measurement of pulmonary gas exchange in the icu. stephen rees center for model-based medical...
TRANSCRIPT

Measurement of pulmonary gas exchange in the ICU.
Stephen Rees
Center for Model-based Medical Decision Support, Department of Health Science and Technology, Aalborg University.
Disclosure: Board- member and minority share holder of Mermaid Care, who produce the ALPE system.

Our goal: To see if well know physiological models can be useful in clinical practice.
• Poor ventilator therapy increases mortality (ARDSNet. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. NEJM 2000; 342.)
• Standardization helps, if used.Young et al. Ventilation of patients with acute lung injury and acute respiratory distress syndrome: has new evidence changed current practice? Crit. Care Med 2004; 32: 1260-5.
Esteban et al. Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med 2008; 177:170-8.
• Automation can achieve standardization
• Current automated mechanical ventilator tools do not apply physiological models.

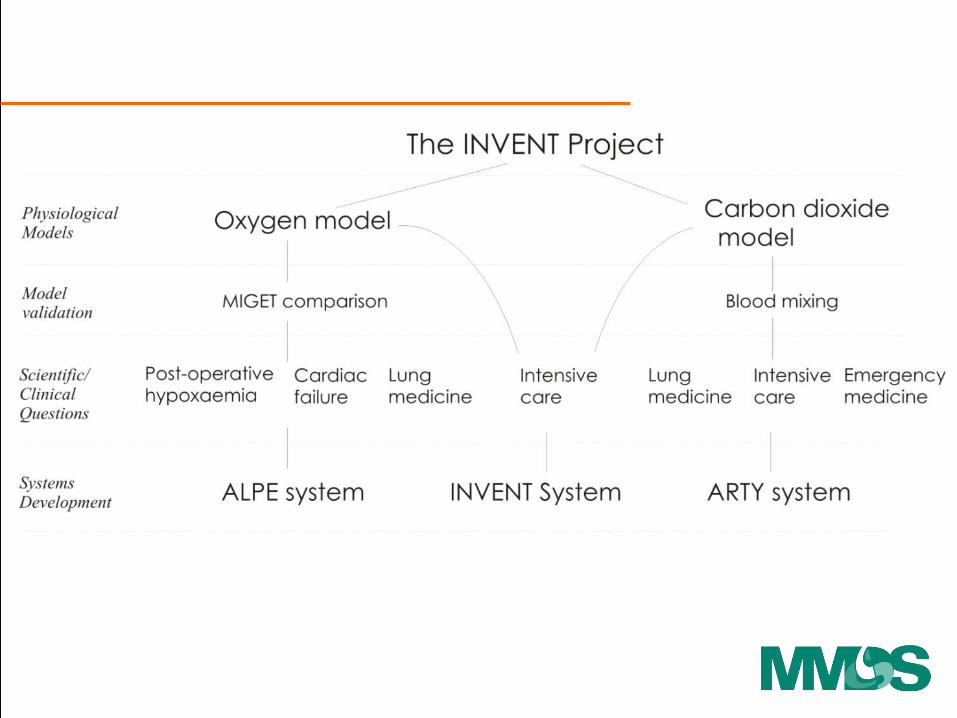
INVENT approach – physiological models

INVENT approach – physiological models
Find me the ventilator settings for this individual giving simulations which clinically preferred.

• How is pulmonary gas exchange measured today?
• How could pulmonary gas exchange be measured?
• How might these measurements be used in clinical practice?
Why was this path interesting to pursue?

• How is pulmonary gas exchange measured today?
• How could pulmonary gas exchange be measured?
• How might these measurements be used in clinical practice?

How is pulmonary gas exchange measured today?
The PaO2/FiO2 ratio
• Used in the definition of ALI, ARDS
• Sensitive to changes in FiO2
30% of the patients change disease classification.
• Poor quantification of gas exchange
D S Karbing et al. Variation in the PaO2/FiO2 ratio with FiO2: Mathematical and experimental description, and clinical relevance. Critical Care. 2007;11(6):R118.
Clinical

How is pulmonary gas exchange measured today?
The Multiple Inert Gas Elimination Technique (MIGET)
ExperimentalThe PaO2/FiO2 ratio
• Used in the definition of ALI, ARDS.
• Sensitive to changes in FiO2
30% of the patients change disease classification.
• Poor quantification of gas exchange.
D S Karbing et al. Variation in the PaO2/FiO2 ratio with FiO2: Mathematical and experimental description, and clinical relevance. Critical Care. 2007;11(6):R118.
Clinical
Wagner PD, Saltzman HA, West JB. Measurement of continuous distributions of ventilation-perfusion ratios: theory. J Appl Physiol. 1974 May;36(5):588-99
• The basis of our understanding of ventilation/perfusion distribution in the lungs.
• Complex – requiring tracer gases and gas chromatography.

Data analysed using a 50 compartment model.
To give ventilation and perfusion distributions.
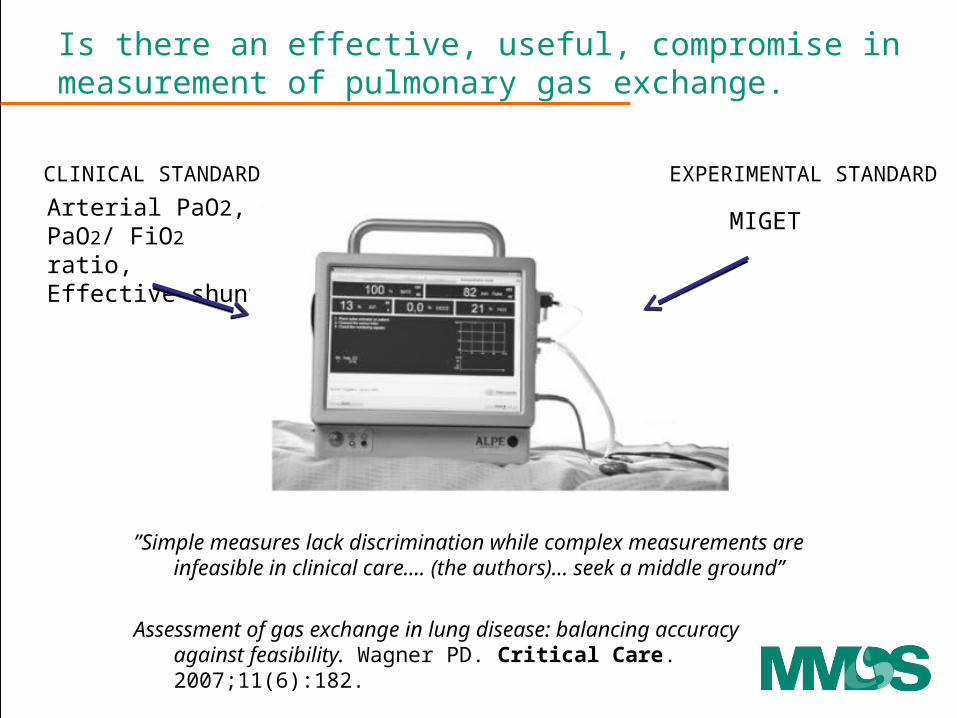
Is there an effective, useful, compromise in measurement of pulmonary gas exchange.
Arterial PaO2,PaO2/ FiO2 ratio,Effective shunt.
CLINICAL STANDARD
”Simple measures lack discrimination while complex measurements are infeasible in clinical care…. (the authors)… seek a middle ground”
Assessment of gas exchange in lung disease: balancing accuracy against feasibility. Wagner PD. Critical Care. 2007;11(6):182.
MIGET
EXPERIMENTAL STANDARD

• How is pulmonary gas exchange measured today?
• How can pulmonary gas exchange be measured using the ALPE technology?
• How might these measurements be used in clinical practice?
is

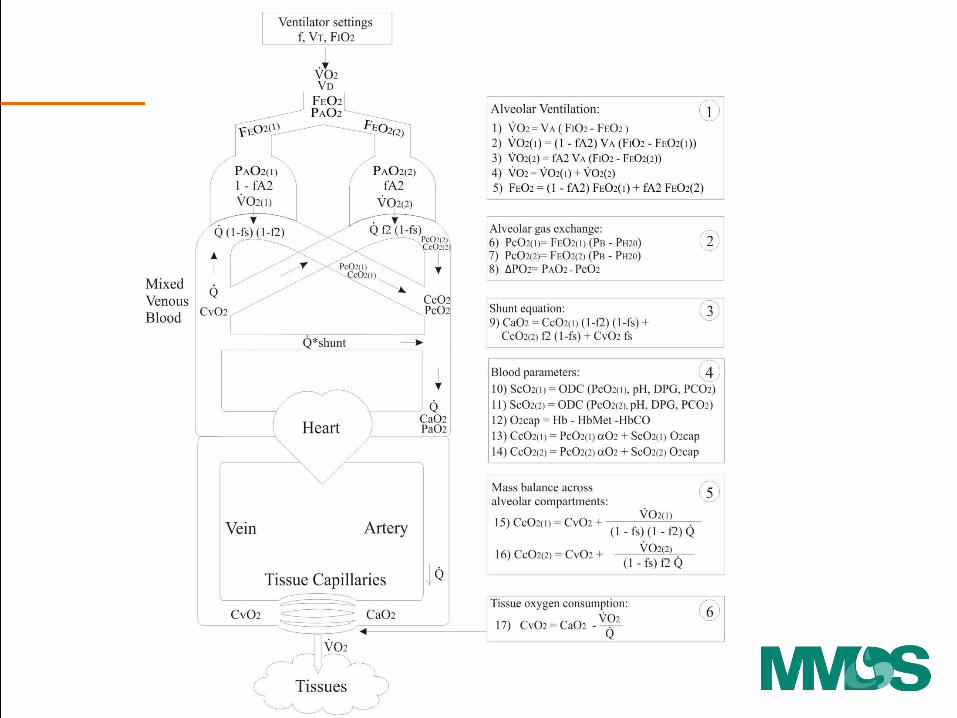
The principle and procedure
• Variation of FIO2 and measurement of ventilatory flow, gasses,SpO2 plus a single blood gas, can be used to calculate pulmonary shunt, low V/Q and high V/Q.
• Three to five step changes in FIO2, each to steady state.
• Model analysis and parameter estimation.


low V/Qhigh V/Q

low V/Qhigh V/Q
Welloxygenated
Poorlyoxygenated
Venous oxygenation

low V/Qhigh V/Q
Poorlyoxygenated
Oxygen responsive
Venous oxygenation
Not oxygen responsive
Welloxygenated

low V/Qhigh V/Q
Oxygen responsive
Not oxygen responsive
Oxygen loss = PAO2 - PcO2

low V/Qhigh V/Q
Oxygen responsive
Not oxygen responsive
Oxygen loss = PAO2 - PcO2

Clinical values of ‘shunt’ and ‘O2 loss’
aa
Kjærgaard S, Rees S, Malczynski J, Nielsen JA, Thorgaard P, Toft E, Andreassen S. Non-invasive estimation of shunt and ventilation-perfusion mismatch. Intensive Care Medicine 2003 May;29(5):727-34.
0 0.2 0.4 0.6 0.8 186
88
90
92
94
96
98
100
FEO2
SaO2(%)
Preoperative patient (x)Shunt = 1.0 %PO2 = 2.05 kPa
CABG patientDay 3 after surgery (*)Shunt = 12.0 %PO2 = 2.95 kPa
ICU patient (ARDS) (+)Shunt = 21.0 %PO2 = 16.87 kPa
Pre-op patient (x) Shunt = 1% O2 loss = 2 %
Post- op CABG patient (*) Shunt = 12% O2 loss = 3%
ICU patient (ARDS) (+) Shunt = 21% O2 loss = 17%

What does this mean clinically?
aa
Kjærgaard S, Rees S, Malczynski J, Nielsen JA, Thorgaard P, Toft E, Andreassen S. Non-invasive estimation of shunt and ventilation-perfusion mismatch. Intensive Care Medicine 2003 May;29(5):727-34.
0 0.2 0.4 0.6 0.8 186
88
90
92
94
96
98
100
FEO2
SaO2(%)
Preoperative patient (x)Shunt = 1.0 %PO2 = 2.05 kPa
CABG patientDay 3 after surgery (*)Shunt = 12.0 %PO2 = 2.95 kPa
ICU patient (ARDS) (+)Shunt = 21.0 %PO2 = 16.87 kPa
Shunt
O2 loss(Low V/Q)
Pre-op patient (x) Shunt = 1% O2 loss = 2 %
Post- op CABG patient (*) Shunt = 12% O2 loss = 3%
ICU patient (ARDS) (+) Shunt = 21% O2 loss = 17 %
Clinical values of ‘shunt’ and ‘O2 loss’

What does this mean clinically?
aa
Kjærgaard S, Rees S, Malczynski J, Nielsen JA, Thorgaard P, Toft E, Andreassen S. Non-invasive estimation of shunt and ventilation-perfusion mismatch. Intensive Care Medicine 2003 May;29(5):727-34.
0 0.2 0.4 0.6 0.8 186
88
90
92
94
96
98
100
FEO2
SaO2(%)
Preoperative patient (x)Shunt = 1.0 %PO2 = 2.05 kPa
CABG patientDay 3 after surgery (*)Shunt = 12.0 %PO2 = 2.95 kPa
ICU patient (ARDS) (+)Shunt = 21.0 %PO2 = 16.87 kPa
Shunt
O2 loss(Low V/Q)
Pre-op patient (x) Shunt = 1% O2 loss = 2 %
Post- op CABG patient (*) Shunt = 12% O2 loss = 3%
ICU patient (ARDS) (+) Shunt = 21% O2 loss = 17 %
Clinical values of ‘shunt’ and ‘O2 loss’

• Classifying and monitoring ICU patients
• D S Karbing, et al. Variation in the PaO2/FiO2 ratio with FiO2: Mathematical and experimental description, and clinical relevance. Critical Care. 2007;11(6):R118.
• S Kjærgaard, et al. Non-invasive estimation of shunt and ventilation-perfusion mismatch. Intensive Care Medicine 2003 May;29(5):727-34.
• Assessment of respiratory function, before during and after surgical intervention
• Kjærgaard S et al. Modelling of hypoxaemia after gynaecological laparotomy. Acta Anaesthesiol.Scand. 2001 Mar;45(3):349-356
• Kjærgaard S et al. Hypoxaemia after cardiac surgery: Clinical application of a model of pulmonary gas exchange. EJA. 2004 Apr;21(4):296-301.
• Rasmussen BS et al. Oxygenation within the first 120 h following coronary artery bypass grafting. Influence of systemic hypothermia (32 degrees C) or normothermia (36 degrees C) during the cardiopulmonary bypass: a randomized clinical trial. Acta Anaesthesiol. Scand. 2006 Jan;50(1):64-71.
• Rasmussen BS et al. Oxygenation and release of inflammatory mediators after off-pump compared to after on-pump coronary artery bypass surgery. Acta Anaesthesiol. Scand. 2007, 51(9):1202-10.
• Standardising and optimising ventilator therapy• Karbing DS, et al. Retrospective evaluation of a decision support system for control of mechanical ventilation.
Med Biol Eng Comput. 2011 Nov 22. [Epub ahead of print]• Karbing DS, et al. Prospective evaluation of a decision support system for setting inspired oxygen in intensive
care patients. J. Crit Care, 2010, 25(3):367-74.• C Allerød, et al. A Decision Support System for suggesting ventilator settings: Retrospective evaluation in
cardiac surgery patients ventilated in the ICU. Comput. Meth Prog. Biomed 2008, vol. 92, nr. 2, s. 205-212
References

• The ALPE model adequately describes MIGET data in a physiological situation analogous to acute lung injury, and gives similar parameter values to the MIGET model
• The ALPE model gives accurate predictions of PaO2 across a range of PEEP, Inspiratory : Expiratory (IE) ratio, and FIO2 settings compatible with clinical treatment of acute lung injury
We did not show, or try to show that
• The ALPE adequately describes injury similar to mature ARDS or other more complex situations.
• FiO2 v SaO2 curves give V/Q distributions similar to MIGET.
Comparison to MIGET – We showed
Rees S.E, et al., J Appl Physiol. 101(3),826-32, (2006).
Rees SE. Intensive Care Med. 36(12),2117-24. (2010).

• How is pulmonary gas exchange measured today?
• How can pulmonary gas exchange be measured using the ALPE technology?
• How might these measurements be used in clinical practice?

How might these measurements be used in clinical practice?
• Appropriate setting of FIO2
• Monitoring the effects of PEEP
How might these measurements improve clinical practice?
• Appropriate setting of FIO2
– How might one use these parameters “shunt” and “Oxygen loss” to set FIO2.
• Monitoring the effects of PEEP

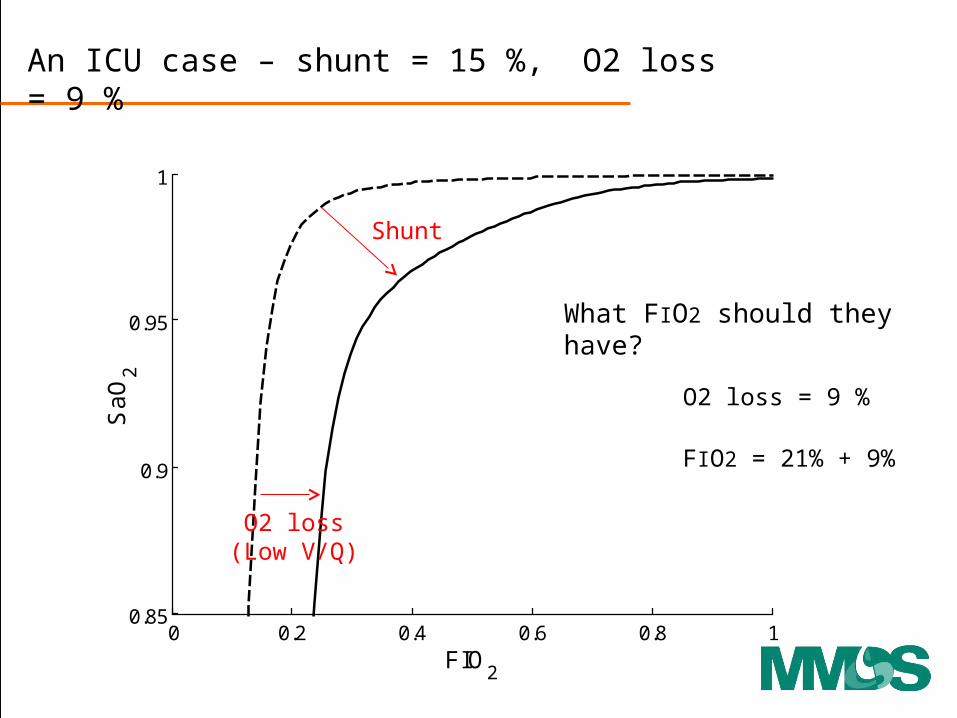
An ICU case – shunt = 15 %, O2 loss = 9 %
0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2

0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2
An ICU case – shunt = 15 %, O2 loss = 9 %
O2 loss(Low V/Q)
Shunt
0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2
An ICU case – shunt = 15 %, O2 loss = 9 %
What FIO2 should they have?
O2 loss = 9 %
FIO2 = 21% + 9%
O2 loss(Low V/Q)
Shunt

A normal person – shunt = 15 %, O2 loss = 9 %
FIO2 = 21+9 = 30 % ≈ 30 kPa ≈ 225 mmHg
FEO2 = 14+9 = 23 % ≈ 23 kPa ≈ 173 mmHg
PcO2 ≈ 23-9 =14 kPa ≈ 105 mmHg ScO2 ≈ 98 %
SaO2 ≈ 94% PaO2 ≈ 9.5 kPa ≈ 71 mmHg
O2 loss = 9 % ≈ 9 kPa ≈ 67 mmHg
shunt = 15 % SvO2 ≈ 70%

0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2
An ICU case – shunt = 15 %, O2 loss = 9 %
FIO2 = 30 %SaO2 = 94 %
Normal oxygenation of that which is “oxygen responsive”

ALPE control of FiO2
Baseline Clinician System
Karbing DS, Allerød C, Thorgaard P, Carius AM, Frilev L, Andreassen S, Kjærgaard S, Rees SE. Prospective evaluation of a decision support system for setting inspired oxygen in intensive care patients. Journal of Critical Care, 2010, 25(3):367-74.
How might these measurements improve clinical practice?
• Appropriate setting of FIO2
• Monitoring the effects of PEEP

Physiological rational for PEEP monitoring with gas exchange
• Most PEEP monitoring techniques based upon mechanical rather than functional measurements.
• Opening may not be the same a improving functionality, and the functionality is the gas exchange.
• We know from MIGET that changing PEEP modifies the V/Q distribution in the lung.
Dantzker DR, et al. Ventilation-Perfusion distributions in the Adult Respiratory Distress Syndrome. Am Rev Resp Dis. 1979, 120:1039-52.

0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2
• Support ventilation, 6 days in the ICU.
• FIO2 = 60 %, PEEP 6 cm H2O.
• Shunt = 10 %, O2 loss = 11%
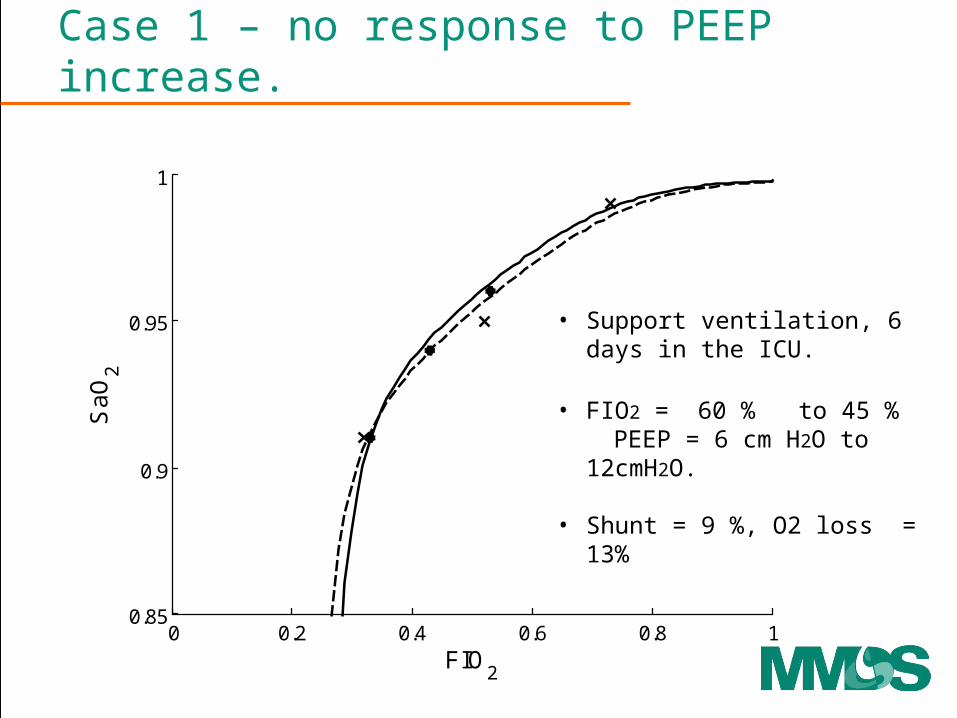
Case 1 – no response to PEEP increase.
0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2
Case 1 – no response to PEEP increase.
• Support ventilation, 6 days in the ICU.
• FIO2 = 60 % to 45 % PEEP = 6 cm H2O to 12cmH2O.
• Shunt = 9 %, O2 loss = 13%

0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2
FIO2 40 %, PEEP 5 cm H2OShunt 20%, O2 loss 2%
FIO2 40 %, PEEP 15 cm H2OShunt 10 %, O2 loss 5 %
Case 2 – response to PEEP increase.
Controlled ventilation, 1 day in the ICU.

0 0.2 0.4 0.6 0.8 10.85
0.9
0.95
1
FIO2
Sa
O2
Case 2 – response to PEEP increase.
FIO2 40 %, PEEP 5 cm H2OShunt 20%, O2 loss 2%
FIO2 40 %, PEEP 15 cm H2OShunt 10 %, O2 loss 5 %
PEEP = 10 cm H2O

Conclusions• We are trying to find a balance, bringing well known
physiology into clinical tools.
• Goals– Provide a physiological description of gas exchange– Help find appropriate FIO2
– Help monitor the functional effects of PEEP

Future and thoughts
• Comparison with CT scans in ARDS
• Comparison with HRCT in COPD patients
• Tidying up assumptions– HPV, steady state conditions, etc.
• A thought, oxygen is also used as a tracer to estimate EELV. These could be combined.