medical imaging of the heart and cardiovascular system · · 2013-02-15medical imaging of the...
TRANSCRIPT

CHAPTER 14
Medical Imaging of the Heart andCardiovascular System
Zhonghua Sun1, Kwan-Hoong Ng2, Patrick C. Brennan3
1Discipline of Medical Imaging, Department of Imaging and Applied Physics,Curtin University, Perth 6845, Australia2Department of Biomedical Imaging, University of Malaya,Kuala Lumpur 50603, Malaysia3Department of Medical Imaging and Radiation Sciences, University of Sydney,Sydney 2141, Australia
CONTENTS
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 214
2. Imaging Principles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 214
3. Invasive Imaging Modalities . . . . . . . . . . . . . . . . . . . . . . . . 215
3.1. Invasive Cardiac Angiography . . . . . . . . . . . . . . . . . 215
3.2. Intravascular Ultrasound . . . . . . . . . . . . . . . . . . . . . . 215
4. Less Invasive Imaging Modalities . . . . . . . . . . . . . . . . . . . . 217
4.1. Chest Radiography . . . . . . . . . . . . . . . . . . . . . . . . . . 217
4.2. Electron Beam Computed Tomography . . . . . . . . . . . 217
4.3. Computed Tomography . . . . . . . . . . . . . . . . . . . . . . 219
4.4. Magnetic Resonance Imaging . . . . . . . . . . . . . . . . . . 222
4.5. Doppler Ultrasonography . . . . . . . . . . . . . . . . . . . . . 224
4.6. Echocardiography . . . . . . . . . . . . . . . . . . . . . . . . . . . 226
5. Nuclear Medicine Imaging Modalities . . . . . . . . . . . . . . . . . 226
5.1. Single Photon Emission Computed Tomography . . . . 227
5.2. Positron Emission Tomography . . . . . . . . . . . . . . . . . 228
5.3. Hybrid Imaging Modalities . . . . . . . . . . . . . . . . . . . . 229
6. Ionizing Radiation Examinations-Radiation Dose Issue . . . . 230
6.1. Radiation Doses Relevant to Cardiac Angiographyand Associated Interventional Procedures . . . . . . . . . 231
ISBN: x-xxxxx-xxx-xCopyright © 2011 by American Scientific PublishersAll rights of reproduction in any form reserved.
213
Distributed Diagnosis and Home HealthcareEdited by E. Y. K. Ng, U. Rajendra Acharya,
and Toshiyo TamuraVolume 3: Pages 213–239

214 Medical Imaging of the Heart and Cardiovascular System
6.2. Chest Radiography . . . . . . . . . . . . . . . . . . . . . . . . . . 2326.3. Computed Tomography . . . . . . . . . . . . . . . . . . . . . . 2326.4. Nuclear Medicine Imaging . . . . . . . . . . . . . . . . . . . . 233
7. Summary and Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . 234References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 234
1. INTRODUCTION
Numerous diagnostic imaging studies are performed to visualize the vasculature of theheart and cardiovascular system that transports blood to and from the heart. The circu-latory system is responsible for moving the blood throughout the body so as to carryoxygen and nutrients to the various tissues in the peripheral body and remove any wasteproducts for elimination. As in any closed system, problems can occur that compromisethe normal function of the circulatory system supplying the heart and cardiovascular sys-tem. Common situations that cause malfunction of the system are reduced or increasedblood flow, and directional anomalies that can cause flow in the wrong direction betweendifferent cardiac chambers. The purpose of diagnostic and interventional imaging proce-dures is to identify and manage these problems.
In most industrialized countries cardiovascular disease is still the leading cause of mor-bidity and mortality [1]. The most threatening manifestations of cardiovascular diseaseare carotid artery stenosis, coronary artery disease, renal artery stenosis, peripheral arterystenosis, or occlusion with potentially fatal consequences of stroke, myocardial infarction,hypertension or limb loss, respectively [2–4]. Since cardiovascular disease is not only life-threatening but also presents a major economic burden to the health care system, earlydetection and a comprehensive assessment of detected atherosclerotic changes or diseasescreening are very important to improve treatment outcome and patient management.Medical imaging plays an important role in the early detection and diagnosis of cardio-vascular disease. Imaging of the heart and cardiovascular system has undergone rapiddevelopments over the last decade due to advancement in medical imaging techniques,such as multislice computed tomography (MSCT), magnetic resonance imaging (MRI),and nuclear medicine imaging, especially hybrid functional and anatomic imaging tech-niques, such as positron emission tomography and computed tomography (PET/CT). Thefollowing sections in this chapter will discuss imaging principles, followed by a descrip-tion of each imaging modality used in cardiac imaging with reference to the advantagesand disadvantages.
2. IMAGING PRINCIPLES
Imaging of the heart and cardiovascular system is different from that of other parts ofthe body, since the heart is a fast-moving organ and peripheral vessel branches are smallin diameter. This puts a strong demand on the technical aspects of imaging modalities.In order to acquire high-resolution artifact-free images of the heart and cardiovascularsystem, two technical aspects are essential to accomplish this goal, namely, high temporaland spatial resolution. This translates into fast image acquisition times and multipledata acquisition at submillimeter slice thickness. High temporal resolution is particularlyimportant for heart imaging as it relates to the speed of data acquisition, which is neededto image the beating heart without motion artifacts. Multiple data acquisition with highspatial resolution refers to the need to cover the heart and cardiovascular system in itsentirety within a single breath-hold. This is necessary to visualize and demonstrate thetiny artery branches such as the coronary artery and its branches, since the coronaryartery tree has a small diameter of 1.5–3 mm.
Traditionally, imaging of the heart and cardiovascular system is performed with inva-sive catheter-based angiography, which is still regarded as the gold standard technique.However, it is not only an invasive procedure, but also associated with procedure-relatedcomplications [5]. Less invasive modalities have developed rapidly, such as MSCT and

Medical Imaging of the Heart and Cardiovascular System 215
MRI, achieving improved diagnostic value in cardiovascular imaging when compared toinvasive angiography [6–8]. Furthermore, physiological evaluation modalities includingsingle photon emission computed tomography (SPECT) and PET, have also been increas-ingly used in cardiac imaging due to their unique ability to provide functional assessmentof the heart and cardiovascular disease [9, 10].
3. INVASIVE IMAGING MODALITIES
Invasive imaging modalities include catheter-based invasive angiography, which isregarded as the gold standard method, and intravascular ultrasound, which is useful forassessing both normal appearance and abnormal changes of blood vessels in the pres-ence of pathologies, such as plaque formation in the artery wall. Despite invasivenessand presence of procedure-related complications, these modalities still continue to playan important role in the diagnosis and assessment of cardiovascular disease.
3.1. Invasive Cardiac Angiography
Invasive angiography is a radiographic technique used to diagnose vascular disease ofthe main artery, aorta, and its distal branches such as those supplying the lower extrem-ities. It is performed by introducing the catheter into the aorta via vascular access. Themost common vascular access for catheter insertion to perform all angiography pro-cedures is the percutaneous route. The transfemoral artery approach is the most com-mon one for aortography, which is normally performed to image the aorta and itsartery branches. Transaxial puncture is alternatively selected when pathology, such asatherosclerosis or aortofemoral grafts, make the transfemoral approach undesirable. If theaim of the procedure is to assess the right heart or pulmonary circulation, the trans-femoral venous route is desirable.
Selective studies, such as left and right heart catheterisation and coronary angiography,can be performed following aortography depending on patient history, clinical diagnosis,and electrocardiography anomalies. One of the most common selective procedures iscoronary angiography. It is performed to image the coronary, its branches, and collateralcirculations for diagnosis of coronary artery disease, as well as treatment planning.
Cardiac angiography is the method of choice for cardiac imaging owing to its highspatial and temporal resolution, which is still unsurpassed by other imaging modalities.It is performed on patients with coronary artery disease, conduction disturbances, orcongenital heart disease and provides excellent information regarding heart and vesselanatomy (Fig. 1). Cardiac angiography also allows for intracardiac and arterial pressuremeasurements as the catheter passes through the various areas of the heart. This helpsthe cardiologist make an accurate diagnosis of the pathology in order to determine thecardiac function and proper intervention procedures.
Cardiac angiography is also increasingly used to perform therapeutic angiographythrough expanded use of interventional procedures. Percutaneous transluminal coronaryangioplasty (PTCA) is a therapeutic procedure commonly performed to dilate stenosedor occluded coronary arteries with a balloon catheter, followed by placement of stents inthe vessel with the aim of maintaining the patency of narrowed vessels. Thrombolysisis a procedure in which an anticoagulant drug is administered onto a clot to dissolve it.With embolization, devices, such as coils, are used to clot off vessels, for instance, vesselsfeeding tumors (to shrink the tumor and reduce peri-operative bleeding), arteriovenousmalformations, occlude fistulae, or other abnormalities to prevent excessive bleedingduring open surgery.
3.2. Intravascular Ultrasound
Invasive cardiac angiography, as the gold standard technique for evaluating cardiovas-cular disease, provides excellent information on lumen size and pathological changessuch as degree of vessel stenosis; however, it is limited to assessment of vascular remod-elling and is not used for the evaluation of wall thickness or plaque composition. Instead,

216 Medical Imaging of the Heart and Cardiovascular System
Figure 1. Cardiac angiography. Invasive coronary angiography shows the normal right coronary artery (A)and left coronary artery (B) with excellent resolution. (Image courtesy of University of Malaya Medical Centre,Kuala Lumpur, Malaysia.)
intravascular ultrasound (IVUS) is considered a more accurate method for visualizingthe artery wall, especially the coronary artery and intraluminal plaque composition andvolume [11].
IVUS is performed as part of the invasive diagnostic procedure. Following cardiacangiography, the IVUS catheter is introduced after the patient has been given an intravas-cular administration of nitroglycerin. The ultrasound catheter tip position is determinedby fluoroscopy angiography through infusion of contrast medium, and the catheter ispositioned distal to the lesion of interest. During pullback, gray scale IVUS data is storeddigitally and assessed offline by the IVUS software system [12].
IVUS is a recently developed imaging technique that generates high-quality tomo-graphic images of cardiovascular disease, such as coronary atheroma [13]. Using a motor-ized pullback apparatus, a series of cross-sectional measurements can be obtained andsummated to determine plaque composition, plaque volume, or atheroma burden. Sev-eral characteristics inherent to IVUS imaging offer potential advantages in the evaluationof cardiovascular disease. This tomographic orientation allows for visualization of thefull circumference of the vessel wall, examination of arterial remodelling, and assessmentof the thickness and echogenicity of atherosclerotic plaques [14, 15]. Gray scale IVUS is auseful modality for characterizing the extent and distribution of atherosclerotic plaquesin vivo, as well as for determining the morphology of atherosclerotic plaques and thevessel wall [16, 17] (Fig. 2). It has been reported that there was a significantly higher fre-quency and greater degree of positive remodelling, as well as a larger amount of necroticcore, non-calcified plaques in acute coronary syndrome as visualized on IVUS [18, 19].However, the region of low echogenicity, which is believed to represent the compositionof lipid-containing and mixed plaque, remains relatively uncharacterized by gray scaleIVUS [17]. This limitation is overcome by the recent development of a novel techniquecalled virtual histology (VH) IVUS.
VH IVUS is an advanced radio-frequency analysis of intravascular ultrasound sig-nals which provides an in vivo opportunity to assess plaque morphology [20, 21]. VHIVUS has been shown to demonstrate 80% to 92% in vitro accuracy for identification ofdifferent types of atherosclerotic plaques [20]. Nasu et al. concluded that correlation ofin vivo IVUS radio-frequency data analysis with histopathology shows a high accuracyfor the classification of different types of coronary components [21]. VH IVUS may allowbetter detection of features associated with future plaque rupture, thus improving ourunderstanding of the atherosclerotic disease behavior and progression according to thebaseline plaque composition [22].

Medical Imaging of the Heart and Cardiovascular System 217
Figure 2. Cardiac intravascular ultrasound (IVUS). IVUS shows the visualization of the right coronary ostiumintraluminally. (Image courtesy of Dr. Gim-Hooi Cho, Consultant Cardiologist, Selangor Medical Centre,Malaysia.)
4. LESS INVASIVE IMAGING MODALITIES
A number of techniques ranging from chest radiography to CT, MRI, Doppler ultrasonog-raphy and nuclear medicine techniques, belong to the category of less invasive modalitieswhen compared to the above-mentioned invasive techniques. Some of these procedures,such as radiography and CT, can be done within a very short time, while others, suchas cardiac MRI and cardiac perfusion study, may be time-consuming. Because of thereduced invasiveness and increased diagnostic value in cardiovascular disease due totechnological developments, these less-invasive imaging modalities are increasingly usedin the assessment of cardiovascular disease with some of them being used as a reliablealternative to invasive examinations.
4.1. Chest Radiography
Conventional chest radiography continues to play a very important role in the diagnosisand management of cardiovascular disease. Chest radiographs provide information aboutheart shape and size, which may be affected by many factors (Fig. 3). Estimation of theheart chamber size is difficult due to the overlapping of the atria and ventricles. However,chest radiography is excellent in demonstrating the great vessels and vascular changeswithin the lung fields, which offer critical information regarding cardiac functions (Fig. 4).
The image quality of chest radiographs is affected by many factors such as patientposture, degree of inspiration, correct positioning, geometric factors, and exposure tech-nique selection. These factors can be controlled by the medical imaging technologists.Factors that are not under the technologist’s control but can affect cardiac shape andsize include patient body habits, bony thorax abnormalities, and pathological conditionssuch as pneumothorax or pulmonary emphysema. These factors should be taken intoconsideration when selecting appropriate imaging parameters so as to ensure optimumacquisition of chest radiographs.
Despite its limited diagnostic value in cardiac imaging, chest radiography is the mostcommonly performed procedure, and the importance of these basic radiographic princi-ples to ensure the accuracy of diagnostic chest radiographs should not be underestimatedby medical imaging technologists.
4.2. Electron Beam Computed Tomography
Electron beam computed tomography (EBCT) was developed in the early 1980s. It isregarded as an ultrafast or high-speed CT scanner as it made CT imaging of heart andcoronary arteries feasible. EBCT differs from conventional CT systems with the immov-able X-ray source that enables fast data acquisition in a very short time. High temporal

218 Medical Imaging of the Heart and Cardiovascular System
Figure 3. Chest radiography. Chest radiograph shows normal appearance of the heart and aorta. (Image cour-tesy of Dr Evelyn LM Ho, Consultant Radiologist, Imaging Department, Sime Darby Specialist Centre MegahSdn. Bhd., Petaling Jaya, Malaysia.)
resolution (50–100 milliseconds) makes this technique well-suited for imaging the heartand coronary tree, with the capability of evaluating tiny abnormalities such as coronarycalcium and plaques, even in the presence of the motion of a rapidly beating heart. Themain clinical application of EBCT is in the detection and evaluation of calcification inthe coronary arteries (calcium scoring), which is considered a risk indicator of coronaryartery disease [23, 24]. It has significant value in determining calcium scores, which areassociated with the degree and severity of coronary artery disease and thus assists inpredicting the probability of future cardiac events [25].
The main limitation of EBCT is its inferior spatial resolution, which is between1.5–3.0 mm. This restricts its diagnostic value to accurately evaluate the severity of coro-nary artery disease. After the arrival of MSCT scanners in the late 1990s, the use of EBCTbecame scarce and was eventually replaced by MSCT from 2003 onwards.
Figure 4. Chest radiography. Chest radiograph shows abnormal heart appearance in a patient diagnosed withhypertension with left ventricle enlargement. (Image courtesy of Associate Professor Yang Faridah Abdul Aziz,University of Malaya Medical Centre, Kuala Lumpur, Malaysia.)

Medical Imaging of the Heart and Cardiovascular System 219
4.3. Computed Tomography
The first clinical CT scanner was developed by Godfrey Hounsfield from the UnitedKingdom in 1973. It was immediately recognized as a very useful diagnostic imagingtechnique as it allows visualization of the cross-sectional views of the body structures.In the early 1990s, the introduction of helical or spiral CT scanners was considered amajor breakthrough for CT technology. With spiral CT, the patient table is continuouslymoving and translated through the gantry while scan data are acquired simultaneously.Spiral CT scanning does not have misregistration problems or loss of anatomic detailssince the scan is performed in a single breath-hold, thus enabling acquisition of volumedata. Images could be reconstructed at any position along the patient longitudinal axis,and overlapping image reconstruction could be generated (normally 50% overlap) toimprove longitudinal resolution. Acquisition of volume data has become the very basisfor applications such as CT angiography [26] (Fig. 5).
The introduction of MSCT is considered a major evolutionary leap in CT technology.By late 1998, all major CT manufacturers launched MSCT scanners capable of at leastfour slices per X-ray tube rotation. The total number of detector elements depends onthe number of detector elements in the X-ray plane (700–900) times the number of rowsof detectors (2 to 4, 8, 16, 64, or more rows), yielding the total detector elements in therange of 1,400–60,000 [27]. The MSCT scanner, with its cone-shaped beam and multipleslices per rotation, allows for acquisition of multiple slices during one gantry rotation.This difference along with the reduced gantry rotation time in the MSCT scanners, leadsto a shorter scanning time and greater coverage of scanning volume per gantry rotationand provides superior image quality [28].
The advantages of MSCT technology include: (1) the ability to obtain a large number ofthin slices resulting in greater spatial resolution in both axial and longitudinal directions.For example, isotropic volume data (cubic voxels) can be acquired with 64- or more sliceCT, resulting in improved resolution of the volume data (images are equally sharp in
Figure 5. Abdominal multislice CT angiography. Multislice CT angiography shows an infrarenal aorticaneurysm (long arrows) with excellent demonstration of aortic branches from the abdominal aorta to externaliliac arteries (short arrows).

220 Medical Imaging of the Heart and Cardiovascular System
Figure 6. 64-slice CT coronary angiography. Multislice CT angiography with curved planar reformation clearlyshows the normal right coronary artery.
any plane) (Fig. 6). This capability is obtained with multiple sections of submillimeterthickness. The speed can be used for fast imaging of a large volume of tissue with variableslice thickness. This is particularly useful in cardiac imaging studies and other studieswhere patient motion is a limiting factor such as in trauma or paediatric patients. With4-slice CT and a gantry rotation of 0.5 s, the volume data can be acquired eight timesfaster than with the single slice, 1-s scanner. With 16- and 64-slice CT and rotation timesof less than 0.5 s, the volume data are acquired at an even greater rate than that of earlygeneration MSCT scanners (Fig. 7). With 256- and 320-slice CT, the entire heart can becovered in a single gantry rotation with a slice thickness of 0.5 mm or less [29, 30] (Fig. 8).
The most common application of MSCT is to detect hemodynamically significant coro-nary stenosis with high sensitivity and specificity (Fig. 9). The quality of MSCT coronaryangiography improved significantly with the introduction of 16- and 64-slice CT systemsand satisfactory results have been achieved [31–33]. Several meta-analyses of 64-slice CT
Figure 7. Dual-source CT coronary angiography. 3D volume clearly shows the heart and left coronary arterybranches.

Medical Imaging of the Heart and Cardiovascular System 221
Figure 8. 320-slice CT coronary angiography. 3D volume rendering demonstrates the heart and coronary arterybranches with data acquired in a single heart beat. Main coronary arteries and their side branches are clearlyvisualized.
studies have reported moderate to high sensitivities and specificities with respect to coro-nary artery disease (CAD), and an extremely high negative predictive value (96–100%)[32–36]. Further technical developments, such as 256- and 320-slice CT scanners, allowlonger z-axis coverage, ranging from 12.8–16 cm in one gantry rotation, which permitsrapid scanning of the entire heart [29, 30].
MSCT has also been confirmed to be valuable in the diagnosis of many other car-diovascular diseases, and in some areas it has replaced invasive angiography due to itshigh diagnostic value. MSCT angiography has been reported to be superior to invasiveangiography in the assessment of abdominal aortic aneurysm pre-and post-endovascularaneurysm repair [37, 38]. MSCT angiography has been shown to be more sensitive thaninvasive angiography, and it is the preferred method for diagnosis of aortic dissectionwith a sensitivity and specificity of nearly 100% [39, 40] (Fig. 10). As a reliable alterna-tive to conventional pulmonary angiography, MSCT angiography has been recognizedas the first line technique for detection and diagnosis of pulmonary embolism (Fig. 11).With the rapid developments of CT techniques, MSCT pulmonary angiography wasinitially used as an adjunct and an alternative to other imaging modalities. Recently, it hasbecome widely recognized as the method of choice for diagnosis of suspected pulmonary
Figure 9. Dual-source CT coronary angiography. Curved planar reformatted CT angiography shows significantcoronary stenosis (arrows) caused by mixed plaques at the right coronary artery in a patient suspected ofcoronary artery disease. Reprinted with permission from [31], Z. Sun and K. H. Ng, Singapore Med. J. 51, 282(2010). © 2010, Singapore Medical Association.

222 Medical Imaging of the Heart and Cardiovascular System
Figure 10. Thoracic CT angiography. CT angiography shows Stanford type A dissection with the dissectionoriginating at the aortic root. The intimal flap is clearly displayed on 2D axial and coronal reformatted images(long arrows in 10A and 10B) with left coronary artery arising from the true lumen (arrowhead). IF indicatesintimal flap. T and F refer to true lumen and false lumen, respectively.
embolism due to its superior sensitivity and specificity to ventilation-perfusion radioiso-tope scanning [41–43]. MSCT angiography has demonstrated a high diagnostic value(more than 90% sensitivity and specificity) in the diagnosis of peripheral arterial diseasewhen compared to invasive peripheral angiography [44]. Moreover, 64-slice CT angiogra-phy has been reported to have high sensitivity and specificity for the detection of signifi-cant in-stent or persistent restenosis in patients with peripheral artery stent implantation,and therefore is considered as a valuable non-invasive technique for stent evaluation andsurveillance [45].
4.4. Magnetic Resonance Imaging
MRI provides excellent soft tissue contrast with inherent 3D capabilities and allows acqui-sition in any anatomical plane. Diagnosis of cardiac disease requires accurate assessmentof both morphology and function of the heart and cardiovascular system. MRI is widelyused to image patients with renal dysfunction or impairment which prevents them fromundergoing contrast-enhanced CT scans. Cardiac MRI has recently gained popularity asa clinical diagnostic modality to evaluate many cardiac and great vessel abnormalities.It may be used to evaluate several important diagnostic features including cardiac mor-phology, regional and global ventricular function, myocardial fusion, and coronary arteryflow and anatomy. Since the heart displays complex motion due to both cardiac contrac-tion and respiration, the MRI pulse sequences should provide breath-hold or adequaterespiratory-triggered acquisition as well as electrocardiography (ECG) gating acquisition.Contrast-enhanced MRI can demonstrate myocardial perfusion and blood flow velocitieswithin the heart and cardiovascular system.
MRI has been widely applied in the diagnosis of various cardiovascular diseases withhigh diagnostic accuracy being achieved. There are several different imaging techniques

Medical Imaging of the Heart and Cardiovascular System 223
Figure 11. Pulmonary CT angiography. Pulmonary embolism is shown at the bilateral pulmonary arterybranches. A large thrombus is present in the left main pulmonary artery and it extends to the right side (topleft image). Orthogonal views show that the viewing position is located in the pulmonary trunk (bottom rowimages). The intraluminal thrombus was demonstrated on virtual endoscopy image (arrows on the right topimage).
for MR angiography, and the most suitable technique is contrast-enhanced MR angiog-raphy, which provides visualization of the heart and entire arterial vascular system. MRIis used to evaluate aortic aneurysms and is reported to be as accurate as CT angiog-raphy and invasive angiography for preoperative measurement of aneurysm size andextent [46, 47]. In patients treated with endovascular stent grafts, MRI has been shownto demonstrate changes in the aneurysm and in the stent-graft morphology, throm-bus formation, periaortic inflammation, and vertebral body infarction [48, 49]. Contrast-enhanced MR angiography has been reported to be a feasible and accurate method todepict significant stenoses and occlusions in lower extremity arteries [50, 51]. Contrast-enhanced MR angiography was also found to demonstrate high diagnostic value in thediagnosis of carotid artery stenosis or occlusion, thus it could be used as an effectivealternative to invasive angiography [52] (Fig. 12).
Recent technical developments in hardware and software as well as introduction ofnew imaging parameters has enabled MRI to become the standard of reference for func-tional evaluation of cardiovascular diseases such as evaluation of global cardiac functionand perfusion [53, 54]. As such, MR angiography has replaced most of the invasive car-diac angiography examinations [55]. ECG-gated multiplanar fast gradient echo MRI is atechnique for demonstrating morphology of the heart and great vessels. With this tech-nique, bright blood images at different cardiac phases on multiple slice locations can beacquired within a single breath-hold. A complete cardiac MR examination consists offunctional imaging of the left ventricular myocardium with the aim of detecting regionalor global wall motion abnormalities, which can be caused by several diseases. Most of

224 Medical Imaging of the Heart and Cardiovascular System
Figure 12. Cerebral MR angiography. 3D MR angiography shows left internal carotid artery (ICA) stenosis(arrow). (Image courtesy of Associate Professor Kartini Rahmat, University of Malaya Medical Centre, KualaLumpur, Malaysia.) TOF MRA – time of flight MR angiography.
these common abnormalities are caused by atherosclerosis-induced coronary artery dis-ease due to insufficient blood/oxygen supply to the myocardium or myocardial scarsfollowing myocardial infarction [55]. Perfusion imaging of the myocardium that is per-formed at rest and with pharmacologically-induced stress allows analysis of the con-dition of coronary arteries [56]. Delayed contrast-enhanced imaging allows detection ofmyocardial infarction, scars, and otherwise structurally changed myocardium due to anincreased interstitial space [57].
Several studies have shown the excellent diagnostic accuracy of MR myocardial perfu-sion imaging for detecting obstructive coronary artery disease when compared to inva-sive coronary angiography [58, 59], and hemodynamically significant CAD compared toinvasive functional measurements [60, 61]. It has been reported that MR myocardial per-fusion imaging is as accurate in demonstrating CAD as SPECT and of similar prognosticvalue [62–64]. Because MR myocardial perfusion imaging does not use ionizing radiation,it may serve as an ideal additional functional imaging technique along with coronaryCT angiography for evaluating patients suspected of having CAD [65]. Recent studieshave shown the improved diagnostic performance of combined coronary CT angiogra-phy and perfusion cardiac MRI when compared to invasive coronary angiography in thecomprehensive workup of hemodynamically stenosed CAD [65, 66].
4.5. Doppler Ultrasonography
Doppler ultrasound is an adjunct, non-invasive procedure used to study the heart andperipheral vascular tree and corresponding abnormalities. Since the 1970s, it has becomethe mainstay of non-invasive imaging of blood flow through the heart and cardiovas-cular system by displaying flow data on the two-dimensional sonographic image. It isused to determine the direction and velocity, as well as the presence or absence of bloodflow in both arteries and veins. With Doppler ultrasonography, the blood flow is notaffected until any obstruction present is at least 50%. This technique is valuable in vas-cular imaging as it helps reveal physiological characteristics (blood flow pattern andvelocity changes) and define anatomy such as plaque morphology (Fig. 13).
Color Doppler depicts local flow by color-encoding an estimate of the mean Dopplerfrequency shift at a particular position in color. It has the capability of identifying valvu-lar, congenital, and other forms of heart disease, as the color flow image provides spatialinformation to the Doppler data. Color flow display makes the Doppler data more read-ily understandable because of the avoidance of complex spectral velocity displays. Power

Medical Imaging of the Heart and Cardiovascular System 225
Figure 13. Carotid Doppler ultrasound. Doppler ultrasound shows a thrombus formation in the right commoncarotid artery in a 66-year old man with strong bruits, but no symptoms of stroke. (Image courtesy of Dr EvelynLM Ho, Consultant Radiologist, Imaging Department, Sime Darby Specialist Centre Megah Sdn. Bhd., PetalingJaya, Malaysia.)
Doppler has added a color Doppler mode that encodes the power rather than the veloc-ity and direction of the Doppler signal [67, 68]. Power Doppler ultrasonography is ableto improve the sensitivity to flow and provide better delineation of tortuous vessels dueto its dynamic range and relative angle independence [69].
Doppler ultrasonography has been used widely for imaging the cardiovascular sys-tem, and the most common applications include evaluation of carotid artery stenosisand peripheral vascular disease [52, 70–72]. Doppler ultrasonography has been validatedby several large multi-center randomized control trials investigating the treatment ofocclusive carotid disease and is considered the gold standard technique [73-75]. This isconfirmed by a recent study showing that Doppler ultrasonography is more accuratethan CT in assessing the carotid artery disease, and is useful for evaluating patients withsignificant stenosis of the carotid tree [76]. A meta-analysis reported the diagnostic valueof Doppler ultrasonography in peripheral arterial disease to have fairly good sensitivity(87.6%) and specificity (94.7%), but is inferior to MR angiography (97.5% and 96.2% forpooled sensitivity and specificity, respectively) [72].
Doppler ultrasonography has been considered to be a potentially attractive alterna-tive to CT angiography in the follow-up of patients treated with aortic stent grafts,since ultrasound is less expensive and does not involve ionizing radiation or potentiallynephrotoxic contrast [77, 78]. Color Doppler ultrasonography was inaccurate in the mea-surements of aneurysm diameters when compared to CT angiography [79], however,contrast-enhanced ultrasound improved the diagnostic value of Doppler ultrasonographyfor detection and evaluation of vessels in case of low flow, slow flow, or deep vessels [80].Several studies have supported the use of contrast agents for increasing the sensitivityof color Doppler ultrasonography for detection of endoleak, the most common complica-tion of endovascular repair or aortic aneurysms, although CT angiography still remainsthe modality of choice in the follow-up of patients with abdominal aortic aneurysmafter endovascular repair [79, 81, 82]. With the prevailing concerns about increasing radi-ation dose and cost associated with CT scans, Doppler ultrasonography was recentlyshown to be a safe and effective tool in the monitoring of patients following endovascu-lar repair [83]. Where Doppler ultrasonography is validated as sensitive and with highnegative predictive value, it may replace CT angiography for follow-up of endovascu-lar repair, with CT angiography reserved for cases of positive or inconclusive Dopplerultrasonography.
226 Medical Imaging of the Heart and Cardiovascular System
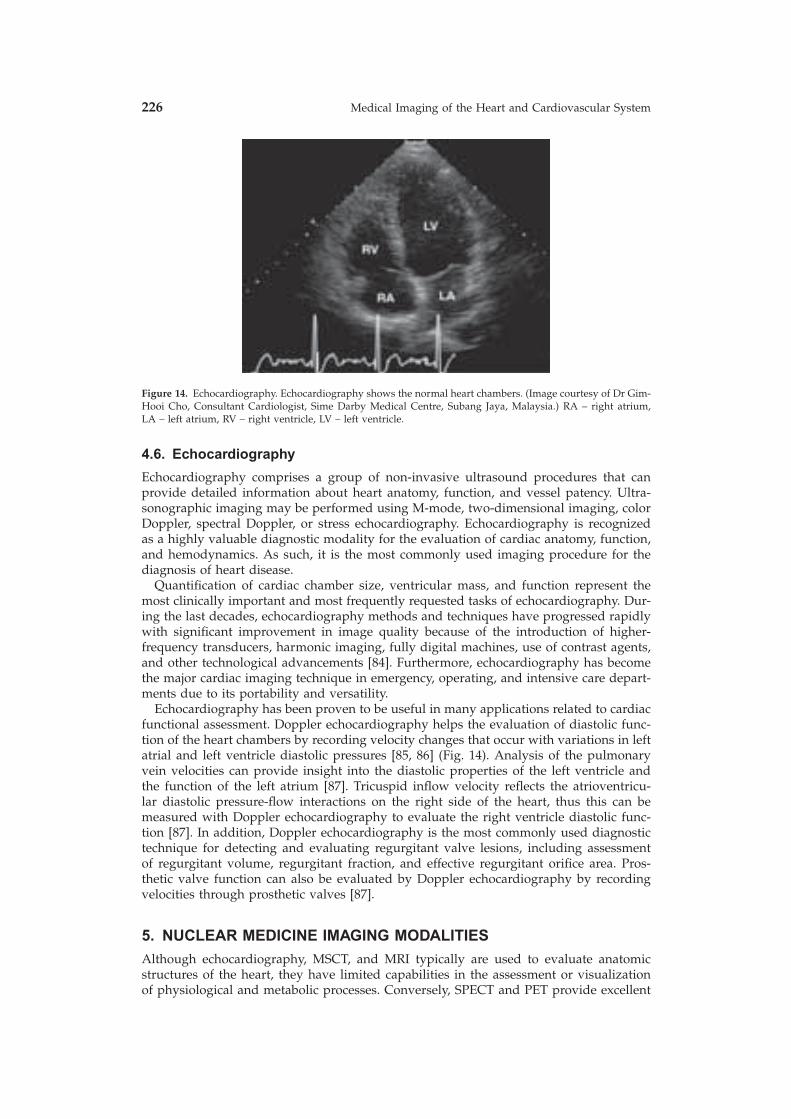
Figure 14. Echocardiography. Echocardiography shows the normal heart chambers. (Image courtesy of Dr Gim-Hooi Cho, Consultant Cardiologist, Sime Darby Medical Centre, Subang Jaya, Malaysia.) RA – right atrium,LA – left atrium, RV – right ventricle, LV – left ventricle.
4.6. Echocardiography
Echocardiography comprises a group of non-invasive ultrasound procedures that canprovide detailed information about heart anatomy, function, and vessel patency. Ultra-sonographic imaging may be performed using M-mode, two-dimensional imaging, colorDoppler, spectral Doppler, or stress echocardiography. Echocardiography is recognizedas a highly valuable diagnostic modality for the evaluation of cardiac anatomy, function,and hemodynamics. As such, it is the most commonly used imaging procedure for thediagnosis of heart disease.
Quantification of cardiac chamber size, ventricular mass, and function represent themost clinically important and most frequently requested tasks of echocardiography. Dur-ing the last decades, echocardiography methods and techniques have progressed rapidlywith significant improvement in image quality because of the introduction of higher-frequency transducers, harmonic imaging, fully digital machines, use of contrast agents,and other technological advancements [84]. Furthermore, echocardiography has becomethe major cardiac imaging technique in emergency, operating, and intensive care depart-ments due to its portability and versatility.
Echocardiography has been proven to be useful in many applications related to cardiacfunctional assessment. Doppler echocardiography helps the evaluation of diastolic func-tion of the heart chambers by recording velocity changes that occur with variations in leftatrial and left ventricle diastolic pressures [85, 86] (Fig. 14). Analysis of the pulmonaryvein velocities can provide insight into the diastolic properties of the left ventricle andthe function of the left atrium [87]. Tricuspid inflow velocity reflects the atrioventricu-lar diastolic pressure-flow interactions on the right side of the heart, thus this can bemeasured with Doppler echocardiography to evaluate the right ventricle diastolic func-tion [87]. In addition, Doppler echocardiography is the most commonly used diagnostictechnique for detecting and evaluating regurgitant valve lesions, including assessmentof regurgitant volume, regurgitant fraction, and effective regurgitant orifice area. Pros-thetic valve function can also be evaluated by Doppler echocardiography by recordingvelocities through prosthetic valves [87].
5. NUCLEAR MEDICINE IMAGING MODALITIES
Although echocardiography, MSCT, and MRI typically are used to evaluate anatomicstructures of the heart, they have limited capabilities in the assessment or visualizationof physiological and metabolic processes. Conversely, SPECT and PET provide excellent

Medical Imaging of the Heart and Cardiovascular System 227
information about physiological and metabolic characteristics but are limited in theircapability to visualize anatomical structures. By using anatomical imaging modalitiescombined with molecular imaging technologies such as SPECT and PET, it is possible todetect disease processes at the anatomical, physiological, metabolic, and molecular levels[88]. Therefore, this allows early detection of diseases, objective monitoring of therapies,and better prognosis of disease progression [89].
5.1. Single Photon Emission Computed Tomography
SPECT is composed of conventional scintigraphy and computed tomography techniquesthat present three-dimensional and functional information about the patient’s anatomyin more detail. Myocardial perfusion imaging (MPI) with SPECT is a widely establishedmethod for non-invasively evaluating the myocardial viability, left ventricular function,and coronary artery stenosis. SPECT has been used as a routine technique in the clinicalpractice for myocardial perfusion imaging for decades [90]. The most important applica-tions of SPECT are in the diagnosis of CAD, prediction of prognosis, selection for revas-cularization, and assessment of acute coronary syndromes (Fig. 15). Moreover, SPECThas special value in some particular patient subgroups [91–94].
Many studies have reported the varying degree of diagnostic accuracy of SPECT fordetection of CAD. Specificity varies among studies depending upon patient population,nature of reporting, and referral bias [95]. In the largest single study of 2560 patientsrandomized to each of the three radiotracers (thallium, MIBI, and tetrofosmin) and usingmainly adenosine stress, overall sensitivity, and specificity in the subset of patients under-going angiography was 91% and 87%, respectively, with no significant difference betweenthe three tracers [96]. In general, the sensitivity of stress SPECT for detecting CAD definedby invasive coronary angiography is consistently above 70%, but in the better designedstudies it is within the range of 85–90% [97–99]. Reported specificity varies from 33% to100% but in the better quality studies it is within the range of 70–75% [99–101].
Figure 15. Cardiac SPECT. SPECT shows the myocardial perfusion defect in the left anterior coronary segmentin a 63-year old woman with suspected coronary artery disease. (Image courtesy of Professor Mu-Hua Cheng,Chief of Department of Nuclear Medicine, Third Hospital Affiliated Sun Yat-Sen University, People Republicof China).

228 Medical Imaging of the Heart and Cardiovascular System
5.2. Positron Emission Tomography
PET is a powerful, quantitative imaging modality that has been used for decades tonon-invasively investigate cardiovascular biology and physiology. Due to its inherentlyquantitative nature, its superior detection sensitivity, and its advantageous spatial andtemporal resolution over conventional nuclear medicine techniques, PET has been consid-ered a gold standard for non-invasive assessment of myocardial perfusion and viability.Nonetheless, the lack of widespread availability of PET scanners and radiotracers, itshigh cost, the limited data supporting its application, and reimbursement issues in somecountries have all contributed to the limited clinical acceptance of PET as a routine diag-nostic tool. However, recognition of the value of cardiac PET has been changing recentlybecause of its widely accepted clinical role in oncology. This has led to an increase in thenumber of PET scanners installed worldwide, thereby creating opportunities for morecardiac applications.
PET has been reported to be valuable in the diagnosis of CAD as it allows for assess-ment of myocardial perfusion (Fig. 16). In an early review of eight studies consisting ofa total of nearly 800 patients that compared perfusion PET with coronary angiography,results were summarized and a mean sensitivity and specificity of 93% and 92% wasobserved, respectively [102]. A more recent review from nine studies that looked at 877patients, reported a weighted sensitivity of 90% and specificity of 89% with most of thescans performed with rubidium-82 (82Rb) [103]. For detection of myocardial ischemia,myocardial perfusion PET is considered to have superior diagnostic accuracy when com-pared with the more widely available and more frequently used SPECT technique [103].Bateman et al. in their prospective study compared matched pharmacological stresspatients and concluded that myocardial perfusion PET was superior to SPECT in imagequality, certainty in interpretation, and diagnostic accuracy [94]. This was also confirmedby a recent study comparing PET with SPECT in two comparable patient cohorts withinvasive coronary angiography as the gold standard. Husmann et al. reported that 13N-ammonia PET is more sensitive and specific in the detection and localization of coronarystenoses, and more specific in the detection of ischemia than SPECT [104].
Figure 16. Cardiac PET. Myocardial viability study using 18F FDG PET in a 47-year old man shows that thedistribution of FDG is homogeneous and no defect is observed in the cardiac chamber. (Image courtesy ofAssociate Professor Abdul Jalil Nordin, Director, Diagnostic Nuclear Imaging Centre, University Putra Malaysia,Selangor, Malaysia.)

Medical Imaging of the Heart and Cardiovascular System 229
In addition to the high diagnostic accuracy, PET has been shown to demonstrate prog-nostic value with potential to predict adverse cardiac events [105]. Studies have shownthat PET has an independent and prognostic value with increased annual mortality ratebeing associated with abnormal scans [105, 106]. A recent study confirmed the prognosticvalue of PET in 1441 patients with suspected or known CAD, and it demonstrated anincremental value of stress in the left ventricular ejection fraction from gated PET [107].The ability to quantify myocardial blood flow and coronary flow reserve in absoluteterms is another feature of unique PET imaging [108]. Quantitative flow measurementsmay be useful and complementary to the current standard of visual/semi-quantitativeanalysis. PET imaging may be useful for detection and evaluation of extensive multives-sel CAD with balanced ischemia, evaluation of collateral flow, identification of endothe-lial dysfunction in pre-clinical disease, and reliable monitoring of therapeutic strategies[109–111].
Myocardial viability testing has been developed to serve as a guide to the most appro-priate therapy in patients with advanced CAD and severe left ventricular dysfunction.PET has played a key role in understanding the myocardial response to severe ischemiadamage and in establishing the identification of myocardial viability as a diagnostictarget. It is well-known that PET with the use of the metabolic radiotracer FDG (fluo-rodeoxyglucose) is able to accurately predict improvement of regional wall motion andglobal left ventricular ejection fraction after revascularization. In a recent meta-analysisof 24 studies consisting of 756 patients, PET demonstrated a weighted mean sensitivityand specificity of 92% and 63%, respectively, for regional functional recovery [112]. Theusefulness of PET in cardiac imaging has been supported by growing evidence, althoughmore rigorous studies are needed to confirm its clinical value.
Recently, several reports have highlighted the potential role of PET for the assessmentof various aortic diseases based on the FDG accumulation [113–117]. FDG PET findingscan provide additional information for the diagnosis of aortic aneurysm [114], aortitis orperiaortitis [115], Takayasu arteritis [116], intramural hematoma [117] and vascular graftthrombus and infection [92].
5.3. Hybrid Imaging Modalities
5.3.1. Hybrid Single Photon Emission Computed Tomography and
Computed Tomography
More recently, integrated SPECT/CT scanners have become available, including systemscombining a state-of-the-art multihead gamma-camera and MSCT scanner side by sidewith a common imaging table. Combined SPECT/CT provides both functional informa-tion from SPECT and anatomical information from CT in a single examination. Stud-ies have demonstrated that the information obtained by SPECT/CT is more accuratein evaluating patients than that obtained from either SPECT or CT alone [118, 119].Rispler et al. [120] used an integrated SPECT/CT scanner to identify the presence ofcoronary stenoses, and at the same time, determined their functional significance throughmyocardial perfusion imaging. Diagnostic performance of SPECT/CT, especially speci-ficity and positive predictive value was found to be superior to CT and SPECT alone, thushybrid SPECT/CT may induce physiology-based planning of interventional proceduresin patients with demonstrated CAD.
Hybrid cardiac SPECT/64-slice CT is the latest technology that allows performingboth myocardial perfusion SPECT and coronary CT angiography in a single session withsubsequent co-registration of data obtained from each imaging modality into a fusedimage, thus enabling simultaneous evaluation of coronary artery anatomy and assess-ment of the physiological relevance of coronary stenosis. It has been shown that combinedSPECT/CT provides a good assessment of the left ventricular function with good corre-lation to those determined by CT angiography or SPECT, with a very low inter-observervariability [121].

230 Medical Imaging of the Heart and Cardiovascular System
5.3.2. Hybrid Positron Emission Tomography and Computed Tomography
Despite improved diagnostic performance, the SPECT/CT scanner might not be suffi-ciently accurate to be established as the new diagnostic and therapeutic regime in patientswith known CAD. Segments with coronary stenosis but normal SPECT still showed sig-nificantly reduced coronary flow reserve. Thus, it might be desirable to invest in hybridPET/CT scanners, so as not to underestimate the extent of inducible cardiac ischemia.The advent of hybrid PET/CT has led to the unique opportunity to combine CT-derivedmorphological information with PET-derived functional, physiological, and biologicalinformation. Most PET/CT scanners are equipped with MSCT, allowing CT measure-ment of coronary calcium and coronary CT angiography for analysis of CAD in additionto PET imaging procedures.
Initial studies suggested that both CT coronary angiography and perfusion PET maybe complementary rather than competitive, although more evidence is needed to con-firm the value of integrated modalities [118]. Integrated PET/CT provides an opportu-nity to assess the presence and magnitude of subclinical atherosclerotic disease burden,and measure myocardial blood flow as marker of endothelial health and atherosclero-sis disease activity [119]. Contrast-enhanced CT enables the detection of non-calcifiedor vulnerable plaque; however, this information is best combined with PET imaging asPET/CT offers insights into atherothrombotic processes, better risk-stratification, opti-mal selection of therapeutic targets, and the effective means for monitoring therapeuticresponses [122].
PET/CT has been shown to have high diagnostic performance in the detection ofobstructive atherosclerosis among patients with suspected CAD. Sampson et al. [123]reported that diagnostic sensitivity of PET/CT in patients with single-vessel disease was92% higher than that reported with conventional techniques [124], while the specificity ofPET/CT was comparable with that reported in previous studies using PET alone (83% vs86%) [91, 125]. In addition, the diagnostic sensitivity was equally high in obese and non-obese patients (mean BMI >30 kg/m2�. Similarly, Santana et al. [126] applied a newlydeveloped normal database and criteria in a prospective population to test the diagnosticaccuracy of database quantitative PET/CT. The quantitative approach was validated intheir study with high accuracy achieved for the detection and localization of CAD. Theyrecommended that physicians consider using the quantitative method in their study asdecision support tools to aid with image interpretation.
6. IONIZING RADIATION EXAMINATIONS-RADIATION
DOSE ISSUE
Globally, the use of ionizing radiation in medical application has increased significantly.It is being used daily for imaging of patients in more than 10 million diagnostic radi-ology procedures and 100,000 diagnostic nuclear medicine procedures worldwide [127].It is also used daily for radiotherapy of patients as well as many therapeutic nuclearmedicine procedures. It has proven to be able to bring tremendous medical benefits tomankind. However, as ionizing radiation is associated with risks due to stochastic andnon-stochastic effects, it is essential to consider the protection of patients from potentialharm resulting from the use of ionizing radiation.
The main issue in radiation protection of patients is the rapidly increasing collectivedose to patients from medical exposure. This is due to the rapid increase of new technolo-gies for medical exposure, and the corresponding speed at which these technologies areadopted into clinical practice. In particular, the increased use of CT with associated highradiation dose is an example of a clear and prominent upward trend [128]. Other currentimportant directions include increased awareness of radiation risks from both health careprofessionals and the public, inappropriateness of a substantial number of diagnosticimaging examinations performed, as well as recurring safety issues in interventional andtherapeutic procedures.

Medical Imaging of the Heart and Cardiovascular System 231
6.1. Radiation Doses Relevant to Cardiac Angiography and
Associated Interventional Procedures
The hazards associated with cardiac angiography and associated interventional proce-dures are well documented in the literature, with effects ranging from mild erythemato skin ulceration and necrosis [129–140]. In regional and national legislative documents[141, 142], the need to focus on such high dose examinations is acknowledged so thatregional variations can be highlighted, causal agents for such variations can be identified,and appropriate corrective action put into place wherever possible. With interventionalprocedures in general it is often quite rightly argued that many of the patients under-going these procedures are very ill and require these procedures for palliative effects.In cardiac procedures, however patients are often relatively young and once interven-tional procedures are performed they can live heathily for many years, underlining theimportance of dose optimization if adverse radiation-induced side-effects are not to beexperienced.
Radiation doses can vary substantially across the same cardiac angiographic and inter-ventional procedures, which is often a result of varying complexities of examinationor patient size, but can be a consequence of technological or procedural preference. Ina recent study involving almost 2,000 cardiac procedures [143], a regression analysisdemonstrated that the most important causal agent for dose variations (as with manyother fluoroscopic examinations) was fluoroscopic time. This factor alone accounted for61%, 59%, 44%, and 37% of the dose variation seen for percutaneous coronary inter-vention, permanent pacemaker insertion, coronary arteriography, and coronary arteriog-raphy with percutaneous coronary intervention procedures, respectively. Other factorsidentified as being responsible for variations in dose included patient body mass index,complexity of procedure, cine run time, number of previous grafts, number of stents, andexperience of operator.
The relevance of diagnostic reference levels (DRLs) to cardiac procedures is debatable.DRLs are radiation dose values for specific examinations that should not be consistentlyexceeded when good practice is in place and if regularly exceeded remedial action shouldbe sought. These are legal requirements in a number of jurisdictions [141, 142], and havebeen shown to be very effective in reducing dose and dose variations for a variety ofinvestigations since their introduction two decades ago. It is often argued that DRLscannot work for cardiac procedures since patient size variations and complexity of exam-inations mean that variations will always exist and these would be difficult to control.Indeed, excessive standardization of doses may be at the detriment of the patient. Thecounter-argument to this is that since fluoroscopic time is the main variable and this isshown to vary significantly for other much less complex examinations, operator prefer-ence may well be a factor in these dose variations. Also, DRLs can be set for groupsof specific patient sizes. Clearly, further work is required to explore the relevance andapplication of DRLs for cardiac procedures and to establish if such complex factors, suchas operator practices, can be standardized to some extent.
Collective dose is also another issue. While the individual doses as shown above arehigh, due to the cost effectiveness, low patient morbidity, and the opportunity for suchexaminations to be performed on a day-case basis, cardiac angiography and associatedinterventional procedures are increasingly popular. In a population such as the UK, in asingle year, over 162,000 cardiac angiography cases are performed in addition to almost122,000 cardiovascular interventions. These data were presented in 2002 and it is likelythat these numbers are on the increase. Whatever the precise numbers are at the timeof this publication, the product of these procedural numbers and the radiation doseper examination suggest that cardiac angiography procedures contribute significantly tothe average annual radiation dose delivered to an individual within a given populationwhere these examinations are performed regularly.
In summary, while cardiac angiographic procedures are of huge clinical value, goodoptimization and justification procedures should be in place. Doses delivered oftenexceed the threshold of non-stochastic effects and present significant stochastic risk to

232 Medical Imaging of the Heart and Cardiovascular System
patients and staff. Dose optimization and standardization of procedures should be imple-mented to maximize the investigative and therapeutic benefit for patients who undergosuch procedures.
6.2. Chest Radiography
Chest radiography is the most commonly performed x-ray examination in clinical prac-tice. Chest radiographs are valuable for solving a variety of clinical problems, and serveas the first line diagnostic technique for determining further steps in the establishment ofa diagnosis, treatment, and follow-up procedure [144]. Although individual patient dosein chest radiography is relatively low, its contribution to the collective dose is signifi-cant due to the frequent use of this examination. About 30–40% of all diagnostic X-rayexaminations are reported to be chest radiography [145–147]. The associated estimatedcontribution to the collective dose is about 18% [145]. Thus, optimization of image qualityand radiation dose in chest radiography is an important ongoing activity.
In the past decades a shift has occurred from the principle of ‘image quality as goodas possible’ to ‘image quality as good as acceptable.’ Radiation dose to patients shouldbe ‘as low as reasonably achievable’ (ALARA), while still providing diagnostic imagequality [148, 149]. Dose reduction of up to 50% can be achieved by adjusting the imag-ing parameters such as tube voltage or tube current without compromising diagnosticperformance [150, 151]. Therefore, optimization of chest radiography should comprise asignificant component of good routine clinical practice.
6.3. Computed Tomography
Although CT represents 10–15% of all X-ray examinations, it contributes up to 70% ofthe radiation exposure. Radiation dose is becoming a major issue for MSCT angiography,since 64- or more-slice CT shows improved diagnosis of CAD [152, 153]. It is estimatedthat in daily practice, the effective dose of cardiac MSCT angiography may reach upto 40 mSv in female patients if no dose optimization strategies are applied, and this isassociated with radiation exposure to breast tissues. Cardiac patients may also be exposedto other sources of medical radiation (including from nuclear medicine and invasivecoronary angiography examinations). With repeated examinations and the cumulatedradiation dose, radiation exposure has become a definite risk to patients. Given the factthat CT is a high-dose imaging modality, it is critical to minimize the radiation doseassociated with cardiac MSCT examinations.
Two recent studies published in the Archives of Internal Medicine highlighted theimportance of standardization of common CT examinations including cardiac CT imag-ing, as well as the cancer risk associated with radiation [154, 155]. Smith-Bindman et al.[154] analyzed the radiation doses for the most commonly performed CT examinationsat four institutions and found a surprising variation in radiation dose—a mean 13-foldvariation between the highest and lowest dose for each CT examination studied (range,6- to 22-fold difference across study types). The researchers estimated that 1 in every 27040-year-old women undergoing a CT coronary angiogram will develop cancer from theprocedure. In another study, de Gonzalez et al. [155] estimated that CT scans done in 2007could have led to 29,000 excess cancers. These cancers will appear in the next 20 to 30years and according to their estimation, at a 50% mortality rate, will cause approximately15,000 deaths annually.
Radiation-induced malignancy is a problem that has been addressed by the NationalResearch Council of the United States [156]. It is reported that radiation dose from aCT examination has been significantly underestimated by the radiologists and physicians[157, 158]. Despite the increased awareness of radiation risk, they have not realized theamount of radiation exposure associated with cardiac CT and the possibility of optimiz-ing the scanning protocols to reduce radiation dose. An international, multicenter studyof 50 study sites, looking at estimated radiation dose during cardiac CT angiography, hasshown a wide range of median effective dosea that ranged from 5 to 30 mSv [159]. The

Medical Imaging of the Heart and Cardiovascular System 233
study also indicated that radiation exposure can be reduced substantially by implement-ing available strategies for dose reduction; however, these strategies are not frequentlyused in clinical practice.
Recently tremendous progress has been made to lower radiation dose for cardiac MSCTangiography, and various strategies have been proposed to address this issue. Readersare referred to some excellent review articles with regard to the dose reduction and justi-fication of the use of MSCT in cardiac imaging [160–162]. In addition, the benefits of theusing coronary MSCT angiography in the diagnostic workup and patient managementmust be weighed against the potential risks related to radiation exposure.
In summary, radiation exposure associated with cardiac MSCT angiography hasincreased substantially over the past two decades, and it is a major concern that requiresthe attention of both clinicians and manufacturers. Radiation exposure is especiallyimportant for young, female patients who present with atypical symptoms, but do nothave high pre-test likelihood for actually having hemodynamically significant coronarystenosis. Cardiac CT angiography should be performed with dose optimization strategieswhenever possible to reduce the radiation dose to patients. MSCT scanning protocols incardiac imaging should be standardized across institutions with the aim of reducing dosevariation across patients and facilities. Physicians need to follow guidelines, such as thenational DRL, for dose optimization, and they are encouraged to participate in radiationdose registry to obtain feedback on radiation dose levels when compared to other insti-tutions. Utilization of cardiac MSCT angiography must be defined as to whether it leadsto the greatest benefit and whether the radiation risk may be greater than the benefitexpected from the CT examinations.
6.4. Nuclear Medicine Imaging
The medical use of ionizing radiation and radionuclides contributes significantly to theradiation exposure of individuals and populations. It has become common to quantifythe patient’s exposures in terms of the effective dose [163]; however, in nuclear medicineimaging, the radiation dose can only be assessed indirectly via known amounts andtypes of administered radiopharmaceuticals. Overall, the diagnostic practice with radio-pharmaceuticals accounts for a small proportion of all radiological examinations withthe annual number of nuclear medicine examinations and their collective doses repre-senting only 2% and 6%, respectively, of the corresponding values for X-ray examina-tions. However, the mean dose per procedure for nuclear medicine imaging (4.6 mSv)is higher than that for conventional X-ray examinations (1.2 mSv) and similar to thatfor CT scan (2–8 mSv) [164, 165]. Thus, this collective dose arising from nuclearmedicine examinations allows evaluation of the additional risk of radiation-inducedmalignancy.
Nuclear medicine imaging is different from other imaging modalities as medical staff,especially nuclear medicine technologists, are at potential risk of exposure to ionizingradiation while carrying out a variety of tasks associated with each nuclear medicine
Table 1. Average effective doses for various imaging modalities (Revised from Refs. [165, 172–174]).
Examination Average effective dose (mSv)
Chest radiography-Posteroanterior and lateral 0.05–0.24Cardiac CT angiography (retrospective gating) 7.6–31.8Cardiac CT angiography (prospective gating) 1.7–12.6Electron beam CT 0.6–1.3Cardiac SPECT (rest+ stress) 8.5–14.4Cardiac PET (rest+ stress) 2.2–7.0Cardiac SPECT/CT 24.1–41.5Cardiac PET/CT 5–20Whole body PET/CT 20–25Diagnostic cardiac angiography 2–9Percutaneous cardiac intervention 15.0

234 Medical Imaging of the Heart and Cardiovascular System
procedure. Many studies have demonstrated that the exposure of nuclear medicine tech-nologists arises mainly from radioactive patients rather than from the preparation ofradiopharmaceuticals [166–168]. Various measurements of technologists’ exposure havebeen proposed and methods are recommended with the aim of reducing the radiationexposure during routine nuclear medicine procedures [169–172]. In addition, with com-bined imaging modalities such as SPECT/CT or PET/CT, the radiation dose to the patientis the combination of the radiation dose from the SPECT or PET radiopharmaceuticals,as well as the radiation dose from the CT portion of the study.
Table 1 shows the average effective dose for various imaging modalities reported inthe literature.
7. SUMMARY AND CONCLUSION
Medical imaging techniques play an important role in the visualization and diagnosis ofcardiovascular diseases. As mentioned above, these techniques range from conventionalradiographic imaging such as chest radiography to advanced modalities such as MSCTin cardiac imaging and PET or PET/CT imaging. Rapid technological developments ofimaging modalities have challenged the conventional invasive angiography proceduresince less-invasive modalities offer high diagnostic accuracy for detection and diagno-sis of a variety of cardiovascular diseases. In some areas, invasive angiography hasbeen replaced by less-invasive modalities such as in the diagnosis of abdominal aorticaneurysm, pulmonary embolism, and peripheral arterial disease where MSCT angiogra-phy offers superior diagnostic performance over invasive angiography. In the diagnosisof CAD, MSCT angiography demonstrates promising results due to its increased perfor-mance with 64- or more slice CT, although presently MSCT has not reached the diagnosticaccuracy to replace invasive coronary angiography. In particular, the very high negativepredictive value of MSCT angiography indicates that it can be used as a reliable screeningmodality for patients with suspected CAD.
Functional imaging modalities, such as SPECT and PET, are increasingly used in theassessment of myocardial perfusion with the aim of predicting disease progress andproviding prognostic information which is valuable for patient management. Combinedfunctional imaging and anatomical modality, such as PET/CT, is developing and willplay an increasing role in the assessment of cardiovascular diseases by maximizing theperformance of each individual modality. Another advantage of functional imaging is itsability to provide molecular imaging, which will influence the management and improveunderstanding of the major cardiovascular diseases that have substantial clinical impactand research interest. This area is fast-growing, and more research outcomes are antici-pated to be published in the near future.
Despite promising results having been achieved with these imaging modalities, atten-tion must be paid to the limitations or disadvantages associated with each modality. Mostimportantly, radiation dose is a major issue that has raised serious concern in the medicalfield. Therefore, clinicians need to be aware of the potential risks associated with radi-ation exposure to patients and justify the selection of imaging modalities for diagnosticand management purposes.
REFERENCES
1. S. San, H. Kesteloot, and D. Kromhout, Eur. Heart J. 18, 1231 (1997)2. M. R. Adams and D. S. Celermajer, Clin. Sci. (Lond) 97, 615 (1999).3. J. Dormandy, L. Heeck, and S. Vig, Semin. Vasc. Surg. 12, 123 (1999).4. M. Goyen, C. U. Herborn, K. Kroger, T. C. Laurenstein, J. F. Debatin, S. G. Ruehm, Radiology 227, 277
(2003).5. T. J. Noto, Jr., L. W. Johnson, R. Krone, W. F. Weaver, D. A. Clark, J. R. Kramer, Jr., and G. W. Vetrovec,
Cathet. Cardiovasc. Diagn. 24, 75 (1991).6. Z. A. Fayad, V. Fuster, K. Nikolaou, and C. Becker, Circulation 106, 2026 (2002).7. K. Nieman, M. Oudkerk, B. J. Rensing, P. van Ooijen, A. Munne, R. J. van Geuns, and P. J. de Feyter, Lancet
357, 599 (2001).

Medical Imaging of the Heart and Cardiovascular System 235
8. P. K. Woodard, D. Li, E. M. Haacke, P. J. Dhawale, S. Kaushikkar, B. Barzilai, A. C. Braverman, P. A.Ludbrook, A. N. Weiss, J. J. Brown, S. A. Mirowitz, T. K. Pilgram, and F. R. Gultierrez, AJR Am. J. Roentgenol.170, 883 (1998).
9. M. F. D. Carli and R. Hachamovitch, J. Nucl. Cardiol. 12/1 (2006).10. R. Hachamovitch, D. S. Berman, L. J. Shaw, H. Kita, I. Cohen, J. A. Cabico, J. Friedman, and G. A. Diamond,
Circulation 97, 535 (1998).11. J. Sun, Z. Zhang, B. Lu, W. Yu, Y. Zhang, Y. Zhou, Y. Wang, and Z. Fan, AJR Am. J. Roentgenol. 190, 748
(2008).12. S. E. Nissen and P. Yock, Circulation 103, 604 (2001).13. D. Y. Lee, N. Eigler, H. Luo, T. Nishioka, S. W. Tabak, J. S. Forrester, R. J. Siegel, Am. Heart J. 129, 1084
(1995).14. G. S. Mintz, A. D. Pichard, J. A. Kovach, K. M. Kent, L. F. Satler, S. P. Javier, J. J. Popma, and M. B. Leon,
Am. J. Cardiol. 73, 423 (1994).15. P. G. Yock and D. T. Linker, Circulation 81, 1715 (1990).16. R. A. Nishimura, W. D. Edwards, C. A. Warnes, G. S. Reeder, D. R. Holmes, Jr., A. J. Tajik, and P. G. Yock,
J. Am. Coll. Cardiol. 16, 145 (1990).17. M. Nakamura, H. Nishihkawa, S. Mukai, M. Setsuda, K. Nakajima, H. Tamada, H. Suzuki, T. Ohnishi,
Y. Kakuta, T. Nakano, and A. C. Yeung, J. Am. Coll. Cardiol. 37, 63 (2001).18. G. Pundziute, J. D. Schuijf, J. W. Jukema, I. Decramer, G. Sarno, P. K. Vanhoenacker, E. Boersma, J. H.
Reiber, M. J. Schalij, W. Wijns, and J. J. Bax, Eur. Heart J. 29, 2373 (2008).19. A. Nair, B. D. Kuban, E. M. Tuzcu, P. Schoenhagen, S. E. Nissen, and D. G. Vince, Circulation 106, 2200
(2002).20. A. Nair, B. D. Kuban, N. Obuchowski, and D. G. Vince, Ultrasound Med. Biol. 27, 1319 (2001).21. K. Nasu, E. Tsuchikane, O. Katoh, D. G. Vince, R. Virmani, J. F. Surmely, A. Murata, Y, Takeda, T. Ito,
M. Ehara, T. Matsubara, M. Terashima, and T. Suzuki, J. Am. Coll. Cardiol. 47, 2405 (2006).22. T. Kubo, A. Maehara, G. S. Mintz, H. Doi, K. Tsujita, S. Y. Choi, O. Katoh, K. Nasu, A. Koenig, M. Pieper,
J. H. Rogers, W. Wijns, D. Bose, M. P. Margolis, J. W. Moses, G. W. Stone, and M. B. Leon, J. Am. Coll.Cardiol. 55, 1590 (2010).
23. J. G. Goldin, H. Yoon, L. E. Greaser, S. B. Heinze, M. M. McNitt-Gray, M. S. Brown, J. W. Sayre, A. M.Emerick, and D. R. Aberle, Radiology 221, 213 (2001).
24. G. P. Reddy, D. M. Chernoff, J. R. Adams, and G. B. Higgins, Radiology 208, 167 (1998).25. A. D. Guerci, L. A. Spadaro, K. J. Goodman, A. Lledo-Perez, D. Newstein, G. Lerner, and Y. Arad, J. Am.
Coll. Cardiol. 32, 673 (1998).26. G. D. Rubin, M. D. Dake, and C. P. Semba, Radiol. Clin. North Am. 33, 51 (1995).27. M. Mahesh, “MDCT Physics: The Basics, Technology, Image Quality and Radiation Dose.” Lippincott
Williams and Wilkins, Philadelphia, USA, 2009.28. E. K. Fishman and K. M. Horton, Eur. J. Radiol. 62(S), S1 (2007).29. T. Kido, A. Kurata, H. Higashino, Y. Sugawara, H. Okayama, J. Higaki, H. Anno, K. Katada, S. Mori,
S. Tanada, M. Endo, and T. Mochizuki, Radiat. Med. 25, 38 (2007).30. F. Rybicki, H. Otero, M. Steigner, G. Vorbiof, L. Nallamshetty, D. Mitsouras, H. Ersoy, R. T. Mather, P. F.
Judy, T. Cai, K. Coyner, K. Schultz, A. G. Whitmore, and M. D. Di Carli, Int. J. Cardiovasc. Imaging 24, 535(2008).
31. Z. Sun and K. H. Ng, Singapore Med. J. 51, 282 (2010).32. Z. Sun, C. H. Lin, R. Davidson, C. Dong, and Y. Liao, Eur. J. Radiol. 67, 78 (2008).33. J. Abdulla, Z. Abildstrom, O. Gotzsche, E. Christensen, L. Kober, and C. Torp-Pedersen, Eur. Heart J.
28, 3042 (2007).34. G. Mowatt, E. Cummins, N. Waugh, S. Walker, J. Cook, X. Jia, G. S. Hillis, and C. Fraser, Health Technol,
Assess. 12, iii-iv, ix-143 (2008).35. P. Vanhoenacker, M. Heijenbrok-Kal, R. Van Heste, I. Decramer, L. R. Van Hoe, W. Wijns, and M. G.
Hunink, Radiology 244, 419 (2007).36. P. D. Stein, A. Y. Yaekoub, F. Matta, and H. D. Sostman, Am. J. Cardiol. 121, 715 (2008).37. M. D. Armerding, G. D. Rubin, C. F. Beaulieu, S. M. Slonim, E. W. Oclott, and S. L. Samuels, Radiology
215, 138 (2000).38. Z. Sun, World J. Radiol. 31, 63 (2009).39. E. Castaner, M. Andreu, X. Gallardo, J. M. Mata, M. A. Cabezuelo, and Y. Pallardo, Radiographics 23, S93
(2003).40. C. Sebastià, E. Pallisa, S. Quiroga, A. Alvarez-Castells, R. Dominquez, and A. Evangelista, Radiographics
19, 45 (1999).41. Y. Hayashino, M. Goto, Y. Noguchi, and T. Fukui, Radiology 234, 740 (2005).42. J. P. Guilabert, D. N. Manzur, M. J. Tarrasa, M. L. Llorens, P. Braun, and M. P. Arques, Eu.r J. Radiol. 62, 220
(2007).43. U. J. Schoepf, S. Z. Goldhaber, and P. Costello, Circulation 109, 2160 (2004).44. Z. Sun, J. Vasc. Interv. Radiol. 17, 1915 (2006).45. X. M. Li, Y. H. Li, J. M. Tian, Y. Xiao, J. P. Lu, Z. P. Jing, J. Sheng, A. Edwin, and F. H. Wu, Eur. J. Radiol.
75, 98 (2010).46. S. A. Thurnher, R. Dorffner, M. M. Thurnher, F. W. Winkelbauer, G. Kretschmer, P. Polterauer, and
J. Lammer, Radiology 205, 341 (1997).

236 Medical Imaging of the Heart and Cardiovascular System
47. C. N. Ludman, S. W. Yusuf, S. C. Whitaker, R. H. Gregson, S. Walker, and B. R. Hopkinson, Eur. J. Vasc.Endovasc. Surg. 19, 524 (2000).
48. L. Engellau, E. M. Larsson, U. Albrechtsson, T. Jonung, E. Ribbe, J. Thorne, Z. Zdanowski, and L. Norgren,Eur. J. Vasc. Endovasc. Surg. 15, 212 (1998).
49. S. R. Vallabhaneni, R. G. McWilliams, A. Anbarasu, P. C. Rowlands, J. A. Brennan, D. A. Gould, P. L.Harris, and G. L. Gilliing-Smith, Eur. J. Vasc. Endovasc. Surg. 22, 535 (2001).
50. R. Janka, C. Fellner, E. Wenkel, W. Lang, W. Bautz, and F. A. Fellner, Radiology 235, 319 (2005).51. R. W. Huegli, M. Aschwanden, G. Bongartz G, K. Jaeger, H. G. Heidecker, C. Thalhammer, A. C. Schulte,
C. Hashagen, A. L. Jacob, and D. Bilecen, Radiology 239, 901 (2006).52. A. Al Shuhaimi, K. Ababtain, and Z. Sun, Radiographer 56, 14 (2009).53. M. Fenchel, A. M. Scheule, N. I. Stauder, U. Kramer, K. Tomaschko, T. Nagele, C. Bretschneider, H. P.
Schlemmer, C. D. Claussen, and S. Miller, Radiology 238, 280 (2006).54. H. Kramer, S. O. Schoenberg, K. Nikolaou, A. Huber, A. Struwe, E. Winnik, B. J. Wintersperger, O. Dietrich,
B. Kiefer, and M. F. Reiser, Radiology 236, 300 (2005).55. H. Kramer, K. Nikolaou, and M. F. Reiser, Eur. J. Radiol. 70, 418 (2009).56. D. J. Atkinson, D. Burstein, and R. R. Edelman, Radiology 174, 757 (1990).57. J. P. Laissy, F. Hyafil, L. J. Feldman, J. M. Juliad, E. Schouman-Claeys, P. G. Steg, and M. Faraggi, Radiology
237, 75 (2005).58. N. Al-Saadi, E. Nagel, M. Gross M, A. Bornstedt, B. Schnackenburg, C. Klein, W. Klimek, H. Oswald, and
E. Fleck, Circulation 101, 1379 (2000).59. J. Schwitter, D. Nanz, S. Kneifel, K. Bertschinger, M. Buchi, P. R. Knusel, B. Marincek, T. F. Luscher, and
G. K. van Schulthess, Circulation 103, 2230 (2001).60. A. A. Barmeyer, A. Stork, K. Muellerleile, A. K. Schofer, C. Tiburtius, R. Koester, T. Heitzer, G. Adam,
T. Meinertz, and G. K. Lund, J. Magn. Reson. Imaging 27, 1005 (2008).61. M. A. Costa, S. Shoemaker, H. Futamatsu, C. Klassen, D. J. Angiolillo, M. Nguyen, A. Siuciak, P. Gilmore,
M. M. Zenni, L. Guzman, T. A. Bass, and N. Wilke, J. Am. Coll. Cardiol. 50, 514 (2007).62. H. Futamatsu, C. Klassen, M. Pilla, N. Wilke, D. J. Angiolillo, S. Smalheiser, A. Siuciak, N. Suzuki, T. A.
Bass, and M. A. Costa, Int. J. Cardiovasc. Imaging 24, 293 (2008).63. J. Schwitter, C. M. Wacker, A. C. van Rossum, M. Lombardi, N. Al-Saadi, H. Ahlstrom, T. Dill, H. B.
Larsson, S. D. Flamm, M. Marquardt, and L. Johansson, Eur. Heart J. 29, 480 (2008).64. C. Jahnke, E. Nagel, R. Gebker, T. Kokocinski, S. Kelle, R. Manka, E. Fleck, and I. Paetsch, Circulation 115,
1769 (2007).65. J. G. Groothuis, A. M. Beek, S. L. Brinckman, M. R. Meijerink, S. C. Koestner, R. Nijveldt, M. J. Gotte, M. B.
Hofman, C. van Kuijk, and A. C. van Rossum, Radiology 254, 384 (2010).66. O. F. Donati, H. Scheffel, P. Stolzmann, S. Baumuller, A. Plass, S. Leschka, and H. Alkadhi, AJR Am.
J. Roentgenol. 194, 920 (2010).67. C. Martinoli, F. Pretolesi, G. Crespi, S. Bianchi, N. Gandolfo, M. Valle, and L. E. Derchi, Eur. J. Radiol. 28,
S133 (1998).68. D. S. Babcock, H. Patriquin, M. LaFortune, and M. Dauzat, Pediatr. Radiol. 26,109 (1996).69. R. W. Baumgartner, C. Schmid, and I. Baumgartner, Stroke 27, 101 (1996).70. D. A. Clevert, T. Johnson, H. Michaely, E. M. Jung, P. M. Flach, T. I. Strautz, D. D. A. Clevert, M. Reiser,
and S. O. Schoenberg, Eur. J. Radiol. 60, 379 (2006).71. C. J. Hammond, S. J. McPherson, J. V. Patel, and M. J. Gough, Eur. J. Vasc. Endovasc. Surg. 35, 405 (2008).72. K. Visser and M. G. M. Hunink, Radiology 216, 67 (2000).73. European Carotid Surgery Trialists’ Collaborative Group, Lancet 337, 1235 (1991).74. H. J. M. Barnett, D. W. Taylor, M. Eliasziw, A. J. Fox, G. G. Ferguson, R. B. Haynes, R. N. Rankin, G. P.
Clagett, V. C. Hachinski, D. L. Sackett, K. E. Thorpe, H. E. Meldrum, and J. D. Spence, N. Engl. J. Med.339, 1415 (1998).
75. MRC European Carotid Surgery Trial (ACST) Collaborative Group, Lancet 363, 1491 (2004).76. P. A. Brennan, R. S. Oeppen, M. C. Bater, N. Khosla, B. Davies, R. Puxeddu, and J. Atchley, Oral Oncol.
44, 1009 (2008).77. M. M. Thompson, J. R. Boyle, T. Hartshorn, C. Maltezos, A. Nasim, R. D. Savers, G. Fishwick, and P. R.
Bell, Br. J. Surg. 85, 346 (1998).78. Y. G. Wolf, B. L. Johnson, B. B. Hill, G. D. Rubin, T. J. Fogarty, and C. K. Zarins, J. Vasc. Surg. 32, 1142
(2000).79. Z. Sun, J. Vasc. Interv. Radiol. 17, 759 (2006).80. J. M. Correas, L. Bridal, A. Lesavre, A. Mejean, M. Claudon, and O. Helnon, Eur. Radiol. 11, 1316
(2001).81. M. F. Giannoni, G. Palombo, E. Sbarigia, F. Speziale, A. Zaccaria, and P. Fiorani, J. Endovasc. Ther. 10, 208
(2003).82. E. N. Parent, G. H. Meier, V. Godziachvili, C. J. LeSar, F. M. Parker, K. A. Carter, R. G. Gayle, R. J. DeMasi,
M. J. Marcinxzyk, and R. T. Gregory, J. Vasc. Surg. 35, 474 (2002).83. B. J. Manning, S. M. O’Neil, S. N. Haider, M. P. Colgan, P. Madhavan, and D. J. Moore, J. Vasc. Surg. 49, 60
(2009).84. R. M. Lang, M. Bierig, R. B. Devereux, F. A. Flachskampf, E. Foster, P. A. Pellikka, M. H. Picard, M. J.
Roman, J. Seward, J. S. Shanewise, S. D. Solomon, K. T. Spencer, M. St. J. Sutton, and W. J. Stewart, J. Am.Soc. Echocardiography 18, 1440 (2005).
Medical Imaging of the Heart and Cardiovascular System 237
85. M. F. Stoddard, A. C. Pearson, M. J. Kern, J. Ratcliff, D. G. Mrosek, and A. J. Labovitz, J. Am. Coll. Cardiol.13, 327 (1989).
86. R. A. Nishimura, M. D. Abel, L K. Hatle, and A. J. Tajik, Mayo Clin. Proc. 64, 181 (1989).87. M. A. Quinones, C. M. Otto, M. Stoddard, A. Waggoner, and W. A. Zoghbi, Am. Soc. Echocardiography
15, 167 (2002).88. J. C. Wu, F. M. Bengel, and S. S. Gambhir, Radiology 244, 337 (2007).89. F. A. Jaffer and R. Weissleder, Cir. Res. 94, 433 (2004).90. R. E. Stewart, M. Schwaiger, E. Molina, J. Popma, G. M. Gacioch, M. Kalus, S. Squicciarini, Z. R. al-Aouar,
A. Schork, and D. E. Kuhl, Am. J. Cardiol. 67, 1303 (1991).91. T. H. Marwick, K. Shan, S. Patel, R. T. Go, and M. S. Lauer, Am. J. Cardiol. 80, 865 (1997).92. M. G. Van der Vaart, R. Meerwaldt, R. H. J. A. Slart, G. M. van Dam, R. A. Tio, and C. J. Zeebregts, Eur.
J. Vasc. Endovasc. Surg. 35, 507 (2008).93. R. Hachamovitch, D. S. Berman, L. J. Shaw, H. Kiat, I. Cohen, J. A. Cabico, J. Friedman, and G. A. Diamond,
Circulation 97, 535 (1998).94. T. M. Bateman, G. V. Heller, A. L. McGhie, J. D. Friedman, J. A. Case, J. R. Bryngelson, G. K. Hertenstein,
K. L. Moutray, K. Reid, and S. J. Cullom, J. Nucl. Cardiol. 13, 24 (2006).95. S. R. Underwood, C. Anagostopoulos, M. Cerqueira, P. J. Ell, E. J. Flint, M. Harbinson, A. D. Kelion,
A. Al-Mohammad, E. M. Prvulvich, L. J. Shaw, and A. C. Tweddel, Eur. J. Nucl. Med. Mol. Imaging 31, 261(2004).
96. A. Kapur, K. A. Latus, G. Davies, R. T. Dhawan, S. Eastick, P. H. Jarritt, G. Roussakis, M. C. Young, C. Anag-nostopoulos, J. Bormanji, D. C. Costa, D. J. Pennell, E. M. Prvulovich, P. J. Ell, and S. R. Underwood, Eur.J. Nucl. Med. Mol. Imaging 29, 1608 (2002).
97. D. Fintel, J. Links, J. A. Brinker, T. L. Frank, M. Parker, and L. C. Becker, J. Am. Coll. Cardiol. 13, 600(1989).
98. M. H. Heijenbrok-Kal, K. E. Fleischmann, and M. G. Hunink, Am. Heart J. 154, 415 (2007).99. A. Iskandrian, J. Heo, B. Kong, and E. Lyons, J. Am. Coll. Cardiol. 14, 1477 (1989).
100. T. Marwick, A. D’Hondt, G. H. Mairesse, T. Baudhuin, W. Wijns, J. M. Detry, and J. A. Melin, Br. Heart J.72, 31 (1994).
101. G. Solot, J. Hermans, P. Merlo, J. M. Chaudron, R. Luwaert, P. Cheron, F. Bodart, and M. Beauduin, Nucl.Med. Commun. 14, 23 (1993).
102. J. Machac, Semin. Nucl. Med. 35, 17 (2005).103. M. F. Di Carli and R. Hachamovitch, Circulation 115, 1464 (2007).104. L. Husmann, M. Wiegand, I. Valenta, O. Gaemperli, T. Schepis, P. T. Siegrist, M. Namdar, C. A. Wyss,
H. Alkadhi, and P. A. Kaufmann, Int. J. Cardiovasc. Imaging 24, 511 (2008).105. L. J. Shaw and A. E. Iskandrian, J. Nucl. Cardiol. 11, 171 (2004).106. T. H. Marwick, K. Shan, S. Patel, R. T. Go, and M. S. Lauer, Am. J. Cardiol. 80, 865 (1997).107. K. Lertsburapa, A. W. Ahlberg, T. M. Bateman, D. Katten, L. Volker, S. J. Cullom, and G. V. Heller, J. Nucl.
Cardiol. 15, 745 (2008).108. F. M. Bengel, T. Higuchi, M. S. Javadi, and R. Lautamaki, J. Am. Coll. Cardiol. 54, 1 (2009).109. R. Parkash, R. A. deKemp, T. D. Ruddy, A. Kitsikis, R. Hart, L. Beauchesne, K. Williams, R. A. Davies,
M. Labinaz, and R. S. Beanlands, J. Nucl. Cardiol. 11, 440 (2004).110. O. Muzik, C. Duvernoy, R. S. Beanlands, S. Sawada, F. Davanikli, E. R. Wolfe, Jr., and M. Schwaiger, J. Am.
Coll. Cardiol. 31, 534 (1998).111. L. L. Demer, K. L. Gould, R. A. Goldstein, and R. L. Kirkeeide, J. Nucl. Med. 31, 259 (1990).112. A. F. Schinkel, J. J. Bax, D. Poldermans, A. Elhendy, R. Ferrari, and S. H. Rahimtoola, Curr. Probl. Cardiol.
32, 375 (2007).113. T. Hayashida, E. Sueyoshi, I. Sakamoto, M. Uetani, and K. Chiba, AJR Am. J. Roentgenol. 195, 229
(2010).114. N. Sakalihasan, H. Van Damme, P. Gomez, P. Rigo, C. M. Lapiere, B. Nusgens, and R. Limet, Eur. J. Vasc.
Endovasc. Surg. 23, 431 (2002).115. M. A. Walter, R. A. Melzer, C. Schindler, J. Muller-Brand, A. Tyndall, and E. U. Nitzsche, Eur. J. Nucl. Med.
Mol. Imaging 32, 674 (2005).116. M. Iwabu, Y. Yamamoto, H. Dobashi, T. Kameda, K. Kittaka, and Y. Nishiyama, Clin. Nucl. Med. 33, 872
(2008).117. A. Ryan, B. McCook, B. Sholosh, D. A. Pryma, E. Jablonowski, C. Fuhrman, and T. M. Blodgett, Clin. Nucl.
Med. 32, 729 (2007).118. M. F. Di Carli, S. Dorbala, Z. Curillova, R. J. Kwong, S. Z. Goldhaber, F. J. Rybicki, and R. Hachamovitch,
J. Nucl. Cardiol. 14, 799 (2007).119. S. Abadi, O. R. Brook, S. Rispler, A. Frenkel, A. Engel, and Z. Keidar, Eur. J. Radiol. 75, 154 (2010).120. S. Rispler, Z. Keidar, E. Ghersin, A. Roguin, A. Soli, R. Dragu, D. Litmanovich, A. Frenkel, D. Aronson,
A. Engel, R. Beyar, and O. Israel, J. Am. Coll. Cardiol. 49, 1059 (2007).121. R. Campisi and M. F. Di Carli, J. Nucl. Cardiol. 11, 3 (2004).122. M. F. Di Carli and S. Dorbala, Q J Nucl. Med. Mol. Imaging 50, 44 (2006).123. U. K. Sampson, S. Dorbala, A. Limaye, R. Kwong, and M. F. Di Carli, J. Am. Coll. Cardiol. 49, 1052
(2007).124. K. E. Fleischmann, M. G. Hunink, K. M. Kuntz, and P. S. Douglas, JAMA 280, 913 (1998).

238 Medical Imaging of the Heart and Cardiovascular System
125. F. J. Klocke, M. G. Baird, B. H. Lorell, T. M. Bateman, J. V. Messer, D. S. Berman, P. T. O’Gara, B. A.Carabello, R. O. Russell, Jr., M. D. Cergueira, M. G. St. John Sutton, A. N. DeMaria, J. E. Udelson, J. W.Kennedy, M. S. Verani, K. A. Williams, E. M. Antman, S. C. Smith, Jr., J. S. Alpert, G. Gregoratos, J. L.Anderson, L. F. Hiratzka, D. P. Faxon, S. A. Hunt, V. Fuster, A. K. Jacobs, R. J. Gibbons, and R. O. Russell,J. Am. Coll. Cardiol. 42, 1318 (2003).
126. C. A. Santana, R. D. Folks, E. G. V. Garcia, L. Verdes, R. Sanyal, J. Hainer, M. F. Di Carli, and F. P. Esteves,J. Nucl. Med. 48, 1122 (2007).
127. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). 2008 report to theGeneral Assembly, annex on medical exposures, New York, 2010.
128. L. Holmberg, J. Malone, M. Rehani, D. McLean, and R. Czarwinski, Eur. J. Radiol. 76, 15 (2010)129. T. B. Shope, Radiographics 16, 1195 (1996).130. D. A. Lichtenstein, L. Klapholz, D. A. Vardy, I. Leichter, M. Mosseri, S. N. Klaus, and L. T. Gilead, Arch.
Dermatol. 132, 663 (1996).131. E. Vano, L. Arranz, J. M. Sastre, C. Moro, A. Ledo, M. T. Garate, and I. Minguez, Br. J. Radiol. 71, 510
(1998).132. L. K. Wagner and B. A. Archer “Minimizing Risks from Fluoroscopic X-Rays,” 3rd Edition. Houston, TX,
RM Partnership, 2000.133. E. Sovik, N. E. Klow, J. Hellesnes, and J. Lykke, Acta Radiol. 37, 305 (1996).134. M. D’Incan and H. Roger, Arch. Dermatol. 133, 242 (1997).135. M. S. Stone, K. J. Robson, and P. E. LeBoit, J. Am. Acad. Dermatol. 38, 333 (1998).136. L. Dehen, C. Vilmer, C. Humilière, T. Corcos, D. Pentousis, L. Ollivaud, D. Chatelain, and L. Dubertret,
Heart 81, 308 (1999).137. R. Miralbell, P. Maillet, N. E. Crompton, P. A. Doriot, P. Nouet, V. Verin, M. Harms, and M. Rouzaud,
J. Vasc. Interv. Radiol. 10, 1190 (1999).138. F. P. Sajben, S. B. Schoelch, and D. J. Barnette, Cutis 64, 57 (1999).139. G. T. Nahass, J. Am. Acad. Dermatol. 36, 881 (1997).140. T. Payne and E. L. Ridley, Diagn. Imaging 17, 15 (1995).141. D. Hart, M. C. Hillier, and B. F. Wall, “Doses to Patients from Medical X-ray Examinations in the UK—2000
Review,” Chilton, NRPB-W14, 2000.142. L. K. Wagner, B. R. Archer, and A. M. Cohen, J. Vasc. Interv. Radiol. 11, 25 (2000).143. C. J. D’Helft, P. C. Brennan, A. M. McGee, S. L. McFadden, C. M. Hughes, J. R. Winder, and L. A. Rainford,
Br. J. Radiol., 82, 296 (2009).144. W. J. H. Veldkamp, L. J. Kroft, and J. Geleijns, Eur. J. Radiol. 72, 209 (2009).145. W. Teeuwisse, J. Geleijns, and W. J. Veldkamp, Eur. Radiol. 17, 1795 (2007).146. H. P. McAdams, E. Samei, J. Dobbins III, G. D. Tourassi, and C. E. Ravin, Radiology 241, 5663 (2006).147. R. Daffner, “Clinical Radiology, The Essentials,” 2nd Edition. Williams & Wilkins, Baltimore, 1999.148. E. Vano, Radiat. Prot. Dos. 114, 126 (2005).149. H. P. Busch and K. Faulkner, Radiat. Prot. Dosim. 117, 143 (2005).150. L. J. Kroft, W. J. H. Veldkamp, B. J. Mertens, J. P. van Delft, and J. Geleijns, Br. J. Radiol. 80, 984 (2007).151. L. J. Kroft, W. J. H. Veldkamp, B. J. Mertens, J. J. P. van Delft, and J. Geleijns, Radiology 241, 392 (2006).152. G. L. Raff, M. J. Gallagher, W. W. O’Neill, and J. A. Goldstein, J. Am. Coll. Cardiol. 46, 552 (2005).153. S. P. Chao, W. Y. Law, C. J. Kuo, H. F. Hung, J. J. Cheng, H. M. Lo, and K. G. Shyu, Eur. Heart J. 31, 1916
(2010).154. R. Smith-Bindman, J. Lipson, R. Marcus, K. P. Kim, M. Mahesh, R. Gould, A. Berrington de Gonzalez, and
D. L. Miglioretti, Arch. Intern. Medm. 169, 2078 (2009).155. A. Berrington de Gonzalez, M. Mahesh, K. P. Kim, M. Bhargavan, R. Lewis, F. Mettler, C. Land, Arch.
Intern. Medm. 169, 2071 (2009).156. Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation, Nuclear and
Radiation Studies Board, Division on Earth and Life Studies, National Research Council of the NationalAcademies. Health Risks From Exposure to Low Levels of Ionizing Radiation, BEIR VII Phase 2Washington, DC, The National Academies Press, 2006.
157. C. I. Lee, A. H. Haims, E. P. Monico, J. A. Brink, and H. P. Forman, Radiology 231, 393 (2004).158. D. J. Brenner and E. J. Hall, N. Engl. J. Med. 357, 2277 (2007).159. J. Hausleiter, T. Meyer, F. Hermann, M. Hadamitzky, M. Krebs, T. C. Gerber, C. McCollough, S. Martinoff,
A. Kastrati, A. Schomig, and S. Achenbach, JAMA 301, 500 (2009).160. Z. Sun and K. H. Ng, Singapore Med. J. 51, 374 (2010).161. A. J. Einstein, M. J. Henzlova, and S. J. Rajagopalan, JAMA 298, 317 (2007).162. International Atomic Energy Agency, International Basic Safety Standards for Protection against Ionizing
Radiation and for Radiation Sources, Safety Seriesb No. 115-1 (Vienna: IAEA) (1994).163. United Nations Scientific Committee on the Effects of Atomic Radiation. Sources, Effects and Risks of
Ionizing Radiation, v. I (NY: UNSCEAR, United Nations) (2000), p. 202.164. Z. Sun, K. H. Ng, and A. Vijayanthan, Singapore Med. J. 51, 200 (2010).165. F. P. Castronovo, Jr. and R. Schleipman, J. Nucl. Med. Tech. 27, 57 (1999).166. C. Chiesa, V. De Sanctis, F. Crippa, M. Schiavini, C. E. Fraigola, A. Bogni, C. Pascali, D. Decise,
R. Marchesini, and E. Bombardieri, Eur. J. Nucl. Med. 24, 1380 (1997).167. N. A. Benatar, B. F. Cronin, and M. J. O’Doherty, Eur. J. Nucl. Med. 27, 583 (2000).

Medical Imaging of the Heart and Cardiovascular System 239
168. T. M. Lundberg, P. J. Gray, and M. L. Bartlett, J. Nucl. Med. Tech. 30, 25 (2002).169. C. D. Greaves and W. B. Tindal, Nucl. Med. Commun. 20, 179 (1999).170. L. K. Harding, A. B. Mostafa, and W. H. Thomson, Nucl. Med. Commun. 11, 271 (1990).171. R. Smart, Radiat. Prot. Dosim. 109, 201 (2004).172. F. A. Mettler, W. Huda, T. T. Yoshizumi, and M. Mahesh, Radiology 248, 254 (2008).173. M. Schwaiger, S. I. Ziegler, and S. G. Nekolla, Eur. J. Radiol. 73, 494 (2010).174. T. H. Wu, Y. H. Huang, J. J. Lee, S. Y. Wang, S. C. Wang, C. T. Su, L. K. Chen, and T. C. Chu, Eur. J. Nucl.
Med. Mol. Imaging 31, 38 (2004).
