the deductible does not apply limited to 7 weeks Notification is required.
100% of Reasonable & Customary; the deductible does not apply limited to 7 weeks Notification is required.
Skilled Nursing or Rehabilitation Facility – Inpatient (custodial care is not covered)
100% of Reasonable and Customary; the deductible does not apply. Maximum confinement 365 days
100% of Reasonable and Customary; the deductible does not apply. Maximum confinement 365 days
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Home Health Care
40 days per year (approved on a case-by-case basis by Claims Administrator). Additional visits are Covered under Major Medical.
40 days per year (approved on a case-by-case basis by Claims Administrator). Additional visits are Covered under Major Medical.
Hospice (Claims Administrator’s guidelines apply, page 55)
100% of Reasonable and Customary; the deductible does not apply; 210 days
100% of Reasonable and Customary; the deductible does not apply; 210 days
Outpatient Treatment Alcohol/Substance Abuse - Physician Care
100% of Reasonable and Customary; the deductible does not apply limited to 30 visits per year 2-year maximum for out-patient care
100% of Reasonable and Customary; the deductible does not apply limited to 30 visits per year 2-year maximum for out-patient care
Outpatient Treatment Mental Health – Physician Care (includes certified psychiatric social worker)
100% of Reasonable and Customary; the deductible does not apply Limited to 30 visits per year
100% of Reasonable and Customary; the deductible does not apply Limited to 30 visits per year

Elmira CSD – rev. 04/28/05 9
Unit members employed before September 1, 1996, may choose between their current ESSAC Health Benefit Plan (Indemnity Plan) and Preferred Provider Organization. All Administrators hired after September 1, 1996 shall be covered by the Option A Plan only, with unit members hired after July 1, 1999 eligible for coverage under the Option B plan only.
INDEMNITY PLAN
ESSAC/NON-UNIT
Plan Features
Active
Retired
Emergency Center or Urgent Care Facility (facility charge)
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Emergency Center or Urgent Care Center Physician (separate charge)
100% of Reasonable and Customary the deductible does not apply
100% of Reasonable and Customary the deductible does not apply
Services must be rendered within 12 hours of a medical emergency or 24 hours of an accidental injury. Emergency center services received outside these time limits are not covered.
Non-emergency care rendered in an Emergency Center: the facility charge and separate physician’s charge are not covered; diagnostic testing and medications are covered.
Physician Surgery-Related Services:
• Surgery and Maternity Care
100% of the Relative Value Schedule (RVS); the deductible does not apply
100% of the Relative Value Schedule (RVS); the deductible does not apply
• Assistant Surgeon 20% of surgeon’s RVS; the deductible does not apply
20% of surgeon’s RVS; the deductible does not apply
• Anesthesia 100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Inpatient Physician Services
100% of Reasonable & Customary; the deductible does not apply
100% of Reasonable & Customary; the deductible does not apply
Preadmission Testing and Interpretation (within 7 days of admission)
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Outpatient Hospital Diagnostic X-ray, Laboratory, and Machine Testing and interpretation
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Outpatient Hospital Physical and Occupational Therapy
100% of Reasonable and Customary; the deductible does not apply; physical therapy must follow hospitalization
100% of Reasonable and Customary; the deductible does not apply; physical therapy must follow hospitalization
Outpatient Hospital Speech Therapy
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Cardiac Rehabilitation (outpatient or facility)
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply

Elmira CSD – rev. 04/28/05 10
Unit members employed before September 1, 1996, may choose between their current ESSAC Health Benefit Plan (Indemnity Plan) and Preferred Provider Organization. All Administrators hired after September 1, 1996 shall be covered by the Option A Plan only, with unit members hired after July 1, 1999 eligible for coverage under the Option B plan only.
INDEMNITY PLAN
ESSAC/NON-UNIT
Plan Features
Active
Retired
Outpatient Hospital Inhalation or Respiratory Therapy and IV Therapy
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Radiation Therapy and Chemotherapy
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Dialysis 100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Physician Services – Office or clinic visit (non-routine)
100% of Reasonable & Customary; the deductible does not apply
100% of Reasonable & Customary; the deductible does not apply office visits while traveling outside- 100% of Reasonable and Customary
Consultations 100% of Reasonable and Customary; deductible does not apply
100% of Reasonable and Customary; deductible does not apply
Diagnostic X –Rays and interpretation
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Diagnostic Laboratory and interpretation
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Elective Sterilization
100% of the Relative Value Schedule (RVS); the deductible does not apply
100% of the Relative Value Schedule (RVS); the deductible does not apply
Well Child Care and Immunizations (for routine in-hospital care at birth and for the first 24 months from birth)
100% of Reasonable & Customary; deductible does not apply Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
100% of Reasonable & Customary; deductible does not apply Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
Adult Routine Physical and Tests Employees and retirees age 50 years and older Limited to one per calendar year Immunizations are not covered
100% of Reasonable and Customary the deductible does not apply
100% of Reasonable and Customary the deductible does not apply
Routine Mammography Screening 35 years and older- One per year
100% of Reasonable and Customary the deductible does not apply
100% of Reasonable and Customary the deductible does not apply
Organ Transplants See Section IV, subsection I, paragraph 2.
See Section IV, subsection I, paragraph 2.

Elmira CSD – rev. 04/28/05 11
Unit members employed before September 1, 1996, may choose between their current ESSAC Health Benefit Plan (Indemnity Plan) and Preferred Provider Organization. All Administrators hired after September 1, 1996 shall be covered by the Option A Plan only, with unit members hired after July 1, 1999 eligible for coverage under the Option B plan only.
INDEMNITY PLAN
ESSAC/NON-UNIT
Plan Features
Active
Retired
Vision Care 100% of Reasonable and Customary: One exam per year for those employees assigned to work with computers on a regular basis; the deductible does not apply
Not covered
Major Medical Benefits
Major Medical Deductible Calendar Year
$150 per individual $300 per Family
$150 per individual $300 per Family
Common Accident Deductible Yes Yes Carry-over Deductible Yes Yes
Percentage Coinsurance 80% of covered charges up to $4,000 after annual deductible is met, 100% thereafter
80% of covered charges up to $4,000 after annual deductible is met, 100% thereafter
Copayments N/A
N/A
Out of Pocket Maximum Per Person for Covered Major Medical Expenses
$800 (does not include deductible) $800 (does not include deductible)
Lifetime Maximum
$1,000,000 $1,000,000
Allergy Treatment 80% coinsurance after deductible 80% coinsurance after deductible
Physical and Occupational Therapy Private Practitioner
80% coinsurance after deductible
80% coinsurance after deductible
Speech Therapy Private Practitioner
80% coinsurance after deductible
80% coinsurance after deductible
Home Health Care 80% coinsurance after deductible for up to 325 days if approved by Claims Administrator
80% coinsurance after deductible for up to 325 days if approved by Claims Administrator
Routine Annual Gyn Exam (employees, retirees, and spouses) Pap smear and tests related to the exam are covered under Diagnostic Laboratory and X-ray benefits
80% coinsurance after deductible 80% coinsurance after deductible
Private Duty Nursing (R.N. only)
80% coinsurance after deductible
80% coinsurance after deductible

Elmira CSD – rev. 04/28/05 12
Unit members employed before September 1, 1996, may choose between their current ESSAC Health Benefit Plan (Indemnity Plan) and Preferred Provider Organization. All Administrators hired after September 1, 1996 shall be covered by the Option A Plan only, with unit members hired after July 1, 1999 eligible for coverage under the Option B plan only.
INDEMNITY PLAN
ESSAC/NON-UNIT
Plan Features
Active
Retired
Medical Supplies Diabetic Supplies
80% coinsurance after deductible
80% coinsurance after deductible
Durable Medical Equipment
80% coinsurance after deductible 80% coinsurance after deductible
Oxygen 80% coinsurance after deductible 80% coinsurance after deductible
Prosthetics Orthotics
80% coinsurance after deductible
80% coinsurance after deductible
Blood products, transfusions, plasma, and processing charges
80% coinsurance after deductible 80% coinsurance after deductible
Alternative Treatment (includes chiropractic care, acupuncture, biofeedback)
Care must be preapproved to be paid. See Section IV, subsection E
Care must be preapproved to be paid. See Section IV, subsection E
Participating Retail Pharmacy: Refer to your current collective bargaining agreement or contact the Business Office for applicable copayments.
Prescription Drug Coverage
Non-participating Retail Pharmacy: The Plan reimburses cost minus the copayment up to the amount that would have been paid at a participating pharmacy.
80% of cost after deductible

Elmira CSD – rev. 04/28/05 13
Option A - Active
Option A - Retired
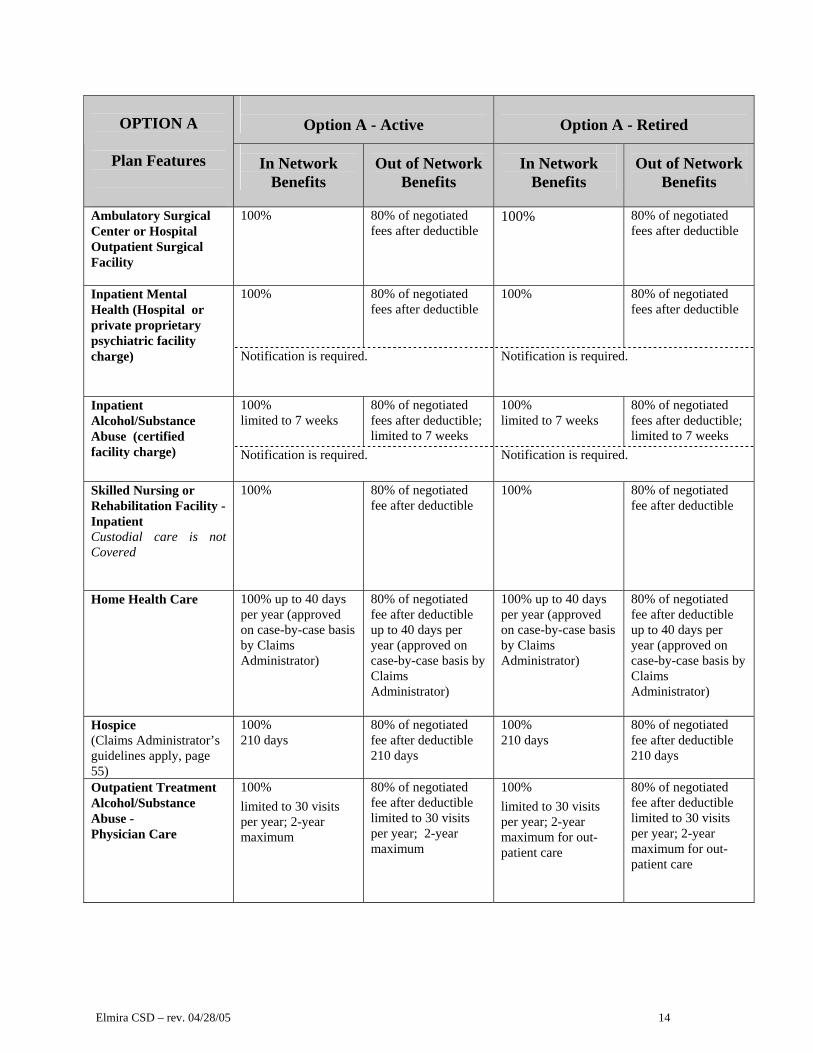
OPTION A
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits
Copayments Refer to current collective bargaining agreement
Refer to current collective bargaining agreement
Refer to collective bargaining agreement in effect at time of retirement
Refer to collective bargaining agreement in effect at time of retirement
Medicare N/A N/A Hospital – The Plan pays the Medicare Part A deductible per spell of illness and daily coinsurance for inpatient confinements; Medial/Surgical – The Plan will pay Medicare Part B deductible and the remaining 20% not paid by Medicare. Major Medical – The Plan pays the difference between the eligible charge and Medicare-approved amount.
Referrals to Non-participating Providers by in-network physicians
100% of negotiated rate, if applicable, or Reasonable and Customary
100% of negotiated rate, if applicable, or Reasonable and Customary
100% of Reasonable and Customary
100% of Reasonable and Customary
100% of Reasonable and Customary
100% of Reasonable and Customary
Out-of-area Services
If you travel outside the Plan’s service area, benefits for Covered services are payable at 100% of the Reasonable and Customary charge. This exception does not apply to pre-arranged procedures outside the Plan’s service area. Please refer to Appendix B using Appendix A for clarification of the Plan’s service area.
Benefit Management Program
Notification applies to inpatient hospital admissions.
Notification applies to inpatient hospital admissions.
Hospital/Surgical /Medical Expense Benefits
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Inpatient Acute Care General Hospital Services (facility charges)
Notification is required. Notification is required.
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Birth Center
Notification is required.
Notification is required.
Ambulance (professional and volunteer)
100% of Reasonable and Customary; deductible does not apply
100% of Reasonable and Customary; deductible does not apply
100% of Reasonable and Customary; deductible does not apply
100% of Reasonable and Customary; deductible does not apply
Elmira CSD – rev. 04/28/05 14
Option A - Active
Option A - Retired
OPTION A
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits
Ambulatory Surgical Center or Hospital Outpatient Surgical Facility
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Inpatient Mental Health (Hospital or private proprietary psychiatric facility charge)
Notification is required. Notification is required.
100% limited to 7 weeks
80% of negotiated fees after deductible; limited to 7 weeks
100% limited to 7 weeks
80% of negotiated fees after deductible; limited to 7 weeks
Inpatient Alcohol/Substance Abuse (certified facility charge)
Notification is required. Notification is required.
Skilled Nursing or Rehabilitation Facility - Inpatient Custodial care is not Covered
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Home Health Care 100% up to 40 days per year (approved on case-by-case basis by Claims Administrator)
80% of negotiated fee after deductible up to 40 days per year (approved on case-by-case basis by Claims Administrator)
100% up to 40 days per year (approved on case-by-case basis by Claims Administrator)
80% of negotiated fee after deductible up to 40 days per year (approved on case-by-case basis by Claims Administrator)
Hospice (Claims Administrator’s guidelines apply, page 55)
100% 210 days
80% of negotiated fee after deductible 210 days
100% 210 days
80% of negotiated fee after deductible 210 days
Outpatient Treatment Alcohol/Substance Abuse - Physician Care
100% limited to 30 visits per year; 2-year maximum
80% of negotiated fee after deductible limited to 30 visits per year; 2-year maximum
100% limited to 30 visits per year; 2-year maximum for out-patient care
80% of negotiated fee after deductible limited to 30 visits per year; 2-year maximum for out-patient care

Elmira CSD – rev. 04/28/05 15
Option A - Active
Option A - Retired
OPTION A
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits
Outpatient Treatment Mental Health – Physician Care (includes certified psychiatric social worker)
100% of Reasonable and Customary Limited to 30 visits per year
80% of negotiated fee after deductible Limited to 30 visits per year
100% of Reasonable and Customary Limited to 30 visits per year
80% of negotiated fee after deductible Limited to 30 visits per year
Emergency Center or Urgent Care Facility (facility charge)
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Emergency Center or Urgent Care Facility Physician (separate charge)
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Services must be rendered within 12 hours of a medical emergency or 24 hours of an accidental injury. Emergency center services received outside these time limits are not covered.
Non-emergency care rendered in an Emergency center: the facility charge and separate physician’s charge are not covered; diagnostic testing and medications are covered.
Physician Surgery-Related Services:
• Surgery and Maternity Care
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
• Assistant Surgeon 100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
• Anesthesia 100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Inpatient Physician Services
100% limited to 7 weeks for alcohol/substance abuse
80% of negotiated fees after deductible; limited to 7 weeks for alcohol/substance abuse
100% limited to 7 weeks for alcohol/substance abuse
80% of negotiated fees after deductible; limited to 7 weeks for alcohol/substance abuse
Preadmission Testing and Interpretation (within 7 days of admission)
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Outpatient Hospital Diagnostic X –Rays, Laboratory, and Machine Testing and interpretation
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible

Elmira CSD – rev. 04/28/05 16
Option A - Active
Option A - Retired
OPTION A
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits
Outpatient Hospital Physical and Occupational Therapy
100%; must follow hospitalization
80% of negotiated fee after deductible; physical therapy must follow hospitalization
100%; must follow hospitalization
80% of negotiated fee after deductible; physical therapy must follow hospitalization
Outpatient Hospital Speech Therapy
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible;
Cardiac Rehabilitation (outpatient or facility)
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Outpatient Hospital Inhalation, Respiratory Therapy, and IV Therapy
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Radiation Therapy and Chemotherapy
100% 80% of negotiated fee after deductible
100%
80% of negotiated fee after deductible
Dialysis 100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
100% after copay 80% of negotiated fees after deductible
100% after copay 80% of negotiated fees after deductible
Physician Services – Office or clinic visit (non-routine)
Refer to your current collective bargaining agreement or contact the Business Office
Refer to your collective bargaining agreement in effect at the time of retirement or contact the Business Office
Consultations 100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Diagnostic X –Rays and Laboratory and interpretation (out of hospital)
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Elective Sterilization
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Well Child Care and Immunizations (for routine in-hospital care at birth and for the first 24 months from birth)
100% Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
80% of negotiated fee after deductible Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
100% Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
80% of negotiated fee after deductible Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age

Elmira CSD – rev. 04/28/05 17
Option A - Active
Option A - Retired
OPTION A
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits
Adult Routine Physical and Tests Employees and Retirees 50 years and older Limited to one per calendar year Immunizations are not covered
100%
80% of negotiated fee after deductible
100%
80% of negotiated fee after deductible
Routine Mammography Screening 35 years and older One per year
100%
80% of negotiated fee after deductible
100%
80% of negotiated fee after deductible
Organ Transplants See Section IV, subsection I, paragraph 2.
See Section IV, subsection I, paragraph 2.
See Section IV, subsection I, paragraph 2.
See Section IV, subsection I, paragraph 2.
100%, subject to copay or benefit limitations
80% of negotiated fee after deductible
Vision Care members of CWA
(one examination and prescription lenses per year)
employees assigned to work with computers on a regular basis (one examination per year)
refer to current collective bargaining agreement for copay or coinsurance percentage and limitations
Not covered
Major Medical Expense Benefits
Major Medical Deductible Calendar Year (a separate deductible applies to in-network and out-of-network charges)
$150 per individual $300 per Family
$150 per individual $300 per Family
$150 per individual $300 per Family
$150 per individual $300 per Family
Common Accident Deductible
Yes Yes
Carry-over Deductible Yes Yes
Percentage Coinsurance (all groups except CWA group described below)
80% of covered charges up to $4,000 after annual deductible is met, 100% thereafter
80% of covered charges until the out-of-pocket maximum is reached after annual deductible is met, 100% thereafter
80% of covered charges up to $4,000 after annual deductible is met, 100% thereafter
80% of covered charges until the out-of-pocket maximum is reached after annual deductible is met, 100% thereafter

Elmira CSD – rev. 04/28/05 18
Option A - Active
Option A - Retired
OPTION A
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits
CWA Active Employees, Retirees, and their Covered Dependents
80% of covered charges up to $5,000 after annual deductible is met, 100% thereafter
80% of covered charges until the out-of-pocket maximum is reached after annual deductible is met, 100% thereafter
80% of covered charges up to $5,000 after annual deductible is met, 100% thereafter
80% of covered charges until the out-of-pocket maximum is reached after annual deductible is met, 100% thereafter
Out of Pocket Maximum Per Person for Covered Major Medical Expenses (all groups except CWA group described below)
$800 (does not include deductible)
$1,600 (does not include deductible) plus 20% of the next $4,000 (total $2400)
$800 (does not include deductible)
$1,600 (does not include deductible) plus 20% of the next $4,000 (total $2400)
CWA Active Employees, Retirees, and their Covered Dependents
$1,000 (does not include deductible)
$1,600 (does not include deductible) plus 20% of the next $4,000 (total $2400)
$1,000 (does not include deductible)
$1,600 (does not include deductible) plus 20% of the next $4,000 (total $2400)
Lifetime Maximum
$1,000,000 $1,000,000
Private Duty Nursing (R.N. only)
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
Physical and Occupational Therapy Private Practitioner
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees deductible
80% of negotiated fees after deductible
Speech Therapy Private Practitioner
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees deductible
80% of negotiated fees after deductible
Allergy Treatment 80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
Medical Supplies Diabetic Supplies
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees
80% of negotiated fees after deductible
Durable Medical Equipment
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
Oxygen 80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
80% of negotiated fees after deductible
Prosthetics Orthotics
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Blood products, transfusions, plasma, and processing charges
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible

Elmira CSD – rev. 04/28/05 19
Option A - Active
Option A - Retired
OPTION A
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits
Home Health Care 80% of negotiated fee after deductible (up to 325 days if approved by Claims Administrator)
80% of negotiated fee after deductible (up to 325 days if approved by Claims Administrator)
Routine Annual Gyn Exam (for employees, retirees, and spouses) Pap smear and tests related to the exam are covered under Diagnostic Laboratory and X-ray benefits
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee
80% of negotiated fee after deductible
Alternative Treatment (includes chiropractic care, acupuncture, biofeedback)
Care must be preapproved to be paid. See Section IV, subsection E
Care must be preapproved to be paid. See Section IV, subsection E
Care must be preapproved to be paid. See Section IV, subsection E
Care must be preapproved to be paid. See Section IV, subsection E
Participating Retail Pharmacy: Refer to your current collective bargaining agreement or contact the Business Office for applicable copayments.
Prescription Drug Coverage
Non-participating Retail Pharmacy: The Plan reimburses cost minus the copayment up to the amount that would have been paid at a participating pharmacy.
80% of cost after deductible

Elmira CSD – rev. 04/28/05 20
Option B Active
Option B Retiree
OPTION B
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits Copayments
Refer to current collective bargaining agreement
Refer to current collective bargaining agreement
Refer to collective bargaining agreement in effect at time of retirement
Refer to collective bargaining agreement in effect at time of retirement
Medicare N/A N/A Hospital – The Plan pays the Medicare Part A deductible per spell of illness and daily coinsurance for inpatient confinements; Medial/Surgical – The Plan will pay Medicare Part B deductible and the remaining 20% not paid by Medicare. Major Medical – The Plan pays the difference between the eligible charge and Medicare-approved amount.
Referrals to Non-participating Providers by in-network physicians Services are available in-
network
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Services are not available in-network
100% of negotiated fee, if applicable, or Reasonable and Customary
100% of negotiated fee, if applicable, or Reasonable and Customary
100% of Reasonable and Customary
100% of Reasonable and Customary
100% of Reasonable and Customary
100% of Reasonable and Customary
Out-of-area Services
If you travel outside the Plan’s service area, benefits for Covered services are payable at 100% of the Reasonable and Customary charge. This exception does not apply to pre-arranged procedures outside the Plan’s service area. Please refer to Appendix B using Appendix A for clarification of the Plan’s service area.
Benefit Management Program
Notification applies to inpatient hospital admissions.
Notification applies to inpatient hospital admissions.
Hospital/Surgical/Medical Expense Benefits
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Inpatient Acute Care General Hospital Services (facility charges)
Notification is required. Notification is required. 100% 80% of negotiated
fees after deductible 100% 80% of negotiated
fees after deductible Birth Center
Notification is required.
Notification is required.

Elmira CSD – rev. 04/28/05 21
Option B Active
Option B Retiree
OPTION B
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits Ambulance (professional and volunteer)
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
100% of Reasonable and Customary; the deductible does not apply
Ambulatory Surgical Center or Hospital Outpatient Surgical Facility
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Inpatient Mental Health (Hospital or private proprietary psychiatric facility charge) Notification is required. Notification is required.
100% limited to 7 weeks
80% of negotiated fees after deductible; limited to 7 weeks
100% limited to 7 weeks
80% of negotiated fees after deductible; limited to 7 weeks
Inpatient Alcohol/Substance Abuse (certified facility charge)
Notification is required. Notification is required.
Skilled Nursing or Rehabilitation Facility – Inpatient Custodial care is not covered
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Home Health Care 100% up to 40 days per year (approved on case-by-case basis by Claims Administrator)
80% of negotiated fee after deductible up to 40 days per year (approved on case-by-case basis by Claims Administrator)
100% up to 40 days per year (approved on case-by-case basis by Claims Administrator)
80% of negotiated fee after deductible up to 40 days per year (approved on case-by-case basis by Claims Administrator)
Hospice (Claims Administrator’s guidelines apply, page 55)
100% 210 days
80% of negotiated fee after deductible 210 days
100% 210 days
80% of negotiated fee after deductible 210 days
Outpatient Treatment Alcohol/Substance Abuse - Physician Care
100% limited to 30 visits per year
80% of negotiated fee after deductible limited to 30 visits per year
100% limited to 30 visits per year
80% of negotiated fee after deductible limited to 30 visits per year
Outpatient Treatment Mental Health – Physician Care (includes certified psychiatric social worker)
100% of Reasonable and Customary Limited to 30 visits per year
80% of negotiated fee after deductible Limited to 30 visits per year
100% of Reasonable and Customary Limited to 30 visits per year
80% of negotiated fee after deductible Limited to 30 visits per year

Elmira CSD – rev. 04/28/05 22
Option B Active
Option B Retiree
OPTION B
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits Emergency Center or Urgent Care Facility (facility charge)
100% 100% 100% 100%
Emergency Center or Urgent Care Facility Physician (separate charge)
100% 100% 100% 100%
Services must be rendered within 12 hours of a medical emergency or 24 hours of an accidental injury. Emergency center services received outside these time limits are not covered.
Non-emergency care rendered in an Emergency center: the facility charge and separate physician’s charge are not covered; diagnostic testing and medications are covered.
Physician Surgery-Related Services:
• Surgery and Maternity Care
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
• Assistant Surgeon 100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
• Anesthesia
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Inpatient Physician Services
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Preadmission Testing and Interpretation (within 7 days of admission)
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Outpatient Hospital Diagnostic X –Rays, Laboratory, and Machine Testing and interpretation
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Outpatient Hospital Physical and Occupational Therapy
100%; must follow hospitalization
80% of negotiated fee after deductible; physical therapy must follow hospitalization
100%; must follow hospitalization
80% of negotiated fee after deductible; physical therapy must follow hospitalization
Outpatient Hospital Speech Therapy
100% 80% of negotiated fee after deductible
100%; must follow hospitalization
80% of negotiated fee after deductible;
Cardiac Rehabilitation (outpatient or facility)
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible

Elmira CSD – rev. 04/28/05 23
Option B Active
Option B Retiree
OPTION B
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits Inhalation or Respiratory Therapy and IV Therapy (Outpatient Hospital)
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Radiation Therapy and Chemotherapy
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
Dialysis 100%
80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible
100% after the copay
80% of negotiated fees after deductible
100% after the copay
80% of negotiated fees after deductible
Physician Services – Office or clinic visit (non-routine) Refer to your current collective bargaining
agreement or contact the Business Office Refer to your collective bargaining agreement in effect at the time of retirement or contact the Business Office
Consultations 100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Diagnostic X –Rays and Laboratory (out of hospital) and interpretation
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Elective Sterilization
100% 80% of negotiated fees after deductible
100% 80% of negotiated fees after deductible
Well Child Care and Immunizations (for routine in-hospital care at birth and for the first 24 months from birth)
100% Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
80% of negotiated fee after deductible Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
100% Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
80% of negotiated fee after deductible Limited to 6-visit and up to $300 maximum benefit after discharge up to 24-months of age
Adult Routine Physical and Tests Employees and retirees age 50 years and older Limited to one per calendar year; Immunizations are not covered
100%
80% of negotiated fee after deductible
100%
80% of negotiated fee after deductible
Routine Mammography Screening 35 years and older One per year
100% 80% of negotiated fee after deductible
100% 80% of negotiated fee after deductible

Elmira CSD – rev. 04/28/05 24
Option B Active
Option B Retiree
OPTION B
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits Routine Annual Gyn Exam (employees, retirees, and spouses) Pap smear and tests related to the exam are covered under Diagnostic Laboratory and X-ray benefits
100% up to $30 benefit, balance subject to 80% of negotiated fee after deductible
80% of negotiated fee after deductible
100% up to $30 benefit, balance subject to 80% of negotiated fee after deductible
80% of negotiated fee after deductible
Organ Transplants See Section IV, subsection I, paragraph 2.
See Section IV, subsection I, paragraph 2.
See Section IV, subsection I, paragraph 2.
See Section IV, subsection I, paragraph 2.
100%, subject to copay or benefit limitations
80% of negotiated fee after deductible
Vision Care members of CWA (one
examination and prescription lenses per year)
employees assigned to work with computers on a regular basis (one examination per year)
refer to current collective bargaining agreement for copay or coinsurance percentage and limitations
Not covered
Major Medical Expense Benefits
Major Medical Deductible Calendar Year (a separate deductible applies to in-network and out-of-network charges)
$100 per individual $200 per Family
$200 per individual $600 per Family
$100 per individual $200 per Family
$200 per individual $600 per Family
Common Accident Deductible
Yes Yes
Carry-over Deductible
Yes Yes
Percentage Coinsurance (all groups except CWA group described below)
80% of covered charges up to $2,000 after annual deductible, 100% thereafter
80% of covered charges up to $5,000 after annual deductible, 100% thereafter
80% of covered charges up to $2,000 after annual deductible, 100% thereafter
80% of covered charges up to $5,000 after annual deductible, 100% thereafter
CWA Active Employees, Retirees, and their Covered Dependents
80% of covered charges up to $5,000 after annual deductible, 100% thereafter
80% of covered charges up to $5,000 after annual deductible, 100% thereafter
80% of covered charges up to $5,000 after annual deductible, 100% thereafter
80% of covered charges up to $5,000 after annual deductible, 100% thereafter

Elmira CSD – rev. 04/28/05 25
Option B Active
Option B Retiree
OPTION B
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits Out of Pocket Maximum Per Person for Covered Major Medical expenses (all groups except CWA)
$400 (does not include deductible)
$1,000 (does not include deductible)
$400 (does not include deductible)
$1,000 (does not include deductible)
CWA Active Employees, Retirees, and their Covered Dependents
$1,000 (does not include deductible)
$1,000 (does not include deductible)
$1,000 (does not include deductible)
$1,000 (does not include deductible)
Lifetime Maximum
$2,500,000 $1,000,000 $2,500,000 $1,000,000
Private Duty Nursing (RN only)
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Physical and Occupational Therapy Private Practitioner
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Speech Therapy Private Practitioner
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Allergy Treatment 80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Medical Supplies Diabetic Supplies
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Durable Medical Equipment
If a participating provider of DME is not available in-network, benefits for services received out-of-network will be subject to the in-network deductible.
If a participating provider of DME is not available in-network, benefits for services received out-of-network will be subject to the in-network deductible.
Oxygen 80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Prosthetics Orthotics
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Blood products, transfusions, plasma, and processing charges
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
80% of negotiated fee after deductible
Home Health Care 80% of negotiated fee after deductible 40 visits plus up to 325 days if approved by Claims Administrator
80% of negotiated fee after deductible 40 visits plus up to 325 days if approved by Claims Administrator
Alternative Treatment (includes chiropractic care, acupuncture, biofeedback)
Care must be preapproved to be paid. See Section IV, subsection E
Care must be preapproved to be paid. See Section IV, subsection E
Care must be preapproved to be paid. See Section IV, subsection E
Care must be preapproved to be paid. See Section IV, subsection E

Elmira CSD – rev. 04/28/05 26
Option B Active
Option B Retiree
OPTION B
Plan Features
In Network
Benefits
Out of Network
Benefits
In Network
Benefits
Out of Network
Benefits Participating Retail Pharmacy: Refer to your current collective bargaining agreement or contact the Business Office for applicable copayments.
Prescription Drug Coverage
Non-participating Retail Pharmacy: The Plan reimburses cost minus the copayment up to the amount that would have been paid at a participating pharmacy.
80% of cost after deductible

Elmira CSD – rev. 04/28/05 27
SECTION II - ELIGIBILITY AND ENROLLMENT
A. Eligibility for Plan Enrollment
Plan coverage for you and your Dependents will be according to the eligibility, enrollment, Effective Dates, and cancellation provisions of the Plan. Rules concerning eligibility for Plan enrollment are established through the applicable collective bargaining agreements. This section shows the current general rules for enrollment, Effective Dates and coverage continuation; it is not intended to constitute, or be validated as, the origin or basis for Plan eligibility requirements. The Business Office can provide full details concerning your eligibility for Plan coverage. 1. Active Employees. Persons in the following categories are considered employees eligible for Plan
enrollment.
a. Custodial, Maintenance, and Cafeteria Workers (CMCW) whose members: • Work 25 or more hours per week, or • Work less than 25 hours per week and pay full premium for medical and/or dental coverage.
CMCW - Unit members employed before December 15, 1999 may choose coverage under either Option A or Option B. Members hired after December 15, 1999 may only be eligible to participate in Option B. An employee who would otherwise be ineligible for health and dental care coverage shall be eligible to enroll in the Health and/or Dental Care Plan if he pays the premium equivalent. An ineligible employee may enroll in the Health and Dental Care Plan only during the annual open-enrollment period held during September.
b. Communication Workers of America (CWA) whose members work 30 or more hours per week or
earn $3,000.00 per year (exclusive of overtime pay) and: • who are hired prior to July 1, 1999 may enroll in Option A or Option B, or • who are hired after July 1, 1999 may enroll in Option B only.
CWA - Unit members employed before July 1, 1999 may choose coverage under either Option A or Option B. Members hired after July 1,1999 may only be eligible to participate in Option B.
c. Elmira Teachers Association (ETA) whose members are employed full-time, regularly work at least
20 hours per week.
ETA - Unit members employed before January 1, 2000 may choose coverage under either Option A or Option B. Members hired after January 1, 2000 may only be eligible to participate in Option B.
d. Instructional Support Employees Association (ISEA) whose members were:
• Hired prior to July 1, 1973, work 20 or more hours per week or earn $2,000.00 per year; • Hired after July 1, 1973, but before July 1, 1986, work 30 or more hours per week or earn
$3,000.00 per year; or • Hired after July 1, 1986, regularly employed for 30 hours per week and
o Hired prior to November 1, 1999 may enroll in Option A or Option B, or o Hired after November 1, 1999 – may enroll in Option B only
ISEA - Unit members employed before November 1, 1999 may choose coverage under either Option A or Option B. Unit members hired after November 1, 1999 may only be eligible to participate in Option B.

Elmira CSD – rev. 04/28/05 28
e. Elmira School Supervisory and Administrative Council (ESSAC) whose members work 20 or more hours per week.
ESSAC - Unit members employed before September 1, 1996, may choose between the Indemnity Plan, Option A, or Option B. All Administrators hired after September 1, 1996, but before July 1, 1999, may choose either Option A or Option B. Unit members hired after July 1, 1999 are eligible to participate in Option B only.
f. Non-Unit Employees who work 20 or more hours per week.
Non-Unit - Individuals employed before September 1, 1996, may choose between the Indemnity Plan, Option A, or Option B. All Administrators hired after September 1, 1996, but before July 1, 1999, may choose either Option A or Option B. Members hired after July 1, 1999 are eligible for coverage under the Option B plan only.
2. Retirees. Individuals, who as Active Employees, have participated in the Plan for at least ten years
with the District and have a letter from the Retirement System approving retirement benefits.
Please note: Be it resolved that the language specified in the Master Plan Document, referring to Section
II.A.2.Retirees, does not appear to accurately reflect the Plan benefits as they should for some of the participants in the Plan and that said language does not pertain until such time that it is negotiated
and agreed upon.
3. Active Employees not Eligible. Persons in the following categories are not eligible for Plan enrollment:
a. Any terminated or laid-off employee who was not enrolled in the Plan at the time active employment ended.
b. Per diem/casual employees, persons hired on a temporary basis, or student interns or students employed during school holidays.
c. Employees who do not meet the minimum qualifications established for coverage. d. Any unenrolled employee who submits an initial application while temporarily removed (i.e., leave
of absence, disability, military service) from the payroll. e. Former employees who do not meet retiree eligibility requirements. f. Any employee on active duty in the military service of any country except as unilaterally determined
by the Board of Education.
4. Dependents. The term Dependent means your eligible spouse and eligible children. Documentation of Dependent status may be required. Criteria of support will be considered met if the Employee or Retiree, or eligible Spouse, shows that the child qualifies as an exemption on a current federal income tax return or is the subject of a court order. Eligibility of dependents of an Eligible retiree is limited to those dependents who were covered under the Plan prior to the employee’s retirement.
If you are not eligible for Plan enrollment, you cannot enroll your Dependents under this Plan.
To be eligible for enrollment in your family coverage, your dependents must meet the following requirements:
a. Legal Spouse. - A legal spouse may be enrolled in the Plan, but a divorced spouse is not eligible. If
you are a retiree, you may only enroll your current spouse at the time of retirement who is covered under the Plan at the time of retirement.

Elmira CSD – rev. 04/28/05 29
b. Unmarried Children. Your unmarried children may be considered dependents. To be eligible for enrollment in your family coverage, the children must meet the following child definition and age requirements. A retiree may only enroll dependent children existing at the time of retirement who are covered under the Plan at the time of retirement.
1) Child Definition. A child (children) means:
a) The Employee's or Retiree’s own unmarried child or legally adopted unmarried child; b) Any unmarried stepchild of the Employee or Retiree’s who permanently resides in the
Employee’s or Retiree’s home and qualifies as a Dependent under federal income tax rules; c) Any other unmarried child placed under legal guardianship of the Employee before the
child is age 19 and who is permanently living in the Employee’s home; supported by the employee and qualifies as a dependent under federal income tax rules;
d) Any unmarried child placed for adoption before the child reaches age 18. The term placed for adoption means a child placed in the Employee’s or Retiree’s home and the Employee’s or Retiree’s assumption and retention of a legal obligation for total or partial support of a child in anticipation of adoption of the child. This eligibility ends when such legal obligation terminates. Proof of pre-adoption status will be required by the Elmira City School District to establish eligibility. Once the child is legally adopted, he or she retains eligibility as a legally adopted child shown above;
e) Any child who lives with the Employee or Retiree and qualifies as a dependent under federal income tax rules; or
f) Pre-adoptive Newborn from the moment of birth under a family Plan when all of the following conditions are met: (1) You enroll the child that you intend to adopt in your family coverage within 30 days of
the birth and applicable family Contribution is made; (2) You take physical custody of the child upon discharge from the Hospital or Birth Center;
and (3) Within 30 days of the child's birth, you file a petition to adopt or for temporary legal
guardianship under New York State Domestic Relations Law.
Coverage will not be provided for initial Inpatient treatment of a pre-adoptive Newborn, if the child’s biological parent has health coverage for that care. Also, if a notice of revocation of the adoption has been filed, or a biological parent revokes consent to the adoption, coverage will not be provided. If Plan benefits were paid for pre-adoptive Newborn, whose adoption was revoked, you may be requested to reimburse the Plan in the amount of those payments. Coverage is not provided for any expenses Incurred by the natural mother or any medical care or treatment of the Newborn before actual physical birth and delivery of the Newborn.
2) Age Requirements. Eligibility is limited to your Dependent children who meet the above child definition and who are:
a) Under 19 years of age. Your Newborn child is eligible as a Dependent from the moment of
birth. An unmarried child whose 19th birthday occurs during a school vacation period will continue to be eligible for benefits, provided the child is enrolled in a school and is anticipating full-time student status at the end of the vacation period.
b) Over 19 years of age, but under age 24 years, who are claimed as a qualified dependent for
federal income tax purposes by you or your Spouse, and are full-time students (12 or more credit hours) at an accredited secondary school, College, or University.

Elmira CSD – rev. 04/28/05 30
In the event a Dependent child between the ages of 19 and 24 who is a full-time student is disabled and is granted a medical leave by the school that he or she is attending, eligibility will continue for a maximum of 12 calendar months following the month in which the child withdraws from school. If the end of the 12 calendar months occurs during a vacation period, benefits will be extended to the beginning of the next regular semester. Your unmarried child between the ages of 19 and 24 who previously was not eligible for benefits, or had benefits ended, and returns to a full-time student status, may be reinstated to family coverage effective the actual date the student commenced full-time attendance at the high school or an accredited institute of higher learning.
c) Nineteen years of age, or older, who is incapable of self-support because of mental or physical
disability and became so disabled before reaching age 19. The eligibility of such a Dependent should be established as early as possible. This should be done at the time of your initial enrollment if the child is age 19, or older, at that time. If the child has not yet attained age 19, at the time you first enroll in the program, eligibility for continued benefits should be established at the time of his or her 19th birthday. You must request handicapped child continuation within 30 days after the child’s 19th birthday. Failure to do so could result in loss of eligibility and benefits.
Please Note
The residence and support rules are waived if you are required to provide health coverage due to a court order or divorce decree or qualified medical support order for a child who is under age 19 and not living in your home and/or not dependent for more than 50% of his or her support.
To obtain Plan coverage for children, you may be required by the Business Office to document appropriate certification of guardianship, preadoptive status and/or that the child resides in your home and is dependent on you for support and maintenance. After initial enrollment, the Plan may require periodic proof to verify that Plan eligibility requirements continue to be met. To obtain Plan coverage for full-time students, you may be required to document, at least annually, appropriate certification of this fact to the Business Office. After eligibility for the disabled or handicapped child has been established, proof that the child remains physically or mentally unable to earn his or her own living and continues to be dependent on you for most of his or her support and maintenance may be requested periodically from the District’s Business Office. After two years, this proof will usually not be requested more than once each year. The District, at its expense, may have a Physician of their choice examine the child to clarify the extent of the child’s handicap. Such examinations will not be required more than once each year. Failure to participate in a required Physician examination will result is loss of coverage for that child. The Business Office will advise you, based on their review of the proof submitted or the results of an independent Physician’s examination, whether the child meets the eligibility requirements for disabled or handicapped child eligibility.
Failure to provide the required information, when requested, will result in the child being removed from enrollment and eligibility for benefits until proof is provided which supports continued eligibility for Plan enrollment. This could cause a lapse in coverage and/or loss of benefits.
5. Persons Not Considered Eligible Dependents for Plan Enrollment. The following persons are not
considered eligible for Plan enrollment as dependents:
a. Married children. Eligibility ends on the date of marriage. b. Any unenrolled Dependent on active duty in the military service or armed forces of any government
or country.

Elmira CSD – rev. 04/28/05 31
c. Any person who does not meet the Plan definition or eligibility requirements as a Spouse or child. 6. Qualified Medical Child Support Orders. Federal Law requires the Elmira City School District, under
certain circumstances, to provide Plan coverage for your children when you or your Spouse divorce or separate. The law also provides for children born out of wedlock. The District must comply with qualified medical child support orders (QMCSO) that relate to Plan benefits. QMCSO means orders, judgment, settlement, or a decree issued from a court of competent jurisdiction, magistrates or other officials with the power to issue a QMCSO pursuant to a state’s domestic laws, that requires an employer to provide available health plan coverage for your child. This coverage is provided even if you no longer have custody and even if you would not have chosen to cover the child under the existing health Plan. The child’s custodial parent, legal guardian or state agency can apply for coverage even if you don’t. If the Plan receives a QMCSO, it will provide immediate Plan enrollment. This means the child identified will be included for Plan coverage, as required according to the QMCSO requirements. You will be required to pay any new or added monthly participation costs for the child's enrollment. The Elmira City School District Business Office will send you written notification and provide further information about the QMCSO rules should they receive an order that applies to you.
7. Leave of Absence. If you are on an authorized leave, you have the right to continue to participate in the
Plan during your leave of absence, in accordance with the terms of the applicable collective bargaining agreement or as mandated by law. The Business Office can give you full details concerning the costs for continued Plan participation. The following are general rules for continuing participation in the Plan.
a. Authorized Leave of Absence. You may retain your individual coverage or family coverage under
the Plan for an approved leave of absence due to total disability or other leave when authorized by the District, according to its established rules or according to Federal and State laws including the Family and Medical Leave Act shown below. If any part of the leave is without pay, you must submit your designated participation payments on a timely basis to maintain coverage.
If you continue to be absent from work beyond the approval period, your Plan coverage will end at midnight on the last day of your approved absences. However, you and your Dependents may be eligible for Continuing Coverage under COBRA shown later in this section. If you fail to pay a scheduled Plan participation Contribution within 30 days of the due date, coverage will end for you and your Dependents at the end of the month for which your last participation Contribution was made. If Plan coverage ends while you are absent from work, you cannot be reinstated until you return to work and enroll in the Plan. You will be considered a new Employee if more than 60 days have passed since your last day of approved absence.
b. Family and Medical Leave Act. Under the Family and Medical Leave Act (FMLA) of 1993, a
federal law, eligible Employees are entitled to receive up to 12 weeks of unpaid leave in any 12 consecutive months for certain family and medical reasons. If you are on an FMLA leave of absence, you may continue Plan coverage by paying your monthly-designated participation Contribution, if any, for Individual or Family coverage. Plan continuation will be according to the FMLA law, as amended. The District’s Business Office can provide the details of your rights under the FMLA and your costs to continue coverage while on the FMLA.
8. Survivor Dependents. A surviving spouse or dependent has the right to continue coverage under the
Plan. The Board of Education will continue to pay the cost of coverage for two months after the death of the employee or retiree. After two months, the spouse or dependent may elect to continue the coverage by paying the full premium equivalent. In the case of a surviving spouse, the coverage may be continued while he or she remains unmarried. Coverage for a dependent child may be continued under the surviving spouse’s family coverage or under his or her own individual coverage, if there is no surviving spouse, until he or she no longer qualifies as a Dependent under the terms of this Plan.

Elmira CSD – rev. 04/28/05 32
B. Enrollment
The Business Office can provide forms and explanations needed for any enrollment updates or changes. Failure to report enrollment changes could result in Plan overpayment. If this happens, you will be required to reimburse the full amount of any overpayment.
Enrollment in the Plan is not automatic. You are required to enroll yourself and your Dependents in medical and/or dental coverage. You must be Actively Employed as an eligible Employee or be an eligible retiree to enroll in the Plan. Employee enrollment options for dental coverage are shown in Section IV, Covered Services, subsection J. Dental Expense Benefits.
1. Active Employees. CMCW – Unit members employed before December 15, 1999 may choose coverage under either Option A or Option B. Members hired after December 15, 1999 may only be eligible to participate in Option B. An employee who would otherwise be ineligible for health and dental care coverage shall be eligible to enroll in the Health and/or Dental Care Plan if he pays the premium equivalent. An ineligible employee may enroll in the Health and Dental Care Plan only during the annual open-enrollment period held during September. CWA – Unit members employed before July 1, 1999 may choose coverage under either Option A or Option B. Members hired after July 1,1999 may only be eligible to participate in Option B. ESSAC - Unit members employed before September 1, 1996, may choose between the Indemnity Plan, Option A, or Option B. All Administrators hired after September 1, 1996, but before July 1, 1999, may choose either Option A or Option B. Unit members hired after July 1, 1999 are eligible to participate in Option B only.
ETA – Unit members employed before January 1, 2000 may choose coverage under either Option A or Option B. Members hired after January 1, 2000 may only be eligible to participate in Option B.
ISEA – Unit members employed before November 1, 1999 may choose coverage under either Option A or Option B. Unit members hired after November 1, 1999 may only be eligible to participate in Option B.
Non-Unit – Individuals employed before September 1, 1996, may choose between the Indemnity Plan, Option A, or Option B. All Administrators hired after September 1, 1996, but before July 1, 1999, may choose either Option A or Option B. Members hired after July 1, 1999 are eligible for coverage under the Option B plan only.
2. Retirees may only elect the medical plan option in which he or she was enrolled at the time
of retirement. Your enrollment categories are as follows: 1. Individual Coverage shall mean that the Plan covers only that eligible and enrolled person even if other
members of the family meet eligibility requirements. 2. Family Coverage shall mean that the Plan covers the eligible enrolled Employee, retiree, or surviving
Spouse, or ex-Spouse and eligible enrolled Dependents even if other family members meet eligibility requirements.

Elmira CSD – rev. 04/28/05 33
3. Enrollment Changes. a. It is your responsibility to apply for any enrollment changes including, but not limited to:
1) Adding a newly acquired Spouse or Dependent child; 2) Adding an existing Spouse previously enrolled as an Employee; 3) Adding a previously eligible, but unenrolled Spouse or Dependent child; 4) Changing from individual coverage to family coverage any time you acquire a Spouse or
Dependent child or elect to enroll a previously eligible, but unenrolled Spouse or Dependent child;
5) Changing from family coverage to individual coverage any time you no longer have Eligible Dependents or when you no longer wish to provide coverage for Dependents;
6) Changing from two individual enrollments to one family coverage, or from one family coverage to two individual enrollments, when you or your Spouse are both eligible as Employees.
7) Changing or adding new Dependents, or removing existing Dependents, from family coverage; or 8) Reporting other group plan(s) and Medicare coverage information and changes.
b. Covered Employees may elect to change from Option A to Option B (and vice versa) in the
month of November (open enrollment period). The following re-enrollment procedure will apply:
1) Enrollees with Option A who elect to switch to Option B may switch back to Option A during the following annual enrollment period with no penalty.
2) A re-enrollment fee of $100 will apply if the enrollee again chooses to switch from Option to Option B and back to Option A.
3) If the enrollee chooses to switch from Option A to Option B and back to Option A for a third time, a re-enrollment fee of $500 will apply.
C. Effective Dates of Benefits
The Business Office can provide full details concerning the Effective Date of benefits for you or your Dependents. The following are general rules for Effective Dates of benefits: 1. Employment Waiting Period. If you are eligible and enrolled in the Plan, coverage is effective the
first day of the month following the date of hire. Benefits will not be payable for any expenses Incurred during a waiting period. The waiting period is the period between the first day of employment and the first day of the following month.
If you enroll in the Plan before the applicable Waiting Period has elapsed, coverage will automatically become effective when the Waiting Period has been met, if you are Actively Employed as an eligible employee at that time.
2. Employees/Retirees.
a. On Effective Date of the Plan. Each Eligible Employee or retiree whose employment or retirement commenced on or before the Effective Date of the Plan will be Covered on the Effective Date of the Plan if:
1) He or she was enrolled as an eligible employee or retiree in the previous Plan when this Plan
went into effect; or 2) He or she is Actively Employed as an eligible employee and enrolls in this Plan at the time this
Plan became effective.

Elmira CSD – rev. 04/28/05 34
b. Effective Date of Coverage. If you are eligible to participate in the Plan and your employment starts after the Plan Effective Date, your eligibility date for Plan enrollment is the first day of the month following your date of hire. If you enroll within 31 days following your eligibility date, the effective date of your individual or family coverage will be your eligibility date. You must be actively employed as an eligible employee on your effective date of coverage. If you do not enroll within 31 days after your eligibility date, coverage begins the first of the month after you enroll.
3. Dependent General Rules. If they are enrolled at the time of your initial enrollment, coverage for your
Dependents becomes effective on the same date as your effective date. If you did not enroll existing dependents at the time of your initial enrollment, coverage for dependents begins no sooner than the Effective Dates shown later in this section under Special Enrollment Effective Dates.
4. Special Enrollment Effective Dates.
a. Adding New Dependents.
1) If you are an active Employee and are enrolled in the Plan and acquire new Dependents after
your initial enrollment and enroll the new Dependents in family coverage within 31 days after the date the Dependents are acquired, Plan coverage for the new Dependent will begin on the date you acquired the Dependent, but no sooner than your Effective Date of Coverage. You will be required to pay the family coverage participation payments, if any.
2) If you are an active Employee and not enrolled in the Plan when you acquire a Spouse you may
enroll yourself and your Spouse under family coverage. If you acquire a Newborn child, or a newly placed or adopted child (under age 18), you may enroll yourself and/or your Spouse and the newly acquired Newborn child, newly placed for adoption or adopted child under family coverage. For coverage to be effective on the date you acquired the new Dependent (but no sooner than 31 days of consecutive eligible employment), you must enroll within 31 days after the date of marriage, birth, placement for or adoption, whichever applies. This immediate coverage rule does not apply to children existing at the time of your initial eligibility.
3) If you fail to enroll yourself or Dependents within 31 days from the date the Dependents were
acquired, Cancellation of Another Health Plan rules shown below apply. b. Cancellation of Another Health Plan. Eligible persons who were not enrolled in this Plan under
active Employee coverage, due to other health plan coverage, may elect coverage under this Plan. To be effective from the date the other coverage ended, the following conditions must be met:
1) The person had health coverage at the time this coverage was previously offered; and 2) The person stated in writing at the time he or she declined enrollment in this Plan that the reason
for declining was due to the other coverage; and 3) The other coverage was involuntarily terminated due to loss of eligibility; or exhaustion of the
prior plan continuation of coverage; or cessation of employer Contributions to the other plan; or cancellation of coverage by the employer, insurer, or other issuing entity; and
4) The person requests enrollment within 31 days after the date the other plan was canceled. If you fail to enroll yourself or Dependents within 31 days after involuntary cancellation of the other plan, coverage begins not sooner than the first day of the month following enrollment. This rule also applies to persons who voluntarily cancel the other plan then seek late enrollment in this Plan. Voluntary cancellation includes, but is not limited to, cancellation or withdrawal from the other coverage by the enrollee; removal of Dependents from family coverage by the enrollee; or cancellation of coverage due to enrollee fraud or enrollee nonpayment of required participation premiums or Contributions.

Elmira CSD – rev. 04/28/05 35
D. Monthly Participation Contributions
To maintain your eligibility in the Plan, you must pay your designated participation Contribution. If your payment is not done by payroll deduction, you must pay your designated participation Contributions to maintain Plan coverage. If you fail to pay designated participation Contributions within 30 days after the due date, coverage will stop at the end of the month for which the last Contribution was paid. The Business Office can provide details concerning your participation costs for individual or family coverage.
E. End of Coverage
Plan coverage for you or your Dependents will end on the first of the month following when you or your Dependents no longer meet the eligibility requirements of the Plan. Expenses incurred after coverage ends will not be considered for Plan benefits. However, you or your Dependents may be eligible and elect to continue coverage under COBRA. Refer to Continuing Benefits Under COBRA, shown later in this section. Eligibility and coverage ends for the following unless enrollment under COBRA is made: 1. For any and all Plan participants when the Plan is terminated. 2. For an Employee and all his or her enrolled Dependents when you are no longer eligible because of
termination of employment, reduction in hours or non-eligible retirement. Coverage ends on the first day of the month following the date employment status or eligibility terminated.
3. For Employee and all his or her Dependents, coverage ends on the date after 30 days of full time active duty in the military service or armed forces of any country. However, the employee may elect Continuing Coverage under USERRA shown later in this section.
4. For Employee or Retiree and all his or her Dependents for Nonpayment of Plan participation Contribution, if any. For Dependents, for non-payment of Plan participation contribution for Dependent Coverage.
5. Divorce, annulment or other dissolution of your marriage. Coverage ends for your ex-Spouse on the date dissolution of your marriage becomes final.
6. If the retiree or employee dies, coverage ends for the retiree or employee and all his enrolled dependents unless the dependents are eligible as survivors. A surviving spouse or dependent of an employee or a retiree may elect to continue coverage. The District will pay the full cost of coverage for two months, thereafter, the survivor pays the full cost of participation.
a. Coverage for a surviving spouse will terminate upon remarriage. b. A Dependent child’s coverage will end when he or she is no qualifies as a Dependent under the
terms of this Plan. 7. For a Dependent, coverage ends for that Dependent on the date after 30 days of full time active duty by
that Dependent in the military service or armed forces of any country. 8. For a Dependent Child, coverage also ends on:
a. The date the child marries. b. The date the child no longer qualifies as a dependent according to eligibility rules shown in Section
II - Eligibility and Enrollment. For example: 1) The last day of the month in which the child is no longer dependent on the Employee or retiree
for support or no longer resides in the Employee’s or retiree’s home. 2) The last day of the month in which the child reaches age 19 and is not a full-time student or is no
longer eligible as a disabled/handicapped child dependent on the Employee or retiree for support. 3) The last day of the month in which the child between ages 19 and 24 is no longer eligible as a
full-time student. 4) The last day of the month in which the full-time student reaches age 24. 5) The last day of the month in which a preadoptive child is removed from placement for adoption
or the Employee is no longer legally responsible for total or partial support of the preadoptive child.

Elmira CSD – rev. 04/28/05 36
6) The last day of the month in which a child previously eligible as a handicapped or disabled child marries, is able to earn his or her own living, fails to provide proof of disability, or to participate in a required Physician exam or the date the District establishes that the child not longer meets criteria as a disabled or handicapped child based on submitted proof of disability and examination results.
Coverage may be stopped immediately if you or your Dependent knowingly submits a claim or allows a claim to be submitted with false information, or conceals any facts that would affect the outcome of a claim determination. In this case, you or your Dependents will not be eligible for COBRA continuation.
F. Extension of Coverage.
Please contact the District’s Business Office if you have any questions or concerns regarding Total Disability requirements. This extension of coverage is not available to Covered Persons who are covered under the Plan's continuation of coverage under USERRA or COBRA. 1. Limited Total Disability Extension. This extension of coverage applies when Plan coverage ends due to
termination of eligible active employment with the District or termination of the Covered Person's eligibility or termination of the Plan.
If a covered individual is confined in a Hospital within a period of three months or undergoes a surgical
procedure within a period of one month immediately following the discontinuance of the coverage of such individual under this part, Hospital expenses or surgical procedure benefits shall be payable as though the procedure had been performed prior to such discontinuance, if:
a. the confinement or surgical procedure is due to an accidental injury or to an illness which occurred
prior to the termination, and
b. the person was Totally Disabled as a result of that injury or illness on the date of termination of coverage, and he or she remained continuously disabled until the date that the confinement began or the surgical procedure was performed.
2. Total Disability Extension. An extension of coverage for Total Disability provides continued coverage
for you or your eligible dependents who are Totally Disabled at the time coverage terminates. This extended Coverage provides benefits solely for expenses incurred for the illness or injury that caused the total disability. Plan Coverage under this provision will remain in effect until the earliest of the following dates:
a. The date the Covered Person is no longer Totally Disabled; b. The date the maximum benefits under the Plan have been received; c. The date the Covered Person obtains coverage under another group health plan which provides
coverage for the disabling condition; or d. The period ending on December 31 of the calendar year following the calendar year in which the
termination of coverage occurred. You or your Dependent may be requested to submit an attending physician's certification of total disability to the Plan’s Claims Administrator. You will be advised, in writing, whether or not extension of coverage has been approved. If extension of coverage is approved, additional proof of Total Disability could be requested from time to time.
Elmira CSD – rev. 04/28/05 37
G. Continuing Coverage Under USERRA
The District’s Human Resources Office must be notified, in writing (in advance when practical), should your eligible employment stop due to active United States Military Service. The following information is a brief summary. The Business Office can provide information regarding the cost to continue coverage while on active military duty. The following information is a brief summary. This Plan excludes health expenses resulting from injuries or sickness Incurred in or aggravated while on military duty. This Plan excludes any illness or injury caused by or resulting from military service. The Board of Education may unilaterally adopt a policy providing additional benefits.
Employees going into or returning from military service may elect to continue Plan coverage as mandated by the Uniformed Services Employment and Reemployment Rights Act under the following circumstances. These rights apply only to Employees and their Dependents covered under the Plan before leaving for military service.
1. The maximum period of coverage of a person under such an election shall be the lesser of:
a. The 18 month period beginning on the date on which the person's absence begins; or
b. The 24 month period beginning on the date on which the person's absence begins for elections on or after December 10, 2004; or
c. The day after the date on which the person was required to apply for or return to a position of
employment and fails to do so.
2. A person who elects to continue health plan coverage may be required to pay up to 102% of the full contribution under the Plan, except a person on active duty for 30 days or less cannot be required to pay more than the Employee's share, if any, for the coverage.
3. An exclusion or Waiting Period may not be imposed in connection with the reinstatement of
coverage upon reemployment if one would not have been imposed had coverage not been terminated because of service. However, an exclusion or Waiting Period may be imposed for coverage of any Illness or Injury determined by the Secretary of Veterans Affairs to have been incurred in, or aggravated during, the performance of uniformed service.
Should you return to work when military service ends, the Business Office can provide full details concerning your eligibility for immediate enrollment and Plan coverage according to USERRA regulations.
H. Continuing Coverage Under COBRA
Under federal law, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA), certain Employees and their families covered under POMCO Standard Health Plan (the Plan) will be entitled to the opportunity to elect a temporary extension of health coverage (called "COBRA continuation coverage") where coverage under the Plan would otherwise end. This notice is intended to inform Plan Participants and beneficiaries, in summary fashion, of their rights and obligations under the continuation coverage provisions of COBRA, as amended and reflected in final and proposed regulations published by the Department of the Treasury. This notice is intended to reflect the law and does not grant or take away any rights under the law. The Plan Administrator is the Elmira City School District. COBRA continuation coverage for the Plan is administered by POMCO, 2425 James St., Syracuse, New York 13206. Complete instructions on COBRA, as well as election forms and other information, will be provided by the Plan Administrator to Plan Participants who become Qualified Beneficiaries under COBRA.

Elmira CSD – rev. 04/28/05 38
What is COBRA continuation coverage? COBRA continuation coverage is the temporary extension of group health plan coverage that must be offered to certain Plan Participants and their eligible family members (called "Qualified Beneficiaries") at group rates. The right to COBRA continuation coverage is triggered by the occurrence of a life event that results in the loss of coverage under the terms of the Plan (the "Qualifying Event"). The coverage must be identical to the Plan coverage that the Qualified Beneficiary had immediately before the Qualifying Event, or if the coverage has been changed, the coverage must be identical to the coverage provided to similarly situated active employees who have not experienced a Qualifying Event (in other words, similarly situated non-COBRA beneficiaries). Who can become a Qualified Beneficiary? In general, a Qualified Beneficiary can be:
1. Any individual who, on the day before a Qualifying Event, is covered under a Plan by virtue of being on that day either a covered Employee, the Spouse of a covered Employee, or a Dependent child of a covered Employee. If, however, an individual is denied or not offered coverage under the Plan under circumstances in which the denial or failure to offer constitutes a violation of applicable law, then the individual will be considered to have had the Plan coverage and will be considered a Qualified Beneficiary if that individual experiences a Qualifying Event.
2. Any child who is born to or placed for adoption with a covered Employee during a period of
COBRA continuation coverage, and any individual who is covered by the Plan as an alternate recipient under a qualified medical support order. If, however, an individual is denied or not offered coverage under the Plan under circumstances in which the denial or failure to offer constitutes a violation of applicable law, then the individual will be considered to have had the Plan coverage and will be considered a Qualified Beneficiary if that individual experiences a Qualifying Event.
3. A covered Employee who retired on or before the date of substantial elimination of Plan
coverage which is the result of a bankruptcy proceeding under Title 11 of the U.S. Code with respect to the Employer, as is the Spouse, surviving Spouse or Dependent child of such a covered Employee if, on the day before the bankruptcy Qualifying Event, the Spouse, surviving Spouse or Dependent child was a beneficiary under the Plan.
The term "covered Employee" includes not only common-law employees (whether part-time or full-time) but also any individual who is provided coverage under the Plan due to his or her performance of services for the employer sponsoring the Plan (e.g., self-employed individuals, independent contractor, or corporate director). An individual is not a Qualified Beneficiary if the individual's status as a covered Employee is attributable to a period in which the individual was a nonresident alien who received from the individual's Employer no earned income that constituted income from sources within the United States. If, on account of the preceding reason, an individual is not a Qualified Beneficiary, then a Spouse or Dependent child of the individual will also not be considered a Qualified Beneficiary by virtue of the relationship to the individual. A domestic partner is not a Qualified Beneficiary. Each Qualified Beneficiary (including a child who is born to or placed for adoption with a covered Employee during a period of COBRA continuation coverage) must be offered the opportunity to make an independent election to receive COBRA continuation coverage. What is a Qualifying Event? A Qualifying Event is any of the following if the Plan provided that the Plan participant would lose coverage (i.e., cease to be covered under the same terms and conditions as in effect immediately before the Qualifying Event) in the absence of COBRA continuation coverage:
1. The death of a covered Employee.

Elmira CSD – rev. 04/28/05 39
2. The termination (other than by reason of the Employee's gross misconduct), or reduction of hours, of a covered Employee's employment.
3. The divorce or legal separation of a covered Employee from the Employee's Spouse.
4. A covered Employee's enrollment in any part of the Medicare program.
5. A Dependent child's ceasing to satisfy the Plan's requirements for a Dependent child (for
example, attainment of the maximum age for dependency under the Plan).
6. A proceeding in bankruptcy under Title 11 of the U.S. Code with respect to an Employer from whose employment a covered Employee retired at any time.
If the Qualifying Event causes the covered Employee, or the covered Spouse or a Dependent child of the covered Employee, to cease to be covered under the Plan under the same terms and conditions as in effect immediately before the Qualifying Event (or in the case of the bankruptcy of the Employer, any substantial elimination of coverage under the Plan occurring within 12 months before or after the date the bankruptcy proceeding commences), the persons losing such coverage become Qualified Beneficiaries under COBRA if all the other conditions of the COBRA are also met. For example, any increase in contribution that must be paid by a covered Employee, or the Spouse, or a Dependent child of the covered Employee, for coverage under the Plan that results from the occurrence of one of the events listed above is a loss of coverage. The taking of leave under the Family and Medical Leave Act of 1993 ("FMLA") does not constitute a Qualifying Event. A Qualifying Event will occur, however, if an Employee does not return to employment at the end of the FMLA leave and all other COBRA continuation coverage conditions are present. If a Qualifying Event occurs, it occurs on the last day of FMLA leave and the applicable maximum coverage period is measured from this date (unless coverage is lost at a later date and the Plan provides for the extension of the required periods, in which case the maximum coverage date is measured from the date when the coverage is lost.) Note that the covered Employee and family members will be entitled to COBRA continuation coverage even if they failed to pay the employee portion of premiums for coverage under the Plan during the FMLA leave. What is the procedure for obtaining COBRA continuation coverage? The Plan has conditioned the availability of COBRA continuation coverage upon the timely election of such coverage. An election is timely if it is made during the election period. What is the election period and how long must it last? The election period is the time period within which the Qualified Beneficiary can elect COBRA continuation coverage under the Plan. The election period must begin not later than the date the Qualified Beneficiary would lose coverage on account of the Qualifying Event and must not end before the date that is 60 days after the later of the date the Qualified Beneficiary would lose coverage on account of the Qualifying Event or the date notice is provided to the Qualified Beneficiary of her or his right to elect COBRA continuation coverage. Note: If a covered employee who has been terminated or experienced a reduction of hours qualifies for a trade readjustment allowance or alternative trade adjustment assistance under a federal law called the Trade Act of 2002, and the employee and his or her covered dependents have not elected COBRA coverage within the normal election period, a second opportunity to elect COBRA coverage will be made available for themselves and certain family members, but only within a limited period of 60 days or less and only during the six months immediately after their group health plan coverage ended. Any person who qualifies or thinks that he and/or his family members may qualify for assistance under this special provision should contact the Plan Administrator for further information.

Elmira CSD – rev. 04/28/05 40
Is a covered Employee or Qualified Beneficiary responsible for informing the Plan Administrator of the occurrence of a Qualifying Event? The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Plan Administrator or its designee has been timely notified that a Qualifying Event has occurred. The employer (if the employer is not the Plan Administrator) will notify the Plan Administrator of the Qualifying Event within 30 days following the date coverage ends when the Qualifying Event is:
(1) the end of employment or reduction of hours of employment,
(2) death of the employee,
(3) commencement of a proceeding in bankruptcy with respect to the employer, or
(4) enrollment of the employee in any part of Medicare. IMPORTANT: For the other Qualifying Events (divorce or legal separation of the employee and spouse or a dependent child's losing eligibility for coverage as a dependent child), you or someone on your behalf must notify the Plan Administrator or its designee in writing within 60 days after the Qualifying Event occurs, using the procedures specified below. If these procedures are not followed or if the notice is not provided in writing to the Plan Administrator or its designee during the 60-day notice period, any spouse or dependent child who loses coverage will not be offered the option to elect continuation coverage. You must send this notice to the Plan Sponsor.
NOTICE PROCEDURES: Any notice that you provide must be in writing. Oral notice, including notice by telephone, is not acceptable. You must mail, fax or hand-deliver your notice to the person, department or firm listed below, at the following address:
Elmira City School District Business Office 951 Hoffman St
Elmira, NY 14905 If mailed, your notice must be postmarked no later than the last day of the required notice period. Any notice you provide must state: • the name of the plan or plans under which you lost or are losing coverage, • the name and address of the employee covered under the plan, • the name(s) and address(es) of the Qualified Beneficiary(ies), and • the Qualifying Event and the date it happened. If the Qualifying Event is a divorce or legal separation, your notice must include a copy of the divorce decree or the legal separation agreement. Be aware that there are other notice requirements in other contexts, for example, in order to qualify for a disability extension.
Once the Plan Administrator or its designee receives timely notice that a Qualifying Event has occurred, COBRA continuation coverage will be offered to each of the qualified beneficiaries. Each Qualified Beneficiary will have an independent right to elect COBRA continuation coverage. Covered employees may elect COBRA continuation coverage for their spouses, and parents may elect COBRA continuation

Elmira CSD – rev. 04/28/05 41
coverage on behalf of their children. For each Qualified Beneficiary who elects COBRA continuation coverage, COBRA continuation coverage will begin on the date that plan coverage would otherwise have been lost. If you or your spouse or dependent children do not elect continuation coverage within the 60-day election period described above, the right to elect continuation coverage will be lost. Is a waiver before the end of the election period effective to end a Qualified Beneficiary's election rights? If, during the election period, a Qualified Beneficiary waives COBRA continuation coverage, the waiver can be revoked at any time before the end of the election period. Revocation of the waiver is an election of COBRA continuation coverage. However, if a waiver is later revoked, coverage need not be provided retroactively (that is, from the date of the loss of coverage until the waiver is revoked). Waivers and revocations of waivers are considered made on the date they are sent to the Plan Administrator or its designee, as applicable. When may a Qualified Beneficiary's COBRA continuation coverage be terminated? During the election period, a Qualified Beneficiary may waive COBRA continuation coverage. Except for an interruption of coverage in connection with a waiver, COBRA continuation coverage that has been elected for a Qualified Beneficiary must extend for at least the period beginning on the date of the Qualifying Event and ending not before the earliest of the following dates:
(1) The last day of the applicable maximum coverage period.
(2) The first day for which Timely Payment is not made to the Plan with respect to the Qualified Beneficiary.
(3) The date upon which the Employer ceases to provide any group health plan (including a
successor plan) to any employee.
(4) The date, after the date of the election, that the Qualified Beneficiary first becomes covered under any other Plan that does not contain any exclusion or limitation with respect to any pre-existing condition, other than such an exclusion or limitation that does not apply to, or is satisfied by, the Qualified Beneficiary.
(5) The date, after the date of the election, that the Qualified Beneficiary first enrolls in the Medicare
program (either part A or part B, whichever occurs earlier).
(6) In the case of a Qualified Beneficiary entitled to a disability extension, the later of:
(a) (i) 29 months after the date of the Qualifying Event, or (ii) the first day of the month that is more than 30 days after the date of a final determination under Title II or XVI of the Social Security Act that the disabled Qualified Beneficiary whose disability resulted in the Qualified Beneficiary's entitlement to the disability extension is no longer disabled, whichever is earlier; or
(b) the end of the maximum coverage period that applies to the Qualified Beneficiary
without regard to the disability extension. The Plan can terminate for cause the coverage of a Qualified Beneficiary on the same basis that the Plan terminates for cause the coverage of similarly situated non-COBRA beneficiaries, for example, for the submission of a fraudulent claim. In the case of an individual who is not a Qualified Beneficiary and who is receiving coverage under the Plan solely because of the individual's relationship to a Qualified Beneficiary, if the Plan's obligation to make

Elmira CSD – rev. 04/28/05 42
COBRA continuation coverage available to the Qualified Beneficiary ceases, the Plan is not obligated to make coverage available to the individual who is not a Qualified Beneficiary. What are the maximum coverage periods for COBRA continuation coverage? The maximum coverage periods are based on the type of the Qualifying Event and the status of the Qualified Beneficiary, as shown below.
(1) In the case of a Qualifying Event that is a termination of employment or reduction of hours of employment, the maximum coverage period ends 18 months after the Qualifying Event if there is not a disability extension and 29 months after the Qualifying Event if there is a disability extension.
(2) In the case of a covered Employee's enrollment in the Medicare program before experiencing a
Qualifying Event that is a termination of employment or reduction of hours of employment, the maximum coverage period for Qualified Beneficiaries other than the covered Employee ends on the later of:
(a) 36 months after the date the covered Employee becomes enrolled in the Medicare
program; or
(b) 18 months (or 29 months, if there is a disability extension) after the date of the covered Employee's termination of employment or reduction of hours of employment.
(3) In the case of a bankruptcy Qualifying Event, the maximum coverage period for a Qualified
Beneficiary who is the covered retiree ends on the date of the retiree's death. The maximum coverage period for a Qualified Beneficiary who is the covered Spouse, surviving Spouse or Dependent child of the retiree ends on the earlier of the Qualified Beneficiary's death or 36 months after the death of the retiree.
(4) In the case of a Qualified Beneficiary who is a child born to or placed for adoption with a
covered Employee during a period of COBRA continuation coverage, the maximum coverage period is the maximum coverage period applicable to the Qualifying Event giving rise to the period of COBRA continuation coverage during which the child was born or placed for adoption.
(5) In the case of any other Qualifying Event than that described above, the maximum coverage
period ends 36 months after the Qualifying Event. Under what circumstances can the maximum coverage period be expanded? If a Qualifying Event that gives rise to an 18-month or 29-month maximum coverage period is followed, within that 18- or 29-month period, by a second Qualifying Event that gives rise to a 36-months maximum coverage period, the original period is expanded to 36 months, but only for individuals who are Qualified Beneficiaries at the time of both Qualifying Events. In no circumstance can the COBRA maximum coverage period be expanded to more than 36 months after the date of the first Qualifying Event. The Plan Administrator must be notified of the second qualifying event within 60 days of the second qualifying event. This notice must be sent to the Plan Sponsor. How does a Qualified Beneficiary become entitled to a disability extension? A disability extension will be granted if an individual (whether or not the covered Employee) who is a Qualified Beneficiary in connection with the Qualifying Event that is a termination or reduction of hours of a covered Employee's employment, is determined under Title II or XVI of the Social Security Act to have been disabled at any time during the first 60 days of COBRA continuation coverage. To qualify for the disability extension, the Qualified Beneficiary must also provide the Plan Administrator with notice of the disability determination on a date that is both within 60 days after the date of the determination and before the end of the original 18-month maximum coverage. This notice should be sent to the Plan Sponsor.

Elmira CSD – rev. 04/28/05 43
Does the Plan require payment for COBRA continuation coverage? For any period of COBRA continuation coverage under the Plan, qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation coverage. Qualified beneficiaries will pay up to 102% of the applicable premium and up to 150% of the applicable premium for any expanded period of COBRA continuation coverage covering a disabled Qualified Beneficiary due to a disability extension. The Plan will terminate a Qualified Beneficiary's COBRA continuation coverage as of the first day of any period for which timely payment is not made. Must the Plan allow payment for COBRA continuation coverage to be made in monthly installments? Yes. The Plan is also permitted to allow for payment at other intervals. What is Timely Payment for payment for COBRA continuation coverage? Timely Payment means a payment made no later than 30 days after the first day of the coverage period. Payment that is made to the Plan by a later date is also considered Timely Payment if either under the terms of the Plan, covered employees or Qualified Beneficiaries are allowed until that later date to pay for their coverage for the period or under the terms of an arrangement between the Employer and the entity that provides Plan benefits on the Employer's behalf, the Employer is allowed until that later date to pay for coverage of similarly situated non-COBRA beneficiaries for the period. Notwithstanding the above paragraph, the Plan does not require payment for any period of COBRA continuation coverage for a Qualified Beneficiary earlier than 45 days after the date on which the election of COBRA continuation coverage is made for that Qualified Beneficiary. Payment is considered made on the date on which it is postmarked to the Plan. If Timely Payment is made to the Plan in an amount that is not significantly less than the amount the Plan requires to be paid for a period of coverage, then the amount paid will be deemed to satisfy the Plan's requirement for the amount to be paid, unless the Plan notifies the Qualified Beneficiary of the amount of the deficiency and grants a reasonable period of time for payment of the deficiency to be made. A "reasonable period of time" is 30 days after the notice is provided. A shortfall in a Timely Payment is not significant if it is no greater than the lesser of $50 or 10% of the required amount. Must a qualified beneficiary be given the right to enroll in a conversion health plan at the end of the maximum coverage period for COBRA continuation coverage? If a Qualified Beneficiary's COBRA continuation coverage under a group health plan ends as a result of the expiration of the applicable maximum coverage period, the Plan will, during the 180-day period that ends on that expiration date, provide the Qualified Beneficiary with the option of enrolling under a conversion health plan if such an option is otherwise generally available to similarly situated non-COBRA beneficiaries under the Plan. If such a conversion option is not otherwise generally available, it need not be made available to Qualified Beneficiaries. If You Have Questions. If you have questions about your COBRA continuation coverage, you should contact the COBRA Administrator or you may contact the nearest Regional or District Office of the U.S. Department of Labor's Employee Benefits Security Administration (EBSA). Addresses and phone numbers of Regional and District EBSA Offices are available through EBSA's website at www.dol.gov/ebsa. Keep Your Plan Administrator Informed of Address Changes. In order to protect your family's rights, you should keep the Plan Administrator informed of any changes in the addresses of family members. You should also keep a copy, for your records, of any notices you send to the Plan Administrator. COBRA Coverage and Pre-existing Conditions. The Health Insurance Portability and Accountability Act of 1996 (HIPAA), a federal law, makes it easier for an employee to change jobs and become Covered by a new employer’s plan even if the employee or his or her dependents have a pre-existing medical condition.

Elmira CSD – rev. 04/28/05 44
COBRA beneficiaries must notify POMCO when they become Covered by another employer or other Group plan. HIPAA requires that the time, in which you and your Dependents had continuous health Coverage (including COBRA) before changing jobs, will reduce, day by day, the new plan’s pre-existing condition exclusions. In this situation, COBRA Coverage ends for a beneficiary when that beneficiary becomes Covered under the new employer’s group health plan and pre-existing limitations do not apply to that beneficiary. In general, if a beneficiary or participant had health Coverage for the previous 12 months, he or she will be Covered by a new employer’s plan without regard to any pre-existing conditions. Contact your new employer to verify your Coverage and any applicable pre-existing exclusions. If you or your Dependents become eligible under a new plan, you should contact POMCO to send you a Coverage certification under this Plan. When your COBRA Coverage ends, you will be provided with a Coverage certification that will describe the duration of your Coverage under COBRA. Your new employer may request Coverage certifications.
Please Note Any individual who elects to continue Coverage under COBRA will be eligible for the same Coverage in effect at the time that person first lost Plan eligibility status. Subsequent Plan Amendments apply to COBRA continuation in the same manner as for individuals who maintained Plan Coverage eligibility requirements. Benefits will not be payable for Covered Expenses Incurred during a period of COBRA continuation until the applicable Contribution payment has been made for that period of continuation.
This continuation Coverage could be secondary payer after other group plans or Medicare. See Section VII Coordination of Benefits. If a COBRA participant is already eligible for Medicare when COBRA continuation takes effect, the Medicare Secondary Payer Rules for persons without employment status may apply. If not already enrolled in Medicare, persons without employment status should do so immediately. Refer to Section VI - Medicare Integration with Plan Benefits. If a person becomes eligible for Medicare or another health plan after COBRA continuation takes effect, Coverage under this Plan will end on the effective date of Medicare eligibility.

Elmira CSD – rev. 04/28/05 45
SECTION III - BENEFIT MANAGEMENT PROGRAM The Benefit Management Program is designed to answer questions and explore your choices when you or your Dependents face Hospitalization, surgery or extensive medical care. The Benefit Management Program consists of Preadmission Review, Concurrent Review, and Medical Case Management. It applies to all participants whose primary coverage is this Plan. Participants are advised to contact POMCO's Benefit Management Program, prior to having non-emergency/urgent care, to obtain a precertification for medical care. This will assure that you or your dependent will know whether or not a service will be covered before the care is provided, based on the information provided at the time of the preadmission review. It does not apply if your primary coverage is Medicare or another group health benefit plan.
Please note Do not contact the School District regarding claims pertaining to your or your dependent’s personal medical care.
The program is administered by:
POMCO Benefit Management Unit P.O. Box 6329
Syracuse, NY 13217-6329 Telephone Toll-Free: 1-866-317-7386
This is a 24-hour service. If you wish to talk to a POMCO nurse, you must call between 8:00 A.M. and 4:30 P.M., Monday through Friday. Otherwise, please provide complete information as requested by the voice mail recording. When calling the POMCO Benefit Management Unit, be prepared to supply the following information:
• Enrollee’s Social Security number (shown on the Plan Identification Card) • Patient's name and address • Physician's name, address, and phone number • Name of Hospital or other provider • Anticipated date of admission or date admitted or date that the service scheduled to start
Please Note
Federal Newborns’ and Mothers’ Provision. Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However, Federal Law generally does not prohibit the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and insurers may not, under Federal law, require that a provider obtain authorization from the plan or issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours). Under Section III - Benefit Management Program, this Plan requires notification of a Hospital length of stay that follows the first 72 hours after a normal delivery or 96 hours after a cesarean section.
A. Preadmission Review The preadmission review is a preliminary evaluation by the POMCO Benefit Management staff to decide whether an inpatient setting is Medically Necessary according to the provisions of the Plan. The admission will be certified if the Medical Necessity of the inpatient setting is established, based on the available information. If the Medical Necessity is not established based on available information, the inpatient admission will not be certified. Written notification of the POMCO Benefit Management Unit decision will be mailed to you, your Physician, and the facility.

Elmira CSD – rev. 04/28/05 46
1. Participant Telephone Requirement for Elective/Scheduled Admissions. If this Plan is primary, you
must call POMCO:
a. Before an admission to a Hospital, Birth Center, Skilled Nursing Facility, psychiatric or substance abuse facility, or any other inpatient facility.
b. Within 72 hours after an emergency or urgent admission, or for inpatient care following the first 72 hours after a normal delivery or 96 hours after a Caesarean section for delivery of newborn. For all other maternity admissions, follow instructions shown in a. above.
c. Within 24 hours following the first 96 hours of inpatient care for newborns.
Please Note A family member, doctor or hospital staff member, or other individual may initiate the required phone call. However, it is your responsibility to confirm that the call was made. This review applies to any Hospital or other covered facility in the USA, including Hawaii and Alaska.
2. Non-compliance Benefit Reduction. In the event of non-compliance with the Prenotification/Benefit
Management Program, benefits beyond the medically appropriate length of stay will be reduced to eighty percent (80%) of the normal benefit up to a maximum reduction of $500 for the following services: hospital in-patient, surgery, assistant surgery, anesthesia, in-hospital visits by physicians. The penalties for non-compliance (maximum of $500) will not be paid under any part of your benefit plan, nor will these amounts be included in your annual out-of-pocket maximum medical expenses.
Please Note
Preadmission certification does not guarantee benefits to you or your provider and will not result in payment of benefits that would not otherwise be payable. It is a preliminary review of the inpatient setting based entirely on the limited information provided to the Benefit Management Unit at the time of the preadmission review. If medical documentation at the time services are rendered is other than provided during this initial review, and it is decided according to Plan provisions and limitations that the hospitalization was not Medically Necessary or excluded under the Plan, benefits may be denied.
B. Concurrent Review
If you or your eligible dependent are confined in a hospital or other approved facility, the POMCO Benefit Management Unit staff will monitor the patient's progress, severity of illness, and intensity of services through their concurrent review procedures. Based on this review, if it is decided that inpatient care is no longer Medically Necessary, you, the attending Physician, and the inpatient facility will be notified no later than the day before the day on which inpatient benefits will cease.
C. Medical Case Management
If you or your eligible dependent require extended care or home care, the POMCO Benefit Management Unit staff will help you make decisions regarding treatment plans and facilities for coordinating medical services and Plan benefits. This can be initiated by you or by the Benefit Management Unit. Participation is voluntary and can be ended anytime. Coordination of services could include alternate treatment or an alternate facility. The Benefit Management Unit staff will work with you and your Physician to assist you with services Covered by the Plan.
Elmira CSD – rev. 04/28/05 47
SECTION IV - COVERED SERVICES The Plan pays benefits for a broad range of healthcare services that are Medically Necessary to treat an illness or injury when such care is recommended by the attending Physician. This section shows the types of services Covered by the Plan. This listing does not guarantee Plan payment: all of the listed Service or Supplies are subject to Plan exclusions and limitations. Be sure to read this entire MPD for full details on Copayments and benefit limits, Covered Services, exclusions and other limitations. Section I - Summary of Benefits and Section V - Plan Exclusions contain information on benefit limits. Section X - Definitions provides further explanation of terms that apply to your coverage under this Plan. Except as shown otherwise in Section I - Summary of Benefits, Allowable Fees for covered services are subject to the Plan Copayments and benefit maximums. All benefits are based on Allowable Fees for Covered Services and Supplies. Charges that exceed Allowable Fees are not Covered. A separate deductible applies to Major Medical expenses provided by participating and non-participant providers.
A. Pre-existing Condition Limitations
These limitations do not affect benefits for any conditions that are unrelated to the pre-existing condition. 1. Plan Pre-existing Exclusion. A pre-existing condition is a mental or physical condition for which
medical advice, diagnosis, care, or treatment was recommended or received within the six-month period ending on the enrollment date of a Covered person. Medical expenses for pre-existing conditions are excluded unless they incurred on or after the earliest of the following:
a. Until eleven consecutive months have passed during which the covered person is continuously
enrolled in the Plan, or b. For removal of tonsils or adenoids, until six consecutive months have passed during which the
covered person is continuously enrolled in the Plan. 2. Conditions not Considered Pre-existing. Federal law requires that certain conditions cannot be treated
as pre-existing conditions. A pre-existing limitations does not apply to covered expenses incurred for:
a. Pregnancy, no matter when the baby was conceived. b. Newborns, newly adopted children, or children placed for adoption (under age 18), if they are
enrolled as dependents within 30 days from the date of birth, adoption, or placement for adoption. c. Genetic information, if there has been no diagnosis of a condition.
3. Reduction by Prior Creditable Coverage. Federal law requires that this Plan allow a pre-existing
limitation period to be reduced by proof of creditable coverage. Any portion of the pre-existing condition period will be reduced on a day-by-day basis by any aggregate creditable coverage that the Covered Person had before he enrolled in this Plan.
Creditable coverage is defined as any prior group or individual health coverage that has not been followed by a break in coverage of more than 62 days, ending on the date the person enrolled in this Plan. Group or individual coverage means group health plans, federal employee and military plans, public health plans and individual or personal health plans, and short-term and limited term personal health policies. Creditable coverage does not include coverages such as disability or accident income insurance, liability insurance, workers’ compensation or similar insurance, limited scope dental or vision plans, long term care only or similar plans.
Elmira CSD – rev. 04/28/05 48
To receive a reduction credit, you must present written proof of creditable coverage for you or for your eligible dependent at the time of enrollment. This proof should be provided by previous employers, insurance companies or other entities that provided health coverage for you or your eligible dependents. They are required by federal law to provide certification of their periods of creditable coverage, including COBRA, whenever coverage ends. If you or your dependents do not receive such proof, you should contact them for this certification.
B. Participating Provider Network Program
The local Participating Provider Network is offered through your District's Health Plan, as well as through the POMCO/Allied Network. These networks are subject to change. The POMCO/Allied Network is a nationwide network of Participating Providers and Hospitals, consisting of more than 108,000 Professional Healthcare Providers and 33,600 Hospitals and ancillary facilities. You or your Dependents are free to choose either a Network Provider or an Out-of-Network Provider. However, as Network Provider’s fees are generally lower than Out-of-Network Provider’s fees, you save costs for you and the Plan. A directory of area Network Providers is available at the Business Office or you may call POMCO for information on Network Providers near you. You may also find the POMCO/Allied Network directory on the POMCO website: www.pomcoplus.com. Participating Providers (Network Providers) have a written agreement to accept a scheduled or negotiated (Network) allowance as their charge for most Covered Services or Supplies. Available Plan benefits are paid directly to the Network Provider. The Network Provider submits claims directly to POMCO. Each Network Provider maintains his own professional liability insurance coverage. Neither POMCO nor the POMCO/Multiplan Allied Network gives advice relating to medical care; they are administrative bodies only. Elmira City School District's Preferred Provider Network provides benefits for Covered Services which will, in most circumstances, be considered as payment in full, after your applicable Copayments. If you or your Dependents choose any Network Provider for healthcare, you need only pay the Network Copayment amount, if applicable. Benefit limits and Copayment amounts are shown in Section I - Summary of Benefits. If you do not choose an Elmira City School District's Health Plan Preferred Provider, you will be responsible for charges that exceed the Usual, Customary and Reasonable fees plus any applicable medical expense Percentage Copayment balance, including any out of pocket expenses. The Plan review requirements, limitations and exclusions apply to services rendered by both Network Providers and Out-of-Network Providers. Use of a Network Provider is not a guarantee of benefits. Benefits will be allowed only to the extent the service or supply is Covered under the terms and provisions of the Plan.
C. Maternity Care
Maternity Care is covered in the same manner as any other Illness. Benefits are available for you and your eligible Spouse. Dependent children are not covered for maternity care. The Plan excludes any expenses related to elective abortions. The Plan excludes expenses related to surrogate maternity care. Coverage includes services by certified Birth Center and/or certified nurse midwife on the same basis as services by a Hospital or Physician. Federal Newborns’ and Mothers’ Provision. Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a Caesarean section. However, Federal Law generally does not prohibit the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and insurers may not, under Federal law, require that a provider obtain authorization from the plan or issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours). Under Section III - Benefit Management Program, this Plan requires notification of a Hospital length of stay that follows the first 72 hours after a normal delivery or 96 hours after a cesarean

Elmira CSD – rev. 04/28/05 49
section. D. Federal Mastectomy Provision
According to the Women’s Health and Cancer Rights Act, a health plan providing medical and surgical benefits with respect to a mastectomy covered by that plan must also provide the following coverage to a health plan participant who elects breast reconstruction in connection with the covered mastectomy: 1. Reconstruction of the breast on which the mastectomy has been performed. 2. Surgery or reconstruction of the other breast to produce symmetrical appearance; and 3. Coverage for prostheses and physical complications of all stages of the mastectomy, including
lymphedema; 4. Coverage to be provided in a manner determined in consultation with the attending Physician and the
patient.
E. Alternative Treatment Provision
If alternative procedures, services, or treatments can properly treat an Illness or Injury, the Plan will cover such alternatives if they are more cost effective or medically sound, even if such procedures, services, or treatments are not specifically covered (in part or in full) under this Plan. The Plan Administrator shall authorize alternative treatments, subject to agreement by the Covered Person. Examples of alternate treatments are chiropractic care, acupuncture (for pain relief or anesthesia), and biofeedback.
F. Preventive Care (Well or Routine Care) Coverage is available for limited routine screening exams for preventive or well care. Preventive or well care is routine care unrelated to the diagnosis or treatment of specific symptoms or specific Illness or Injury. Expenses related to specific symptoms or treatment of an Illness or Injury are Covered separately. If care or management of an Illness or Injury requiring minimal time or minimal professional expertise is done during a visit that is primarily for routine preventive or well care, the visit will be considered as routine preventive care, subject to Plan limitations. Only the following routine services are Covered for preventive or well care. Refer to Section I - Summary of Benefits for benefit limits. 1. Well Child Care. Benefits are available for routine well child care rendered for eligible and enrolled
Dependent children from birth to age 24 months includes only the following services:
a. Newborn Nursery Care. Benefits are available for inpatient care by physicians including routine newborn exam and visits up to four days in a hospital or birth center. Payment will not be made for routine care after four days. For example, routine care extended due to the mother’s continued Hospital stay will not be Covered. However, if the child is ill, usual Plan benefits will apply. Plan includes coverage for routine circumcisions. Routine Newborn care billed by an anesthesiologist or the delivering Physician is not Covered.
b. Routine Well Child Care/Immunizations. Routine well child care in a Physician’s office, Hospital,
or clinic is limited to six visits and up to $300 maximum benefit after discharge up to 24-months of age. For example: 1) Usual well child laboratory screening and testing. 2) Usual routine well child physical exams. 3) Developmental assessments. 4) Age appropriate immunizations for diphtheria, tetanus, pertussis, polio, measles, mumps, rubella,
hepatitis b, Haemophilus influenza type b., or other immunizations based on the most recent

Elmira CSD – rev. 04/28/05 50
schedule for immunizations recommended by the American Academy of Pediatrics. Please note
Immunizations for children are provided by the County Health Department at no charge.
2. Routine Mammography Screening. Benefits are available for Allowable Fees billed by a Hospital, clinic or Physician for an annual routine mammography screening for Covered Persons 35 years of age or older.
3. Routine Adult Physicals or Exams. Benefits are available for routine or preventive physical
examinations rendered by Physicians, including related diagnostic tests, for Employees and retirees age 50 years and older. Prostate exams and related testing and colorectal screening to include sigmoidoscopy and fecal occult test are Covered. Immunizations are not Covered. Routine gynecological exams, Pap smears, and mammography are Covered under subsections 2. and 4.
4. Routine Gynecological Examination. Benefits are available for one annual routine gynecological
examination for Employees, retirees, and dependent spouses only. Dependent children are not covered for this benefit. Pap smear and tests related to the exam are covered under Diagnostic Laboratory and X-ray benefits.
G. Hospital and Other Facilities
Remember that all inpatient admissions require a phone call as part of the Benefit Management Program. Refer to Section III - Benefit Management Program for details. 1. Acute Care General Hospital (Hospital). Benefits are available for Inpatient care billed by a Hospital.
Services or Supplies must be furnished by the Hospital and given by its employees. Refer to Section I - Summary of Benefits for limits.
Separate charges for professional services of the Hospital‘s employees are not Covered under this section.
Separate charges for Inpatient private duty nursing are covered separately. Separate professional charges for interpretation of Hospital testing and other medical services are not considered Hospital expenses; these charges are considered Physician charges and are considered separately from Inpatient Hospital expenses. Charges for take home Supplies, equipment or drugs are not considered Inpatient expenses and are considered for benefits separately from Inpatient Hospital expenses.
Benefits are available for the following Service or Supplies:
a. Inpatient Hospital Expenses. Medical Service or Supplies received by a Covered Person during an Inpatient stay when ordered by the attending Physician and found Medically Necessary for short term acute care of Illness or Injury. If you or your Dependent review your in-patient Hospital bill to ensure that charges billed were actually rendered and you disclose any overcharges to the Plan, you or your dependent will be paid 50% of any savings to the Plan.
1) Room and Board, including general nursing, in rooms of two or more beds, semi-private,
intensive care units, cardiac care unit or similar rooms. Charges for a private room will be Covered if a private room is deemed to be Medically Necessary. Room and Board charges billed after the time of discharge are not Covered.
2) Hospital Miscellaneous or Ancillary medical Services or Supplies received while the patient is
eligible for room and board benefits may be allowed when ordered by the attending Physician and found Medically Necessary for treatment of Illness or Injury. This includes, but is not limited to, drugs and medicines; biologicals, sera, intravenous preparations, lab and pathology tests; use of operating room, delivery room or other treatment room and related Supplies;

Elmira CSD – rev. 04/28/05 51
administration of anesthesia, agents and related Supplies; use of physical or occupational therapy equipment and related Supplies; oxygen and Supplies to administer; administration and processing of blood but not including charges for blood and plasma; use of equipment and Supplies for x-rays and radiation therapy including visualizing dyes, radioactive or nuclear materials; use of equipment, drugs and related Supplies for non-Experimental chemotherapy: use of dialysis equipment and related Supplies. Coverage is not provided for personal expenses including, but not limited to, television, hairdressing service, telephone, and clothing.
3) Medical/Surgical Conditions are Covered, based on Medical Necessity for acute Inpatient Care.
Refer to Section I - Summary of Benefits for any benefit limits.
Please note See separate coverage limits for Mental Illness care and Substance Abuse care set forth in paragraphs 5. and 6. below.
4) Maternity/Nursery Care. Pregnancy or maternity care is Covered the same as any other Illness.
However, the Plan excludes expenses related to surrogate maternity care.
Benefits are available for your newborn child from the moment of birth. However, benefits will not be provided unless you enroll your newborn child in family coverage. You should enroll in family coverage within 31 days after the date of birth. Benefits will be available for unlimited inpatient days if the baby is sick, injured, premature or born with congenital defects and requires medical care above that needed for routine nursery care. However, coverage for Hospital Service or Supplies considered primarily Routine Newborn Nursery Care is limited to four days. After four days, continued care must be approved due to a medical condition of the Newborn that required continued Inpatient treatment. Extended days due primarily to the mother’s continued stay are not covered even if the mother is providing personal care such as breastfeeding. Newborn care includes Services or Supplies related to routine circumcision.
According to the Newborns’ & Mothers’ Health Protection Act, a federal law, a health plan or its managed care program that offers coverage for Hospital stays in connection with childbirth cannot limit that coverage to less than a 48-hour Hospital stay following an uncomplicated normal delivery; or less than a 96-hour Hospital stay following a Caesarean section delivery. In addition, the health plan cannot restrict benefits for any portion of the required minimum stays in a way that is less favorable than the benefits provided for any preceding portion of the stay. Under Section III - Benefit Management Program, this Plan requires notification of a Hospital length of stay that follows the first 72 hours after a normal delivery or 96 hours after a cesarean section.
5) Mental Illness or Psychiatric Care is only allowed when the patient requires such care for the
protection of himself or others or when the course of treatment can only be carried out on an Inpatient basis. Refer to Section I - Summary of Benefits for benefit limits.
Benefits are available for Covered Inpatient stays in a Hospital or private proprietary psychiatric
facility. Please refer to subsection H. - Other Medical/Surgical Services and Supplies, paragraph 6b. pertaining to Physician charges.
6) Substance Abuse Detoxification. Inpatient detoxification is considered a medical condition
eligible for acute care Hospital benefits. However, detoxification coverage is limited to no more than seven days in a Calendar Year. Expenses for Inpatient Substance Abuse (alcohol or drug abuse) rehabilitation are Covered separately. See Substance Abuse Facility shown later in this Section.

Elmira CSD – rev. 04/28/05 52
b. Outpatient Hospital Expenses. Benefits are available for Service or Supplies ordered by the attending Physician in accordance with the Plan. Services and Supplies must be provided by the Hospital and rendered by employees of the Hospital. Refer to Section I - Summary of Benefits for benefit limits. Private Physician expenses are Covered separately. Benefits are available for the following Service or Supplies:
1) Preadmission Testing. Benefits are available for preadmission testing done by the admitting
Hospital before surgery or other planned admission. Separate charges for use of Hospital emergency rooms or outpatient rooms are not Covered under this section. Preadmission testing will be considered for benefits when all of the following requirements are met:
a) The tests are ordered by a Physician as a preliminary requirement for admission as a
registered bed patient for surgery or other treatment in the same Hospital; b) Tests must be consistent with the diagnosis and treatment of the condition; c) The reservation for a Hospital bed and operating room is made before testing was done; d) The patient must be physically present at the Hospital for needed tests; and e) If the admission is for Surgery, the procedure(s) must take place within seven days after the
tests are given.
2) Emergency Medical Care. Benefits are available for the initial Emergency Medical Care found Medically Necessary for treatment of Accidental Injury and Sudden and Serious Illness. Coverage includes use of the Hospital emergency or outpatient room and related Hospital Service or Supplies for necessary treatment. The Plan will not cover the emergency center facility charge and separate physician’s charge when the condition is not considered to be Emergency Medical Care. However, diagnostic testing and medications for treatment of the non-emergency care condition will be Covered.
To be considered Emergency Medical Care, the Covered Person’s medical condition must satisfy
the circumstances shown in Section X - Definitions under of Emergency Medical Care and the following coverage limitations:
a) Serious Accidental Injury. Coverage is limited to initial treatment of an Accidental Injury
rendered within 24 hours of the accident to a Covered Person whose Injury requires immediate medical care.
b) Sudden and Serious Illness. Coverage is limited to initial treatment for a sudden,
unexpected onset of a medical condition of such nature that failure to render immediate care could reasonably result in deterioration to the point of placing the Covered Individual's life in jeopardy or cause serious impairment to the Covered Individual. In no event, shall benefits for such care be provided unless the care was rendered less then 12 hours after the first appearance of the symptoms of the illness.
3) Surgery. Coverage includes use of the emergency room, outpatient room or Ambulatory
Surgery room and necessary Services or Supplies rendered during the Covered surgical procedure, including recovery. This includes surgical procedures, maternity delivery procedures, or setting of fractures or dislocations. Coverage does not include use of the emergency room or outpatient rooms for any non-emergency follow-up care including but not limited to, removal of sutures, removal of casts, recheck exams.
4) Rehabilitative Therapy. Benefits are available for physical therapy, speech therapy,
occupational therapy, and inhalation/respiration therapy rendered to improve a function lost due to an Illness or Injury. Such care must be ordered by the attending Physician and rendered by qualified therapists licensed to render such care. Care must meet same criteria as Rehabilitative

Elmira CSD – rev. 04/28/05 53
Therapy shown later in this section under Medical/Surgical Services and Supplies. Separate charges for use of Hospital emergency or outpatient rooms are not Covered under this section.
5) Other Outpatient Hospital Services and Supplies. Benefits are available for other Hospital
Service or Supplies when ordered by the attending Physician and found Medically Necessary according to Plan provisions. Coverage includes all necessary medical Supplies used during the Covered treatment. To be eligible for this benefit, the medical Service or Supplies must otherwise be Covered under the Plan. Such services will be subject to the same criteria and limitations applied to the same type of services Covered under Medical/Surgical Services and Supplies shown later in this section. Separate charges for use of Hospital emergency or outpatient rooms are not Covered under this benefit. Other services include, but are not limited to:
a) Diagnostic tests including x-rays, laboratory, pathology, and machine tests; b) Radiation or x-ray therapy for non-Experimental treatment of an Illness or Injury; c) Kidney dialysis; d) Chemotherapy for non-Experimental treatment; e) Clinic Service or Supplies, or f) Intravenous therapy.
Please Note
A person receiving kidney dialysis could be eligible for Medicare due to End Stage Renal Disease (ESRD). Refer to Section VI - Medicare Integration with Plan Benefits.
2. Birth Center Facility. Benefits are available for Service or Supplies for maternity or Pregnancy care
rendered by an approved licensed Birth Center to the extent such expenses would have been allowed if provided by a Hospital. Coverage includes services by midwives and Routine Newborn Nursery Care.
3. Ambulatory Surgical Facility. Coverage is available for Service or Supplies rendered and billed by an
Ambulatory Surgical Facility for Covered surgical procedures. Coverage includes all necessary Service or Supplies rendered by the facility related to surgical care on the day of the surgery and within 48 hours following the surgery. Coverage is limited to procedures that cannot be safely done in a Physician’s office due to complexity of procedure or the patient’s condition or when rendered for Emergency Medical Care.
4. Emergency Center or Urgent Care Facility. Coverage is available for Service or Supplies rendered
and billed by an Emergency Center or Urgent Care Facility when found Medically Necessary for treatment of an Illness or Injury. Coverage includes all necessary Supplies used during the Covered treatment. To be eligible for this benefit, medical Service or Supplies must otherwise be Covered under the Plan. Such services will be subject to the same criteria and limitations applied to the same type of services Covered under Medical/Surgical Services and Supplies shown later in this Section.
5. Skilled Nursing Facility /Convalescent Facility/Rehabilitation Facility (SNF)
a. Inpatient SNF Services. Benefits are available for Skilled Nursing Facility, convalescent facility and Rehabilitation Facility (facilities shown collectively hereafter as SNF) Inpatient Service or Supplies that meet all of the following criteria:
1) SNF admission must be ordered by the attending Physician and the patient must remain under the
care of a Physician during the SNF confinement; 2) Care must be found Medically Necessary and at a skilled level of care, according to Plan
provisions. Skilled level of care is care of an acute nature that must be furnished by skilled personnel (qualified technical or professional health personnel) on a daily basis. In no event are

Elmira CSD – rev. 04/28/05 54
benefits provided for Custodial, Maintenance, long term, nursing home or residential care; 3) Coverage may only be provided for as long as Hospitalization would have been necessary if care
in a Skilled Nursing Facility were not provided; or when rehabilitation care is so intense it requires an Inpatient stay;
4) Diagnostic and therapeutic services must be provided and billed by the facility and rendered by
employees of the facility; 5) Covered Services include the following:
a) Room and board charges, including general nursing care. Private room charges will be limited to Average Semi-private Room Rates, whatever the reason for use. You will be responsible for the payment of charges over the facility's Average Semi-private Room Rates. Room and board charges billed after the time of discharge are not Covered;
b) Rehabilitative physical, cardiac, occupational, speech, or inhalation therapies; c) Medical social services; and d) Ancillary or miscellaneous Service or Supplies, appliances, or equipment that are ordinarily
provided by the facility for its patients, furnished for use in the facility, and would be Covered if the patient was an Inpatient in a Hospital.
Obstetrical conditions or psychiatric conditions do not qualify for this benefit. Benefits are not payable for any period that care is found residential, Custodial, or Maintenance Care, according to Plan provisions. Separate charges for Inpatient private duty nursing are excluded, whatever the reason for use. Take home Supplies or drugs are not Covered under this benefit. Personal services such as telephone, TV, hairdressing service, etc. are not considered medical expenses and will not be paid.
Coverage limits that may apply are shown in the Summaries of Benefits. Private room charges are limited to Semi-private room rates, unless the private room use is Medically Necessary. Room and Board charges after the time of discharge are not covered.
b. Outpatient SNF Services.
1) Rehabilitative Therapy. Benefits are available for outpatient physical therapy, cardiac rehabilitation, speech therapy and inhalation/respiration therapy rendered to improve function lost due to an Illness or Injury. Such care must be ordered by the attending Physician and rendered by Professional Healthcare Providers licensed to render such care. Care must meet same criteria as Rehabilitative Therapy shown later in this section under Medical/Surgical Services and Supplies. Refer to Section I - Summary of Benefits for benefit limits.
2) Other Outpatient Services and Supplies. Benefits are available for other outpatient facility
Service or Supplies when found Medically Necessary according to Plan provisions. Coverage includes all necessary Supplies used during the Covered treatment. To be eligible for coverage under this title, medical Service or Supplies must otherwise be Covered under the Plan. Such services will be subject to the same criteria and limitations applied to the same type of services Covered under Medical/Surgical Services and Supplies shown later in this section.
6. Alcohol/Substance Abuse Facility. Allowable fees for inpatient and outpatient services billed by a
certified alcohol or substance abuse facility (freestanding agency or facility or a hospital center) for an approved plan of inpatient or outpatient care rendered for you or your eligible dependent are covered. Services and supplies must be provided by the facility and rendered by its employees.
a. Inpatient Care. Coverage is limited to 7 weeks per calendar year, with a 2 year maximum. Private
room charges are limited to average semi-private rates, whatever the reason for use of a private room. Room and board charges billed after the time of discharge are not covered.

Elmira CSD – rev. 04/28/05 55
b. Outpatient Care. Each outpatient visit must consist of at least one of the following: Individual or
group counseling; activity therapy; and diagnostic evaluations by a doctor or other licensed professional to decide the nature and extent of the patient's illness. Benefits are not payable for visits that consist primarily of participation in programs of a social, recreational, or companionship nature. Services must be rendered by the employees of the facility for services provided by the facility. Refer to Section I - Summary of Benefits for benefit limits.
7. Home Health Care Agency. Benefits are available for an approved plan of care for services rendered
and billed by an accredited and certified home health care agency. The attending physician must order the care and certify that the patient’s condition would require continued hospitalization or SNF inpatient care if Home Health Care was not provided. Coverage limits are indicated in the Summary of Benefits; additional days must be approved by the Claims Administrator. The following services are covered under this benefit:
a. Part-time or intermittent home nursing care by or under the supervision of a registered professional
nurse (RN). Full-time care is not covered; b. Part-time or intermittent home health aide services rendered primarily for the care of the patient.
Full-time care is not covered; c. Physical, occupational and speech therapy; d. Medical supplies, drugs and medicines that would have been allowed if the patient were confined; e. Laboratory services if they would have been covered as a bed patient in a hospital or skilled
nursing facility; and f. Each visit by a member of the home care team is considered one visit. Four hours of care by a
home health aide is considered one visit. Please refer to Section I - Summary of Benefits for benefit limits.
8. Hospice Care Agency. If you or your eligible Dependent should need the services of a certified hospice
care agency, benefits are available for a maximum 210 days of hospice care. The patient must be diagnosed as terminally ill, with six months or less to live, and palliative care is considered to be most appropriate. During this period, all the patient’s medical services must be provided by or obtained through the hospice care agency. All services must be billed by the Hospice Agency.
Benefits will be provided for the following Covered Services: a. Bed patient either in a designated hospice unit or in a regular Hospital bed; b. Day care service provided by the Hospice Agency; c. Home care and Outpatient services provided by the hospice including intermittent nursing by a
registered nurse or licensed practical nurse or by a Home Health Aide; d. Physical, occupational, speech, and respiratory therapy; e. Medical social services and nutritional services; f. Laboratory, x-ray, chemotherapy, and radiation therapy when needed to control symptoms; g. Medical supplies and drugs and medications considered approved for the patient's condition.
Benefits are not payable if the drugs or medications are of an Experimental nature; h. Durable medical equipment; i. Medical care provided by the Hospice Physician or other Physician designated to render services by
the Hospice Agency; and j. Bereavement counseling, before or after the patient’s death, for the family.
H. Other Medical/Surgical Services and Supplies Coverage is available for expenses Incurred for the following services rendered for you or your Dependents. To be Covered, services must be rendered or ordered by the attending Physician and found Medically

Elmira CSD – rev. 04/28/05 56
Necessary, according to Plan limitations. Be sure to read this section carefully. Some care or treatment, Services or Supplies are shown separately and are subject to different limitations. Covered Services or Supplies must be rendered and billed by Covered Professional Healthcare Providers. Refer to Section I - Summary of Benefits for benefit limits. 1. Surgeon Expenses. Benefits are available for Covered surgical procedures rendered for you or your
Dependents by a Doctor, podiatrist or by a Dentist whether done at a Hospital, clinic, office, or other location. When two or more surgical procedures are performed during the same operative session, the fees for the secondary procedures could be allowed at a reduced fee (usually 50% of Allowable Fees for a second procedure). The surgical allowance includes the usual care given by the surgeon before and after surgery. Separate charges by the surgeon, (or by another doctor filling in for the surgeon), for usual care after surgery (post operative care) will not be paid. Refer to Section X - Definitions under Surgery for definition of surgery.
Separate charges for any procedure considered part of or incidental to a major procedure will not be Covered. An incidental procedure (i.e., incidental appendectomy, lysis of adhesion, extension of previous scar, puncture of ovarian cyst) is one that does not substantially increase the time of the operative session or the amount of post-operative care for the patient and/or is undertaken primarily as a precautionary measure or for general health and well being of the patient.
2. Maternity Expenses. Benefits are available for services by a medical doctor, or certified nurse midwife,
for childbirth, caesarean section and other maternity care rendered for you or your Spouse. Expenses related to pregnancy incurred by your dependent children are excluded. Coverage is not provided for expenses connected with elective abortion. The Plan excludes Service or Supplies related to surrogate maternity care. The payment for childbirth, Caesarean section or other termination of a Pregnancy will include the usual care given by a provider before and after the obstetrical procedure (prenatal or postnatal care). Separate charges for this usual prenatal or postnatal care will not be covered.
3. Assistant Surgeon. Benefits are available for assistant surgeon services when found Medically
Necessary for performance of the Covered procedure. A Hospital or other facility regulation, in itself, does not establish Medical Necessity. If the procedure is performed in a hospital or other facility, assistant surgeon expenses are covered only when there is no qualified facility staff available to assist the surgeon. The assistance must be given and billed by another surgeon (medical doctor, osteopath, podiatrist or Dentist) qualified to assist during the Covered surgery. The benefit for the assistant surgeon will be based on 20% of the applicable surgeon allowance. Under no circumstances are Plan benefits paid for standby services. Separate charges by an assistant surgeon for postoperative Inpatient visits are not Covered.
4. Anesthesia. Benefits are available for administration of general anesthesia found Medically Necessary
for Covered surgical procedures. Coverage is limited to anesthesia administration by anesthesiologists or administration by Certified Nurse Anesthetists who have contracted with an eligible Hospital or those under the direct supervision of the operating surgeon and the indirect supervision of an anesthesiologist. The Plan will not pay charges for administration of anesthesia given by the surgeon or the assistant surgeon. The Plan will not pay administration of anesthesia rendered for non-Covered surgery. The allowance for anesthesia includes the usual patient consultation before anesthesia and the usual care after surgery. The Plan will not pay separate charges for this usual care before and after surgery. Anesthesia administration expenses are not Covered if the surgery is not Covered by the Plan.
Coverage is also available for administration of general anesthesia for non-surgical procedures when
found Medically Necessary according to Plan provisions, for example, Covered electroshock therapy.
If pre-approved, acupuncture is Covered when used as anesthesia or for palliative pain relief and

Elmira CSD – rev. 04/28/05 57
performed by a certified acupuncturist. 5. Inpatient Physician Services.
a. Medical/Surgical Care. Benefits are available for Inpatient Physician evaluation and management or therapeutic services given during an approved Inpatient stay in a Hospital or SNF. This benefit does not include surgeon, assistant surgeon, anesthesiologist or obstetrical postoperative care. If services are provided in a SNF, coverage is provided only for days approved for room and board. Benefits are not payable for any period of inpatient care found to be Custodial or long term care. Treatment or care for Inpatient Substance Abuse rehabilitation is not covered under this benefit. See Substance Abuse Facility shown previously in this section. See separate limits for Inpatient Mental Illness care shown below.
b. Mental Illness Care. Benefits are available for Inpatient visits or therapy for Mental Illness care, only
to the extent Hospital room and board days were approved. Coverage is limited to one hour per day and up to one group therapy session limited to eight persons (1 ½ hours per day) per day when part of an Approved Plan of Care.
6. Consultations. Benefits are available for consultations given in a Hospital, or SNF, Rehabilitation
Facility, clinic, home, or the consultant’s office. A consultation is an examination requested by an attending Physician to obtain an opinion or advice in the evaluation and/or treatment of an Illness or Injury. When the attending Physician refers a patient to a specialist or other Physician for the treatment of an Illness or Injury, the visits are not considered consultations.
7. Office, Outpatient, and Home Visits. Benefits are available for outpatient evaluation and management
or therapeutic medical visits when found to be Medical Necessary according to Plan provisions. Outpatient care means care given other than on an Inpatient basis. Consultations, surgery and obstetrical procedures are Covered separately. Services must be given and billed by Covered healthcare providers and found Medically Necessary according to Plan provisions. Outpatient Mental Illness care, podiatrist care or foot care, rehabilitation, and other services may be Covered separately as shown later in this section. Outpatient and Inpatient Substance Abuse rehabilitation is Covered separately under Substance Abuse Facility shown previously in this Section.
8. Foot Care and Podiatry Services. Benefits are available for treatment related to care of the feet.
Coverage includes Services or Supplies rendered and billed by licensed Physicians (medical doctors, osteopaths or podiatrists) for conditions of the feet. Coverage for foot care is provided on the same basis as care for other Illnesses or injuries. Charges for routine foot care are Covered for patients with severe systemic disorders, such as diabetes. However, Services or Supplies for routine foot care, shoes, or shoe inserts are not covered. Please refer to Section V - Plan Exclusions.
Foot orthotics are covered on a limited basis for certain conditions, but not when needed primarily for treatment of weak, strained, flat, unstable or unbalanced feet. Generally, orthotics ordered by a physician to control change in the shape of the foot during growth or take pressure off injured or inflamed parts of the foot would be allowable. For example, conditions such as; calcaneal bone spur, club foot, hallux valgus, metatarsal bursitis, Morton's neuroma, nerve injury, and osteoarthritis would be considered for benefit determination. Foot orthotics would not be allowable for conditions such as; internal derangement of the knee, ankle sprain, leg length inequality, lumbar and/or pelvic instability/dysfunction, tibial tendonitis. Replacement of a covered orthotic is allowable only when needed due to growth or due to change in patient's condition which makes the previous orthotic no longer serviceable. A predetermination of coverage is recommended to avoid any misunderstanding of allowable services.
9. Outpatient Mental Health Care. Benefits are available for outpatient Mental Illness care given for you or your Dependents. Services must be given and billed by a medical doctor (psychiatrist) or a licensed

Elmira CSD – rev. 04/28/05 58
clinical psychologist or billed by a Hospital or a mental health facility, Physician’s corporation or clinic for the services of a licensed psychiatrist, licensed clinical psychologist, or licensed psychiatric social worker. Coverage is limited to 30 visits per calendar year for each covered person. However, Coverage will be provided separately for an individual and a group therapy visit given on the same day and will count toward the 30-visit calendar year limit. Alcohol or drug addiction treatment is not Covered under this benefit. See Substance Abuse Rehabilitation Facility shown previously in this section.
10. Diagnostic Tests. Benefits are available for diagnostic x-ray, laboratory, pathology and other diagnostic testing and related medical supplies (such as electrocardiograms, pulmonary stress testing, electroencephalograms, allergy skin tests, etc.) given on an outpatient basis by Professional Healthcare Providers, Clinics, Emergency Care Center, Hospitals or other Covered facilities, or independent labs. Tests must be required or ordered due to related symptoms or treatment of an Illness or Injury or for routine or preventive tests rendered in conjunction with Covered routine physical examinations. Genetic testing is also Covered if deemed Medically Necessary. Coverage includes separate Physicians' charges for interpretations of Covered diagnostic tests given by a Hospital, Skilled Nursing Facility or other Covered facility.
11. Radiation Therapy. Benefits are available for radiation or x-ray therapy for non-Experimental treatment
of an Illness or Injury. Services or Supplies must be found Medically Necessary and rendered and billed by an outpatient Hospital, medical doctor or freestanding radiation therapy facility or clinic. Coverage includes all necessary radiation therapy procedures, related services, Supplies, and the cost for purchase or rental of substances used for the therapy. Charges for office visits, consultations and diagnostic x-rays are Covered separately.
12. Private Duty Nursing/Visiting Nurse. Coverage is available for private duty nursing when services are
ordered by a doctor and found Medically Necessary according to Plan provisions. Services must be provided by and require the skills of a registered professional nurse (RN). Skilled nursing must be needed to manage the care of acutely ill patients and must not be ordered primarily at the request of a family or household member. If rendered during a covered inpatient stay, care must be so intense that the hospital or skilled nursing facility staff could not be expected to render such care. Shortage of general nursing staff does not establish medical necessity for private duty nurses. Benefits are not payable for custodial or maintenance care or care that is primarily assistance with daily living or other care that does not require the skills of an RN. A licensed practical nurse will be allowed if the doctor certifies that a registered nurse is unavailable for an approved plan of skilled nursing care.
Coverage is also available for part-time or intermittent visiting nurse services when rendered in the patient’s home and ordered by the attending physician. Care must be billed by a certified visiting nurse agency or by a state or county visiting nurse service for professional nurse services.
13. Rehabilitation Therapy. Benefits are available for outpatient rehabilitation therapy. However, if part of an Approved Plan of Care for home health care or Hospice, coverage is provided separately. Coverage is limited to the following outpatient rehabilitation therapy services:
a. Physical Therapy. Benefits are available for physiotherapy of the type and duration prescribed by
the attending Physician. Therapy must be rendered by a licensed physical therapist or other Professional Healthcare Provider licensed to perform physical therapy and billed by the therapist or by a Hospital, SNF, clinic or other Covered provider.
Therapy must be needed to significantly and measurably restore body function lost due to an Illness or Injury. If you or your Dependent reach maximum potential for significant and measurable
Elmira CSD – rev. 04/28/05 59
improved function, or if care is found by the Claims Administrator to be Maintenance in nature, benefits will no longer be payable. If care is given beyond the type or duration ordered by the attending Physicians, benefits will not be payable for that care. Massage, exercise programs, and use of body exercise equipment are not Covered. Long-term care is not Covered.
Physical therapy is Covered, for example, when body function is lost due to conditions such as Accidental Injury, cerebrovascular accident, stroke, acute stages of arthritis, multiple sclerosis or other progressive Illness. Physical therapy is not Covered, for example, when physical dysfunction is due to conditions such as mental retardation, spina bifida, developmental delay, autism, educational or occupational deficits, or syndromes associated with perceptual and conceptual dysfunctions.
b. Speech Therapy. Benefits are available for outpatient short-term speech therapy services when
ordered by the attending Physician. Outpatient speech therapy must be given by a licensed speech therapist and billed by the therapist or by a Covered facility, clinic or other Covered provider. Therapy must be ordered and given to restore Speech Function lost due to Illness or Injury or to improve Speech Function following surgery for correction of a birth defect that caused the speech dysfunction. Speech therapy must be directed at significant and measurable restoration and improvement of Speech Function. If the patient reaches maximum potential for improved, or age appropriate, function, benefits will no longer be payable. Long-term speech therapy is not Covered.
Speech therapy is not Covered for conditions such as stammering, stuttering, lisping, articulation disorders, changing an accent, dyslexia, abnormal speech development, hearing loss that is not medically documented, or similar disorders. Benefits are not payable for myofunctional or tongue thrust therapy. Speech dysfunctions due to congenital anomalies, brain dysfunction, or developmental delays will not be paid.
Speech therapy is Covered, for example, when Speech Function is lost due to conditions such as a cerebrovascular accident, craniotomy, head Injury, meningitis, congenital anomalies corrected by surgery (such as cleft lip or cleft palate), vocal cord nodules, or surgery. Speech dysfunction due to medically documented chronic otitis media or middle ear infections, during the formative years of speech, that cause a delay in either speech or language (nonacute, nonrecurrent otitis media does not meet these criteria) would be Covered. Speech therapy is not Covered, for example, when speech dysfunction is due to conditions such as environment, psychosocial delays, mental retardation, spina bifida, autism, educational or occupational deficits, cerebral palsy, syndromes associated with perceptual and conceptual dysfunctions, dyslexia, or attention deficit disorders.
c. Inhalation Therapy. Benefits are available for short-term outpatient inhalation therapy given for
you or your Dependents when ordered by the attending Physician. Charges must be billed by a Hospital, SNF, clinic, or by a Physician for therapy services given by certified licensed respiratory therapists or other qualified Professional Healthcare Provider.
14. Chemotherapy. Benefits are available for non-Experimental chemotherapy for outpatient services given
n a clinic, outpatient department of a Hospital, or Physician’s office. Coverage includes professional chemotherapy services and related Supplies. Home chemotherapy is Covered when ordered by the attending Physician and home setting is found medically appropriate according to Plan provisions. Home therapy includes the chemotherapy Supplies, non-Experimental drugs and equipment needed to render the chemotherapy in the home.
15. Kidney Dialysis. Benefits are available for Service or Supplies related to outpatient hemodialysis
procedures given and billed by Physicians, or Hospitals, or Medicare-certified dialysis centers. Home self-dialysis is also Covered when ordered by the attending Physician and home setting found medically appropriate according to Plan provisions. If you are on home dialysis, coverage includes related laboratory tests and consumable or disposable Supplies needed for the dialysis. Equipment found Medically Necessary by the Claims Administrator may also be Covered. Benefits are not payable for

Elmira CSD – rev. 04/28/05 60
expenses such as alterations to the home, installation of electrical power, water supply, sanitation waste disposal, or air conditioning, or for convenience or comfort items.
Please Note
A person receiving kidney dialysis could be eligible for Medicare due to End Stage Renal Disease (ESRD). See Section VI - Medicare Integration with Plan Benefits.
16. Ambulance. Benefits are available for emergency ambulance transportation for you or your Dependents when found Medically Necessary, according to Plan provisions.
Coverage is provided for ambulance emergency services to the nearest Hospital that can treat the patient’s
condition. Emergency ambulance transportation to other locations may be considered based on patient’s condition, reason for transfer (e.g., to a preferred provider hospital), and Medical Necessity. For example, the Plan will not pay to have a patient transferred to another Hospital when the primary reason is to be near his or her home. However, benefits would be allowed if the transfer was necessary because the first Hospital could not provide the necessary care and the patient required transfer to the nearest Hospital that could provide the needed care.
Benefits are only payable for emergency transportation by professional ambulance or volunteer
ambulance. Benefits are not payable if the patient could have been safely transported by any other means of transportation.
17. Durable Medical Equipment (DME). Benefits are available for the rental or purchase, if appropriate, of
DME when ordered by the attending Physician and found Medically Necessary, according to Plan provisions. The equipment must customarily be used for therapy and suitable for home use. The purchase of equipment is Covered only when it cannot be rented, or when the duration the DME is needed makes the purchase less expensive than rental. Coverage will be provided based on medical documentation and Plan limitations in effect at the time the DME is purchased.
Coverage includes the necessary Supplies to operate the equipment. Duplicate equipment is not Covered. The replacement of purchased DME may be Covered only when the existing equipment is no longer serviceable due to change in body condition, or is no longer repairable. DME replacement due to negligence is excluded. The necessary repairs and maintenance of purchased equipment may be allowed, unless Covered by a warranty or purchase agreement.
Examples of Covered DME are; standard Hospital beds, respirators, canes, crutches, walkers, and wheelchairs. Such equipment, for example, does not include hearing aids, eyeglasses, contact lenses, blood pressure monitors, thermometers, shoes or other articles of clothing, communication devices, computers, air conditioners or purifiers, humidifiers, exercise equipment, comfort items or convenience items. For additional limitations on this service, See Section X - Definitions under Durable Medical Equipment.
Option B only:
If no participating provider of DME is available in-network, and services are received out-of-network, benefits will be paid as though services were received and billed by an in-network participating provider, subject to the in-network deductible.
18. Prosthetics/Orthotics/Braces. The purchase or repair of prosthetic devices or appliances that replace
physical organs or parts or aid in their function is covered. Orthotics or braces needed to support or align movable parts of the body, prevent or correct deformities are covered, except the Plan excludes braces, orthotics or splints primarily for athletic use. Orthotic devices must be found Medically Necessary as established by a physician and a letter of Medical Necessity must be provided to the Claims Administrator.
Replacement of prosthetic, orthotic or brace devices will be covered when needed due to change in body

Elmira CSD – rev. 04/28/05 61
condition or when the device is no longer repairable. Replacement due to negligence is excluded.
Examples of covered devices or appliances are leg braces, internal prosthetics such as knee or shoulder joint replacements. Examples of devices not covered by the Plan are cosmetic devices, communication devices, computers, alterations to a home, dentures, other devices used in connection with teeth, hearing aids or vision aids (except initial glasses following surgery as specifically shown later in this section) or devices otherwise excluded under the Plan.
19. Medical Supplies (Home Use). Benefits are available for certain medical Supplies used in the home by
you or your Dependents when ordered by the attending Physician and found Medically Necessary according to Plan provisions. For example: a. Ostomy bags and Supplies required for their use. b. Catheters and Supplies required for their use. c. Syringes and needles necessary for conditions such as diabetes. d. Extensive dressings necessary for conditions such as cancer, diabetic ulcers and burns.
e. Diabetic insulin and syringes; covered diabetic supplies; colostomy supplies; catheter supplies, and supplies approved for home kidney dialysis or home chemotherapy specifically shown as covered expenses.
20. Blood Services. Benefits are available for blood transfusions, including the cost of blood, blood
products, and blood processing when found Medically Necessary, according to Plan provisions. Coverage is limited to the extent that the blood, Supplies, or services could not be obtained without cost. Separate charges for storage of blood or blood products are not Covered.
Coverage also includes services related to blood donations, autologous (patient donates own blood) or directed (donation of blood by individual chosen by patient), when there is a scheduled surgery that customarily requires blood transfusions. Coverage includes Services or Supplies for obtaining and processing the blood only to the extent that such Services or Supplies could not be obtained without cost. Benefits are not payable for separate charges billed for autologous or directed blood, or blood products, or for the storage of autologous or directed blood.
21. Contact Lens or Eyeglasses Following Intraocular Surgery. Benefits are available for the initial pair
of contact lenses or eyeglasses and related exams when ordered by a Physician following intraocular surgery. The lenses or eyeglasses must replace the function of the human lens and be medically required due to intraocular surgery or cataract surgery. No other eyeglasses, contact lens or visual aids, or related exams are Covered under this benefit.
22. Oxygen and its Administration. Benefits are available for oxygen and the needed Supplies for its
administration when ordered by an attending Physician and found Medically Necessary and appropriate for self-care home use. Oxygen must be found Medically Necessary, according to Plan limitations, for use in the treatment of severe hypoxemia (low oxygen levels in the blood) caused by chronic pulmonary conditions. For example: chronic obstructive pulmonary disease, pulmonary fibrosis, congestive heart disease, pulmonary hypertension, cystic fibrosis.
23. Diabetic Supplies, Equipment and Education. a. The following supplies and equipment are Covered for the treatment of a diabetic condition when such
supplies are ordered or recommended by a Physician and when they are found to be Medically Necessary according to the Plan provisions:
Retired Employees eligible for Medicare:

Elmira CSD – rev. 04/28/05 62
When Medicare is primary, this Plan will pay the 20% balance of the Medicare-approved amount, subject to this Plan’s deductible and coinsurance, for diabetic supplies covered under Medicare Part B and obtained from a pharmacy or supplier that is enrolled in Medicare. If a diabetic supply is not Covered under Medicare Part B as described above, this Plan’s Major Medical Benefits will apply.
1) Blood glucose monitors (standard) and blood glucose monitors for the legally blind; 2) Test strips for glucose monitors, visual reading and urine testing; 3) Injection aids; 4) Cartridges for the legally blind; 5) Syringes; 6) Data management systems; 7) Insulin pumps or insulin infusion pumps when Medically Necessary and when conventional
injection therapy is found to be inadequate to treat the patient's condition.
Items such as alcohol, swabs, adhesive tape and gauze are not Covered. Insulin, oral agents to control blood glucose, syringes, and test strips are Covered under the separate Prescription Drug Expense Benefits.
b. Diabetic self-management education and education relating to diet may be Covered for a Covered person with a diabetic condition. Self-management education or diet instruction will only be Covered when the patient is initially diagnosed with diabetes or when a Physician diagnoses a significant change in the patient's symptoms or condition that requires changes in the patient's self-management. These educational services will be Covered when provided by:
1) A Physician or his/her staff during an office visit for diabetes diagnosis or treatment. When the self-management service education is provided during an office visit, the one benefit payment for the office visit will include payment for the self-management education;
2) A certified diabetes nurse educator, certified nutritionist or certified and registered dietician when referred by a Physician. This education must be provided in a group setting. If it is decided that group education is not available in your area, the Plan may cover individual education;
3) A professional Provider as described above may be Covered for services rendered in the patient's home. However, it must be found to be Medically Necessary for the patient to receive services at home.
I. Miscellaneous Covered Expense Provisions
1. Voluntary or Elective Sterilization. Benefits are available for Service or Supplies related to voluntary
or elective sterilization such as tubal ligation and vasectomy for you or your eligible Spouse on the same basis as treatment of an Illness or Injury. The reversal of voluntary or elective sterilization is not Covered.
2. Transplants - Organ/Autologous Bone Marrow/Stem Cell.
Unless otherwise specifically included, transplants are considered Investigational unless specifically included for Medicare coverage by the Centers for Medicare & Medicaid Services (CMS) formerly known as Health Care Financing Administration. Transplants must meet the Medicare criteria for coverage to be considered for coverage under this Plan. Benefits are not available for expenses related to transplants that have not been approved by CMS or that fail to meet CMS criteria for coverage. Plan coverage for Hospitals will be based on the same criteria set forth by CMS criteria. If CMS restricts coverage for a transplant to approved Hospitals only, then this Plan will only cover those transplants when rendered in the approved Hospital.
Benefits are available for expenses related to non-Investigational organ or tissue transplants the same as any other Illness. Benefits will be available for the following in connection with a Covered transplant.
a. Recipient Expenses. Coverage for a Covered Person receiving a covered transplant (recipient)
Elmira CSD – rev. 04/28/05 63
includes all Plan benefits available for Medically Necessary care and treatment related to Covered organ transplants including, but not limited to; pre-transplant care including evaluation, diagnostic tests and x-rays by the transplant Hospital; procurement/tissue harvest and preparation; recipients transplant Surgery and recovery; and post discharge care.
b. Donor Expenses. Coverage for the person receiving the organ(s) includes expenses Incurred by the
live donor(s) for expenses related to procurement of an organ and for transportation of the organ(s) to the extent such charges are not reimbursed by the donor’s plan. If you or your Dependent act as a donor, this Plan will not pay your donor expenses unless the person receiving a covered transplant under this Plan. Then, donor expenses will be considered as part of the organ recipient’s claim. Donor charges and donor search charges will be deemed to be Incurred on the date of the transplant even if the services were rendered before such date. No benefits will be paid for pre-transplant testing in connection with a search for a donor who is not a family member.
c. Autologous Bone Marrow/Stem Cell. Courses of treatment involving high dose chemotherapy or
radiotherapy and autologous bone marrow, stem cell rescue, or other hematopoietic support procedures are not covered as organ and tissue transplants, except for the following (and only then for candidates who meet established national health and age standards): acute leukemia in remission, resistant non-Hodgkin’s lymphoma, Hodgkin’s disease, and neuroblastoma as allowed under CMS guidelines. If CMS guidelines change, adding or deleting coverage under Medicare, this Plan will include or exclude those procedures. Recipient and donor expenses for covered procedures will be considered on the same basis as organ transplants shown above.
3. Dental Care. Medical Expense Benefits are available for you or your Dependents for limited dental care.
Services or Supplies must be given and billed by a Physician or Dentist. Coverage is limited to the following dental or medical care for: a. The diagnosis and treatment of oral tumors, cysts, and cancer, cleft palate, tongue surgery and other
disorders considered medical rather than dental that would otherwise have been Covered if rendered by medical doctors.
b. An Injury to Sound Natural Teeth, dental structures, and alveolar processes due to an Accidental Injury that was not caused, directly or indirectly, by biting or chewing. Coverage includes, but is not limited to, x-rays of the teeth, surgery, extraction, and prostheses.
4. Infertility Treatment. Charges for fertility drugs are covered under J. Prescription Drug Expense
Benefits. All other treatments, including procedures intended to facilitate a pregnancy, such as artificial insemination, are not covered.
5. Chiropractic Services. Under the Alternate Treatment Provision, benefits are available for the detection
or correction of the structural imbalance or subluxation in the human body to remove nerve interference resulting from, or related to distortion, misalignment or subluxation of or in the vertebral column. Care must be rendered and billed by licensed chiropractor, medical Doctor, or osteopath. A written recommendation of a physician is required; however, if such services are rendered without a written recommendation, the Plan Administrator may authorize benefits if it concludes that the treatment meet the criteria of the Alternate Treatment Provision.
The therapeutic care must be directed at functional improvement (active treatment). Benefits will not be
paid for any Maintenance Care or care to prevent worsening. 6. Vision Care. Benefits are available for one annual eye examination for: a. Employees who routinely work with computers on a regular basis, or b. Members of the CWA. Prescription lenses are also Covered under the CWA vision care benefit.
7. Wigs for Covered Persons who are undergoing cancer therapies or treatment of burns are Covered up to

Elmira CSD – rev. 04/28/05 64
the maximum benefit of $500.
8. Prescription Drug Expenses (Retired Employees and their Covered Dependents only) are subject to deductible and coinsurance. The prescription drug exclusions described below under subsection J.7. apply.
J. Prescription Drug Expense Benefits (Applies to Active Employees and their Covered Dependents)
Please note
Paragraph 7. Prescription Drug Exclusions also applies to Retirees and their Dependents.
You and your Dependents may purchase drugs from any Pharmacy. However, if you or your Dependents choose a Network Retail Pharmacy or if you use the Mail Service pharmacy for maintenance drugs, you save on prescription costs for yourself and the District. Your member information kit will provide additional information on this program. The following is a brief summary. 1. Covered Prescription Drug Expenses. The quantity of each Covered drug purchased at a retail
Pharmacy is limited to a maximum of a 31-day supply, except for maintenance drugs for which a 90-day supply may be obtained. Mail service drugs will be limited to a maximum quantity of a 90-day supply. Nitroglycerin and natural thyroid products will be covered for a maximum quantity of 100 doses. Prescription refills will be paid for up to one (1) year from the date of the original prescription. All drugs must be obtainable only by prescription, ordered by the attending Physician, and found to be Medically Necessary unless certain drugs are specifically included by name. Please refer to Prescription Drug Exclusions shown later under this benefit. Unless a drug is otherwise excluded, Plan benefits are available for medications that are Federal legend drugs, or insulin.
2. Prior Authorization is required for some medications. For example, Lovenox (anticoagulant),
biotech drugs (Copaxone), Betaseron and Avonex (immune response modifiers), Toradol (for short-term pain management), and cosmetic agents for a patient after age 18. Weight loss medications and oral contraceptives must be Medically Necessary to be authorized.
3. Generic Drug Substitution Program. As part of a continuing effort to control costs and preserve the
quality of the Plan, you are encouraged to use generic drugs whenever appropriate for your condition. A generic drug is a drug that is chemically equivalent to the original brand name drug. The only difference is that the patent on the brand name medication has expired, allowing other manufacturers to sell the drug. As a result, the generic manufacturer does not incur research costs and can charge significantly less for the drug. Since generic drugs cost less than brand name drugs, cost savings may result for you and the District when you substitute the lower priced drug. If you have any questions about generic drugs, ask your Physician or your pharmacist.
A penalty may apply if your Physician allows a generic substitution but the Covered Person requests the
brand name version. Please note (Applies to ISEA only): if a prescription for a brand name drug with a generic equivalent is filled and the prescribing physician provides medical documentation for review by EHS who concurs that the brand name drug is appropriate, EHS will reimburse the difference between the $30.00 copayment and the generic drug copayment. Documentation may be sent to:
EHS Clinical Department. 620 Epsilon Drive
Pittsburgh, PA 15238 Fax 412-967-2364
Elmira CSD – rev. 04/28/05 65
4. Network Pharmacy. A Network Pharmacy has an agreement with the prescription drug Claims Administrator to accept the Plan benefit as payment in full after any applicable Copayment. The copayments do not apply toward the deductible or coinsurance limits. If you or your Dependents use a Network Retail Pharmacy, you will be required to pay only the following Copayments:
a. Copayments. Please refer to the appropriate Summary of Benefits or collective bargaining agreement
for the copayment amount. A penalty may apply if your physician allows a generic substitution but the Covered Person requests the brand name version.
b. Plan Identification Card. You can use your Plan identification card at any Network Pharmacy. The
Pharmacy may display the participation logo or you may ask the pharmacy if it participates as a Network Pharmacy. You may also call the Claims Administrator’s customer service department for information on Network pharmacies located near you.
c. Obtaining Network Pharmacy Drugs. To obtain your Covered drug or supply at Network Provider
costs, you need only present your Plan identification card, the written prescription, and any applicable Copayment amount to the Network pharmacist. The Pharmacy will bill the drug Claims Administrator and will receive its payment directly from them.
5. Out-of-Network Pharmacy. If you or your Dependents purchase Covered drugs at an Out-of-Network
Pharmacy, the Plan will reimburse the cost minus the copayment up to the amount that would have been paid at a participating retail pharmacy.
6. Mail Service for Maintenance Drugs. You or your Dependents may obtain up to a 90-day supply of
maintenance drugs from the Mail Service. You need only pay the applicable copayment; the mail service bills the Plan for the balance. The copayments do not apply toward the deductible or coinsurance limits. This service delivers the drug directly to your home. Maintenance drugs are those medications to treat chronic disorders such as hypertension, heart disease, thyroid disease, and diabetes.
a. Mail Service Copayment. Please refer to the appropriate Summary of Benefits for the copayment
amount. A penalty may apply if your physician allows a generic substitution but the Covered Person requests the brand name version.
b. How to Use the Mail Service Pharmacy Program.
1) When the Physician writes a prescription for a "maintenance drug" (one taken regularly on a long-term basis), he or she should indicate the number of refills allowed (maximum three refills).
2) For your first mail service order, obtain an initial patient profile/registration form from the District’s Business Office or in each District Building. Complete the form, include the original prescription(s) and the applicable copayment, and mail to the Mail Service Pharmacy. You may wish to keep a photocopy for your records.
3) A new order form and envelope will be included with each drug delivery. For subsequent original and refill prescriptions:
a) Mail a completed order form with your copayment; b) E-mail and order utilizing the Internet; or c) Call the mail order pharmacy directly. 4) The medication will be delivered to you or your Dependent by first-class mail or UPS. You
should allow 10-14 days from the time the prescription forms are mailed to the mail service Pharmacy until delivery of your medication. However, to ensure that you or your Dependents are not left without an adequate supply of medication, you should order when you or your Dependents have a minimum of a 30-day supply remaining from the current medication.

Elmira CSD – rev. 04/28/05 66
7. Prescription Drug Expense Exclusions (Applies to Active Employees, Retirees, and their Covered Dependents). In addition to limitations shown otherwise in the Plan, the following drugs or Supplies are not Covered even if only obtainable by prescription and ordered by a Physician. See also Medical Expense Exclusions shown later in this Part 1 and Part 3 - General Plan Exclusions shown later in this section. a. Non-Legend drugs/over the counter (OTC) that are obtainable without a prescription, unless
otherwise specifically named for coverage; b. Weight loss drugs, anti-obesity/appetite suppressants unless Medically Necessary; c. Contraceptives or birth control medicines, drugs, or devices. However, oral contraceptive drugs
which are Medically Necessary to treat an Illness are Covered; proof of Medical Necessity will be required.
d. Drugs for treatment of impotency or sexual dysfunction (e.g., Viagra and Caverject); e. Therapeutic devices, equipment, and appliances; f. Injectable delivery devices (syringes) for uses other than insulin injection; g. Implantable, time-release medication unless otherwise noted h. Cosmetic medication, including but not limited to, anti-wrinkle medications, dermatological
medications, hair growth medications, and any drugs FDA-approved for cosmetic use only (such as Renova, Rogaine, and Propecia). However, drugs such as Accutane, Retin-A, Differin, and Avita are Covered to age 18; prior authorization is required for Covered Persons over age 18;
i. Immunization agents, vaccines, biologicals, biological serum j. Vitamins (including prenatal vitamins), minerals, fluoride prep and dental rinses, food or nutritional
supplements. Single entity-vitamins to treat pernicious anemia, folic acid, and iron products are covered.
k. Growth hormones and anabolic steroids; l. Immune response modifiers other than Betaseron and Avonex; prior authorization is required for
these two drugs; m. Drugs labeled “Caution-limited by federal law to investigational use,” Experimental drugs or drugs
prescribed for Experimental (non-FDA approved/unlabeled) indications; n. Charges for the administration of any medication; o. Medication which is to be taken by or administered, in whole or part, to an individual while confined
in a Hospital, rest home, sanitarium, skilled nursing facility, extended care facility, convalescent Hospital, nursing home or similar institution which operates on its premises, or allows to be operated on its premises, a facility for dispensing pharmaceuticals;
p. Drugs that are not considered to be Medically Necessary for treatment of an Illness or Injury even if obtainable only by prescription and even if prescribed by a Physician.

Elmira CSD – rev. 04/28/05 67
K. Dental Expense Benefits (Active Employees and their Covered Dependents Only)
Benefits are available for a wide range of dental services when deemed to be necessary dental treatment for a dental disease or Injury. Subject to the Plan’s limitations and exclusions, benefits shall be provided for the services and supplies described in the Section J. when billed by a Dentist for services rendered by the Dentist or his professional employee who is licensed to render such service. Coverage will be based on the most appropriate standard procedures needed to adequately correct or treat the dental condition. Please refer to the Dental Exclusions below for further details on your dental Coverage. The Covered services and supplies provided to you or your Dependent will be used to decide the Plan benefits, not the number of Providers who render such services. If your dental care is transferred from one Dentist to another Dentist during treatment, the total Plan payment will not exceed the Plan allowance that would have been paid had one Dentist rendered the Covered dental services.
Please Note
All claims are subject to review to decide whether services are Covered according to Plan limitations and exclusions. There may be occasions when differences of opinion arise regarding your dental care. In such cases, the Plan Administrator will rely on the findings of the Claim Administrator's dental consultant. You must comply with requests for additional dental/medical documentation as deemed necessary by the Claims Administrator to evaluate a claim for benefits. Failure to submit requested documentation or information could result in denial of benefits. The Claims Administrator confidentially maintains all medical/dental documents. Treatment decisions are independent from payment decisions. The patient's Dentist or Physician is responsible for determining whether treatment should be rendered despite whether the charges are totally or partially included in, or excluded from, coverage under the Plan. 1. Option A Schedule of Dental Allowances. Services Covered under Option A are subject to the schedule of allowances, or the amount of the Dentist’s actual charges, whichever is less. There are no yearly deductible and benefit maximum amounts. The Claims Administrator reserves the right to determine the amount of the allowance, if any, to be paid for services listed as “By report.”
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit Diagnostic CLINICAL ORAL EVALUATION
• Periodic oral evaluation D0120 $6.00 • Limited oral evaluation - problem focused (emergency) D0140 BR • Comprehensive oral evaluation D0150 $8.00
RADIOGRAPHS • Intraoral complete series incl. bitewings
Adult Child
D0210
$31.00 $20.00
• Intraoral periapical –first film • Intraoral periapical – each add’l film
D0220 D0230
$5.00 $2.00
• Intraoral – occlusal film D0240 $7.00 • Extraoral – first film • Extraoral – each add’l film
D0250 D0260
$10.00 $8.00
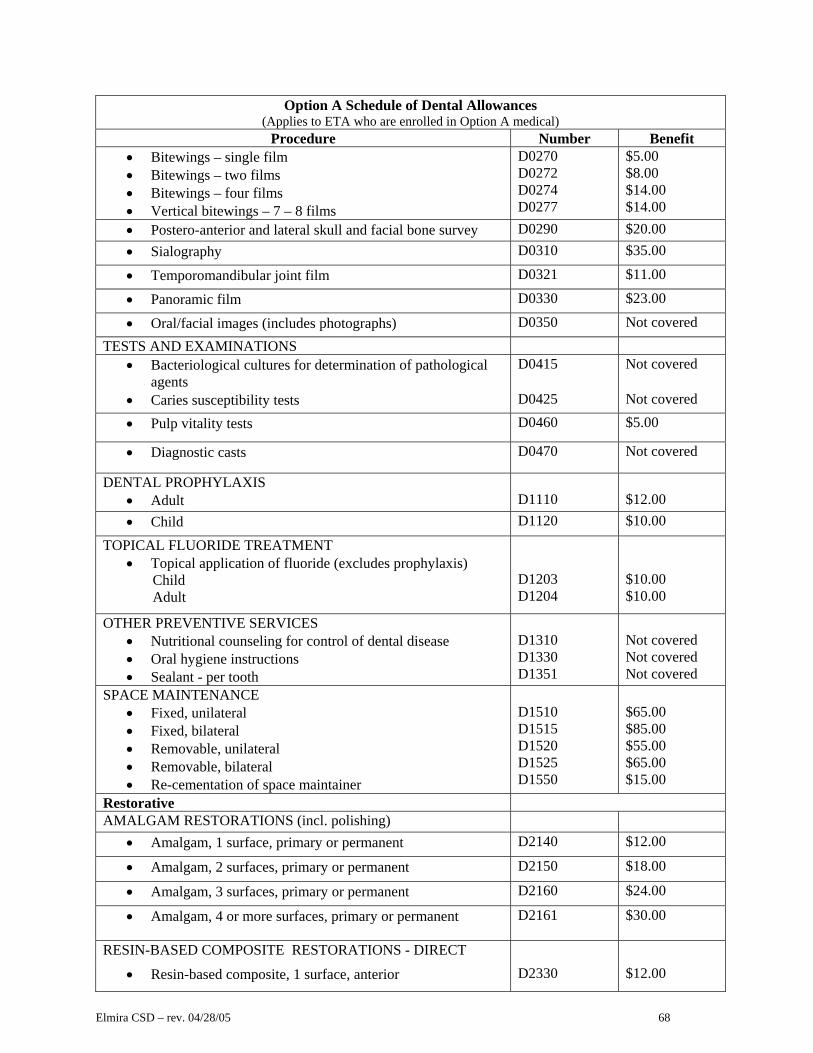
Elmira CSD – rev. 04/28/05 68
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit • Bitewings – single film • Bitewings – two films • Bitewings – four films • Vertical bitewings – 7 – 8 films
D0270 D0272 D0274 D0277
$5.00 $8.00 $14.00 $14.00
• Postero-anterior and lateral skull and facial bone survey D0290 $20.00 • Sialography D0310 $35.00
• Temporomandibular joint film D0321 $11.00
• Panoramic film D0330 $23.00
• Oral/facial images (includes photographs) D0350 Not covered TESTS AND EXAMINATIONS
• Bacteriological cultures for determination of pathological agents
D0415 Not covered
• Caries susceptibility tests D0425 Not covered
• Pulp vitality tests D0460 $5.00
• Diagnostic casts D0470 Not covered
DENTAL PROPHYLAXIS • Adult
D1110
$12.00
• Child D1120 $10.00
TOPICAL FLUORIDE TREATMENT • Topical application of fluoride (excludes prophylaxis) Child Adult
D1203 D1204
$10.00 $10.00
OTHER PREVENTIVE SERVICES • Nutritional counseling for control of dental disease • Oral hygiene instructions • Sealant - per tooth
D1310 D1330 D1351
Not covered Not covered Not covered
SPACE MAINTENANCE • Fixed, unilateral • Fixed, bilateral • Removable, unilateral • Removable, bilateral • Re-cementation of space maintainer
D1510 D1515 D1520 D1525 D1550
$65.00 $85.00 $55.00 $65.00 $15.00
Restorative AMALGAM RESTORATIONS (incl. polishing)
• Amalgam, 1 surface, primary or permanent D2140 $12.00
• Amalgam, 2 surfaces, primary or permanent D2150 $18.00
• Amalgam, 3 surfaces, primary or permanent D2160 $24.00
• Amalgam, 4 or more surfaces, primary or permanent D2161 $30.00
RESIN-BASED COMPOSITE RESTORATIONS - DIRECT
• Resin-based composite, 1 surface, anterior D2330 $12.00
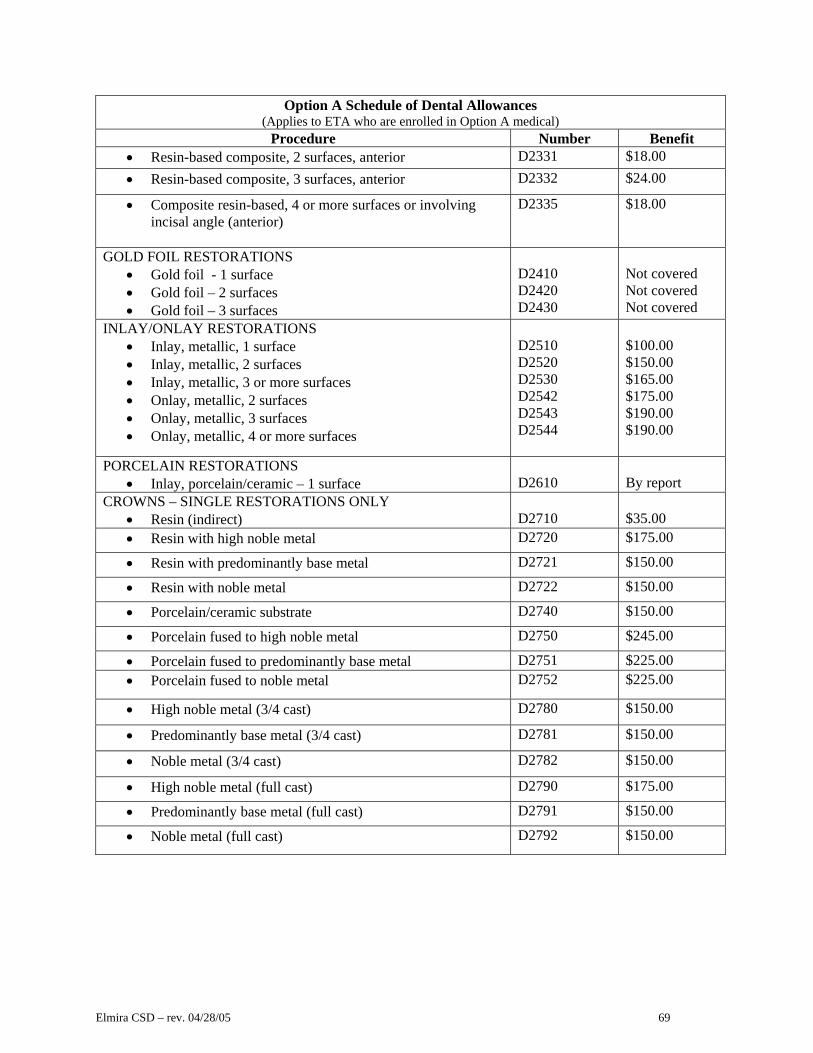
Elmira CSD – rev. 04/28/05 69
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit • Resin-based composite, 2 surfaces, anterior D2331 $18.00 • Resin-based composite, 3 surfaces, anterior D2332 $24.00
• Composite resin-based, 4 or more surfaces or involving incisal angle (anterior)
D2335 $18.00
GOLD FOIL RESTORATIONS • Gold foil - 1 surface • Gold foil – 2 surfaces • Gold foil – 3 surfaces
D2410 D2420 D2430
Not covered Not covered Not covered
INLAY/ONLAY RESTORATIONS • Inlay, metallic, 1 surface • Inlay, metallic, 2 surfaces • Inlay, metallic, 3 or more surfaces • Onlay, metallic, 2 surfaces • Onlay, metallic, 3 surfaces • Onlay, metallic, 4 or more surfaces
D2510 D2520 D2530 D2542 D2543 D2544
$100.00 $150.00 $165.00 $175.00 $190.00 $190.00
PORCELAIN RESTORATIONS • Inlay, porcelain/ceramic – 1 surface
D2610
By report
CROWNS – SINGLE RESTORATIONS ONLY • Resin (indirect)
D2710
$35.00
• Resin with high noble metal D2720 $175.00
• Resin with predominantly base metal D2721 $150.00
• Resin with noble metal D2722 $150.00
• Porcelain/ceramic substrate D2740 $150.00
• Porcelain fused to high noble metal D2750 $245.00
• Porcelain fused to predominantly base metal D2751 $225.00 • Porcelain fused to noble metal D2752 $225.00
• High noble metal (3/4 cast) D2780 $150.00
• Predominantly base metal (3/4 cast) D2781 $150.00
• Noble metal (3/4 cast) D2782 $150.00
• High noble metal (full cast) D2790 $175.00
• Predominantly base metal (full cast) D2791 $150.00
• Noble metal (full cast) D2792 $150.00

Elmira CSD – rev. 04/28/05 70
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit OTHER RESTORATIVE SERVICES
• Recement inlay • Recement crown • Prefabricated stainless steel - primary • Prefabricated stainless steel - permanent • Sedative filling • Core buildup, including any pins • Pin retention, in add’n to restoration, per tooth first each additional • Cast post and core in add’n to crown • Prefabricated post and core in add’n to crown • Temporary crown (fractured tooth)
D2910 D2920 D2930 D2931 D2940 D2950 D2951 D2952 D2954 D2970
$12.00 $12.00 $30.00 $30.00 $15.00 $50.00 $5.00 $3.00 $50.00 $50.00 $35.00
Endodontics PULP CAPPING
• Pulp cap, direct (excl. final restoration) • Pulp cap, indirect (excl. final restoration)
D3110 D3120
$10.00 $8.00
PULPOTOMY • Therapeutic pulpotomy (excl. final restoration)
D3220
$20.00
ENDODONTIC THERAPY (incl. treatment plan, clinical procedures, and follow-up care)
• Anterior (excl. final restorations) • Bicuspid (excl. final restorations) • Molar (excl. final restorations)
APEXIFICATION/RECALCIFICATION PROCEDURES • Apexification/recalcification - initial • Apexification/recalcification - interim • Apexification/recalcification - final
D3310 D3320 D3330 D3351 D3352 D3353
$120.00 $150.00 $185.00 $50.00 $50.00 $50.00
APICOECTOMY/PERIRADICULAR SERVICES • Apicoectomy/periradicular surgery - anterior • Apicoectomy/periradicular surgery - bicuspid- 1st root • Apicoectomy/periradicular surgery - molar- 1st root • Apicoectomy/periradicular surgery - each add’l root • Retrograde filling - per root • Root amputation – per root • Endodontic endosseous implant
D3410 D3421 D3425 D3426 D3430 D3450 D3460
$75.00 $75.00 $75.00 $75.00 $25.00 $75.00 Not covered
OTHER ENDODONTIC PROCEDURES • Surgical procedure for isolation of tooth with rubber dam • Hemisection (incl. any root removal), not incl. root canal
therapy • Canal preparation and fitting of preformed dowel or post • Unspecified endodontic procedure
D3910 D3920 D3950 D3999
Not covered Not covered Not covered By report

Elmira CSD – rev. 04/28/05 71
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit PERIODONTICS Surgical Services
Gingivectomy or gingivoplasty - per quadrant Gingival flap procedure, incl. root planning Clinical crown lengthening - hard tissue Osseous surgery (incl. flap entry and closure)- per quadrant Bone replacement graft - first site in quadrant
D4210 D4240 D4249 D4260 D4263
$175.00 $206.00 $235.00 $332.00 $100.00
Non-Surgical Periodontic Services Periodontal scaling and root planing, per quadrant Full mouth debridement to enable comprehensive
periodontal evaluation & diagnosis
D4341 D4355
$47.00 $31.00
Other Periodontal Services Periodontal maintenance
D4910
$20.00
PROSTHODONTICS Repairs to Partial Dentures
• Repair resin denture base D5610 $25.00 • Repair cast framework D5620 $30.00
• Repair or replace broken clasp D5630 $45.00
• Replace broken teeth – per tooth D5640 $25.00
• Add tooth to existing partial denture D5650 $35.00
• Add clasp to existing partial denture D5660 $35.00
Repairs OTHER FIXED PARTIAL DENTURE SERVICES
• Recement fixed partial denture D6930
$16.00
Oral Surgery EXTRACTIONS (incl. local anesthesia, suturing, and routine postoperative care)
• Extraction , erupted tooth or exposed root
D7140
$20.00
SURGICAL EXTRACTIONS (incl. local anesthesia, suturing, and routine postoperative care)
• Surgical removal of erupted tooth requiring elevation of mucoperiosteal flap and removal of bone
D7210
$30.00
• Removal of impacted tooth - soft tissue D7220 $45.00 • Removal of impacted tooth - partially bony D7230 $60.00 • Removal of impacted tooth completely bony D7240 $85.00 • Removal of impacted tooth - completely bony with unusual
surgical complications D7241 $85.00
• Surgical removal of residual tooth roots D7250 $35.00 • Oroantral fistula closure D7260 $120.00

Elmira CSD – rev. 04/28/05 72
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit Other Surgical Procedures
• Tooth reimplantation and/or stabilization • Tooth transplantation • Biopsy of oral tissue (hard) • Biopsy of oral tissue (soft) • Surgical repositioning of teeth
D7270 D7272 D7285 D7286 D7290
$120.00 $120.00 $35.00 $35.00 By report
ALVEOPLASTY (surgical preparation of the ridge for dentures)
• Per quadrant, in conjunction with extractions • Per quadrant, not in conjunction with extractions
D7310 D7320
$30.00 $50.00
VESTIBULOPLASTY • Ridge extension • Ridge extension, incl. soft tissue grafts, and management of
hypertrophied and hyperplastic tissue
D7340 D7350
By report By report
SURGICAL EXCISION OF LESIONS • Excision of benign lesion up to 1.25 cm • Excision of benign lesion greater than 1.25 cm • Excision of malignant tumor, lesion diameter up to 1.25 cm • Excision of malignant tumor, lesion diameter greater than
1.25 cm
D7410 D7411 D7440 D7441
$50.00 By report $58.00 By report
• Removal of odontogenic cyst or tumor, up to 1.25 cm • Removal of odontogenic cyst or tumor, greater than 1.25
cm in diameter • Removal of nonodontogenic cyst or tumor, up to 1.25 cm • Removal of nonodontogenic cyst or tumor, greater than
1.25 cm in diameter • Destruction of lesions by physical or chemical methods
D7450 D7451 D7460 D7461 D7465
By report By report By report By report By report
EXCISION OF BONE TISSUE • Removal of lateral exostosis, maxilla or mandible • Radical resection of mandible with bone graft
D7471 D7490
By report By report
SURGICAL INCISION • Incision and drainage of abscess, intraoral soft tissue • Incision and drainage of abscess, extraoral soft tissue • Removal of foreign body from muscosa, skin, or
subcutaneous alveolar tissue • Removal of reaction-producing foreign bodies,
musculoskeletal system • Partial osteoectomy/sequestrectomy for removal of non-
vital bone • Maxillary sinusotomy for removal of tooth fragment or
foreign body
D7510 D7520 D7530 D7540 D7550 D7560
$25.00 $35.00 By report By report By report By report
TREATMENT OF FRACTURES (simple) • Maxilla, open reduction (teeth immobilized, if present)
D7610
$520.00
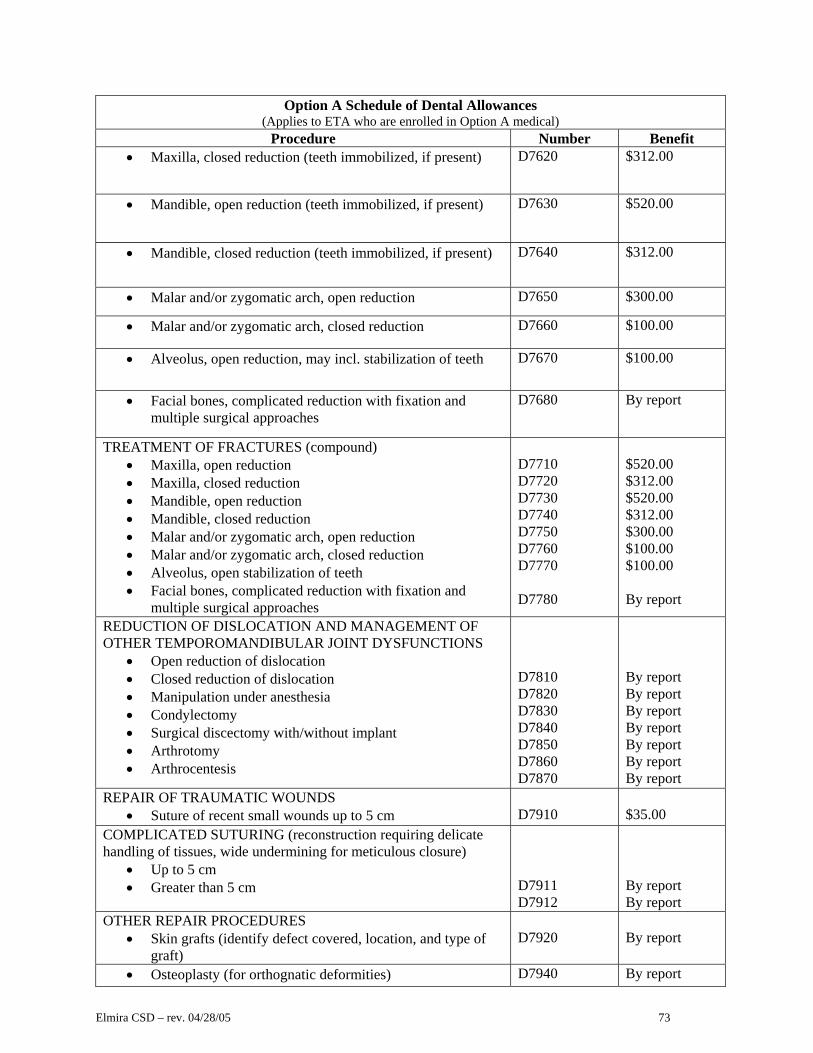
Elmira CSD – rev. 04/28/05 73
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit • Maxilla, closed reduction (teeth immobilized, if present) D7620 $312.00
• Mandible, open reduction (teeth immobilized, if present) D7630 $520.00
• Mandible, closed reduction (teeth immobilized, if present) D7640 $312.00
• Malar and/or zygomatic arch, open reduction D7650 $300.00
• Malar and/or zygomatic arch, closed reduction D7660 $100.00
• Alveolus, open reduction, may incl. stabilization of teeth D7670 $100.00
• Facial bones, complicated reduction with fixation and multiple surgical approaches
D7680 By report
TREATMENT OF FRACTURES (compound) • Maxilla, open reduction • Maxilla, closed reduction • Mandible, open reduction • Mandible, closed reduction • Malar and/or zygomatic arch, open reduction • Malar and/or zygomatic arch, closed reduction • Alveolus, open stabilization of teeth • Facial bones, complicated reduction with fixation and
multiple surgical approaches
D7710 D7720 D7730 D7740 D7750 D7760 D7770 D7780
$520.00 $312.00 $520.00 $312.00 $300.00 $100.00 $100.00 By report
REDUCTION OF DISLOCATION AND MANAGEMENT OF OTHER TEMPOROMANDIBULAR JOINT DYSFUNCTIONS
• Open reduction of dislocation • Closed reduction of dislocation • Manipulation under anesthesia • Condylectomy • Surgical discectomy with/without implant • Arthrotomy • Arthrocentesis
D7810 D7820 D7830 D7840 D7850 D7860 D7870
By report By report By report By report By report By report By report
REPAIR OF TRAUMATIC WOUNDS • Suture of recent small wounds up to 5 cm
D7910
$35.00
COMPLICATED SUTURING (reconstruction requiring delicate handling of tissues, wide undermining for meticulous closure)
• Up to 5 cm • Greater than 5 cm
D7911 D7912
By report By report
OTHER REPAIR PROCEDURES • Skin grafts (identify defect covered, location, and type of
graft)
D7920
By report
• Osteoplasty (for orthognatic deformities) D7940 By report

Elmira CSD – rev. 04/28/05 74
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit • Osseous, osteoperiosteal, or cartilage graft of the mandible,
autogenous or nonautogenous D7950 By report
• Repair of maxillofacial soft and hard tissue defect D7955 By report
• Frenulectomy, separate procedure (frenectomy or frenotomy)
D7960 $60.00
• Excision of hyperplastic tissue, per arch D7970 By report
• Sialolithotomy D7980 By report
• Excision of salivary gland D7981 By report
• Sialodochoplasty D7982 By report • Closure of salivary fistula D7983 By report
• Emergency tracheotomy D7990 By report
Orthodontics • Pre-orthodontic treatment visit D8660 $75.00
MINOR TREATMENT TO CONTROL HARMFUL HABITS • Removable appliance therapy • Fixed appliance therapy
D8210 D8220
$100.00 $100.00
COMPREHENSIVE ORTHODONTIC TREATMENT Case type – fixed appliances (incl. diagnostic procedures, retention – formal, full banded treatment)
• Treatment of the Transitional Dentition D8070
By report
• Periodic orthodontic treatment visit (incl. appliances $37.50 maximum per month; yearly maximum $450.00; three-year maximum $1,350.00)
D8670
Orthodontic Retention - 10 visits per 18 months, $75.00 D8680 Maximum allowance for orthodontia - $1,500.00
Orthodontic Retention Post-Treatment Stabilization – 10 visits, maximum $75.00
D8680
Adjunctive General Services UNCLASSIFIED TREATMENT
• Palliative emergency treatment of dental pain, minor procedure
D9110
$15.00

Elmira CSD – rev. 04/28/05 75
Option A Schedule of Dental Allowances (Applies to ETA who are enrolled in Option A medical)
Procedure Number Benefit ANESTHESIA
• Local (not in conjunction with operative or surgical procedures)
• Regional block anesthesia • Trigeminal division block anesthesia • Deep sedation/general anesthesia – first 30 min. • Analgesia, anxiolysis, inhalation of nitrous oxide
D9210 D9211 D9212 D9220 D9230
Not covered Not covered Not covered $10.00 Not covered
PROFESSIONAL CONSULTATION (diagnostic services provided by a physician or dentist other than the practitioner providing treatment)
• Consultation
D9310
Not covered
PROFESSIONAL VISITS • House/extended care facility call • Hospital call • Office visit – during regularly scheduled office hours (no
other services performed)
D9410 D9420 D9430
$10.00 $10.00 Not covered
DRUGS • Therapeutic drug injection • Other drugs and/or medicaments
D9610 D9630
Not covered Not covered
MISCELLANEOUS SERVICES • Application of desensitizing medicaments • Treatment of complications (post-surgical – unusual
circumstances) • Occlusion analysis (mounted case) • Internal bleaching - per tooth • Unspecified adjunctive procedure
D9910 D9930 D9950 D9974 D9999
Not covered Not covered Not covered Not covered Not covered

Elmira CSD – rev. 04/28/05 76
2. Option B Schedule of Dental Allowances. Services and Supplies Covered under Option B are subject to a benefit maximum and allowances. An annual deductible applies to all services except diagnostic and preventive care.
Option B Dental Services
(Applies to CMCW, CWA, ESSAC, Non-Unit, Administrators, and ETA who are enrolled in Option B Medical; ISEA who are enrolled in either Option A or Option B medical)
Deductible $50 individual
$150 family
Maximum Benefit $1500 per Plan Year
Diagnostic 75% of UCR, no deductible
Preventative 75% of UCR, no deductible
Basic Restorative 50% of UCR
Oral Surgery 50% of UCR
Endodontic 50% of UCR
Periodontic 50% of UCR
Major Restorative 50% of UCR
Prosthodontic 50% of UCR
Orthodontia for dependent children to age 19
50% of UCR $1000 per lifetime (separate from contract year maximum)
3. Benefits After Termination. No benefits will be payable for expenses incurred for dental procedures
which are completed more than one month from the date that the Covered Person’s dental expense benefits terminate under this Plan.
4. Dental Exclusions. No benefits are payable for charges for: a. Dental services received from a dental or medical department maintained by or on behalf of an
employer, a mutual benefit association, labor union, trustee, or similar person or group; b. Dental services for which there is no charge; c. Treatment by a Dentist outside the scope of his license; d. Services primarily intended for cosmetic or aesthetic purposes; e. Procedures, appliances or restorations whose primary purpose is to alter vertical dimension, restore or
maintain the occlusion (except to the extent that orthodontic treatment is Covered); f. Bridgework (other than repairs); g. Dentures, other than repairs; h. Expenses incurred by retirees of the District; and i. Services and Supplies that are listed under Section V, Plan Exclusions.

Elmira CSD – rev. 04/28/05 77
SECTION V - PLAN EXCLUSIONS In addition to limitations and exclusions shown elsewhere in this document, charges for the following expenses will not be paid by the Plan, unless they are specifically shown otherwise for Plan coverage. Also, please refer to Section X - Definitions. 1. Plan Coverage not in Effect. Services or supplies incurred while an individual is not eligible and
enrolled in the Plan or incurred before the Plan became effective or after the Plan is canceled. Services or supplies which are not covered according to Plan limitations and exclusions in effect at the time expenses were Incurred.
2. Unreasonable Charges. Charges that exceed any fees found to be Usual, Customary, and Reasonable
according to Plan provisions. See Section X - Definitions under Usual, Customary and Reasonable Charges.
3. Not Physician Approved/Not under Care of Physician. Services or Supplies not recommended or
approved by a Physician, or received while the Covered Person is not under the regular or ongoing care and treatment of the ordering Physician. Services given by a provider who is not covered by the Plan are excluded.
4. Not Medical Necessity/Preventive Care/Routine Screening. Services or supplies that are not
Medically Necessary for the treatment of an Illness or Injury according to Plan provisions or related to preventive care or routine screening. This includes, but is not limited to, well child or adult care, routine physicals, screening exams, premarital exams, school exams, camp or sport exams; tests unrelated to symptoms or treatment of Illness or Injury; inoculations, immunizations, vaccinations, or other preventive shots; precautionary Services or standby services even if ordered by the Physician or due to hospital regulations. Exception: Limited preventive care expenses specifically included for coverage.
5. Blood Products/Donations. The cost of blood, blood plasma, other blood products and blood processing
and storage charges when they are available free of charge. Services or Supplies for autologous or direct blood donations and storage as precautionary measures if the need for blood arises. Exception: Charges by a Hospital, Ambulatory Surgery center or certified blood bank for autologous or direct donation Service or Supplies preceding scheduled surgery that could require blood transfusion as specifically included in the Plan.
6. Experimental or Investigational/Alternative Care. Services or supplies related to clinical or research
studies or care that is considered Experimental or Investigational according to Plan provisions at the time expenses are Incurred. See Section X - Definitions under Investigational or Experimental. Transplants will be considered investigative, except those transplant procedures that are specifically covered by and meet the Federal Health Care Financing Administration coverage criteria in effect at the time expenses are Incurred. This exclusion includes all services related to an Experimental transplant, including chemotherapy or other services that are integral to the transplant care and would not otherwise have been given. Services or supplies connected with care such as holistic medicine, hypnotherapy, environmental health, and other alternative-type medicine are not covered unless such services meet the criteria of Alternative Treatment provision.
7. Drugs/Infertility/Birth Control/Vitamins/Supplements. Medicines or drugs whether or not prescribed
by a Physician's prescription, contraceptive (birth control) drugs and devices, infertility drugs, or vitamins and supplements, including nutritional supplements, food products, and enteral formulas (even if ordered in writing by a Physician). Exceptions: Prescription drugs dispensed by a covered inpatient facility during an approved inpatient stay or within 60 days following inpatient discharge; drugs and medicines

Elmira CSD – rev. 04/28/05 78
dispensed by an outpatient facility, clinic, urgent care center, physicians as part of covered outpatient treatment or surgery; billed by a home health care agency as part of an approved plan of care, billed as part of an approved plan of home chemotherapy or home dialysis; or as otherwise specifically included in the Plan, by name. Fertility drugs and Medically Necessary oral contraceptive drugs covered under J. Prescription Drug Expense Benefits.
8. Home Medical Supplies. Medical supplies for home use that are not directly supplied by professional
home care services during an approved plan of home care, or that are not for the operation of covered durable medical equipment unless otherwise specifically included for coverage. Items primarily intended for comfort or to support activities of daily living, such as diapers, ice bags, incontinence pants, more than two pair of support stockings, nutritional supplements, cervical or lumbar pillows. Items such as gauze pads, swabs, alcohol, deodorizers, and adhesive tape are not Covered.
9. Personal Items. Personal comfort items such as a telephone, radio, television, or hairdressing services
charged by any facility or other provider. 10. Durable Medical Equipment/Braces/Prosthetics/Devices. Services or supplies related to duplicate
medical equipment, braces, prosthetics or other devices or the replacement of Durable Medical Equipment, braces, prosthetics or other devices due to loss, theft or destruction. The purchase of Durable Medical Equipment that can be rented unless the length of time that the equipment will be needed makes the purchase less costly than the rental. The purchase or replacement of any biomechanical prosthetic device. Specialized equipment when standard equipment is adequate for the patient's condition. Services or supplies related to durable equipment, braces, orthotics, or splints that are primarily for athletic use. Personal, household, or environmental items including, but not limited to, air conditioners, air purification units, communication devices, computers, swimming pools, any type of pillows, blankets or mattress covers, orthopedic mattresses, exercise equipment, elevators and stair lifts, blood pressure monitors, thermometers, stethoscopes, scales, elastic bandages or stockings, first aid supplies, non-hospital adjustable beds, and special equipped vehicles will not be covered.
11. Vision. Services or supplies related to vision therapy, visual aids, eyeglasses or contact lenses, or their
repairs, and related examinations to determine the need for, adjustments or repair of them. Treatment or surgery for the correction of a refraction error, including but not limited to radial keratotomy. Exception: Plan covers lenses for aphakia and soft lenses or scleral shells intended for treatment of illness or injury and initial contacts following cataract or other intraocular surgery or the limited vision care benefit specifically included in this Plan.
12. Hearing. Services or supplies related to hearing aids, tinnitus masking devices (or similar devices),
communication devices, and examinations to determine the need for, adjustments or repair of them. 13. Anesthesia. Services or supplies for the administration of anesthesia for any surgery or treatment that is
not Covered by the Plan. 14. Prescription Drug Co-pay. The Employee Prescription Drug co-pay is not a reimbursable expense as
any other part of the Plan. (NOTE: If the Employee establishes a voluntary Flexible Spending Account, the prescription co-pay would qualify as an eligible reimbursement.)
15. Midwife/Doctor Duplicate Services. Services that are duplicative because they are provided by both a
nurse midwife and doctor. 16. Surgical Assistance. Expenses billed for surgical assistance in a Hospital if the Hospital has qualified
staff Physicians to provide such assistance. Expenses billed for surgical assistance by providers other than qualified surgeons (M.D., D.O., or a D.P.M for foot surgery, or a D.D.S., D.M.D. for Covered oral surgery.)

Elmira CSD – rev. 04/28/05 79
17. Educational/Cognitive/Training/Therapy for Developmental and Birth Defects. Services or Supplies related to special education, training, vocational training or cognitive therapy for any reason; occupational, physical, speech therapy, psychological or other therapy that is primarily directed at educational, mental or physical development for learning deficiencies, mental retardation, developmental disorders, birth defects, autism, spina bifida, educational or occupational deficits or perceptual and conceptual dysfunctions; or similar disorders. This applies whether or not the charges are associated with manifest Mental Illness or other disturbances. Services or Supplies considered remedial or educational. Services or Supplies that any school system is required to provide under any law unless the law makes this Plan primary for expenses otherwise Covered by the Plan. This applies even if the Covered Person, parent, or guardian does not seek provision of such Services or Supplies through the school system.
18. Counseling/Analysis/Support Groups. Services or Supplies primarily directed at raising the level of
consciousness, social enhancement, counseling limited to everyday problems of living such as marriage counseling, family counseling, pastoral counseling; gender identity counseling, sex therapy, or support groups.
19. Foot Care/Shoes/Orthotics/Supports. Services or supplies related to routine foot care such as cutting or
removal of corns, calluses, nails, routine hygienic care, or preventive maintenance care (ordinarily within the realm of self-care). Orthopedic shoes are excluded unless custom made and ordered by a physician. Foot orthotics or other supportive foot devices for treatment of weak, strained, flat, unstable or unbalanced feet, metatarsalgia, bunions or subluxations of the feet despite underlying pathology. Exceptions: The removal of nail roots, open cutting corrective procedures, and routine foot care provided to a Covered Person with a severe systemic disease such as diabetes.
20. Weight Reduction/Diet Management /Exercise. Services or supplies related to weight reduction or diet
management for treatment of obesity no matter the age, condition, diagnosis or prognosis of the patient, even if it is part of a treatment plan for another medical condition. Diet management, exercise programs, or general conditioning programs for any condition even if ordered by a Physician. Exceptions: Limited coverage specifically included in the Plan for diabetic education and coverage for weight loss medications as described under J. Prescription Drug Expense Benefit.
21. Inpatient Room and Board/Private Room. Room and Board charges in any facility during a period
when the Covered Person (patient) is not physically present. Private room charges that are not Medically Necessary. Room and Board charges for a Friday or Saturday admission date unless significant medical treatment is given on these days. Significant treatment includes care not normally connected with room and board and general nursing care.
22. Hospital Non-Acute Care Area. Room and Board and general nursing charges by a Hospital made
during an Inpatient stay or portion of an Inpatient stay for special non-acute level of care areas by whatever name called. These areas include, but are not limited to, areas designated as a Skilled Nursing Facility, convalescent or other non acute care center, Hospice, Substance Abuse treatment center, ambulatory surgical center, Birth Center, partial hospitalization, adult or child day or night care center, halfway house, vocational rehabilitation center, or any other area of a Hospital that renders services on an Inpatient basis for other than acute care of a sick or injured person. Benefits for a Covered facility that is part of a Hospital and meets the definition of a Covered facility are payable at the coverage level for that facility, not the coverage level for a Hospital. If the area does not qualify as a Covered facility, the charges for the miscellaneous Service or Supplies found Medically Necessary will be considered on the same basis as Hospital outpatient charges.
23. Inpatient Custodial/Non-Acute Care/Long Term Care. Services or supplies related to any part of an
inpatient stay that is primarily for physical checkups, physical therapy, hydrotherapy, occupational therapy, diagnostic testing, custodial, residential, sanitarium type, rest cures, or for environmental change. Services or supplies given in a place of rest, a place for the aged, a nursing home or in an education

Elmira CSD – rev. 04/28/05 80
facility, a place mainly for treatment of alcoholism, drug addiction, mental disorders or tuberculosis unless the facility meets the Plan’s requirements for Skilled Nursing Facility benefits and substance abuse rehabilitation benefits. Services or supplies related to any portion of an inpatient stay for care that cannot reasonably be expected to lessen the patient’s disability enabling him or her to leave an institution. Exception: hospice care services specifically included in the Plan.
24. Inactive Care/Custodial/Maintenance Care. Services or Supplies related to care that is not expected
to improve the Covered Person’s condition or related to care found Custodial or Maintenance according to Plan provisions. Long-term or other care that does not, or cannot reasonably be expected to, lessen the patient’s disability and enable him or her to leave an institution, unless the care meets the Plan requirements for Hospice care. For persons whose care is found primarily custodial with limited skilled care, benefits will be provided only for the skilled services and Custodial Care will be denied.
25. Reversal of Sterilization Procedures. Services or Supplies related to the reversal of sterilization
procedures, whatever the reason. 26. Birth Control. Services or supplies related to family planning, oral contraceptives or other birth control
devices. 27. Infertility/In vitro/Artificial Insemination. Services or Supplies relating to or in connection with
fertility studies, sterility studies, procedures to restore or enhance fertility, procedures which are used to induce or enhance the probability of conception or to enhance the probability of a viable pregnancy, artificial insemination, in-vitro fertilization, and any other services, by whatever name called, which are intended to assist or facilitate any person in becoming pregnant. Exception: fertility drugs covered under J. Prescription Drug Expense Benefits.
28. Surrogate Pregnancy. Services or Supplies related to surrogate maternity care, including but not limited
to, those needed to initiate a Pregnancy, prenatal care, delivery or other procedures, and postnatal care or any other related care of the Pregnancy. Benefits are available for Newborns who meet the child eligibility requirements and who are enrolled under family coverage.
29. Dependent Child Pregnancy. Services or supplies related to maternity care of a dependent child,
including but not limited to prenatal care, delivery or other procedures, postnatal care or any other care related to the Pregnancy. Benefits are available for Newborns who meet the child eligibility requirements and are enrolled under family coverage.
30. Elective or Voluntary Abortions. Services or supplies connected with elective or voluntary abortion
procedures. 31. Organ Donors. Expenses Incurred by organ donors are not Covered. However, donor expenses for
Covered transplants will be considered Incurred by the transplant recipient who is a Covered Person if the expenses are not Covered by the donor’s health coverage.
32. Cosmetic/Beautifying Care Services or supplies connected with elective care, cosmetic surgery, or
beautifying care. Reversal of elective, cosmetic surgery or beautifying surgery will not be covered unless found to be Medically Necessary according to Plan provisions. Exception: Care required to significantly restore tissue damaged by an illness or injury or for reconstructive surgery that is incidental to or follows surgery resulting from a trauma, an infection or other disease of the involved part or reconstructive surgery because of a congenital disease or anomaly of a dependent child that has resulted in a functional defect.
33. Hair Loss/Baldness. Service or supplies related to hair loss or baldness including, but not limited to, human or artificial hair transplants, other professional care to stimulate hair growth, drugs to eliminate
Elmira CSD – rev. 04/28/05 81
baldness or stimulate hair growth, and wigs and artificial hairpieces. Exception: wigs for Covered Persons who are undergoing cancer therapies or treatment of burns are Covered up to the maximum benefit of $500.
34. Smoking Cessation/Tobacco. Services, supplies, or drugs related to therapy for cessation of smoking or
other use of tobacco products whether or not recommended, ordered, or prescribed by a Physician. Exception: Prescription medications as described under J. Prescription Drug Expense Benefit.
35. Transportation/Travel. Services or supplies related to transportation or travel by any means other than
an ambulance even if ordered, recommended, or prescribed by a Physician. Services or Supplies related to non-Emergency ambulance Services. Ambulance transportation when a person could have been safely transported by other means unless ordered by a Physician, a police officer or firefighter unless the Hospital is a preferred provider. Ambulance transportation that is not to the nearest local hospital or inpatient facility that can treat the patient’s condition. Ambulance emergency transportation from a hospital unless the Covered Person is being transferred between two inpatient facilities due to Medical Necessity and cannot be safely transported by any other means.
36. Care by Relative/Household Member. Services given by an Immediate Relative or household member.
See Section X - Definitions under Immediate Relative. 37. Facility Employees. Separate charges for services by members of the staff employed by a Hospital,
Skilled Nursing Facility, convalescent facility, Rehabilitation Facility, or by any inpatient facility where care is received.
38. Free Care/Obligation to Pay. Services or Supplies received for which no charges would have been
made without coverage under the Plan or for which there is no legal obligation for payment by the enrollee or dependent. Exception: Coverage to the extent federal and state law requires the Plan to allow benefits that would have been otherwise payable.
39. Condition Due to Military Service. Services or Supplies for which benefits are, or can be, provided due
to related Illness or Injury arising from the past or present military service in the armed forces of any government or international authority.
40. Illegal Care. Services or Supplies considered illegal according to the laws of the state of jurisdiction or
according to Federal law. Benefits will not be provided if these excluded services are obtained outside the USA even if these services are legal in the foreign country.
41. Out of USA. Services or Supplies incurred outside the USA if the Covered Person traveled to the foreign
country or locality for the sole purpose of receiving the services or supplies. 42. Act of War. Services or Supplies received due an injury or illness resulting from an act of war, whether
declared or undeclared. 43. Work-Related/Occupational Conditions. Services or supplies received because of an occupational
injury or an occupational illness that entitles the Covered Person to benefits under a worker's compensation, occupational disease law, or similar legislation. Payment will not be made even if you or your dependent do not claim the entitled benefits. Note: this Plan will automatically exclude expenses denied by the workers compensation health plan when due to claimant’s late filing, failure to provide documentation, failure to attend a hearing, or because the services related to the occupational condition was not medically necessary.
44. Government Programs. Services or Supplies that could be provided by or paid by any governmental
(domestic or foreign) program (other than Medicaid) under which you or your dependents are or could be

Elmira CSD – rev. 04/28/05 82
covered. Exception: Coverage to the extent that the government regulations for the program require the Plan to allow benefits that would have been otherwise payable. Medicare as specifically included in Section VI - Medicare Integration with Plan Benefits. Note: If a Covered Person is not enrolled in Medicare when Medicare becomes primary according to Medicare Secondary Payer rules, the Plan estimates Medicare’s payment. These estimated amounts could reduce available benefits.
45. Government Facilities/Institutions. Services or Supplies received in an institution owned or operated
by federal, state, or local governments for which no charges would have been made if this health plan were not in effect. USA facilities for the treatment of active military personnel will not be covered. Military hospitals for the care of active military personnel will not be covered. Federal Veteran hospitals will not be covered for the treatment of conditions related to military service. Government facilities that do not meet the Plan definitions for coverage will not be covered except if a Covered Individual is seriously injured and taken to such a hospital for emergency care because of its proximity and taken only for so long as emergency care is necessary and it is impossible to transfer the Covered Individual to another hospital facility and the individual is not eligible for benefits under Title 38 of the United States Code.
46. No-Fault Auto Insurance. Services or Supplies to the extent they are covered under a mandatory motor
vehicle liability law that requires benefits be provided for personal injury without regard to fault. This applies whether or not a claim is made for payment under that coverage. Benefits under this Plan will automatically be denied if the no-fault auto insurance or other payer of mandatory liability coverage denies benefits due to its felony exclusions (including felony DWI or DUI), as not Medically Necessary, or for late filing. Charges for Services or Supplies not paid by the no-fault coverage due to its deductible or maximum payment limits will be covered under this Plan to the extent Allowable Fees would have otherwise been payable by this Plan. Note: No-fault is considered another plan under the Coordination of Benefits provision of this Plan.
47. Third Party Claim Settlement/Action. Services or Supplies for which payment is received or are
reimbursable because of claim settlement or legal action (third party claim or actions) other than from an insurance carrier under an individual policy issued to you or your dependent. Exception: Conditional payments shown in Section IX - Other Procedures and Provisions under Right of Subrogation. Failure to comply with the conditions of the Plan's right to subrogation could result in denial of benefits.
48. Forms/Missed Appointments/Phone Calls/No Care Given. Medical summaries, invoice preparation,
completion of claim forms, or fees for missed appointments, telephone consultations, charges for standby services. Services or Supplies not actually received by the patient or incurred by someone other than the patient unless specifically included in this Plan such as coverage limits for organ donors.
49. Plan Penalties/Copayments/Benefit Limits. Services or supplies to the extent they are not reimbursed
due to benefit penalties, copayments or other benefit limits under any portion of this Plan. Exception: When this Plan pays benefits as a secondary payer to another Plan according to the coordination of benefits provision.
50. Late Claim Filing. Services or supplies for which an adequate claim is not filed with the Claims
Administrator within the Plan time limit for claim submissions. Exception: Claim filing extensions for delays due to Medicare and other health plans shown under Section VIII - Claims Submissions and Review Procedures, Time Limit on Claim Submission. Other exceptions may be made at the discretion of the Claims Administrator or the Plan Administrator for late claim filing due to extenuating circumstances beyond the control of the enrollee.
Elmira CSD – rev. 04/28/05 83
SECTION VI- MEDICARE INTEGRATION WITH PLAN BENEFITS If Medicare is primary, Plan benefits will be reduced by Medicare’s benefits. Medicare primary plan status is determined according to Medicare Secondary Payer (MSP) rules established by federal regulations; revisions or changes in these MSP rules will automatically apply. If you or your Dependents are eligible for Medicare primary benefits, claims should be submitted to Medicare first. When you submit expenses to this Plan, Medicare’s explanation of benefits should be attached to your claim. Please refer to the "Medicare and You” handbook for information and details on Medicare coverage. This handbook is mailed to Medicare beneficiaries or can be obtained from the U.S. Department of Health and Human Services, Heath Care Financing Administration, 7500 Security Blvd., Baltimore, MD 21244-1850. You can telephone Medicare for information at 1-800-633-4227 or visit their website at www.medicare.gov. You or your Dependents are responsible for Medicare enrollment. If you or your Dependent are not contacted by the Social Security Office at least three months before a 65th birthday or within 12 months after starting Social Security disability benefits, you or your Dependent should call your local Social Security office for assistance. Persons of any age who are diagnosed with end state kidney disease or with Lou Gehrig’s disease (amyotrophic lateral sclerosis or ALS) should contact the Social Security Office for eligibility and enrollment details. If this Plan is primary coverage for your health care, Medicare regulations allow you to delay Medicare enrollment until this Plan becomes secondary according to Medicare Secondary Payer rules. Your local Social Security Office can provide details on enrollment requirements and penalties for late enrollment. This Medicare integration provision applies to all persons eligible for primary Medicare coverage even if the person is not actually enrolled in Medicare. If you or your Dependent are not enrolled for primary Medicare coverage, Medicare benefits will be estimated. Please note: For this Plan to be the secondary payor of benefits, retirees of ISEA must enroll for Medicare.
A. Medicare Secondary Payer (MSP) Rules Currently, the following general MSP rules apply: 1. Persons Eligible for Medicare Due to Age (65 and over). Medicare Secondary Payer rules for
employer plans are based on the number of full and/or part-time employees for each working day in each of 20 or more calendar weeks in the current calendar year or the preceding calendar year. The requirements are based on the number or employees, not the number of people covered under the Plan. Your employer can clarify which rule applies to you based on the requirements of Medicare Secondary Payer law.
a. Current Employment Status (working aged).
1) For Plans that have employers with less than 20 employees, Medicare is primary to the plan that covers this person as a person with current employment status, or the Dependent of a person with current employment status.
2) For Plans that have employers with 20 or more employees, Medicare is secondary to the plan that
covers this person as a person with current employment status, or the Dependent of a person with current employment status. For plans that have multiple employers, Medicare is

Elmira CSD – rev. 04/28/05 84
secondary if at least one of the participating employers has 20 or more employees unless the Plan exempts the employees of a particular employer with fewer than 20 employees. This exemption must be documented in accordance with Medicare Secondary Payer law.
b. Retirees/Persons without Current Employment Status. Medicare is primary to the plan that covers
this person as a retiree or a person without current employment status, or the Dependent of a retiree or person without current employment status. (The 20 employee rules do not apply).
2. Persons Eligible for Medicare Due To Disability. Medicare Secondary Payer rules for employer plans
are based on the number of full and/or part-time employees for 50% or more of its business days during the preceding calendar year. The requirements are based on the number or employees, not the number of people covered under the Plan. Your employer can clarify which rule applies based on the requirements of Medicare Secondary Payer law.
a. Current Employment Status (Working Aged). In most cases, employees eligible for Medicare due
to disability would be considered to be without employment status. 1) For Plan of employer with less than 100 employees, Medicare is primary to the plan that covers
this person as a person with current employment status, or the Dependent of a person with current employment status.
2) For Plans that have employers with 100 or more employees, Medicare is secondary to the plan
that covers this person as a person with current employment status, or the Dependent of a person with current employment status. For plans that have multiple employers, Medicare is secondary if at least one of the participating employers has 100 or more employees.
b. Retirees/Persons without Current Employment Status. Medicare is primary to the plan that covers
this person as a retiree or a person without current employment status, or the Dependent of a retiree or person without current employment status. (The 100 employee rules do not apply)
3. Persons Eligible for Medicare due to End Stage Renal Disease (ESRD). Once Medicare eligibility is
established due to ESRD, the eligible person is entitled to full Medicare coverage. Medicare coverage is available for other conditions and is not limited only to ESRD expenses.
a. Medicare Eligibility Solely Due to ESRD
1) 18-Month Rule. Before July 31, 1997, Medicare is secondary for the first 18 months following
the month of the ESRD eligibility date for persons eligible solely due to ESRD. If an ESRD-eligible person did not complete 18 months of ESRD eligibility before August 1, 1997, the following 30-month rule applies.
2) 30-month Rule. On or after August 1, 1997, Medicare is secondary for the first 30 months
following the month of the ESRD eligibility date for persons eligible solely due to ESRD. The 18-month rule is extended to 30 months for persons who did not complete 18 months of ESRD eligibility on or before July 31, 1997. This 30-month rule does not apply if the Covered Person completed 18 months of ESRD eligibility before August 1, 1997.
b. Medicare ESRD Dual Eligibility. ESRD dual eligibility means a person who is either eligible for
Medicare due to age and ESRD or due to disability and ESRD.
1) If a group plan is appropriately paying secondary to Medicare according to MSP rules for eligibility due to age or disability and ESRD entitlement then becomes effective, Medicare remains the primary payer. The 18-month or 30-month ESRD period does not apply.

Elmira CSD – rev. 04/28/05 85
2) If the group plan is paying primary according to MSP rules for eligibility due to age or disability
and ESRD entitlement then becomes effective, Medicare remains secondary until after the 18-month or 30-month ESRD period. At the end of the 18-month or 30-month ESRD period, the group plan becomes the primary or secondary payer based on the MSP rules for age and disability.
3) If a group health plan is paying primary to Medicare according to the MSP rules for ESRD, and
the person then becomes eligible due to age or disability, Medicare remains secondary until the end of the 18-month or 30-month ESRD period. At the end of the 18-month or 30-month ESRD period, the group plan becomes primary or secondary payer based on the MSP rules for age and disability.
B. Effects of Medicare on Plan Benefits
If Medicare is primary for you or your Dependent, the benefits of the Plan will be integrated as follows: 1. Medicare Payment Integration. Medicare payment for health expenses Covered by this Plan will
supplement Medicare’s benefits payable under Part A and B. The Plan will pay the Part A deductible per benefit period and any coinsurance per day of confinement. For Part B covered services, the Plan will pay the calendar year deductible and the 20% coinsurance not covered by Medicare. In addition, the Plan will pay the difference between the Medicare-approved amount and the eligible charges for expenses Covered under Major Medical portion of this Plan.
2. Not enrolled in Medicare. This integration will apply to persons eligible for Medicare whether or not
actually enrolled in Medicare. If Medicare is primary for an eligible person who is not enrolled in Medicare Part A and Part B or in Part C, the Medicare benefit will be estimated and used to reduce Allowable Fees. This could result in significant reduction or denial of the Plan benefits. For this Plan to be the secondary payor of benefits, retirees of ISEA must enroll for Medicare.
3. Medicare Private Contract Options. This integration will apply to persons eligible for Medicare
primary benefits if Medicare benefits are not paid due to a Medicare Private Contract Option with Physicians and certain other practitioners. (When a Medicare beneficiary agrees to the terms of a Private Contract with certain providers, Medicare will not pay. The patient is responsible for the entire charge. The provider may bill more than the charges allowed by Medicare.) Under this Plan, if a private contract is used, Medicare benefits will be estimated. Part A services will be estimated according to Medicare payment rules. Part B or similar services under Part C will be estimated based on 80% of Usual, Customary and Reasonable Charges for Covered Services or Supplies without regard to Medicare Deductibles and other coinsurance limits. The estimated Medicare benefits will be used to coordinate benefits. This could result in significant reduction or denial of the Plan benefits.
C. Allowable Fees
Allowable Fees for Medicare integration only will be based on the following: 1. If the provider accepts Medicare assignment of benefits, the Allowable Fees will be the same fees allowed
by Medicare. 2. If the provider does not accept Medicare assignment, the Allowable Fees will be paid in accordance with
the Plan Option the retiree is enrolled in. 3. If the provider provides services under a Medicare Private Contract Option, Allowable Fees will be in
accordance with the Plan Option the retiree is enrolled in. According to Medicare regulations, a beneficiary cannot be billed the difference between the Medicare

Elmira CSD – rev. 04/28/05 86
allowed amounts and the provider's charges when that provider accepts Medicare assignment. If a provider does not accept assignment, a beneficiary cannot be billed for charges over the limiting charge established by Medicare for that service by that provider. However, if services are provided under the Medicare Private Contract Option, the provider’s charges can exceed the Medicare allowable fees.
D. Medicare Premiums If this Plan is the secondary payor, the Participant is entitled to reimbursement of Medicare Part B premiums, in accordance with the applicable collective bargaining agreement, as modified. You must present your Medicare card to the District Business Office in order to verify Part B enrollment. Part B premium reimbursement only begins after you notify the Business Office and provide verification; it is not retroactive.
SECTION VII - COORDINATION OF BENEFITS (COB)
Information necessary to administer the COB provision will be required when claims are submitted. If you or your Dependents are covered by more than one plan, all claims should be filed with each plan. You should file claims first with the primary plan, then submit copies of the primary plan explanation of benefits or denial to the secondary plan(s). Special rules apply when you or your Covered Family Members are covered by more than one group health plan. This can happen if you, your Spouse, and/or children are covered under this Plan and another plan (with your Spouse's employer, for example). Coordination of Benefits (COB) means that the benefits payable under this Plan, as shown in the preceding pages, are coordinated with the benefits payable under another group plan. The purpose of COB is to avoid duplicate payments that could exceed 100% of the total allowable expenses. One of the two or more plan(s) involved is the primary plan and the other plan(s) is the secondary plan(s). The order of benefit determination shown later in this section determine which plan will pay as the primary plan. The primary plan pays first without regard to the possibility that another plan may cover some expenses. The secondary plan pays after the primary plan and may reduce its benefits so that payments from all involved plans do not exceed 100% of Allowable Fees.
A. COB Terms and Definitions The following definitions show the meaning of terms used in the administration of this COB provision. 1. This Plan. Whenever the term "this Plan" is used in this section, it means The Elmira City School
District Self Insured Health and Dental Plan. 2. Plan. The term 'plan' includes any of the following:
a. A group insurance or group type coverage, whether insured or uninsured, including, but not limited to, coverages such as prepayment; indemnity; Hospital or medical service organizations; group practice or individual practice; health maintenance organizations or similar type organizations; group auto plan or individual auto health coverage on an automobile leased or owned by an employer; student coverage sponsored by, or provided through, a school or other educational facility except school accident type coverage.
b. Coverage under a governmental plan, or coverage required or provided by federal, state, or local
laws, including mandatory No-fault Automobile Coverage. This does not include government coverage, such as Medicaid that by its terms, prohibits coordination for the allowable expenses. This Plan integrates its benefits with Medicare. See Section VI - Medicare Integration with Plan

Elmira CSD – rev. 04/28/05 87
Benefits.
Each contract, policy or other arrangement for coverage under a. or b. shown above is a separate plan. Also, if an arrangement has two parts and COB rules apply only to one, each part is a separate plan.
3. Primary Plan/Secondary Plan. The order of benefit rules determine whether this Plan is a primary or
secondary plan to another plan covering the person. When this Plan is primary, its benefits are determined before those of the other plan and without regard to the other plan benefits. When this Plan is the secondary plan, its benefits are determined after those of the other plan and may be reduced because of the primary plan benefits. If a person is covered by more than one secondary plan, the order of benefit rules determine the order in which secondary plans are determined in relation to each other. Each secondary plan will take into consideration the benefits of the primary plan or plans and the benefits of any other plan which, under the order of benefit rules, has its benefits determined before those of that secondary plan.
4. Claim Determination Period. The claim determination for coordination of benefits is done on an
Incurred expense basis and based on a Calendar Year period. However, it does not include any Allowable Fees Incurred during any part of a Calendar Year during which a person has no coverage under this Plan, or any part of the year before the date this COB provision takes effect.
5. Allowable Expense. The term 'allowable expense' means medical care expenses, including deductibles
and copayments or coinsurance, that are covered at least in part by any of the plans covering the person. When a Plan provides benefits in the form of medical services (for example an HMO), the reasonable cash value of each service will be considered an allowable expense and a benefit paid. Any expenses or services that are not covered by any of the plans will not be considered allowable COB expenses. The following are examples of expenses not considered allowable expenses or otherwise limited under this COB provision:
a. If a covered Person is confined in a private Hospital room, the difference between the cost of a semi-
private room and the private room is not an allowable expense unless the private room is found Medically Necessary according to this Plan's provisions or the primary plan routinely includes coverage for Hospital private rooms.
b. If a person is covered by two or more plans that determine benefit payments based on Usual and
Customary (UCR) Charges, any amount more than the highest of the UCR charges for the specific medical benefit is not an allowable expense.
c. If a person is covered by two or more plans that provide benefits or services based on negotiated fees,
any amount more than the highest of the negotiated fees for the specific medical benefit is not an allowable expense.
d. If a person is covered by one plan that determines its benefits based on UCR charges and another
provides benefits or services based on negotiated fees, the primary plan’s payment arrangements will be the allowable expense for all plans.
e. The amount benefits are reduced by the primary plan because a covered person does not comply with
the plan provisions will be excluded under this COB provision. Examples of these provisions include, but are not limited to, mandatory requirements of a benefit management program, second surgical opinions, medical procedure review, preadmission review or prenotification of Inpatient admissions, preapproval requirements for certain treatment, and HMO or preferred provider arrangement.

Elmira CSD – rev. 04/28/05 88
f. As secondary payer, long term care, prescription drug expenses, dental or vision or hearing aid expenses excluded under this Plan will not be considered allowable expenses, even if such expenses were covered by the primary plan.
g. As secondary payer, this Plan will not consider any health benefits paid due to Mandatory No-fault
Automobile Coverage laws as allowable expense for COB. However, charges for health expenses applied to no-fault plan deductibles, copayments or more than the cumulative benefit maximum per accident will be considered as allowable expenses, if otherwise covered by this Plan.
h. If Medicare is primary, charges more than the allowable expenses permitted under Medicare regulations will not be considered allowable expenses for COB.
B. Order of Benefit Determination
If a Covered Person is eligible for Medicare, the order of benefit determination can be affected by Medicare Secondary Payer (MSP) rules. Current MSP rules and any future changes in MSP rules will automatically apply. Rule # 4 shown below applies if you or your Dependents are continuing Coverage under COBRA or USERRA.
The order of benefit determination rules shown below designate which plan is the primary coverage and which are secondary. The primary plan pays first without regard to the possibility that another plan could pay some expenses. A secondary plan pays after the primary plan and reduces its available benefits so that payments from all involved plans do not exceed 100% of the total allowable expenses. This Plan is always secondary payer to any health plans that pay without regard to coverage by other plans. This Plan is always secondary to government plans or coverages provided by federal, local, or state laws unless otherwise prohibited by that law. For example: this Plan is secondary to New York State mandatory No-fault Automobile Coverage. To determine the order plans should pay, for expenses covered by two or more plans with a COB feature, an order of benefit determination has been established as follows: 1. Non-Dependent or Dependent. Unless otherwise determined by law or governmental plans, the plan
that covers the person other than as a dependent is primary. The plan that covers the person as a dependent is secondary. This changes if the person is eligible for Medicare primary benefits.
2. Child Covered under More than One Plan. The following order of benefits is used when a child is
covered by more than one Plan.
a. This Plan follows the “gender rule.” The primary plan is the plan of the male parent if the parents are married, not separated (whether or not they have ever been married), or a court decree awards joint custody without specifying that one party has the responsibility to provide health care coverage.
b. When specific terms of a court decree state that one parent is responsible for the child’s health care
expenses or health care coverage and the plan of that parent has actual knowledge of those terms then that plan is primary. This rule applies to claim determination periods or plan years commencing after the plan is given notice of the court decree.
c. If the parents are not married, or are separated (whether or not they have ever been married) or are
divorced; the order of benefits is the plan of the custodial parent, then the plan of the Spouse of the custodial parent, then the plan of the noncustodial parent and then the plan of the Spouse of the noncustodial parent. The custodial parent is the parent awarded custody by a court decree. Without a court decree, it is the parent with whom the child resides more than half the Calendar Year without regard to temporary visitations. Without a degree or court order, it will also be presumed that the person who claims child as a dependent on their Federal Income Tax will be the custodial person.

Elmira CSD – rev. 04/28/05 89
3. Active/Inactive Employee. The benefits of a plan that covers a person as an employee who is neither laid-off nor retired are determined before the plan that covers that person as a laid-off or retired employee. The same rule would hold true for that person’s dependents.
4. Continuation Coverage. If a person elects or is covered under continuation of coverage pursuant to
federal or state laws, such as COBRA or USERRA, and is also covered under another plan, the order of benefit rules change. The plan providing coverage for the individual as an employee, member, subscriber, Enrollee, or retiree is primary for that person and/or that person's dependents. The plan providing continuation coverage is secondary.
If the preceding order of benefit rules fail to establish the primary plan(s), then the plan that has covered the person for the longer time will consider its plan benefits first. If according to the above rules, this Plan is secondary and another health plan's rules conflict making this Plan primary, then this Plan will use the National Association of Insurance Commissioners (NAIC) Model Regulation and any court cases to determine the validity of the conflicting rules.
C. Medicare Effect on the Order of Benefit Determination
Please refer to the "Medicare and You” handbook which can be obtained at your local Social Security Office for details on current Medicare Secondary Payer (MSP) rules. Also, see Section VI - Medicare Integration with Plan Benefits. Generally, if Medicare is considered primary coverage, the order of benefit determination could be changed as follows: 1. For individuals eligible for Medicare due to age (65 or over) or due to disability who are covered under a
plan as a person with current employment status, or a dependent of a person with current employment status, the following order of benefit determination applies: a. All active plans (employees with current employment status and their eligible dependents) pay first. b. Medicare pays second. c. Retired plans, or employees without current employment status plans, pay last.
2. For individuals eligible for Medicare solely due to ESRD, the order of benefit determination is as follows:
a. Medicare pays last for the first 30 months following the month of first eligible ESRD treatment. Usual order of benefit determination would apply for other group plans.
b. Medicare pays first after the first 30 months. Other plans would be secondary following the order of benefit determination.
D. COB Effect on Plan Benefits
When this Plan is secondary, benefits will be reduced so that the total benefits paid or provided by all plans are not more than 100% of the allowable expenses Incurred during a claim determination period. When benefits are so reduced, each benefit is reduced in proportion and applied against any applicable benefit limit of the Plan. When this Plan is secondary, payment could be reduced if the benefits available for the Covered Expenses under this Plan without COB provision and the benefits payable by all other involved plans are more than 100%. Then, the benefits of this Plan will be reduced so that they, and the benefits payable under the other plan(s), do not total more than the total allowable expenses Incurred during a claim determination period. When the benefits of this Plan are so reduced, each benefit is reduced in proportion. It is then charged against any applicable benefit limit of this Plan. If a Covered Person fails to file a claim with the primary payer, benefits for the primary plan will be
Elmira CSD – rev. 04/28/05 90
estimated. If a person is eligible for Medicare primary coverage according to Medicare secondary payer rules, and is not enrolled in Medicare Part A and/or Part B or in Part C, then Medicare benefits will be estimated. The estimated Medicare payments will be used to determine the benefit reduction under this COB provision.

Elmira CSD – rev. 04/28/05 91
E. Right to Receive and Release Needed Information Certain facts are needed to apply these COB rules and to determine benefits payable under this Plan and other plans. The Claims Administrator may get the facts it needs from, or give them to, any other organization or person for the purpose of applying these rules and determining benefits payable under this Plan and other plans covering the person for whom claim is made. The Claims Administrator need not tell, nor obtain the consent of, any person to do this. Each person claiming benefits under the Plan must give the Claims Administrator any facts required to pay the claim.
F. Facility of Payment A payment made under another plan may include an amount that should have been paid under this Plan. If it does, the Claims Administrator may pay the amount to the organization that made that payment. That amount will then be treated as though it was a benefit paid under the Plan. The Plan Administrator will not have to pay that amount again. The term "payment made" includes providing benefits in the form of services in which case "payment made" means reasonable cash value of the benefits provided as services.
G. Right of Recovery If the amount of the payments made by the Claims Administrator is more than should have been paid under this COB provision, then the Plan Sponsor or Claims Administrator has a claim to recover the overpayment: 1. From the enrollee or dependent who has received an overpayment, 2. from any provider which received overpayment, and 3. from any insurer of other entity responsible for such payments.
H. Examples of COB Order of Benefits 1. I am eligible for the District Plan benefits as an active employee and am also eligible as a retiree under
the ABC Mfg. health plan. (I am not eligible for Medicare). Which plan pays first? Your active Plan is primary over your retiree plan. The District Plan would pay first.
2. I am eligible for the District plan coverage as an active employee. My Spouse is enrolled in my family
coverage. She is covered as a retiree under XYZ, Inc. Plan. Neither of us is eligible for Medicare. Which plan pays first for my health claims? For my Spouse's health claims?
a. Health Claims for yourself:
The District active plan pays first. XYZ, Inc. retiree plan pays second.
b. Health Claims for Spouse:
XYZ, Inc. retiree plan pays first. The District active plan pays second.
3. I am eligible for the District plan benefits as an active employee and also eligible as a retiree under the
ABC Mfg. health plan. I have family coverage under both plans. My Spouse also covers our dependent children and me under his or her group plan through XYZ, Inc. (We are not eligible for Medicare) My birth date is July 10, 1950. My Spouse was born June 15, 1951. What is the order of benefit determination for my Spouse, my children, and me? a. Health Claims for yourself. Your Health plans would pay before the health plan of your Spouse.
Order of benefit determination is: The District active plan pays first.

Elmira CSD – rev. 04/28/05 92
ABC Mfg. retiree plan pays second. XYZ, Inc. Active plan for Spouse pays last
b. Health Claims for Spouse. Your Spouse's plan pays before your health plans. Order of benefit determination is:
XYZ, Inc. active plan for Spouse pays first. The District active Plan pays second. ABC Mfg. retiree plan pays last.
c. Health Claims for Dependent Child. The order of benefit determination is based on the gender of the child's parents. The plan(s) of the parent who is male pays before the plan(s) of the parent who is female. As your Spouse’s is male, the order of benefit is:
XYZ Inc. active plan of Spouse pays first. The District active Plan pays second. ABC Mfg. retiree plan pays last.
The above order of benefit applies to children whose parents are not separated or divorced
4. I am eligible for the District plan benefits under COBRA continuation and eligible for Medicare coverage due to age. Does Medicare or the Elmira City School District pay first?
According to Medicare Secondary Payer rules, Medicare would pay first for persons without employment status. COBRA participants in the District’s Plan are considered without employment status.
5. I am eligible for District plan continuation coverage under COBRA. I am also eligible under the retiree
Plan of my Spouse through XYZ, Inc. Continuation of Coverage pays after other Plans. XYZ, Inc. Plan pays first.
The District continuation under COBRA pays last. 6. I am eligible for District plan benefits as an active employee. My Spouse is eligible for benefits
through his or her employer, XYZ Inc. We both include our Spouse as an eligible Dependent. My Spouse is eligible for Medicare due to end stage renal disease. What is the order of benefit determination for my Spouse's claims?
Current Medicare Secondary Payer rules establish the employer health plans as primary payer for the first 30 months of Medicare Eligibility due to end stage renal disease. Medicare becomes primary payor after the first 30 months.
The order of benefit determination for the first 30 months would be
XYZ Inc. Spouse's plan pays first. The District plan pays second. Medicare pays last.
The order of benefit determination after 30 months would be
Medicare pays first. XYZ Inc. Spouse's plan pays second. The District plan pays last.

Elmira CSD – rev. 04/28/05 93
SECTION VIII - CLAIM SUBMISSION AND REVIEW PROCEDURES
A. How to Submit a Claim If not using a Network provider, be sure to save all bills and attach original copies to the claim form when submitting claims. If this Plan is the secondary payer, you may attach copies of the original bills with the explanation of benefits or denial from the other Plan. If Medicare is primary for medical Services or Supplies, the provider will usually bill Medicare directly. All you need to do is provide the necessary information to enable the provider to submit to Medicare. The provider may then bill you or POMCO directly.
If Medicare or another health plan is considered to be the primary plan, claims should first be submitted to those plans and then to POMCO with copies of their statement of explanation of benefits or denial. Claims for Services or Supplies needed for an Illness or Injury resulting from no-fault auto accidents or incidents, or for which benefits could be payable by a third party plan not owned by you or your Dependent, should be submitted to the appropriate insurance company. The No-fault Automobile Coverage or third party plan is always primary for expenses resulting from these situations. Claims for Services or Supplies needed for expenses resulting from an occupational Illness or Injury should not be submitted for benefits under this Plan. This Plan excludes such expenses. Be sure to give the provider full details on other coverages to avoid overpayment of Plan benefits. 1. Network Claims (Participating Providers). You do not have to submit claims. A Network provider
will bill the Claims Administrator directly and receive payment directly from the Claims Administrator. You or your Dependents need only present your Plan identification card to confirm Plan eligibility and complete any information requested by the provider. The provider could request your Network Copayments, if applicable, at the time services are Incurred. Be sure to give the Participating Provider full information on other health plans and a history of any accidental injuries.
2. Hospital Inpatient or Outpatient Claims. The Hospital will usually mail claims directly to POMCO.
If you are billed directly, follow the instructions for Other Claims Submissions shown later in this section. If a person is covered by more than one plan, the Hospital will usually bill the plans according to the order of benefit determination shown previously in Section VII - Coordination of Benefits. Example: If Medicare is primary, the Hospital will first bill Medicare and then POMCO, if Medicare does not pay full benefits. The Hospital will usually provide payment information for Medicare and/or other health plan benefits when it submits your claim to POMCO. If not, POMCO will contact you with a written request for copies of the other Plan’s explanation of benefits or denial. Be sure to give the Hospital all your health plan information to facilitate proper billing.
3. Other Claim Submissions. You must take the following steps to submit a claim for benefits anytime
you are billed directly by a provider:
a. A claim form should be obtained from the District’s Business Office or from POMCO. Complete the form according to the instructions shown on the form. Remember: You must attach a completed claim form each time you send in bills and a separate claim form is needed for each family member.
b. Once you have completed your portion of the claim form, the Physician or Dentist can complete his
portion, if needed, or you may attach itemized bills. If an itemized bill is attached, it must clearly state the patient's name, diagnosis, a full description of services rendered and an itemized list of charges with dates of service. If benefits have been assigned to the provider, the bill should also include the provider's signature and tax identification number. Any bill from a nurse must show the date, place and hours of duty, charge per hour, total charges per day, and nurse’s signature, credentials and registration number.
Elmira CSD – rev. 04/28/05 94
c. If services are due to an Accidental Injury, you must provide complete details on how, where, the
date, and the time that the Injury was sustained.
d. Attach Medicare or other plan explanation of benefits or denial, if appropriate, and submit completed forms and bills to:
POMCO
P.O. BOX 6329 SYRACUSE, NY 13217- 6329
POMCO, the Claims Administrator, will accept other valid claim forms that provide the necessary information to decide coverage. If you fail to provide necessary information, POMCO could return your claim for missing information, or POMCO could request additional details which could delay the determination of your benefits. POMCO will advise you of the approval or rejection of your claim by mail.
B. Time Limit on Claim Submission Claims should be submitted as Incurred. Claims for covered expenses may not be submitted later than one year from the date of service. Claims submitted after this time limit will automatically be denied unless a request for an extension has been received and approved by the Claims Administrator or Plan Administrator. This request must be in writing and include the circumstances that show it was not reasonably possible for you to submit the claim for those expenses during that time limit and the late submission was sent as soon as possible. Under no circumstances, will payment be made for claims received more than two years after expenses Incurred.
C. Payment of Benefits/Authorization to Pay Provider All payments made by the Plan under this title will constitute full disbursement of the available benefit and this Plan will not duplicate its payments. Under no circumstances will any authorization obligate the Plan to pay benefits that are not available. Hospital Expense Benefits are paid directly to the Hospital or other facility, if you have not already paid charges. Participating Provider benefits are also paid directly to the Network Provider. All other health benefits are generally paid directly to you unless you sign the authorization on the appropriate section of the claim form to have payment made directly to the provider. A separate claim form should be used for each provider to whom you want direct payment to be made. The Plan may, at its option, accept such authorization of payment to a Hospital, facility, Physician or other Covered provider. The Plan may, at its option, elect to pay benefits directly to a provider or other entity, if appropriate. Without provider tax identification information, the Plan may, at its option, reimburse benefits to you rather than the provider, even if you authorized benefit payment to that provider. When this Plan is considered secondary coverage, the Plan may, at its option, pay you, the provider, or pay the primary plan for its overpaid benefits. In the case of your death or legal incompetence, the Plan may elect to pay benefits to any unpaid provider, your guardian or person with power of attorney, your estate, your Spouse, your parents, your children, or your brothers and sisters as deemed appropriate.
D. Your Right to Benefits,
Although direct payment may be authorized as shown above under Payment of Benefits/Authorization to Pay Provider, under no circumstances may you assign your right to benefits under this Plan to any person, corporation or other organization. You may not assign your right to take legal action under this Plan to any Provider of service. Any assignment of your right to benefits or assignment of your right to legal action

Elmira CSD – rev. 04/28/05 95
under this Plan will be void. No benefit payment under this Plan shall be subject in any way to alienation, sale, transfer, pledge, attachment, garnishment, execution, or encumbrance of any kind, any attempt to accomplish this shall be void. If the Plan administrator finds that such attempts have been made, the Plan Administrator, in its sole discretion, may terminate the interest of such Covered Person or former Covered Person in such payment. If such payments are made, the Plan Administrator may consider such payments as complete discharge of all liability with respect to the Covered Expenses resulting in such payments.
E. Health Claim Inquiries When you have any questions concerning your coverage, you may call the District Business Office or phone POMCO's toll-free number: 1-866-317-7386.
F. Claim Appeals Procedure
If a Covered Person's claim for benefits under this Plan is denied, in whole or in part, the Claims Administrator will provide written notice of the denial within ninety (90) days after its submission. The notice denying a claim for benefits will be written and will include: 1. The specific reasons for the denial; 2. Specific references to the pertinent Plan provisions on which the denial is based; 3. A description of additional information necessary for the claimant to appeal the claim and an
explanation of why such material or information is necessary; and, 4. Information about how to submit the claim for review. 5. A phone number you can call should you need assistance on submitting your appeal. If special circumstances require an extension of time for processing the initial claim, a written notice of the extension and the reason therefore will be furnished to the claimant before the end of the initial 90-day period. In no event will such extensions exceed an additional 90 days. If a claim for benefits is denied or if the applicant had no response to such claim within 90 days of its submission (in which case the claim for benefits will be deemed to have been denied), the applicant may appeal the denial to the Claims Administrator within 120 days from the date of the receipt of written notice of the denial. In pursuing such appeal, the applicant or his or her duly authorized representative: 1. May request in writing that the Plan Administrator or the Claims Administrator review the denial; 2. May review pertinent documents; and, 3. May submit issues and comments in writing, stating in clear and concise terms the reason or reasons for
the disagreement with the claims determination. The request for appeal must be in writing and sent to POMCO, Claims Review, P.O. Box 6329, Syracuse, NY 13217-6329. Failure to send a written appeal within 120 days from the date of the receipt of the written denial could result in continued denial without further claim review by the Plan Administrator or Claims Administrator. If the appeal is denied by POMCO, you may have additional appeal rights. Please refer to your applicable Collective Bargaining Agreement for procedures.
G. Legal Proceedings No action at law or equity or by arbitration if such case is arbitrable under the applicable collective bargaining agreement shall be brought to recover payment under the Plan unless all rights of appeal under the Plan have been exhausted. No action at law or equity shall be brought against the Plan unless such action is commenced within one hundred twenty (120) days of receipt of final denial of the appeal from the

Elmira CSD – rev. 04/28/05 96
Claims Administrator. No arbitration proceeding shall be brought from the final denial of an appeal unless commenced within the applicable time limits for arbitration after receipt of the denial of the appeal.
SECTION IX - OTHER PROCEDURES AND PROVISIONS
A. Not a Contract
All rights accruing to any person under the Plan shall be subject to the terms and conditions of the Plan. The Plan shall not constitute a contract between the Plan Administrator, Plan Sponsor, or the Claims Administrator, and any Covered Employee or Dependent. Maintenance of the Plan shall not be construed to give any Employee enrolled in the Plan the right to be retained as an Employee, or to any benefits not specifically provided by the Plan.
B. Verification of Claim Information The Plan Administrator and the Claims Administrator have the right to request from you or your Dependents, Hospitals, approved facilities, Physicians or other providers, any medical records or information that is necessary for the proper handling of claims. When you become Covered under the Plan, you automatically give permission to the Plan Administrator and the Claims Administrator to obtain, and use, those records and that information. Failure to release such information on a timely basis, or failure by the enrollee, patient, parent, or guardian to authorize the release of appropriate information, could result in denial of benefits. The Claims Administrator confidentially maintains all medical records.
C. Workers' Compensation Payment will not be made for care for any injury, condition, or disease if payment is available to you under a Workers' Compensation Law or similar legislation. POMCO will not make any payments even if you do not claim benefits you are entitled to receive under the Workers' Compensation Law. Also, payment will not be made even if you bring a lawsuit against the person who caused the injury or condition. Payment will not be made even if you receive money from that lawsuit and you have repaid the hospital or other provider.
D. Indemnity Benefits
Benefits under the Plan are only payable for services actually rendered or delivered. Except as otherwise specified, benefits cannot be preapproved or prepaid. Benefit determination will be based on Plan limitations (eligibility, benefits, etc.) and exclusions in effect at the time services are rendered.
E. Misrepresentation/Fraud If it is found that a claim for benefits, or any materials provided for evaluating a claim for benefits under the Plan, contains materially false information, or that you or your Dependent or a provider conceals, for the purpose of misleading, information concerning any fact material to a claim for benefits thereto, such claim may be denied in total and the Plan Administrator and/or the Claims Administrator may recover any benefits paid to you and/or a provider. This paragraph does not affect the right of the Plan Administrator to pursue any criminal or civil remedies that may exist under applicable state or federal law.
F. Refund Due to Overpayment of Benefits If payment has been made for Covered Services or Supplies under the Plan that are more than the benefits that should have been paid, or for Services or Supplies that should not have been paid under the provisions of the Plan, the Plan Administrator or the Claims Administrator shall have the right to recover the

Elmira CSD – rev. 04/28/05 97
overpayment or improper payment, or to offset future payments (1) from such Covered Person who received an overpayment or improper payment, (2) from any provider which received an overpayment or improper payment, or (3) from any insurer or other entity which benefited from the overpayment or improper payment. The Plan Administrator reserves the right to deduct any excess or improper payment from any present or future amounts payable to a provider, carrier, or entity. Payments made in error for Services or Supplies not Covered by this Plan shall not be considered certification of coverage and will not limit the enforcement of any provision of the Plan for any and all claims submitted under the Plan.
G. Right of Subrogation/Reimbursement
The conditions shown below do not apply to any payments made under any insurance policy, plan or certificate issued to you or your Dependents. This Plan specifically does not provide any coverage with respect to any Injury or Illness for which a third party may be liable or legally responsible. If you or your Dependent receive payment or expect payment from a third party insurance, surety or other type plan not owned by or issued to you or your Dependent for medical expenses resulting from such Injury or Illness, you should not submit a claim under this Plan for such medical expenses. Any Plan benefits paid against such claims will be considered an overpayment. The Plan will exercise its right to full reimbursement for resulting overpayments. However, if for some reason the third party claim payment or settlement is expected to be delayed for an extended time, the Plan Administrator may, at its option, authorize Plan benefits for medical expenses that would otherwise be Covered by this Plan. The rules shown below govern how this Plan pays benefits in such situations. 1. Conditional Benefit Payment. If a Covered Person has medical expenses resulting from an Injury, or
Illness for which a third party is, or may be, held responsible and such third party payment or settlement is withheld for an extended period, the Plan Administrator may, at its option, authorize conditional interim benefit payments for medical expenses that would otherwise be Covered by the Plan. However, any advance payments are subject to the Plan’s subrogation rights. Before such benefits are conditionally made, you and/or your eligible Dependent, or authorized representative, if a minor, must execute an agreement that acknowledges and affirms (a) the conditional nature of such benefit payments and (b) the Plan’s rights of subrogation, as shown below.
2. Subrogation Agreement. If benefits are paid or payable by this Plan as the result of an action of a
third party, this Plan will be subrogated to all rights of recovery of any Covered Person under this Plan in respect to such action. In addition, once it is determined that a third party is liable in any way for the injuries, or Illnesses, causing these expenses, in order to receive benefits, or to continue receiving benefits from this Plan, you must take the following steps or all benefit payments to you will be stopped.
You are required to advise the Claims Administrator, in writing, of any expenses for which a third party may be liable. You and/or your eligible Dependent, or authorized representative if a minor or if unable to sign, must execute and deliver such documents, notices or papers as may be required and must do whatever else is needed to secure the Plan rights, including the following:
a. You and/or your eligible Dependent, or legal representative must agree, in writing, to give the
Claims Administrator written notice whenever a claim is asserted or could be asserted against and/or recovery is received from any third party (or insurer or surety thereof) for damages as the result of the Injury or Illness; and
b. You and/or your eligible Dependent, or legal representative must agree, in writing, on a form
acceptable to the Claims Administrator, to reimburse this Plan for any Plan payment resulting from such Injury or Illness. Plan benefits must be reimbursed 100% from any settlement, judgment or other payment that you obtain from the liable third party before any other expenses, including
Elmira CSD – rev. 04/28/05 98
attorneys' fees, are deducted. c. You and/or your eligible Dependent, or legal representative must provide, in writing, an assignment
of proceeds or a lien against such proceeds, in favor of the Plan in the amount of any benefits paid by the Plan due to such Injury or Illness; such assignment to be valid against any judgment, settlement, or recovery in any manner that is or will be received from such third party or such third party's insurer or surety.
If you or your Dependent fail to tell the Plan Administrator, or the Claims Administrator, that you or your Dependent has a claim against a third party; if you or your Dependent fail to assign your claim against the third party to the Plan when required to do so (and to cooperate with this Plan’s subsequent recovery efforts); if you or your Dependent fail to require any attorney subsequently retained to sign the Plan’s lien forms; if you and/or your Dependent and/or authorized representative or attorney fail to fully reimburse this Plan out of any payment obtained from the third party or fail to fully reimburse the Plan, then you are personally liable to this Plan for the reimbursement owed this Plan as the result of the third party payment or settlement. This Plan may then request reimbursement from you and offset the amount you owe from any future benefit claims for any Covered Family Member or, if necessary, take legal action against you. The amounts to be recovered by the Plan pursuant to this provision cannot be reduced by any attorney’s fees, court costs or other disbursements.
The Plan Administrator or the Claims Administrator reserves the right to deny benefits for any charges that are, or could be, considered subject to the Plan’s right of subrogation for failure by you and/or your eligible Dependent or legal representative to comply with the above conditions.
H. Amendments or Termination of the Plan
The Plan may be amended, from time to time, to be in accordance with Law, or Regulation, or as required by the Collective Bargaining Agreements. If the Plan terminates, coverage will end for all persons enrolled under the Plan.
I. Named Fiduciary and Plan Administrator
The named fiduciary and Plan Administrator is the Elmira City School District, which has the authority to control and manage the operation and administration of the Plan. The Plan Administrator may delegate responsibilities for the operation and administration of the Plan. Such delegations shall be in writing. The Plan Administrator will have the authority to appoint or remove plan supervisors, plan managers or claim administrators, fix their compensation, if any, and exercise general administrative authority over them.
J. Severability If any provision of the Plan shall be found by a court of competent jurisdiction to be void, invalid, or unenforceable, the same shall either be reformed to comply with applicable law or stricken, if not so conformable, so as not to affect the validity or enforceability of the remainder of the Plan.
K. Waiver and Estoppel
No term, condition, or provision of this Plan shall be deemed waived, and there shall be no estoppel against enforcing any provision of the Plan, except through a writing of the party to be charged by the waiver or estoppel. No such written waiver shall be deemed a continuing waiver unless explicitly made so, and shall operate only regarding the specific term or condition waived, and shall not be deemed to waive such term or condition in the future, or as to any act other than specifically waived. No Enrollee, participant or beneficiary other than as named, or described by class, in the waiver shall be entitled to rely on the waiver for any purpose.

Elmira CSD – rev. 04/28/05 99
L. Headings
All article and section headings in this Plan have been inserted for convenience only and shall not determine the meaning of the content thereof.
M. Federal and State Laws
This Plan shall be governed and construed according to Law. Laws will affect the provisions of this Plan only when directed at this type of self-funded health Plan for Plan Sponsors regulated by the particular Law.
SECTION X - DEFINITIONS
Certain words and phrases applicable to or used in this Master Plan Document (MPD) are listed below with the definition or explanation of the manner in which the term is used for the purpose of the Plan. Masculine pronouns shall include masculine or feminine gender, unless the context shows otherwise. ACCIDENTAL INJURY - Non occupational bodily Injury caused by an event that is sudden and not foreseen, and is exact as to time and place. The Injury must be unexpected and unavoidable. For example, the breakdown or fracture of Natural Teeth caused by chewing will not be considered Accidental Injury. ACTIVE EMPLOYEES - See Section II, Eligibility and Enrollment. ALCOHOL FACILITY - See Substance Abuse Facility. ALLOWABLE FEE - The Usual, Customary and Reasonable Charge as determined by the Claims Administrator for Covered medical services rendered and billed by a Covered Out-of-Network Provider. If billed by a Network Provider, the term Allowable Fee means the Network scheduled allowance or negotiated allowance based on the provider’s Network agreement with the Claims or Plan Administrators. If Medicare is primary, the Allowable Fees could be based on Medicare’s allowance or limiting charges. The Plan will not pay charges that exceed Allowable Fees. The Enrollee may be responsible for payment of any charges that are not allowed under the Plan. ALLOWABLE SERVICES or SUPPLIES - See Covered Services or Supplies. AMBULATORY SURGERY - Surgery rendered on other than an Inpatient basis. Examples include surgery performed in a Physician’s office, clinic, outpatient department of a Hospital, ambulatory facility, or other outpatient location. AMBULATORY SURGICAL FACILITY - A specialized facility operated according to the applicable laws of the jurisdiction in which it is located; or accredited by the Joint Commission for the Accreditation of Healthcare Organizations or the Accreditation Association for Ambulatory Care; or approved by Medicare to render outpatient services for Ambulatory Surgery. The facility must be organized and used mainly for outpatient surgery, have a staff of surgeons, anesthesiologists, and full-time professional nurses. If the center is part of a Hospital, it will not be considered an Ambulatory Surgical Facility. AMENDMENT - A change, revision, deletion, or addition to the Master Plan Document and/or Summary Plan Description by the Plan Administrator, consistent with the Collective Bargaining Agreement. APPROVED CARE or APPROVED PLAN OF CARE - Any service or course of treatment approved for benefits by the Claims Administrator under the terms and limitations of the Plan.

Elmira CSD – rev. 04/28/05 100
AVERAGE SEMI-PRIVATE ROOM RATE - The standard semi-private rate for room and board charges by a Hospital or other Covered Inpatient health facility. If the Inpatient facility does not have a semi-private rate, the rate shall be deemed to be 80% of the room and board charges made by the facility for its lowest priced private room accommodations. If the facility has several semi-private rates, the prevailing, or the most common rate, shall be used. Semi-private accommodations are usually rooms with two or more beds. BEAUTIFYING PROCEDURES - See Cosmetic Procedures. BIRTH CENTER or BIRTHING CENTER -A free standing facility or Hospital center established, equipped and operated, according to the applicable laws of the jurisdiction in which it is located, or accredited by either the Joint Commission for Accreditation of Healthcare Organizations or the Accreditation Association for Ambulatory Care, or by Medicare, to provide Inpatient and outpatient maternity care for uncomplicated pregnancies, including routine prenatal care, routine full-term delivery, and immediate postpartum care. The facility must have an agreement with a local Hospital to accept emergency admissions of its maternity patients with serious complications. CALENDAR YEAR - A period of twelve consecutive months, starting at 12:01 A.M. of January 1 and ending at midnight on December 31. CLAIMS ADMINISTRATOR - The person or organization under contract with the Plan Administrator for determining payment and processing of the claims under the Plan. CLOSE RELATIVE - See Immediate Relative. COBRA - The continuation of Plan Coverage according to Federal regulations under the Consolidated Omnibus Budget Reconciliation Act of 1986 and subsequent Federal COBRA regulations affecting this type of Plan. COLLEGE or UNIVERSITY - An institution listed in the current American Council on Education publication of Accredited Institutions of Post-Secondary Education. CONTRIBUTION - The portion of the Plan costs that the Plan Administrator or Plan Sponsor collects from Plan Enrollees or participants to provide coverage under the Plan. CONVALESCENT CARE FACILITY - See Skilled Nursing Facility. CONVALESCENT PERIOD - A period of time commencing with the date of a covered inpatient admission by a Covered Person to a skilled nursing facility and ending when the covered person has been free of inpatient care in any and all institutions providing hospital and nursing care for 90 consecutive days. COPAYMENT - That figure shown as a percentage used to compute the benefits payable or a dollar amount applied to Allowable Fees. The Covered Person is responsible for payment of any Copayment balance not paid by the Plan. COSMETIC PROCEDURES - Services or Supplies related to procedures performed solely for the improvement of a Covered Person's appearance rather than for improvement or restoration. COVERAGE OR COVERED - Medical Services or Supplies for which benefits are payable according to Plan limitations, provisions and exclusions. COVERED DEPENDENT - See Dependent.

Elmira CSD – rev. 04/28/05 101
COVERED EXPENSES - Allowable Fees charged by Covered providers for medical Service or Supplies that are Covered according to Plan provisions, limitations and exclusions. The Enrollee or participant may be responsible for payment of any expenses not Covered by the Plan. COVERED FAMILY MEMBER -The Enrollee and his or her Eligible Dependents enrolled in the Enrollee’s family coverage. COVERED PERSON - Any person eligible and enrolled for benefits or coverage under this Plan, according to Plan provisions, limitations and exclusions. COVERED PROVIDER - See Provider COVERED SERVICES OR SUPPLIES - Services or Supplies found medically necessary and covered under the Plan limitations, provisions and exclusions. CUSTODIAL or CUSTODIAL CARE - Any institutional, outpatient, or professional care that is not related to the diagnosis or treatment of an Illness or Injury. Care is also custodial when it is primarily to meet personal needs. Examples of Custodial Care include, but are not limited to, assistance in the activities of daily living (such as help in walking, getting in and out of bed, bathing, dressing, eating, and taking medicine); administration of oral medications; assistance with supportive or Maintenance physical therapy; care due to incontinence; turning and/or positioning in bed; services of a companion or sitter; or nurse aide services. Care that cannot reasonably be expected to lessen the patient’s disability enabling him or her to leave an institution will be considered Custodial Care. DEPENDENT - An Enrollee's Spouse or an Enrollee's child who meets the conditions shown in Section II - Eligibility and Enrollment. DOCTOR - A person legally licensed to practice medicine (M.D.) or osteopathy (D.O.). See also Physician. DRUG ABUSE FACILITY - See Substance Abuse Facility. DURABLE MEDICAL EQUIPMENT - Equipment determined by the Claims Administrator to be Medically Necessary for the treatment of disease or Accidental Injury or to improve body function lost as the result of a disease, Injury or congenital abnormality which meets all of the following requirements. Durable Medical Equipment must be: 1. Prescribed by a Physician who indicates the necessity of the item, including diagnosis, reason for use,
purpose, expected duration of use and a full description of item prescribed; 2. Non-aesthetic in nature; 3. Safe and effective for home use without medical supervision; 4. The most appropriate equipment or model for the reported condition. Deluxe equipment is not
allowable when standard equipment is available and medically adequate for the reported condition; 5. Made to stand extended and repeated use. Disposable Supplies may be allowed if required to operate
the medical equipment; 6. Required to replace body function lost or impaired due to disease, Injury or congenital abnormality or is
Medically Necessary to carry out necessary activities of daily living connected to the patient's health or hygiene with little to no aid from others. It must not be solely for the convenience of the patient or the patient's caregiver; and
7. Used to serve a medical purpose. It must not be useful without disease or Injury and must not be for comfort, used to enhance the patient's home or environment, communication, alter air quality or temperature or for exercise or training.

Elmira CSD – rev. 04/28/05 102
EFFECTIVE DATE or EFFECTIVE DATE OF COVERAGE - The date coverage is effective with respect to an eligible and enrolled Employee or Dependent, after any designated Waiting Periods. See Waiting Periods. ELIGIBLE DEPENDENTS - See Dependents. ELIGIBILITY WAITING PERIOD - See Waiting Period. EMERGENCY MEDICAL CARE - Treatment for a sudden, unexpected onset of a medical condition of such nature that failure to render immediate care could reasonably result in deterioration to the point of placing the Covered Individual's life in jeopardy or cause serious impairment to the Covered Individual. In no event, shall benefits for such care be provided unless the care was rendered less then 12 hours after the first appearance of the symptoms of the illness. EMERGENCY CENTER or URGENT CARE FACILITY - A legally operated emergency clinic or center that meets the requirements in the jurisdiction of license to provide outpatient Emergency Medical Care or emergency minor surgery, but in no way is owned or operated by a Hospital. It must be a facility that is primarily engaged in providing minor emergency and episodic care to a Covered Person. A qualified Physician, a registered nurse, and a registered x-ray technician must be in attendance at all times when the center is open. The center must have x-ray and lab equipment and a life support system on the premises. A clinic, center, or facility meeting these requirements will be considered an urgent care center by whatever actual name it may be called. EMPLOYEE - Any person who is considered an eligible Employee according to criteria established by the Plan Administrator as set forth in Section II - Eligibility and Enrollment. It does not mean persons without employment status, such as former employees that have been retired, terminated or laid off, unless they are continuing coverage during an authorized leave of absence. ENROLLEE or COVERED ENROLLEE - An employee or retiree who is eligible for coverage and elects to be enrolled as a Plan participant. A survivor or COBRA participant or USERRA participant whose Social Security number is used for Plan enrollment. EXPERIMENTAL - Any care that is not widely accepted professionally in the United States as effective, appropriate and essential treatment of a reported Illness or Injury based upon recognized standards of health care in effect at the time Services or Supplies were Incurred. A drug, device, medical treatment or procedure is Experimental if: 1. The drug or device cannot be lawfully marketed without approval of the U.S. Food and Drug
Administration (FDA) and approval for marketing has not been given at the time the drug or device is furnished or an FDA-approved drug or device is used for purposes other than those conditions for which approved;
2. Reliable evidence shows that the drug, device or medical treatment or procedure is the subject of ongoing Phase I, II or III clinical trials or under study to decide its maximum tolerated dose, its toxicity, its safety, its efficacy, or its efficacy as compared with the standard means of treatment or diagnosis;
3. Reliable evidence shows that the consensus among experts regarding the drug, device or medical treatment or procedure is that further studies or clinical trials are necessary to determine its maximum tolerated dose, its toxicity, its safety, its efficacy, or its efficacy as compared with the standard means of treatment or diagnosis;
4. Reliable evidence shows that the consensus among experts is that the drug, device or medical treatment or procedure once recognized as effective is no longer considered usual, customary, reasonable or necessary care;
5. The Centers for Medicare & Medicaid Services (CMS) coverage criteria are not met for the drug, device or medical treatment or procedure; or

Elmira CSD – rev. 04/28/05 103
6. The Claim Administrator decides that the treatment, procedure, device, drug or medicine is Experimental.
Reliable evidence shall mean only published reports and articles in the authoritative medical and scientific literature; the written protocol or protocols used by the treatment facility or the protocol(s) of another facility studying substantially the same drug, device or medical treatment or procedure; or the written informed consent used by the treating facility or by another facility studying substantially the same drug, device or medical treatment or procedure. If any of the entities used to determine the status of a drug, a drug, device, supply, treatment or any other medical service reverses, modifies, or establishes its policy for such expenses, and makes such changes retroactive, the Plan will not make payment for related retroactive Incurred expenses. The Plan will not seek refund for its previous payments, nor make payments for any previously denied expenses, affected by such retroactive changes. EXTENDED CARE FACILITY - See Skilled Nursing Facility. FULL-TIME - A basis of employment that requires the Enrollee to be at work for at least the qualifying hours per week based on criteria established by the employer or by negotiated agreement. GENERAL HOSPITAL - See Hospital. HEALTH CARE BENEFITS - Medical Expense Benefits according to Plan provisions and paid by the Plan Administrator. HOME HEALTH AIDE - A person, other than a Physician or a nurse who provides care that is primarily to aid a homebound patient in performing daily activities while recovering from an Injury or sickness. The aide must report to and be under the direct supervision of a home health care agency which bills for the aide’s services. Services must be part of an approved plan of home health care. HOME HEALTH CARE AGENCY - A licensed agency or Hospital that has been issued a current operating certificate as a certified home health agency by the New York State Department of Health. Outside New York State, the agency must have a similar operating certificate issued by the state of jurisdiction; or be certified by Medicare as a participating Home Health Care Agency. HOME HEALTH CARE PLAN - A plan to provide out of Hospital care to a person rendered by an approved home health care agency. To qualify, the established care plan must be approved in writing by an attending Physician who certifies that the person would require confinement in a Hospital or convalescent nursing home/extended care facility/Skilled Nursing Facility if he did not have the care and treatment stated in the care plan. The patient must remain under the supervision and care of the attending Physician during the period home health care is provided. HOSPICE AGENCY - An organization that has an appropriate operating certificate issued by the New York State Department of Health to provide hospice care. Outside New York State, the hospice organization must be certified under criteria similar to those used in New York by a state agency in the state where the hospice care is provided, or it must be approved by Medicare. HOSPITAL - A short term acute care institution that makes charges and is engaged primarily in providing medical care and treatment to sick and injured persons on an Inpatient, or outpatient, basis at the patient's expense, which fully meets all of the following requirements: 1. It is an institution operating and licensed according to the law of the jurisdiction in which it is located
concerning institutions identified as Hospitals; 2. It is primarily engaged in providing diagnosis, treatment and care of injured or sick persons on an
Inpatient basis and receives compensation from its patients. It maintains organized departments on the

Elmira CSD – rev. 04/28/05 104
premises for major operative surgery, and it provides twenty-four (24) hour nursing services by or under the full time supervision of professional registered nurses;
3. If located in New York State, it has in effect a hospitalization review plan, applicable to all patients, which meets at least the standards set forth in section 186 (k) of United States Public Law 89-87 (42 USCA 1395x (k)). If not located in New York State, it is a Hospital accredited by the Joint Commission on Accreditation of Healthcare Organizations as an acute care facility.
4. It is not, other than incidentally, a Skilled Nursing Facility, extended care facility, convalescent facility, extended care facility, a nursing home, a place for rest, Custodial Care, education or rehabilitation care, for the aged, a place for the mentally ill or emotionally disturbed, or a place for the treatment of drug addiction or alcoholism.
HOSPITAL MISCELLANEOUS - Charges made by a Hospital on its own behalf for medical Service or Supplies given to a Covered Person either on an Inpatient or outpatient basis. Such Service or Supplies must be Medically Necessary for the patient’s treatment. Room and board and professional services (including intensive nursing care by whatever name called), are not considered Hospital miscellaneous expense whether given under the direction of the Hospital or otherwise. ILLNESS -Any Non occupational Injury, sickness, disease, bodily disorder, functional mental disorder that manifests treatable symptoms and requires the professional medical treatment of the affected Covered Person. IMMEDIATE RELATIVE of patient or Enrollee - Any of the following: 1. Spouse of the patient or Enrollee; 2. Natural or adoptive parent, child or sibling; 3. Stepparent, stepchild, stepbrother or stepsister; 4. Father-in-law, mother-in-law, brother-in-law, or sister-in-law; 5. Grandparent or grandchild; or 6. Spouse of grandparent or grandchild. INCURRED DATE - The date the service or supply was rendered or received. INCURRED or INCURRED EXPENSES - Those Services or Supplies given to or received by a Covered Person. Such expenses shall be considered to have accrued at the time or date the service or supply is actually provided. INJURY – See Accidental Injury. INPATIENT or INPATIENT CARE - The period during which a Covered Person is treated in a Hospital or any other Covered facility as a registered bed patient for whom room and board charges are made. INSURERS - An insurance or reinsurance company and excess or stop loss carriers. INVESTIGATIONAL - See Experimental. LATE ENTRANT - An eligible Employee or eligible Dependent who is enrolled for Plan coverage more than 31 days after initial eligibility. LEGAL SPOUSE - See Spouse. LEGEND DRUG - a drug or compound which requires a prescription order and which is required by Law to bear the legend "Caution - Federal Law prohibits dispensing without prescription."

Elmira CSD – rev. 04/28/05 105
LIFETIME - Any reference to Lifetime shown in this Plan means all periods during which the person is Covered under the Plan. Under no circumstances, does the Plan pay benefits for any period during which the person does not meet Plan eligibility or continuation requirements. MAINTENANCE CARE - Care rendered and directed at relieving discomfort or preserving function secondary to conditions where further enhancement of function cannot be demonstrated or expected. Care that cannot be reasonably expected to lessen the patient’s disability enabling him or her to leave an institution. Maintenance Care does not imply the absence of symptoms nor does it imply such services are not necessary. It implies care rendered to maintain a function and prevent the condition from worsening. MEDICAL EXPENSE BENEFITS or MEDICAL BENEFITS - Plan payment for Covered medical services, Supplies, or devices related to treatment of Illness or injuries and for specified preventive services. MEDICALLY NECESSARY or MEDICAL NECESSITY - Services, drugs, Supplies or equipment provided to a patient for the treatment of an Illness or Injury, only when it meets all of the following requirements: 1. It is consistent with the symptom or diagnosis and treatment of the sickness, disease, ailment or Injury; 2. It is according to generally accepted standards of good medical practice in the USA at the time expenses
Incurred; 3. It is the most appropriate level of service, drugs, Supplies or equipment that can be safely
provided to the Covered Person. With respect to Inpatient Care, appropriate level of service means that the medical condition requires Inpatient Care and that safe and effective treatment cannot be rendered as an outpatient.
4. It is not Experimental, Investigational, or of an educational nature, primarily for medical or other research;
5. It is not considered Maintenance Care or Custodial Care; and 6. It is care requiring the credentials and technical skills of the provider of service. The fact that a Physician or other health care professional may prescribe, recommend, order or approve a service or supply does not, by itself, determine Medical Necessity or make such service or supply eligible for benefits, even if not expressly excluded under the Plan. The determination will be based upon the findings and assessment of the following: 1. The Office of Medical Application of Research of the National Institutes of Health, the Office of
Technology Assessment of the United States Congress, the Federal Health Care Finance Administration (HCFA), or any similar entities;
2. The National Medical Associations, Societies and Organizations; 3. The Federal Drug Administration (FDA); or 4. The Claim Administrator's or Plan Administrator's own medical and legal consultants and advisors. If any of the entities used to determine the Medical Necessity of a drug, device, supply, treatment or any other medical service, reverses, modifies, or establishes its policy for such expenses and makes such changes retroactive, the Plan will not make payment for retroactive Incurred expenses. The Plan will not seek refund for it previous payments, nor make payments for any previously denied expenses affected by such retroactive changes. MEDICARE - The coverage of health care costs provided under the provisions of the Federal Social Security Act (42 USC 1395 et seq.), as amended. MENTAL HEALTH CARE - Treatment for a diagnosed mental disease or disorder or a functional nervous disorder, as shown in the most current edition of American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders. See also Illness.

Elmira CSD – rev. 04/28/05 106
MENTAL ILLNESS - See Mental Health Care. NATURAL TEETH - Organic conical structures of the oral cavity used for chewing that is formed by the natural development of the body (not manufactured). NETWORK PROVIDER - An organization, Physician, Hospital, Pharmacy or other professional healthcare provider that, at the time Covered Services or Supplies are provided, is part of the participating Network (s) selected by the plan. The Network Provider has a contract or agreement with the Network organization and the Plan or the Claim Administrators to bill negotiated charges or scheduled allowances for Covered Services or Supplies when Incurred by Covered Persons. NEWBORN - An infant from the date of birth until the initial Hospital discharge or until the infant is fourteen days old, whichever event occurs first. NO-FAULT AUTOMOBILE COVERAGE - The basic reparations provisions of a law providing for payments without determining fault in connection with injuries or conditions sustained in the use or operation of an automobile or other vehicle, as mandated under the applicable law. NON OCCUPATIONAL - A disease or Injury that does not arise and is not caused or contributed to, by or because of, any disease or Injury that arises out of or during any employment or occupation for compensation or profit. NON PARTICIPATING PROVIDER - See Out-of-Network Provider. NON PREFERRED PROVIDER - A provider who does not have a contract for services directly with the Plan. OUT-OF-NETWORK PROVIDER - An organization, Physician, Hospital, Pharmacy or other healthcare provider that, at the time Covered Services or Supplies are provided, does not have a contract or agreement with the Claim Administrator or the Participating Provider Network selected by the Plan Administrator to provide medical Services or Supplies to the Covered Persons under the Plan for scheduled or negotiated charges or allowances. OUTPATIENT - Care rendered in the outpatient or emergency department of a Hospital or other health facility, care rendered in the provider's office, patient's home or other care rendered on other than an Inpatient basis. PARTICIPATING PROVIDER - See Network Provider. PERCENTAGE COPAYMENT - See Copayment. PHYSICIAN - The following who are legally licensed and providing Covered medical services within the scope and jurisdiction of their license: A medical doctor (M.D.), osteopath (D.O.); Dentists (D.D.S. or D.M.D.) for Covered dental care; chiropodist/podiatrist (D.P.M) for treatment of the feet; licensed clinical psychologists for Mental Illness care; certified nurse midwife for maternity care. PREFERRED PROVIDER - A provider whose services are paid for pursuant to a contract directly with the Plan. PREGNANCY - That physical state of Pregnancy which results in childbirth, abortion or miscarriage. This definition includes medical complications of the physical state of Pregnancy. Pregnancy or maternity care will be considered for benefits the same as any other Illness subject to Plan limitations and exclusions.

Elmira CSD – rev. 04/28/05 107
PREMIUM EQUIVALENT - The amount that equals the designated monthly enrollee contribution for Plan participation plus the employer's determined contribution toward Plan costs. PROSTHETICS - The making and application of any artificial part that replaces all or part of a body part, organ or function lost or impaired as the result of disease or Injury. This does not include, for example, eyeglasses or contact lenses, hearing aids, wigs, orthopedic shoes or supportive devices for the feet. PROVIDER - Any legally licensed Physician or any physical therapist, speech therapist, certified psychiatric social worker (for Mental Illness care), or other health care providers giving a covered service ordered by a Physician. Any licensed independent laboratory, Hospital, Skilled Nursing Facility, Substance Abuse Facility, Hospice Agency, Home Health Care Agency; or other facility/agency included for Plan coverage. Coverage includes charges billed by Urgent Care Facilities, and other health centers or clinics for Covered Services given by Covered Physicians or other healthcare providers that would otherwise be Covered by the Plan. Also, see definitions for certain providers. To be Covered, a provider must meet Plan definitions and limitations, render a Covered service within Plan limitations, be operating within the scope of their license, and operating according to the laws of the jurisdiction where Services or Supplies are given or delivered. PSYCHIATRIC CARE - See Mental Health Care REHABILITATION FACILITY - A facility established, equipped and operated, according to the applicable laws of the jurisdiction in which it is located to provide restorative therapy to disabled persons on an Inpatient or outpatient basis. The facility must be approved by the Joint Commission on Accreditation of Healthcare Organizations for rehabilitation care or be a Medicare approved facility for Medicare Part A Skilled Nursing Facility benefits. See Skilled Nursing Facility. ROUTINE NEWBORN NURSERY CARE - Charges made by the caring Hospital or a similar institution and/or the attending Physician for the custodial and nursing care, including circumcision, of a Newborn infant who is deemed to be free of any identifiable Illness or disease requiring treatment. SEMI-PRIVATE ROOM CHARGE - See Average Semi-private Room Rates. SERVICES OR SUPPLIES - See Covered Services or Supplies. SICKNESS - See Illness. SKILLED NURSING FACILITY - An institution or part thereof that meets one of the following requirements: 1. The facility or part thereof must be licensed and operating within the jurisdiction of applicable state
laws, if any, and accredited as a Skilled Nursing Facility, by the Joint Commission on Accreditation of Healthcare Organizations; or
2. The facility or part of the facility (including a facility referring to itself as an extended care facility, Rehabilitation Facility or convalescent nursing home or any other similar nomenclature) must be certified by Medicare as a facility eligible for Medicare Part A Skilled Nursing Facility benefits.
SPEECH FUNCTION – A person’s ability to express thoughts, speak words, and form sentences. SPOUSE - A person who is the legal husband or wife of an eligible Employee, according to the laws of the state or other jurisdiction in which the eligible Employee resides. SUBSTANCE ABUSE - A condition caused by regular excessive compulsive drinking of alcohol or physical habitual dependence of drugs that result in chronic disorders affecting physical health and/or

Elmira CSD – rev. 04/28/05 108
personal or social functioning. This does not include tobacco dependence and ordinary caffeine-containing drinks. SUBSTANCE ABUSE FACILITY - An agency or freestanding facility or a Hospital center that is certified by the New York State Office of Alcoholism and Substance Abuse Services (OASAS) for the outpatient treatment of Substance Abuse (drugs and alcohol). For services given outside New York, the facility must be certified by a state agency similar to the New York State OASAS. If a state does not have a certification regulation, the facility must be approved by the Joint Commission on Accreditation of Healthcare Organizations for the outpatient treatment of Substance Abuse. SUPPLIES - Drugs, medicines, devices, appliances, equipment, braces, casts, prosthetics, materials, or other items manufactured and used for medical care. SURGERY - Any of the following: 1. To incise, excise or cauterize any organ or body part, except for dental services; 2. To repair, revise or reconstruct any organ or body part; 3. To treat or to reduce by manipulation a fracture or dislocation; 4. To use endoscopy to diagnose or explore for or to remove a stone or other object from the larynx,
bronchus, trachea, esophagus, stomach, intestine, urinary bladder or ureter; 5. An injection for contrast media testing or for therapeutic purposes; 6. Other procedures may be considered as surgery by the Claims Administrator. USERRA - The federal laws under The Uniformed Services Employment and Reemployment Rights Act, as amended. USUAL, CUSTOMARY AND REASONABLE CHARGE (UCR) - The lowest of: 1. The actual charge for the Covered service or supply; 2. The usual charge by the Physician or other provider for the same or similar service or supply; or 3. The usual charge of other providers in the same or similar geographic area for the same or similar
service or supply (prevailing fee). In the determination of benefits for a claim, the usual level of charges may be modified by a relative value study, where appropriate, to model actual claims experience in a given area across a range of percentiles. The term "area" as it would apply to any particular service, medicine, or supply means a zip code, county or such greater area as is necessary to obtain a representative cross section of level charges. The part of the cost that exceeds that of any other services that would have been sufficient to safely and adequately diagnose or treat an individual's physical or mental condition will not be deemed as usual, customary or reasonable charges. The determination of the Usual, Customary and Reasonable Charges for Covered Services or Supplies is made by the Claims Administrator. WAITING PERIOD - The designated period between the Employee's date of eligible employment and the date the Employee becomes eligible for Plan coverage and benefits.

Elmira CSD – rev. 04/28/05 109
In Witness Whereof, the Plan Administrator, has caused this restated Summary Plan Description and Master Plan Document for the self-funded Elmira City School District Health and Dental Plan to be executed in its name and behalf as of the 28th day of April 2005. Elmira City School District (Authorized Signature) (Title)

Elmira CSD – rev. 04/28/05 110
Whereas, on June 13, 2002, the Elmira City School District Self Insured Health Plan (“The Plan”) Health Committee established a subcommittee composed of Jean Biggs, Paul Mayo, Robert Gosden, Shawn Morris and Sue Skidmore to draft a Master Plan Document (“MPD”) for the Plan, and Whereas, the Subcommittee which also came to include, Tim O’Brien, Mike Thomas, Carol Allington, Kevin O’Shea, and POMCO met periodically between June 13, 2002 and August 23, 2003 for the purpose of developing a MPD based on the existent documentation as understood by the subcommittee, and Whereas, the Subcommittee, did not have the authority to increase or diminish the Plan’s benefits, as a result of its work, and Whereas, from time to time the Subcommittee reported to the Plan’s Health Committee on its progress, and, in fact, presented a MPD to the Plan’s Health Committee, with the consensus of the Subcommittee, for its review and consideration, and Whereas, on August 25, 2003, the Plan’s Health Committee adopted a resolution approving the MPD as revised, Be it resolved, that on this date, April 28, 2005, the Plan’s Health Committee hereby commends Jean Biggs, Paul Mayo, Robert Gosden, Shawn Morris, Sue Skidmore, Tim O’Brien, Mike Thomas, Carol Allington, Kevin O’Shea, and POMCO for their work, and furthermore, The Plan’s Health Committee approves the attached Elmira City School District Self Insured Health Plan Summary Plan Document (“SPD”). By approving the SPD, the Health Committee does not intend to increase or decrease the Plan’s benefits. Likewise, this Committee’s prior resolution of August 25, 2003 adopting the MPD was not intended to increase or decrease the Plan’s benefits.

Elmira CSD – rev. 04/28/05 111
APPENDIX A
Elmira Area Zip Code List for All Plan Options
Enrollees and healthcare providers in the following zip codes are considered to be in-area.
13617 13734 13840 14805 14812 14814 14816 14821 14824 14825 14827 14830 14838 14844 14845 14858 14859 14861 14864 14865 14867 14869 14870 14871
14872 14883 14889 14891 14892 14894 14897 14901 14902 14903 14904 14905 15478 16914 16825 16929 16936 18471 18810 18817 18840

112
APPENDIX B Elmira Area Benefit Clarifications
Plan A Plan B
Enrollee lives inside zip code area:
uses ELM provider inside zip code
Inside Option A Plan Network benefits apply, using ELM fee schedule. (Inside Option A Plan Network deductible and out of pocket where applicable)
Inside Option B Plan Network benefits apply, using ELM fee schedule. (Inside Option B Plan Network deductible and out of pocket where applicable)
uses POMCO provider inside zip code
Inside Option A Plan Network benefits apply, using POMCO fee schedule. (Inside Option A Plan Network deductible and out of pocket where applicable)
Outside Option B Plan Network benefits apply, using POMCO fee schedule. (Outside Option B Plan Network deductible and out of pocket expenses shall apply)
uses POMCO provider outside zip code area with referral
Inside Option A Plan Network benefits apply, using POMCO fee schedule. (Inside Option A Plan Network deductible and out of pocket where applicable) Letter of Referral from Physician is necessary.
If referred to POMCO provider but services were available inside ELM - Outside Option B Plan Network benefits apply, using POMCO fee schedule. (Outside Option B Plan Network deductible and out of pocket expenses shall apply) If referred to POMCO provider but no services were available inside ELM, Inside Option B Plan Network benefits apply, using POMCO fee schedule. (Inside Option B Plan Network deductible and out of pocket where applicable) Letter approving referrals from Medical Director at Guthrie or Medical Director at STAP as applicable.
uses non contracted provider inside zip code
Inside Option A Plan Network benefits apply, using UCR. (Inside Option A Plan Network deductible and out of pocket where applicable)
Outside Option B Plan Network benefits apply, using UCR. (Outside Option B Plan Network deductible and out of pocket expenses shall apply)

113
Plan A Plan B
Enrollee lives inside zip code area:
uses non contracted provider outside zip code area with referral
Inside Option A Plan Network benefits apply, using UCR. (Inside Option A Plan Network deductible and out of pocket where applicable) Letter of Referral from Physician is necessary.
If referred to Non contracted provider but services were available inside ELM - Outside Option B Plan Network benefits apply, using UCR. (Outside Option B Plan Network deductible and out of pocket expenses shall apply) If referred to POMCO provider but no services were available inside ELM, Inside Option B Plan Network benefits apply, using UCR. (Inside Option B Plan Network deductible and out of pocket where applicable) Letter approving referrals from Medical Director at Guthrie or Medical Director at STAP as applicable.
uses non contracted provider outside zip code with no referral
Outside Option A Plan Network benefits apply, using UCR. (Outside Option A Plan Network deductible and out of pocket where applicable).
Outside Option B Plan Network benefits apply, using UCR. (Outside Option B Plan Network deductible and Out of Pocket expenses shall apply).
Enrollee lives outside zip code area:
uses ELM provider inside
zip code area
Inside Option A Plan Network benefits apply, using ELM fee schedule. (Inside Option A Plan Network deductible and out of pocket where applicable)
Inside Option B Plan Network benefits apply, using ELM fee schedule. (Inside Option B Plan Network deductible and out of pocket where applicable)
uses POMCO provider inside zip code
Inside Option A Plan Network benefits apply, using POMCO fee schedule. (Inside Option A Plan Network deductible and out of pocket where applicable)
Outside Option B Plan Network benefits apply, using POMCO fee schedule. (Outside Option B Plan Network deductible and out of pocket expenses shall apply)
uses POMCO provider outside zip code
Inside Option A Plan Network benefits apply, using POMCO fee schedule. (Inside Option A Plan Network deductible and out of pocket where applicable)
Inside Option B Plan Network benefits apply, using POMCO fee schedule. (Inside Option B Plan Network deductible and out of pocket where applicable)

114
Plan A Plan B
Enrollee lives outside zip code area
uses non contracted provider inside zip code
Inside Option A Plan Network benefits apply, using UCR. (Inside Option A Plan Network deductible and out of pocket where applicable)
Outside Option B Plan Network benefits apply, using UCR. (Outside Option B Plan Network deductible and out of pocket expenses shall apply)
uses non contracted provider outside zip code
Inside Option A Plan Network benefits apply, using UCR. (Inside Option A Plan Network deductible and out of pocket where applicable)
Inside Option B Plan Network benefits apply, using UCR. (Inside Option B Plan Network deductible and out of pocket where applicable)
Traveling outside zip code: Enrollee lives inside or outside zip code area
Inside Option A Plan Network benefits apply, using applicable fee schedule if POMCO/MP or UCR. Inside Option A Plan Network deductible and out of pocket where applicable).
Inside Option B Plan Network benefits apply, using applicable fee schedule if POMCO/MP or UCR. Inside Option B Plan Network deductible and out of pocket where applicable.
Plan C - Indemnity Plan
Enrollee lives inside zip code area:
uses ELM provider inside zip code
Benefits payable at ELM fee schedule - patient responsibility may be deductible and 20% up to the ELM fee schedule.
uses POMCO provider inside or outside zip code
Benefits payable at POMCO fee schedule - patient responsibility may be deductible and 20% up to the POMCO fee schedule.
uses non-contracted provider inside or outside zip code
Benefits payable up to 100% UCR, patient responsibility may be deductible and 20% which is held to OOP. The amount over UCR is also the patient’s responsibility.
Enrollee lives outside zip code area:
uses ELM provider inside zip code
Benefits payable at ELM fee schedule, patient responsibility may be deductible and 20% up to the ELM fee schedule.
uses POMCO provider inside or outside zip code
Benefits payable at POMCO fee schedule, patient responsibility may be deductible and 20% up to the POMCO fee schedule.
uses non contracted provider inside or outside zip code
Benefits payable up to 100% UCR, patient responsibility may be deductible and 20% which is held to OOP. The amount over UCR is also the patient’s responsibility.

115
APPENDIX C
PRIVACY ADDENDUM TO THE ELMIRA CITY SCHOOL DISTRICT SELF-INSURED HEALTH AND DENTAL PLAN (PLAN)
This Addendum is effective on April 14, 2003, and amends and is made part of the Elmira City School District Self-Insured Health and Dental Plan (PLAN).
The PLAN modifies the plan documents as required under the Administrative Simplification requirements of the Health Insurance Portability and Accountability Act of 1996 ("HIPAA"), to allow the disclosure of Protected Health Information ("PHI") as defined under HIPAA for the purposes specified below. If the terms or conditions of the plan documents conflict with this Addendum, this Addendum shall control.
1. Disclosure of PHI to Elmira City School District (PLAN SPONSOR). The PLAN shall disclose PHI to PLAN SPONSOR only to the extent necessary for the PLAN SPONSOR to perform the following plan administrative functions: (A) For enrollment/termination and eligibility; (B) To maintain accurate eligibility information regarding names, Social Security Numbers,
birth dates and employment dates; (C) To maintain current addresses and phone numbers; (D) To maintain information about dependents; (E) To maintain information about other insurance coverage; (F) To verify students status as dependents; (G) To provide information for COBRA notification; (H) To provide information for certificates of Credible Coverage; (I ) To respond to specific inquiries from a participant; (J) To individuals, such as family members, involved in a participants health care; (K) To allow benefit payment for medical services, prescription drugs and supplies; (L) For health care operations including medical case management, processing and
payments of a claim and/or appeal, for Coordination of Benefits with other insurers and responding to participant inquiries;
(M) To Business Associates to allow them to conduct their PLAN-related business on behalf of the PLAN;
(N) As required by law; (O) To individuals, such as family members, involved in a Participant’s Health Care 2. Use and Disclosure of PHI by PLAN SPONSOR. PLAN SPONSOR shall use and/or disclose PHI only to the extent necessary to perform the following Plan Administration functions, which it performs on behalf of the PLAN: (A) Establishing and determining eligibility; (B) Maintaining accurate eligibility information regarding names; Social Security numbers,
birth dates, and employment dates; (C) Maintaining current addresses and phone numbers; (D) Maintaining information about dependents; (E) Maintaining information about other insurance coverage; (F) Verifying student status of dependents (G) Providing information for COBRA notification

116
(H) Providing information for certificates of creditable coverage; And
(I) Responding to specific inquiries from a Participant. 3. PLAN SPONSOR Certification. The PLAN agrees that it will only disclose PHI to the PLAN SPONSOR upon receipt of a certification that this addendum has been adopted and the PLAN SPONSOR agrees to abide by such conditions. PLAN SPONSOR is subject to the following:
i. Prohibition on Unauthorized Use or Disclosure of PHI. The PLAN SPONSOR will not use or disclose any PHI received from the PLAN, except as permitted in these documents or required by law. ii. Subcontractors and Agents. The PLAN SPONSOR will require each of its subcontractors or agents to whom the PLAN SPONSOR may provide PHI to agree to written contractual provisions that impose at least the same obligations to protect PHI as are imposed on the PLAN SPONSOR. iii. Permitted Purposes. The PLAN SPONSOR will not use or disclose PHI for employment-related actions and decisions or in connection with any other of the PLAN SPONSOR’S benefits or employee benefit plans. iv. Reporting. The PLAN SPONSOR will report to the PLAN any impermissible or improper use or disclosure of PHI not authorized by the plan documents.
v. Access to PHI by Participants. The PLAN SPONSOR will make PHI available to the PLAN to permit participants to inspect and copy their PHI contained in the designated record set.
vi. Correction of PHI. The PLAN SPONSOR will make a participant's PHI available to
the PLAN to permit participants to amend or correct PHI contained in the designated record set that is inaccurate or incomplete and PLAN SPONSOR will incorporate amendments provided by the PLAN.
vii. Accounting of Disclosures of PHI. The PLAN SPONSOR will make a participant's
PHI available to permit the PLAN to provide an accounting of disclosures. viii. Disclosure to Government Agencies. The PLAN SPONSOR will make its internal
practices, books and records relating to the use and disclosure of PHI available to the PLAN and to DHHS or its designee for the purpose of determining the PLAN’S compliance with HIPAA.
ix. Return or Destruction of Health Information. When the PHI is no longer needed for
the purpose for which disclosure was made, the PLAN SPONSOR must, if feasible, return to the PLAN or destroy all PHI that the PLAN SPONSOR received from or on behalf of the PLAN. This includes all copies in any form, including any compilations derived from the PHI. If return or destruction is not feasible, the PLAN SPONSOR agrees to restrict and limit further uses and disclosures to the purposes that make the return or destruction infeasible.
x. Minimum Necessary Requests. The PLAN SPONSOR will use best efforts to
request only the minimum necessary type and amount of PHI to carry out the functions for which the information is requested.
4. Adequate Separation. The PLAN SPONSOR represents that adequate separation exists
117
between the PLAN and the PLAN SPONSOR so that PHI will be used only for plan administration. The following employees or persons under the control of the PLAN SPONSOR have access to participants' PHI for the purposes set forth under number 1 above: (A) Trustees – Elmira City School District Health Plan Committee Members (B) Consultants (C) Plan Administrator (D) Chief Payroll Clerk (E) Senior Account Clerk (Payroll Department) (F) Account Clerk Typist (Payroll Department) (G) Treasurer (Business Office) (H) Deputy Treasurer (Business Office) (I) Account Clerk (Business Office) (J) Assistant Superintendent For Management Services (K) Confidential Secretary II (Business Office) (L) School Attorney (M) Confidential Secretary I (School Attorney’s Office) (N) Clerk (Business Office) (O) (2) School Personnel Clerks (Personnel Office) (P) Records Management Officer (Q) Stores Clerk (Booth Storeroom)
5. Adequate Separation Certification. The PLAN requires the PLAN SPONSOR to certify that the employees identified above are the only employees that will access and use participants' PHI. The PLAN SPONSOR must further certify that the such employees will only access and use PHI for the purposes set forth under number 1 above.
6. Reports of Non-Compliance. Anyone who suspects an improper use or disclosure of PHI
may report the occurrence to the Plan's Privacy Official, the Insurance Coordinator, at Elmira City School District, 951 Hoffman Street, Elmira, New York 14905; telephone: (607) 735-3058; fax: (607) 735-3002.